
Abstract
This research introduces a novel conceptualization of immersive service, defined as service that consumers are embedded in and surrounded by, such that their life experience is within the service and, in great part, constructed by it for some period of time (e.g., hospital stays, residential care, air travel). The authors examine two key questions: (1) How can characteristics of immersive service challenge consumer agency? (2) How do consumers bolster their agency in immersive service? They study these questions through a novel theoretical lens (figured worlds theory) and based on an ethnography in a residential care facility. The analyses unearth, define, and describe four conceptually novel characteristics of immersive service: encapsulation, positionality, multivocality and protocolization. These characteristics are crucial for marketers because, as the authors find, these structural aspects of immersive service can threaten consumer agency. The research also shows how consumers overcome challenges to agency. Specifically, consumers pursue five pathways toward their individual and collective agency: expanding the figured world, voicing, seeking task responsibility, challenging figured world protocols, and playing and imagining within the figured world. These findings break new conceptual ground for scholars while also being relevant for managers, consistent with ideals of Better Marketing for a Better World and transformative service research.
Keywords
Nancy (93 years old), a resident in a residential care facility, enjoys using her agency as an acknowledged spokesperson for herself and others by voicing their opinions and stances to the service staff and service organization. However, she also describes how a resident's agency becomes threatened in this service environment where she lives: “I overheard in the corridor, a caregiver saying, ‘She [Nancy] is not the one who decides; we [staff] are the ones that decide!’”
This research, guided by the ideals of Better Marketing for a Better World 1 (BMBW; Chandy et al. 2021) and the well-being emphasis of transformative service research (e.g., Anderson et al. 2013), proposes a novel lens into consumer experiences of immersive service. We define immersive service as a service that consumers are embedded in and surrounded by, such that their life experience is within the service and, in great part, constructed by it for some period of time. Although the notion of immersion is not new in marketing (e.g., Stuart and Tax 2004), it often has been associated with extreme, voluntary, or hedonic experiences in leisure (Carù and Cova 2006), tourism (Lunardo and Ponsignon 2020), or technology (e.g., virtual reality; Jennett et al. 2008) contexts. In such work, immersion has been envisioned as a way for consumers to “escape into experiential contexts that are simultaneously enclavised and secure” (Cova, Carù, and Cayla 2018, p. 449). The previous work on immersion is insightful, but its emphasis on extraordinary experiences (Becker and Jaakkola 2020; Carù and Cova 2003) overlooks more mundane experiences. We adopt a conceptually distinct and broader view as we propose that consumers frequently experience immersive service in health care (e.g., hospital stays, residential care), education (e.g., school/university attendance), or hospitality (e.g., air travel, resorts), among others, where consumers are embedded in and surrounded by the service environment, often for considerable lengths of time and as part of their everyday experience. Such immersive services are provided to millions of consumers daily and are of major economic importance. Deepening marketing understanding of how consumers experience immersive service, our analyses unearth, define, and describe four conceptually novel and managerially relevant characteristics that reflect the structures and processes of immersive service: encapsulation, positionality, multivocality, and protocolization (defined subsequently). Identifying these characteristics is crucial for marketers because these structural aspects of immersive service can threaten consumer agency. 2 In our research, we adopt Baker's (2005, p. 448) definition of agency as “the capacity of individuals to act independently and to make their own free choices,” and we are concerned with both individual and collective agency. Agency is linked to well-being and, thus, important for all consumers (Lamberton, Saldanha, and Wein 2024), but it is key in immersive services (e.g., health care), where consumers’ life experience resides within what is often a highly structured service that may limit agency and conflict with consumers’ desire to control their lives. Thus, we focus on two main questions: (1) How can characteristics of immersive service challenge consumer agency? (2) How do consumers bolster their agency in immersive service?
We examined these questions via an ethnographic study of a residential gerontological care facility. In doing so, we drew on a theoretical lens that is new to marketing: figured worlds theory (FWT; Holland et al. 1998). A figured world is a social and cultural landscape that supplies the context of meanings, activities, and structures of positions, privilege, and influence. In light of this landscape, people need to figure out how to be and how to act given the structure and power configurations within a figured world. Figured worlds are therefore crossroads of structure and agency, as they provide the context for people figuring out how “to direct their own behavior in these worlds” (Holland et al. 1998, p. 60). As part of this figuring out, FWT points to the concept of improvisation, which describes a person using their resources to creatively change certain facets of the figured world and to find a space for themself within it (O’Neill 2011; Rush and Fecho 2008). Conceptualizing immersive services as figured worlds, we draw on FWT as an enabling theory as we study the interplay of immersive service and consumer agency.
Our work makes multiple contributions to the marketing literature. First, we introduce a conceptualization of immersive service via four characteristics: encapsulation, positionality, multivocality, and protocolization. This conceptual contribution aligns with what MacInnis (2011, p. 138) described as “discovery by identifying something new,” and enables scholars and managers to become aware of these characteristics, which transfer across various service realms. This discovery expands marketing theory and offers actionable implications for organizations to improve the service experiences of their customers.
Second, with FWT facilitating our exploration, we uncover how the four characteristics of immersive service can affect consumer agency. While it is well-established that agency is related to well-being (e.g., Berry, Yadav, and Hole 2024), little research has delved deeper to identify underpinnings that challenge agency. Such challenges are crucial to understand for managers, because they affect how consumers experience services.
Third, we show how consumers overcome challenges to their agency. Specifically, we discovered that consumers pursued five distinct pathways toward their individual and collective agency: expanding the figured world, voicing, seeking task responsibility, challenging figured world protocols, and playing and imagining within the figured world. Building on FWT, these pathways reflect consumer improvisation within their figured world. Notably, we extend prior research on collective agency by introducing the distinction between pathways to horizontal collective agency (the consumer initiates a pathway in collaboration with other consumers) or vertical collective agency (the consumer initiates a pathway in collaboration with the organization).
Fourth, our context (residential senior care) also contributes to marketing, as it helps reduce the dearth of marketing research that directly captures the voice of seniors (rather than relying on family to speak for them; Gentry, Phillips, and Barnhart 2014). Such approaches, which rely on others rather than the seniors themselves, risk dismissing the lived experiences of seniors and can create serious voids in marketing understanding of senior consumers and their well-being. Focusing on older adults, as advocated by MacInnis et al. (2020) for boundary-breaking marketing research, our ethnographic work draws directly on the lived experiences of seniors in residential care (average age of 92 years); thus, it offers a more accurate perspective of the oldest-old, which remains rare in marketing and other fields (Grossmann et al. 2010; Lund and Wang 2020).
Together, the discovery of these characteristics of immersive service breaks new conceptual ground for marketing scholars (Kindermann et al. 2024; MacInnis 2011), while also being relevant for managers, consistent with ideals of BMBW and transformative service research. Next, we draw on extant research on immersive consumption and consumer agency for key insights that assist our conceptual development of immersive services as figured worlds.
Theoretical Development: Toward a Conceptualization of Immersive Service
Key Insights from Research on Immersive Consumption
A dedicated literature stream has provided valuable insights on customer experiences (e.g., Gahler, Klein, and Paul 2023; Lemon and Verhoef 2016; Siebert et al. 2020) and explored various facets of immersion and consumption (see Table 1). This prior research assumes that immersion is beneficial to the experience and that consumers can immerse into moments of enchanted, multifaceted, and spectacular encounters (Firat and Dholakia 1998), or “moments of intensity that a consumer lives through” (Carù and Cova 2006, p. 10). Immersion is thereby voluntary and positively related to satisfaction (Hudson et al. 2019). The idea of consumers’ being physically and/or mentally immersed (Carù and Cova 2003; Suh and Prophet 2018) is pervasive in this literature. Surroundings encouraging immersion vary from themed, firm-created environments (Lunardo and Ponsignon 2020; Pine and Gilmore 1998) to natural, difficult-to-access environments (Blumenthal and Jensen 2019; Hansen and Mossberg 2013). In many cases, immersion is treated as an extreme state where consumers lose track of time and place, offering an escape from everyday life into another world (Cova, Carù, and Cayla 2018). Some authors also posit that immersion is the final stage of a deepening of consumer focus (Jennett et al. 2008) that tends to be momentary (Carù and Cova 2006) or a limited time frame (e.g., gaming; Jennett et al. 2008); others (Hansen and Mossberg 2013, p. 223) argue that immersion “creates a bounded, thematized and manageable liminal world that contrasts with the consumer's everyday life.”
Illustrative Key Insights from Research on Immersive Consumption.
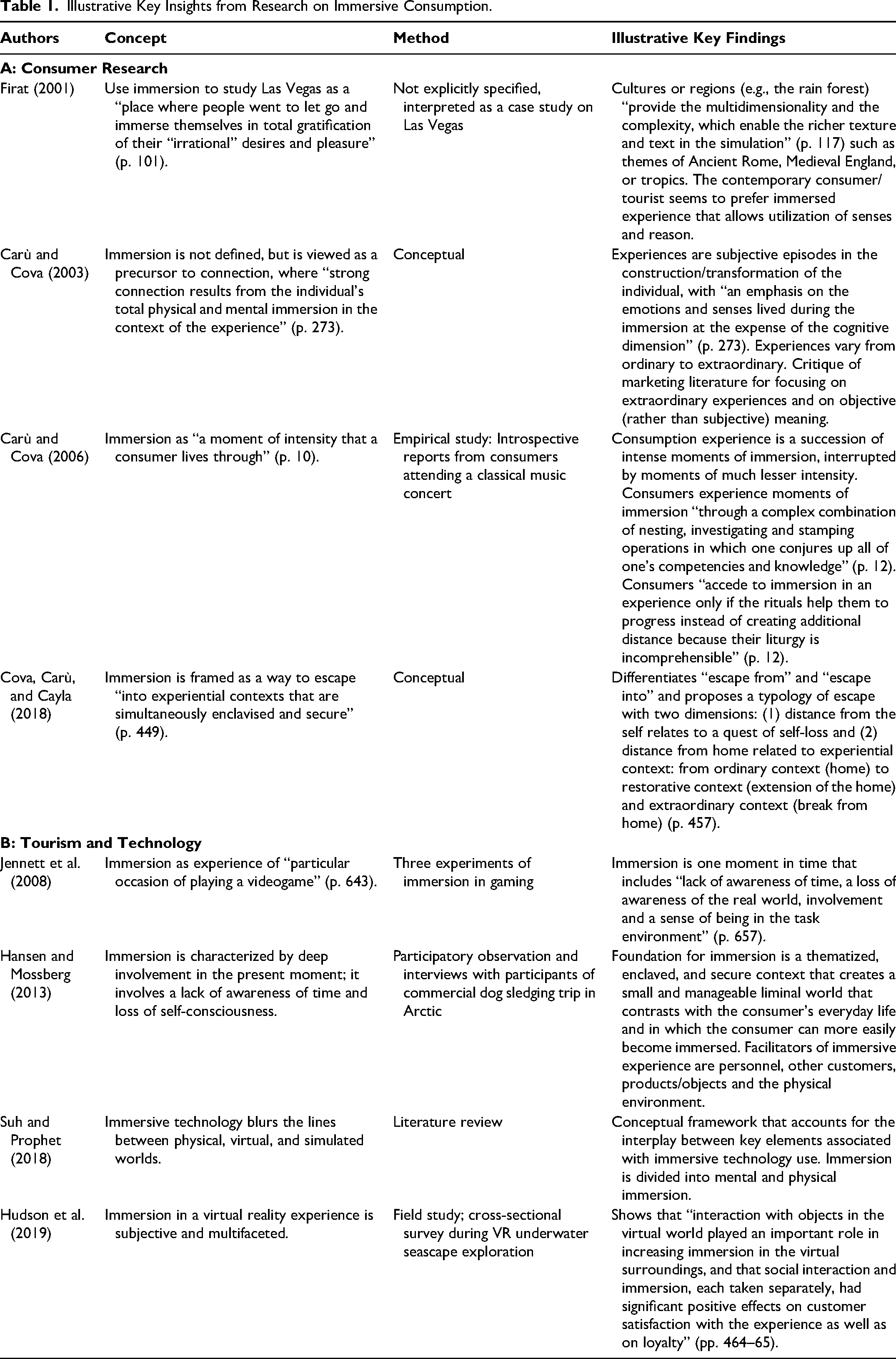
As Table 1 illustrates, prior research offers valuable insights into consumer immersion, often linked to consumer satisfaction and benefits for firms. This literature typically adopts a focus on consumers’ voluntary, hedonic, and extreme experiences that are often detached from their everyday life. Yet, this literature pays little attention to immersion as a characteristic of service experiences where a consumer's more mundane life and the service coalesce. Most relevant for our research, this focus on services that consumers voluntarily seek out for a limited period (at times even with the desire to abdicate their agency) neglects involuntary, utilitarian, and long-term/open-ended experiences where agency is desired and sought.
Key Insights from Research on Consumer Agency
Research on agency is associated with general measures of human well-being (Pepe et al. 2024) and specific aspects such as dignity (Lamberton, Saldanha, and Wein 2024), life satisfaction (Welzel and Inglehart 2010), and eudaimonic well-being (i.e., finding meaning and purpose; Alkire 2008). The conceptual logic for these associations is that the freedom to decide how to live one's life increases well-being (Hojman and Miranda 2018).
Our review of research on agency and well-being suggests that there are two major foci: one on developing a person's capability to be agentic (e.g., Martinez-Mendia et al. 2024; Renes and Aarts 2018; Welzel and Inglehart 2010) and another on the structural and power opportunities for and constraints on agency (e.g., Mele and Russo-Spena 2024; Moilanen et al. 2021; Narayan and Petesch 2007). Although both foci emphasize important aspects of agency, consistent with our interest in the structural characteristics and processes of immersive service as related to consumer agency, we draw more so on the second focus as we examine how individuals figure out how to exercise their agency given the structure of an immersive service. With that, we note that agency is often discussed in contrast to structure, which refers to “the recurrent patterned arrangements which influence or limit the choices and opportunities available” (Baker 2005, p. 448). Indeed, Kotan (2010) observes that well-being is affected when the exertion of agency is hindered by structural elements. The notion of structures is critical because immersive services typically have many structural features that can interfere with consumer agency; this led us to FWT (Holland et al. 1998), which studies the crossroads of agency and structure.
Figured World as Enabling Theory
FWT expands on the idea of cultural worlds as sociocultural contexts where aspects such as values, beliefs, norms, positional power, and protocols provide structure for the world. In light of the structure of this world, individuals can use their agency to figure out how they are expected to act and, subsequently, how they will act within these worlds (Holland et al. 1998; Urrieta 2007). In this process of figuring out, agency and structure intersect. As Holland et al. (1998, p. 60) state, “Figured worlds in their conceptual dimension supply the context of meaning for actions, cultural productions, performances, disputes, for the understandings that people come to make of themselves, and for the capabilities that people develop to direct their own behavior in these worlds.” Figuring out is work, often contentious work, that is compounded by multiple discourses and voices rather than one clear narrative within the figured world; furthermore, the process of figuring out is mediated by positions of power within the figured world (Urrieta 2007). Accordingly, and parallel to our research, FWT asks questions such as “How might figured worlds challenge human agency?” and “How do people become agents in these worlds?” (Holland et al. 1998, p. 8). In examining such questions, FWT underscores the importance of human agency as it views figured worlds as “sites of possibility” in which individuals can engage in improvisation as part of the figuring-out process (Holland et al. 1998). Importantly, the term “improvisation” is not used in its usual sense here; instead, in FWT improvisation refers to “behaviors that work outside the lines drawn by the cultural expectations [structure and power position] of the figured world … [such that improvisation] is finding a space for one's self within a larger social construct” (Rush and Fecho 2008, pp. 124–26). Relatedly, O’Neill (2011) describes improvisation as a person's agentic work of using their resources to creatively change a norm or process of the figured world. Through improvisation, individuals interpret, orchestrate, and even challenge expectations or narratives to figure out how to act in and change their figured world (Holland et al. 1998). In short, improvisation emphasizes that people are not passive recipients, but active participants within figured worlds. The concepts of “figuring out” and “improvisation” reflect the idea of agency that we are concerned about within an immersive service with its structure and power configurations. Drawing on FWT, we consider immersive services as figured service worlds.
Methodology
Research Context: Residential Care as an Immersive Service and Figured Service World
With increases in longevity, people over the age of 90 are now the fastest-growing segment of the population in most of the world (Kawas, Legdeur, and Corrada 2021), and “two out of three older people are likely to need [long-term] care and support” (World Health Organization 2022). Thus, the demand for long-term care services, especially residential care facilities, will increase, and the global market for long-term care is anticipated to reach over 1.92 trillion USD by 2032 (Precedent Research 2023).
A rich literature in gerontology has examined a plethora of issues related to residential care (see Web Appendix A). Notably, scholars in gerontology identify two important voids in their literature that marketing can help address: (1) the need for a more customer-centric lens in geriatric care and (2) the importance of examining aspects related to consumer agency in geriatric residential care. Addressing these voids is also central to our research. Regarding the first void, research on residential care has aimed to broaden its perspective from a medical to a social one (Armstrong 2018). According to this social perspective, research needs to focus more on the older persons’ lived experiences in residential care (Van Loon et al. 2021; Van Steenwinkel, De Casterlé, and Heylighen 2017). This social perspective emerged from calls in health care for more comprehensive and nuanced investigations of the patient experience (beyond surveys; e.g., Hefner et al. 2019; Kuppelwieser and Klaus 2020). For example, in their forecast of how health care will have to change in light of future societal needs, Wolf (2019, p. 3) underscores that the “focus on human experience will root itself at healthcare's core.” Regarding the second void, scholars in gerontology are calling for more research on how older people's autonomy and agency in residential care are affected by their environment, their social life, as well as service organizations and their practices, norms, policies, and rules (Bradshaw et al. 2023; Knight, Haslam, and Haslam 2010; Moilanen et al. 2021). This concern for the consumer experience and agency, along with the highly immersive conditions of residential care, provide an excellent context for our conceptualization of immersive service.
An Ethnographic Field Study in a Residential Care Setting
We draw on an ethnographic field study in a residential care setting to conceptualize immersive service and to examine how agency is pursued and exercised in response to immersive services. This care home provides 24-hour support by care professionals and assistance in activities of daily living (e.g., getting in and out of bed, eating, bathing). It also offers organized programs of activities, rehabilitation, and basic medical services. In its marketing communication, the care home describes its services as follows: We provide a homelike, inviting, and harmonious environment where older adults can enjoy life both physically and mentally. The tranquil surroundings are beneficial for well-being, and the body thrives on physical activities and good food, while the mind is stimulated by diverse and entertaining programs. The care home is known for offering its residents a life with added value.
Located in Northern Europe, at the time of the study, 50 seniors (average age of 92 years old) were living in the facility. Due to their longer life expectancy, most of the residents were women (95%). The high average age is due to a recent national policy that advocates aging in place (i.e., living at one's own home) as long as possible. Some of these older adults moved to the care home because they preferred to do so, while others moved because they felt they had to. Most residents stayed for a long and indefinite time, most often to the end of their lives.
Data Collection
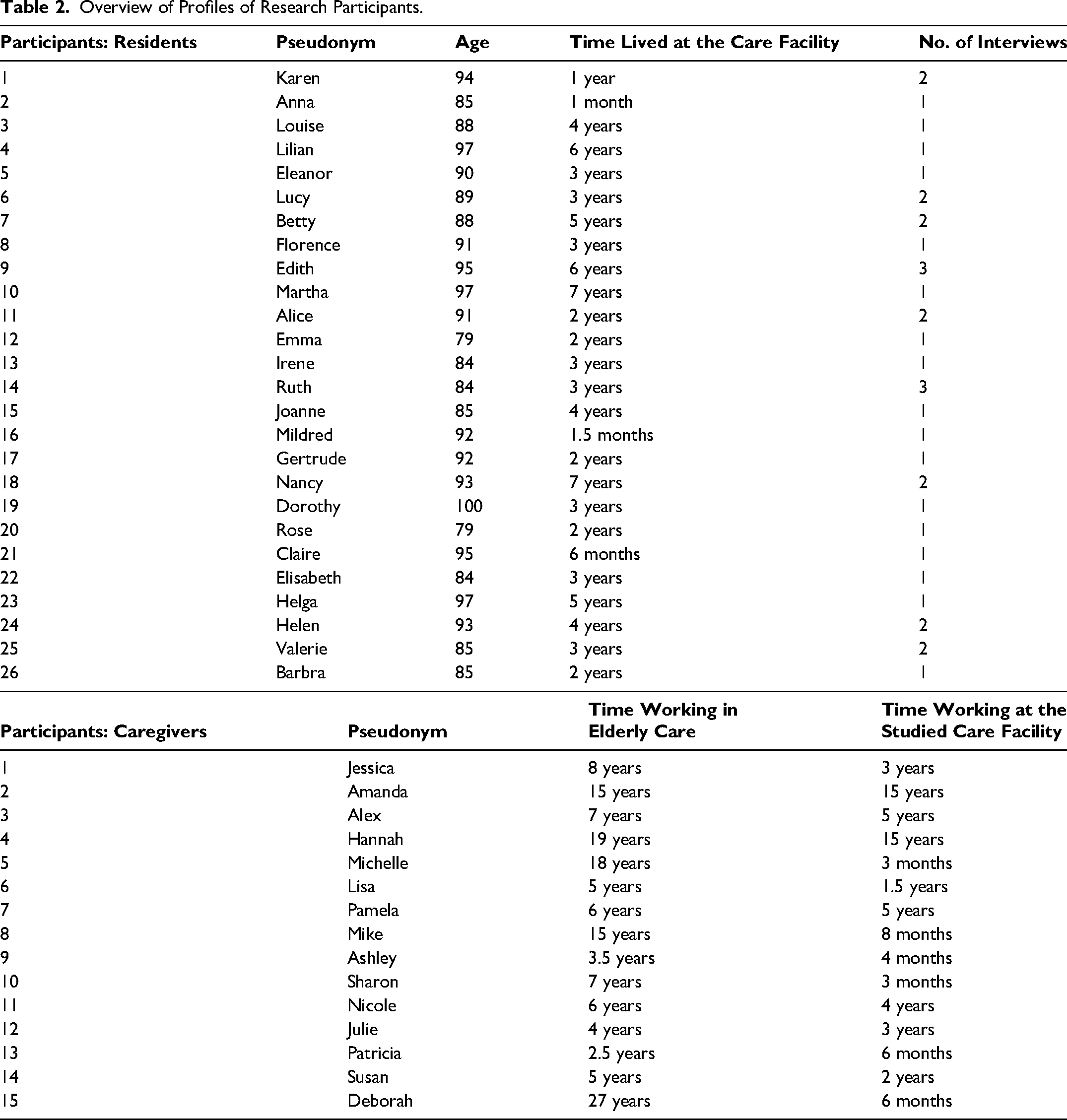
Ethnography was deemed the most appropriate method because it is “about understanding human experience … by studying events, language, rituals, institutions, behaviors, artifacts, and interactions” (Cunliffe 2010, p. 227). One author immersed herself in the care home, spending one to three days a week there over eight months, explicitly identifying herself to residents and staff as a researcher and reminding them of her role throughout the field study. A multimethod approach was used that combined (1) participant observation that included conversations and interactions with residents, service personnel, and managers, (2) interviews with residents, (3) interviews with staff and managers, and (4) examination of documents. First, the researcher engaged in participant observation, where she focused on the lived realities and experiences from the perspectives of the participants in situ (MacInnis et al. 2020). This included assisting residents in their morning routines; helping during meals; reading the newspaper to residents; accompanying residents on walks; participating in weekly activities such as hobby groups; sitting with residents in communal areas; and conversing about current life situations, memories, activities, and experiences of the service. Second, to deepen understanding of the consumer experience, the researcher conducted 37 personal interviews with 26 female residents (see Table 2). The youngest interviewee was 78 years old and the oldest was 100 (average age was 92). Due to interruptions or respondents’ preferences, some residents were interviewed more than once. Residents with cognitive impairments were excluded from the study. An interview guide was used and included (1) resident background, (2) the circumstances and experience of the transition to the facility, (3) their current situation (such as a typical day, perceptions of activities, staff, other residents, family interactions), and (4) how they think and feel about the future. The interviews took place in the residents’ rooms and ranged from 10 to 100 minutes, averaging 68 minutes. The transcripts totaled 708 double spaced pages. Third, to further understand the different voices within this setting, the researcher conducted personal interviews with 15 caregivers (see Table 2). These focused on caregivers’ insights as cocreators and their reflections on residents’ experiences and sought to capture caregivers’ perceptions of daily assistance (e.g., helping with hygiene, dressing), non-task-oriented interactions (e.g., socializing), and how they believed residents perceived their assistance and their own life in the care home. These interviews ranged from 35 to 120 minutes, averaging 70 minutes. The transcripts totaled 486 double-spaced pages. To build rapport and encourage natural conversations (Davies 2005), interviews with residents and caregivers began three months into the field study. In this way, observation enhanced interview quality, enriched data interpretation, and strengthened research rigor (von Koskull 2020). Fourth, internal and external documents were reviewed and triangulated with data from observations and interviews. Internal documents included communication materials and organizational policies. External documents covered trends in the aging population and their care service needs, regulations, and media reports on residents’ care home experiences. Web Appendix B provides an overview of our various data sources’ contributions to our study.
Overview of Profiles of Research Participants.
Data Analysis
The ethnographic material, composed of participant observation, interview transcripts, and documents, formed the corpus for our analysis. We began by exploring the data to code emergent recurrent terms, themes, and patterns (Spiggle 1994) across the data sources. We focused on the residents’ perceptions, feelings, and actions around everyday life in the care home and what managers could change for the better. As the analysis progressed, the data surrounding challenges and opportunities to well-being became preponderant. This process led us to identify consumer agency as the central feature to well-being challenges and opportunities. Supported by research showing agency's importance in residential care (e.g., Berry, Yadav, and Hole 2024), we delved further into the data. The finding that residents experience and live in the world of an immersive service with structures that influence agency steered us toward the concept of figured worlds (Holland et al. 1998) as an enabling theory (Dolbec, Fischer, and Canniford 2021). We engaged in dialectical tacking between our data and figured worlds theory to form, revise, and expand our understanding of the immersive service phenomenon. After several rounds of (re)analysis, we discovered that what we had originally interpreted as challenges were, in fact, reflections of structural characteristics of immersive services. We labeled these encapsulation, positionality, multivocality, and protocolization. Moreover, what we had originally seen as residents’ well-being opportunities were related to their pursuit of agency, and consequently we labeled these pathways to agency. Web Appendices C and D present our coding with representative quotes for each characteristic and pathway to agency, triangulated across data sources used.
To affirm that the analysis was meaningful and authentic (Davies 2005), we presented our emergent findings to the research participants at the studied field setting. In addition, our emerging themes were presented to older people, service professionals, and citizens beyond the studied setting. These presentations allowed us to “test-market” our ideas (MacInnis et al. 2020, p. 6) and to ensure that our interpretations resonated with stakeholders (Davies 2005).
Findings
Next, we discuss the four characteristics we identified as the basis for our conceptualization of immersive service. We also show that, as part of experiencing these characteristics, consumers faced challenges to their agency; in parallel, they also created agency by figuring out how to be and to act within the figured world of this immersive service. Specifically, they engaged in improvisation to pursue pathways toward individual and collective agency (Figure 1). 3
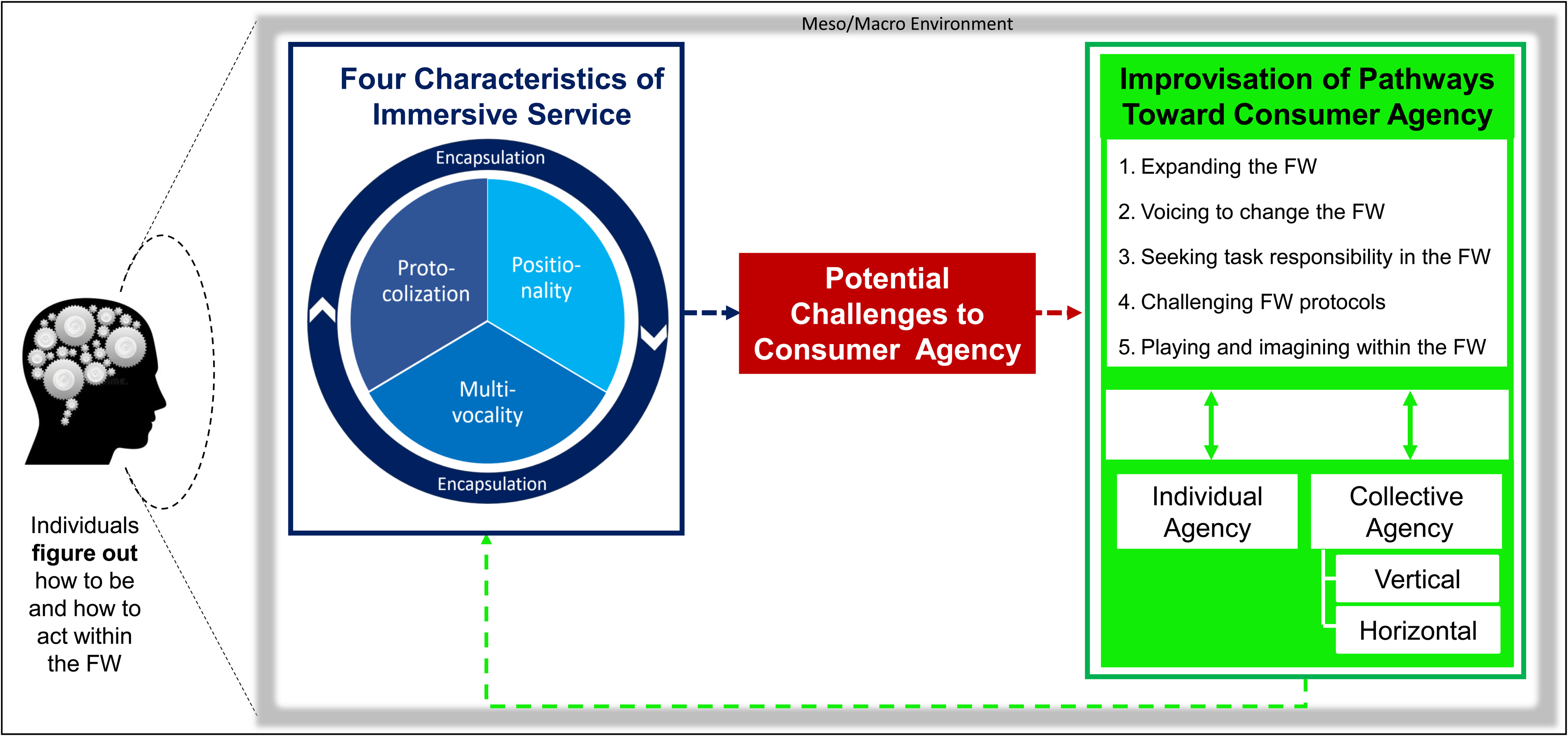
Conceptual Framework of Immersive Service: Characteristics, Challenges, and Pathways to Consumer Agency.
Four Characteristics of Immersive Service and Consumer Agency
Our research unearthed four major characteristics of immersive service: encapsulation, positionality, multivocality, and protocolization. We discuss these characteristics in light of FWT as they reflect sociocultural aspects of structures (here, a service organization) that bring implications for and restrictions of consumer agency as the residents figure out how to be and act in this figured world (Holland et al. 1998; Urrieta 2007). These aspects of structure may threaten agency if they limit the consumers’ ability to act independently or to make their own choices. This threat may vary depending on whether the structures limit what consumers value or rather free them from actions or decisions experienced as burdensome. That is, each of the four characteristics can contribute both positively and negatively to well-being. We focus on consumer-perceived challenges, as these offer more actionable managerial insights into how to improve the service. Finally, as we illustrate the characteristics via our data, it will become clear that these characteristics do not operate in isolation but interact with each other in immersive service.
Encapsulation: figuring out embeddedness
Encapsulation is a foundational characteristic of an immersive service, which makes the impact of the other three characteristics on the consumer even more profound (Figure 1). We define encapsulation as the consumer being embedded in the sociocultural world of the service during a service experience and, to a great degree, separated from other worlds. The notion of a figured world means that a consumer is surrounded by its different voices, stances, narratives, and positions of power in addition to the usual cultural elements such as norms, values, and beliefs (Holland et al. 1998). Thus, encapsulation typically corresponds to a reduction in options and choices (i.e., agency) for consumers, which can include separation from important others and spaces and limitation of with whom, when, and how they are interacting. Frequently, as in our care facility, encapsulation included physical encapsulation, which resonates with Holland et al. (1998, p. 274) referring to individuals being “inhabitants” of a figured world. In our context, this is literally the case as consumers live 24/7 in this world: the service and their everyday life coalesce to a large extent as the consumers eat, socialize, sleep, bathe, and so on within the immersive service. Thus, residents had to figure out how to fit and function within this immersive service, often regardless of their preferences (Holland et al. 1998). Nancy (93 years old) talks about this encompassing nature as she equates the immersion in the care facility service to immigrating: “they [the residents] are immigrants in this life, similar to a Kenyan coming to Northern Europe. We know as little about this ‘country’ [metaphor for the care home] that we call home.”
Main challenges of encapsulation included being embedded in the immersive service world and being separated from other worlds. Emma (79 years old) laments that she experiences her life in the service world separated from her usual social contacts: “It's a bit lonely sometimes. When you sit here alone, when you should have someone.” Although some residents kept connections to their previous figured worlds, Lucy (89 years old) talks about the physical and social separation from desired spaces outside of the care facility's immersive service: Lucy: I have six hectares that will be for my use as long as I live. So that I can go home whenever I want. And I sure want to [chuckles] but I have to survive [there] too. Researcher: So, you don’t call this home? Lucy: No. It doesn’t feel like it. No. But it's a great room and very pleasant. But I haven’t gotten any close friends here that I would be able to simply discuss things with.
The physical separation of this immersive service was further underscored by the locked-door policy (care facilities often have locked exterior doors). Although the doors are locked for safety reasons, this policy was, at times, viewed as an affront to the older adults’ agency, as well as a harsh separation from other people and other physical spaces.
An ancillary to being encapsulated was that residents were highly limited to interactions with people within the immersive service. In fact, who they were encapsulated with was one of the most frequent challenges mentioned by residents. The national “aging in place” policy meant that older consumers often did not move to the care facility until they were frail or had memory impairments. This reality made it difficult for residents to develop relationships with many others in the care home and with people they would have preferred to interact with, as Martha (97 years old) describes: The shock is huge, no question about that, and sometimes, for example, when you sit there and eat, and a lady [another resident] takes some oatmeal and her pants fall down, and then a man who has been in the sauna enters wearing nothing but a robe, so you almost believe you’re in a mental hospital.
Relatedly, in an encapsulated space, it can be difficult to avoid other residents. Florence (91 years old) talks about difficulties with avoiding another resident: There is somebody who's stuck on me, she has tried several times like: “Can I come to you and watch that and that?” and I have refused. She keeps hanging on. She comes and as I eat, she watches and she talks and talks, and I can’t get rid of her.
Encapsulation within the immersive service also means that the usual delineation of public and private spaces can become blurred. Spaces that are typically private (e.g., a resident's bedroom and bathroom) are within the immersive service. There is no completely private space. In the care facility, these spaces also constituted the workspace for staff, where they, consequently, often became the scene of exposure and vulnerability as employees assisted the residents with personal and intimate everyday tasks (e.g., washing, bathing). This created challenges, especially as consumers felt that they had little to no agency and had to accept with whom, when, and how to coproduce these assisting services. Just as there were residents that others may not wish to be encapsulated with, there were staff members that residents did not wish to be encapsulated with. For example, Mike (caregiver) talked about how some female residents do not like it when a male caregiver assists them with a shower, illustrating this in one instance where a resident “starts to get nervous at the beginning of the week” in anticipation of her Friday shower, wondering whether she might have assistance from a male staff member. Going beyond these aspects, encapsulation gave rise to the importance of the other three characteristics in the quest for and management of the residents’ agency: positionality, multivocality, and protocolization.
Positionality: figuring out social position, power, status
We define positionality as a consumer's understanding of differences in social position, and their negotiation of these aspects within an immersive service. As in any figured world, consumers’, providers’, and others’ positions within the immersive service differ, matter, and affect their experiences (Holland et al. 1998; Urrieta 2007). Positions are linked to differing levels of agency as well as to who makes decisions within the figured service world. In our facility—although position may be sought out, rejected, offered, and negotiated—positional power usually favored the staff or organization rather than the residents. This reality challenged residents’ agency. Challenges related to the positionality between service providers and residents were especially evident in that the protocols and processes that regulate the immersive service were (to a large extent) decided by the providers/organization rather than the residents. The staff played a more active role while the residents played a more passive role (less agency) in decision-making. Nancy (93 years old) rejected this position and felt that residents should have more agency: You should be involved, very little is asked from us, what we want. We are passivated. Rather, it is being said that “we have decided upstairs that it is done like this.” It should come from the bottom up. We should be stimulated to take part in our own lives for as long as possible, but instead, it is kind of stifled from above.
Dorothy (100 years old) echoes the sentiment about the importance of the voices of older people in the sense that they did not hold high positionality: “Even older people need to be seen as living creatures. … Being here, we are too much treated like … a school class. … We should be heard!”
We noticed not only the residents’ desire for a stronger voice but also pronounced friction over how much positional power the staff members have relative to the consumers. This was evident in our introductory quote, when Nancy (93 years old) overheard a caregiver talking about her: I overheard in the corridor, a caregiver saying, “She is not the one who decides; we are the ones that decide!”, and that's not what it should be like; this is my home.
While acknowledging the importance of meaningful positionality of residents and, at times, the disconnect of this with the service provision, staff also recognized their own positionality. Caregiver Mike illustrates concern for this disconnect with an example where the staff's “magic” (i.e., their skills to perform medical tasks) is practiced in a perfunctory way due to holding higher positionality: In the evening, one of the residents likes it very much if you sit down and ask her a little bit about her day. … I think it's awful, when you just go there to give them eye drops and then you turn around and leave, in 30 seconds you do your “magic,” and then you go out and close the door. That's it. And sometimes even forget to say goodnight.
In addition, the recognition of the position of the staff (i.e., consumers are often highly dependent on staff) in an immersive service may also push consumers themselves to dampen their voice, as Nancy (93 years old) stated about critical customer feedback, “How many are there who do not dare to say anything?” We observed that the older adults’ perceptions of their position played a role in their assertiveness and willingness to express their voice regarding their desires. For many, this assertiveness could also be a double-edged sword, as Ruth (84 years old) recognizes: My background is a nurse, so I have that experience, so I always have the feeling that some of the staff think of me as being “difficult,” because I might set [certain standards] and say—so that it is how I want it to be. But, this is my home. I pay for my place here, and I’ve been promised help, help that I need, but this I’ve for sure had to fight to get.
Ruth perceives that taking a more agentic role in terms of asserting her preferences, based on her nursing experience, may cause discomfort to the staff. Her concern of being seen as “difficult” stems from her perception that in this figured world consumers ought to subordinate their position and comply with the professional authority of caregivers.
Notably, positionality also exists between residents, as some are perceived to hold more power than others due to their past experiences or expertise. In fact, some residents welcome these individuals taking on a more active “advocate” role, which can benefit residents. However, we also observed positionality in how residents perceived others who were frail and in more vulnerable positions. Accordingly, some residents positioned themselves apart from other residents who had memory impairments stating, “I am not one of them!”—indicating the perceived position of those who are “one of them.” Similarly, Valerie (85 years old) reflects: Some of them are so old that they are completely lost, and the staff try to help them to eat. … I wouldn’t want to live for that long, because I would only be a burden to the people around me.
Valerie's concerns highlight her awareness of, and distinction from, others in more vulnerable positions. This seemed to contribute to heightened anxiety and concerns of her agency. Notably, positionality interplays with the other characteristics, most especially the influence of different voices.
Multivocality: figuring out different voices, narratives, and stances
FWT recognizes that various voices and dialogues operate within a figured world (Holland et al. 1998). Indeed, we found “multivocality,” such that there was not just one clear narrative but multiple voices in this immersive service world. We define multivocality as different external and internal voices consisting of interpretations, narratives, and stances that influence both self and others regarding how to be and how to act in the immersive service.
First, on a broader level, we identified two dominant narratives operating within this immersive service that, at times, clashed: the “home” and the “caring organization.” Narratives are explanations or stories that are told and repeated in order to perpetuate a social group's stances and values (Bacon and Lalvani 2019). For the residents, the dominant narrative of the immersive service was “home.” We heard phrases such as “it doesn’t feel homey,” “this is my home,” “it is more like home, home-like.” This narrative of home, which for most meant warmth, caring, and the freedom to live as one wishes, contrasted with the service organization's narrative of “caring organization.” While the caring organization narrative had the desire to be nurturing, create belonging, be compassionate, and make a meaningful difference for the elderly residents, as we heard from the staff and residents, these were balanced against the priorities of ensuring the safety of the older adults, maintaining organizational effectiveness, and operating efficiently. The caring organization narrative was reflected in the emphasis on adhering to schedules, limiting time (for staff) to socialize with residents, keeping residents safe, deciding and setting up protocols, and encouraging resident compliance. The melding of the two narratives took extensive work on the part of residents and was related to more specific aspects of multivocality, as we discuss next.
For residents, staff constituted a frequent challenge to agency due to different voices. This is understandable, given that the impact of the different voices was influenced by positionality in that certain voices were assumed by some to have more power. To illustrate, recall Nancy's, Ruth's, and Dorothy's impressions that suggest the residents felt that other voices (e.g., the organization/staff) were trying to limit dialogue, gain compliance, and potentially silence the residents.
In addition to the general concern about their voice not being taken into consideration, there were specific incidents when there were conflicting voices. For example, in situations where the residents wanted to stay in their rooms and not engage with others, the staff advocated and, at times, insisted that residents participate in routines such as weekly leisure activities or eating their lunch in the communal dining area, as this was seen as promoting their well-being. Residents lost some of their agency, in that they usually complied with the staff. Conflicting voices between residents and caregivers were also evident with regard to perceptions of the residents’ capabilities. Consider the example of a doctor assuming that seniors need assisting technologies (here, a walker), which clashes with Helen's (92 years old) view: The doctor kept on saying that I should start using a walker. I said “no.” She said, “When you are at this age you must have a walker.” … And she kept on going on about my age so that I finally said, “I’m sorry now, but I do know how old I am … I’m not taking it.” See, one should not start relying on a walker in advance, one should try to maintain one's condition and what one is capable of.
Similar to Barnhart and Peñaloza's (2013) research, this physician's voice indicating “age-appropriate” roles and tasks was not in line with Helen's stance, and she used agency to voice her disagreement. As this example shows, consistency of voices within the organization was not always the case; in fact, it was not unusual to see conflicting voices within the organization that advocated the opposite. In contrast to the situation with Helen, caregivers advocating for well-being often voiced that a resident could and should be doing more for themselves, which at times did not align with the resident's wish to be taken care of and to abstain from activities. Mildred's (92 years old) observation recognizes such different voices: her own, the caregiver's, and the organization's: It's like the personnel here are in conspiracy; they want me to do more on my own. But the organizational policy says “the personnel is here to help.” They want me to “put in more effort.” I put in effort every day when I manage to get out of bed and get dressed by myself. I do what I can, and I can’t do more than that!
At times, we observed different voices between residents themselves, usually related to norms within the immersive service. For example, Dorothy (100 years old) wanted to wear her nightgown in the common areas in the evening. She tried this, but was met with disapproval (i.e., different voices) by what she felt were disparaging looks and comments. As a consequence, she stayed in her room more; thus, this restriction in her agency isolated her more. There were similar norms that were shown through a voice subscribed to and monitored by the majority of residents with regard to such “correct” practices while sauna bathing and eating.
The older consumers were also subject to multiple internal voices, which can result in challenges. That is, some residents had different internal voices that debated with each other, at times emphasizing one stance versus another as they used their agency in an effort to orchestrate the different voices. For example, Alice (91 years old) discusses the tension between voices and illustrates figuring out how to be with regard to remaining in the facility: Well, I’ve been thinking that how am I supposed to look forward. … Is this the way I’m supposed to live the rest of my life? I have to say that I have a bit of a hard time … accepting that … but on the other hand, I realize that I’m a very two-sided person in that way. … I experience it very often, like the sense telling me that it's good the way it is [to stay in the care facility], but the heart says no.
As the fourth characteristic of immersive service, we identified protocolization, which evidenced organizational efforts to manage multivocality, positionality, and encapsulation.
Protocolization: figuring out routines, protocols, and processes
Protocolization reflects the reality that immersive service organizations, as structures (Baker 2005) and figured worlds (Holland et al. 1998), impose a certain way of doing things. A figured world forms and perpetuates itself through “significant regularities” in everyday life (Holland et al. 1998, p. 53); indeed, we saw the figured service world constructed and maintained through protocols. We define protocolization as the establishment of a set of procedures, processes, and routines that consumers are expected to abide by within an immersive service. We found that decisions regarding protocols were mainly made by the immersive service, as reflected in the residents’ (Nancy, Ruth and Dorothy) concerns about decisions coming “from above.” In this care facility—overtly reflecting the managerial care narrative—protocolization served two major purposes to the organization: (1) to guard the safety and security of consumers and (2) to accomplish effectiveness and efficiency. In protocols, voices and narratives are structured into the figured world. As discussed previously, while there were efforts to take into account the residents’ narrative of home, this was often subordinate to the protocols reflecting the managerial care narrative. Corresponding challenges of protocolization were evident in the time frames given to staff to take care of every resident, which often forced the employees to rush their patients and offer noncustomized care. Recognizing this issue, the caregiver Lisa described service interactions in the mornings as residents got out of bed: What makes it a little difficult sometimes when you’re working within health care is receiving help. You’re like “yes, yes, come, come, come, up, up, up,” “no I can’t,” “no, you have to get up now, come on up, up, up, I don’t have time, I also have to see others.”
Protocolization often limits options and, thus, agency. In the care facility with its dominant managerial care narrative that is especially concerned with safety, certain protocols were deemed important, especially with seniors who may take risks seen as unacceptable by the organization. For example, to mitigate the risks of accidents, many residents were not allowed out of the facility without a caregiver or another accountable person. Likewise, protocolization includes many routines and procedures that providers had to follow in part to ensure safety and to ward off risks of subjective and differing judgments by different staff. For example, there were routines for giving medications to avoid errors. In our facility, protocols also promoted efficiency in a service that has high turnover and often overextends employees.
4
Protocols and their efficiency encompassed daily activities and determined the activities’ temporal aspects (e.g., when to get up in the morning), spatial aspects (e.g., meals primarily served in a shared dining area), procedural aspects (e.g., lunch served in a specific pattern), and occasionally even quantity aspects (e.g., number of assisted showers per week). This protocolization restricted the residents’ control of their daily life. For example, Ruth (84 years old) described what a typical day looked like: Ruth: So, the morning starts with somebody knocking on the door and enters. … Then, they help me with the morning routines … between seven and seven thirty. Researcher: So, you are a morning person? Ruth: No, they come when it suits them; they [day shift] start at seven; they have to do their morning routines, and breakfast is [served] at eight thirty.”
Notably, Ruth talks about “their” morning routines as if the residents are not involved in them, indicating restricted agency. In short, a structure's protocolization can limit choices for consumers and employees. This lack of agency can cause challenges, as indicated by Alice (91 years old), who feels less at home due to the scheduled routines that ignore her home narrative: I can’t say that I feel like home here. The fact that everything happens at certain times of the day makes it less homey and … honestly, I have to say that, although I’m not confused, that sometimes I have to think hard, what day is it today? … Because you don’t need to know. I would like to see that one day would be a bit different than the other.
These set structures can create challenges, especially if consumers feel that they have little to no choice or influence but simply must function within the service's protocols. The reflection by Lisa (a caregiver we quoted previously) regarding the lack of time to socialize with residents because of the need to accomplish the morning routines also reflects protocolization and recognizes that staff can also feel this challenge to agency.
To summarize, our data unearthed four structural characteristics of immersive service and revealed that they can limit consumer agency, which can affect well-being. Yet, as part of the process of “figuring out” how to be, we discovered that consumers improvised pathways toward agency.
Consumer Improvisation of Pathways Toward Individual and Collective Agency
Through a FWT lens, consumer efforts toward agency are consistent with the concepts of figured worlds as sites of possibility and improvisation as people negotiate narratives while they figure out how to act or bring positive change to their figured world (Holland et al. 1998). Thus, we view consumer improvisation as consumers crafting pathways to pursue agency and having an impact on the figured service world by alleviating perceived challenges to their agency.
We identified five general pathways that consumers used to pursue agency within the figured service world of the care facility (Figure 1): expanding the figured world, voicing to change the figured world, seeking task responsibility in the figured world, challenging the figured world protocols, and playing and imagining within the figured world. These pathways can overlap and vary across situations and consumers; they can also be pursued individually and collectively by consumers, as we further discuss next.
Expanding the figured world
Through this pathway, residents exert influence and control over time and space on their own terms, as a way to create a realm to do more of whatever and whenever is desired. That is, within these self-created realms, consumers shape their experiences by engaging in activities of their own choice or by grasping a moment in time in which they are in charge and not “being run” by protocols or positionality. There were numerous examples of how residents chose to act to foster their agency, either within the immersive service but outside the structured daily routine, or entirely outside the residential setting. For example, Helen (92 years old) created “breathing time,” or an “oxygen hole,” as she called it, through her walking routine away from the encapsulated confines and protocolized structures: I go out for a walk. I walk a lot. I take a walk in the mornings, see that's my only, that's like my “oxygen hole.” Yes, so I go out for walks every day, not terribly far, but still.
This routine created a realm of time and space where Helen was in charge and able to make choices such as whether to go out or not and deciding on the route and the length of the walk. Similarly, Martha (97 years old) explained how she used her own kitchenette, in which she could eat and drink whenever she wanted without the presence of others. I enjoy having the possibility of a kitchen. … I will make my coffee in the morning on my own, and I will eat my evening snack and grab a beer on my own and I enjoy it.
The kitchenette allowed Martha to circumvent some immersive service characteristics (e.g., protocolization) and to choose, in this case, what, when, and with whom to eat and drink. In addition, consumers expanded their figured service world in ways that leveled some of the positionality, emphasized the importance of their voices, and promoted social interaction, cognitive stimulation, and physical, emotional, and spiritual support. Consider the quarterly magazine produced by a group of residents. This group met regularly as an editorial team that decided on the magazine’s content and structure and encouraged other residents to join and contribute to the journal. Other examples include the weekly swimming exercise class that some residents found available at another facility and jointly engaged in, and the “wine and cheese evenings” initiated by a group of residents and contributed to by the care facility, as Elisabeth (84 years old) notes: We are a number of ladies who meet on Saturday nights, the house [service organization] buys the cheese, and we have our own wine that we each bring … and we have a really great time. So, it's the highlight of the week to sit together, drink, and talk.
In this gathering, the residents created a realm where they went beyond the life prescribed by the protocolization and expanded the boundaries of the encapsulation, as Eleanor (90 years old) illustrates: Everybody gets to be as they are. And we talk very little about [name of the care facility]; rather, we talk about everything that happens and has happened, and I like that more. We have enough of it [the immersive service] during the day, we get quite enough of [the facility], so we have something else during those evenings.
With such collectively created pathways, residents crafted agency by pooling their efforts to achieve a common goal of their own, a feeling of “we-ness” and of more agency. Although certainly not exclusively, the expanding figured worlds pathway was frequently used to address encapsulation challenges, but also compounded by positionality and protocolization.
Voicing to change the figured world
Voicing—the residents’ overt articulation of thoughts, opinions, and feelings related to positionality, protocolization, encapsulation, or multivocality—was another pathway to agency. With the multivocality of immersive services, residents often felt that their voices were not considered, which undermined their agency. To address that, some residents voiced thoughts, opinions, and feelings, especially if they experienced “wrongdoings” with caregivers, or when they felt they needed to stand up for their own or other residents’ rights. For example, Helen (92 years old) refused to conform to the authoritative voice of a caregiver and expressed an alternative view: The caregiver simply said, “Take it,” but I did not recognize the pill and said, “I want to know what it is, or I am not taking it!”
Voicing entailed suggestions to caregivers of how they should assist or could provide better service, as well as complaints to managers. One of the caregivers (Susan) reflected on feedback from the residents and how that influenced how she thinks about providing service: Well, a positive thing is that you get the feedback immediately. They [the residents] are fast to [judge/comment], and I have received [positive feedback], they are very satisfied. But, the negative feedback is just as important, like you have to be able to discuss things. You can give constructive feedback and then it makes you think, “How could I do it in another way?”
As mentioned in the discussion of positionality, some residents were more expressive than others and spoke on behalf of others, or as Florence (91 years old) puts it, “Nancy is a spokesperson for all of us, she used to work as the chairperson for an association of retirees and she looks after all of us here.” Nancy's previous position gave her more experience in voicing her stance; thus, her voicing was a pathway to agency not only for herself but also for others. Yet, similarly related to positionality, voicing can be experienced as a double-edged sword, as it was not always met with enthusiasm by providers. Nevertheless, through voicing consumers can create new possibilities and changes within the figured service world. A new breakfast routine was one such example where the residents’ voicing made the organization change the procedure from a full-service system to include some self-service elements, as Jessica (a caregiver) explains: It used to be like “I don’t want this” and “I want toast and I don’t want this kind of bread.” So, we [caregivers] became very frustrated, and we decided that we’ll try this, and it's actually worked out well. Now, we have this new system where they make their sandwiches themselves, it has become twice as quiet. … The change has been very positively received.
Seeking task responsibility in the figured world
With this pathway, residents engage in agency-promoting tasks directed toward oneself, other residents, caregivers, or even the organization more broadly. In terms of promoting their agency, most residents emphasize the importance of taking care of their daily living tasks by themselves. This connects to their feeling of position, respect, and worth within the facility. As we often heard, in the midst of declining capacities, the residents want both to be of value and to not be a burden to others. Such tasks included routine activities such as dressing, grooming, using the bathroom, eating, or moving from one area of the facility to another. In addition to fostering health (e.g., mobility), being self-responsible allows the residents to perform daily living tasks more to their personal preference and to avoid some of the impersonalized protocols. For example, despite some physical challenges, Valerie (85 years old) was determined not to give up dressing herself as she wanted to maintain her independence: My left leg is getting worse. I really struggle to put on my socks. I find it incredibly difficult, but I don’t give up, I try and try and try and eventually it works, because I don’t want to give up. If you start giving up and asking for help, then it's over.
Beyond seeking responsibilities for themselves, residents also expressed the importance of assisting other residents and how the position of being a “helper” made them feel useful; examples included calling for help for others or conversing, as Lucy (89 years old) illustrates: I don’t feel like I’m completely unnecessary in this world. If I can help them, I most gladly do. For example, if there aren’t any personnel around and they have to wait, I search; I get someone. I can do that. In that way, then I don’t feel so useless.
Finally, residents also pursued agency by being responsible for certain household chores. Some of these tasks were based on formalized agreements between the residents and the organization, such as taking care of the indoor plants on the ward, performing gardening tasks, and setting the tables for dinner. In any case, task responsibilities promoted consumer agency.
Challenging the figured world protocols
Residents often chafed against the protocols, rules, and norms of the figured service world. Thus, they pursued this pathway by exploring new ways to coproduce that are beyond the protocols, rules, and norms of the immersive service, in light of their own needs and preferences. One such example is Emma (79 years old), who used to be a full-time smoker. Unsurprisingly, smoking in the care home is not allowed; yet, Emma created agentic space by challenging protocols as she smokes occasional cigarettes out the window of her room. Some caregivers also recognize that strict adherence to schedules and routines might not always be suitable in a care home setting or for the home narrative. As Nicole (a caregiver) points out: They [colleagues] don’t always seem to remember that this is not an institution, it's actually their home, so everything doesn’t have to go exactly by the clock and routines. They [residents] should get to take some individual liberties, so why do some staff get annoyed if someone wants to do something a little differently? It's not the whole world.
Nicole's reflection points to the importance of balancing structure with compassion, suggesting that accommodating residents’ individual choices might require some flexibility with routines.
Playing and imagining within the figured world
Through this pathway, residents pursued agency by engaging in playful activities (e.g., games, dancing, sing-alongs, joking) and even by imagining other worlds, to celebrate life as well as to reframe and mask vulnerability. Being playful allowed residents to reframe and shape meanings and situations to align with their needs and preferences and to generate more favorable experiences. Playfulness was visible in social interactions among residents as well as between residents and caregivers, which fostered social cohesion, as expressed by Florence (91 years old): “You’re joking with each other and so on. So, the atmosphere is good, and that means a lot.” Playing as a pathway to agency seemed particularly important when residents experienced uncertainty, vulnerability, or loss of control. For example, Ruth (84 years old) drew on humor while she was assisted with a shower. The uncomfortable situation was further exacerbated by the consumer's lack of choice, as well as by embarrassment caused by being undressed with a caregiver, sometimes of the opposite sex (who is wearing a waterproof gown): No, you cannot [choose who will assist you]. It's the one who has time who comes, but it's nicer if it's a girl than if it's a boy. And they usually wear big rubber aprons and rubber boots too while assisting me, so I usually joke with some that “Well, you are on your way to the lingonberry forest!” [to pick berries].
We found that humor was not used to belittle the experienced challenge; rather, residents used their agency to make the situation less threatening. Being playful made residents feel safe to express their vulnerability and to become more comfortable with adverse situations. Residents would also use playfulness collectively to reframe their position and vulnerability in a positive manner. For example, we observed residents dance with their walkers, defying stereotypes of being weak and depressed. They would also refer to their walkers with playful metaphors such as “my Mercedes-Benz” or “my fiancé.” Playfulness and imagination allowed residents to create another “world.” For example, through make-believe and playful language, residents referred to the care home as being “haunted by ghosts,” as some residents with memory disorder occasionally wandered at night and walked into the wrong rooms. Residents also relabeled the reality of the care home with terms from the outside world; for example, Florence (91 years old) explains meeting her friend who also lives in the unit: “Ruth makes me happy. It's really fun. She lives on the other side of the corridor. … So, we meet often. We talk about meeting at the street corner.” As these quotes illustrate, playing and imagining enabled consumers to reframe challenges to their agency into more positive experiences.
Individual and Vertical/Horizontal Collective Agency
In reflecting on the five pathways, we found that they can be distinguished by whether residents pursued agency individually or collectively, and whether collective agency is manifest as vertical or horizontal (Table 3 illustrates these distinctions in our findings). Vertical collective agency refers to pathways where consumers initiate a collaboration with service providers/organizations. Such initiatives connect formal levels of authority, as they take into account positionality and protocolization and integrate consumers with higher-level authorities (e.g., employees, the organization). In contrast, horizontal collective agency describes pathways where consumers initiate a collaboration with other consumers. Conceptually, these efforts are nonhierarchical collective agency in that people pool resources and operate at an equal level. Here, although they are not part of a formal hierarchy, the voices of consumers are more salient than organizational voices. This increases the likelihood of developing pathways that are meaningful to residents, which is likely to elevate the adoption and impact of the focal initiative.
Illustration of Individual and (Vertical/Horizontal) Collective Agency in Light of Pathways to Agency.
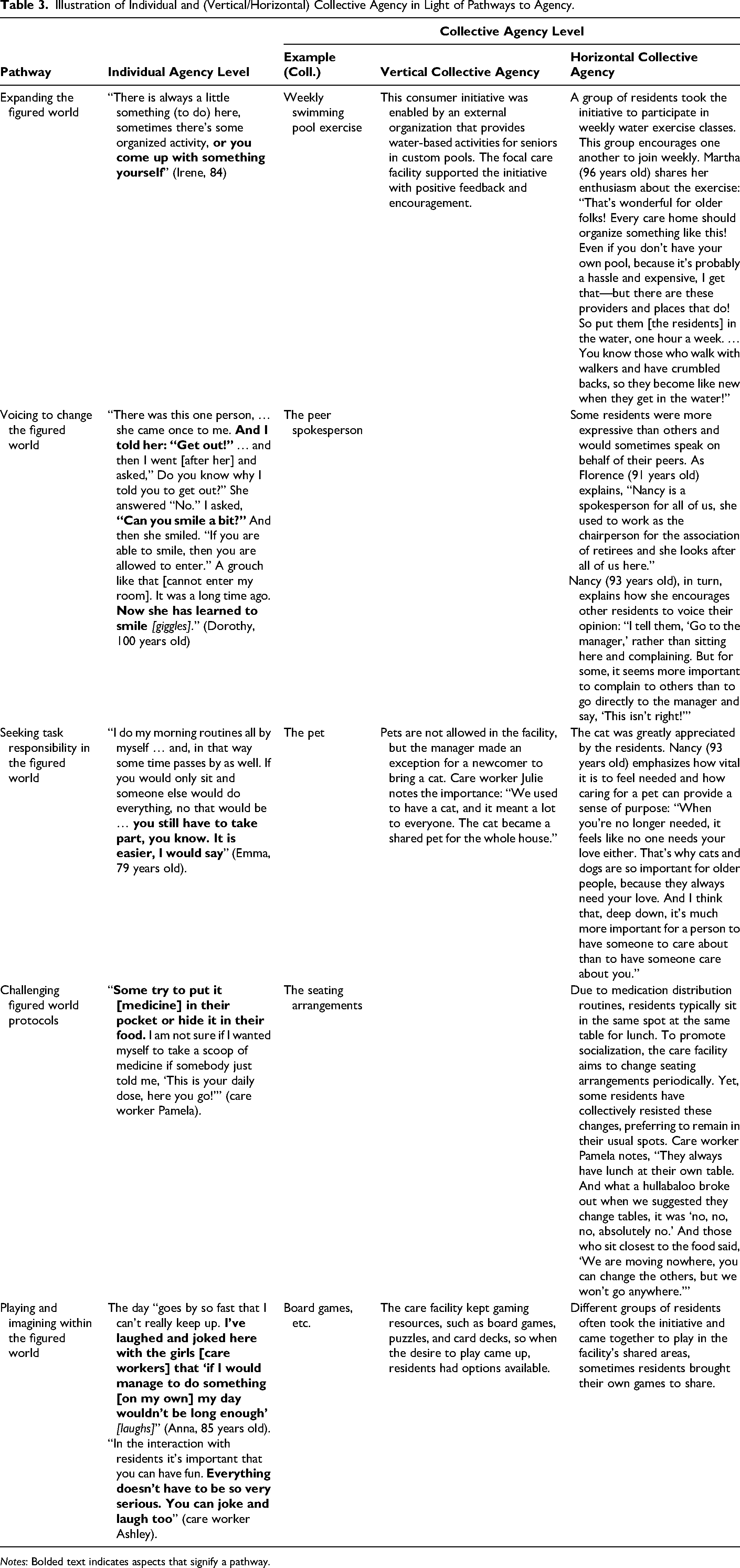
Notes: Bolded text indicates aspects that signify a pathway.
General Discussion
This research examines how characteristics of immersive services might challenge consumer agency, and how consumers bolster their agency in immersive services.
Theoretical Contribution
We identify encapsulation, positionality, multivocality and protocolization as novel characteristics of immersive service. Our work “envisions” something new (MacInnis 2011), thereby expanding marketing theory and the extant conceptual landscape of service types (e.g., Cook, Goh, and Chung 1999; Jaakkola et al. 2017). In addition, our research not only expands important recent work on customer experience (Lemon and Verhoef 2016; Siebert et al. 2020), which did not address any facets of immersive experience, it also directly answers Lemon and Verhoef's (2016, p. 85) call for more research, as these authors underscored “much room for additional research to strengthen the overall conceptualization of customer experience.” Moreover, in contrast to recent research on service design through highly analytical and big data perspectives (e.g., Bellos and Kavadias 2021; Holmlund et al. 2020), we contribute to a stream of literature that positions a “focus on human experience” at the center of service design (Wolf 2019, p. 3), which is especially crucial in the realm of immersive services.
In parallel, our findings are not at odds with prior immersion literature (Jennett et al. 2008) or literature that identified variations within services, including positive versus negative (Morgan and Rao 2006; Rayburn 2015), voluntary versus involuntary (the latter referred to as “captive”; Rayburn 2015), or temporality (short vs. long; Conlon et al. 2004). Rather, our framework unearths a new parsimonious lens into services that have been discussed before (e.g., elderly care, hospitals, educational services) but have never before been examined through the lens of characteristics of immersive services. Catalyzed by FWT (Holland et al. 1998), our work enables marketers to become aware of the four structural characteristics, and reveals how these characteristics affect consumer agency. FWT enriches marketing as it uncovers processes related to consumers “figuring out” how to be and how to act throughout their service experiences. Consistent with FWT, we found that consumers improvise via pathways toward their individual agency and their (vertical and horizontal) collective agency. That is, we show that immersive service may challenge the agency of the oldest-old consumers; yet, far from being passive recipients of the service, our oldest-old adults pursued agency via different pathways meaningful to them. Through these agency pathways the consumers individually or collectively modified or shaped the immersive service to their benefit and for their well-being.
In summary, FWT helps marketers better capture and understand the rich and dynamic nature of service experiences, especially because it accounts for the importance of agency in interactions within service structures. As such, our findings and the FWT lens are closely aligned with work on marketplace dignity and well-being that emphasizes the human need “to be seen and heard, to feel that we have agency in or control over our interactions and transactions, and to be treated equitably and fairly” (Lamberton, Saldanha, and Wein 2024, p. 2).
Extended Contribution: Transferability of the Framework
Transferability refers to the extent to which findings from one context can be meaningfully applied to similar situations (Coghlan and Brydon-Miller 2014). Thus, the degree to which another service context is composed of the four characteristics of immersive service impacts the transferability of our framework and findings. Encapsulation transfers to other services where consumers are surrounded by and embedded within a service and separated from others, such as a school/college day, a hospital stay, a plane ride, or even certain hospitality services (e.g., commercialized mountain climbing tours; Tumbat and Belk 2011). While the duration of these service experiences may vary across individuals or contexts, the fundamental aspect of embeddedness and separation remains. Positionality transfers to other immersive services where a hierarchy of explicit or implicit power exists. Consider, for example, expert providers (e.g., physicians, lawyers, teachers), immersive services with few alternatives (e.g., welfare services) and services with considerable safety considerations (e.g., air travel). Vivid indicators of positionality include the use of titles in services (Professor, Doctor, Captain, Purser, Principal, etc.). Multivocality (i.e., various internal and external discourses operating regarding how to be and what to do in the figured service world) likely transfers to any service where consumers and multiple providers interact, especially when a service experience affects perceived consumer agency. Finally, regarding protocolization, we note that protocols are ubiquitous to structure figured service worlds. Yet, what may vary are aspects such as how those protocols are developed, the extent of protocolization throughout the immersive service, and the flexibility of protocols for customers and employees. Taken together, we expect that our findings are likely to transfer to settings where at least one of the characteristics is present at levels that are detected by consumers (however, our framework does not claim to speak to services where the four characteristics are rather low and might not be detected by consumers).
Contextual Boundary Conditions: Volition, Duration, Intensity of Immersion
Although the four characteristics of immersive service remain the same across many settings, certain situational and individual variables can affect the effect of those characteristics, their impact on consumer agency, and downstream outcomes, as we briefly illustrate.
Volition
The (in)voluntary nature of the service consumption should influence the effects of the four characteristics on agency. For example, in the case of a drastic form of immersive service, namely voluntary versus involuntary admission to health care (e.g., inpatient substance use treatments), research found that voluntary (vs. involuntary) treatment results in better patient satisfaction and social functioning (Kallert, Glöckner, and Schützwohl 2008; Opsal, Kristensen, and Clausen 2019). Thus, ceteris paribus, the effects of immersive service characteristics on perceived agency should be intensified for involuntary (vs. voluntary) consumption experiences; voluntary consumption is preferred for respecting consumer agency and well-being.
Time-related effects
Time likely affects the relationship between the four characteristics and consumer agency. First, in terms of duration of a service experience (e.g., a two-day vs. two-week stay in the hospital, a two-hour vs. ten-hour flight), we expect the associations between encapsulation, positionality, multivocality, protocolization, and agency to become more emphasized with increasing durations, at least up to a certain point (i.e., this could be a nonlinear effect that plateaus after a certain period). Relatedly, it is relevant whether an immersive service experience is of a predetermined duration or whether it is open-ended and ambiguous, with the latter further emphasizing the effects of the four characteristics. Finally, another lens on time is stage-specific, which suggests that challenges of the four characteristics for agency are particularly salient in initial stages of the service experience as consumers engage in considerable figuring-out work.
Intensity (extent) of immersion
Considering the intensity of immersion points to a configurational lens in which each of the four characteristics can vary on a continuum (i.e., from low to high levels, thereby forming different configurations). Progressing from lower to higher levels in each characteristic, challenges to consumer agency likely increase, albeit in a nonlinear manner. This configurational view suggests that even short-term experiences can be characterized by high levels of one or more of the four characteristics (e.g., a two-hour air plane ride where all four characteristics are on relatively high levels). Moreover, the configurational lens allows scholars to study the effects of very high levels of a single characteristic and potential additive, interactive, or compensatory effects between the four characteristics. While our qualitative data allowed us to gain a deep understanding of the consumer experience of an immersive service and identify themes related to this experience, a quantitative approach (e.g., experimental approaches and corresponding manipulations [Botti, Orfali, and Iyengar 2011], big data analytics [Holmlund et al. 2020]) can help answer questions about the impact of a continuum of the four characteristics, or the interaction of individual and situational aspects such as volition, duration, and intensity on the impact of a focal characteristic on agency and well-being that a qualitative approach does not allow.
Cultural contexts
Culture can also influence the association between immersive service characteristics and consumer-perceived agency. For example, consumer beliefs related to power distance, a cultural dimension referring to the extent to which people expect and accept differences in power (Winterich, Gangwar, and Grewal 2018), might affect the degree to which positionality, protocolization, or encapsulation might be more (or less) accepted by consumers and employees.
Managerial Implications
Previously, we had noted calls for more research on residential care that emphasizes the older persons’ lived experiences (Van Loon et al. 2021; Van Steenwinkel, De Casterlé, and Heylighen 2017; Wolf 2019) and promotes their agency (Bradshaw et al. 2023; Knight, Haslam, and Haslam 2010; Moilanen et al. 2021). Against this backdrop, managers can draw on our framework to identify strategic options and achieve strategic goals. First, while there are different possible categorizations of strategic options, we believe that a set of meaningful strategic options emerges from the intersection of leveraging technology to manage spaces and empathic relationships in immersive service (see Table 4 for illustrations). For example, to address challenges related to encapsulation, organizations can support consumers in expanding the figured service world. To illustrate, managers can provide technology such as virtual reality (VR) to allow residents 24/7 access to virtual experiences that expand their figured service world in terms of time and space (e.g., residents can go for virtual walks at a beach or stroll through ancient Rome; Hsieh et al. 2022). In addition, organizations can employ GPS technology (e.g., tracking residents’ phones if they give consent) to expand the physical/geographical safe spaces for consumers to enjoy. These examples illustrate how managers can leverage technology to create consumer agency with regard to virtual and physical spaces. And lastly, interpersonal relationships and empathy options such as shared decision-making, empowering employees and customers, resident councils, or “staff buddy” programs offer other contextual opportunities to expand consumer agency (Table 4). Such approaches not only address challenges related to positionality by fostering an organizational culture where spontaneous and creative expressions are encouraged, but also strengthen the relationships between customers and service staff. Similar approaches offer further synergies related to positionality and seeking task responsibility, as managers and/or staff can encourage consumers to engage in peer support (e.g., leading a group activity) or engage in the facility operations (e.g., identify fitting opportunities for occasional or more formal tasks over longer periods of time, such as meal planning for a week).
Illustrative Managerial Implications to Foster Agency in Immersive Service (Generally) and in Residential Care.
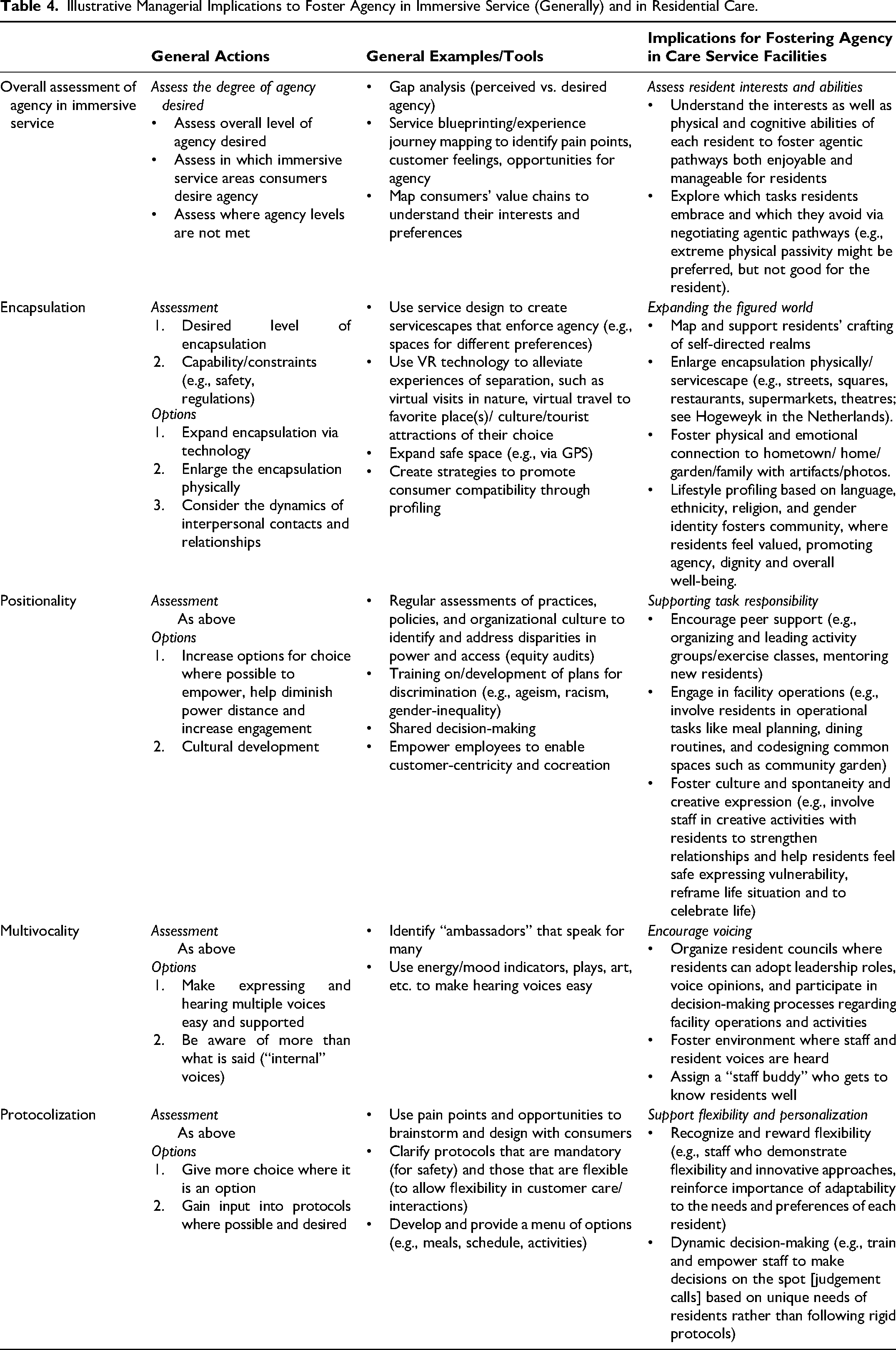
Second, our framework can serve as a customer-focused foundation to derive and achieve strategic service goals. Managers should routinely and systematically analyze customer needs/preferences related to their agency. Specifically, we envision a two-pronged approach that extends seminal gap analyses in service (Zeithaml et al. 2024). The first prong examines customer-perceived gaps (e.g., difference scores via surveys) for each of the four characteristics of encapsulation, positionality, multivocality, and protocolization. Organizations could further enrich such characteristics-specific measures and track, for instance, the intensity, frequency, and duration with which consumers experience challenges linked to these four characteristics. The second prong analyzes customer-perceived gaps for each of the pathways toward individual and collective agency in our framework (Table 3 offers examples of pathways toward individual and collective [vertical and horizontal] agency, but other pathways likely exist). Taken together, this two-pronged approach results in detailed and actionable scorecards that reveal opportunities for improved customer experiences in residential care and other immersive services.
That said, managers should go beyond self-report surveys and draw on the rich literature on service recovery that has emphasized the importance of genuinely encouraging complaints to hear the customers’ voices (e.g., Fornell and Wernerfelt 1987). Equally important, managers should employ technology to collect observational and behavioral data about their customers. For example, customers in health care contexts might carry wearables that allow organizations (if consent is given) to collect and analyze fine-grained, highly personalized data—for example, where and how customers spend their time in a residential care facility and what activities they participate in (e.g., meals, exercise classes, social gatherings, excursions outside the focal facility); such data provide insights into challenges or pathways toward agency. Together with survey and complaint data, such observational and behavioral data can then fuel state-of-the-art predictive analytics to boost personalized service design and delivery in immersive service. Predictive analytics can identify patterns in consumer needs, preferences, and behavior that empower managers not only to offer timely medical interventions and optimize staffing allocations, but also to curate service offers and activities (e.g., pathways toward agency) in light of real-time individual-level preferences. As such, predictive analytics offers truly customized service and also accounts for the reality that not every consumer may wish to pursue pathways toward agency (e.g., expand figured service world, engage in playing and imagining, engage in voicing, challenge protocols) all the time.
Taken together, our proposed approach combines gap-based scorecards with predictive analytics to enhance operational efficiency of the organization and elevate the experience and well-being for residents, thereby successfully balancing the two narratives of “home” and an efficient “caring organization” that we had discovered within our immersive service.
Limitations and Future Research
Our research has limitations (e.g., one setting, ethnography) that bring to light many different areas worthy of further research. First, our concept of immersive service offers a fertile foundation for future research on the characteristics and their subdimensions: for example, we found that protocolization includes temporal, spatial, and procedural facets that affect consumers’ experiences and deserve further attention. Second, marketing scholars need to examine which moderators or mediators help us better understand and manage immersive service (e.g., duration, volition). Relatedly, the decision process of whether, when, and why to enter immersive service deserves further attention, which is an important aspect our work did not examine.
Similarly, more work is needed to understand agency pathways, such as whether pathways occur spontaneously or systematically and whether the duration of such agency is momentary or extends over time. Pointing to other boundary conditions, pathways can be influenced by aspects such as economic resources, personality, prowess, or functional capacity, among others. Thus, pathways are not necessarily one-size-fits-all, and we need work that can guide service organizations in providing “fitting” solutions. Relatedly, we see a need for work on whether high levels of perceived consumer agency in immersive service might backfire in terms of well-being (e.g., consumer overconfidence, risk-taking). Similarly, research should explore unintended consequences of consumer agency (e.g., could vertical agency result in organizations “taking over,” thereby, ironically, reducing consumer agency?).
Another fruitful platform is to connect our view on immersive service to prior work in marketing on customer experience and journeys and specific (sub)stages (e.g., Lemon and Verhoef 2016). As such, temporal and stage-specific differences in the immersive service experience should also be explored. For example, older adults—when first entering residential care—are likely heavily occupied with figuring out who they are and their identity within a care facility (Rötzmeier-Keuper and Wünderlich 2024) and find the immersive service characteristics more strongly affecting agency than those accustomed to the service, who have figured it out.
In parallel, future research on immersive service can draw on theories that have received relatively little attention in marketing but that examine related phenomena, such as research on “place immersion” (Buttazzoni et al. 2022) or “place attachment” (Rosenbaum et al. 2007). We see another promising connection between immersive service and theories on human dignity and respect (e.g., Kirchhoffer 2016; Lamberton, Saldanha, and Wein 2024) and related phenomena that undermine well-being such as employees dehumanizing and objectifying certain service consumers.
Finally, although we included some voices of service providers, our examination was focused on the consumer's experience of immersive service. A dedicated focus on understanding the experience of caregivers in residential care homes is crucial for an even deeper understanding of the effects of encapsulation, positionality, multivocality, and protocolization in immersive service. Caregivers not only provide care and support to residents, thereby ensuring their physical and emotional well-being; in addition, they also connect residents, families, and health care professionals and organizations. Investigating how the four characteristics affect employees can inform improvements in service design and management, for example, to develop strategies to support and retain these employees and to enhance the quality of care in residential settings. With such objectives, marketing research should examine not only the providers’ experiences but also service dyads (provider–consumer) or service triads (provider–consumer–organization) (see Web Appendices C and D, which include some voices of caregivers that can inspire such future work).
Supplemental Material
sj-pdf-1-jmx-10.1177_00222429251319312 - Supplemental material for Immersive Service: Characteristics, Challenges, and Pathways to Consumer Agency
Supplemental material, sj-pdf-1-jmx-10.1177_00222429251319312 for Immersive Service: Characteristics, Challenges, and Pathways to Consumer Agency by Laurel Anderson, Catharina von Koskull, Martin Mende and Johanna Gummerus in Journal of Marketing
Footnotes
Acknowledgments
This article is based on an extensive ethnography conducted by the second lead author. The authors extend their most grateful appreciation and respect to the older persons who shared their wisdom and entrusted her with their stories. We also thank the managers and frontline personnel for granting substantial access to the care home and their daily work. The authors are very impressed by and grateful to the JM review team for their invaluable direction, feedback, and constructive suggestions.
Authors Contributions
The first two authors are both lead authors and contributed equally.
Coeditor
Cait Lamberton
Associate Editor
Amber Marie Epp
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an award to the first author from the Fulbright Foundation of Finland and an award to the second author from the Academy of Finland (grant number 275526).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.