
Abstract
Charitable donations are increasingly shifting to online fundraising platforms, where numerous campaigns are displayed simultaneously. This research examines the role of campaign titles in attracting online traffic in this competitive environment, focusing specifically on a major category of medical fundraising. While fundraisers commonly include the names of critical illnesses in campaign titles (critical illness titles), the findings suggest that this emotion-laden driver can negatively impact donation performance. A series of seven studies—combining secondary data, field experiments, and controlled experiments—provides robust evidence for this undesirable critical illness title effect. Moreover, three studies offer mediation and moderation evidence showing that anticipated distress drives this effect. Donors tend to avoid critical illness title campaigns, opting instead for alternatives that still enable them to express empathy. However, this effect diminishes when there is a nondistress cue or when the alternatives are nonjustifiable. This research contributes to the literature on charitable crowdfunding, prosocial behavior, and title effects, offering important practical implications for fundraisers.
With the rapid rise of digitalization and social media, charitable donations are increasingly shifting from traditional channels (e.g., door-to-door fundraising and charitable events) to online platforms like GoFundMe. These platforms enable nonprofit organizations (NPOs) and individuals to solicit public support more efficiently and cost-effectively (e.g., Adena and Huck 2020; Kwak et al. 2018). In 2024, approximately 40% of U.S. donors had contributed through online charitable crowdfunding platforms (Double the Donation 2024; Nonprofits Source 2024). For instance, GoFundMe, a leading U.S. platform, raised over $25 billion by 2022, with 28 million individuals providing or receiving help that year alone (GoFundMe 2022). By early 2024, its cumulative donations had grown rapidly and surpassed $30 billion (Business Standard 2024). In China, an emerging philanthropy market, online giving participation exceeded 51 billion instances between 2016 and 2023, raising $5 billion—a sharp increase from $290 million in 2016 (China News Network 2023). 1
The shift to online platforms brings both opportunities and challenges. In particular, charitable campaigns face fierce competition on these platforms. Unlike traditional channels, where a single campaign is presented in detail via posters or brochures (e.g., Lacetera, Macis, and Slonim 2014; Xu, Mehta, and Dahl 2022; Yang and Hsee 2022; Zhou et al. 2012), online platforms categorize campaigns (e.g., medical, education, environment) and display them collectively. Each category's listing page presents numerous similar campaigns side by side, offering only limited information—typically just a title and brief abstract. This forces potential donors to choose from a crowded field of similar campaigns, making the decision inherently difficult (Broniarczyk and Griffin 2014; Dhar 1997; Tversky and Shafir 1992). Titles, the most prominent feature on listing pages (see Web Appendix A for examples), play a critical role in influencing which campaigns donors click on or screen out (e.g., Defazio, Franzoni, and Rossi-Lamastra 2021).
In light of this, we investigate the impact of campaign titles on donation performance within an important category of medical expenses and explore better title design to enhance outcomes. Medical donations represent a significant market, estimated to have reached $60.51 billion in the United States in 2024 (Giving USA 2025). Yet, rising medical costs continue to leave many struggling to pay their bills (Mayer 2022). As a result, online crowdfunding has become a key alternative, with over one-third of GoFundMe donations dedicated to medical expenses (Martinez 2019). A study by NORC at the University of Chicago (2020) found that 8 million Americans have launched crowdfunding campaigns for themselves, 12 million have launched campaigns for others, and 20% of adults have donated to medical campaigns. The need is particularly acute for critical illnesses, where medical costs are often exorbitant. Thus, enhancing donations for these cases is not only an important research issue but also one with significant social impact.
In this article, we examine a question of particular relevance to fundraisers: whether a critical illness campaign should include the name of the illness in its title. In general, a critical illness refers to a life-threatening condition characterized by vital organ dysfunction (Kayambankadzanja et al. 2022; Painter 2013); examples include severe trauma, burn injuries, and diseases like cancer (Sharma, Mogensen, and Robinson 2019; Shudy et al. 2006). Perhaps unsurprisingly, campaigns for critical illnesses often include their names in titles (hereafter, we denote campaigns that include the name of the critical illness in the title as “critical illness title” and those that do not as “non–critical illness title”). Two prestudies conducted in the United States (N = 716) and China (N = 4,171) showed that a majority of fundraisers—both current and former—strongly prefer critical illness titles when launching campaigns (68.30% in the United States; 80.20% in China; see Web Appendix B for details). These findings suggest a widespread belief among fundraisers that critical illness titles improve fundraising outcomes.
However, contrary to the prevalent belief, this research reveals that critical illness titles, as an emotion-laden driver, can reduce clicks/choices on online fundraising platforms’ listing pages—a phenomenon we term the “undesirable critical illness title effect.” Seven empirical studies, including a secondary dataset of 6,677 fundraising campaigns and six experiments (using both field and experimental data) conducted in the United States and China, consistently support this effect. Furthermore, one mediation study and two moderation studies demonstrate that this effect is driven by anticipated distress: Donors tend to avoid critical illness title campaigns, perceiving that they could lead to greater distress, and instead opt for other campaigns that are just one click away.
In the following sections, we first outline the theoretical background for the proposed effect. Next, we detail the empirical studies that test our hypotheses. Last, we discuss the theoretical and managerial implications of our findings.
Theoretical Background
The Role of Titles on Online Charitable Fundraising Platforms
Titles in online settings are brief summaries that appear at the top of content, such as product descriptions, advertisements, news articles, or online stores. On charitable fundraising platforms, titles refer to short descriptions of campaigns displayed on listing pages. Unlike titles for isolated campaigns in traditional contexts (e.g., charitable events, donation posters, and fundraising emails; Munz, Jung, and Alter 2020; Touré-Tillery and Fishbach 2017; Zhou et al. 2012) or titles for a small set of campaigns that display all information at the same time (Cryder, Botti, and Simonyan 2017; Ein-Gar, Levontin, and Kogut 2021; Sharps and Schroeder 2019), online fundraising platforms typically display numerous campaigns simultaneously on their listing pages, providing only limited information (e.g., title) for each campaign.
Given the simultaneous display of numerous campaigns on fundraising platforms and the resource constraints individuals face (e.g., time and money), donating to all campaigns becomes impractical, necessitating a selection process. This process is cognitively demanding, as platforms typically organize campaigns by category, requiring individuals to first choose a category and then decide among similar campaigns within it. Prior research on decision difficulty and choice overload shows that choosing from similar options is challenging (Dhar 1997; Tversky and Shafir 1992) and cognitively taxing (Broniarczyk and Griffin 2014), especially when the choice set is large (Iyengar and Lepper 2000; Schwartz 2004; Shah and Wolford 2007). Some research on charitable giving has also found that choosing among similar options in the charitable giving context is not only cognitively taxing but also morally taxing and can lead to avoidance behavior (Ein-Gar, Levontin, and Kogut 2021). In the case of online fundraising platforms, where choice sets are extensive and within-category options are often similar, we argue that titles, one of the most salient pieces of information on the listing page, are essential in facilitating the screening and selection process. Their concise format helps reduce cognitive effort when navigating numerous similar options.
The role of titles has been studied in other online settings, such as online news (Kuiken et al. 2017), online advertising (Bergkvist, Eiderbäck, and Palombo 2012), and online shopping (Amazon 2023). However, their impact on charitable fundraising platforms remains underexplored. While there are a handful of articles investigating the cognitive drivers of donations on fundraising platforms, such as peer effects (Castillo, Petrie, and Wardell 2014; Smith, Windmeijer, and Wright 2015), the price of charitable giving (Meer 2014), the effect of matching grants (Meer 2017), the impact of pronouns on perceived credibility and donation (Sepehri et al. 2021), the impact of linguistic framing on perceived dependency and donation (Su et al. 2024), and the quality signaling effect of self-donation (Liu, Gao, and Rao 2025), limited research has studied the emotion-laden driver of donations on these platforms. One exception is a recent article by Yazdani, Chakravarty, and Inman (2025), which investigates how emotions expressed in the cover image and the detail description interact with each other to influence potential donors’ engagement.
In this research, we aim to fill this gap by investigating the role of titles on these platforms with a special focus on an emotion-laden driver, critical illness title, and its underlying mechanism, anticipated distress. We study this driver in one of the most critical categories on online platforms: medical campaigns.
How Titles Can Influence Donations to Critical Illness Campaigns
This research examines whether a fundraising appeal for a critical illness should include the name of the illness in its title (i.e., critical illness title). Critical illnesses, by definition, are severe. Past research on donations to medical campaigns generally finds that highlighting the severity of such cases can increase donations (Ren, Raghupathi, and Raghupathi 2020; Snyder et al. 2017). This is because a higher level of severity in the recipient's need can elicit greater empathy (Chambers and Davis 2012; Cialdini et al. 1997; Fisher and Ma 2014), which is a key driver of charitable behavior (e.g., Bagozzi and Moore 1994; Coke, Batson, and McDavis 1978; Ein-Gar and Levontin 2013; Fisher and Ma 2014; Lee, Winterich, and Ross 2014).
In the context of fundraising titles, one might predict that a critical illness title (vs. non–critical illness title) would better highlight the severity of the recipient's need, thereby increasing empathy and subsequent charitable giving. However, on the listing pages of fundraising platforms, donors encounter countless similar campaigns simultaneously, with only limited information available, such as the title. Thus, this research posits that while donors may feel empathy for many recipients, titles containing words like “cancer” or “tumor” may trigger an expectation that distressing information will appear on the detail page once they click on these titles. In this case, we observe an avoidance behavior: Donors tend to avoid this emotion-laden driver (i.e., critical illness title) due to anticipated distress. This context differs from past research on isolated distressing events, where donors cannot avoid distress and still express empathy (Bagozzi and Moore 1994; Fisher, Vandenbosch, and Antia 2008; Xu, Kwan, and Zhou 2020).
What follows is the detailed reasoning behind why we believe that a critical illness title, compared with a non–critical illness title, may induce greater anticipated distress and avoidance behavior on fundraising platforms.
Critical illness title and anticipated distress
First, by definition, a critical illness title signals a more severe situation for the recipient. Past research suggests that observing or knowing others in severe situations can elicit significant personal distress (e.g., Batson et al. 1983; Batson, Fultz, and Schoenrade 1987; Cialdini et al. 1997). Specifically, Batson et al. (1983) find that witnessing someone in a severe situation can lead to the feeling of personal distress, which increases with the severity of the recipient's situation (Cialdini et al. 1997). Thus, we propose that donors encountering critical illness title campaigns likely anticipate experiencing intense distress if they continue to engage with them.
Second, our argument that a critical illness title elicits greater anticipated distress than a non–critical illness title is supported by extensive research on psychological distancing and emotion regulation. This literature shows that concrete words tend to evoke more intense negative emotions (e.g., distress, anxiety, shame) than abstract words (Kross et al. 2014; Nook, Schleider, and Somerville 2017; Orvell et al. 2019). Moreover, abstracting is an effective way to regulate emotions (Holmes et al. 2024; Kross et al. 2014; Nook et al. 2025; Orvell et al. 2019). For instance, the use of socially close words (i.e., first-person-singular pronouns) increases negative affect compared with socially distant words (i.e., non-first-person-singular pronouns) when people reflect on their own negative experiences (Orvell et al. 2019). Similarly, using temporally close words (i.e., present tense) when writing thoughts and feelings about a negative image heightens negative affect compared with using temporally distant words (i.e., past or future tense; Nook, Schleider, and Somerville 2017). In this context, critical illness terms such as cancer, leukemia, and malignant tumor are inherently more concrete than non–critical illness terms such as condition, illness, and disease. We argue that critical illness titles (vs. non–critical illness titles) prompt more concrete thoughts about the specific disease, thereby increasing anticipated distress. In contrast, non–critical illness titles are more likely to induce abstract thoughts, thus mitigating negative emotions—aligning with the linguistic distancing effect found in the emotion regulation literature (Holmes et al. 2024; Nook et al. 2025; Orvell et al. 2019).
Furthermore, we propose that donors are likely to avoid reading the details of critical illness title campaigns due to greater anticipated distress; that is, greater anticipated distress leads to greater avoidance behavior. This proposition is consistent with prior research suggesting that distress is perceived as a negative, aversive state (e.g., Kopp 1989; Xu, Kwan, and Zhou 2020) that people tend to avoid if possible. For instance, Shaw, Batson, and Todd (1994) find that people are more inclined to avoid emotion-laden appeals for help, particularly when helping is costly, due to the greater anticipated distress these appeals could evoke. A similar pattern has been widely observed in the medical domain. According to this line of research, people tend to avoid learning the risk status of their breast cancer (Melnyk and Shepperd 2012) and accepting genetic counseling when they anticipate the experience of distress associated with their diseases (Thompson et al. 2002). Taking these considerations together, we formally hypothesize:
Possible moderators for the undesirable critical illness title effect
First, if—as we hypothesize—anticipated distress drives the undesirable critical illness title effect, a cue that reduces this distress should mitigate this effect. Here we refer to this cue as a nondistress cue. As discussed previously, witnessing someone in a severe situation and forming concrete thoughts about specific diseases can trigger distress. We therefore propose that a nondistress cue that can turn off donors’ thoughts about the details of severe diseases can reduce the undesirable critical illness title effect. Cues such as uplifting messages, colorful imagery, or soothing music all have the potential to become nondistress cues. Specifically, including such a nondistress cue on the listing page can signal to donors that they are unlikely to encounter distressing content, even if they click on campaigns with critical illness titles. Formally, we hypothesize:
Second, it could be argued that the effect of greater empathy might outweigh the effect of avoidance induced by greater anticipated distress for critical illness title campaigns. While this may hold true in settings where donors consider only one campaign at a time, we argue that the effect could differ in the context of online fundraising platforms. Because the listing pages of these platforms display many similar campaigns concurrently, donors have a convenient and low-cost way (i.e., just one click) to avoid distress while still expressing empathy toward others. In such contexts, we propose that donors are more likely to avoid critical illness title campaigns than non–critical illness title campaigns.
This proposition aligns with past research showing that the ease of escape plays an important role in influencing people's avoidance behavior (e.g., Batson et al. 1981; Batson, Fultz, and Schoenrade 1987; Staub and Baer 1974). When escape is easy and low cost, people tend to avoid experiencing distress (Batson, Fultz, and Schoenrade 1987; Klimecki and Singer 2012). For example, in one experiment, Batson et al. (1981) demonstrated that when escape was made easier, the motivation to reduce one's own distress led to a lower intention to help. In another experiment, Staub and Baer (1974) found that people were less likely to help when escape from the recipient's distress was easy (vs. difficult).
Following this logic, we argue that when online fundraising platforms list justifiable alternatives (e.g., campaigns featuring other needy recipients or situations) alongside critical illness title campaigns, these alternatives provide donors with an easy escape. As a result, donors would be more likely to avoid critical illness title campaigns (i.e., the undesirable critical illness title effect). Conversely, if these alternatives are less needy (e.g., campaigns that have already reached their fundraising goals), making them less justifiable options to avoid distress, the undesirable critical illness title effect is less likely to occur. Formally, we hypothesize:
We tested these hypotheses in seven studies. Study 1, based on a secondary dataset of 6,677 disease-related campaigns from Tencent Charity (the leading online fundraising platform in China), provided preliminary empirical evidence for the undesirable critical illness title effect (H1). Studies 2a and 2b, two field experiments conducted on Tencent Charity and Facebook, respectively, showed that critical illness titles (vs. non–critical illness titles) led to lower click-through rates (CTRs) on both platforms, demonstrating the robustness of the undesirable critical illness title effect (H1). Study 3, a controlled experiment, revealed that the undesirable critical illness title effect occurred on the listing page (rather than the detail page) of the fundraising platform. This finding suggests that the undesirable critical illness title effect is more likely to occur when donors have numerous opportunities available to avoid distress. Study 4 directly measured anticipated distress and tested its role through a mediation approach (H2). Study 5 manipulated the anticipated distress by adding a nondistress cue. The results showed that the undesirable critical illness title effect disappeared when there was a nondistress cue (H3). Finally, Study 6 examined the moderating role of justifiable alternatives, showing that the undesirable critical illness title effect disappeared when the alternatives were nonjustifiable (H4). We provide an overview of all the experimental studies in Web Appendix C (Table W1), which includes a priori power analyses used to determine the sample sizes for Studies 3–6.
Study 1
Study 1 aimed to provide empirical evidence for the undesirable critical illness title effect (H1). The study was conducted on Tencent Charity, a leading online charitable fundraising platform in China, which is accessible via WeChat, the country's most popular social media app. Both NPOs and individuals can initiate fundraising campaigns, which are displayed on the platform's listing pages. 2 When browsing the listing page (see Web Appendix A for an example), users can view a campaign's title, labels, and abstract (limited to the first 16 characters at the time). To access more detailed information, users can click on a campaign's title, which directs them to the detail page containing the fundraising target, full description, and other specifics. Donations are made by clicking the donation button on the detail page and selecting an amount to complete the transaction.
We collected campaign-level data from the medical category of Tencent Charity. The dataset included 6,677 campaigns initiated between 2011 and 2018, all of which had concluded by the end of 2018. These campaigns received over 10 million donations, totaling more than $33 million. 3 For each campaign, we collected the following variables: number of donations, total donation amount, fundraising target, start and end dates, whether the campaign was initiated by an NPO, and the text from its title, abstract, labels, and detailed description.
Notably, because the platform lacks data on the number of clicks on the listing page, we used the total number of donations as a proxy. We acknowledge that this is not a perfect proxy as the total number of donations reflects not only the clicks on the title (i.e., the dependent variable in our hypotheses) but also the subsequent donation decisions made after accessing the campaign's detail page. To mitigate this limitation, we included control variables in our model to account for the content presented on the detail page. Despite this limitation, we believe this large-scale, real-world study provided a valuable context for testing H1. To address this issue further, we obtained direct measures of clicks on the title in subsequent studies.
Dictionary of Critical Illnesses
For clarity, in this section we refer to the textual information in the title, abstract, and labels displayed on the listing page as “title information.” Identifying the link between a campaign's title information and the critical illness it addresses is important for this analysis. Unfortunately, no universal dictionary of critical illnesses exists. To construct such a dictionary, we followed a two-step process. First, we extracted nouns representing illnesses from the title information of all campaigns in our sample to construct a dictionary of illnesses. Second, we classified each illness in this dictionary as either critical or noncritical using various sources. The final output was a dictionary of critical illnesses, developed based on different criteria. The details of each step are outlined subsequently, with the procedures illustrated in Web Appendix D.
Step 1
We first segmented the words from the title information of all campaigns and classified them into parts of speech (e.g., adjective, verb, noun). Next, we retained only the nouns, as they typically represent names of illnesses. This resulted in a set of 8,445 words. Three research assistants (RAs), who were masked to the study's hypotheses, were then hired to identify illnesses within this set based on predefined guidelines (see Web Appendix D). Specifically, each RA independently reviewed all words and labeled those they believed to be illnesses. Nouns that were identified as illnesses by all three RAs were directly included in the illness list. For nouns that were labeled as illnesses by some but not all RAs, independent external validation (e.g., internet searches) was conducted, and the RAs engaged in discussions among themselves to reach a consensus; only nouns that were unanimously agreed on were included as illnesses. Ultimately, 403 nouns were identified by all RAs and marked as illnesses. We refer to this compilation as the “illness list.” The complete list in both Chinese (the original source) and English (translation) is provided in Web Appendix D.
Step 2
We classified the illnesses in the illness list as either critical or noncritical using two sources: medical experts and potential donors. The first source provided a more professional definition of critical illness. However, professionally differentiating critical (vs. noncritical) illnesses requires specialized, and sometimes extensive, medical knowledge that is not available to potential donors. To address this, the second source sought to capture the perceived criticality of illnesses from the perspective of potential donors.
First, we recruited two medical experts to review the illness list and identify those they considered critical. 4 In total, 105 illnesses were labeled as critical; we refer to this categorization as “critical_expert.” Second, we conducted an online survey targeting potential donors. We partnered with a research team specializing in nationwide donor research in China that used a survey panel from InsightWorks. 5 We embedded our questionnaire within their survey's redirect link. Only participants who had previously donated were directed to our survey.
A total of 3,665 participants who had previously donated participated in our study for a small monetary compensation (42.51% male, 57.49% female, .00% other; Mage = 33 years, SD = 11.54). To manage the task load, each participant reviewed 10 of the 403 illnesses from the illness list and was asked to indicate if they were critical illnesses (i.e., “Please determine whether each illness is a critical illness”; 1 = “yes,” and 2 = “no”). We conducted a series of one-sample proportion tests with 50% as the hypothesized value. The results showed that 190 illnesses were significantly more likely to be identified as critical. We refer to this categorization as “critical_donor.”
In Web Appendix D, we provide the complete lists of critical illnesses according to the critical_expert and critical_donor categorizations. These two categorizations are based on different criteria. As a result, they overlap: 89 illnesses are classified as critical by both groups. However, the two lists are not nested within each other. We refer to the set of illnesses meeting both groups’ criteria as “critical_both.”
Data Summary
We classified a campaign as a critical illness title campaign if its title information included any item from the previously constructed list of critical illnesses. Based on critical_expert, 3,501 campaigns (52.43%) were critical illness title campaigns, while 3,830 campaigns (57.36%) were classified as critical illness title campaigns according to critical_donor. A total of 3,387 campaigns (50.73%) were critical illness title campaigns under both criteria.
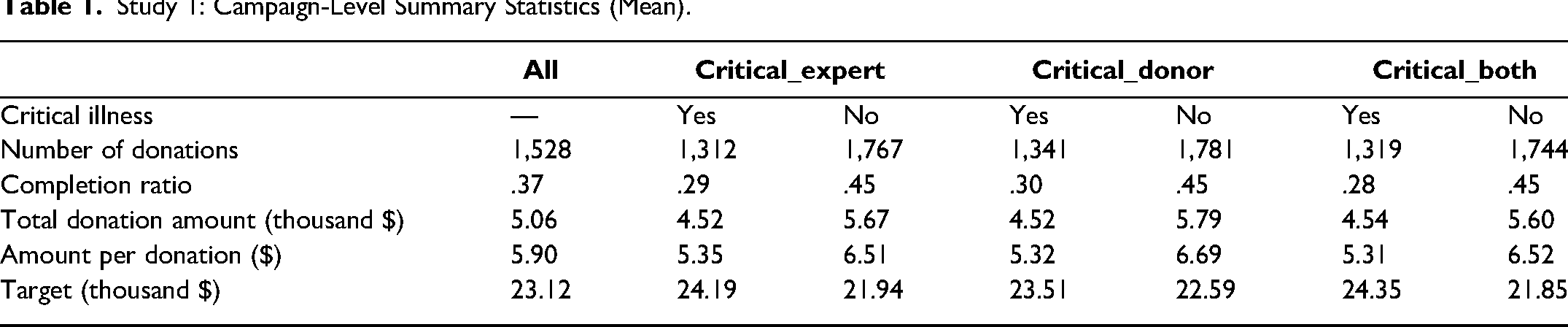
We present the campaign-level summary statistics for several key variables in Table 1 (see Web Appendix D for more descriptive statistics), broken down by title types based on different definitions of critical illness. On average, these campaigns set a target of $23,000, received 1,528 donations, raised $5.90 per donation, and achieved 37% of their fundraising target. On average, critical illness title (vs. non–critical illness title) campaigns consistently received fewer donations regardless of the classification criteria, which aligns with our main hypothesis. In the following analysis, we further explore this relationship using formal regression methods. Additionally, the data reveal interesting patterns for other variables outside the scope of this article. Specifically, critical illness title (vs. non–critical illness title) campaigns had larger targets, lower completion ratios, smaller total donation amounts, and lower amounts per donation.
Study 1: Campaign-Level Summary Statistics (Mean).
Regression Analysis for Total Number of Donations
In this section, we conducted formal regression analysis to test H1. As noted previously, we used the total number of donations as a proxy for the number of clicks on the title. Our goal was to examine whether critical illness titles were associated with the total number of donations for the campaigns. Specifically, we ran the following regression:
The variable Xi included a set of controls as follows. First, since campaign size and initiator type were important factors, we controlled for the campaign's target and its square, as well as whether it was initiated by an NPO. Second, seasonality could influence donations, given that our sample covered multiple years; thus, Xi included calendar year-month dummies for the date when campaign i was launched. Third, a campaign's title information might correlate with its detailed description, which appears on the campaign's detail page after users click on the title. To isolate the effect of the title, we controlled for variables capturing content on the detail page. We first included the total number of words in the detailed description. Next, we used the Chinese version of Linguistic Inquiry and Word Count (LIWC; Netzer, Lemaire, and Herzenstein 2019), a widely used dictionary for textual analysis. This dictionary categorizes nearly 6,400 words into 65 categories that include pronouns, tenses, social, cognition, and affect. Specifically, we included the percentages of words in campaign i's detailed description belonging to each of the 65 categories. Finally, some aspects of the campaign's title information could confound the results, as they might be related to the key explanatory variable, CITitlei (whether campaign i is a critical illness title campaign), and also affect the dependent variable. Thus, we controlled for two important factors: the length of the title information (i.e., the number of words) and the percentages of words in the title information that belong to each of the four emotion categories (positive emotion, anxiety, anger, and sadness) in LIWC.
We ran regressions using the three definitions of critical illness (i.e., critical_expert, critical_donor, and critical_both) as described previously. The results are reported in Panel A of Table 2. All findings were consistent across these definitions. For clarity, we focus on the results based on critical_expert. Critical illness title (vs. non–critical illness title) campaigns attracted significantly fewer donations by an average of 498. This aligns with H1. Given that the average number of donations across all campaigns was 1,528 (see Table 1), the effect is sizable. To test the robustness of our results, we replicated the analysis using a more specific estimation sample that included only campaigns where the detail page mentioned critical illnesses (5,181, 5,844, and 5,123 campaigns based on the critical_expert, critical_donor, and critical_both definitions, respectively). This sample focused on campaigns specific to critical illnesses. The results, shown in Panel B of Table 2, are largely consistent with those in Panel A.
Study 1: Main Regression Results (DV: Total Number of Donations).
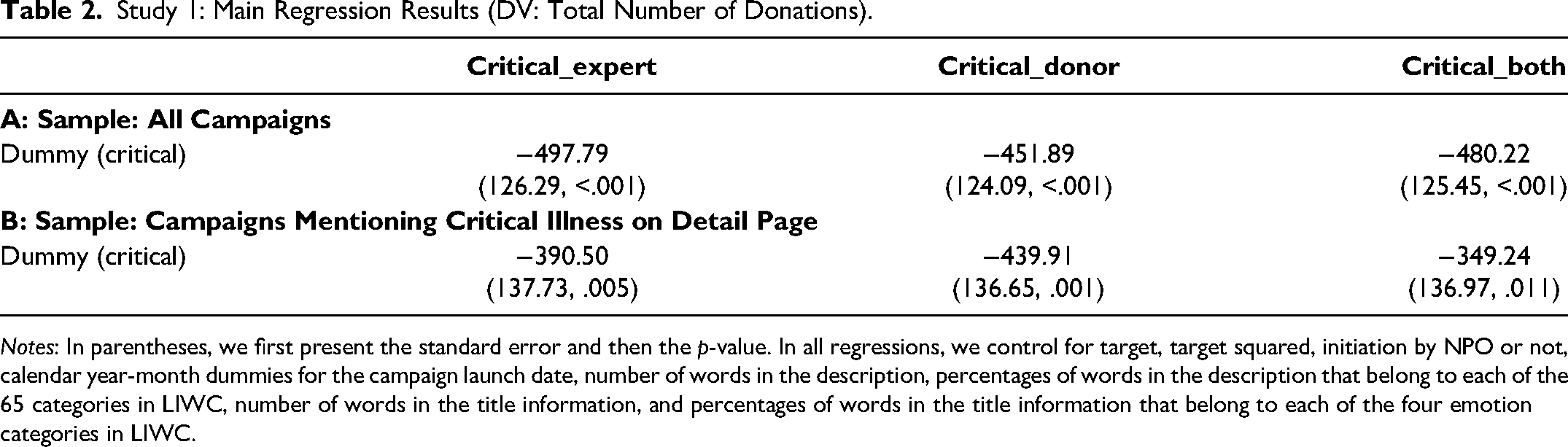
Notes: In parentheses, we first present the standard error and then the p-value. In all regressions, we control for target, target squared, initiation by NPO or not, calendar year-month dummies for the campaign launch date, number of words in the description, percentages of words in the description that belong to each of the 65 categories in LIWC, number of words in the title information, and percentages of words in the title information that belong to each of the four emotion categories in LIWC.
Regression Analysis for Other Outcome Variables
Though other outcome variables—such as completion ratio, total donation amount, and amount per donation—are beyond the scope of this article, they are also important measures of fundraising outcomes. For completeness, we examine their relationship with critical illness titles in this section. We replicate the analyses from the previous section using different dependent variables and report the results in Web Appendix D. All results were generally consistent across the three definitions, though significance levels occasionally varied. In most cases, critical illness title (vs. non–critical illness title) campaigns had a significantly lower completion ratio and total donation amount. The previous finding—that critical illness titles decrease the total number of donations—appears to be the main driver of these patterns as the amount per donation did not differ significantly between these two types of campaigns.
Summary
The data from Tencent Charity provided initial support for the undesirable critical illness title effect in a large-scale, real-world context. Specifically, our results indicated that critical illness title (vs. non–critical illness title) campaigns attracted significantly fewer donations, consistent with H1. This finding held after controlling for potential confounders and was robust across different definitions of critical illness and estimation samples. Further analysis of other outcome variables showed that critical illness title (vs. non–critical illness title) campaigns fell short of fulfilling their targets, primarily due to the decline in the number of donations.
A limitation of Study 1 is the lack of direct data on the CTRs of campaign titles on the listing page. While our results show that critical illness titles lead to fewer donations, this could be due to a lower CTR on the listing page or to a lower donation rate (i.e., donations conditioned on viewing the detail page). Although we controlled for variables related to the detail page content, we cannot completely rule out the possibility of a lower donation rate on the detail page. Another limitation is that titles on the listing page are presented alongside pictures. Given that images can influence potential donors’ affective and cognitive responses (Hsee and Rottenstreich 2004; Hung and Wyer 2009), the presence of pictures may have affected the title effect observed in this study. While the impact of pictures on donations is an interesting avenue of investigation, it lies outside the scope of this research and warrants future exploration. Additionally, as shown in Table 1, critical illness title campaigns, on average, had higher fundraising targets, which may signal greater severity and induce a “drop-in-the-bucket” effect. To mitigate this confounding effect, we controlled for the campaign target (and its square) in Study 1. In addition, we conducted Studies 2a, 2b, and 3 with random assignment, better controls, and direct measurements of clicks/choices on the listing pages to further test H1.
Study 2a
The goal of Study 2a was to further test the undesirable critical illness title effect on a real-world charitable fundraising platform, Tencent Charity, which is also the source of data for Study 1. Unlike Study 1, which used a large-scale secondary dataset, Study 2a employed a randomized field experiment. 6 This design allowed us to create identical campaigns with either critical illness titles or non–critical illness titles. Additionally, we were able to directly observe CTRs and investigate the causal impact of title type on CTRs on the listing page.
Design and Procedure
Study 2a was conducted in collaboration with Tencent Charity in China and involved three fundraising campaigns for critical illnesses: tumor, leukemia, and neuroblastoma. These campaigns were grouped together in a single section on the platform's listing page, which was themed around medical relief. This medical section is one of several on the platform, with others focusing on topics like education, environmental protection, rural development, and support for disadvantaged groups. Each section typically contains three to four related campaigns. Tencent Charity agreed to share experimental data with us only at the section level, not at the individual-campaign level.
To investigate the impact of critical illness titles versus non–critical illness titles on the CTR of this medical section, we designed two versions of titles for the three campaigns within the section (see Web Appendix E for the stimuli). One version included a “critical illness” word in each title (e.g., “[Tumor] children living in remote rural areas need your help”), while the other omitted the “critical illness” word (e.g., “Children living in remote rural areas need your help”). Notably, the campaign images remained identical across both versions to control for the influence of visuals, isolating the effect of the title wording. Using Tencent Charity's A/B testing function, we randomly assigned potential donors to view one of the two versions. Some viewers saw the critical illness titles, while others saw the non–critical illness titles. After clicking a specific campaign, viewers were directed to the campaign's detail page, where they could proceed to make a donation (as shown in Web Appendix E).
This field experiment ran for five days, from Friday, February 10, to Tuesday, February 14, 2023, none of which were holidays. During this period, the campaigns on the platform's listing page remained unchanged except for the manipulated titles in our experimental campaigns. All other campaigns retained their titles and content throughout the experiment.
Tencent Charity provided section-level data for each version (critical illness titles vs. non–critical illness titles), including the number of impressions (i.e., users exposed to each version) and the number of clicks (i.e., users who clicked on each version). The section's CTR, calculated as the ratio of clicks to impressions, served as our key dependent variable.
Results and Discussion
A total of 23,286 users on Tencent Charity were exposed to the target section, and 3,251 users clicked on one of the two versions. A comparison of the two versions showed that critical illness titles (vs. non–critical illness titles) generated 173 fewer clicks (see Table 3). To assess the effect of critical illness titles on CTR, we conducted a two-proportion z-test. The results revealed a significant difference in CTR between the two versions (z = 2.40, p = .016, d = .03). Critical illness titles produced a lower CTR than non–critical illness titles (13.41% vs. 14.50%), 7 representing a 7.52% decrease (i.e., 1 − 13.41/14.50). This study demonstrates the undesirable critical illness title effect in a randomized experiment on a large fundraising platform with real donors, further supporting H1.
Study 2a: Data Summary for Critical Illness Title Versus Non–Critical Illness Title Campaigns.

As an additional exploration beyond the scope of this article, we found that critical illness titles (vs. non–critical illness titles) were associated with a lower amount per donation (12.69 RMB vs. 17.47 RMB) and a lower total donation amount (14,321.47 RMB vs. 20,069.91 RMB) on the detail page. However, since randomization occurred at the impression level, these differences on the detail page are correlational, not causal.
Study 2b
The goal of Study 2b was to further test the robustness of the undesirable critical illness title effect on a social media platform: Facebook. Unlike the charitable fundraising platform in Study 2a, where users likely have an active goal to donate and are likely in the decision-making stage of selecting a campaign, Facebook is a general social media platform where users are less likely to have an active goal to donate. This study aimed to examine whether the undesirable critical illness title effect persists on a platform primarily used for daily social interactions.
Design and Procedure
Study 2b was a preregistered field study conducted on Facebook (https://aspredicted.org/g7mr-wkkb.pdf). To minimize potential familiarity effects, we created HopeWeb (https://sites.google.com/view/hopeweb), a new fundraising site, and promoted it through Facebook ads. HopeWeb featured four fundraising campaigns: one target campaign and three control campaigns. The target campaign raised funds for children with tumors and was used to manipulate critical illness title versus non–critical illness title. The three control campaigns raised funds for children lacking water, affected by hurricanes, and impacted by floods, respectively. Each campaign was linked to an active fundraising campaign, and we presented these on HopeWeb with direct links to their original pages.
Using Facebook's A/B testing function, we ran two sets of carousel ads to promote HopeWeb. Each set began with the introduction: “Support a fundraising campaign and make a difference today! Your contribution can truly help someone in need!” This was followed by four carousel cards, each corresponding to one of the four campaigns featured on HopeWeb (see Web Appendix E for the stimuli).
For the target campaign, we designed two versions of the titles: one with a “critical illness” word (e.g., “Heartbreaking Urgency: Desperate Children Overwhelmed by Malignant Tumors”) and the other replacing the “critical illness” word with a “non–critical illness” word (e.g., “Heartbreaking Urgency: Desperate Children Overwhelmed by Illnesses”). Depending on the assigned carousel ad set, users viewed either the set with the critical illness title target campaign or the set with the non–critical illness title target campaign, both with the same three control campaigns. Once viewers clicked on a card within the carousel ads, they were directed to the corresponding campaign's detail page on HopeWeb. The CTR of the target campaign—calculated as the ratio of clicks (i.e., users who clicked on the target campaign) to impressions (i.e., users exposed to the ads)—served as our key dependent variable.
This field experiment ran for seven days, from Saturday, September 8, to Friday, September 14, 2024, with no holidays during this period. The settings were as follows: objective—traffic; age—18–65; location—United States; language—English; optimization—link clicks; bid strategy—highest volume; and budget—$20 per carousel ad set per day.
Results and Discussion
A total of 25,932 impressions and 467 clicks were recorded for these carousel ads (see Web Appendix E for details). Of these, 109 clicks were on the target campaign. Compared with the non–critical illness title version, the critical illness title version generated 19 fewer clicks (Table 4).
Study 2b: Data Summary for Critical Illness Title Versus Non–Critical Illness Title Campaigns.

To examine the effect of critical illness title on the CTR of the target campaign, we conducted a two-proportion z-test. The results revealed a significant CTR difference between the two versions (z = 1.99, p = .047, d = .03), with the critical illness title yielding a lower CTR than the non–critical illness title (.34% vs. .50%), a 32.00% decrease (i.e., 1 − .34/.50).
Study 2b demonstrated the robustness of the undesirable critical illness title effect on a social media platform, further supporting H1. It also offers practical implications for NPOs and other fundraisers on how to effectively promote critical illness campaigns on social media. Together, Studies 1, 2a, and 2b demonstrated the robustness of the undesirable critical illness title effect. These studies were conducted using a large secondary dataset and two field experiments, one on a charitable fundraising platform and the other on a social media platform, involving both Chinese and U.S. participants.
In this research, we argue that the undesirable critical illness title effect is driven by anticipated distress. This effect is likely to occur on the listing page, where donors have many alternatives to avoid distress while still expressing empathy. On the detail page, however, donors are immediately faced with distressing information. They cannot undo this exposure by choosing not to donate to the critical illness title campaign. As a result, avoidance behavior is less likely to occur.
Study 3
Study 3, a controlled experiment that manipulated the listing and detail pages in a between-subjects manner, aimed to demonstrate that the undesirable critical illness title effect is more likely to occur on the listing page, where donors have many alternatives to avoid distress while still expressing empathy. In contrast, on the detail page, this avoidance behavior is less likely to occur.
To achieve this goal, we manipulated title type (critical illness title vs. non–critical illness title) and donation stage (listing page vs. detail page) in a 2 × 2 between-subjects design. This was a preregistered study, with a target sample of 400 U.S.-based participants recruited through Prolific (https://aspredicted.org/NYN_K8F). A total of 400 participants completed the survey for $.18 (£.15) in compensation. As preregistered, we excluded participants who failed an attention check (N = 52), yielding a final sample of 348 participants (47.70% male, 51.15% female, 1.15% other; Mage = 40 years, SD = 12.19).
Design and Procedure
This study employed a 2 × 2 between-subjects design, with two factors: title type (critical illness title vs. non–critical illness title) and donation stage (listing page vs. detail page). In the listing page condition, the key dependent variable was campaign choice. In the detail page condition, we used donation rate and amount per donation as key dependent variables to mirror real donation decisions.
In this study, participants were first asked to imagine browsing an online charitable fundraising platform for people in need. In the listing page condition, participants were randomly assigned to one of two title type versions. In the critical illness title version, there were two critical illness title campaigns (e.g., “Gasping for Air: Save This Child from a Deadly Cancer”) and four control campaigns. In the non–critical illness title version, there were two non–critical illness title campaigns (e.g., “Gasping for Air: Save This Child from a Deadly Condition”) and four control campaigns. These two critical illness title/non–critical illness title campaigns were the target campaigns. The four control campaigns were the same in both versions. Participants were asked to select one campaign they preferred to learn more about from the list of six. Their choice of target campaign from the list constituted our key dependent variable in the listing page condition: campaign choice.
In the detail page condition, participants were not shown a listing page to avoid any influence of previous choices on decisions made on the detail page. Instead, they were directly shown the detail page, which provided only the detailed information of the same fundraising campaign (i.e., a story about a seven-year-old girl with lung cancer). This fundraising campaign was presented with either a critical illness title (“Gasping for Air: Save This Child from a Deadly Cancer”) or a non–critical illness title (“Gasping for Air: Save This Child from a Deadly Condition”); see Web Appendix F for stimuli. In this condition, participants saw only one fundraising campaign with detailed information. They were asked to specify what portion (0%‒100%) of their compensation they would donate to this campaign. The donation amount was calculated by multiplying the chosen percentage by £.15. This measure captured two key dependent variables in the detail page condition: the donation rate (i.e., the proportion of participants who indicated a nonzero donation percentage) and the amount per donation.
Prior research has shown a robust link between individuals’ past donation behavior and their propensity for future donations (e.g., Gneezy et al. 2012). To capture this, we included a binary question asking participants whether they had donated before. Demographic information, including age and gender, was also collected.
Results and Discussion
For the listing page condition, a chi-square test was run to examine the relationship between title type (critical illness title vs. non–critical illness title) and campaign choice. The analysis revealed a significant difference in campaign choices based on title type (χ2(1, N = 182) = 4.28, p = .039, d = .31). Specifically, participants in the critical illness title condition were less likely to choose target campaigns (vs. control campaigns) compared with those in the non–critical illness title condition. In the critical illness title condition, 15.91% chose target campaigns, while 28.72% did so in the non–critical illness title condition. After controlling for age, gender, and past donation experience, this effect remained significant (Wald χ2(1) = 4.19, p = .041, d = .42; see Web Appendix F for details).
For the detail page condition, we ran a chi-square test to examine the relationship between title type (critical illness title vs. non–critical illness title) and donation rate. The analysis revealed no significant difference in donation rates based on title type (82.72% vs. 74.12%; χ2(1, N = 166) = 1.81, p = .179). A one-way ANOVA with title type (critical illness title vs. non–critical illness title) as the independent variable and amount per donation as the dependent variable also showed no significant effect (Mcritical illness title = .09, SD = .06 vs. Mnon–critical illness title = .08, SD = .06; F(1, 164) = 1.90, p = .170).
Overall, the results from the listing page condition of Study 3 further support the undesirable critical illness title effect (H1). Specifically, participants were less likely to choose critical illness title campaigns when presented with a set of alternatives, allowing them to express empathy while avoiding distress. In contrast, the results from the detail page condition of Study 3 showed that title type did not significantly influence donation behavior. On the detail page, participants saw only a single campaign without alternatives. Since participants could not undo the exposure to distressing information by not donating to the critical illness title campaign, it is possible that their lack of avoidance behavior occurred as a result.
Taken together, Studies 1, 2a, 2b, and 3 provide consistent evidence of the undesirable critical illness title effect on the listing page, supporting H1. While a more thorough comparison between the listing and detail pages is beyond the scope of this article, Study 3 suggests that when distress is unavoidable on the detail page, the negative effect of critical illness titles on donation behavior disappears. This implies that avoidance behavior precipitated by anticipated distress is a possible driver of the undesirable critical illness title effect.
Next, Studies 4 to 6 aimed to explore the role of anticipated distress in driving the undesirable critical illness title effect, using both mediation and moderation approaches.
Study 4
The goal of Study 4 was to examine whether anticipated distress drives the undesirable critical illness title effect (H2). This preregistered study targeted 300 U.S.-based participants on Prolific (https://aspredicted.org/1L2_CCZ). A total of 300 participants completed the survey in exchange for $.18 (£.15). As preregistered, we excluded participants who failed an attention check (N = 26), resulting in a sample of 274 participants (50.37% male, 47.81% female, 1.82% other; Mage = 40 years, SD = 12.28).
Design and Procedure
This study followed a one-factor (title type: critical illness title vs. non–critical illness title) between-subjects design. The design was similar to the listing page condition of Study 3. Participants were randomly assigned to view one of two title type versions. The critical illness title version included two critical illness title campaigns and four control campaigns, and the non–critical illness title version included two non–critical illness title campaigns and four control campaigns. These two critical illness title/non–critical illness title campaigns were the target campaigns. The four control campaigns were the same in both versions. Participants were asked to select one campaign they preferred to learn more about from the list of six. Their choice of target campaign from the list constituted our key dependent variable: campaign choice.
After making their choice, participants were asked to rate their anticipated distress for each of the six campaigns on a seven-point scale (“If you learn more about this fundraising campaign, you may feel:” 1 = “very distressed,” and 7 = “not at all distressed”). For each participant, we calculated a “relative anticipated distress score,” which is the average reverse-coded rating for the two target campaigns minus the average reverse-coded rating for the four control campaigns. A higher score indicated greater anticipated distress for target campaigns relative to control campaigns. Finally, participants’ past donation experience and demographic details, such as age and gender, were collected.
Results and Discussion
A chi-square test revealed a significant difference between title type (critical illness title vs. non–critical illness title) and campaign choice (χ2(1, N = 274) = 4.76, p = .029, d = .27). Specifically, participants in the critical illness title condition were less likely to choose target campaigns (relative to control campaigns) than those in the non–critical illness title condition. In the critical illness title condition, 22.39% chose target campaigns, compared with 34.29% in the non–critical illness title condition.
A one-way ANOVA with title type (critical illness title vs. non–critical illness title) as the independent variable and the relative anticipated distress score as the dependent variable revealed a significant effect (F(1, 272) = 5.52, p = .020, d = .29). Specifically, participants reported higher anticipated distress when exposed to critical illness titles compared with non–critical illness titles (Mcritical illness title = .51, SD = 1.03 vs. Mnon–critical illness title = .23, SD = .93).
To examine the role of anticipated distress in the impact of title type on campaign choice, we conducted a mediation analysis using 5,000 bootstrapped samples (PROCESS Model 4; Hayes 2018). Title type (critical illness title vs. non–critical illness title, with non–critical illness title as the reference group) was the independent variable, anticipated distress was the mediator, and campaign choice (target vs. control, with control campaigns as the reference group) was the dependent variable. The results showed that the effect of title type on campaign choice was mediated by anticipated distress (indirect effect = −.15, SE = .08, 95% CI = [−.349, −.019]; see Web Appendix G). Specifically, critical illness titles (vs. non–critical illness titles) significantly increased participants’ anticipated distress (b = .28, p = .020, d = .28), which subsequently decreased their likelihood of choosing critical illness title campaigns (b = −.55, p = .001, d = .40). As a robustness check, we repeated the mediation analysis with age, gender, and past donation as covariates. The results supported the mediation role of anticipated distress (indirect effect = −.17, SE = .09, 95% CI = [−.379, −.032]; see Web Appendix G).
However, one might argue that the decreased likelihood of choosing target campaigns in the critical illness title (vs. non–critical illness title) condition could stem from perceptions of lower effectiveness (Erlandsson, Björklund, and Bäckström 2015; Exley 2020), familiarity (Smith and Schwarz 2012), trustworthiness (Chapman, Hornsey, and Gillespie 2021), urgency (Vieites, Goldszmidt, and Andrade 2022) or process fluency (Mukhopadhyay and Johar 2007). To address these concerns, we posttested (N = 94) all the critical illness title/non–critical illness title campaigns on these potential alternative explanations, using participants from the same pool. We also posttested two important donation drivers: perceived severity (Fisher and Ma 2014) and empathy (Coke, Batson, and McDavis 1978). Results showed that the critical illness title (vs. non–critical illness title) campaigns were not perceived as having lower effectiveness, familiarity, trustworthiness, urgency, process fluency, severity, or empathy (see Web Appendix G). Thus, the observed undesirable critical illness title effect was unlikely to be driven by these alternative explanations.
Overall, Study 4 again demonstrated the undesirable critical illness title effect and identified anticipated distress as its driver through mediation analysis. The posttest ruled out several alternative explanations, including effectiveness, familiarity, trustworthiness, urgency, process fluency, severity, and empathy, as factors contributing to the effect. In the following studies, we aimed to further validate the anticipated distress account using a moderation approach and explore the boundary conditions of the undesirable critical illness title effect.
Study 5
The goal of Study 5 was to further examine the role of anticipated distress in the critical illness title (vs. non–critical illness title) effect on campaign choice. If anticipated distress indeed drives the effect, a nondistress cue (e.g., informing participants that the detail page information is not distressing) that can turn off anticipated distress should reduce the undesirable critical illness title effect. Specifically, Study 5 tested whether or not a nondistress cue on the listing page could reduce the critical illness title effect (H3). This was a preregistered study with a target sample of 1,000 U.S.-based participants on Prolific (https://aspredicted.org/ss25-q8qn.pdf). A total of 1,002 participants completed the survey in exchange for $.36 (£.30) as payment. As preregistered, we excluded participants who failed an attention check (N = 385), leaving a sample of 617 participants (53.00% male, 45.87% female, 1.13% other; Mage = 40 years, SD = 10.72). Since only 61.58% of participants passed the attention check, we conducted all analyses using both the valid sample (discussed subsequently) and the full sample (see Web Appendix H). All results were essentially the same.
Design and Procedure
This study followed a two-factor (title type: critical illness title vs. non–critical illness title) × (nondistress cue vs. control) between-subjects design. Participants were first asked to imagine browsing an online fundraising platform. As in Studies 3 and 4, they were randomly assigned to one of two title type conditions. In the critical illness title condition, participants chose from a list of six campaigns: two critical illness title target campaigns and four control campaigns. In the non–critical illness title condition, they chose from a list of six campaigns: two non–critical illness title target campaigns and four control campaigns (see Web Appendix H for stimuli). The four control campaigns were the same in both conditions.
We manipulated the nondistress cue and control conditions in a between-subjects manner by assigning participants to two different listing page descriptions. In the nondistress cue condition, participants were told that clicking on a campaign title would direct them to “a detail page that includes drawings and uplifting messages created by K-12 students,” followed by two smiley faces (see Web Appendix H for stimuli). In the control condition, the description was similar to that of Studies 3 and 4, without any nondistress cue. Specifically, participants were told that clicking on a campaign title would direct them to “a detail page that includes images and a full description of the campaign.” A manipulation check study with 99 participants from the same pool confirmed the effectiveness of this manipulation. Participants in the nondistress cue condition rated the potential content as less distressing than those in the control condition (see Web Appendix H). Participants’ choices of target campaigns from the list of six campaigns were our key dependent variable.
To better control for the potential influence of alternative drivers on the key dependent variable, we also collected participants’ ratings of these factors. Specifically, participants were asked to rate their perceived effectiveness, familiarity, trustworthiness, urgency, process fluency, severity, and empathy toward each of the six campaigns on seven-point scales (1 = “not at all,” and 7 = “very much”; see Web Appendix H for descriptive results). Finally, we collected demographic details (age and gender) and participants’ past donation experience.
Results and Discussion
A logistic regression analysis with title type (critical illness title vs. non–critical illness title) and nondistress cue (vs. control) as the independent variables and campaign choice as the dependent variable revealed a significant interaction effect (Wald χ2(1) = 7.83, p = .005, d = .53).
As predicted, for the control condition (similar to Studies 3 and 4), participants in the critical illness title condition were less likely to choose the target campaigns compared with those in the non–critical illness title condition (χ2(1, N = 307) = 4.59, p = .032, d = .25; see Figure 1). Specifically, 27.33% chose target campaigns in the critical illness title condition, while 38.85% chose target campaigns in the non–critical illness title condition. However, for the nondistress cue condition, this effect disappeared (χ2(1, N = 310) = 3.33, p = .068; see Figure 1), with 39.74% choosing target campaigns in the critical illness title condition and 29.87% choosing target campaigns in the non–critical illness title condition. This means that when donors did not anticipate being stressed, there seems to be a tendency toward choosing the critical illness title target campaigns compared with the non–critical illness target campaigns.
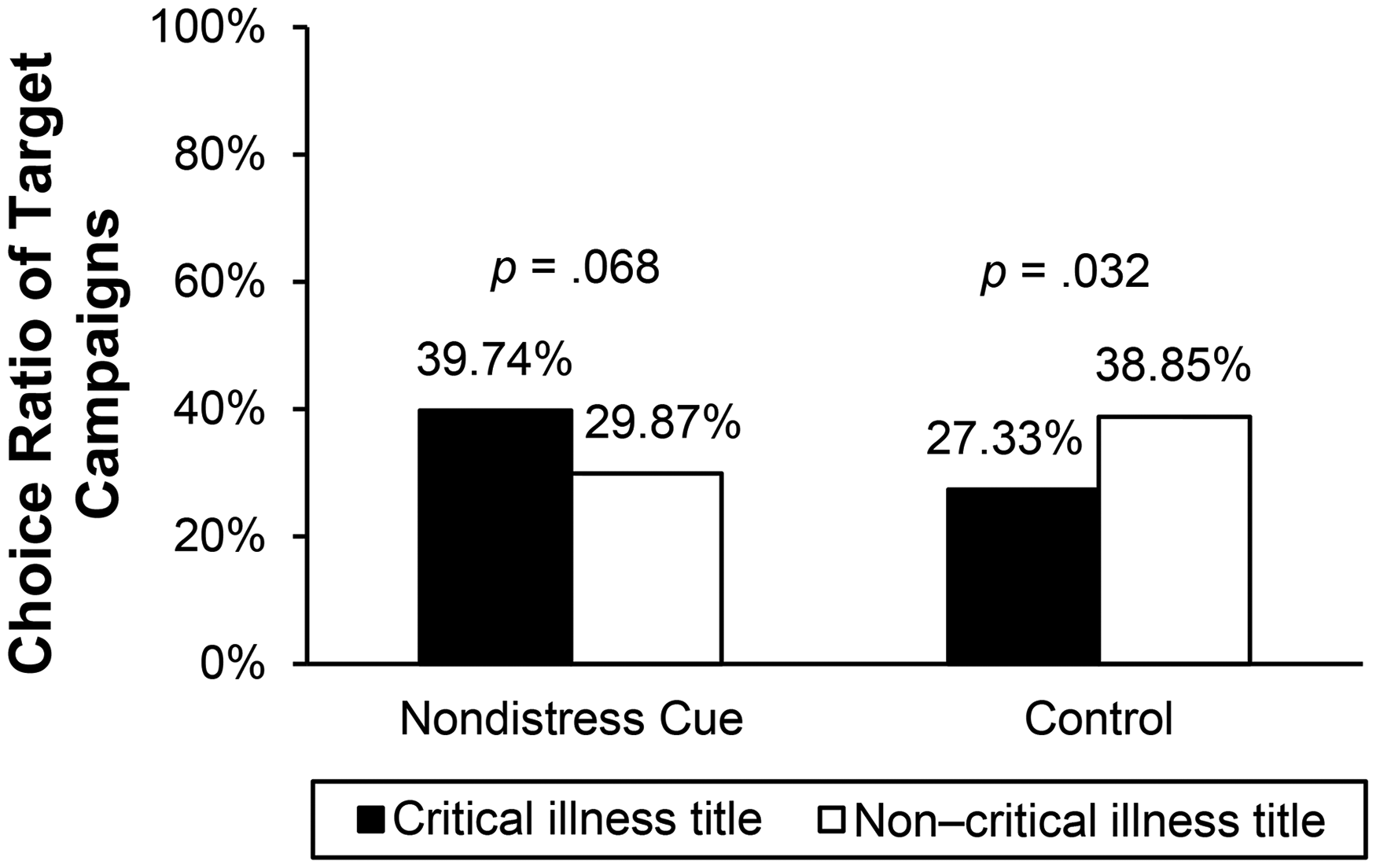
Nondistress Cue Moderates the Undesirable Critical Illness Title Effect (Study 5).
To further examine the role of nondistress cues, two additional contrast analyses were conducted. The results showed that adding a nondistress cue significantly increased the likelihood of choosing the target campaigns in the critical illness title condition (39.74% vs. 27.33%; χ2(1, N = 306) = 5.27, p = .022, d = .26), while the difference in the non–critical illness title condition was insignificant (29.87% vs. 38.85%; χ2(1, N = 311) = 2.78, p = .095). This means that the undesirable critical illness title effect can be reduced by adding a nondistress cue. Additionally, there was a significant main effect of title type (Wald χ2(1) = 4.55, p = .033, d = .29), such that participants in the critical illness title condition were less likely to choose the target campaigns compared with those in the non–critical illness title condition. The main effect of the nondistress cue (vs. control) was not significant (Wald χ2(1) = 2.77, p = .096).
To test the robustness of our proposed effect while ruling out potential alternative drivers, we conducted another logistic regression analysis. The dependent variable was campaign choice. The independent variables were title type (critical illness title vs. non–critical illness title) and nondistress cue (vs. control), with perceived effectiveness, familiarity, process fluency, and empathy included as control variables. 8 Results showed that process fluency and empathy positively influenced campaign choice (process fluency: Wald χ2(1) = 11.52, p < .001, d = .13; empathy: Wald χ2(1) = 6.79, p = .009, d = .11). However, our proposed interaction effect still held (Wald χ2(1) = 8.67, p = .003, d = .58) after controlling for these alternative drivers. As an additional robustness check, we ran another logistic regression analysis with title type (critical illness title vs. non–critical illness title) and nondistress cue (vs. control) as the independent variables, campaign choice as the dependent variable, and age, gender, and past donation experience as control variables. Our proposed interaction effect still held (Wald χ2(1) = 8.61, p = .003, d = .56), although age had a positive effect on campaign choice (Wald χ2(1) = 4.76, p = .029, d = .01).
To replicate the undesirable critical illness title effect found in Studies 1‒4, we conducted another logistic regression analysis using data from only the control condition. The results showed that participants in the critical illness title condition were less likely to choose target campaigns than those in the non–critical illness title condition (Wald χ2(1) = 4.55, p = .033, d = .29), replicating the undesirable critical illness title effect found in previous studies. Furthermore, this effect persisted after controlling for alternative drivers (Wald χ2(1) = 6.88, p = .009, d = .38) and after controlling for age, gender, and past donation experience (Wald χ2(1) = 4.62, p = .032, d = .30).
Overall, through a moderation approach that directly manipulated the mediator, Study 5 showed that once anticipated distress was turned off by a nondistress cue, the undesirable critical illness title effect disappeared. This finding supports H3 and provides further evidence for the anticipated distress account (H2). In addition to directly manipulating the mediator to turn off anticipated distress, another way to reduce the undesirable critical illness title effect is to turn off the opportunity to avoid distress. Study 6 was designed to test the role of justifiable alternatives (i.e., alternatives that allow participants to avoid distress while still expressing empathy) in the impact of critical illness title (vs. non–critical illness title) on campaign choice.
Study 6
We posit that the undesirable critical illness title effect is more likely to occur on the listing page of fundraising platforms, where donors have many alternatives to avoid distress while still expressing empathy. Based on this reasoning, we propose that the effect is stronger when these alternatives are justifiable—providing donors with a valid avenue to avoid distress while expressing their empathy—compared with when alternatives are nonjustifiable (H4). Study 6 was designed to test this moderation effect. This was a preregistered study with a target sample of 800 U.S.-based participants on Prolific (https://aspredicted.org/79H_7RF). A total of 850 participants completed our survey in exchange for $.18 (£.15) as payment. As preregistered, we excluded participants who failed an attention check (N = 34), resulting in a sample of 816 participants (49.76% male, 48.77% female, 1.47% other; Mage = 37 years, SD = 11.61).
Design and Procedure
This study followed a two-factor (title type: critical illness title vs. non–critical illness title) × (alternatives: justifiable vs. nonjustifiable) between-subjects design. Similar to Studies 3 and 4, participants were randomly assigned to one of two title type conditions (critical illness title vs. non–critical illness title). They then received a list of six campaigns, with two target campaigns (either critical illness title or non–critical illness title) and four control campaigns that were identical in both conditions.
In a between-subjects manner, we manipulated the four control campaigns as either justifiable or nonjustifiable alternatives. In the justifiable condition, we adopted a design similar to that in Studies 3 and 4. In the nonjustifiable condition, we added progress bars 9 to all campaigns. The two target campaigns were shown as reaching 62% and 63%, respectively. The four control campaigns were shown to have reached 100%, indicating full funding (see Web Appendix I for the stimuli). This manipulation assumed that fully funded alternatives were more likely to be perceived as nonjustifiable because they no longer appear to need help. Choosing such alternatives deviates from the common goal of donating to help someone in need. This aligns with prior research suggesting that decision-makers view options deviating from, rather than aligning with, task goals as less justifiable (Hsee 1995). A manipulation check study with 196 participants from the same pool confirmed the effectiveness of this manipulation. Participants in the nonjustifiable condition perceived the control campaigns as less in need of help compared with those in the justifiable condition (see Web Appendix I for details).
Participants’ choice of target campaigns from the list of six constituted our key dependent variable. Finally, participants’ past donation experience and demographic details (age and gender) were collected.
Results and Discussion
A logistic regression analysis with title type (critical illness title vs. non–critical illness title) and alternatives (justifiable vs. nonjustifiable) as the independent variables and campaign choice as the dependent variable revealed a significant interaction effect (Wald χ2(1) = 4.90, p = .027, d = .35).
As predicted, when alternatives were justifiable, participants in the critical illness title condition were less likely to choose the target campaigns than those in the non–critical illness title condition (χ2(1, N = 409) = 4.25, p = .039, d = .20; see Figure 2). Specifically, 32.04% chose target campaigns in the critical illness title condition, while 41.87% chose target campaigns in the non–critical illness title condition. However, when alternatives were nonjustifiable, this effect disappeared (χ2(1, N = 407) = 1.13, p = .288; see Figure 2), with 60.59% choosing target campaigns in the critical illness title condition and 55.39% choosing target campaigns in the non–critical illness title condition. After controlling for age, gender, and past donation experience, this interaction effect remained significant (Wald χ2(1) = 5.12, p = .024, d = .36; see Web Appendix I for details).
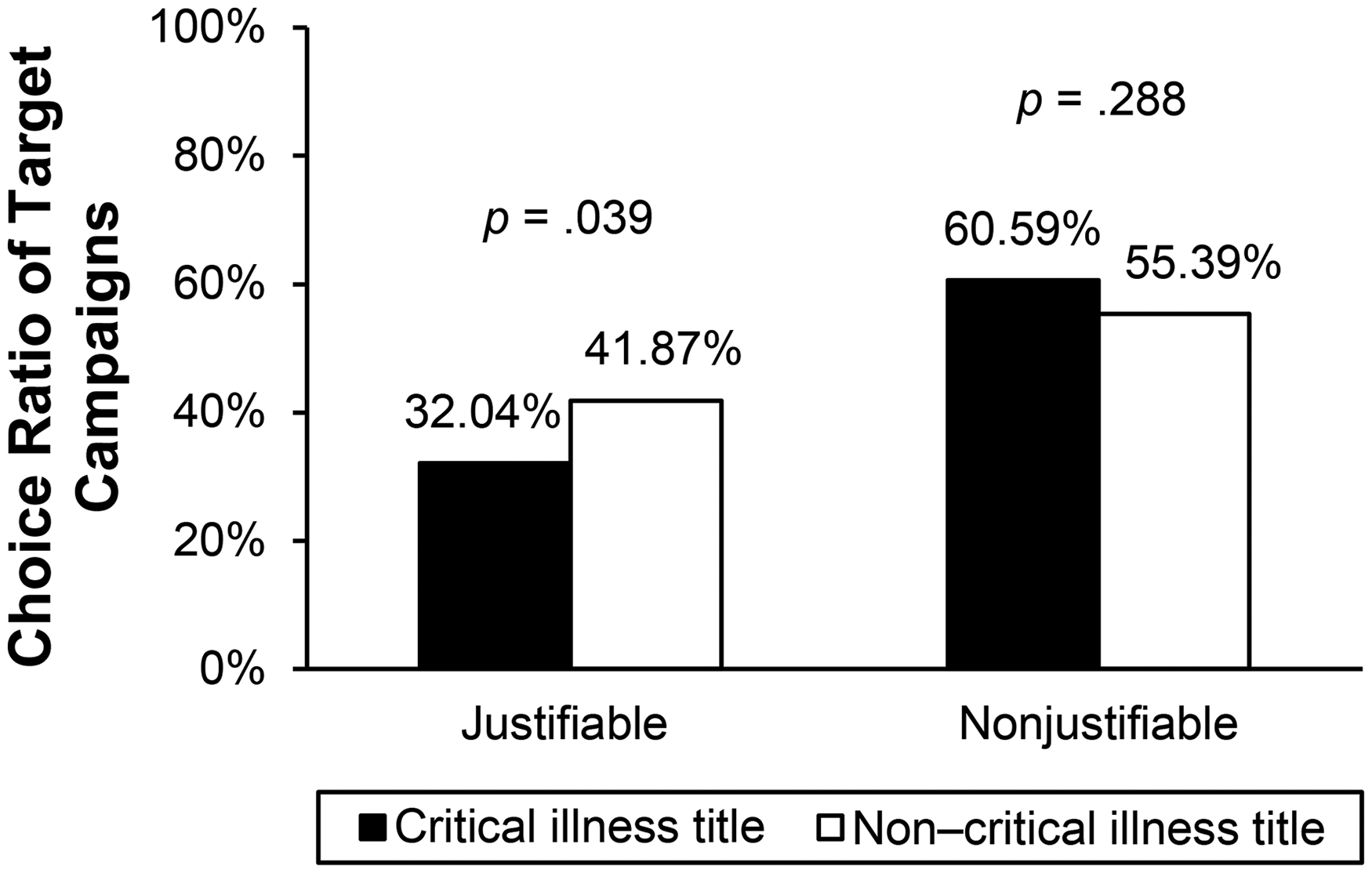
Justifiable Versus Nonjustifiable Alternatives Moderate the Undesirable Critical Illness Title Effect (Study 6).
To further examine the role of justifiable/nonjustifiable alternatives, two additional contrast analyses were conducted. The results showed that nonjustifiable (vs. justifiable) alternatives significantly increased the likelihood of choosing the target campaigns in both the critical illness title condition (60.59% vs. 32.04%; χ2(1, N = 409) = 33.53, p < .001, d = .60) and the non–critical illness title condition (55.39% vs. 41.87%; χ2(1, N = 407) = 7.45, p = .006, d = .27). The former was stronger than the latter. This means that the undesirable critical illness title effect can be reduced when the alternatives are nonjustifiable. Additionally, there was a significant main effect of justifiable alternatives (Wald χ2(1) = 7.40, p = .007, d = .30), such that participants were more likely to choose justifiable alternatives than nonjustifiable alternatives. The main effect of title type was not significant (Wald χ2(1) = 1.13, p = .288).
These findings support our theory that the undesirable critical illness title effect arises when many justifiable alternatives exist alongside critical illness title campaigns, enabling donors to avoid distress while still expressing empathy. The listing pages of fundraising platforms typically display numerous similar campaigns together, offering donors many opportunities to choose a justifiable alternative to avoid distress. We argue that this context increases the likelihood of the undesirable critical illness title effect.
Taken together, Studies 4, 5, and 6 provide both mediation and moderation evidence that anticipated distress drives the undesirable critical illness title effect. Introducing a nondistress cue reduces anticipated distress, which in turn mitigates the negative impact of critical illness titles (vs. non–critical illness titles) on campaign choice. Displaying nonjustifiable alternatives alongside critical illness title campaigns limits opportunities to avoid distress while still expressing empathy, further reducing the undesirable critical illness title effect. These findings not only identify boundary conditions for the undesirable critical illness title effect but also offer practical insights into how to reduce this effect on charitable fundraising platforms.
General Discussion
Across seven studies using multiple methods (secondary data modeling, field experiments, and controlled experiments), we found consistent evidence supporting our proposition that critical illness titles, as an emotion-laden driver, can harm donation performance in online charitable fundraising. Study 1 showed that critical illness title campaigns were associated with fewer donations after controlling for various factors, marking the first demonstration of the undesirable critical illness title effect using a large sample of real-world campaigns from Tencent Charity. Studies 2a and 2b, two randomized field experiments conducted on Tencent Charity and Facebook, demonstrated that critical illness titles (vs. non–critical illness titles) resulted in lower CTRs on both the fundraising and social media platforms. Using a controlled experiment, Study 3 identified that the undesirable critical illness title effect occurred on the listing page (rather than the detail page), where numerous alternatives were available for donors to avoid distress while still expressing empathy. Together, Studies 1, 2a, 2b, and 3 provided robust evidence for H1. Study 4 directly tested the anticipated distress account through a mediation approach. Study 5 directly manipulated the anticipated distress by adding a nondistress cue. The results showed that adding a nondistress cue can turn off the undesirable critical illness title effect, offering a boundary condition for this effect. Study 6 identified another boundary condition: When alternatives are nonjustifiable, the undesirable critical illness title effect disappeared.
Theoretical Contributions
This work makes several important theoretical contributions. First, it expands the literature on title effects in online contexts (Hagar, Diakopoulos, and DeWilde 2022; Knobloch-Westerwick et al. 2005). While extensive research has examined the impact of titles in online settings, few studies have explored their role in online charitable fundraising. Given the growing digitalization of the charity industry and its societal impact, this research highlights an important consideration in marketing practice for NPOs and individuals: how titles influence donations. Specifically, we focus on a significant domain: fundraising for critical illness campaigns. Our findings suggest that including the names of critical illnesses in titles imposes a psychological cost on potential donors, such as anticipated distress. As a result, critical illness title campaigns experience lower click performance on online fundraising platforms.
Future research could investigate title effects in other donation contexts, such as comparing titles that mention an illness versus those that do not, even when the illness is not critical. We speculate that anticipated distress may play a smaller role in such cases as noncritical illnesses are perceived as less distressing. Additionally, future studies could explore title effects in other domains, such as education or environmental protection. Since these domains are inherently less distressing than medical fundraising, anticipated distress might function differently. In some cases, it could even enhance engagement as a moderate level of anticipated distress may be necessary to motivate long-term support for causes like education or environmental protection. Furthermore, this research only focuses on the effect of titles on clicks/choices on the listing page. Future studies could explore the interaction between title and information on the detail page, for example, whether they should be consistent or complementary.
Furthermore, this research contributes to the donation literature by identifying unique characteristics of donation behavior on online platforms compared with traditional channels. We propose that fundraising campaign titles play a crucial role in influencing donation performance in online settings. Our findings show that online charitable platforms, which display numerous campaigns simultaneously, provide donors with ample opportunities to avoid distress-inducing campaigns by selecting alternative ones. Prior donation research has primarily focused on traditional formats, where donors encounter individual donation appeals in isolated contexts. However, as charitable organizations increasingly shift to online fundraising (Liu, Gao, and Rao 2025), there is limited research on the factors that influence donations in these digital environments. A few articles on online fundraising have emerged in the past few years (Liu, Gao, and Rao 2025; Sepehri et al. 2021; Su et al. 2024); however, they mostly focus on the cognitive drivers of donation on fundraising platforms. Our research complements this literature by identifying an emotion-laden driver of online donation (i.e., critical illness title). Future research could explore more cognitive and emotional drivers on online fundraising platforms, especially those that are distinct from traditional channels. Moreover, this research contributes to the donation literature by identifying anticipated distress as a significant predictor of charitable behavior in online fundraising. While prior studies suggest that experienced personal distress can motivate donors to either alleviate their discomfort (e.g., Batson, Fultz, and Schoenrade 1987; Klimecki and Singer 2012) or escape the distressing situation (e.g., Batson et al. 1981), our findings show that anticipated distress can also shape donors’ behavior by prompting them to seek alternative campaigns. Unlike previous research demonstrating that negative emotions increase helping behavior in isolated donation appeals (Bagozzi and Moore 1994; Fisher, Vandenbosch, and Antia 2008; Xu, Kwan, and Zhou 2020), our findings reveal that anticipated distress may reduce donations when numerous other campaigns allow donors to express empathy without experiencing distress.
One may wonder why critical illness titles (vs. non–critical illness titles) elicit greater anticipated distress. As discussed in the theoretical section, this is likely due to the inherently greater severity of critical illnesses (as evidenced by the posttest in Study 4); personal distress is intensified when individuals learn about others in such severe conditions. Additionally, we argue that critical illness terms such as “cancer,” “leukemia,” and “malignant tumor” are more concrete than non–critical illness terms like “condition,” “illness,” and “disease.” Concrete words evoke more vivid and specific thoughts, which in turn heighten anticipated distress. We conducted three exploratory studies to examine this explanation (see Web Appendix J for details). The first one (N = 144) examined participants’ free association with critical illness words and non–critical illness words from Studies 3 to 6. Participants were asked to write down the first three words that came to mind for each critical illness word (e.g., “cancer,” “malignant tumor”) and non–critical illness word (e.g., “condition,” “illness”). Results showed that the most commonly associated words for critical illness terms were “cancer” (154 occurrences), “death” (153 occurrences), and “sick” (83 occurrences). In contrast, the top associations for non–critical illness words were “sick” (112 occurrences), “sickness” (69 occurrences), and “illness” (60 occurrences; see Web Appendix J for the top ten associated words and their frequencies).
Two follow-up exploratory studies (N = 98 and N = 92, respectively) showed that critical illness words and their associated words were rated as more concrete, vivid, negative, and distressing than non–critical illness words and their associated words (see Web Appendix J for details). These findings offered evidence for why critical illness titles (vs. non–critical illness titles) can elicit greater anticipated distress. This result aligns with the linguistic distancing effect found in past research, which shows that concrete words (vs. abstract words) evoke stronger negative emotions (Kross et al. 2014; Nook, Schleider, and Somerville 2017; Orvell et al. 2019). Future research could further explore the link between critical illness words (vs. non–critical illness words) and anticipated distress. Although this is not the primary focus of the present research, we believe that the impact of emotion-laden words such as critical illness words on emotions and emotion regulation is an interesting topic to explore.
Managerial Implications
This work has important managerial implications. As the charity industry shifts from offline to online appeals, marketing strategies must be reevaluated. The design of fundraising campaign titles is crucial to success as titles play a key role in attracting donations in a highly competitive online environment. Given this, our findings provide valuable insights and practical recommendations.
First, while the importance of titles is widely recognized in the online charity industry, our findings—based on multiple studies using diverse methods and datasets across different countries—validate this business intuition: Titles matter. Our results suggest that title design is strongly linked to the success of fundraising campaigns, reinforcing the need for NPOs and individuals to carefully consider titles when launching campaigns on online platforms.
In addition, our research uncovers an important—and perhaps counterintuitive—finding. In medical fundraising, practitioners often prefer to include the names of critical illnesses in campaign titles, believing this strategy signals the severity of the recipient's need and increases donations (as shown in the prestudies in Web Appendix B). However, our findings challenge this assumption by revealing another key factor: Critical illness titles heighten anticipated distress, prompting potential donors to avoid them. As a result, critical illness titles (vs. non–critical illness titles) may lead to fewer clicks/choices on the listing page, especially when donors have many justifiable alternatives to choose from.
More importantly, our finding that the undesirable critical illness title effect disappears when there is a nondistress cue or when nonjustifiable alternatives exist offers practical insights into mitigating this effect on online charitable fundraising platforms. Specifically, if NPOs choose to include critical illness names in their fundraising titles, they might consider doing so on the detail page, where no justifiable alternatives are displayed. Alternatively, they could incorporate a nondistress cue—such as in a textual description (as in Study 5) or possibly through music, color, or imagery—to reduce anticipated distress. This finding also has implications for platform design. Online fundraising platforms should be mindful of the potential downside of listing critical illness title and non–critical illness title campaigns side by side within the same category. Such placements could reduce donations to critical illness title campaigns, which often require urgent support.
Supplemental Material
sj-pdf-1-jmx-10.1177_00222429251365531 - Supplemental material for Too Painful to Donate: Why Don’t People Donate to Critical Illness Campaigns?
Supplemental material, sj-pdf-1-jmx-10.1177_00222429251365531 for Too Painful to Donate: Why Don’t People Donate to Critical Illness Campaigns? by Jingjing Ma, Yuanjie Zhao and Yitian (Sky) Liang in Journal of Marketing
Footnotes
Acknowledgments
The authors thank Tencent Charity for helping conduct the field study on their platform; Qin Liu, Sean Zhang, Fan Zhang, and Renyu Zhao for administrating the field study at Tencent; Yutian Yue for designing the stimuli; and Hengjing Liu and Leiming Ding for providing group-level data.
Author Contributions
The first two authors contributed equally to this work.
Coeditor
Cait Lamberton
Associate Editor
Amitava Chattopadhyay
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study was approved by the Peking University IRB (approval no. IRB00001052-22154) on December 29, 2022. All participants provided written informed consent prior to participating.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (72222006; 72532007), the Bill & Melinda Gates Foundation (INV-075713; INV-004139; OPP1183979), and the Tencent Foundation (QT21006-3-9; TF-20220506-00007-0003).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.