
Abstract
Preputial dilation is an infrequently reported condition in pigs. The pathophysiology and etiology is unclear. Causes for diverticulum dilation are proposed to be chronic preputial diverticulitis with subsequent fibrosis of the preputial cavity, phimosis of the preputial orifice or the preputial diverticulum, but the large majority of cases are reportedly idiopathic in nature. Surgical interventions include ablative procedures, but many cases are not treated because of an assumed lack of clinical relevance in pigs not used for breeding. We report a case of progressive preputial dilation that recurred after surgical intervention. Histopathological examination revealed no primary inflammatory condition, contrary to literature suggesting a role for inflammatory mediators in pathogenesis. Phimosis of the preputial orifice was noted post mortem and might be a contributing factor.
These findings partially contradict the current assumptions in regards to pathophysiology and treatment choices in the literature and warrant further investigation into alternative therapeutic interventions for this condition.
Case report
Single case reports of dilation of the preputial sac have been reported in boars, most often being observed during puberty. Affected pigs may be unsuitable for breeding purposes as the erect penis might get stuck in the dilated diverticula. 1 The preputial cavity of the boar is significantly longer than the intrapreputial part of the penis. The preputial diverticulum is a pear-shaped, bi-lobed recess of the anterior preputial cavity. Its neck, which is 1 cm to 2 cm in diameter, opens onto the dorsal aspect of the prepuce, 3 cm to 4 cm caudal to the preputial ostium. The boar is the only domestic animal with a diverticulum. Normal contents of the diverticulum include urine, semen, desquamated epithelial cells, bacteria, and occasional concretions. Urination flushes the diverticulum. During breeding, preputial muscle activity causes the contents of the diverticulum to be expelled. This results in semen contamination, a potentially significant problem in swine used for artificial insemination. 1
Reported causes for diverticulum dilation are chronic preputial diverticulitis and consecutive fibrosis of the preputial cavity, phimosis of the preputial orifice or the preputial diverticulum, but the large majority were reportedly idiopathic in nature. Surgical preputial diverticulum ablation or no intervention at all due to no assumed clinical relevance in pigs not used for breeding purposes are being recommended in the literature. A method for surgical correction was published, which is also being used for other indications. Extirpation and ablation of the preputial diverticulum in pigs has been described for various reasons such as reduction of odor in male pet pigs, aesthetics, to relieve or prevent infection of the tissue, for decreasing the risk of contamination when collecting sperm for reproductive purposes, and/or for treatment of preputial diverticulum dilation. Three different methods have been described: removal of the diverticulum via a paramedian incision lateral to the prepuce, or extirpation and excision of either only the diverticular horns or the entire diverticulum through the preputial orifice.1–4 All are considered to be minimally invasive procedures with little potential for complications. However, to our knowledge no study has followed up pigs consecutively treated.
We report here a case of a male Goettingen minipig with progressive preputial dilation and urine retention. This minipig was treated with partial diverticulum resection. We describe clinical outcomes, macroscopic and histopathological findings, and compare those to a healthy age-matched control minipig.
The case
A 5.5-month-old male intact minipig (previously obtained from Ellegaard Goettingen Minipigs ApS, Dalmose, Denmark) with no previous medical history was noticed to show a slightly increased volume of approximately 5 cm of the preputial sac compared to other age-matched animals (approximately 2 cm to 3 cm). Over the course of four weeks, this increased further in size, reaching a volume of approximately 9 cm in diameter (Figure 1) and containing about 250 ml of urine.
Dilated preputial cavity with urine retention in a 5-month old Goettingen minipig.
The urine accumulation had to be manually squeezed out once daily, before surgical intervention. Even though this was performed gently, the animal showed increasing discomfort and distress when manipulated. Under general anesthesia (ketamine 20 mg/kg intramuscularly (IM), xylazine 2 mg/kg IM) an ultrasound of the urogenital region was performed that revealed no abnormalities other than dilated diverticulum horns. Ultrasound-guided cystocentesis allowed sterile collection of urine for urinalysis, which was without abnormal findings. Manual palpation revealed only a fairly small opening to the posterior preputial cavity that was large enough to insert a fingertip of a little finger. Using a rubber tube attached to a 50 cc syringe, negative pressure was applied to the penis tip and we attempted to protrude it from the preputial cavity. However, only the very tip could shortly be visualized through the preputial orifice and it was not possible to advance the penis any further or grasp it with tissue sponges.
The area was prepped in a sterile manner and draped, and the preputial cavity was flushed with 1% diluted povidone iodine solution prior to surgery. The diverticulum pouches were exteriorized one at a time by inserting Allis forceps into the preputial opening and directing them laterally. After grasping the lining with the forceps, the lining was steadily pulled out of the opening. Only the ends of the horns could be exteriorized. The horns were clamped and fixated with curved hemostatic forceps, the horns excised, and the remaining tissue was sutured with single interrupted sutures (Vicryl 4–0) and repositioned (Figure 2). The resected tissue was submitted for histopathological analysis that revealed no abnormal findings.
Surgical resection of the preputial diverticula (schematic drawing).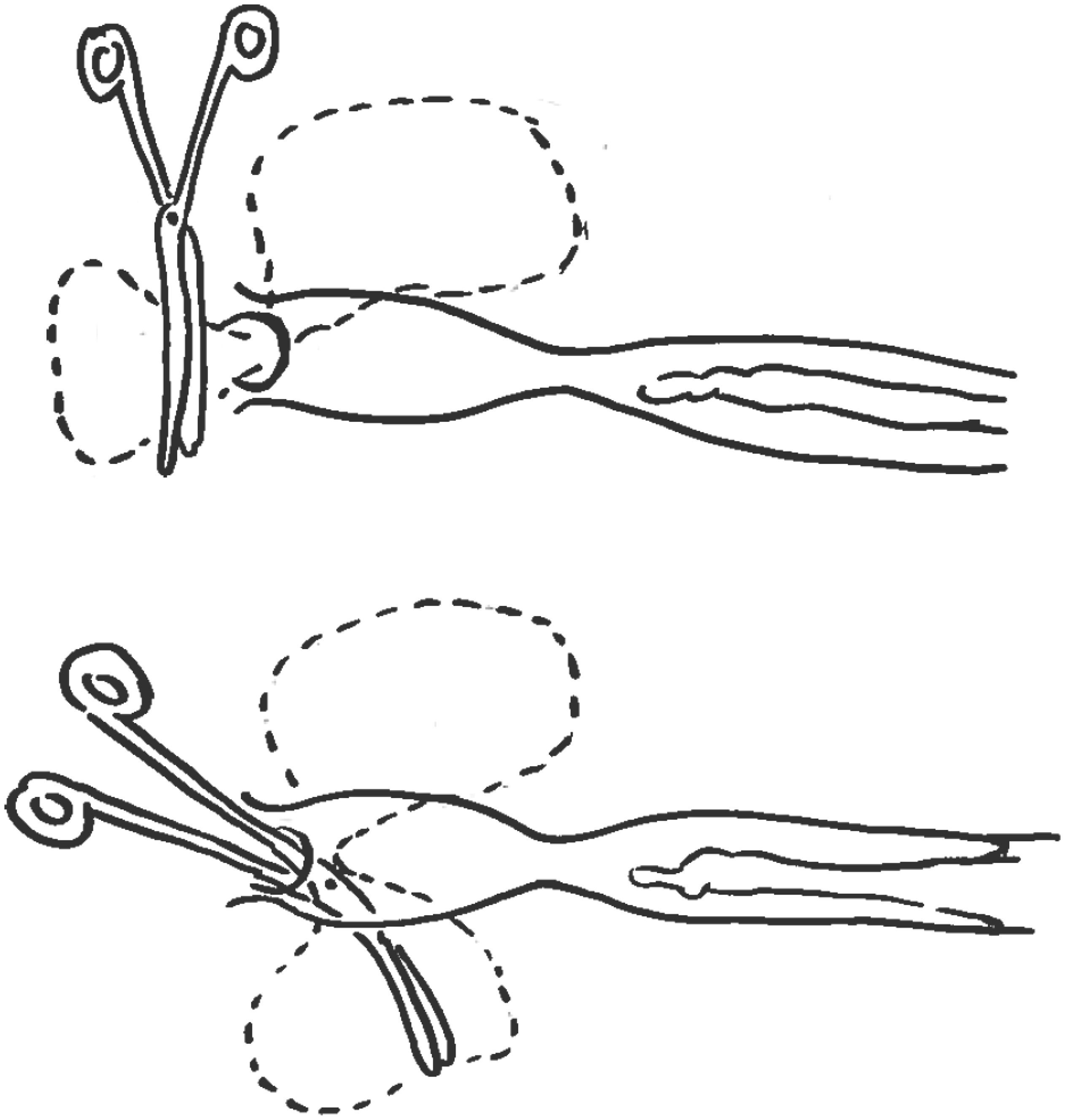
Postoperative analgesia was provided (meloxicam 0.4 mg/kg subcutaneously (SQ), q24 hours) for three consecutive days and the animal recovered smoothly and uneventfully and only a minor swelling of the peripreputial area was observed for two to three days. Immediately after surgery, normal urination and no urine retention was observed for the following three months. Minor bloody discharge was noted the two consecutive days and resolved without further intervention. Consecutively, eight weeks after the surgery and complete recovery, the minipig was included in a terminal pharmacokinetic study with one intravitreal administration of a compound and a follow-up time of one week.
During that study or three months post-surgery, a mostly unilateral increase in volume of the preputial cavity with consecutive urine retention was observed suggesting recurrence (Figure 3).
Recurrence of clinical symptoms unilaterally three months after surgical intervention.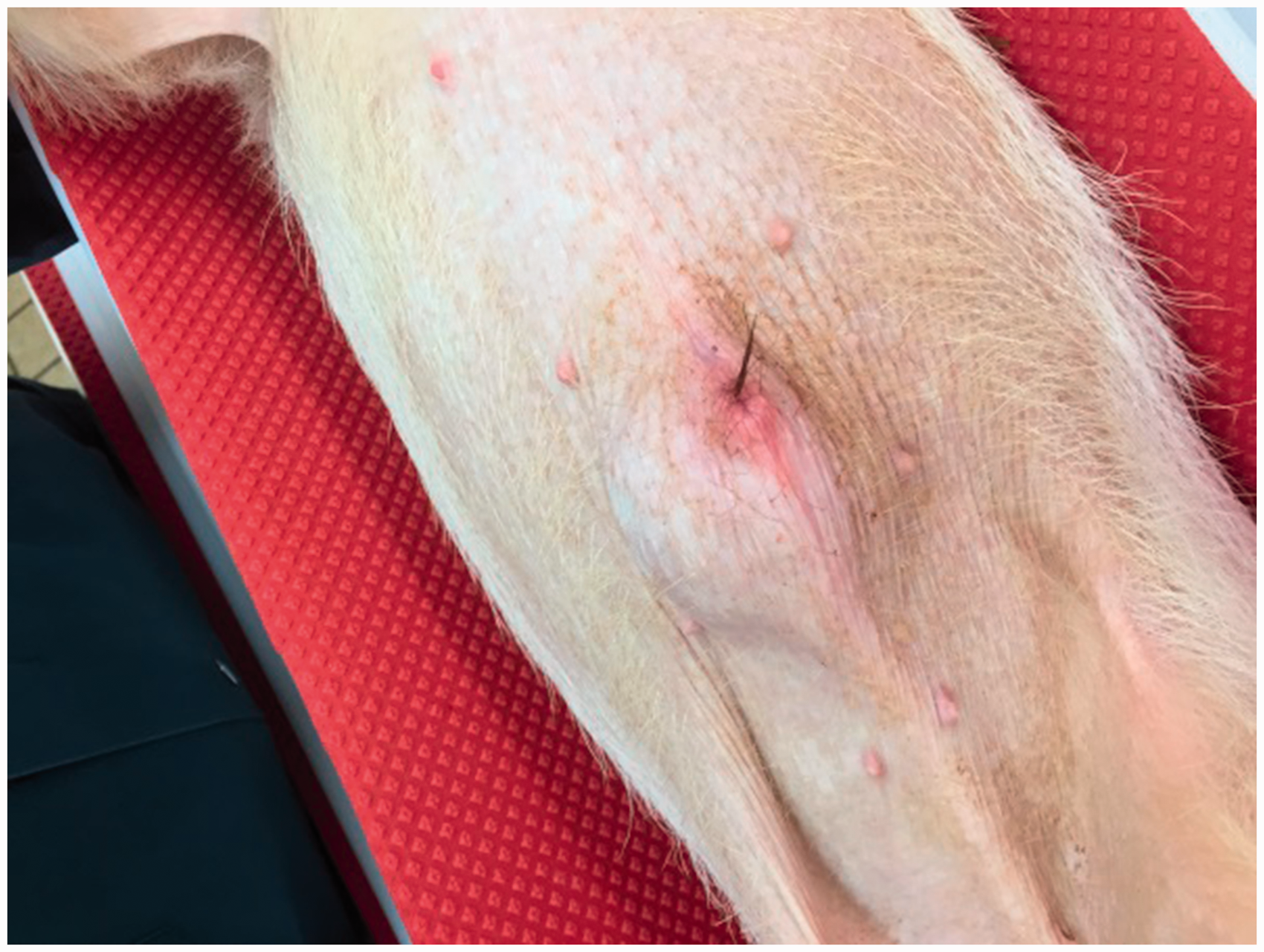
As the animal was at that point scheduled for euthanasia and necropsy because of the terminal study design four weeks later, no further therapeutic interventions were undertaken. During necropsy of the animal, genital tissue (penis within the preputial sac) was sampled for macroscopical and histopathological examination from the affected animal as well as from an age-matched control animal. Macroscopically, the direct preputium cranial of the penis tip showed only a small passable opening of 3 mm to 4 mm (in contrast to 10 mm in the age-matched control). Nevertheless, the penis was freely movable without any malformations or other abnormalities. The left portion of the diverticulum pouch had a diameter of 1 cm and the right portion of 3 cm (symmetric 2.5 mm in diameter in age matched control) and the epidermis exhibited a greenish color. Histologically, the epidermis of the diverticulum and the preputium was regularly keratinized. In the underlying dermis was a moderate chronic histiocytic inflammation with pigmented macrophages (pigment consistent with hemosiderin confirmed by Prussian blue stain; Figure 4) corresponding to the greenish discoloration obtained macroscopically; this finding was considered to be the residue of the surgical intervention with associated hemorrhage rather than part of the primary cause of diverticulum dilation. Additional minimal focal subepidermal follicular aggregates were considered within the normal variation since they were present in the age-matched control as well.
Diverticulum of a minipig, regularly keratinized epidermis of the diverticulum and histiocytic inflammation with pigmented macrophages in underlying dermis (pigment consistent with hemosiderin confirmed by Prussian blue stain), (a) hematoxylin and eosin stain, (b) Prussian blue stain.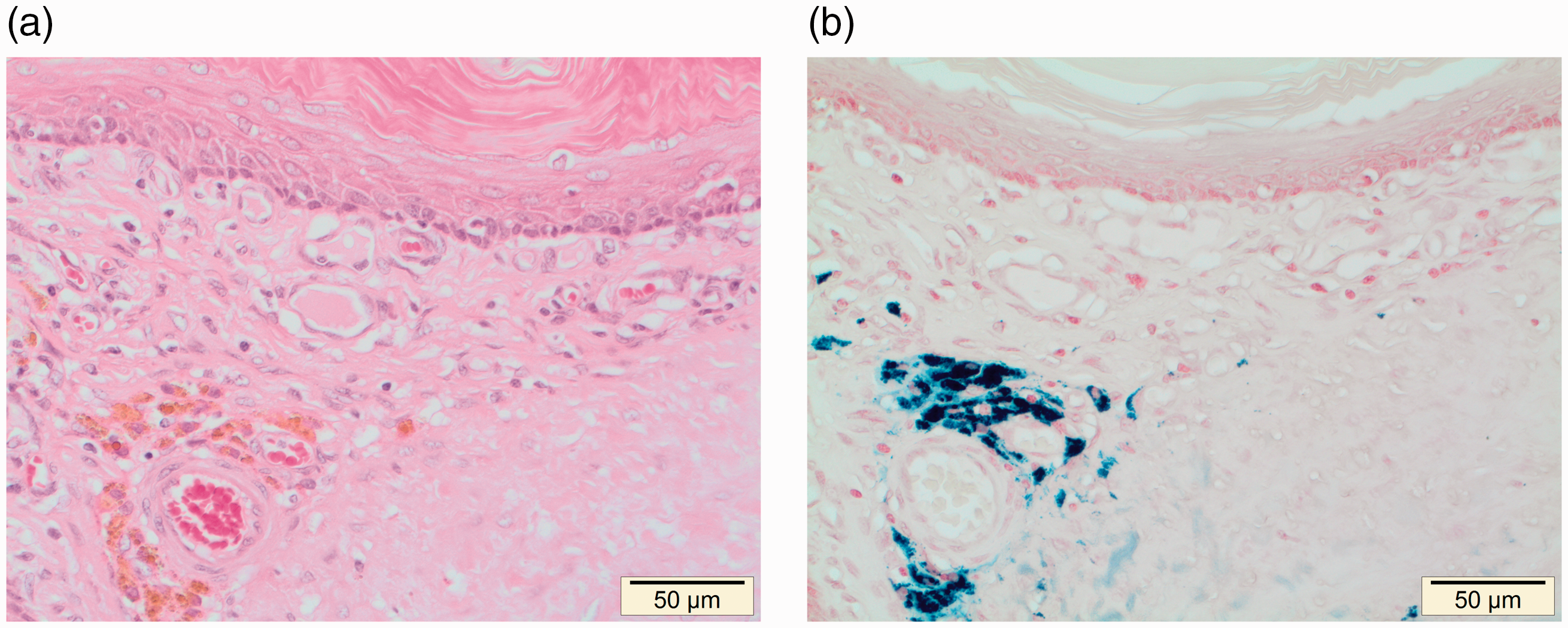
Discussion
To the best of our knowledge, this is the first reported case of preputial dilation in a Goettingen minipig in a laboratory animal setting and in general of recurrence after surgical correction of dilation of the diverticula in a boar. Based on the number and year of publication of the already published cases, it appears to be a rather rare condition in the Goettingen minipig.
The pathophysiology of the observed findings is unclear. One could consider a primary phimosis of the orifice between the cranial and caudal part of the preputium, resulting in a change in dynamics during urination, which may have resulted in consecutive dilation of the diverticula. This would also explain the recrudescence since the phimosis itself was not corrected. Contrary to previously reported assumptions and case reports, we definitively ruled out chronic posthitis or neoplastic changes of the preputium as a primary cause. Notably, acute posthitis was observed only after surgery and was likely unrelated to the diverticula resection. Also, resection of the diverticula alone did not result in a successful long-term management of the issue. For future cases similar to the one described here, different surgical interventions may result in improved clinical outcomes. For example, a removal of the diverticular horns in combination with a surgical correction of the phimosis of the orifice between the cranial and caudal portions of the preputial cavity might provide recurrence-free disease resolution. Removal of the entire cranial portion of the preputium together with the horns, similar to the procedure described by Dutton et al., 3 in combination with dilation and reconstruction of the preputial orifice, may constitute another solution.
In the context of laboratory animal medicine, animals need to be monitored for this condition, despite the rare occurrence. As a treatment strategy for this condition, short-term management with daily manual extrusion of urine can provide symptomatic relief while assessing long-term therapeutic options. However, if the animal needs to be housed or included in a study for a prolonged duration exceeding several weeks, surgical management is inevitable given that the animal reported here showed clear aversion against the persistent required manipulation of the preputium.
Surgical intervention as described here provided three months of relief, but did not prevent recurrence in this case. Therefore a surgical method different from the one described here would be advised, although the specific approach to be applied requires further investigation. In the current case, no effect on the study conducted was observed, although it would not be recommended to include such an animal in a study with urogenital parameters (such as urine, sperm, etc.) as study endpoints. Since a potential genetic predisposition cannot be ruled out, affected animals should not be used for breeding and the original breeding facility should be notified.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.