
Abstract
In pigs, the deep location of the common carotid artery and overlying sternomastoideus muscle in the neck has led to the recommendation for a surgical cutdown for common carotid access, as opposed to minimally invasive techniques for vascular access. We sought to determine if direct percutaneous common carotid artery access in piglets is attainable. Seventeen piglets were anesthetized and intubated. Under two-dimensional and color flow Doppler ultrasound guidance, a 21 gauge needle was utilized to access the right common carotid artery. Following arterial puncture, the Seldinger technique was applied to place a 4 or 5 French introducer. Upon completion of cardiac catheterization with intracoronary stem cell infusion the introducer was removed and manual pressure was applied to prevent hematoma development. Successful access with an introducer was achieved in all 17 piglets. The average weight was 8.5 ± 1.7 kg. One piglet developed a hematoma with hemorrhaging from the catheterization site and was euthanized. This piglet was given bivalirudin for the procedure. After this incident, subsequent piglets were not given anticoagulation and no other complications occurred. Ultrasound guided percutaneous common carotid artery access in piglets is attainable in a safe, reliable, and reproducible manner when performed by microvascular experts.
Dondelinger et al. documented a detailed overview of radiological vascular and visceral anatomy of pigs. 1 The right and left coronary artery origins lie in the bulb of the thoracic aorta cranial to the corresponding cusps of the aortic valve, similar to humans. Standard human diagnostic catheterization techniques and equipment have been utilized for coronary procedures in adult swine. 2 In piglets, the short length of the ascending aorta limits the ability to safely and easily engage the coronary ostia from a femoral arterial approach using standard catheters available in the USA. This difficulty is avoided by utilizing a common carotid artery approach that eliminates the need to traverse the aortic arch.
Historically, direct percutaneous catheterization of the common carotid artery has been avoided. The deep location and position of the common carotid artery in relation to the sternomastoideus muscle in the neck lead to the recommendation of a surgical cutdown for carotid access in pigs generally. 1 Thus, we sought to evaluate the possibility of two-dimensional and color flow Doppler guided access techniques for percutaneous access of the common carotid artery, obviating the need for a surgical cutdown.
Animals, materials and methods
Seventeen piglets aged 4–6 weeks were included in this study. The piglets were offered no food, but did have access to water, on the day of the operation. Intramuscular injections of telazol 5 mg/kg and xylazine 1–2 mg/kg were given for procedural induction. Hair removal over the ventral neck to the upper chest, soap wash and scrub, and peripheral intravenous line placement were performed. Endotracheal intubation was achieved, and anesthesia was maintained with 1–3% isoflurane. The surgical site was scrubbed with a povidone–iodine solution and then draped in a sterile fashion. Under ultrasound guidance using a SonoSite S Series device with a L25× probe (13–6 mHz, 6 cm scan depth) (FUJIFILM SonoSite Inc, Bothell, WA, USA), a 21 gauge needle was used to access the right-sided common carotid artery. The needle was advanced without an attached syringe thus allowing for pulsatile blood return on vessel entry. The needle was replaced with a 4 or 5 French Terumo Pinnacle® Sheath (Terumo Medical Corporation, Somerset, NJ, USA) using the Seldinger technique. 3 Anticoagulation with intravenous bivalirudin 1 mg/kg was used for the first case only. The subsequent 16 cases received no anticoagulation. Cardiac catheterization and direct right coronary artery injection of contrast and stem cells were completed using Optitorque® internal mammary or Amplatz left catheters (Terumo Medical Corporation). After angiography and cell infusion, all catheters and sheaths were removed by applying manual pressure over the vessel insertion site for 10 min. The site was monitored over the following 120 min and twice daily for 48 h after the procedure.
Our approach to vascular access is as follows:
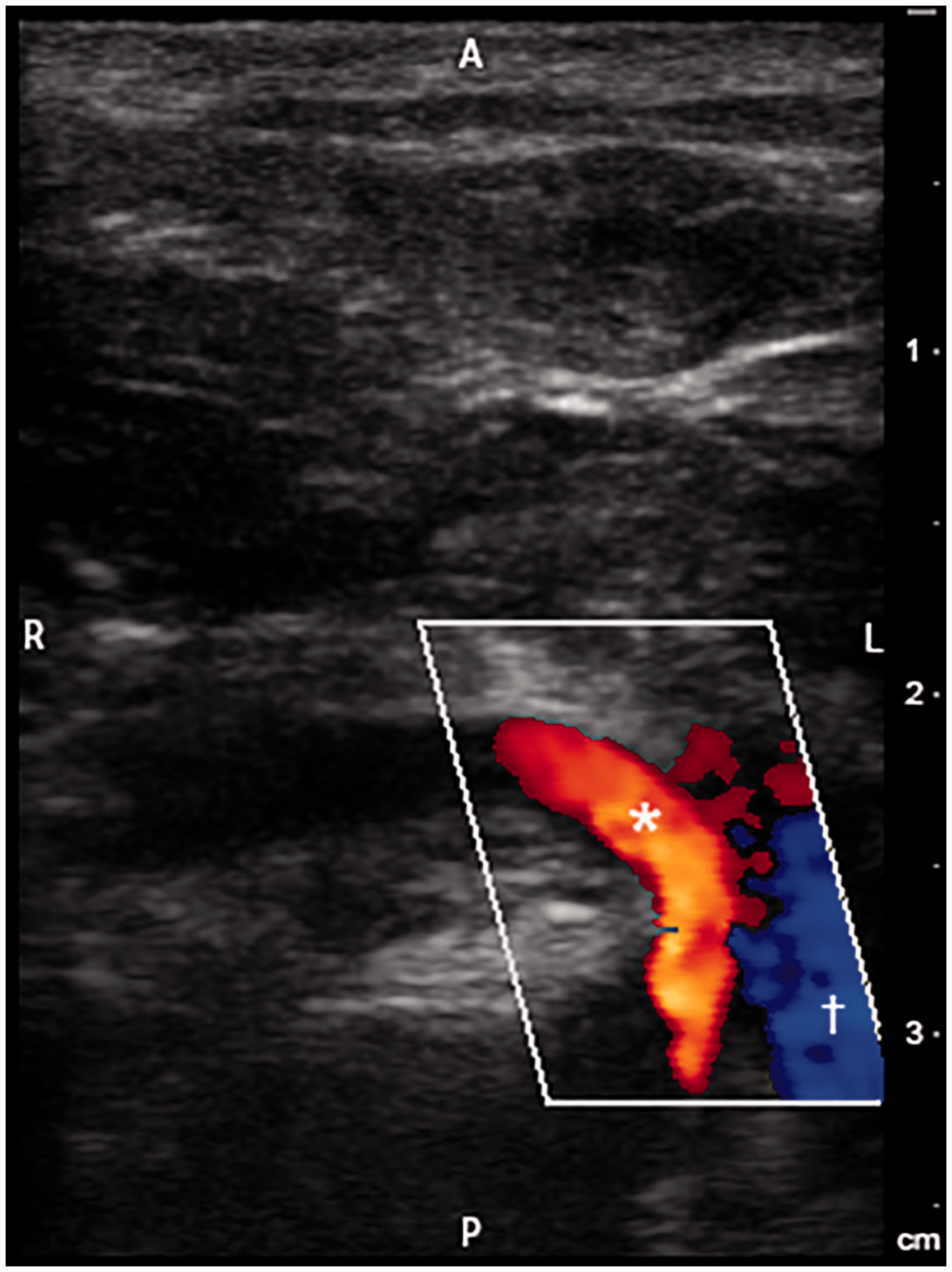
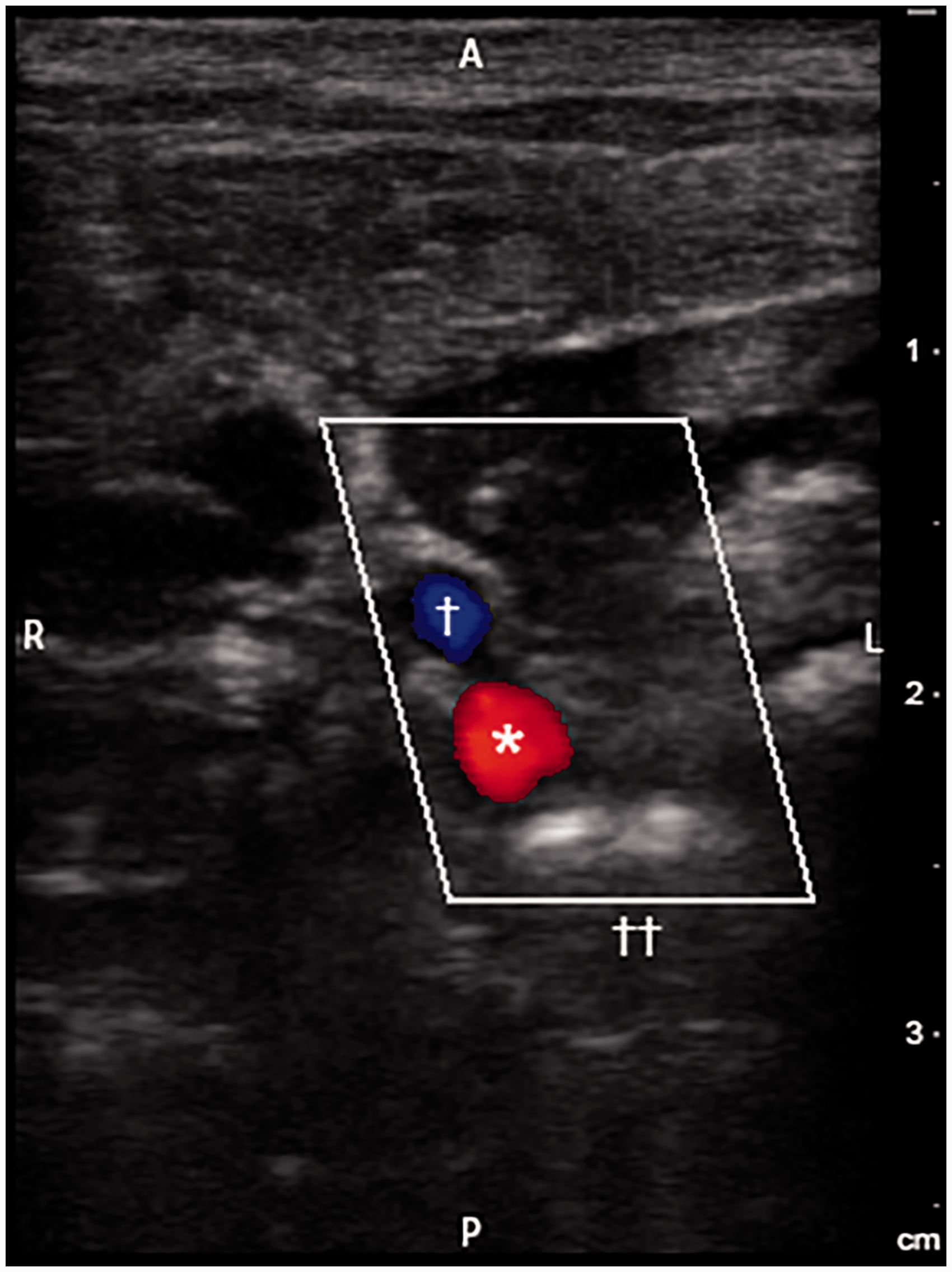
The pig is placed in the supine position under general anesthesia. The manubrium is located with the ultrasound probe placed laterally (the pig’s right side). The left side of the screen is to the pig’s right, confirming the medial/lateral orientation. The probe is swept cranially and caudally on the skin to identify the bifurcation of the right subclavian from the bicarotid trunk (Figure 1). The probe is directed 1–2 cm cranially following the right common carotid as it courses medially to the internal jugular vein (Figure 2). Color flow Doppler assists with vascular identification using this maneuver. Red color indicates flow coming toward the probe (arterial with this orientation) and blue color indicates flow away. The needle is inserted at the central marker of the probe at a 30° angle and advanced through the muscle to the artery. The needle tip is visible on ultrasound. The artery depth is identified on the ultrasound, ranging from 2 to 2.5 cm below the skin with this population. The right common carotid artery or bicarotid trunk is punctured. Pulsatile blood flow from the hub of the needle confirms an arterial source. A wire is advanced through the needle under fluoroscopic guidance. The wire enters the ascending aorta and left ventricle or courses down the descending aorta. If the wire diverts to the right heart border, the access is likely venous and the needle and wire are removed. The needle is removed over the wire, and the hemostatic sheath is advanced. The wire and sheath dilator are removed, and the sheath is flushed prior to cardiac catheterization. When complete, the sheath is removed while applying manual pressure over the vessel insertion site.
Two-dimensional with color flow Doppler ultrasound image obtained in an axial plane at the level of the manubrium. The first brachiocephalic artery bifurcation is visualized with anterior and rightward branching of the subclavian artery (red color; asterisk). Medial to the brachiocephalic artery is the venous confluence forming the origin of the superior vena cava (blue color; cross). A: anterior; P: posterior; R: right; L: left. Two-dimensional with color flow Doppler ultrasound image obtained in an axial plane with the imaging probe cranial to the manubrium. The trachea (double cross) denotes the midline. The common carotid artery (red color; asterisk) courses anteriorly and is rightward of the trachea. Anterior and lateral to the common carotid artery is the internal jugular vein (blue color; cross). A: anterior; P: posterior; R: right; L: left.
All procedures were approved by the Mayo Clinic Institutional Animal Care and Use Committee and conformed to the National Institutes of Health guidelines for ethical animal research.
Results
Successful arterial access and subsequent cardiac catheterization were performed in all 17 piglets. The average weight was 8.5 ± 1.7 kg. The average duration from draping the animal to completion of access was 38.7 ± 15.5 min. If vascular spasm or an inability to pass a wire occurred, the needle was withdrawn and the procedure restarted. The average procedural time from sedation onset to extubation was 100.0 ± 28.8 min. One piglet (1/17, 6%) developed a hematoma with hemorrhaging from the catheterization site and was euthanized. No other complications, such as pneumothorax, vascular perforation, or stroke were encountered.
Discussion
This study describes the successful utilization of ultrasound imaging for percutaneous common carotid access in young domestic swine. Overall, this is a reliable, reproducible, and safe procedure for this population when performed by microvascular experts. Direct access was obtained in all animals, obviating the need for a surgical cutdown. One piglet was euthanized due to hematoma development with hemorrhaging from the access site immediately following line removal. This piglet was the first case and was anticoagulated with bivalirudin, a direct thrombin inhibitor. As a result of this complication, anticoagulation was not administered thereafter and no subsequent hemostatic complications occurred.
The utilization of ultrasound guided arterial access is well established in humans. Seta et al. have reported a reduction in the number of attempts, time to vessel access, and inadvertent vessel access when utilizing ultrasound guidance. 4 Ultrasound imaging facilitates the analysis of vascular depth and size with localization of surrounding structures. A detailed understanding of the vascular anatomy is necessary for this procedure, and this has been previously outlined. 1
Footnotes
Acknowledgements
This work was supported by the Todd and Karen Wanek Family Program for Hypoplastic Left Heart Syndrome, Mayo Clinic Foundation, Rochester, Minnesota, USA. Other members of the Wanek Program for Hypoplastic Left Heart Syndrome Preclinical Pipeline who contributed to this study were: Jennifer Miller, MBA, Joan Wobig, CSA, Jo Powers, Scott Suddendorf, Saji Oommen, PhD and Timothy Nelson MD, PhD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Todd and Karen Wanek Family Program for Hypoplastic Left Heart Syndrome, Mayo Clinic Foundation.
Ethical publication
The authors confirm that they have read the Journal’s publication on issues involved in ethical publication and affirm this report is consistent with those guidelines. This paper is not under consideration elsewhere and none of the paper’s contents have been previously published. All authors have read and approved the manuscript.