
Abstract
Telemetric monitoring is used in many scientific fields, such as cardiovascular research, neurology, endocrinology, as well as animal welfare research. Nowadays, implanted electrocardiogram (ECG) radiotelemetry units are the gold standard for monitoring ECG traces, heart rate and heart rate variability in freely moving mice. Telemetry technology can be a valuable tool when studies utilize it adequately, while prioritizing animal welfare. Recently, concerns have been raised in many research fields, including animal research, regarding the reproducibility of research findings, with insufficient reporting being one of the underlying causes.
A systematic review was performed by making use of three literature databases, in order to include all publications until 31.12.2019, where the surgical placing of ECG recording telemetry devices in adult mice was involved. Data extracted from the publications included selected items recommended by the ARRIVE guidelines. We focused on aspects related to the refinement of the surgery and experimental conditions that aim to improve animal welfare. In general, the quality of reporting was low in the analyzed 234 publications. Based on our analyses, we assume there has been no improvement in this field’s reporting quality since 2010 when the ARRIVE guidelines on reporting were introduced. Additionally, even though expert recommendations on telemetry surgery refinement have been available since many years now, no increase in uptake (or reporting) of these measures prior (e.g., acclimatization), during (e.g., asepsis) or after (e.g., social housing) the surgery could be observed.
The advantages of telemetry for monitoring physiological processes in animals are as follows: unrestricted, continuous data collection, reduction of animal numbers – that is, in multiple-use studies 1 – and the elimination of confounding effects of repeated handling, restraint and anesthesia for data acquisition.2,3 Nowadays, implanted ECG radiotelemetry units are the gold standard for monitoring ECG traces, heart rate and heart rate variability in freely moving mice. Recently, concerns regarding the reproducibility of research findings have been raised in many scientific fields, including animal research,4–7 which may also affect ECG studies. Several factors have been identified to contribute to poor reproducibility – for example, inadequate study design and analysis, as well as insufficient reporting of methods and results. 8 Specifically, proper reporting enables readers to evaluate the quality and conclusions of studies, permits critical reviews, showcases adherence to animal welfare norms and guides other scientists on how to conduct and refine their experiments. Unfortunately, studies show that the quality of reporting remains inadequate in many fields.9–14 This may impair the scientific value of animal experiments and, therefore, may affect their ethical justification. In an effort to improve the quality of animal experimental reporting, the ARRIVE guidelines 4 were published. These guidelines support a more structured approach to reporting of animal experiments, by recommending the format and content of details relating to the animals and the experimental procedure. In 2020, a revision and a detailed explanation of the guidelines were published. 15 In a previous systematic review, on the same set of publications, 16 we analyzed the technical reporting quality in the field of mouse ECG radiotelemetry studies, before and after the ARRIVE guidelines publication, focusing on animal and husbandry characteristics, statistical reporting and measures to avoid bias, as well as some selected ECG radiotelemetry study characteristics. In general, the quality of reporting was low to moderate in the 234 analyzed publications and no improvement was observed in the reporting quality since 2010, when the ARRIVE guidelines were introduced.
Despite the obvious scientific advantages, as well as the potential reduction and refinement opportunities that radiotelemetry offers, it is important to keep in mind that radiotelemetry transponder implantation is a complex, major surgery that may have negative impact on the animals, including post-surgical pain and distress. Additionally, some experimental set-ups for telemetric measurements require the single housing of animals, which in the case of social species like mice can be considered a serious animal welfare issue. Already in 2003, a working group of experts addressed the justification and advantages of radiotelemetry technology in animals. The group’s reports17,18 included recommendations on refinements of the implantation surgery and the experimental housing conditions, as well as suggestions on adequate reporting of methods and results of radiotelemetry studies. In 2014, Hawkins 19 reviewed the most important recommendations of these reports and summed up important considerations regarding new technological developments in the field of radiotelemetry, focusing on potential refinements of housing conditions (i.e. social housing). Taking together the ARRIVE guidelines, the working group reports, as well as Hawkins’ update, practical guidance on refinement and proper reporting has been available for almost two decades now in the field of radiotelemetry studies.
In this systematic review, we therefore focus on the quality of reporting of essential refinement measures implemented in ECG radiotelemetry studies in mice prior (e.g. sufficient acclimatization time, social housing), during (e.g. aseptic techniques, gentle surgery techniques, anesthesia, heat supply) and after the implantation surgery (e.g. analgesia, pain and welfare assessment, social housing, humane endpoints) (see supplementary Table 2 for details). We analyze the (reported) uptake of refinement measures in the field of ECG radiotelemetry studies and identify potential improvements for reporting. To compare the actual reporting quality and refinement implementation, we included articles published before and after the publication of the first ARRIVE guidelines in 2010.
Materials and methods
A systematic review protocol was designed according to SYRCLE (Systematic Review Center for Laboratory Animal Experimentation) guidelines; the protocol and search string were registered before the study commenced, on two platforms (see supplementary material).
Search strategy
Supplementary Table 1 displays the search strategy, as well as the total hits that each literature database (PubMed Central, Web of Science, Embase) yielded. Search terms were chosen to identify all published articles that used the implantation of ECG recording telemetry device in mice and included all publications until 31 December 2019.
Selection of publications
Original articles published until 31 December 2019, which made use of implantable ECG recording telemetry devices in adult mice older than six weeks of age, irrespective of strain or sex, were included (see Figure 1). The following items were excluded: (i) studies not using implantable ECG telemetry devices or using partially implanted telemetry (e.g. tethered devices); (ii) all secondary publications (e.g. reviews); (iii) publications written in languages other than English; (iv) publications dating after 31 December 2019; and (v) studies using other species or mice younger than six weeks of age at the time of implantation. The inclusion/exclusion procedure was performed by two reviewers. Discrepancies during the title/abstract screening were discussed until a consensus was reached. Endnote Web was utilized to manage all publications.
Data extraction
Selected publications were evaluated and items to be extracted (supplementary Table 2) were recorded in Excel. During this phase, additional publications were excluded since they fulfilled the exclusion criteria, or the full text could not be retrieved (two publications). When supporting information was available online, it was evaluated, and the containing data extracted. If a publication referenced another publication regarding aspects related to the inclusion criteria, then the referenced publication was retrieved, evaluated and the relevant data extracted.
A broad array of study characteristics was retrieved (supplementary Table 2), which were considered important regarding the ECG telemetry device implantation refinement (e.g. anesthesia, analgesia, asepsis, social housing). The analyzed refinement measures have been recommended to be implemented and reported by an expert report 19 and the ARRIVE guidelines, 4 to allow for comparisons between manuscripts published until and after 2010 when the ARRIVE guidelines were introduced. Analysis of all publications was performed by one reviewer, and a randomly chosen 25% of the included publications were analyzed by an additional reviewer. Discrepancies were discussed until a consensus was reached.
Scoring procedure
Scores (0–1, 0–1–2, 0–1–2–3) were applied to allow for comparisons of specific items. Details on the scoring procedure for each item can be found in supplementary Table 2. For simple yes/no decisions, items were either reported or not (score 0–1) – for example, the duration of surgery was reported (score 1) or not mentioned (score 0). For items that could be reported in differing detail, items were not reported or reported in increasing detail (score 0–2 or 0–3) – for example, aseptic technique not mentioned (score 0), mentioned but not described (score 1) or aseptic technique described in detail (score 2). In the latter cases, scores below the maximum are described as insufficiently reported.
Completeness scores using the results for measures prior, during and after surgery were calculated for comparisons between the two timeframes (until 2010 vs 2011–2019). We considered the reporting for each group of measures as well as the complete reporting ‘low’ whenever more than half of the publications reached less than half of the maximum score; ‘moderate’ was considered when more than half of the publications reached at least half of the maximum score, and for ‘good’ reporting we expected at least half of the publications to reach three quarters of the maximum score.
Data analysis
Mean ± standard deviation and median completeness scores were calculated for each time span. No further statistical analyses have been performed.
Results
The searches yielded a number of 234 (124 vs 110) relevant studies (Figure 4).
Measures implemented prior to the ECG telemetry implantation surgery
For an overview of the measures implemented prior to the ECG telemetry implantation surgery, see Figure 1.
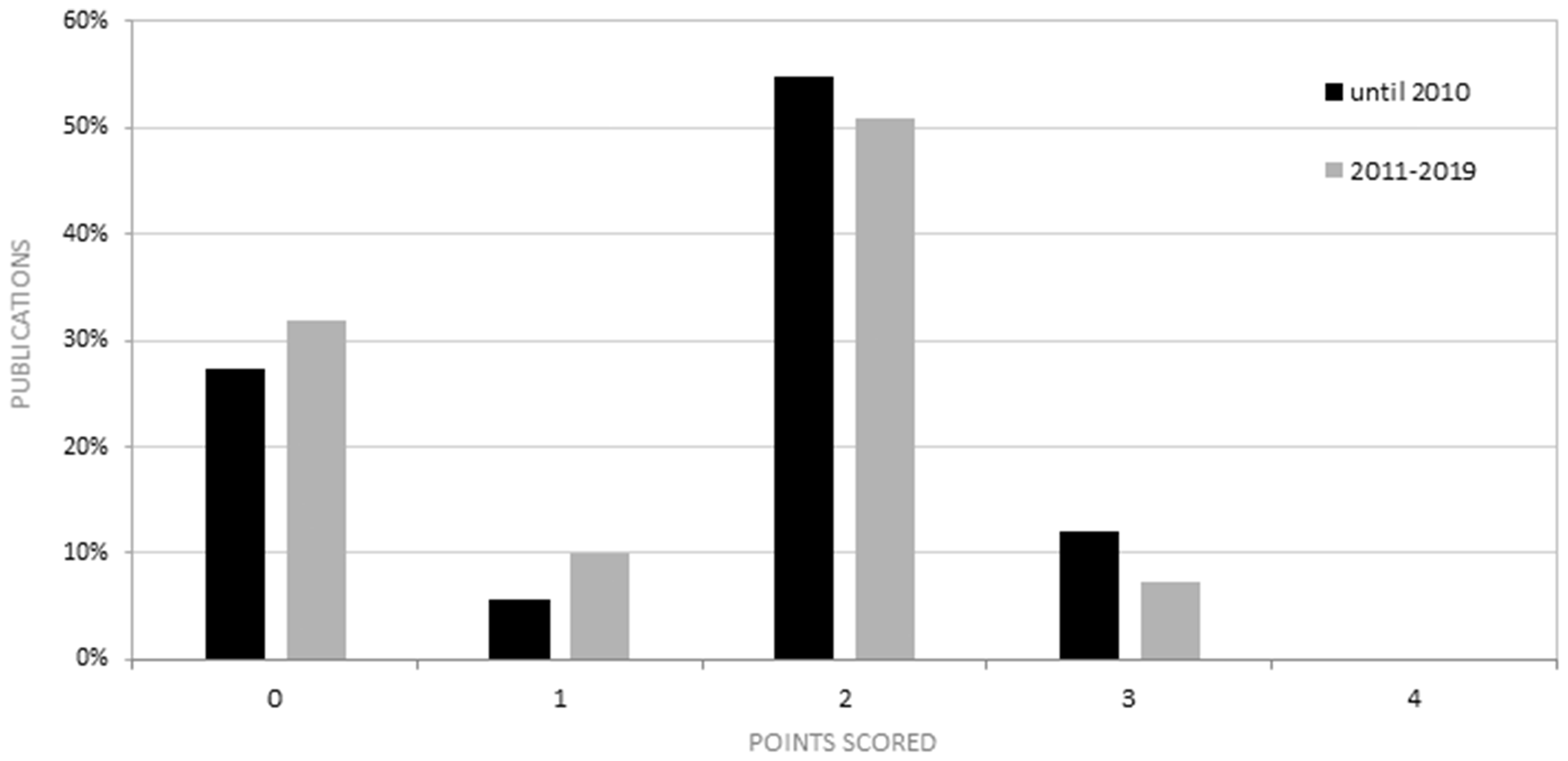
Percentage of publications published until 2010 vs 2011–2019, and the corresponding ‘Measures prior implantation completeness score’ (0–4). No improvement is observed in reporting these aspects.
Acclimatization
More than half of publications reported acclimatization in detail (78/124 vs 63/110). When animals from an external breeder were ordered, mean acclimatization periods of at least one week (10/18 vs 4/10) or more than two weeks (8/18 vs 6/10) were reported.
Housing prior to the implantation surgery
Few publications reported how animals were housed (22/124 vs 16/110), with four between 2011 and 2019 reporting single housing prior to the implantation surgery.
Other refinements prior the implantation surgery
No additional refinement measures prior to the implantation surgery were reported.
Measures implemented during the ECG telemetry implantation surgery
For an overview of the measures implemented during the ECG telemetry implantation surgery, see Figure 2.
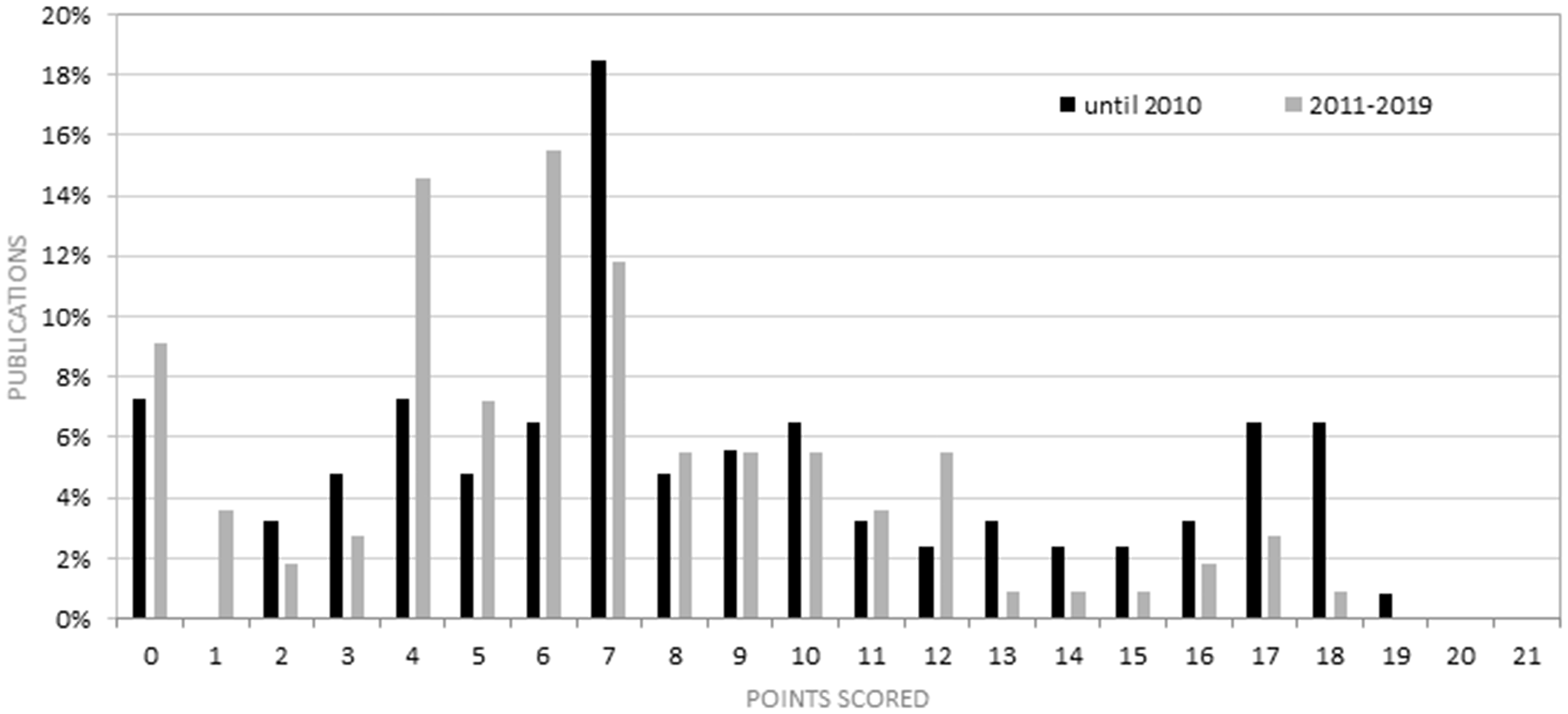
Percentage of publications until 2010 vs 2011–2019, and the corresponding ‘Refinements during implantation surgery completeness score’ (0–21), with no improvement for 2011–2019.
Aseptic technique
Few publications reported sufficiently on the aseptic technique (26/124 vs 8/110), while the remaining publications failed to provide any sufficient information. Hair removal methods were reported, as well as the use of antiseptic and cleaning solutions (e.g. povidone iodine, alcohol or both), the equipment and room sterility (e.g. sterile draping, surgical instruments, transmitters, surgical field, gloves) and disinfected surgical table.
Anesthesia
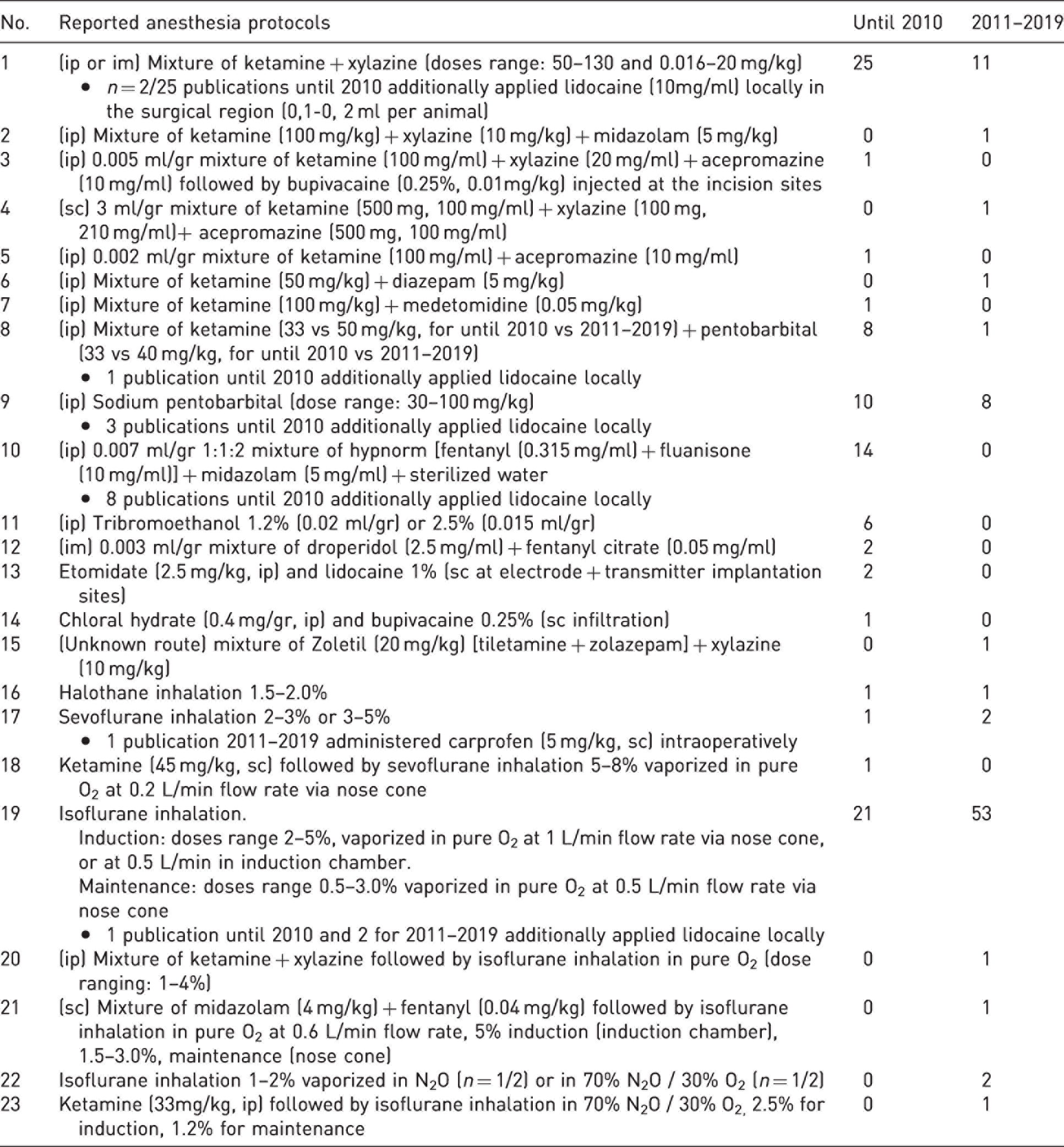
Many publications reported the type, route of administration and dose of anesthesia (type: 95/124 vs 82/110; route: 87/124 vs 77/110; dose: 83/124 vs 60/110). A total of 23 different anesthesia protocols were reported (see Table 1). While until 2010 ketamine with xylazine (25/95 used alone, 2/95 in combination with other agents) or isoflurane inhalation only (21/95) were most often used, and isoflurane inhalation with or without other agents (53/82 alone, 5/82 in combination with other agents) was more frequently used between 2011 and 2019.
Anesthesia protocols reported including preoperative or perioperative analgesia treatments and the number of publications that reported them for each timeframe, as well as the dose and route of application for each method.
Basic aspects of the surgical technique
Location of the telemetry transmitter implantation
Most publications sufficiently reported the implantation site of the transmitter, with a considerably lower number between 2011 and 2019 (102/124 vs 73/110). Publications providing insufficient information either stated insertion in a subcutaneous pocket without reporting the exact site, or reported two different sites for the same protocol. The reported implantation sites were subcutaneous dorsal (cervical, caudal, lateral), ventral (caudal, lateral) or in abdominal pocket, as well as intra-abdominal.
Location of the ECG electrode lead placement
Most publications reported the location of lead placement sufficiently, but less so between 2011 and 2019 (100/124 vs 79/110). The publications that provided insufficient information either only stated that the leads were subcutaneously placed or gave an approximate position. The three different reported lead placement configurations in decreasing frequency were: lead II, lead I and MX deflection.
Location and width of incision
Few publications reported the location and width of incision, with less publications reporting between 2011 and 2019 (location: 46/124 vs 23/110; width: 27/124 vs 9/110). The reported incision width ranged from 1 to 3 cm. While the site was dependent on the location of the transmitter implantation, the midline incision of the lower abdominal wall was most frequently reported.
Transmitter body and electrode leads anchoring material
Only a few publications sufficiently reported on these aspects, with even less reporting the type (e.g. suture/glue or brand name) and nature (e.g. absorbable, non-absorbable) of the material between 2011 and 2019 (32/124 vs 5/110). The types of anchoring material were non-absorbable suture, suture of unknown nature, glue suture of unknown nature and absorbable suture. The reported non-absorbable sutures were Silk, Perma-Hand, Prolene and Ethilon, with gauge size ranging from 4-0 to 7-0. The reported absorbable sutures were Vicryl and Monofilament, with gauge size ranging from 4-0 to 6-0. The reported glue was Vetbond surgical superglue or veterinary tissue adhesive.
Skin closure material
Few publications reported the skin closure material (28/124 vs 8/110). The reported types of anchoring material were absorbable suture, suture of unknown nature, non-absorbable suture, staple clips, staple clips + non-absorbable suture, glue + non-absorbable suture and glue + absorbable suture. The reported non-absorbable sutures were Silk and Prolene, with gauge size ranging from 4-0 to 6-0. The absorbable sutures were Dexon II, Vicryl and PDS, with gauge size ranging from 2-0 to 6-0. The glue was reported as Vetbond surgical superglue.
Mean surgery duration
The number of publications reporting the mean surgery duration was low (16/124 vs 3/110). Reported surgery durations ranged from 20 to 60 min.
Refinements during the ECG telemetry implantation surgery
Refinement of the surgical methodology
Few publications addressed this aspect (22/124 vs 10/110). The most frequently reported refinement was covering the tip of the electrode’s lead metal end with a plastic tube to protect the tissue from irritation. Eye moisturizing during surgery was addressed only by two publications.20,21 Only one publication reported time and place of conducting the procedure, 21 one publication 22 reported measures to avoid perforation of the intestines and measures to keep the surgical site moist, one 23 reported application of neomycin before closing the incision and one publication 22 reported measures to avoid post-surgical skin and tissue irritation.
Temperature maintenance during implantation surgery
Few publications reported on temperature maintenance sufficiently (5/124 vs 5/110). Most frequently reported were heating pads and, less frequently, heating blankets, warming plates and heated tables. Reported temperatures ranged from 36 to 39°C.
Monitoring during the implantation surgery
Most publications failed to report monitoring of anesthesia depth (not reported: 120/124 vs 101/110). Four out of the 124 publications until 2010 and 9/110 between 2011 and 2019 have reported monitoring practice.
Measures implemented after the ECG telemetry implantation surgery
For an overview of the measures implemented after the ECG telemetry implantation surgery, see Figure 3.
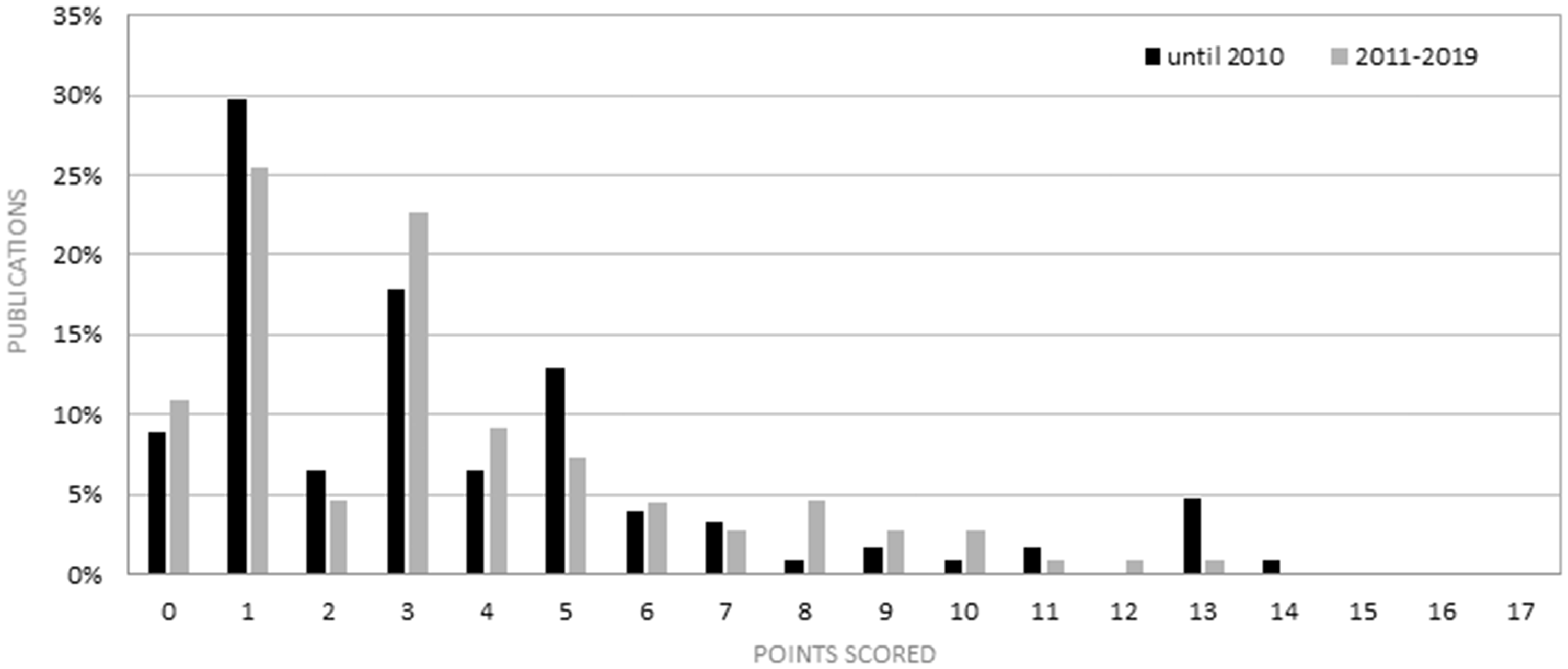
Percentage of papers published until 2010 vs 2011–2019, and the corresponding ‘Measures implemented after the implantation completeness score’ (0–17), which refers to all of the aspects reported under this category. No overall improvement can be observed in reporting these aspects after the publication of the ARRIVE guidelines.
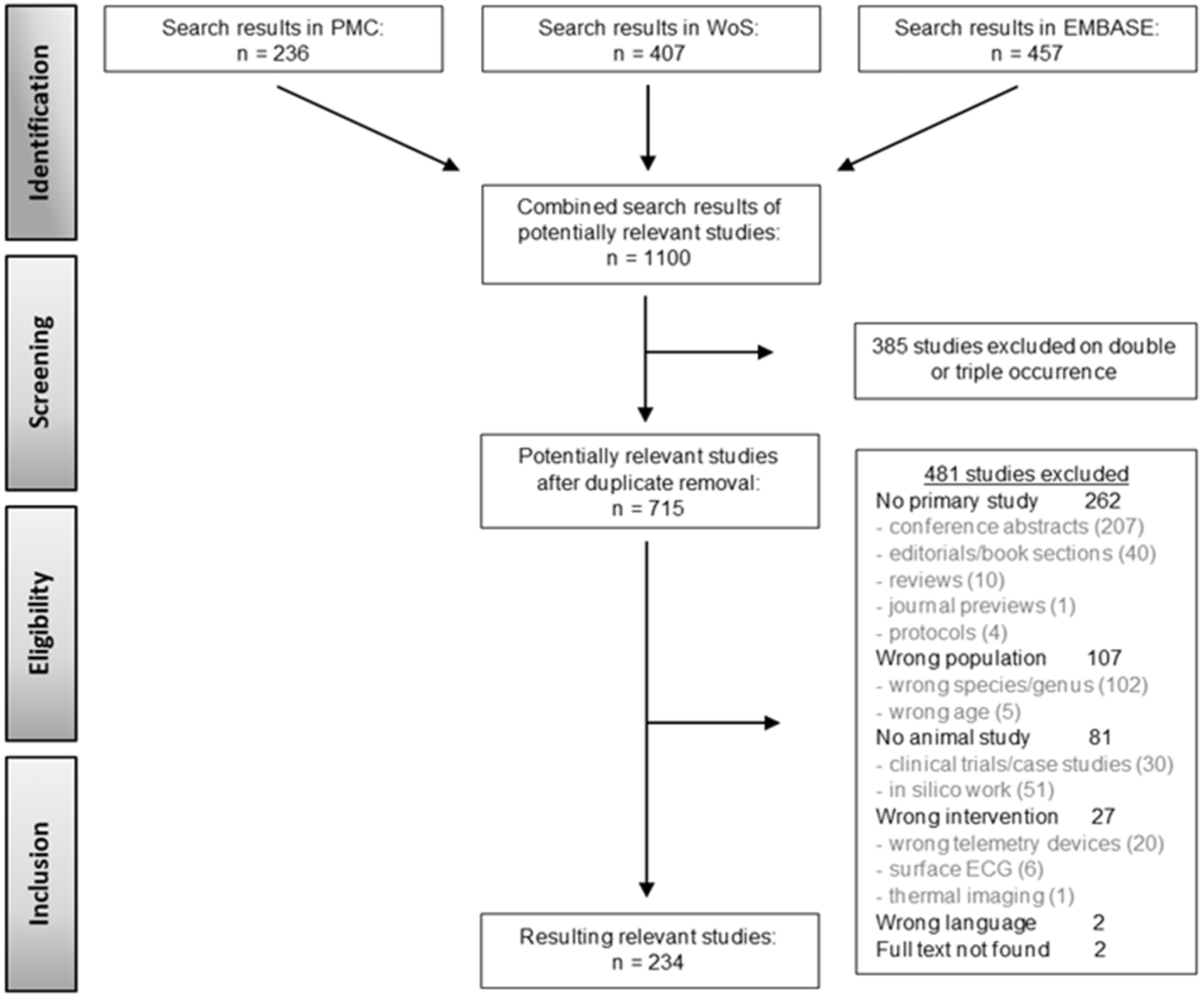
Flow diagram of the systematic literature search including the yielded results.
Analgesia
Although only a few publications reported on analgesia sufficiently, there was a moderate improvement in reporting the type, dose, route, frequency and duration of analgesia administration between 2011 and 2019 (type: 9/124 vs 30/110; route: 5/124 vs 22/110; dose: 9/124 vs 27/110; frequency: 5/124 vs 13/110; duration: 6/124 vs 15/110). Eleven different analgesia regimes were reported (Table 2). Four publications until 2010 stated that no further analgesia was applied after surgery or ‘it was not considered necessary for the animal to be given any postoperative analgesics’.
Analgesia regimes mentioned by publications that reported the type of analgesia.
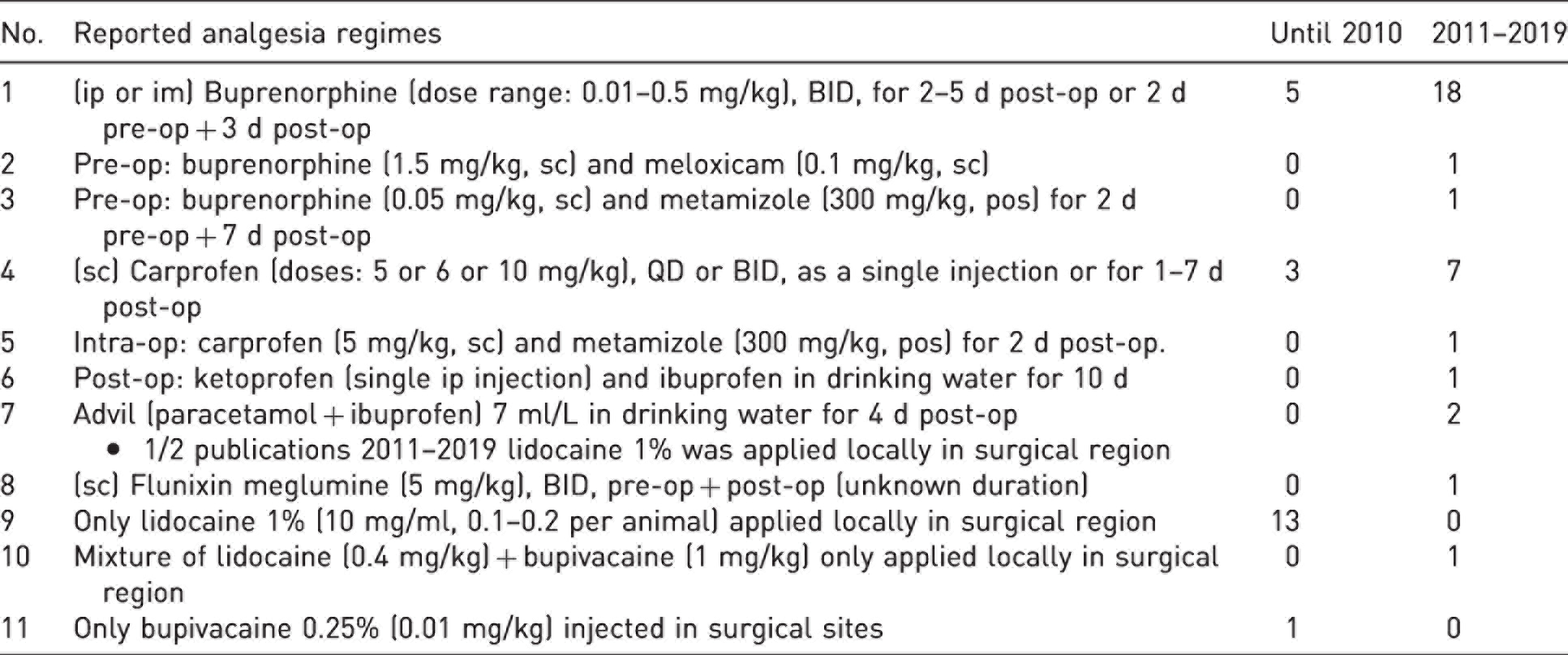
Five out of the 124 publications before 2010 and 21/110 between 2011 and 2019 reported applying preoperative analgesia. As it can be observed from supplementary Table 3, perioperative analgesia was mostly confirmed by pain reflexes suppression, such as no increase in heart rate (monitored via surface ECG), lack of paw withdrawal reflex and absence of irregular or sudden changes in breathing frequency. Publications reporting on the matter were very few (4/124 before 2010 and 11/110 between 2011 and 2019). Some publications reported applying intra-operatively local anesthetics in the surgical region. Specifically, 13/124 publications before 2010 and 1/110 between 2011 and 2019 applied lidocaine 1%, one study between 2011 and 2019 applied a mixture of lidocaine + bupivacaine and one before 2010 applied bupivacaine 0.25%.
Antibiotic prophylaxis
Antibiotic regimes have been reported by 7/124 publications until 2010 and 4/110 between 2011 and 2019. A total of five antibiotic regimes were reported, gentamicin sulfate was most popular in both timeframes, chlortetracycline gained popularity after 2011, and enrofloxacin and amoxicillin were used only before 2010. One study reported applying perioperatively neomycin sulfate in the surgical region before closing the incision. 23
Temperature maintenance during recovery
A minority of publications between 2011 and 2019 reported this refinement (22/124 vs 9/110), and few reported two or more of the following aspects: temperature range, duration or method of temperature maintenance (3/124 vs 5/110). The most frequently reported method was infrared warming lights (34–37°C; 30 min to 24 h post-op), followed by heating pads (32–38°C; 30 min to 48 h post-op).
Other postoperative refinements and environmental enrichment
The number of publications reporting any additional refinements after the implantation surgery is low (13/124 vs 4/110). Reported additional refinements were fluid therapy (n = 2), provision of Solid Drink® and moistened food pellets (n = 1), nesting material (n = 7) and minimization of disturbance of the animals and placing animals in their familiar home cage after the surgery (n = 2). Some publications implemented enrichment as part of their study protocol and not as refinement (n = 3).
Recovery time before commencing measurements
Most publications reported the recovery time before measurements began (110/124 vs 90/110). The reported recovery time ranged from 0 to 96 days. The most frequently reported recovery times in both timeframes were one or two weeks.
Housing after the implantation surgery
Some publications sufficiently reported single or group housing after the implantation surgery (38/124 vs 40/110). Three of the 124 publications until 2010 and none between 2011 and 2019 reported group housing during the entire time the animals spent in the laboratory. Several publications reported single housing during recovery, but group housing – for example, in same-sex groups or with an ovariectomized female companion – during the actual experimental measurements. All other publications reported single housing during recovery, as well as later during the experiments.
Pain and welfare assessment
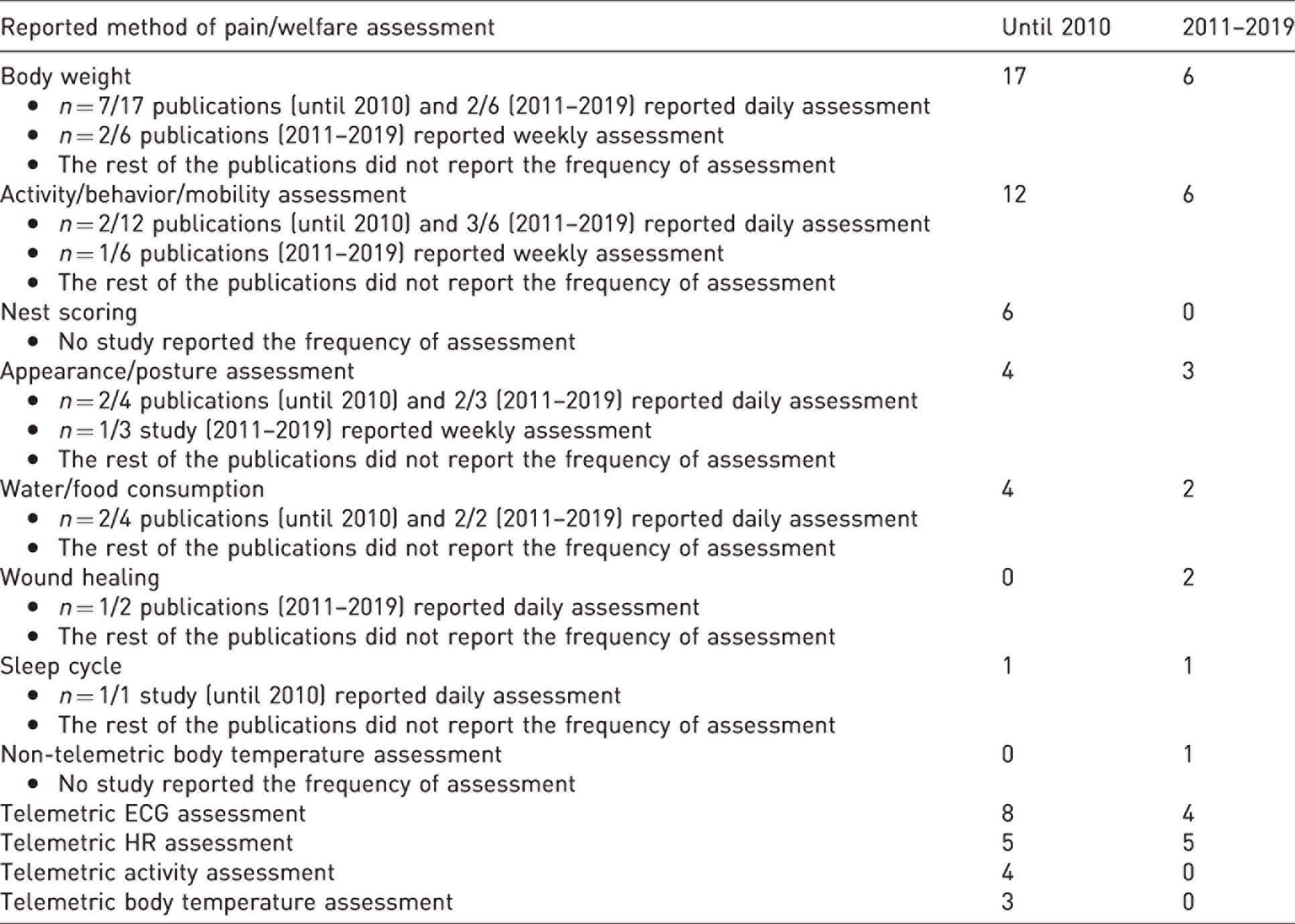
The number of publications that reported pain/welfare assessment and the methods utilized was lower between 2011 and 2019 (47/124 vs 24/110) (Table 3). Different methods were reported – for example, activity/behavior/mobility, nest building, weight loss, appearance/posture, water/food consumption, sleep cycle, as well as non-telemetric body temperature and telemetric ECG/heart rate/activity/temperature. A small number of publications reported that the animals were inspected or monitored during recovery, but failed to mention the methods used (3/124 vs 3/110).
Reported methods of postsurgical pain and welfare assessment. The number of publications reporting, as well as the frequency of assessment, is depicted for each method.
Humane endpoints
Only three publications between 2011 and 2019 reported the use of humane endpoints compared to none until 2010. Among these three publications, signs of distress, lethargy, labored breathing, refusal to eat or drink, significant weight loss, restlessness, impaired mobility, licking or wound guarding, failure to groom or open sores served as humane endpoints.
Euthanasia
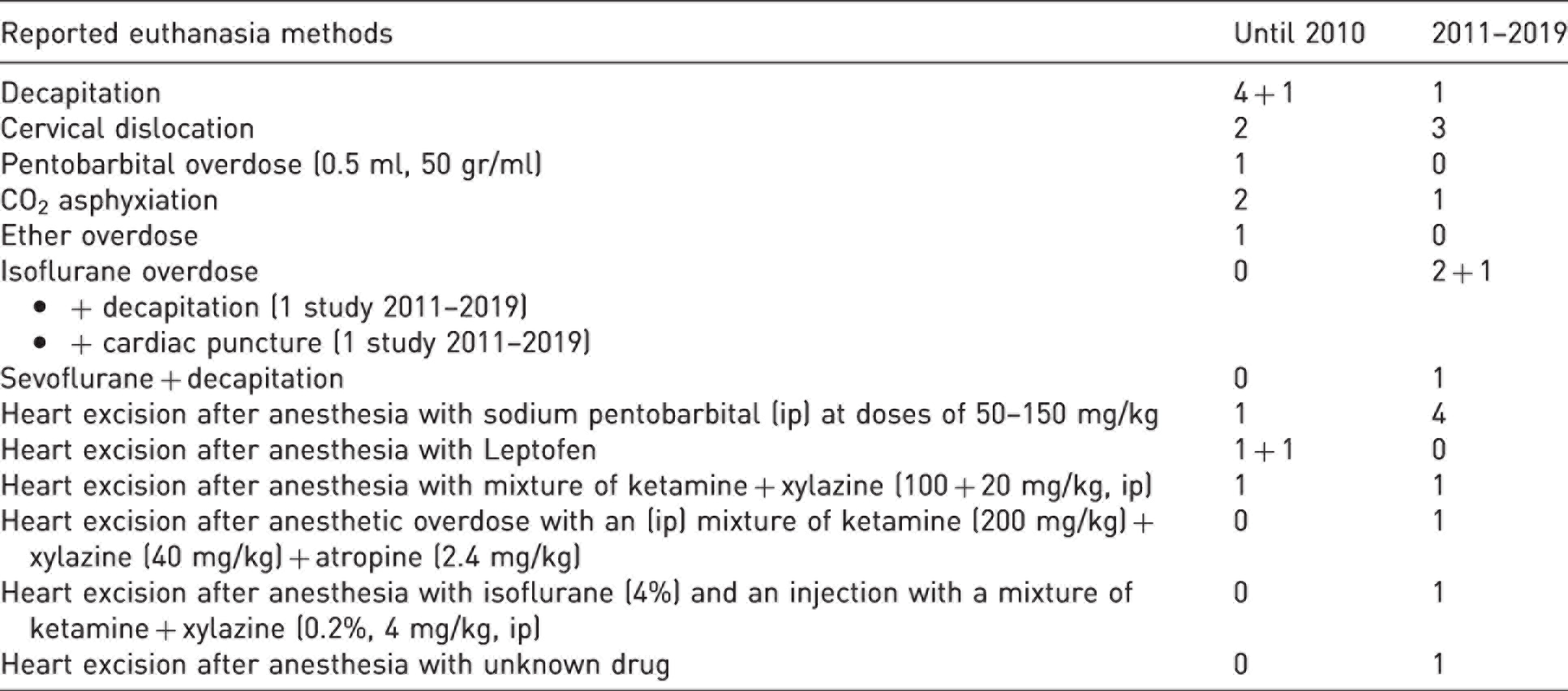
The number of publications that reported euthanasia, as well as the methods used, was higher between 2011 and 2019 (14/124 vs 16/110). Most publications did not report euthanasia at all. A shift is observed from purely mechanical methods to methods where an anesthetic agent is used (Table 4).
Reported euthanasia procedures and the number of publications that reported them. The numbers +X refer to two publications (one until 2010 and one for 2011–2019) that reported the use of two different methods.
Ethical statement
Most publications provided an ethical statement, with more doing so between 2011 and 2019 (102/124 vs 107/110). Between 2011 and 2019, more publications reported having a committee approval of the study protocol, compliance with a specific guideline and/or stating a license number.
Discussion
Transmitter implantation is a complex and, in most cases, major surgery that induces post-surgical pain and distress. Best practice surgical techniques, effective asepsis, anesthesia and analgesia, good peri-operative care, sensitive welfare monitoring, as well as appropriate housing and care are paramount. This has been repeatedly acknowledged by several publications.17–19 Taking into account the above, as well as the publication of the first ARRIVE guidelines in 2010, 4 one could expect a high level of reporting of best practice methods and refinements, especially in more recent publications. Unfortunately, we observed a relatively low reporting quality (a score below 15 (of 34) in the mean completeness score), with no obvious improvement after 2010, neither for items explicitly mentioned by the ARRIVE guidelines, nor in more ‘ECG surgery specific’ refinement items.
Reporting of refinement measures implemented prior to the ECG implantation surgery was, in general, low to moderate (more than half of the publications scored 0–2 out of 4 points). No improvement after 2010 was observed. It is recommended that mice transferred from external rodent colonies should arrive at the facility at least two weeks before the surgery in order to adapt to the environment and to avoid transportation stress that may skew the readouts. 24 More than half of the publications in both timeframes failed to report acclimatization. One week of acclimatization was just as frequently reported as two weeks or more. Acclimatization was, nevertheless, one of the few more frequently reported refinements. Most publications failed to indicate whether they housed animals alone or in groups before the surgery, and no other refinements were reported.
No notable improvement was observed after 2010 in the reporting of refinement measures implemented during the ECG implantation surgery. In summary, the reporting quality was low to moderate (more than half of the publications scored 0–10 out of 21 points). While anesthesia protocols and information on the implantation location of the transmitter device were described by most publications, little information was given on asepsis, incision size, wound closure surgery duration or refinements like temperature maintenance and anesthesia monitoring. This is unfortunate, as such information may give insights into the severity of the procedures and may help to identify potential for refinement.
Most publications failed to provide any information on the aseptic technique they used, despite its importance for surgical success and animal welfare. 17 Implant and skin must be diligently disinfected and only sterile materials should be used during surgery. 17 It is peculiar that a few publications stated using only alcohol and no other disinfectant to prepare the skin. Only a small number of publications addressed transmitter or equipment sterility.
Since cardiovascular parameters can be impacted by anesthesia, 24 anesthesia details are, therefore, of interest in studies using telemetry. The fact that at least two thirds of the publications are reporting anesthesia details is encouraging. While tribromoethanol etomidate and chloralhydrate were used in older publications, none of these have been reported after 2010, which is likely due to their unfavorable anesthetic profile and adverse effects compared to modern agents. Nowadays, low-solubility volatile anesthetics such as isoflurane are considered agents of choice, as they permit effective control of anesthesia depth, are rapidly eliminated and are not (or only minimally) metabolized. 17 This is reflected by the shift from the most used anesthetic agent until 2010 being equally ketamine with xylazine or isoflurane, to the most popular protocol between 2011 and 2019 being mainly isoflurane. Still, it must be kept in mind that isoflurane has no to little lasting analgesic effect.25–27 The fact that very few publications stated additional preemptive analgesia is, therefore, worrying.
Most publications stated the location of the device body implantation, with the most prominent being in the peritoneal cavity or in a dorsal subcutaneous position. In both cases, implantation should be followed by secured lead placement, which was reported in many publications, while care should be taken to prevent seroma, hematoma and migration of the implant. 17 Although subcutaneous implants are generally well tolerated by mice, large subcutaneous implants can cause discomfort and pressurize adjacent tissue, resulting in necrosis of the overlying skin, leading to seromas, infection, dehiscence and sinus formation. 17 This is why larger devices should preferably be situated in the peritoneal cavity. 17 The popularity of intraperitoneal implantation can be explained by the use of devices representing up to more than 10% of the animal’s mass, which were often reported. 16
The transmitter body and electrode leads should be anchored to avoid dislocation or migration while the animal is moving, which is why using inert non-absorbable sutures is recommended. 17 The device body should not be tied to muscle fibers, but to the muscle facia 17 for a secure anchoring without possible hematoma, granulation or scar tissue forming, 28 a refinement reported only by a few publications. Most publications failed to report on the anchoring material they used; non-absorbable sutures were more frequently reported, while several publications between 2011 and 2019 reported using absorbable sutures. The skin closure material was underreported, with absorbable sutures being most frequently reported.
Keeping surgery as short as possible and warming and monitoring the anesthesia carefully can reduce the burden for the animals, but unfortunately only a few publications reported these aspects. Body temperature maintenance during surgery is crucial, since anesthesia can inhibit the body’s ability to maintain normothermia,29–32 especially in small rodents, resulting in hypothermia, potentially leading to delayed recovery 31 and increased rates of postoperative infections and coagulopathies.33–35 Inadequate general anesthesia may lead to intraoperative awareness of the animals due to underdosage, or to delayed recovery and increased risk of postoperative complications due to overdosage. 36 Monitoring of anesthesia depth and vital signs during surgery is, therefore, important, yet still a remarkably large percentage of publications failed to report on this aspect. Also, other measures that should be considered standards of rodent surgery, like the use of eye ointment, were rarely reported.
Only a slight improvement can be observed in reporting refinement measures implemented after the surgery, but in general reporting was rather low (more than half of the publications scored 0–8 out of 17 points). Analgesia is the cornerstone to safeguard animal welfare when surgery is involved. If pain is not controlled it causes suffering, interferes with physiological parameters and can slow the healing process, 37 which could lead to aberrant study outcomes. Also, analgesia as such can of course have undesired effects on study outcomes. 25 That is why reporting the type, dose, route, frequency and duration of analgesia administration not only displays compliance with animal welfare practices, but also assists with reproducibility. 25 Unfortunately, reporting on all aspects of analgesia was lower than anesthesia reporting, with a slight improvement after the ARRIVE guidelines publication. For the reported protocols, an increase in the use of injectable buprenorphine and carprofen is observed between 2011 and 2019, either alone or followed by meloxicam or metamizole. Most publications describe a treatment duration of three to seven days, which seems appropriate for an implantation surgery. Nevertheless, some reported only perioperative, short-term analgesia – that is, local anesthetics applied at the surgical region or treatment durations of only one to two days, while several publications even mentioned that no further analgesia was applied after surgery38,39 or that ‘it was not considered necessary for animal to be given any postoperative analgesics’. 40 The European Union (EU) Directive 2010/63 assigns the surgical implantation of telemetry transmitters to the ‘moderate’ severity classification, as long as appropriate analgesia is given. 41 According to the EU Directive, the implantation procedure without the use of analgesia is considered ‘severe’. It is, therefore, difficult to justify analgesia withdrawal in these kind of surgeries.
Postoperative antibiotics can protect the animal from possible infections. Broad-spectrum prophylactic antibiotics can be justified, in case of extensive surgery. 17 Unfortunately, most publications failed to report whether antibiotic prophylaxis was utilized or not.
Other refinement measures were rarely reported. Specifically, regarding temperature maintenance, which is an essential aspect of recovery and mortality, 41 the temperature range, duration or method were hardly reported. Prevention of dehydration with fluid therapy (sc sterile saline) is recommended, but was described by only two publications.21,22 Restoration of normal feed and water intake by offering soft and/or high caloric food can support recovery.20,42 Unfortunately, only Kramer at al. 20 reported that, in addition to standard food and water, animals received Solid Drink® and moistened food for several days. Although appropriate nesting material is important for efficient thermoregulation, 43 it was reported only in studies until 2010. Environmental enrichments such as nest boxes or running wheels were only mentioned as part of experimental study protocols and not in regards to animal welfare. Kramer et al. 20 and Arras et al. 21 reported that the animals were placed back in their home cage after surgery, to recover in a familiar environment, which might be beneficial for recovery. 44 The recovery time was reported by most publications and ranged from one to two weeks. Some publications had telemetric measurements immediately after implantation, which can be of use for the pain and welfare assessment after surgery. This telemetric data were utilized for welfare monitoring only by four publications.21,45–47
Among the few publications which reported whether group or single housing was implemented after surgery, the percentage was slightly higher between 2011 and 2019. Unfortunately, for telemetric measurements, group housing, which is an important welfare aspect, could be a stumbling block to obtaining accurate reading as most commercially available devices transmit at the same frequency. 18 Nevertheless, there are several solutions – for example, co-housing the implanted mouse with non-implanted animals, using devices that can be switched on and off (which is a possibility for most devices) and used one at a time in group-housed animals, or using implanted data loggers with which data are recorded and then downloaded at the end of the study. 18 Finally, recent devices can surpass this obstacle48,49 and provide the possibility of group housing while collecting data from all the mice simultaneously by using different frequencies. 19 Some publications reported group housing during recovery, as well as during the study,50–52 although manipulation at the surgical sites by cage mates is possible, especially during the first days after implantation. Others21,53–56 implemented single housing during recovery only and group housed the animals during the study. A way to reduce the duration of single housing might be the use of refined suturing techniques that reduce the risk of manipulation by the animals. 17 In summary, there is significant refinement potential and a need for more uptake of social housing protocols for telemetry studies.
Welfare assessment in the form of postoperative monitoring and utilizing score sheets or telemetric measurements, provides valuable information on the general state of the animal after the implantation, helps to adapt post-surgical analgesia and to terminate experiments humanely if necessary. Most publications failed to address this matter, with lower reporting between 2011 and 2019. More general signs of impaired welfare like body weight changes and altered activity/behavior/mobility were most frequently assessed. Other signs of reduced general condition, like increased or reduced muscle tone, vocalization, orbital or nasal discharge and skin tenting due to dehydration, all of which could provide an indication on the overall state of the animals,24,57–60 were not reported. More pain-specific indicators like typical signs of abdominal pain (e.g. press, stretch and writhing)17,24,57–59 or the mouse grimace scale 60 were never mentioned. It is recommended that the health and well-being of implanted animals should be assessed at least twice daily. 17 The majority of publications reporting on the matter stated daily assessment, while the rest stated either weekly assessment – a monitoring frequency that renders adaptation of analgesia protocols or the early termination of experiments impossible and has to be regarded as insufficient – or did not report on frequency at all.
Also, our results regarding the reporting on humane endpoints appear disheartening, with 100% of publications until 2010 and 97.3% between 2011 and 2019 failing to report these. Among the three publications that stated implementing humane endpoints, Lew et al. 61 performed euthanasia when signs of distress, lethargy, labored breathing, refusal to eat/drink or a certain weight loss appeared, while Cutler et al. 62 at any sign of ill health (restlessness, impaired mobility, licking or wound guarding, failure to groom, open sores, loss of appetite or weight loss) consulted a veterinarian for treatment and euthanized the animals if no improvement occurred. Up until 2010, 16.9% of publications reported death as an endpoint, and 20.9% between 2011 and 2019. This is worrisome, since, as stated in the EU Directive 2010/63, 41 ‘the methods selected should avoid, as far as possible, death as an end-point due to the severe suffering experienced during the period before death’ and adds that ‘where possible, it should be substituted by more humane endpoints using clinical signs that determine the impending death, thereby allowing the animal to be killed without any further suffering’. Unfortunately, since a severe underreporting on mortality rates and euthanasia criteria was observed, and also no regular checks by animal care staff, as performed to our knowledge in most facilities, are reported, it remains uncertain what happened to the animals of the largest portion of publications. Our results could possibly lead to the conclusion that in some rare cases animals may have suffered for longer than necessary without being detected.
Although the choice of the most humane killing or euthanasia method is an important aspect in animal experimentation, these were rarely reported. Older publications mainly reported mechanical methods, while recent publications reported mostly chemical methods. Most frequently reported until 2010 was decapitation, and second most reported was carbon dioxide (CO2) asphyxiation. Although acceptable according to the EU Directive, there is evidence of aversion to CO2, due to clinical reports of pain at high concentrations and gasping due to air hunger experienced during exposure; therefore, CO2 is currently not considered an optimal euthanasia agent, 63 which might be the reason for it being less reported between 2011 and 2019. The most frequently reported methods between 2011 and 2019 were non-recovery interventions during anesthesia – for example, cervical dislocation, decapitation and cardiac puncture – which are all acceptable methods by the EU Directive. 41
In summary, this systematic review demonstrated that publications utilizing ECG telemetry instrumentation on mice display a rather low-quality reporting of refinements and items requested by the ARRIVE guidelines (Figure 5), with publications dating after 2010 performing in many cases worse than older publications. Publications until 2010 reached, on average, a mean completeness score of 14.6 ± 8.2 (median 13, min–max 0–34), while publications between 2011 and 2019 reached a mean completeness score of 12.4 ± 6.4 (median 12, min–max 1–30). Therefore, we assume that the impact of the ARRIVE guidelines, or other initiatives to improve reporting quality, was limited in the field of ECG telemetry. The surprisingly large number of publications in the field that underreport and probably insufficiently implement refinements is troubling, since recommendations by expert reports on telemetry methods and refinements17–19 have been available for over a decade now.
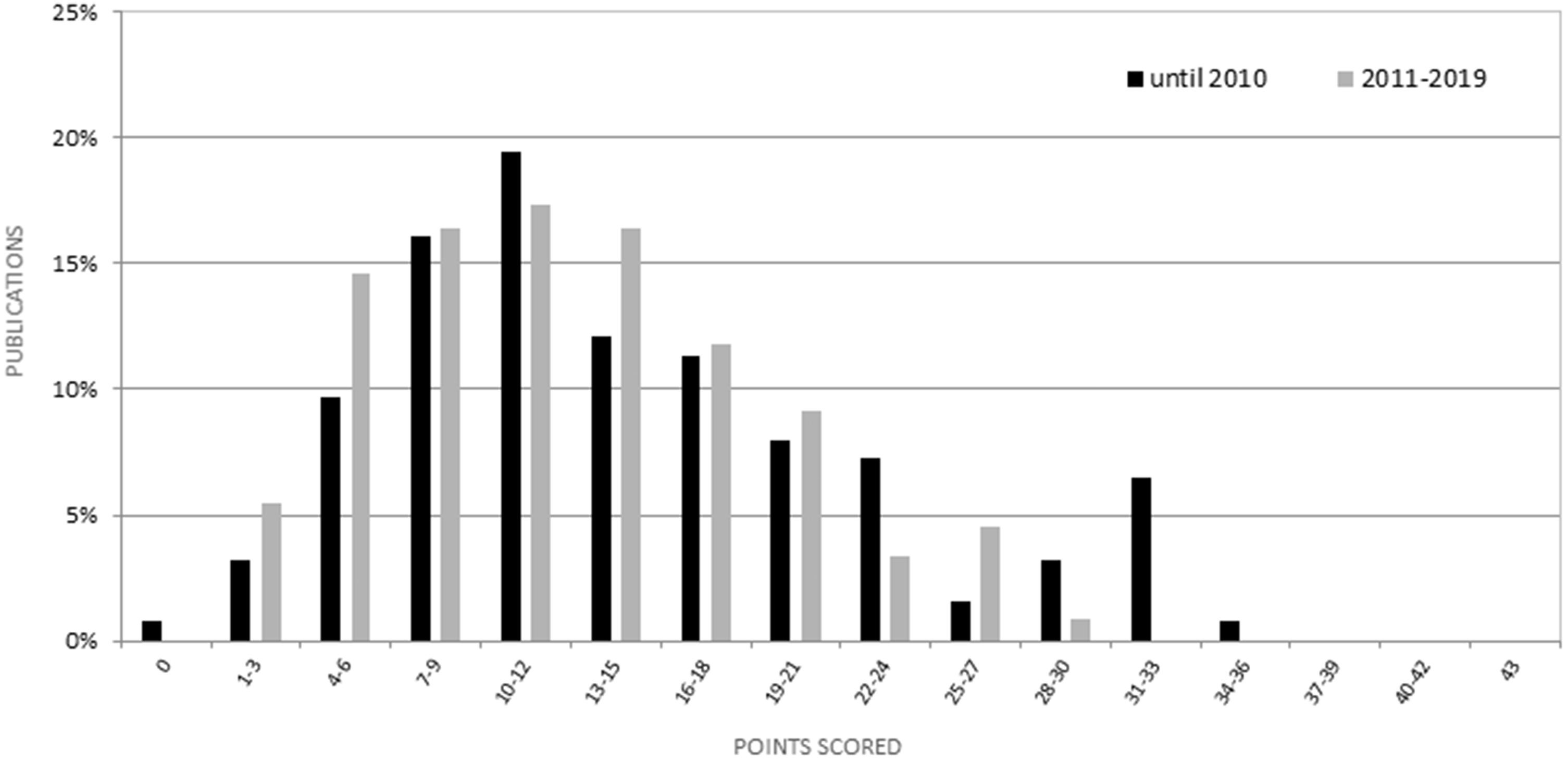
Percentage of publications published until 2010 vs 2011–2019, and the corresponding ‘Total refinement completeness score’ (0–42). No improvement can be observed in reporting the complete set of recommendations laid down by the ARRIVE guidelines after 2010.
Recommendations
This study shows significant refinement potential (or potential for reporting of refinements) for telemetry studies in mice, especially in regards to sufficient acclimatization time, social housing prior and after surgery, multimodal analgesia, environmental enrichment, provision of soft and high-caloric food, gentle handling, as well as careful welfare monitoring including species-specific pain signs and early humane endpoints.
ECG telemetry technology is a valuable tool for a vast array of different scientific fields, but only when scientists utilize it adequately, while prioritizing animal welfare through appropriate experimental method application, can it be ethically justified and yield reproducible results. Unfortunately, our own research 16 and a considerable number of publications assessing the quality of adherence to the ARRIVE guidelines regarding a variety of scientific fields and animal models also came to the same conclusion (e.g. refs64–69).
Nevertheless, we are convinced that especially in fields that include invasive animal procedures, authors have an ethical responsibility to report transparent and complete experimental details. One can argue that even if the underlying science is of good quality, incomplete reporting limits the study’s value. 4 Ethical committees, funding agencies, peer reviewers and journal editors should also be equitable to this task. Failure to sufficiently describe research and refinement methods has potential scientific and ethical implications for the entire research process, as well as for the reputation of those involved.
Limitations of the study
It is important to note that it is unlikely that all scientists, journal editors and referees in the field of telemetry were aware of the ARRIVE guidelines publication in 2010 or shortly after. Therefore, the reporting quality comparison of the reviewed publications before and after the ARRIVE guidelines were published may suffer from some inaccuracy. Of course, neither we nor authors of other systematic reviews can evaluate whether the items we were looking for were applied but not reported or actually not implemented. The fact that most publications included an ethical statement and many described an ethical approval process may indicate that many refinements were applied, but not reported. A speculation on why refinements were underreported might be that the individuals writing the publications did not perform the actual implantation surgery, thus lacking basic information on the procedure, or that strict limitations on page or word counts requested by journals might lead authors to omit information.
Supplemental Material
sj-pdf-1-lan-10.1177_00236772221115492 - Supplemental material for A systematic review on reporting of refinement measures in mouse ECG telemetry implantation surgery
Supplemental material, sj-pdf-1-lan-10.1177_00236772221115492 for A systematic review on reporting of refinement measures in mouse ECG telemetry implantation surgery by Alexandra Gkrouzoudi, Anastasia Tsingotjidou and Paulin Jirkof in Laboratory Animals
Supplemental Material
sj-pdf-2-lan-10.1177_00236772221115492 - Supplemental material for A systematic review on reporting of refinement measures in mouse ECG telemetry implantation surgery
Supplemental material, sj-pdf-2-lan-10.1177_00236772221115492 for A systematic review on reporting of refinement measures in mouse ECG telemetry implantation surgery by Alexandra Gkrouzoudi, Anastasia Tsingotjidou and Paulin Jirkof in Laboratory Animals
Footnotes
Acknowledgements
We would like to thank Professor Renè Tolba, Dr Julia Steitz and Dr Michaela Thallmair for their valuable support in this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.