
Abstract
Investigation of molecular mechanisms and the efficiency of novel therapeutics for the treatment and prevention of a disease require accurate and accessible preclinical models. Recent developments in personalized medicine employing molecular medicine concepts have favored mice because their genetic make-up is well known and easy to manipulate. For lung cancer, however, orthotopic models in mice are difficult to create due to their narrow glottis openings which act as obstacles to intubation. In the present study, we develop an orotracheal intubation device which gives a clearer view of the narrow mouse glottis and increases the success rate of intubation. We achieved anesthetization via orotracheal intubation using this novel device and then performed a thoracotomy by making an incision between the fourth and fifth intercostal ribs on the right side of the chest. Lung tumor cells were then inoculated at this site. Tumor formation was monitored through bioluminescence optical and magnetic resonance (MR) imagings, which was confirmed by histological analysis. Temperature drop (<35℃) and/or loss of body weight (>30% of the initial body weight) observed during any procedure were used as interruption criteria. This method exhibited high tumorigenicity (100%) and a low mortality rate (8%) at specific sites making it ideal for creating orthotopic lung tumor models and making it particularly useful for sequential follow-up studies using in vivo image analysis.
Lung cancer is the leading cause of death worldwide, and the total number of cases is increasing globally.1–4 Investigation of molecular mechanisms and the efficiency of novel therapeutics for the treatment and prevention of lung cancer require accurate and accessible preclinical animal models. Moreover, recent developments in personalized medicine employing molecular medicine concepts have favored the use of mice due to the fully elucidated genetic make-up of their species. In order to enable such investigations, xenograft mouse models of lung cancer are necessary for examining the disease in vivo as well as providing preclinical venues for the optimization and validation of novel drug treatments. 5
A majority of these preclinical tests involve the use of ectopic models that are created through subcutaneous (SC) implantation of human lung cancer cells in mice. Although SC xenograft models have been used commonly in preclinical studies due to their facile cell implantation techniques and tumor growth monitoring procedures, their use still remains controversial as these models do not truly represent a lung tumor’s biological characteristics in vivo. Orthotopic tumor models, on the other hand, are better representations for testing the efficacy of various anti-cancer agents when performed under more practical and clinically applicable conditions providing better preclinical predications of therapeutics than do SC tumor models.6,7 However, orthotopic tumor models of small animals can be difficult to create due to the size limitations of their anatomies. In particular, mice have narrow glottis openings which act as obstacles to intubation, complicating orthotopic lung tumor model creation.
In prior studies, orthotopic lung tumor models have often been made using non-invasive approaches such as through an intrathoracic injection of lung cancer cells into the right or left thorax by inserting a needle into the lateral dorsal axillary line of the mouse.8–12 This method has the benefits of being simple and non-invasive; however, tumor cells may grow non-specifically in various regions of the lung. An alternative non-invasive method involves the injection of lung tumor cells via the trachea. 13 The technical difficulties of this method, however, serve as limitations for this method as the expertise required to perform such a procedure results in overall high mortalities during operation and in low tumorigenesis rates.
In this study, we introduce a simple method for generating orthotopic mouse lung tumor models via a thoracotomy using an orotracheal intubation. We developed an orotracheal intubation device that gives a clearer view of the narrow mouse glottis while delivering anesthesia gas to the nose simultaneously through an attached line, thus increasing the success rate of intubation for stable anesthesia without the pressure of time constraints on the users. A detailed and technical explanation of how to make such mouse models using this orotracheal intubation device is presented in this report.
Materials and methods
Animals
All animal experiments were performed with a license issued by the Institutional Animal Care and Use Committee (IACUC) of the Samsung Biomedical Research Institute (SBRI, Seoul, Korea). SBRI is a facility accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International and abides by the Institute of Laboratory Animal Resources (ILAR) guide. The mice used in this study were cared for in accordance with guidelines set forth by the American Association for the Accreditation of Laboratory Animal Care (AAALAC). The study group comprised 7–8-week-old BALB/c nude mice (n = 12, Oriental Bio, Seoul, Korea) housed under specific pathogen-free conditions. The animals were housed in a controlled temperature (21℃) and a consistent light cycle (12 h of light, 12 h of darkness). Food and water were provided ad libitum. During each of the following procedures, the animals were administered with ketoprofen (5.0 mg/kg of body weight; Ketopro, Uni Biotech, Chungnam, Korea) for pain reduction if necessary.
Tumor cell preparation
Human non-small cell lung cancer cell lines, PC9, previously validated as stable clones, were obtained from Dr Kazuto Nishio (National Cancer Center Research Institute, Tokyo, Japan). 14 PC9-luc cells were generated using a lentivirus, which encoded the luciferase gene driven by an ubiquitin promoter. The luciferase lentivirus was produced in 293T cells. PC9-luc cells were then infected in the virus-containing medium. After 24 h of infection, the cells were washed in a fresh medium containing G418 sulfate (Invitrogen Life Technologies, Carlsbad, CA, USA) in order to select the infected cells. After 2 weeks of selection, the isolated cells were cultured in a RPMI-1640 medium (Invitrogen Life Technologies) that was supplemented with 10% fetal bovine serum and 1% penicillin/streptomycin (Invitrogen Life Technologies) under 5% CO2 at 37℃.
Orotracheal intubation
The mouse was initially anesthetized with 5% isoflurane (JW Pharmaceutical, Seoul, Korea) and 100% oxygen (flow rate = 8 mL/min) in an induction chamber for 2–3 min. Subsequently, the mouse was transferred to the orotracheal intubation device that included an inhalant anesthesia nose cone specially designed for mice (Figures 1a and b). Anesthesia level was assessed by monitoring the loss of reflexes and the decrease in respiration (60 breaths/min) and heart rate. The upper front two teeth (incisors) of the mouse were hung onto a rubber band that was wrapped around the device. Next, the arms and legs were taped to securely fasten the animal onto the device. For orotracheal intubation, the tongue of the mouse was carefully pulled out using blunt forceps and the blade of a laryngoscope was inserted into the trachea (Figures 1c and d). The magnifier that was attached to the laryngoscope provided a clearer view of the narrow glottis of the mouse. Next, the guide wire of an endotracheal tube (intravenous catheter, 22G) was inserted into the center of the vocal cord and the opposite end of the endotracheal tube was connected to the ventilator to induce artificial ventilation. The respiration rate was set at around 80 cycles per minute and the tidal volume was about 300 µL with an anesthesia level set at about 2%. The intubation procedure took about 10 min.
Images illustrating the orotracheal intubation procedure. (a) Set-up depicting the anesthesia device along with the fixed plate for the mouse. (b) The mouse is placed on its back on the fixed plate and is fastened with tape. The arrow indicates the location of the anesthesia device on the plate. (c) The magnifier attached to the laryngoscope. (d) The endotracheal tube of the laryngoscope is inserted into the trachea of the mouse.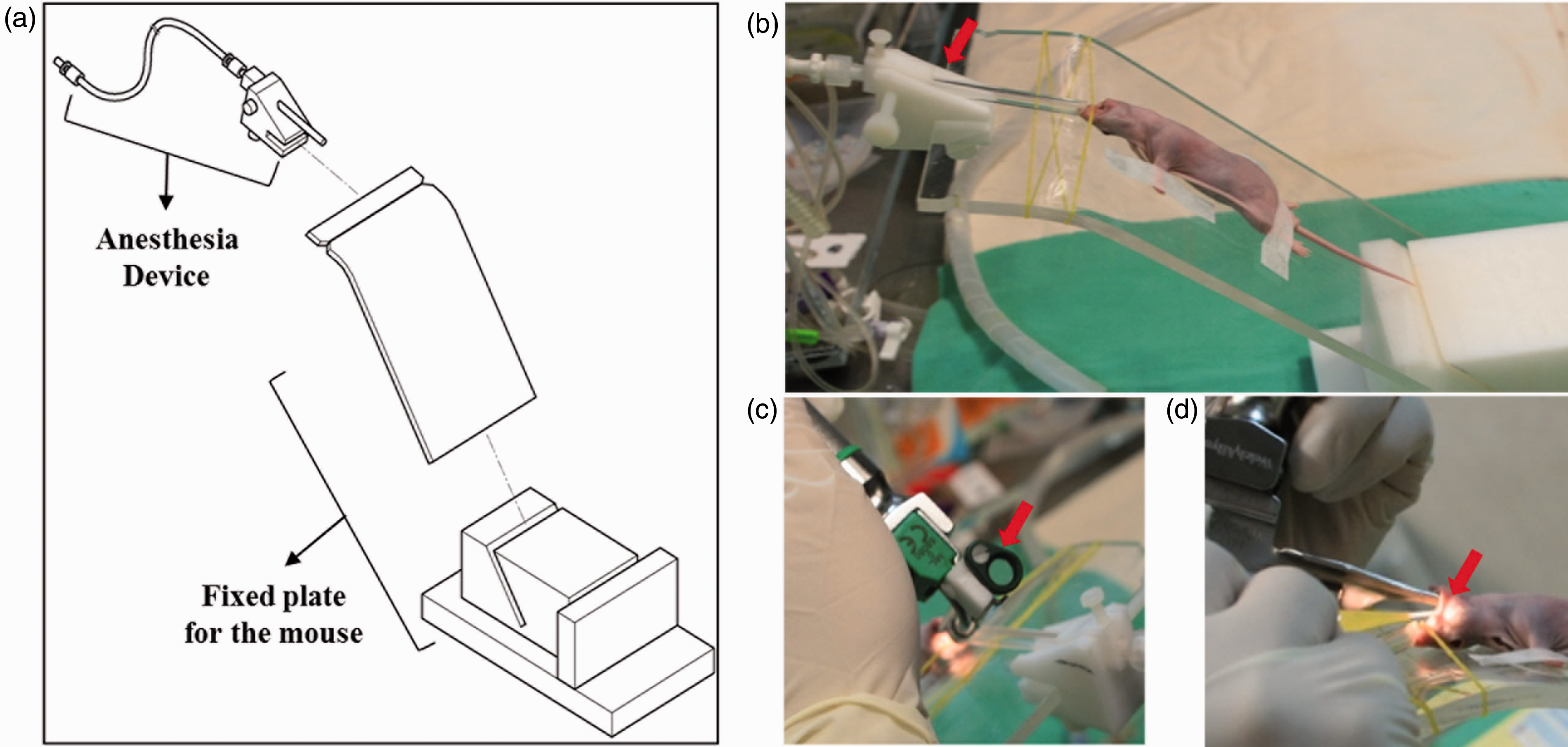
Mouse orthotopic lung tumor model
While maintaining artificial ventilation, the mouse was shifted to the prone position and fastened through taping (Figure 2a). During the procedure, a constant level of anesthesia (70% air, 30% O2 and 1.5% isoflurane) was maintained.
Pictures illustrating the thoracotomy procedure for tumor cell inoculation. (a) The mouse is placed in the prone position. The skin on the right side of the thorax is incised and is exposed through the use of a retractor. (b) Anatomical location of the inoculation point. (c) The first picture (farthest left) is of the middle lobe which is placed aside using a wet gauze. An injection of the tumor cells is made at the inferior lobe and a nodule can be detected afterwards. Following the procedure, the excised skin was closed using sutures.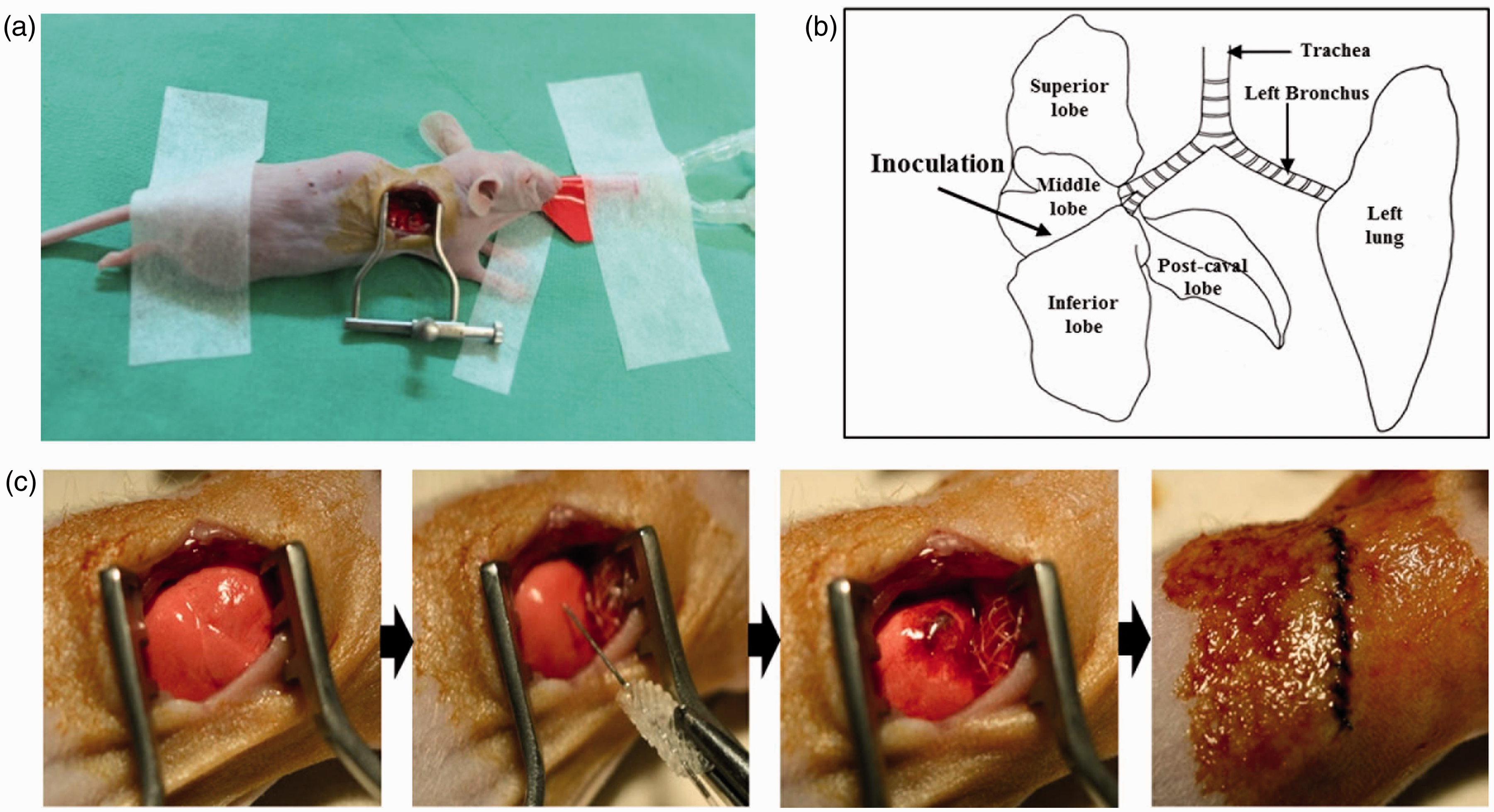
In order to achieve orthotopic inoculation of PC9-luc cells into the lung, the skin covering the right side of the thorax was incised (10–12 mm in length). A transection of the intercostal muscles located between the fourth and fifth intercostal ribs was made and the retractor was used to open up the thoracic cavity to about 15 mm (Figure 2a). In order to prevent damage to the lung tissues, the tidal volume was reduced by one-half. When the retractor was protracted to its fullest, the tidal volume was raised back up to its original level. Afterwards, we used a self-made polyethylene tube (around the size of a P10 catheter) that was connected to the 31G needle of an insulin syringe (Terumo, Leuven, Belgium) in order to inoculate PC9-luc cells into the lung. After finding the middle lobe, a 1 × 1 cm2 square gauze that was soaked in warm saline was used to place the middle lobe aside and to open visibility of the region between the middle and inferior lobes. By holding onto the needle holders, the needle was inserted into the inferior lobe (2–3 mm in depth) (Figures 2b and c). After inserting the needle with precision, 10 µL of the cells (1 × 106 cells per mouse) suspended in Hanks buffered saline solution (HBSS; Invitrogen Life Technologies) containing 1 mg/mL of matrigel (BD Biosciences, San Jose, CA, USA) were injected into the mouse. It was crucial to observe the location where the cells were accumulating, and care was taken to prevent the nodule from bursting (Figure 2c, middle). The rectal temperature of the mouse was also set at around 36–37℃ during the inoculation procedure. After the injection, the wet gauze was removed first, then the rib retractor was removed, and lastly the incised skin was closed using 6/0 silk sutures (Mersilk, Ethicon, Somerville, NJ, USA) (Figure 2c, right end). After the surgical procedure, the animals recovered inside warm water pockets set at 37℃. The time required for tumor cell inoculation through thoracotomy averaged about 10 min per mouse. During each procedural step, if the animal body temperature fell below 35℃, the procedure was stopped in order to avoid needless premature death. Additionally, during the 8 weeks of tumor growth, any animals losing more than 20% of their initial body weight were subjected to euthanasia.
MR imaging
T2-weighted MR images were acquired using a 7 T MR system (Bruker–Biospin, Fallanden, Switzerland) equipped with a 20 cm gradient set capable of supplying up to 400 mT/m with a 100 µs rise-time. A quadrature birdcage coil (35 mm internal diameter) (Bruker–Biospin) was used for excitation and for receiving the signal. The animals that underwent the operation were initially anesthetized using 5% isoflurane and afterwards anesthesia was maintained with 1.5–2% isoflurane in a mixture of O2 and air gases (3:7) by using a facemask. The body temperature (maintained at 36 ± 1℃ using circulating water warming pads) and respiration rates were consistently monitored throughout the duration of the entire scan time. T2-weighted MR images were obtained using a fast spin-echo T2-weighted MR sequence (repetition time (TR)/echo time (TE) = 2000/45 ms, number of experiment (NEX) = 8, echo train length = 4, 100 × 100 mm2 in-plane resolution, slice thickness of 1 mm, and a total of 12 slices). MR imaging was performed at 1, 2, 3, 4, 5, 6, 7 and 8 weeks after tumor cell inoculation.
Optical imaging
In vivo bioluminescence imaging (BLI) was conducted by injecting D-luciferin (150 mg/kg, in phosphate buffered saline (PBS); Caliper Life Sciences, Hopkinton, MA, USA) through the intraperitoneal route in mice inoculated with lung tumor cells. BLI of the mice was performed using an in vivo imaging system (IVIS) (Caliper Life Sciences; exposure time 1–300 s, binning 4/8/16, field of view 23 cm, f/stop 1, emission filter open). Corresponding grayscale photographs and color luciferase images were automatically superimposed and analyzed by using Living Image Software (Xenogen Biosciences Corporation, Cranbury, NJ, USA). Optical imaging was performed at day 1 and weeks 1, 3, 5 and 7 after tumor cell inoculation.
Histology
After conducting follow-up studies for 8 weeks, the mice were sacrificed through CO2 inhalation and their lungs were dissected. The excised lungs were washed in 4% formalin solution and were then embedded in paraffin. The embedded lung tissues were cut into 4 µm sections. Sections of the lung tumors were de-waxed, rehydrated, and rinsed in PBS. Afterwards, heat-induced antigen retrieval was performed in citrate buffer (pH 6.0) for 20 min, endogenous peroxidase was blocked with 3% hydrogen peroxide for 10 min (at room temperature). The isolated lungs were stained using hematoxylin and eosin (H&E) to detect tumor regions in each of the lungs (Figure 3). Tumor regions were identified and differentiations between the tumor and normal tissue regions were made.
Detection of tumor formation through hematoxylin and eosin (H&E) staining of dissected lungs.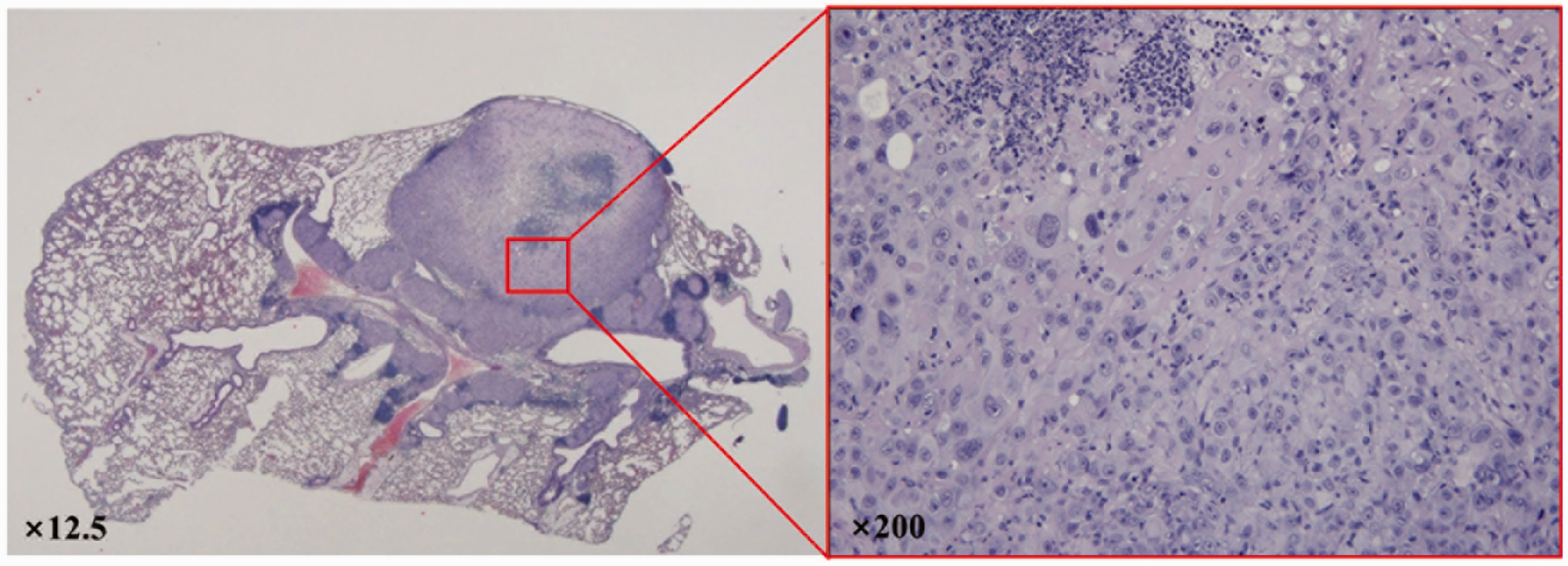
Data analysis
A total of 11 animals which survived through an 8-week follow-up period were included for data analysis. One animal that died within one week of inoculation without any evident reason was excluded for analysis except in the calculation of the mortality rate. To quantify tumor volume from MR images, the area of tumor on each slice of the images were delineated and regions of interest (ROIs) were drawn around the tumor volumes using Paravision software version 5.0 (Bruker–Biospin). Follow-up MR images were taken weekly for 8 weeks after tumor cell inoculation.
Tumorigenicity (number of mice with tumor growth/total number of tumor cell inoculated mice) was evaluated from mice which showed growing tumor nodules from one week to 2∼8 weeks after the inoculation in this work. The paired t-test with a Bonferroni correction was used to evaluate the tumor growth at each measurement point (SPSS 12.0; IBM Corporation, Armonk, NY, USA). All data were expressed as mean ± SD and statistical significance was considered with P < 0.01. The mortality rate was calculated, including the mouse that died within one week after tumor cell inoculation via thoracotomy.
Results
In this study, we demonstrated an improved method for generating orthotopic lung tumor models via thoracotomy using orotracheal intubation in nude mice. We developed an orotracheal intubation device which gave a clearer view of the narrow mouse glottis while delivering anesthesia gas to the nose simultaneously through an attached line, thus, increasing the success rate of intubation for stable anesthesia without the pressure of time constraints for the users. Figure 1 illustrates the orotracheal intubation procedure using the device.
Tumor cell inoculation through thoracotomy using this device allowed tumor growth in an exact location. Figure 2 shows the thoracotomy procedure for tumor cell inoculation. An injection of tumor cells was made at the inferior lobe and a nodule could be detected afterwards (Figures 4a and 5a). During this procedure, significant complications, such as breathing pattern changes, and any behavioral or health problems, were not observed.
Analysis of tumor growth using bioluminescence imaging. (a) Tumor growth was monitored up to 7 weeks and (b) the total flux (photon/s) was also measured from the images. Assessment of tumor growth through magnetic resonance (MR) imaging. (a) T2-weighted MR images acquired weekly for a total of 8 weeks (arrow = location of the lung tumor). (b) Line graph illustrating the variation in tumor volume from the 11 mice observed during the follow-up period.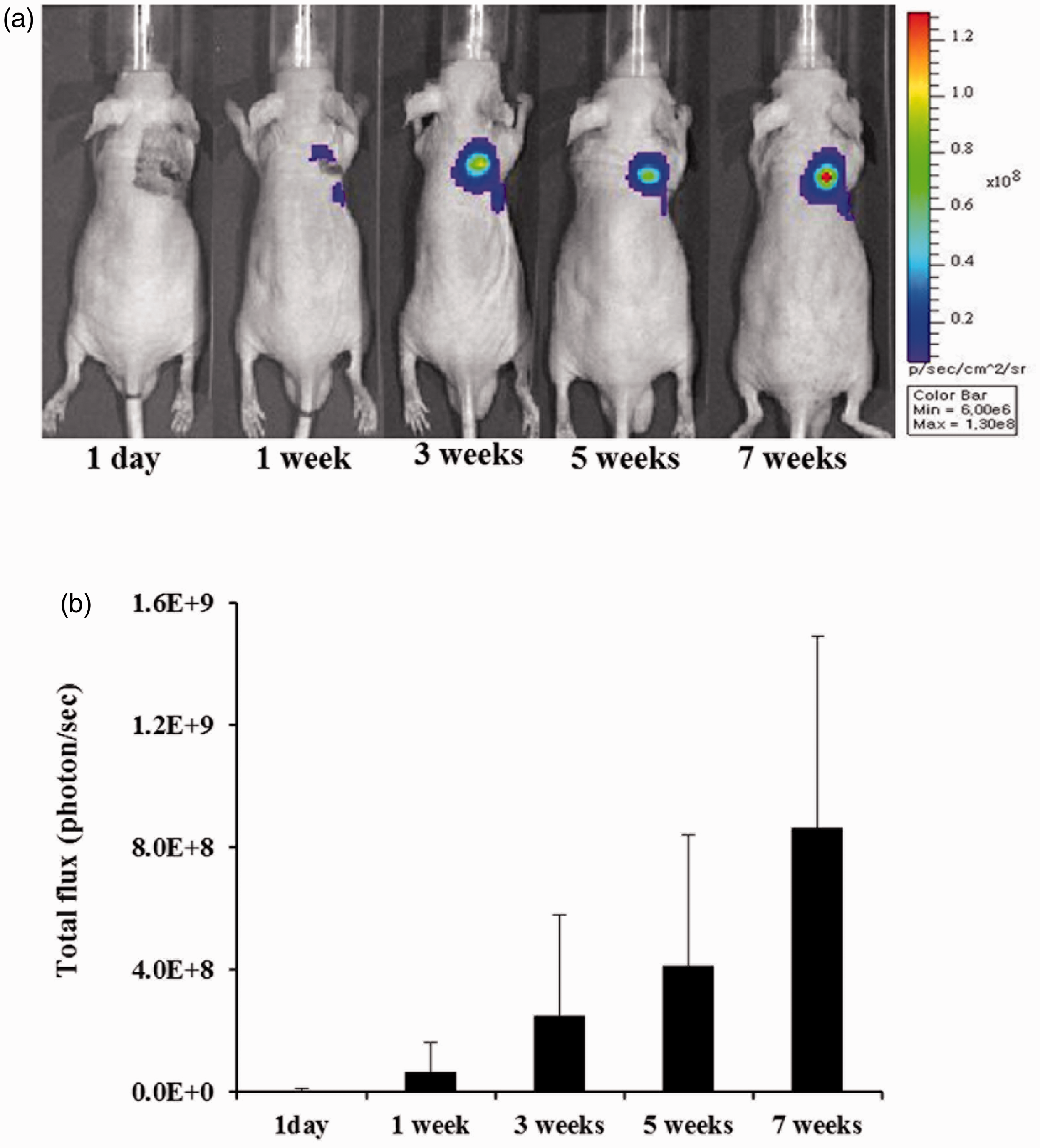
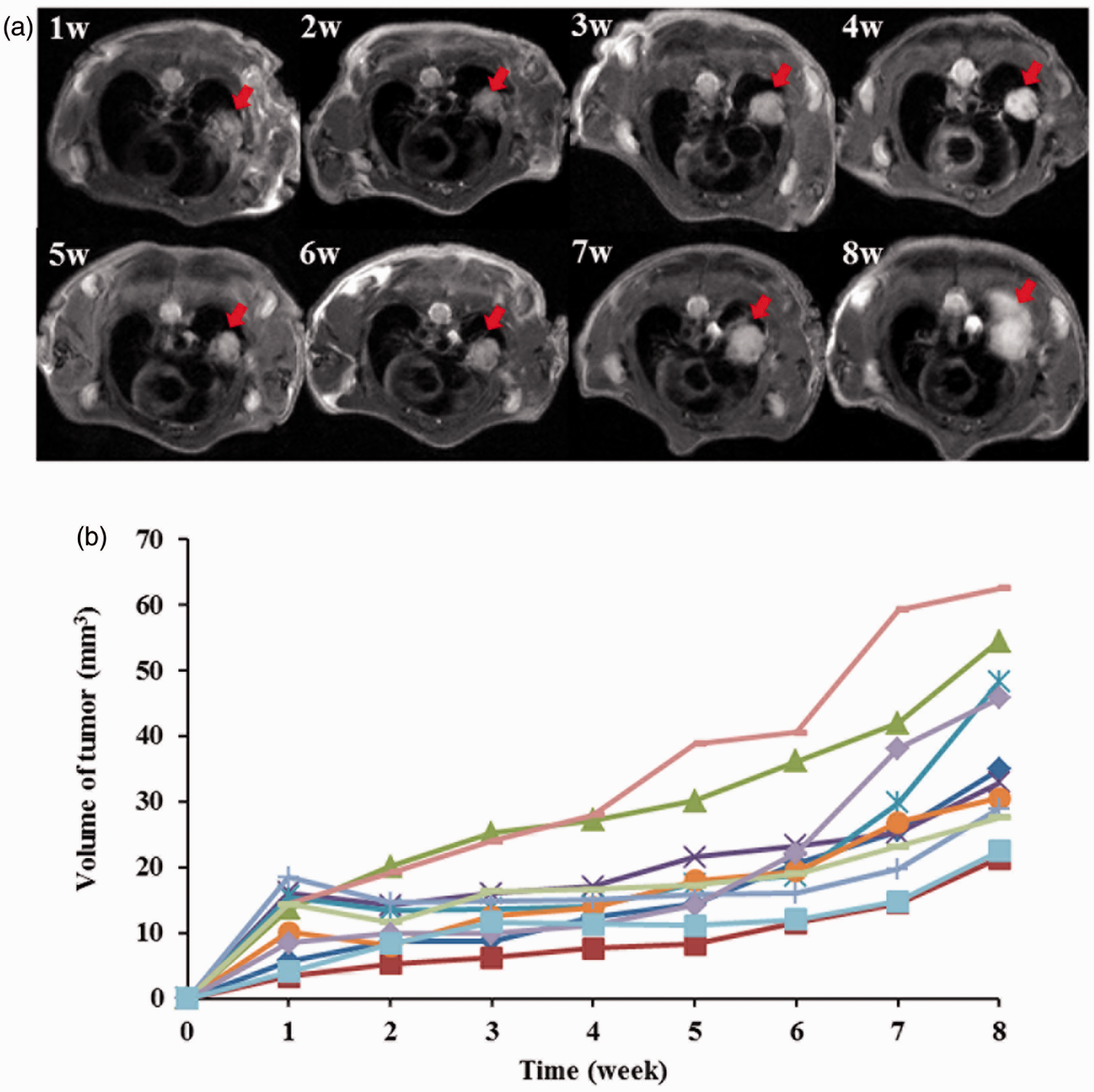
This method is highly useful for imaging studies with long-term follow up because not only can the exact location of the tumor be detected but a clear differentiation can also be made between the tumor and normal tissue. Optical and MR imagings were carried out to confirm the generation of the orthotopic lung tumor model. Both imaging instruments were regularly used for observing tumorigenesis in the lungs for a set amount of time before sacrificing the mice. Since it is easy to confirm tumor progression using optical imaging, we used PC9-luc cells that were encoded with the luciferase gene. Tumor formation and growth were observed from BLIs that were obtained up to 7 weeks after inoculation (Figure 4a). An increase in luciferase expression was also assessed from the increase in total flux (Figure 4b).
Mean tumor volumes (mean ± SD) (n = 11).
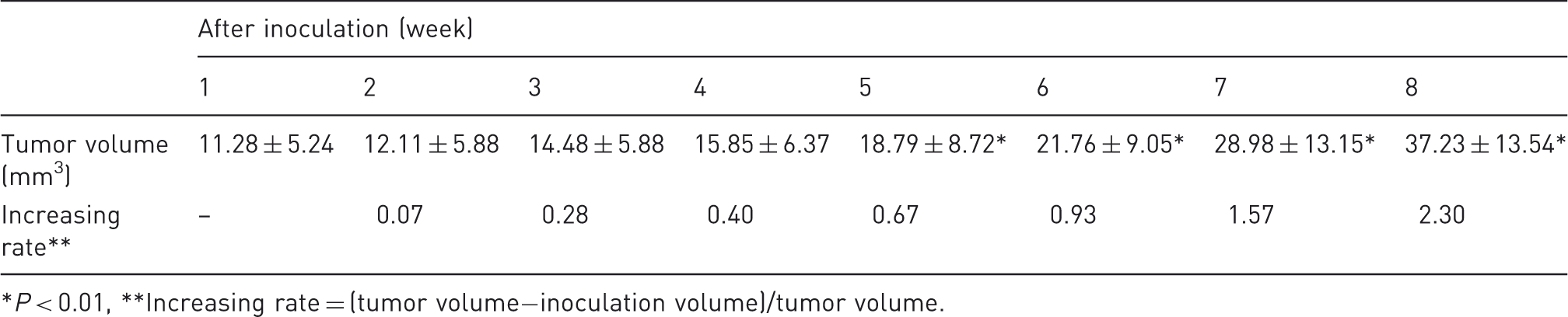
P < 0.01, **Increasing rate = (tumor volume−inoculation volume)/tumor volume.
Through H&E stains, tumor regions were identified and a differentiation between tumor and normal tissue regions was evident (Figure 3).
Discussion
The orthotropic lung tumor model has been used to investigate the molecular mechanisms of the disease and to observe the prognostic process and development of novel therapeutics. Among several orthotopic lung tumor modeling methods, the tail vein injection method has been reported to have a tumor-growing rate of 90–100%. However, this method is disadvantageous in that tumor cells induce pulmonary embolisms which lead to fatality of the animals. 15 The intratracheal injection method also exhibits a high tumor generation rate of about 80%. However, this method also has limitations in that it is difficult to perform without great technical proficiency. 16 Thus, the development of facile orthotopic lung tumor model methods with high tumorigenicity is a present and crucial concern.
In this study, we improved a method used for creating orthotopic lung tumor models through thoracotomy via orotracheal intubation. This method has routinely resulted in high tumorigenicity and low mortality rates. Whereas the advantages of the orthotopic method are two-fold: it provides a biological environment for the tumor to grow as well as a suitable environment for conducting in vivo MR imaging studies of tumors in the lung. In particular, this method is highly recommended when performing active targeting experiments. Depending on cell injection volume, tumor sizes grow rapidly or slowly in orthotropic animal models generated via intra-organ injections. Therefore, thoracotomy seems to be an appropriate method for increasing the success rate as it allows a set cell volume to be injected into a specific region of the target organ.
The procedure also allows non-invasive observations to be made by using imaging modalities such as MR and optical imagings. In non-invasive image analysis, the exact location of inoculated tumor cells as well as consistent size ranges for tumor regions become important factors that must be considered. Tumor location is an absolutely crucial factor to assess during analysis. This matter was recognized as a prime concern from the beginning, in that tumor inoculation was carefully performed solely on the right lung leaving the left lung clean (which is usually preferred). Specifically, the injection was made at the inferior lobe which allowed the lung tumor to form within the borders of the lung instead of growing outside the borders which would have made it difficult to delineate the exact tumor region from the skin and muscle areas. In that respect, the orthotopic lung tumor model made by thoracotomy in this study seems to be extremely useful for longitudinal monitoring of tumor growth. The anatomical accuracy of injected tumor cells makes it easier to assess volumetric measurements and so test drug efficacies using small animal imaging tools.
In conclusion, the intubation procedure developed in this study is efficient and accurate for generating orthotopic lung cancer models allowing delineation of an exact tumor location, along with high tumorigenicity and low mortality. This method is highly useful for imaging studies with long-term follow up because not only can the exact location of the tumor be detected but a differentiation can also be made between the tumor and normal tissue, which can provide valuable information to researchers in the field of cancer. Additionally, evaluation of tumor volume non-invasively using MR imaging can also be beneficial from an animal welfare point-of-view, which may be used as an interruption criterion.
Footnotes
Acknowledgements
This study was supported by the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science, and Technology (2011-0031520 and 2010-0023606), and also by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2008-220-D00112).