
Abstract
Personal disability identity is a predictor of psychosocial functioning among adults with predominantly physical disabilities. In the present study, we examined personal disability identity in adults with learning disabilities (LD) and/or attention-deficit/hyperactivity disorder (ADHD). In samples of 541 adults with LD, 475 with ADHD, and 433 with comorbid LD and ADHD, we examined the structural validity of disability acceptance and disability affirmation scores and the association between these scores and anxiety/depression, life satisfaction, and general self-efficacy. Factor analyses supported a 4-item disability acceptance and 3-item disability affirmation scale in LD-only and ADHD-only samples. Among adults with LD or ADHD, disability affirmation was a meaningful predictor of life satisfaction, and disability acceptance predicted general self-efficacy. Disability identity attitudes are worthy of clinical and scholarly attention in adults with LD and ADHD, and adults with comorbid LD and ADHD may warrant special consideration in the personal disability identity literature.
Keywords
Research has demonstrated vulnerability to negative psychosocial outcomes in adults with attention-deficit/hyperactivity disorder (ADHD; Bernfort et al., 2008; Uchida et al., 2018) and learning disabilities (LD; O’Brien, 2001). Adults with LD or ADHD experience higher anxious and depressive symptomatology compared to the general population (Kessler et al., 2006; Klassen et al., 2013). More ADHD symptoms and greater functional impairment have been associated with lower life satisfaction among adults with ADHD (Gudjonsson et al., 2009), and adult LD status has been associated with lower domain-specific life satisfaction (Undheim, 2003). Adults with ADHD have been found to report lower perceived general self-efficacy than their non-ADHD counterparts (Newark et al., 2016), and a similar finding has been reported for adults with LD (Slemon, 1998).
Although most research on psychosocial functioning in these populations has focused on risk factors, some researchers have also identified protective factors that promote resilience (Wilmshurst et al., 2011). Research is needed on factors with potential to protect against negative psychosocial outcomes in adults with LD and ADHD (Morrison & Cosden, 1997). Disability identity may be one such set of factors. Disability identity attitudes have been found to predict positive psychosocial functioning in individuals with physical disabilities (e.g., Zapata, 2020) and may act as protective factors in adults with ADHD and LD. Disability identity has just begun to be investigated in adult LD and ADHD (Zapata & Worrell, 2023).
Correlates of Disability Identity
Personal disability identity (PDI) is a set of attitudinal constructs that represent self-concept as a disabled person and involve both cognitive and emotive processes (Hahn & Belt, 2004). PDI has been operationalized as disability pride (Darling & Heckert, 2010), disability denial versus acceptance, disability affirmation (Hahn & Belt, 2004), disability self-worth (Putnam, 2005; Zapata, 2021), and personal meaning in disability (Dunn & Burcaw, 2013; Zapata, 2021). Higher scores on positive PDI constructs have been found to predict life satisfaction (Bogart, 2014), lower anxiety and depression (Bogart, 2015; Zapata & Pearlstein, 2022), self-esteem (Bogart et al., 2018), general self-efficacy (Zapata, 2018), and hopeful thinking (Zapata, 2020, 2021) in samples of adults with predominantly physical, or else non-specified, disabilities. In contrast to the predominantly physical disabilities that have been examined in previous studies on PDI, neurodevelopmental disabilities are commonly diagnosed in childhood and adolescence and may be conceptualized as invisible disabilities, such that their manifestations may be non-noticeable, concealable, or mis-attributable to other factors (Santuzzi et al., 2014). The applicability of current PDI conceptualizations to neurodevelopmental disability communities is worthy of investigation.
Attention-deficit/hyperactivity disorder and LD, which include dyslexia, are neurodevelopmental disabilities that frequently co-occur (Mayes et al., 2000) and, together, represent almost half of all students with disabilities served through special education (National Center for Learning Disabilities [NCLD], 2017) and in postsecondary institutions (Gregg, 2009; Wolf, 2001). As neurodevelopmental versus physical disabilities that are commonly served in educational settings, LD and ADHD may benefit from special consideration in disability research within psychology. In a recent study, Zapata and Worrell (2023) examined disability self-worth and personal meaning in disability—PDI scales that were recently developed by the author—as predictors of psychosocial outcomes in a sample of adults with LD, ADHD, or comorbid LD and ADHD. Zapata and Worrell found that (a) self-worth (p < .001, ß = −.25) and personal meaning (p < .001, ß = −.24) predicted lower anxiety/depression, (b) self-worth predicted general self-efficacy (p < .001, ß = .31), and (c) personal meaning predicted life satisfaction (p < .001, ß = .30). These recent results provide support for the emerging finding that PDI constructs represent separate and independent attitudes toward having disability, which are differentially associated with psychosocial outcomes (Hahn & Belt, 2004; Zapata, 2018, 2020, 2021; Zapata & Pearlstein, 2022).
The Current Study
The relationship of disability acceptance and affirmation –the oldest and most popular PDI constructs (Hahn & Belt, 2004)–to previously-explored psychosocial factors has yet to be explored in adults with LD and/or ADHD. Informed by empirical findings from their original measurement development study, Hahn and Belt (2004) described disability affirmation (vs shame) and disability acceptance (vs denial) as indicating “different perspectives that may be the outcome of varied experiences in the process by which disabled people develop feelings about their own disabilities” (p. 458). In the present study, we examined the structural validity of scores on Hahn and Belt’s disability acceptance and affirmation scales in adults with LD and ADHD, as well as these constructs’ associations with psychosocial outcomes that were previously explored in relation to PDI (i.e., anxiety/depression, life satisfaction, general self-efficacy).
Considering findings by Zapata and Worrell (2023), the authors hypothesized that, in the present study, disability acceptance and affirmation would positively predict life satisfaction and general self-efficacy and would negatively predict anxiety/depression. Based on research precedent (see Zapata, 2020; Zapata & Worrell, 2023), the regression models on psychosocial outcome variables also took into account various sociodemographic and disability-related characteristics that have been theorized to relate to psychosocial functioning among people with disabilities, including age at diagnosis, multiple disabilities, presence of friend or family with the same disability, and satisfaction with disability-related services. Considering recent findings from Zapata and Worrell (2023), the authors further hypothesized that overall higher satisfaction with disability services would predict higher general self-efficacy.
Method
Participants and Procedures
Participants were U.S. adult residents with LD (n = 541), ADHD (n = 475), or comorbid LD and ADHD (n = 433). See Table 1 for participant characteristics by disability type. An online questionnaire was developed in Qualtrics and included items related to demographic information, attitudes toward disability, and psychosocial functioning. A link to the questionnaire was posted, using social media, to online groups related to ADHD or LD in the summer of 2021. Inclusion criteria were having a diagnosis of ADHD, LD, or both and being 18 years of age or older. Participants provided informed consent prior to beginning the questionnaire. When they reached the end of the questionnaire, interested participants were entered into a drawing for 1 of 10 US$50 Amazon gift cards. All analyses were conducted in Stata (StataCorp, 2021). The institutional review board at the authors’ institution approved this study. Throughout this article, the authors have adopted person-first language to describe disability status, but we recognize that the exclusive use of person-first language may not be preferred by some members of disability groups (see Dunn & Andrews, 2015, for a discussion of identity-first language).
Characteristics of Participants in Study of Personal Disability Identity.
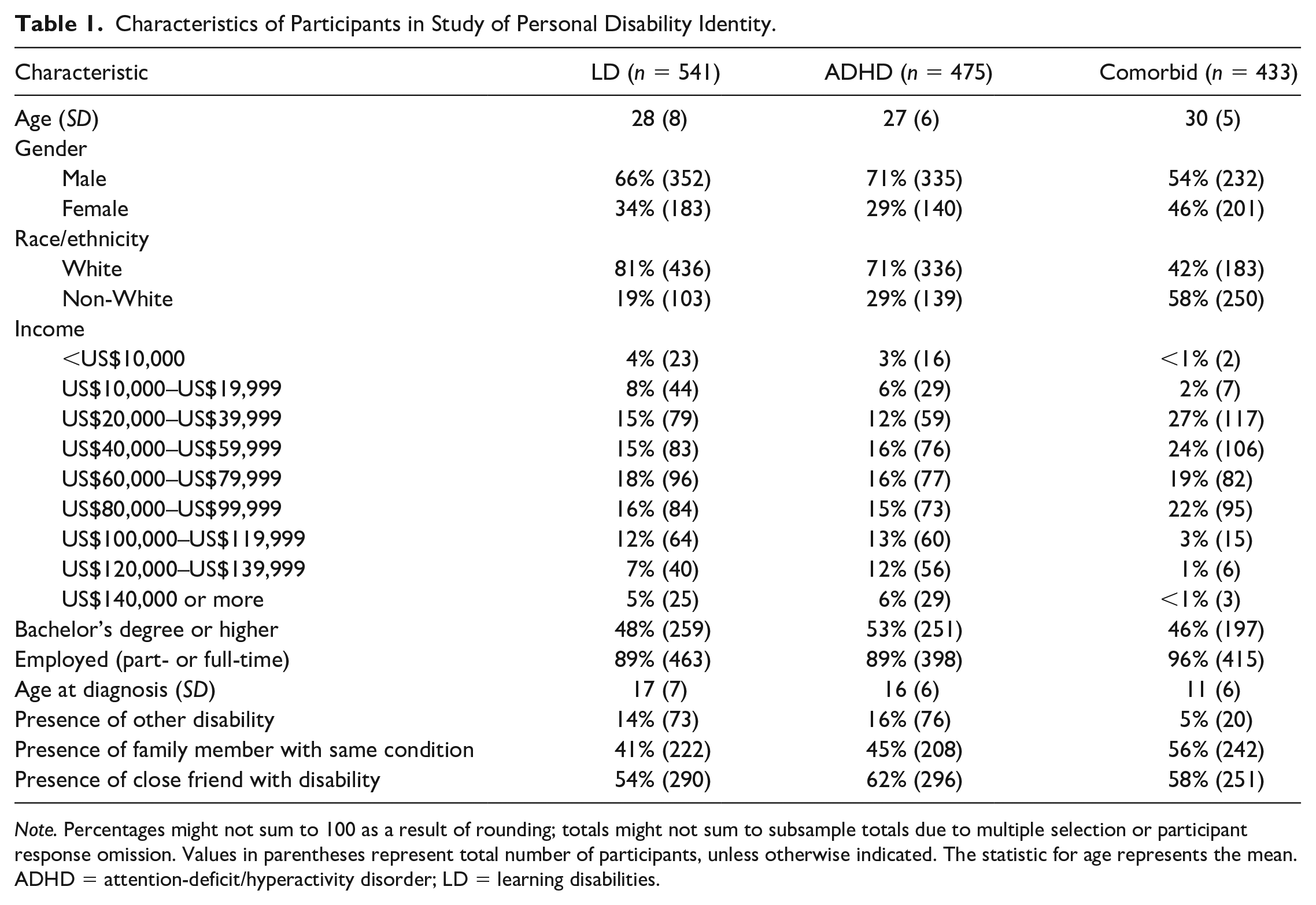
Note. Percentages might not sum to 100 as a result of rounding; totals might not sum to subsample totals due to multiple selection or participant response omission. Values in parentheses represent total number of participants, unless otherwise indicated. The statistic for age represents the mean. ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
Measures
Disability Affirmation and Disability Acceptance
Personal disability identity was investigated using a two-factor instrument developed by Hahn and Belt (2004) to measure disability affirmation (four items) and disability denial versus acceptance (four items). Disability affirmation items included “I feel proud to be a person with a disability.” Disability acceptance items were reverse-scored and included “I do not feel good about being a person with a disability.” Responses for both acceptance and affirmation were on a 5-point Likert-type scale which ranged from 1 (strongly disagree) to 5 (strongly agree). A mean score was calculated for each of two subscales. In previous studies, factor loadings have ranged from .29 to .91 for affirmation scores and from .44 to .91 for acceptance scores (Hahn & Belt, 2004; Zapata, 2018, 2020) Cronbach’s alphas were .83 for acceptance and .82 for affirmation in a recent study involving adults with physical disabilities (Zapata, 2020).
Additional Independent Variables
Participants self-reported age, gender (coded as female = 0, male = 1), race (coded as non-White = 0, White = 1), education (coded as less than bachelor’s degree = 0, bachelor’s degree or higher = 1), and employment status (coded as unemployed = 0, part or full-time employment = 1). Participants reported household income as one of nine ordinal categories ranging from less than $10,000 to $140,000 or more and increasing in increments of $10,000 up to $100,00, and then in increments $20,000 per year (see Table 1). Participants self-reported age at LD or ADHD diagnosis and presence of other disabilities (coded as no additional disabilities = 0, at least one other disability = 1). Participants also reported whether they have at least one member of their family who has the same disability (e.g., LD or ADHD; coded as no one else in the family has condition = 0, at least one family member has the same condition = 1) and whether they had a close friend with any disability (no close friend with a disability = 0, at least one close friend with a disability = 1).
Satisfaction with disability-related services was measured with one item on a seven-point Likert-type scale. In a recent study, satisfaction with disability-related services was found to predict self-efficacy in a sample of adults with LD and/or ADHD that was drawn from the present dataset (Zapata & Worrell, 2023). Disability-related variables were included based on previous PDI research, which has included variables related to age at diagnosis and secondary disability. Congenital disability onset has been found to predict higher life satisfaction among adults with mobility disabilities (Bogart, 2014), but variables related to age at diagnosis or onset have generally not been found to predict psychosocial functioning in PDI research (see Bogart, 2014; Zapata, 2020, 2021). Zapata (2020) found that the presence of secondary disability predicted lower agentic thinking, a domain of hope (see Snyder, 2002). Silverman et al. (2017) found that adults with disabilities who had more friends sharing a diagnosis reported higher life satisfaction; this study included variables related to disability status of family members and friends.
Anxiety and Depression
Symptoms of anxiety and depression experienced over the past 2 weeks were measured using a 4-item, 4-point Likert-type scale instrument (Kroenke et al., 2009). A single mean score was calculated, with higher scores indicating higher anxiety/depression. Depression items were “feeling down, depressed, or hopeless” and having “little interest or pleasure in doing things.” Anxiety items were “feeling nervous, anxious, or on edge” and “not being able to stop or control worrying.” Structural validity and internal reliability evidence for the use of the scale with adults with physical disabilities has been reported. Cronbach’s alpha was .86 for the scores and factor loadings ranged from .73 to .85 (Zapata, 2019). In a more recent study, Cronbach’s alpha for anxiety/depression scores was .65 in a sample of adults with LD and/or ADHD that was drawn from the same dataset (Zapata & Worrell, 2023).
Life Satisfaction
Life satisfaction was measured using a 5-item, 7-point Likert-type scale instrument (Diener et al., 1985). A mean composite score was calculated, with higher scores representing higher life satisfaction. Items included “I am satisfied with my life” and “In most ways my life is close to the ideal.” Structural validity and internal reliability evidence for the use of the scale with adults with physical disabilities has been reported: Cronbach’s alpha was .89 and factor loadings ranged from .65 to .92 (Zapata, 2019). More recently, Cronbach’s alpha for life satisfaction scores was .70 in a sample of adults with LD and/or ADHD that was drawn from the same dataset (Zapata & Worrell, 2023).
General Self-Efficacy
General self-efficacy was measured using a 10-item, 7-point Likert-type scale instrument designed to measure a general sense of personal efficacy, or capability to organize and execute tasks, and to predict adaptation to and coping with life stressors (Jerusalem & Schwarzer, 1992). A mean composite score was calculated, with higher scores representing greater perceived self-efficacy. Items included “I can solve most problems if I invest the necessary effort” and “I can usually handle whatever comes my way.” Supporting the internal reliability of the scale, Cronbach’s alpha was .90 in a previous study among adults with physical disabilities (Zapata, 2018). More recently, Cronbach’s alpha for general self-efficacy scores was .81 in a sample of adults with LD and/or ADHD that was drawn from the same dataset (Zapata & Worrell, 2023).
Results
Structural Validity of PDI Scales
In order to evaluate the acceptability of using the subscales in later regression analyses, confirmatory factor analyses (CFAs) were conducted on the two-factor PDI instrument in three subsamples: participants with LD, ADHD, and comorbid ADHD and LD. Model fit was evaluated using the following fit indices: the root mean square error of approximation (RMSEA), the comparative fit index (CFI), the Tucker–Lewis index (TLI), and the standardized root mean square residual (SRMR). Acceptable model fit was determined based on an RMSEA value at or below .08, CFI and TLI values at or above .90, and an SRMR value of <.08 (Kline, 2005). Factor loadings were interpreted based on recommendations by Comrey and Lee (1992); .71 = excellent, .63 = very good, .55 = good, .45 = fair, and .32 = poor.
The two-factor model of PDI initially demonstrated poor fit across subsamples. The factor loading on Item 3 of affirmation (“I have a clear sense of what my disability means to me”) was below .30 across subsamples and was subsequently removed. This item has consistently yielded a low factor coefficient in previous studies (e.g., Hahn & Belt, 2004; Zapata, 2020), and Zapata (2018) previously found the 3-item affirmation scale to have moderate reliability (ω = .77). Thus, CFAs were rerun using the 4-item acceptance subscale and the 3-item affirmation subscale. Fit indices were acceptable in all three samples (see Table 2), and this model was accepted. However, the results also indicated that several factor loadings were poor in the comorbid ADHD and LD sample, yielding very low internal consistency estimates for subscale scores in that sample. Factor loadings on disability affirmation were .73, .63, and .70 in the LD sample; .69, .59, and .64 in the ADHD sample; and.12, .69, and .20 in the comorbid ADHD and LD sample. Similarly, factor loadings on disability acceptance ranged from .45 to .72 in the LD sample, from .44 to .71 in the ADHD sample, and from .18 to .47 in the comorbid ADHD and LD sample. As the items were not capturing reliable variance in the comorbid sample, this sample was not included in subsequent analyses.
Fit Indices for Two-Factor Model of Acceptance and Affirmation.
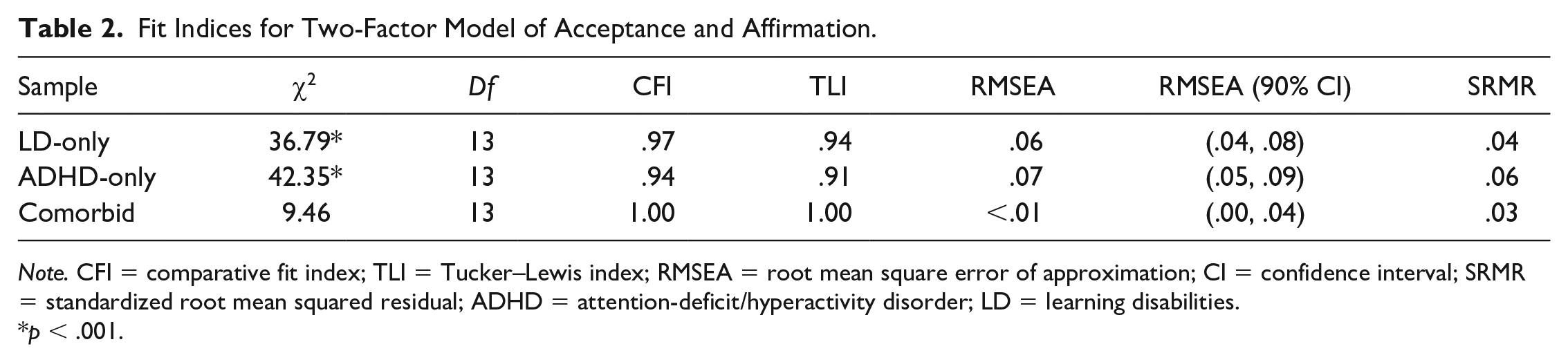
Note. CFI = comparative fit index; TLI = Tucker–Lewis index; RMSEA = root mean square error of approximation; CI = confidence interval; SRMR = standardized root mean squared residual; ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
p < .001.
Descriptive Statistics
Table 3 displays statistics on skewness and kurtosis as well as means and standard deviations for scales used in regression analyses. Participant scale scores were generally normally distributed. Internal consistency estimates on all scale scores ranged from modest to good based on parameters by Pallant (2001). Table 4 displays intercorrelations among scales used in regression analyses.
Descriptive Statistics for Subscales Used in Regression Analyses.
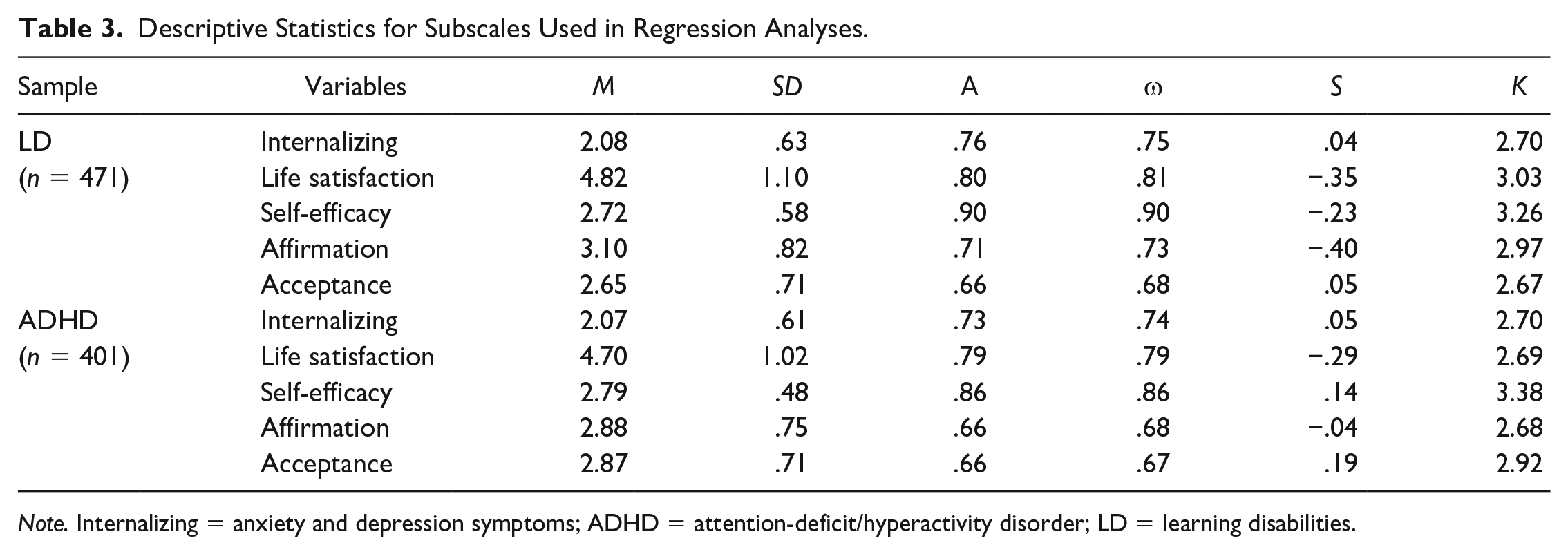
Note. Internalizing = anxiety and depression symptoms; ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
Correlations Among Scales Used in Regression Analyses.
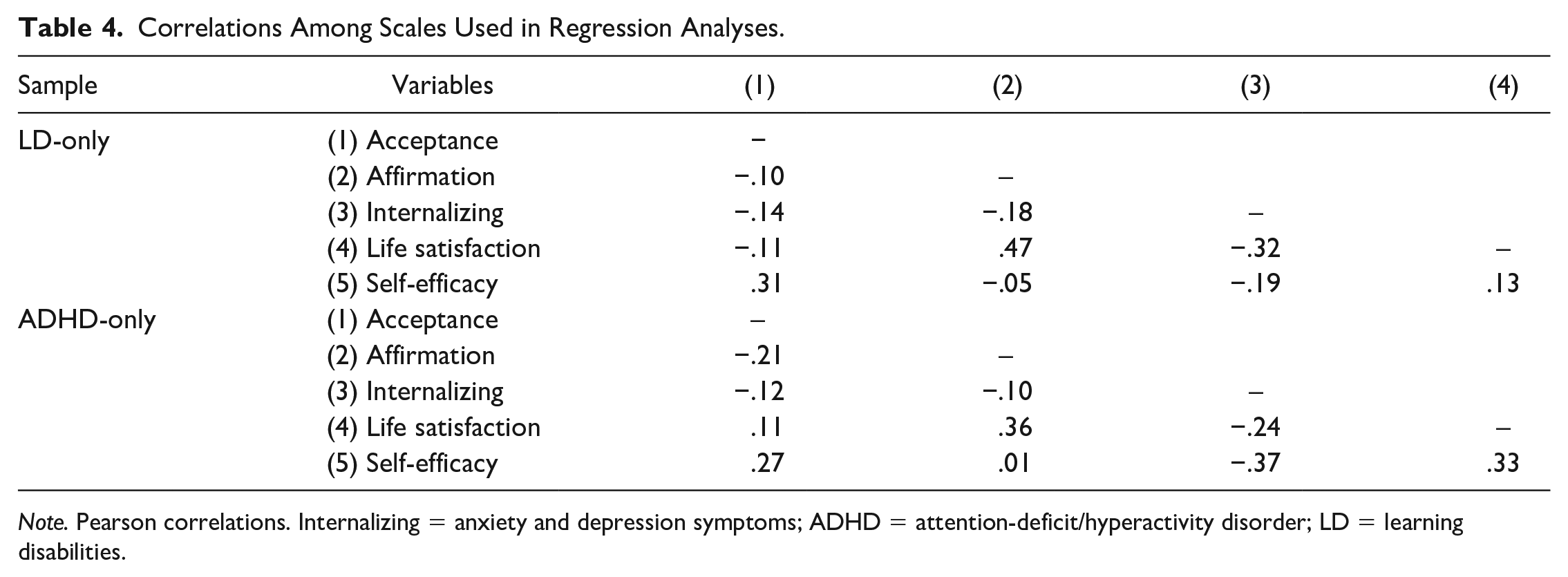
Note. Pearson correlations. Internalizing = anxiety and depression symptoms; ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
Regression Analyses
Each of the three psychosocial outcome variables was included in regression analyses with both the LD-only sample and the ADHD-only sample. Scores on each psychosocial outcome were regressed on disability acceptance, disability affirmation, and the demographic and disability-related variables. To control for Type I error, the Bonferroni adjustment was calculated, yielding a critical alpha of .004.
Anxiety/Depression
Results regarding anxiety/depression are presented in Table 5. Among participants who had only LD, the negative association between disability affirmation and anxiety/depression was statistically significant but the beta coefficient was low (Ferguson, 2009). The model accounted for 2% of the variance in anxiety/depression scores, a small effect (Ferguson, 2009). Among participants who had only ADHD, satisfaction with services meaningfully predicted lower anxiety/depression. The model accounted for 13% of the variance in anxiety/depression scores, which is a meaningful effect (Ferguson, 2009).
Multiple Regression on Anxiety and Depression.
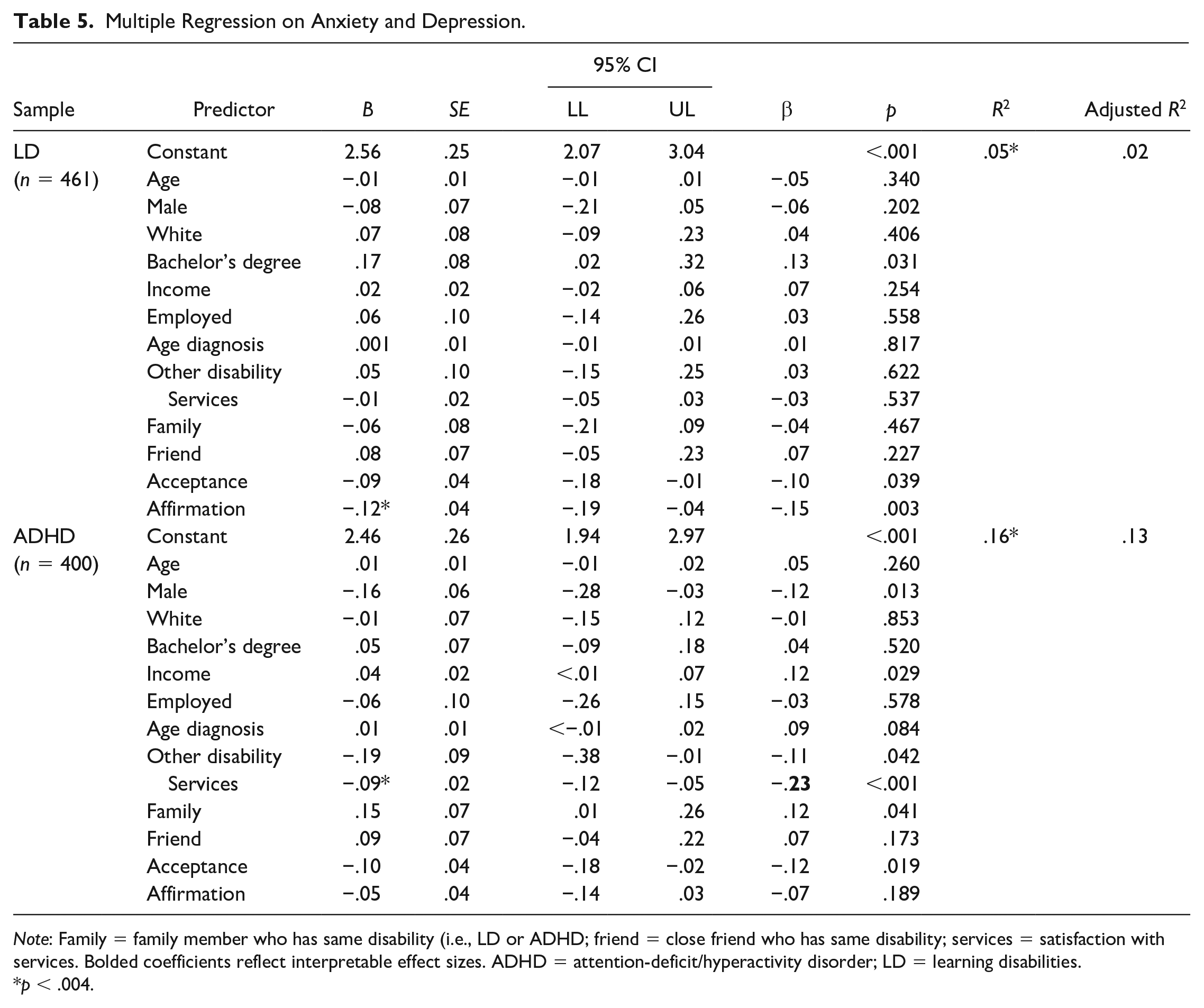
Note: Family = family member who has same disability (i.e., LD or ADHD; friend = close friend who has same disability; services = satisfaction with services. Bolded coefficients reflect interpretable effect sizes. ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
p < .004.
Life Satisfaction
Results regarding life satisfaction are presented in Table 6. Among participants who had only LD, life satisfaction was significantly predicted by disability affirmation and later age at diagnosis, with interpretable betas (Ferguson, 2009). The negative association with disability acceptance was not significant. The model accounted for 24% of the variance in life satisfaction scores, a moderate effect. Among participants who had only ADHD, higher life satisfaction was significantly predicted by disability affirmation, disability acceptance, satisfaction with services, male gender, and being non-White, although only disability affirmation had meaningful associations with life satisfaction. The model accounted for 26% of the variance in life satisfaction scores, a moderate effect.
Multiple Regression on Life Satisfaction.
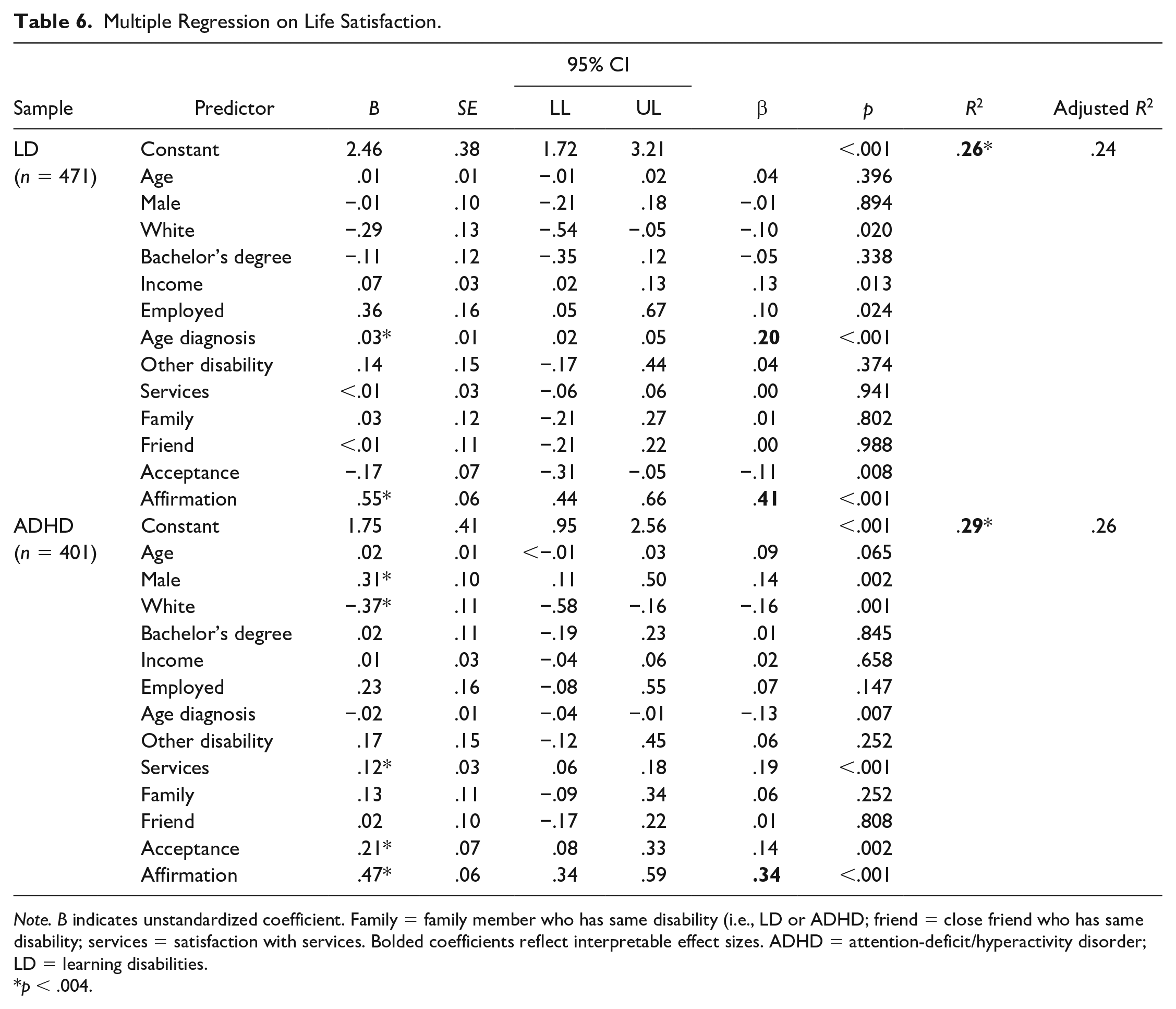
Note. B indicates unstandardized coefficient. Family = family member who has same disability (i.e., LD or ADHD; friend = close friend who has same disability; services = satisfaction with services. Bolded coefficients reflect interpretable effect sizes. ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
p < .004.
General Self-Efficacy
Results regarding general self-efficacy are presented in Table 7. Among participants who had only LD, higher general self-efficacy was significantly predicted by disability acceptance, satisfaction with services, and older age, although the betas for disability acceptance and age were small. The model accounted for 32% of the variance in general self-efficacy scores, a moderate effect. Among participants who had only ADHD, higher general self-efficacy was significantly predicted by disability acceptance, satisfaction with services, and being non-White, again with low betas for disability acceptance as well as being non-White. The model accounted for 27% of the variance in general self-efficacy scores, a moderate effect.
Multiple Regression on General Self-Efficacy.
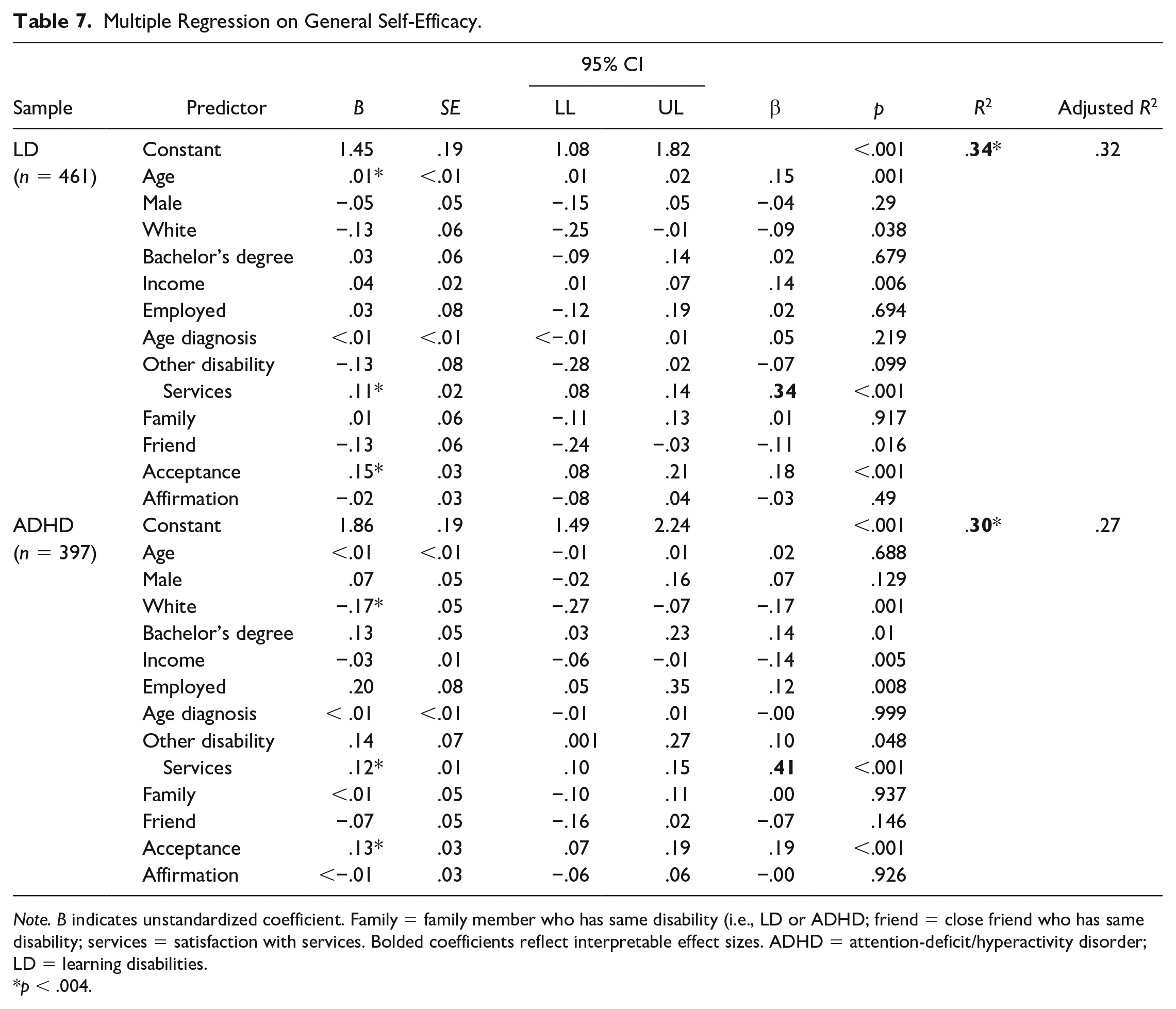
Note. B indicates unstandardized coefficient. Family = family member who has same disability (i.e., LD or ADHD; friend = close friend who has same disability; services = satisfaction with services. Bolded coefficients reflect interpretable effect sizes. ADHD = attention-deficit/hyperactivity disorder; LD = learning disabilities.
p < .004.
Discussion
In this study, we examined the internal consistency and structural validity of disability affirmation and disability acceptance scores in samples of adults with ADHD, LD, and both ADHD and LD. The scores were psychometrically sound in the ADHD and LD samples but not in the sample with comorbid disabilities. Satisfaction with services predicted lower anxiety/depression for adults with ADHD and higher self-efficacy for adults with LD and adults with ADHD. Disability affirmation predicted higher life satisfaction for individuals with LD and with ADHD, and being diagnosed at a later age also predicted higher life satisfaction for individuals with LD. The present study contributes to the emerging literature on psychosocial correlates of positive disability identity by generally replicating prior findings in two samples of adults with neurodevelopmental disabilities.
Disability Acceptance and Affirmation
Disability affirmation was a meaningful predictor of life satisfaction in both samples. Although disability acceptance was a significant predictor of general self-efficacy in both samples and a significant predictor of life satisfaction in the ADHD-only sample, the effect sizes of these associations were low. These findings support the conceptualization of PDI as consisting of diverse attitudes toward having disability which may warrant separate consideration in the literature. These findings further suggest that disability identity constructs, particularly disability affirmation, have relevance to two neurodevelopmental disability communities commonly served within educational settings.
Professionals working with adults with LD or ADHD may benefit from recent scholarship on disability-affirmative therapeutic approaches (Olkin, 2017), cultural competence in service provision—so-called disability-humility (Andrews, 2019), how practitioners can serve as disability allies to clients with disabilities, and how practitioners should individualize facilitated exploration of disability identity based on client readiness (Forber-Pratt et al., 2019). PDI has yet to be explored in younger disability populations. Pending replication in child and adolescent samples, these findings suggest that such fields as special education and school psychology may also benefit from recent scholarship on disability identity development among children and adolescents (DeMatthews & Mueller, 2022; Forber-Pratt et al., 2021; Mueller, 2021). The emergence of research on disability identity, which includes such constructs as acceptance and affirmation, parallels the rise of the neurodiversity movement (see Shmulsky et al., 2021). The neurodiversity framework conceptualizes autism and, more recently, other disabilities in social terms of human rights and identities to accept rather than in medical terms, as deficits and symptoms to cure (Kapp, 2020). The neurodiversity framework has also been extended to people with ADHD and LD (Armstrong, 2015) as well as to people with hidden, or nonvisible, disabilities (Shmulsky et al., 2021). Thus, the findings regarding disability identity may have relevant implications for the neurodiversity movement.
Comorbidity and PDI Measurement
Results from CFA and internal consistency estimates did not support the use of the PDI scales among adults with comorbid LD and ADHD. Participants in this subsample had sociodemographic differences from ADHD-only and LD-only subsamples that may have explained or contributed to this finding (see Table 1). Most notably, participants with comorbid ADHD and LD were predominantly non-White (58%), whereas the LD and ADHD subsamples were over 70% White. Moreover, previous research on PDI constructs has been limited by majority White and European American samples (Zapata, 2020, 2021; see Forber-Pratt et al., 2017). In other words, research has yet to demonstrate the extent to which PDI measurement generalizes to non-White adults with disabilities. Citing research on disproportionality in the representation of Black students in special education, Annamma et al. (2013) argued for the importance of addressing the intersection of disability and race in research and intervention.
Other possible explanations for this finding are at the item- and construct level. For example, participants with comorbid ADHD and LD may have been less certain on how to respond to PDI items, which were worded in terms of a single disability. Participants may have alternated between frames of reference (e.g., remembering disability experiences attributed to one or the other diagnosis) or have otherwise been inconsistent in their responding as a result of their dual diagnosis. Beyond the item level, the PDI constructs themselves might not fully capture how—in the case of LD and ADHD—the experiences and significance of different disabilities are integrated or consolidated. Participants with this particular comorbidity may have been diagnosed at two different time points, with or without a difficult differential diagnosis experience, thus creating interaction or even interference between trajectories of disability adjustment and identity formation.
Learning disabilities and ADHD are also commonly co-occurring, and it may be harder to delineate the significance of one from the other, compared to people with less frequently co-occurring disabilities or different disability types (e.g., physical vs neurodevelopmental). It is also possible that, given the high frequency of co-occurrence, participants with comorbid LD and ADHD may constitute a distinct disability community, with some degree of shared disability experience that does not fit current models of disability acceptance and affirmation. By exploring potential underlying mechanisms, emerging models of disability identity development have potential to inform present findings (see Forber-Pratt et al., 2017).
Other Correlates of Psychosocial Functioning
Satisfaction With Disability-Related Services
Satisfaction with services was meaningfully associated with general self-efficacy in both samples and with lower anxiety/depression in the ADHD subsample. This variable may represent tangible features of disability services, including quality of services and service delivery, but may also represent more psychological factors involved in the pursuit and receipt of disability services. Such experiences may include decisions regarding disclosure and self-advocacy on the part of the consumer and may involve the navigation of ableism and discrimination. Present findings indicate that participants with an overall more positively perceived experience with disability-related services also reported higher self-efficacy, which has been theorized as an important factor in coping with disability-specific challenges and demands (Cramm et al., 2013). People with high self-efficacy exert more effort and persist longer on goal-directed actions than do those with low self-efficacy (Bandura, 1999), and they have quicker recovery and are more likely to maintain goal commitments in the face of setbacks (Cramm et al., 2013).
Age at Diagnosis
Later age at diagnosis predicted life satisfaction in adult LD. Receiving a dyslexia diagnosis has been found to be experienced as both a positive reframing of past events and as a potential counter-narrative to behavioral misattributions (see Armstrong & Humphrey, 2009). A hypothesis for future investigation, perhaps participants who were diagnosed later were able to experience diagnosis as a positive reframing of previous events. For example, a later LD diagnosis could signal that academic difficulties were due to specific and remediable challenges rather than to negatively perceived traits such as laziness. Limiting interpretability of findings, it is also plausible that individuals with more severe or inhibiting LD were diagnosed earlier.
Limitations
Several study limitations are worthy of discussion. Limiting the generalizability of findings, LD and ADHD are highly co-occurring conditions (DuPaul et al., 2009), and participants with comorbid ADHD and LD were not represented in regression analyses due to concerns with the measurement of the identity constructs in this group. Second, we did not account for severity of disability or level of functional impairment, considerations which may partially explain findings regarding such variables as age at diagnosis. Third, the internal reliability of the PDI subscales was not as high as in other samples of adults with predominantly physical disabilities (Zapata, 2018, 2020). Although analyses supported the structural validity and internal consistency of the PDI subscales in the present sample, there may be conceptual differences regarding disability identity attitudes that are unaccounted for by current measurement of disability acceptance and affirmation.
Fourth, as evidenced by the small proportion of variance in anxiety/depression scores explained by the regression model, more comprehensive prediction models are needed to fully understand the correlates of internalizing symptoms in adult LD. Fifth, limiting the interpretability of findings, satisfaction with services was measured using a single item representing an overall feeling of satisfaction with all disability-related services received, currently and historically. Sixth, participants were recruited over social media platforms through groups related to LD and ADHD; thus, the sample represents adults with computer literacy who previously sought disability-specific information or social connectedness and the findings may not generalize to the general population of adult LD and ADHD. Relatedly, the fact that participants self-identified as having LD, ADHD, or both, is an additional limitation. Future studies will be needed in which diagnostic categories are confirmed independent of the participants.
Future Research
We recommend that researchers continue to investigate variables that yielded significant associations but low effect sizes. General self-efficacy was predicted by older age among participants with only LD and by being non-White among those with only ADHD. In contrast to present findings regarding adults with ADHD, previous research has found that, in the general population, White people have higher general self-efficacy, as explained by socioeconomic factors (i.e., education and income; Assari, 2017). Future research using more comprehensive prediction models is necessary for further interpretation. Scholars have proposed that more promising explanations of the association between risk and protective factors and LD or ADHD should depend on compounding multiple factors as well as interactive relationships between risk factors and environmental context (see Beauchaine & Hinshaw, 2017; Morrison & Cosden, 1997).
Conclusion
The present findings suggest that disability identity constructs have relevance to two neurodevelopmental disability communities commonly served within educational settings, adults with LD and those with ADHD. Consistent with research findings from samples of adults with predominantly physical disabilities, disability acceptance, and affirmation were differentially related to psychosocial outcome variables. Taken together, these findings contribute to the literature which theorizes that positive disability identity may protect against the negative psychosocial ramifications of disability-related life stressors (see Forber-Pratt et al., 2017). The present results also support previous findings that PDI consists of diverse attitudes with unique relationships to areas of psychosocial functioning (Hahn & Belt, 2004; Zapata, 2018, 2020, 2021). Developing interventions to cultivate positive disability identity should not, based on present and recent research, follow a one-size-fits-all prescriptive approach (Forber-Pratt et al., 2019; Olkin, 2017). Additionally, analyses of PDI scores from adults with comorbid LD and ADHD, who were majority non-White, did not support current measurement of disability acceptance and affirmation. Current conceptualizations and measures of PDI may not capture the disability experiences and attitudes of adults with both LD and ADHD.
Footnotes
Correction (August 2023):
The article has been updated to correct the following sentence to include ‘from less than $10,000 to $140,000 or’ in the following sentence: Participants reported household income as one of nine ordinal categories ranging from less than $10,000 to $140,000 or more and increasing in increments of $10,000 up to $100,00, and then in increments $20,000 per year (see Table 1).
Authors’ Note
This study was not preregistered and the data set analyzed is not publicly available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by a grant from the Schwab Dyslexia and Cognitive Diversity Center.