
Abstract
Alpha2 receptor agonists (alpha2-agonists) are useful sedative and analgesic agents in sheep, but have adverse pulmonary effects, which are reportedly similar between different alpha2-agonists. This randomized crossover study compared pulmonary function after intravenous administration of an alpha2-agonist, either xylazine or an equipotent dose of medetomidine in 34 female sheep anaesthetized twice. Pulmonary function was assessed using spirometry, volumetric capnography, arterial blood gas analysis 1 min prior to, and 5 and 10 min after administration of the allocated alpha 2 agonist drug. Pulmonary structural changes were subsequently assessed using computed tomography (CT). Tachypnoea or hypoxaemia prompted reversal with atipamezole and exclusion of data. Data were analysed for a fixed effect of drug using a mixed effect linear model with significance set at p < 0.05. Ten sheep administered xylazine required atipamezole while none of sheep receiving medetomidine did. Xylazine produced significantly higher respiratory frequency, airway pressures, airway resistance and arterial carbon dioxide (CO2), and lower dynamic compliance, tidal volume, CO2 elimination and end tidal CO2 tension and arterial oxygen tension than medetomidine. This was associated with a significantly lower % of aerated tissue and higher % poorly and non-aerated tissue in CT images of sheep receiving xylazine versus medetomidine. In conclusion, xylazine administration produced marked decreases in pulmonary function, in ventilated isoflurane anaesthetized sheep, when compared to an equipotent dose of medetomidine when administered as an intravenous bolus supporting the use of medetomidine when alpha2-agonists are required.
Introduction
Sheep (Ovis aries) are frequently used as a model in biomedical research.1,2 Depending on the research performed, general anaesthesia may be required. In this setting it is imperative that anaesthetic and analgesic protocols optimize animal welfare but do not interfere with study findings by impairing perfusion and tissue oxygenation of vital organs. Opioids are the most frequently used analgesic agents in other species, however the analgesic efficacy of opioids has been questioned in sheep,3,4 while alpha2 adrenoreceptor agonists have been shown to have good analgesic efficacy in sheep.5,6 Alpha2 adrenoreceptor agonists, which the remainder of this paper will be referred to as alpha2-agonists, offer alternatives for providing analgesia in this species.
In contrast to other species, adverse pulmonary effects of alpha2-agonists, including increased resistance, reduced compliance and pulmonary oedema with resultant hypoxaemia, are well documented in sheep. Alterations in pulmonary function was first observed following xylazine administration.3,7,8 Further studies revealed similar effects following administration of medetomidine and dexmedetomidine.9–13
Current literature suggests that pulmonary dysfunction associated with different alpha2-agonists is similar in conscious sheep. 9 Only two studies have compared the effects of medetomidine and dexmedetomine on pulmonary function in sheep anaesthetized with isoflurane and sevoflurane,10,11 with similar drug effects reported. Xylazine is currently the only alpha2-agonists licensed for use in sheep, yet no studies compare the pulmonary effects of xylazine and other alpha2-agonists in sheep anaesthetized with inhalational agents. The aim of our study was to compare the effects of intravenous xylazine and medetomidine on pulmonary function in isoflurane anaesthetized sheep during controlled mechanical ventilation (CMV).
Materials and methods
This study was a randomized cross-over prospective experimental study. It was performed in conjunction with a concurrent nutritional study which required sheep to be anaesthetized twice with an interval of 40 days, thus providing the opportunity to compare the effects of both xylazine and medetomidine on pulmonary function in each sheep. The use of these animals for this project was approved by the Murdoch Animal Ethics Committee (R2891/16) in accordance with the Australian code for the care and use of animals for scientific purposes (2013).
Animals
Animal numbers were dictated by number included in the nutritional study. A total of 40 ewes, of which 20 were Merino and 20 were Greeline, were included. The source of animals, transportation, housing, feeding and enrichment is provided in the Supplemental material.
Anaesthesia
Each ewe was anaesthetized twice with an interval of 40 days. Prior to each anaesthetic, sheep were fasted for 24 hours. Immediately prior anaesthesia intravenous catheterization was performed after positioning the sheep in a sitting or ‘shearing’ position. A 20 g cephalic catheter (Angiocath™ Becton Dickinson, Australia) was placed after clipping and disinfecting the site. After catheterization, sheep were sedated with 0.2 mg/kg diazepam (Pamlin, Parnell Laboratories, Australia) administered intravenously (IV) 5 min prior induction of anaesthesia with propofol (Fresefol 1%, Fresenius-Kabi, Australia) 2 mg/kg IV. The trachea was then intubated with a 10 ID mm endotracheal tube and the cuff inflated. Sheep were subsequently positioned in sternal recumbency on the computer tomography (CT) table and connected to a circle system (GE Aestiva 5, Datex Ohmeda, General Electric Healthcare). Anaesthesia was maintained with isoflurane (Isothesia® NXR; Henry Shein) delivered in oxygen, adjusted to maintain adequate depth of anaesthesia, evidenced by relaxed jaw tone, lack of palpebral reflex and ventral eye position. After commencement of study no further adjustment was made. Volume controlled mechanical ventilation was started using a tidal volume (VT) of 10 mL/kg and a respiratory rate (fR) of 10 bpm. An orogastric tube was inserted into the rumen to prevent gas accumulation. Standard anaesthetic monitoring was performed including heart rate, non-invasive blood pressure and pulse oximetry (Surgivet Multiparameter monitor, Sound Veterinary Equipment, Australia). At the end of anaesthesia sheep were returned to hospital pens, and positioned in sternal recumbency, supported by hay bales. Orotracheal intubation was maintained until sheep were actively swallowing. All sheep were individually monitored until able to stand. After complete recovery of all sheep, the sheep were returned to the animal research facility, where food and water were provided immediately.
Instrumentation
Spirometry and volumetric capnography (VCap) data were recorded using the NICO device (Respironics, Wallingford, CT). The combined airway flow and carbon dioxide (CO2) mainstream sensor was placed between the Y-piece of the breathing circuit and the endotracheal tube. The capnograph of the NICO device was calibrated with room air before each experiment (infrared sensor with a response time < 60 ms and accuracy of ±2 mmHg) following manufacturer’s guidelines and the accuracy of the pneumotachograph was verified with a 400 mL calibration syringe before and after all measurements. Data were recorded over 1 min at each sample time using the dedicated software Datacoll (Respironics, Wallingford, USA).
Drug administration
Prior to the first anaesthetic, sheep within each nutritional group were randomly allocated to receive either xylazine or medetomidine using www.randomizer.org. During the second anaesthetic, each sheep received the alternate alpha2-agonist.
Initially 75 µg/kg of xylazine and 5 µg/kg of medetomidine was administered IV, based on work showing that 150 µg/kg of xylazine was equipotent to 10 µg/kg of medetomidine in conscious sheep. 9 As our study was performed in anaesthetized sheep it was expected that anaesthesia would exacerbate the effects of each drug, thus we chose to reduce the dose by 50% in attempt to minimize the frequency of severe adverse effects that could impact the welfare of the sheep. Due to marked hypoxaemia in the sheep receiving xylazine on the first day of study, a further 50% reduction in dose of both drugs was made in an attempt to avoid marked decreases in oxygen and compromised animal welfare but still allow adverse effects of the drugs to be appreciated, the study was subsequently completed using xylazine 37.5 µg/kg or medetomidine 2.5 µg/kg diluted to 10 mL with 0.9% sodium chloride and administered IV over 1 min. Only data from sheep receiving this dose were included in analysis. As these doses reportedly produce adverse pulmonary function, differences in pulmonary function should be detectable if present.3,12
If rapid spontaneous breathing occurred during mechanical ventilation, fR was increased to 15 bpm, but V
Data collection
Pulmonary function was assessed using spirometry, VCap and arterial blood gases. Spirometry data was collected before (T0), and 5 (T5) and 10 (T10) min after administration of the selected alpha2-agonist. Spirometry measured fR, V
CT
CT was performed to assess the structural changes in lung associated with drug administration. Lung tissue was scanned during an inspiratory hold while maintaining an airway pressure of 10 cmH2O. Scanning was performed using a 16 row Multi-Detector Computed Tomography (MDCT) unit (SOMATOM Emotion 16, Siemens Medical). Scan parameters used were: 130 kV tube potential; 180 mAs tube current; 1.5 mm acquisition slice thickness; 0.8 helical pitch; 512 × 512 matrix; 50 cm FOV; and 1.2 × 16 X-ray beam collimation. Whole body images were reconstructed using a standard B42 Soft Tissue Algorithm. These parameters remained consistent for all sheep.
Additional lung image series were reconstructed using the local CT workstation (Siemens Syngo, Siemens Healthcare). These images were reconstructed at a slice thickness of 5 mm with a 2 mm overlap using the U91 ultra-sharp reconstruction kernel and Lung window comprising a window width (WW) of 1400 and window centre (WC) of –500.
Lung series were imported into a third party proprietary DICOM workstation (Osirix MD) and 10 equidistant slices were manually segmented as a representative sample of lung volume. This method is consistent with previously reported methods of CT interpolation for lung volume analysis.13,14 The researcher segmenting these volumes was blinded to both the breed of sheep and the drug used to eliminate selection bias.
These representative slices were analysed using dedicated image analysis software (Maluna 3.17; Göttingen, Germany). The lung parenchyma was manually outlined in each of the 10 images. Mediastinal structures and major vessels were excluded. Any areas of air/gas present on the caudal lung images caused by partial voluming of the stomach abutting the diaphragm were also excluded. The lung parenchyma was then analysed pixel by pixel to determine aeration quality. After processing each slice, total lung volume, tissue (% tissue), air (% AIR) and frequency distribution of lung CT numbers, expressed in Hounsfield units (HU), were calculated. Based on their degree of ventilation, four different lung compartments were quantified according to the usual threshold values 15 hyperinflated tissue (–1000 to –901 HU as % OVER), normally ventilated tissue (–900 to –501 HU as % NORMAL), poorly ventilated tissue (–500 to –101 HU as % POOR) and non-ventilated tissue (–100 to 200 HU as % NON).
Data analysis
The investigators compiling and analysing data were blinded to the drug administered. Responses were tested for normality using Shapiro–Wilk test with rejection of the null hypothesis of normality at p < 0.05. Apart from age, data collected was normally distributed, and thus was described as the mean (95% confidence interval). Age was described as median (range). Measures of pulmonary function were analysed for a fixed effect of drug and time using a mixed effect linear model that included the covariate breed, and the random variance of body weight. Body weight was included to identify influence of varying body weight due to breed or nutrition. The analysis accounted for repeated measurements on each sheep, with a default covariance structure of variance components. Drug order had no effect it was deleted from the final model. Where there were significant interactions of drug and time at p < 0.05, paired post-hoc comparisons of least squares means were compared at time points for each drug against a Tukey adjusted of p < 0.05. The CT findings were analysed at a single time point, thus only drug remained a fixed effect in the model. SAS V 9.4 was used for all analyses.
Results
Of the original 40 sheep, complete data was collected in 33 sheep receiving xylazine and 34 sheep receiving medetomidine. Reasons for exclusion are outlined in Supplemental Figure S1. The sheep were 6 (4–6) years old and weighed 61 (58–64) kg.
Ten sheep receiving xylazine required atipamezole 8 (7–9) min after xylazine administration due to presence of marked tachypnoea at adequate level of anaesthesia that did not respond to increased fR. These sheep were confirmed to have hypoxaemia with a PaO2 of 6.83 (4.99–8.65) kPa measured at T10. The spirometry and capnography data collected at T10 and CT images from these sheep was excluded from analysis. In contrast, none of the sheep receiving medetomidine required atipamezole Spirometry, VCap data and arterial blood gases, included in analysis are summarized in Tables 1–3.
Spirometry data recorded in 34 (17 merino and 17 Greeline) sheep that received medetomidine (2.5 µg/kg) intravenously and 33 (17 merino and 16 Greeline) sheep that received xylazine (37.5 µ/kg) intravenously. The mean (95% confidence interval) of each variable recorded before (T0), 5 min (T5) and 10 min (T10) after drug administration is presented. Significant difference (p < 0.05) indicated as * between drug, # within drug, between T0 and T5/T10, $ within drug, between T5 and T10.
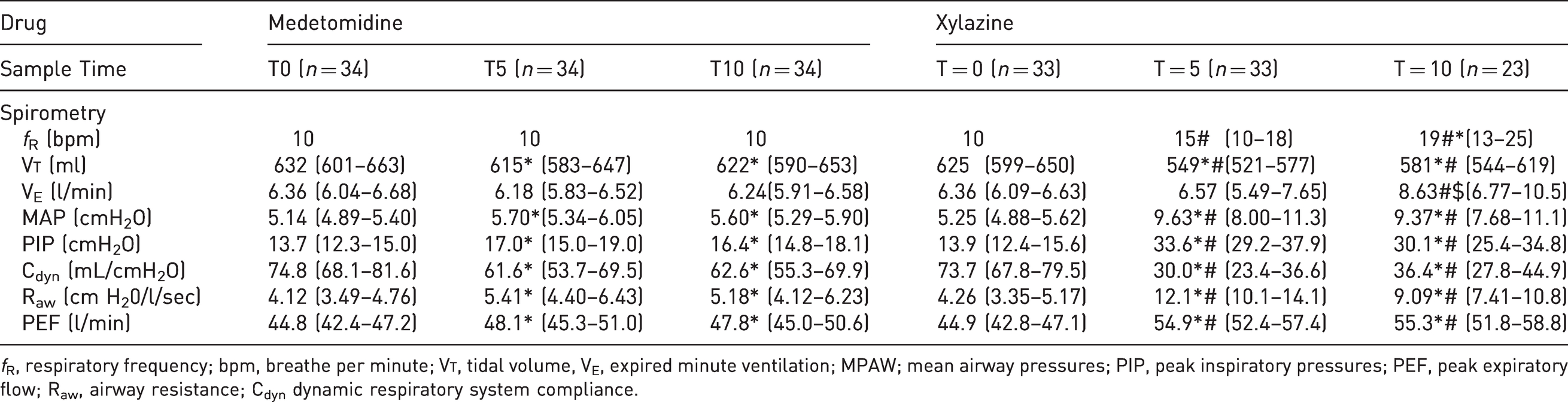
fR, respiratory frequency; bpm, breathe per minute; V
Volumetric capnography data recorded in 34 (17 merino and 17 Greeline) sheep that received medetomidine (2.5 µg/kg) intravenously and 33 (17 merino and 16 Greeline) sheep that received xylazine (37.5 µ/kg) intravenously. The mean (95% confidence interval) of each variable recorded before (T0), 5 min (T5) and 10 min (T10) after drug administration is presented. Significant difference (p < 0.05) indicated as * between drug; # within drug; between T0 and T5/T10; $ within drug, between T5 and T10.
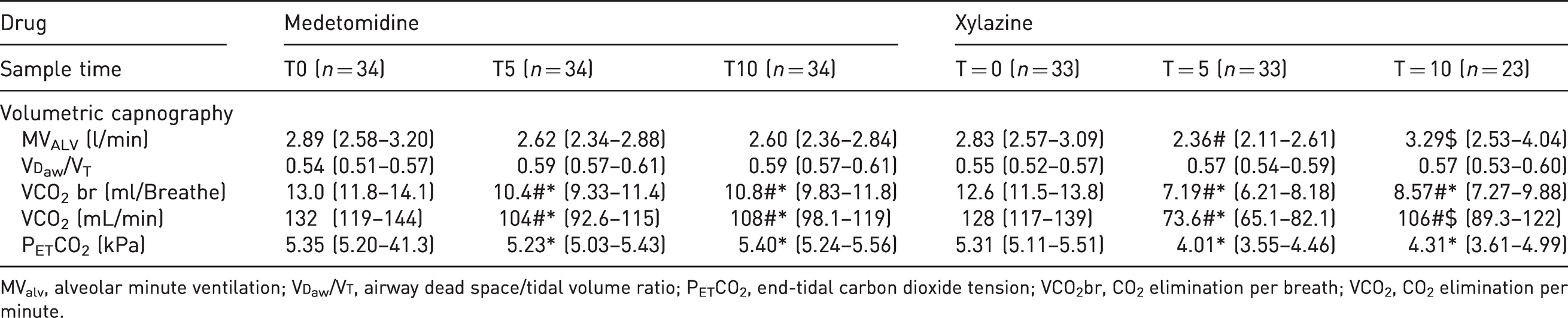
MValv, alveolar minute ventilation; V
Arterial blood gases and calculated variables recorded in 34 (17 merino and 17 Greeline) sheep that received medetomidine (2.5 µg/kg) intravenously and 33 (17 merino and 16 Greeline) sheep that received xylazine (37.5 µ/kg) intravenously. The mean (95% confidence interval) of each variable recorded before (T0), 5 min (T5) and 10 min (T10) after drug administration is presented. Significant difference (p < 0.05) indicated as * between drug; # within drug; between T0 and T5/T10; $ within drug, between T5 and T10.
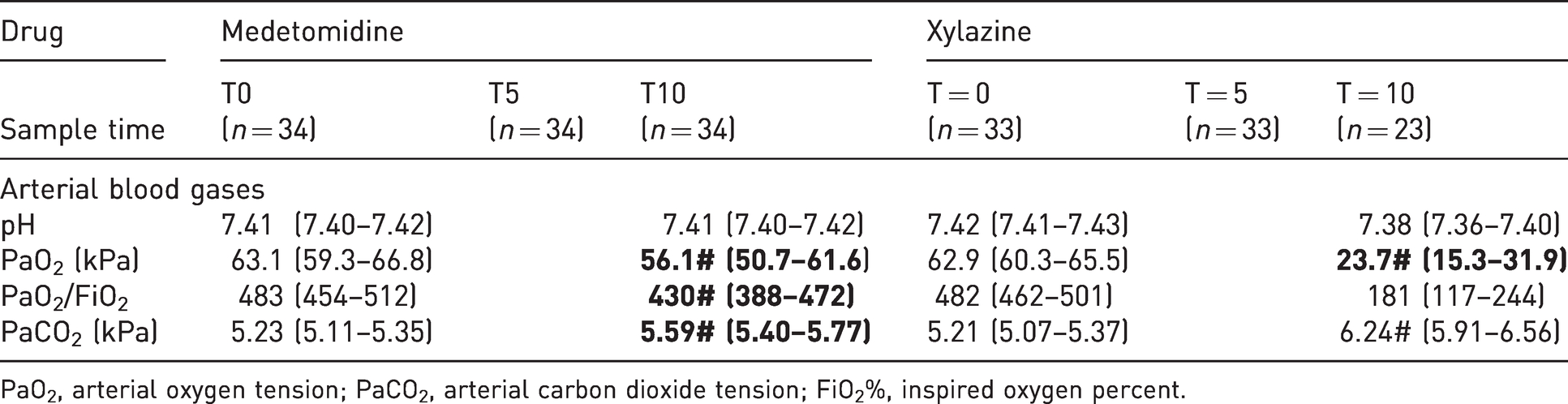
PaO2, arterial oxygen tension; PaCO2, arterial carbon dioxide tension; FiO2%, inspired oxygen percent.
Differences within each drug group
Xylazine administration resulted in a significantly increased MPAW, PIP, Raw, PEF and significantly decreased V
Differences between each drug group
Comparison of xylazine and medetomidine revealed that at T5 and T10, xylazine resulted in significantly higher MPAW, PIP, Raw and PEF and significantly lower V
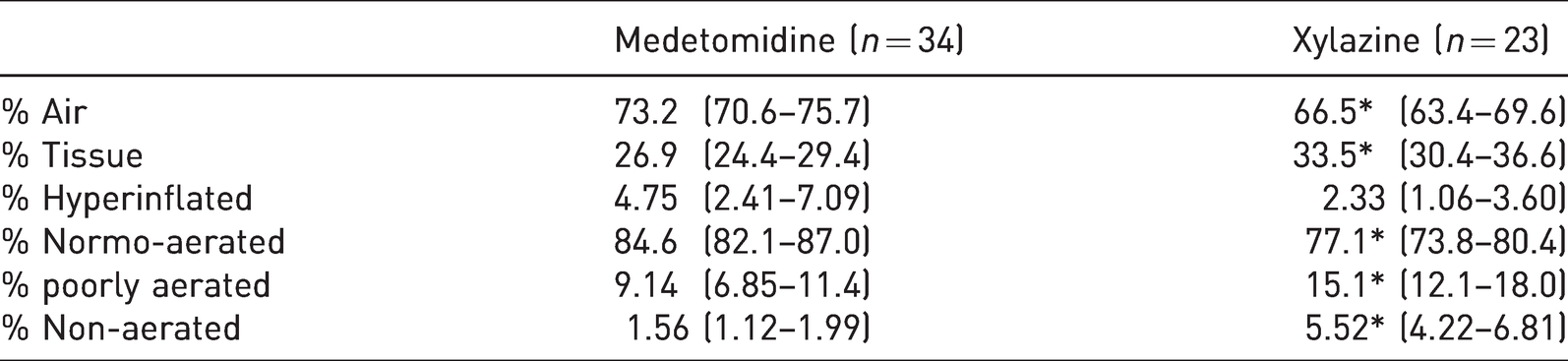
Representative lung images obtained using CT after T10 are presented in Figure 1. Xylazine produced significantly lower % air and significantly higher % tissue on CT images when compared to medetomidine (see Table 4). These differences were associated with a significantly higher % of poorly and non-ventilated lung following xylazine administration.
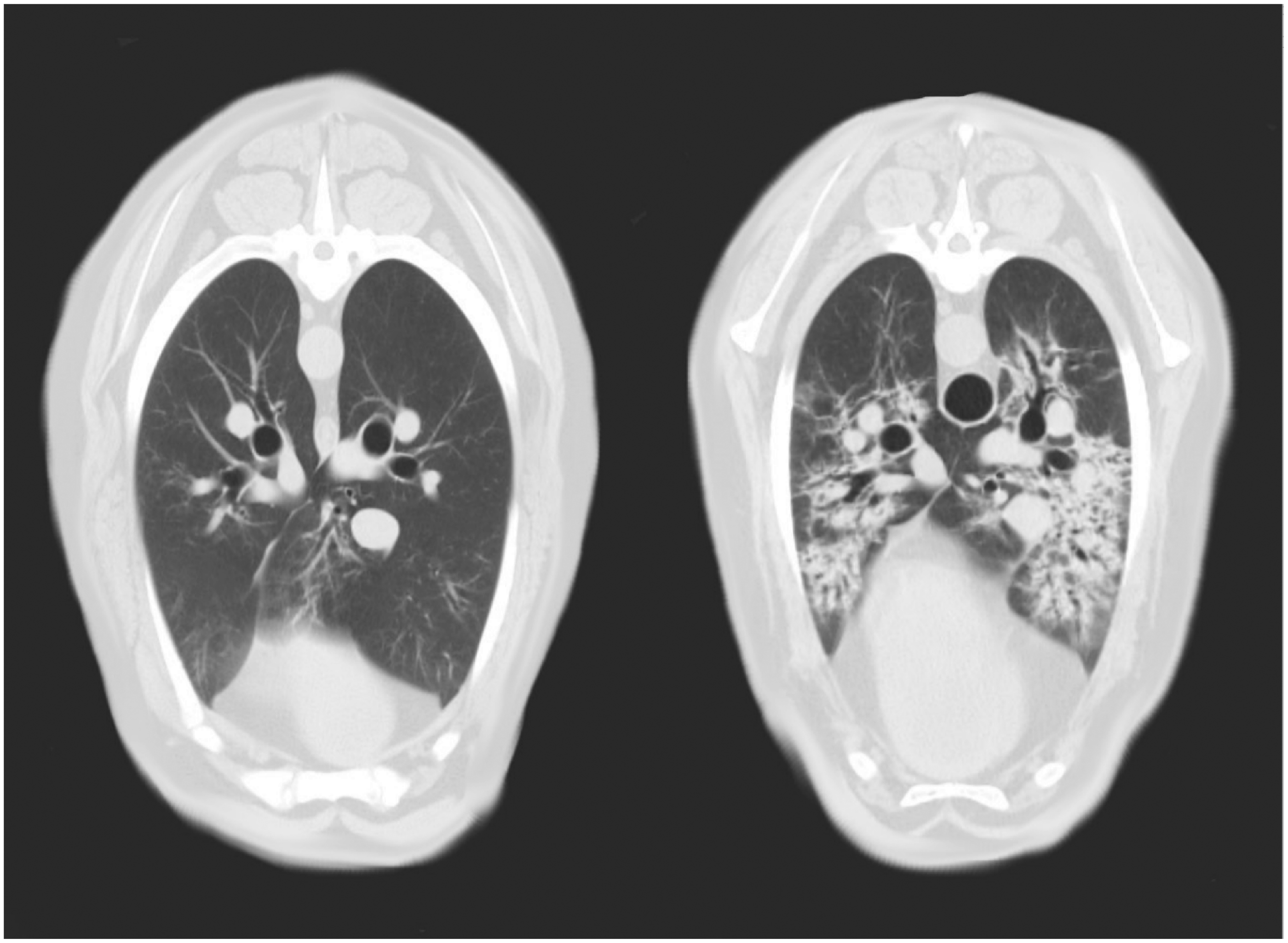
Cross sectional images of lung at the middle of seventh thoracic vertebrae obtained using computer tomography in two anaesthetized sheep receiving medetomidine (left) and xylazine (right).
Computed tomography data recorded in 34 (17 merino and 17 Greeline) sheep that received medetomidine (2.5 µ/kg) intravenously and 33 (17 merino and 16 Greeline) sheep that received xylazine (37.5 µg/kg) intravenously. The mean (95% confidence interval) of each variable is presented. * Significant difference (p < 0.05) between drug.
Discussion
Based on our results, xylazine resulted in a significantly poorer pulmonary function than medetomidine administration. This was supported by spirometry, VCap, blood gases, CT images and the difference in the number of animals requiring atipamezole.
In our study 10 of the 33 (30.3%) sheep receiving xylazine required atipamezole while none of the 34 sheep receiving medetomidine required this drug. The decision to administer atipamezole was initially based on a cut-off SpO2 of < 90%. However, after commencement of the study, marked tachypnoea was observed in some sheep receiving xylazine at adequate depths of anaesthesia. To exclude hypercapnia as a cause of tachypnoea, fR was increased to eliminate CO2 and reduce the stimulus for tachypnoea. When this strategy failed, it was considered likely that tachypnoea represented a response to hypoxaemia 16 and thus administration of atipamezole was considered appropriate in these animals. This theory was supported by a delayed drop of SpO2 < 90% (around 1–2 min after tachypnoea was observed) and confirmed by the extremely low PaO2 (51.2 (37.4–64.9) mmHg) measured at T10, despite administering atipamezole several minutes before blood sampling. This loss of data from sheep that required atipamezole prevented us from analysing the effect of drug on pulmonary function in all sheep at T10. Despite this, the fact that approximately 30% of the sheep receiving xylazine had marked decreases in oxygenation warranting reversal, while none of the sheep receiving medetomidine did, is an important clinically relevant finding when comparing the effects of these two drugs.
Spirometry revealed statistically significant changes in numerous indices of pulmonary mechanics (Cdyn, Raw, MPAW, PIP) after xylazine. The increase in Raw can be explained by bronchoconstriction 17 while the decrease in Cdyn is more likely due to the interstitial and alveolar oedema. These changes are consistent with previous studies (Celly et al., 1999). 12 More detailed breath by breath analysis is required to fully elucidate the mechanisms associated with changes in pulmonary mechanics.
After medetomidine, spirometry was only able to detect a significant decrease in VCO2 with all other pulmonary function variables remaining stable over the time course of the study. These results contrast with those in halothane anaesthetized sheep, 12 where decreases in Cdyn, and increases in pulmonary resistance and changes in transplumonary pressure were observed for 20 min following administration of medetomidine at 1, 2, 4 and 6 µg/kg IV. Thus, the dose of 2.5 µg/kg used in our study does not explain the lack of change in variables of pulmonary function, including Cdyn and Raw, following medetomidine administration. Other factors may be involved such as age or breed, which will be discussed later.
Interestingly, V
After administration of both alpha2-agonists the ability to eliminate the CO2 by the lungs was less efficient compared to baseline, as observed by decreased VCO2br and VCO2 and increased PaCO2 after both drugs. However, the magnitude of decrease after xylazine was much larger with a decrease in VCO2 of more than 40% per breath and per minute. A decrease in VCO2 can be related to a change in lung perfusion or the efficiency of ventilation providing a direct measure of a lung’s functional area for gas exchange.18,19 In our sheep changes in both perfusion and efficiency in ventilation are possible. Both alpha2-agonists have been reported to cause pulmonary vasoconstriction 20 which might cause redistribution of blood towards the more central areas leaving the peripheral areas unperfused, causing an increase in alveolar dead space and therefore decreasing CO2 elimination. In addition, lung areas with low to zero ventilation, due to pulmonary oedema would also contribute. 19 It is also important to note after xylazine, VCO2 remained reduced despite significant increases in VE at T10. As increased VE should improve VCO2, we can say that functional gas exchange capacity after xylazine was majorly impaired.
Major impairment of gas exchange was also confirmed by our blood gas findings following both drugs. However, while the decrease PaO2 following xylazine administration was associated with marked changes in pulmonary function, the decrease in PaO2 following medetomidine administration was not associated with changes in spirometry and volumetric capnography data. It is possible that differences in receptor selectivity may have resulted in greater changes in perfusion following medetomidine and thus reducing oxygen diffusion despite a lack of change in pulmonary mechanics. However, decreased oxygenation has been observed without any changes in Cardiac Index. 12 So, the mechanism for the decreased PaO2 following medetomidine remains undetermined. However, in contrast to that observed following xylazine administration changes in PaO2 following medetomidine would not be considered clinically significant and are smaller than that observed in other studies. 9 The clinical significance is supported by a mean PaO2/FiO2 of <300 following xylazine administration, which is consistent with the definition of acute respiratory distress syndrome (ARDS) 21 .
This is the first study comparing CT lung changes after the administration of xylazine and medetomidine. The CT was performed after collection of data for T10. A significant difference between xylazine and medetomidine was found in all evaluated CT variables. The % of non-aerated lung areas were > 3× higher and the % of poorly aerated nearly double following xylazine compared to medetomidine. This finding is confirmed by a significantly higher percentage of pixels representing HUs corresponding with tissue within the lung areas following xylazine administration. Surprisingly, there was no significant difference in hyperaerated pixels following xylazine compared to medetomidine. It is expected that the reduction in aerated lung tissue would have produced a syndrome similar to that observed in ARDS where overdistension occurs when a set V
There are several factors which could have resulted in differences between our study and previous studies. One factor might be the signalment (age and breed) of the sheep included in our study. Of these factors age is unlikely as older sheep appear less sensitive to the hypoxaemic effects of alpha2-agonists than younger sheep. 23 Although our analysis included breed as a covariant to avoid confounding of any comparisons between drugs, both breeds (Merino and Greeline) of sheep used in our study do differ from majority of the other studies. A review of previous literature suggests there may be a breed difference in response to alpha2-agonists.24 However, it is not clear if this is true for all alpha2-agonists or just xylazine. Studies designed to specifically investigate effect of agents with different alpha1:alpha2 selectivity in different sheep breeds has not been performed to date. However, a breed difference in response to more selective alpha2-agonists such as medetomidine, may explain why we observed such a marked difference between xylazine and medetomidine in our study in contrast to previous studies, 9 and why the effect of medetomidine in our study was less profound than previously reported. 10 It is also worthy of note, that in this study the drugs were administered as an IV bolus. This was considered the most appropriate way to compare the drug effects without the influence of bioavailability or pharmacokinetics that could alter the response to IM administration.
The sample times chosen for data collection in our study may have influenced the results. As mentioned above the peak effects of xylazine and medetomidine are reported to occur within 5 min of IV administration 9 and thus are likely to have been captured by our spirometry and VCap data collection at this time point. However, there was a delay in performing blood gas analysis and CT. CT evaluation was performed after the reported peak effect of the drugs, 9 suggesting that changes may have been even more pronounced if CT had been performed at an earlier time point. This was not possible as movement of the CT table would have interfered with other data collection and it was essential for the anaesthetist to be able to intervene at any time point during the peak effect, which is not possible during CT scanning.
It is also possible that we missed maximal change in some of the indices if they occurred before our first sample time of 5 mins. Analysis of data every 30–60 s may have allowed this maximal effect to be detected. Furthermore, more frequent assessment may have allowed us to detect whether changes in resistance and compliance occur concurrently or consecutively and if so, which change occurs first. This approach may assist in clearly defining the contribution of bronchoconstriction and pulmonary oedema to the development of hypoxaemia in these sheep.
Conclusion
The results of this study showed that, in ventilated isoflurane anaesthetized Merino and Greeline sheep, xylazine administration produced marked decreases in pulmonary function compared to medetomidine when administered as an IV bolus. Our findings support the clinical conclusion that medetomidine is the preferred alpha2-agonist for use in anaesthetized ventilated sheep when optimal pulmonary function is required. However, results of this study also support further investigation in other sheep breeds to determine if the results of this study are applicable to other breeds.
Supplemental Material
sj-pdf-1-lan-10.1177_0023677220983366 - Supplemental material for Comparison of pulmonary function in isoflurane anaesthetized ventilated sheep (Ovis aries) following administration of intravenous xylazine versus medetomidine
Supplemental material, sj-pdf-1-lan-10.1177_0023677220983366 for Comparison of pulmonary function in isoflurane anaesthetized ventilated sheep (Ovis aries) following administration of intravenous xylazine versus medetomidine by Anthea L Raisis, Giselle L Hosgood, Nicholas Crawford, Sabine Kästner, Gabrielle C Musk, Peter Herrmann and Martina Mosing in Laboratory Animals
Supplemental Material
sj-pdf-2-lan-10.1177_0023677220983366 - Supplemental material for Comparison of pulmonary function in isoflurane anaesthetized ventilated sheep (Ovis aries) following administration of intravenous xylazine versus medetomidine
Supplemental material, sj-pdf-2-lan-10.1177_0023677220983366 for Comparison of pulmonary function in isoflurane anaesthetized ventilated sheep (Ovis aries) following administration of intravenous xylazine versus medetomidine by Anthea L Raisis, Giselle L Hosgood, Nicholas Crawford, Sabine Kästner, Gabrielle C Musk, Peter Herrmann and Martina Mosing in Laboratory Animals
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance of Muriel Sacks and Philomena Touhy in assistance of anaesthesia and data collection.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.