
Abstract
Theories of dialogism suggest that dialogical relationships may drive therapeutic change with people diagnosed with psychosis, yet how this occurs in practice remains unclear. This study examines the emergence of dialogical engagement in a psychotherapy session with a person experiencing psychosis and how his expressions shift over the course of the session. A single 45-min session was descriptively analyzed using Conversation Analysis-informed case analysis. A young adult male referred to as Jack presented with experiences interpreted as paranoid ideation, low treatment engagement, and limited response to medication. Dialogical and monological sequences were identified through turn-by-turn analysis, focusing on the therapist's stance, interactional flow, and Jack’s responses. Topic development and epistemic positioning were central analytic foci. Dialogical engagement was fostered through open-ended questions, reflective responses, repetition, and emotional attunement—supporting meaning-making and reflective positioning without pathologizing Jack’s beliefs. Moments of rupture following directive therapist moves required active realignment. Although Jack initially expressed a desire to discontinue therapy, he reported emotional relief and openness to continue. Despite limited polyphony in a one-on-one session, the findings suggest that interactional practices promoting dialogue may still support collaboration and meaningful engagement with people diagnosed with psychosis, while also generating themes relevant for more conventional psychotherapy.
Introduction
Psychosis refers to a mental state marked by distorted perceptions of reality, including hallucinations, delusions, and disorganized thinking. Historically, such experiences have been viewed as incompatible with insight-oriented psychotherapy, leading to a reliance on pharmacological interventions (Alanen, 2009; Maj et al., 2021). Although neuroleptic medications can reduce the intensity of experiences diagnosable as psychotic, long-term outcomes often remain unsatisfactory, with persistent distress, social withdrawal, and limited engagement in treatment (Maj et al., 2021).
In recent decades, the belief that psychosis is untreatable through psychotherapeutic approaches has been challenged from multiple directions. One trajectory involves the substantial volume of research on cognitive behavioral therapy for psychosis (CBTp) (Bighelli et al., 2018), which focuses on collaborative problem conceptualization, examination of unhelpful mental and behavioral patterns, and developing more adaptive coping strategies (Bighelli et al., 2018; Morrison & Wood, 2023). Another development comes from family therapy (Heatherington & Johnson, 2019) and humanistic approaches (Alanen, 2009), advocating for relational and context-sensitive care.
The Open Dialogue (OD) approach is one example of the latter trajectory. Gradually developed in Keropudas hospital in Finnish Western Lapland during the 1980s and 1990s, OD emerged as a social network-oriented approach that prioritizes immediate response, minimal diagnostic gatekeeping, and continuity of care (Seikkula et al., 2011). In OD, therapists adopt a non-expert stance, attending closely to service users’ language and meanings through open-ended or circular questions that explore how individuals perceive and relate to each other’s thoughts, feelings, and behaviors. They also use reflective responses that mirror or paraphrase what has been said. Rather than aiming to correct or reframe experiences, OD emphasizes the co-construction of shared understanding, which can be used to tailor treatment in a case-by-case manner.
Despite some shared features with CBTp—such as a normalizing stance, collaborative engagement, and curiosity toward unusual experiences (Menon et al., 2017)—OD diverges in its therapeutic philosophy and practice. Unlike CBTp, OD avoids structured techniques and theory-driven interpretations, including the educational focus on conceptualization of psychological mechanisms of psychosis. Instead, dialogue itself becomes the principal therapeutic tool, with therapists attuning to the service user’s and their social network members lead (Seikkula, 2011). Regardless of the session’s composition, the therapist’s core task is to engage with the themes introduced by participants, listen actively, reflect openly, and help co-create a dialogical space for something new to emerge (Arnkil, 2019).
OD is associated with improved social functioning and reduced service use compared to standard care (Bergström et al., 2018; Bouchery et al., 2019). Initially understood through a social constructionist lens, where change arises from co-created meanings (Seikkula & Olson, 2003), OD now increasingly draws on embodied and intersubjective understanding of change. Within this framework, therapeutic change can be understood to emerge through the experience of being genuinely heard and responded to in dialogue, enabling the re-establishment of dialogical relationships and the restoration of participants’ sense of agency (Seikkula, 2011).
Despite compelling theoretical accounts, it remains unclear whether and how dialogism itself functions as a mechanism of therapeutic change in the treatment of psychosis—particularly in one-on-one encounters, which are common in clinical practice, as service users diagnosed with psychosis may decline the involvement of their social networks. This study addresses that gap by analyzing how experiences interpreted as psychosis are discussed within a psychotherapy session with a young adult who has low engagement in standard treatment and has declined the participation of his family members. The study explores the real-time dynamics of therapeutic interaction, focusing on how dialogical moments are initiated, sustained, or disrupted. Special attention is given to the therapist’s use of open-ended questions, reflective listening, and a non-knowing stance, and how these practices contribute to the person’s narration of experiences commonly framed as psychotic.
Methods
Case
The data for this study comes from a single psychotherapy session at the beginning of treatment for a person referred to as Jack. Jack is a male under the age of 30 who experienced a first-episode psychosis approximately year prior to the session. He developed a fixed belief that a former friend intended to harm him, despite not having seen this person in years. He began hearing the person’s voice making derogatory comments and believed the person could observe him remotely.
Shortly before hospitalization, Jack believed he had been drugged by this person, leading him to think he had harmed an acquaintance—an event which the alleged victim has firmly denied. Jack had a history of substance use, and the incident, along with associated memories, was interpreted as a drug-induced psychosis. Over time, he developed further paranoid ideation, believing his friends and family were conspiring against him and that their denials were meant to confuse or manipulate him due to what he believed he had done.
Jack has received ongoing outpatient care and periodic hospitalizations with a provisional diagnosis of unspecified non-affective psychosis. His “insight of illness” has consistently been assessed as poor, and he does not believe he has a psychosis. While he has been prescribed multiple neuroleptics, his response has been minimal. During the most recent hospitalization, suspicion of a schizophrenia-spectrum disorder emerged, with the decision to reassess it during longer follow-up.
Despite regular psychoeducation on psychosis and substance use, it was concluded that Jack’s insight and engagement have not improved. As a result, he was referred to a psychologist for therapy and further assessment. The psychologist (author) had met Jack a few times previously, both individually and with the treatment team, but formal psychotherapy-process had not started due to Jack’s recent hospitalization. The session analyzed here is the first one post-discharge and focused on exploring Jack’s views on how treatment should continue.
Jack’s psychotherapy was one of the psychologist’s integrative training psychotherapies. At the time of the session, the therapist had completed over three years of formal integrative psychotherapy training, which emphasizes common therapeutic factors and adapts elements from various models. In addition, he previously accumulated over a decade of clinical experience in psychosis treatment within OD-based services, working as a licensed clinical psychologist at Keropudas hospital.
Analysis
The analyzed session was a 45-min individual psychotherapy meeting that was video-recorded and transcribed verbatim. For the purposes of reporting, relevant transcript extracts were translated from Finnish into English. Extracts followed simplified conventions for clarity, including speaker labels (T for therapist, P for patient) and narrative descriptions of notable paralinguistic features when relevant.
Given that the study is based on a single session with one participant, the analytic approach was primarily descriptive and exploratory, with the aim of remaining close to the empirical material and tracing how interactional sequences unfolded over the course of the meeting.
First, dialogical and monological segments were identified using adapted criteria from the OD Adherence Scale (Lotmore et al., 2023). Dialogical sequences referred to moments where the therapist engaged with Jack’s themes through reflective listening, repetition, and open or circular questioning, maintaining a collaborative stance without imposing new themes. Monological segments involved therapist-led shifts, such as information-seeking questioning, introducing new themes or interpretations, and moving the interaction in a more directive direction.
The analysis of sequences was then informed by Conversation Analysis (CA), a qualitative method focused on the structure of spoken interaction (Peräkylä, 2019). The analysis focused to turn design, sequential organization, topic development, and epistemic positioning (i.e., who is treated as knowing what), in order to examine how dialogical engagement was interactionally accomplished, disrupted, and re-established over the course of the session.
Note that, given the exploratory and descriptive nature of the single-case design, the analysis did not follow a strict inductive CA approach. Instead, dialogical concepts were used heuristically as sensitizing tools to orient analytic attention to shifts between more dialogical and more monological interactional modes. These concepts did not function as a separate coding scheme, but as a descriptive vocabulary for organizing the findings.
Reliability of analysis was supported through consultation with a supervision group, including three psychotherapy trainees and a supervisor. The group reviewed the session recording after being informed of the study’s aims and shared open reflections, independent of the author’s interpretations.
Ethical Considerations
Prior to the session, Jack provided signed, informed consent for the psychotherapy sessions to be recorded for training supervision. He also consented to the use of material from the recordings in an author’s integrative psychotherapy training thesis and in scientific journal publications. Before the session, the Chair and Secretary of the Ethics Committee of the University of Jyväskylä reviewed the study plan and concluded that it did not require ethical review under the guidelines of the Finnish Advisory Board on Research Integrity (TENK) (Statement on the need for an ethical review: 583/13.00.04.00/2025). Jack has read the manuscript and was given the opportunity to comment on it, request changes, or decline its publication. After reading and commenting on the manuscript, written informed consent for publication was obtained from Jack.
Results
At the beginning of the session, Jack states that he has decided to discontinue his psychiatric treatment. He explains that this has been his intention for some time and adds that his family has also expressed disappointment, feeling that the treatment has not provided the hoped-for support. The therapist responds with a circular question, inviting Jack to reflect on what kind of help he thinks his family was expecting (Extract 1, line 1).
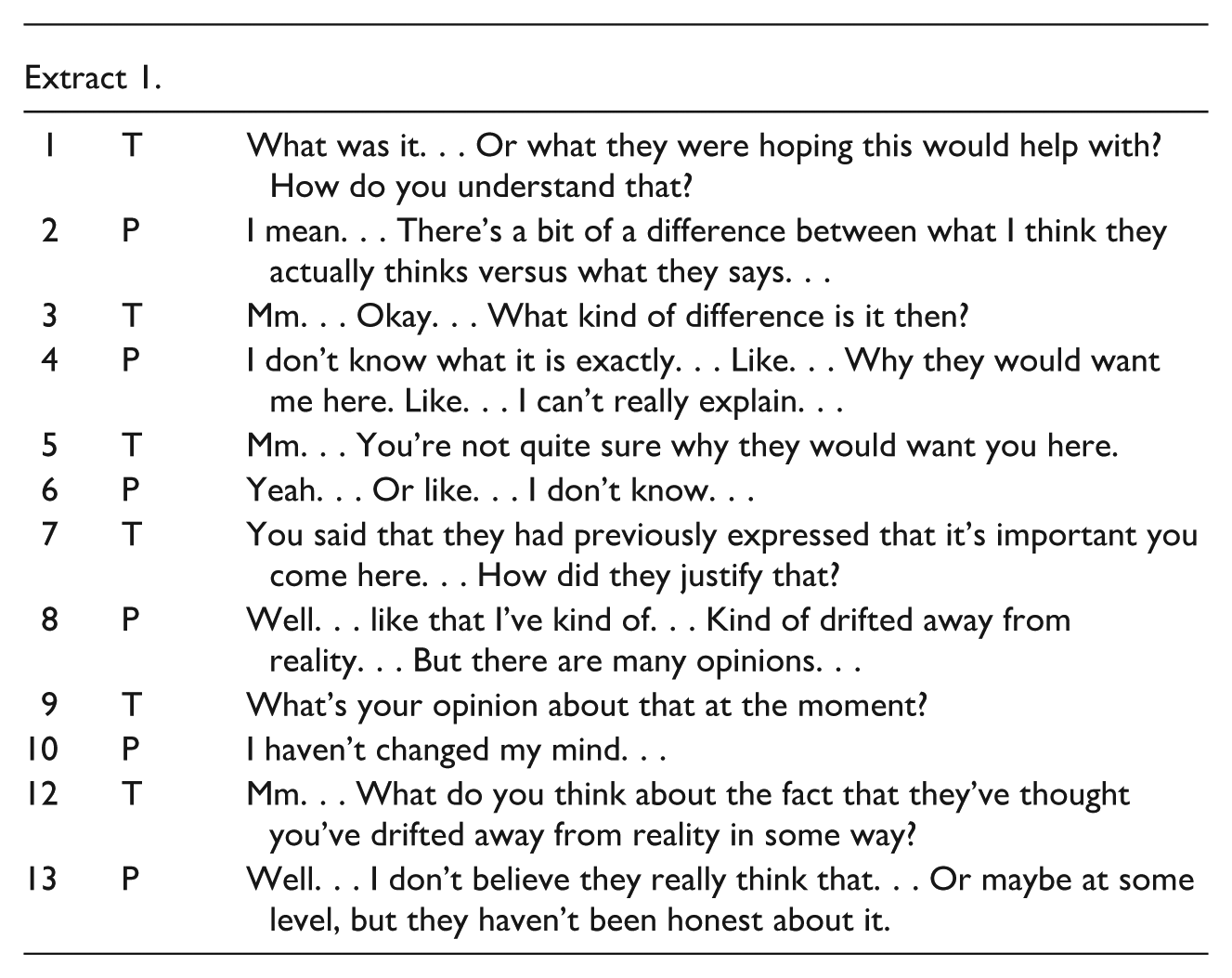
The circular question initiates the first dialogical sequence of the session. Jack’s initial response can be seen as reflecting a thought pattern that has been interpreted as psychotic: he expresses doubts about his family’s true motives and sincerity, which also makes the question difficult for him to answer directly (Extract 1, line 2 and 13).
The therapist responds to this hesitation by repeating Jack’s wording (Extract 1, line 5) and by continuing with open and circular questions (Extract 1, line 7). This interactional strategy begins to encourage Jack to share more about his experiences. For instance, he reports that it has been emotionally distressing not to be able to trust his loved ones, and explains how this affects his daily life. In addition, he says that his own actions have also contributed to his distress.
The therapist then asks for clarification on what Jack means by this, and Jack begins to speak more explicitly about his personal experiences, as shown in extract 2.
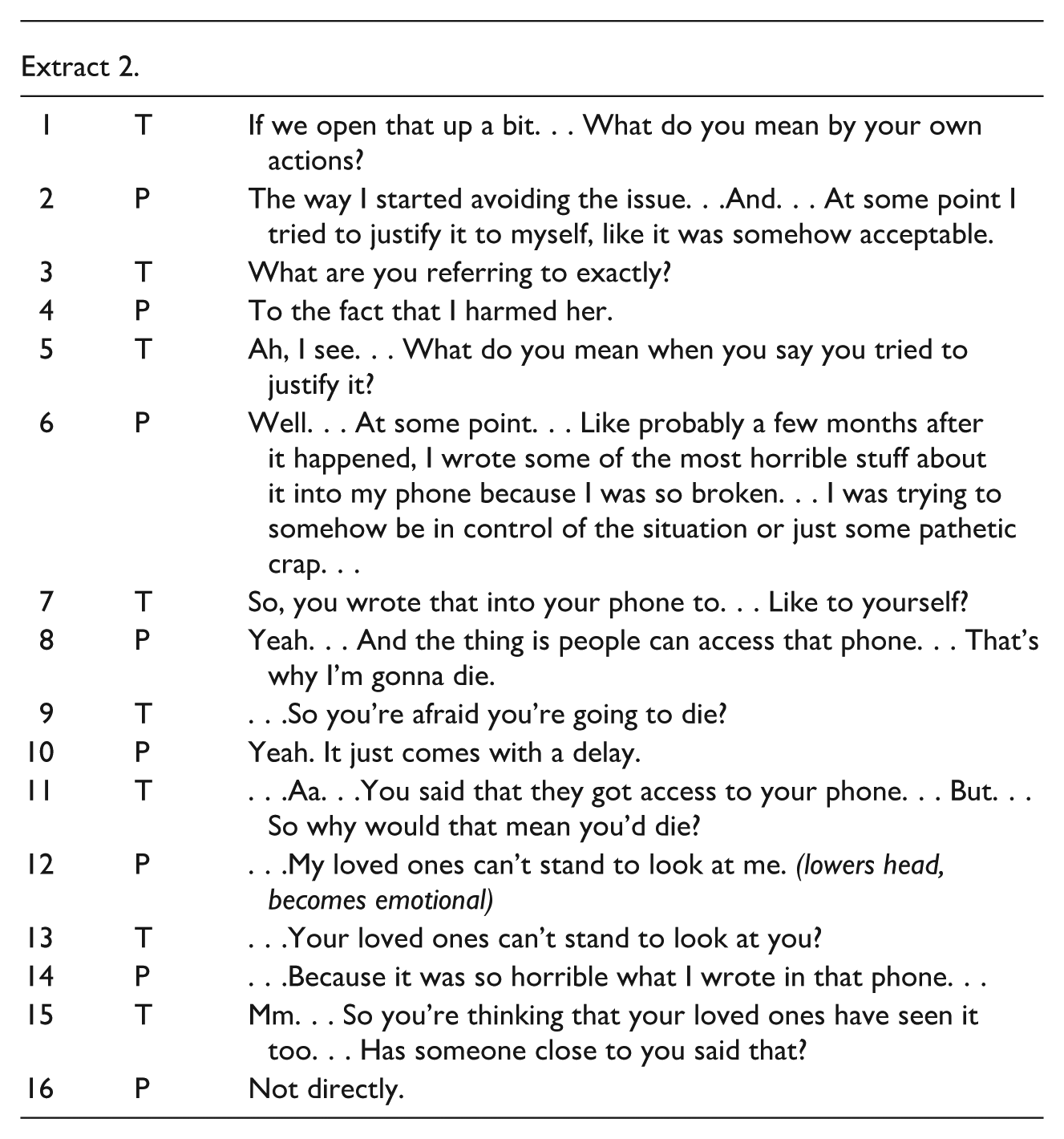
The therapist continues to repeat and reflect upon Jack’s utterances while attempting to further clarify his experiences. Throughout this exchange, the therapist maintains a not-knowing stance, allowing Jack to define the meaning of his experiences in his own terms. When Jack’s talk contains content that might be interpreted clinically as delusional, the therapist does not pathologize or impose a diagnostic frame. Instead, the therapist formulates questions inviting elaboration (Extract 2, line 5).
This approach enables Jack to expand on his account (Extract 2, line 6). He begins to describe how he feels that his loved ones cannot bear to look at him because of what he wrote on his phone. At this point in the conversation, themes emerge that may be therapeutically significant—particularly those related to Jack’s sense of shame and self-worth. The therapist attempts to deepen the exploration of these themes. However, this effort momentarily results in a break in dialogical flow, as the therapist introduces an assumption that Jack is worried others have read what he wrote on his phone (Extract 3, line 1).
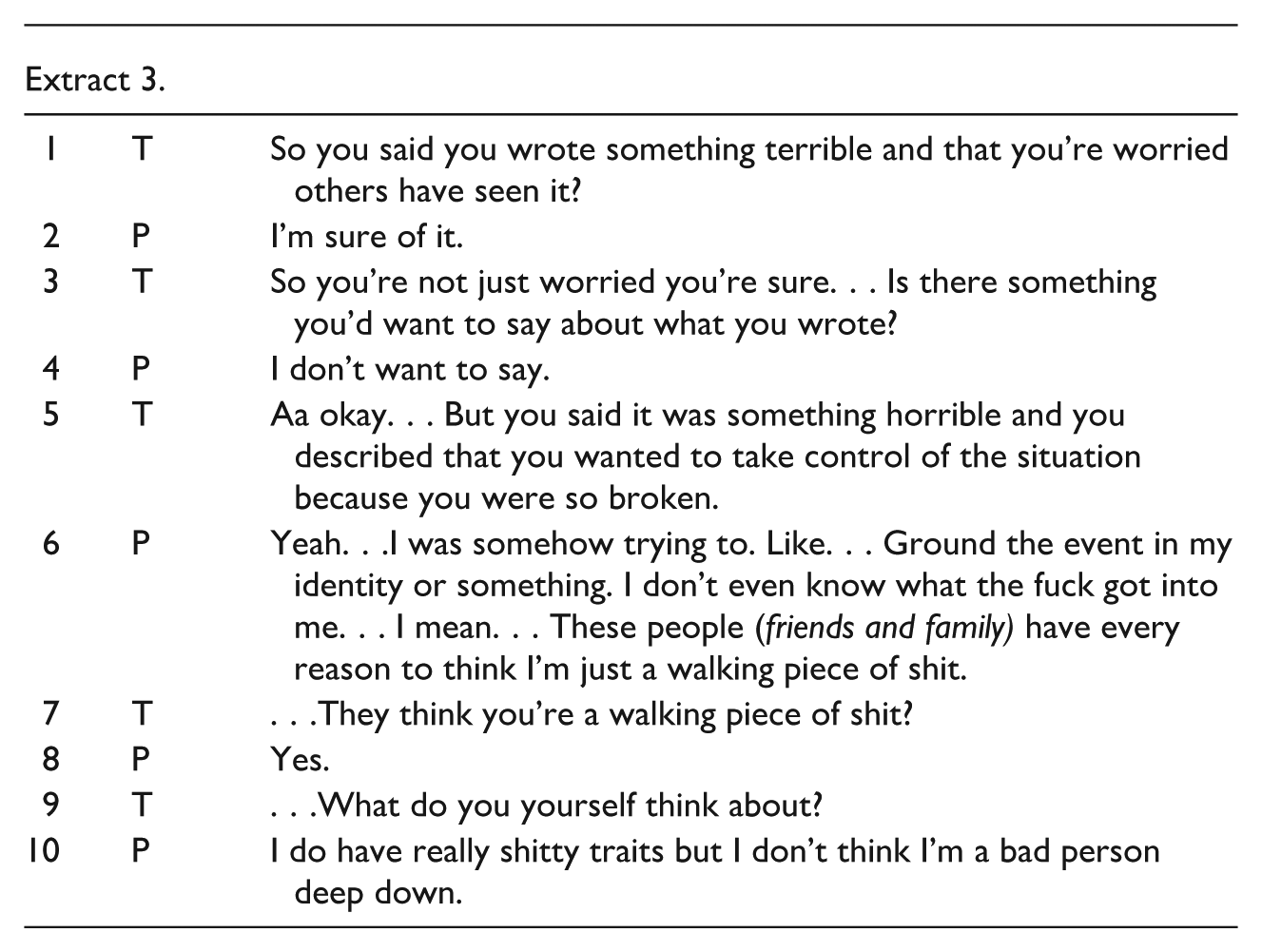
This assumption, while seemingly minor, shifts the interaction from a not-knowing and open stance to a more interpretive and directive position, which is also shown how Jack correcting therapist by saying he is sure of it (Extract 3, line 2). Though the therapist reacts quickly, he continues with a fact-oriented question (Extract 3, line 3) which further sustains the non-dialogical moment. During this brief sequence, the interaction becomes more therapist-led, and Jack’s voice temporarily recedes.
The therapist then makes an effort to re-establish dialogical engagement by returning to a reflective and validating stance (Extract 3, line 5). By summarizing Jack’s earlier statement and checking his understanding, the therapist helps restore the conditions for mutual meaning-making. This formulation, rather than presenting a new interpretation, mirrors Jack’s own words and invites elaboration.
Jack responds by clarifying and deepening his account (Extract 3, line 6). He describes how he tried to integrate a difficult event into his identity, expressing strong self-judgment: that others likely perceive him as “a walking piece of shit.” The therapist reflects this back in a neutral tone and asks what Jack himself think about that. This turn opens space for a more reflective self-positioning. Jack acknowledges having “shitty traits” but also affirms that he does not view himself as fundamentally bad. The therapist attempts to deepen the conversation by asking which aspects of himself Jack dislikes. In response, Jack says he wishes he were braver—something that became evident in a situation where he heard demeaning voices in his apartment commenting on his actions. The therapist follows up by asking what the Jack would have wanted to do in that moment, and Jack replies that he would have wanted to confront them but did not dare to. The therapist then asks an open-ended question about what exactly he was afraid of (Extract 4, line 1), to which Jack responds that he feared physical violence with his former friend because the voices felt so threatening (Extract 4, line 2).
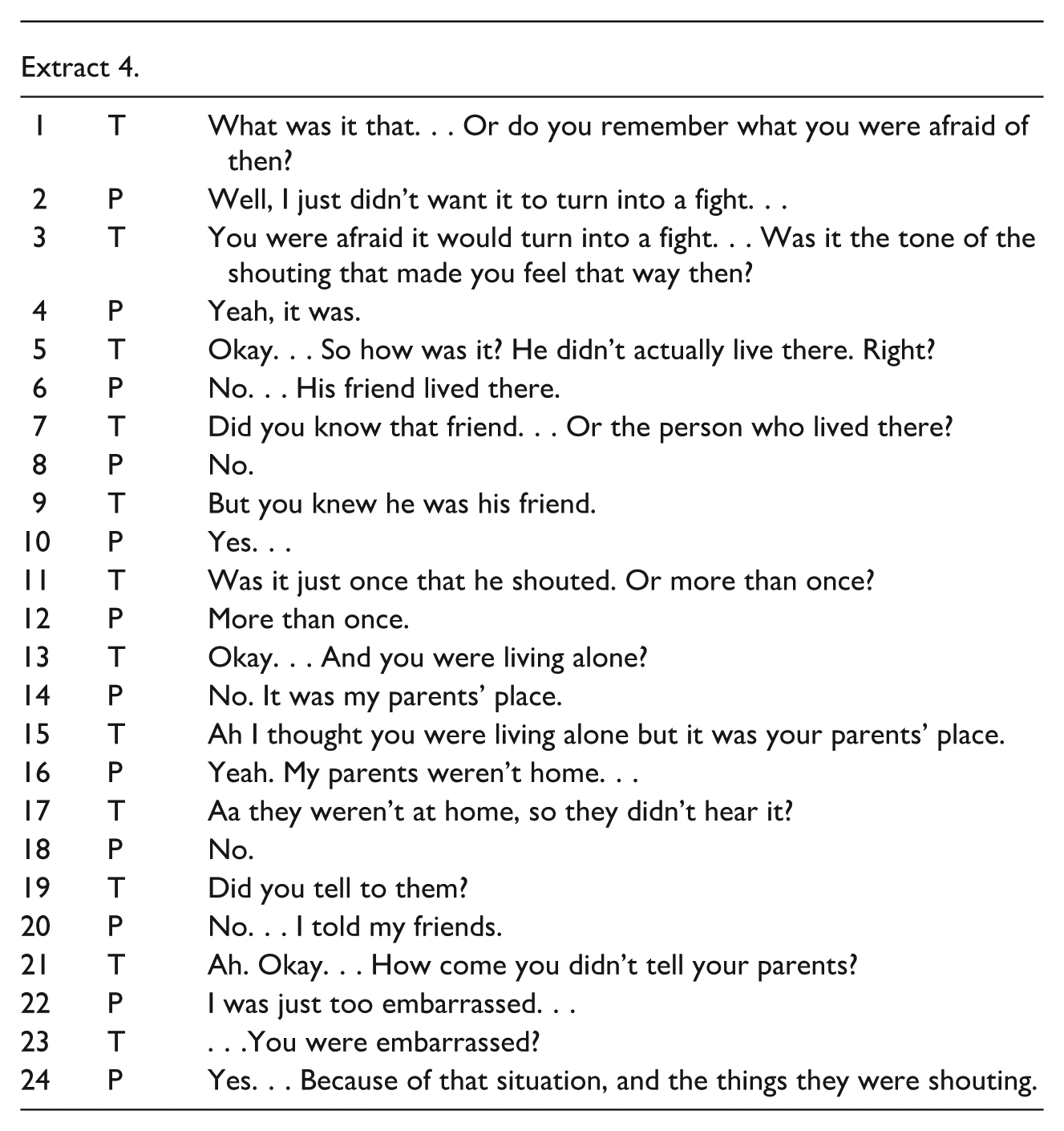
At this point, the dialogue shifts once again into a more monologic phase, as the therapist begins to focus more on clarifying Jack’s life situation at the time (Extract 4, line 5). This is evident in the way Jack’s responses become shorter (Extract 4, line 8), and the therapist starts to ask more closed-ended questions (Extract 4, line 9).
The dialogical flow gradually returns as the therapist transitions to more open-ended inquiries and adopts a more curious and wondering stance, which encourages Jack to start sharing more again as shown in extract 5.
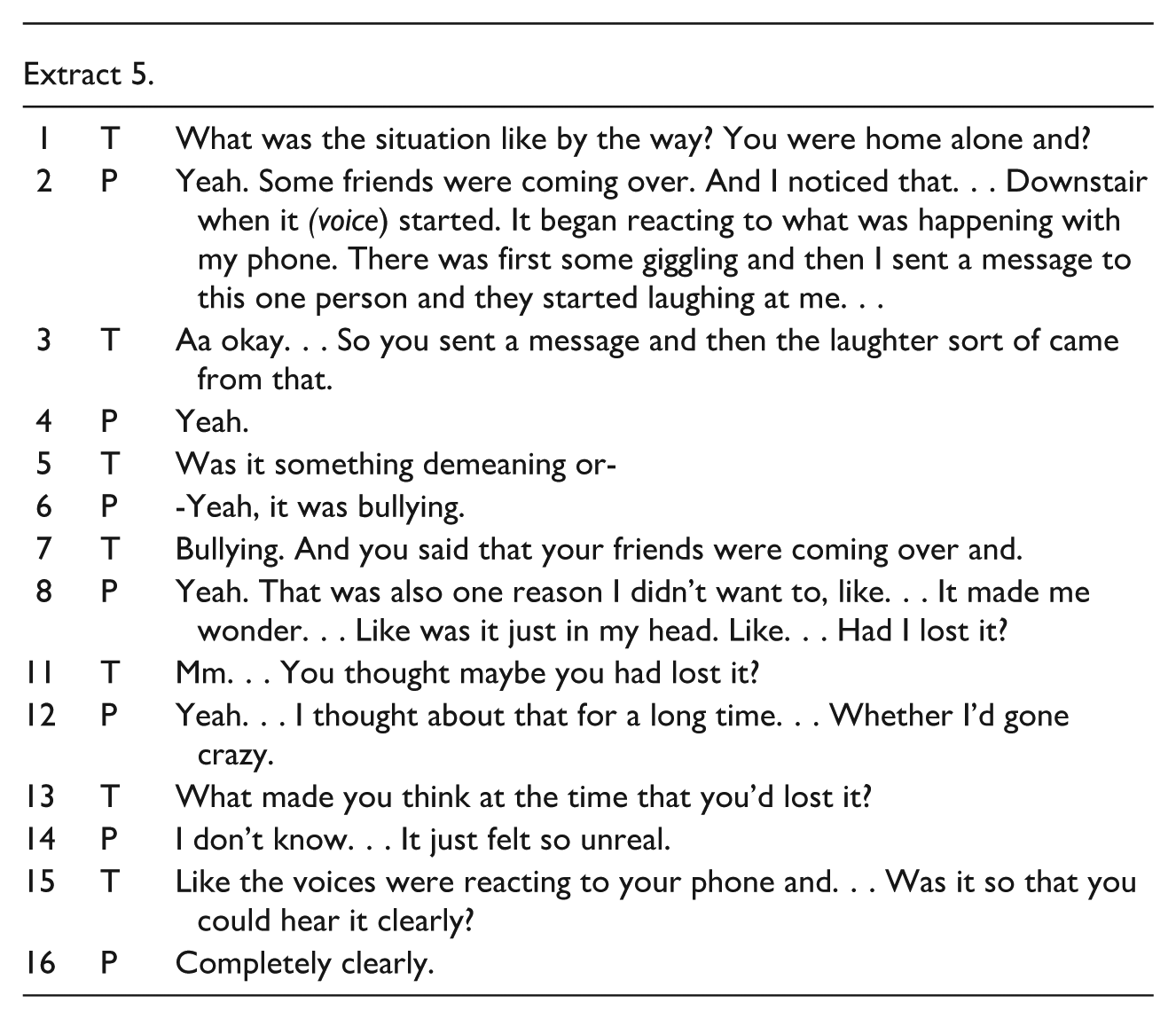
Following an extended period of sharing his experiences that were interpreted as psychotic, Jack begins to adopt a more reflective self-position. He recalls that he had, at the time, contemplated whether he might have “gone mad”, given how improbable the experiences felt (Extract 5, line 8). The therapist continues to support this emerging meta-perspective by offering open-ended follow-up questions (Extract 5, line 13). As a result, Jack starts to reconsider earlier assumptions—such as the belief that his family or friends intended harm—and begins to entertain the possibility that they simply did not know how to respond. He also starts to explore his experiences from different perspectives as illustrated in Extract 6.
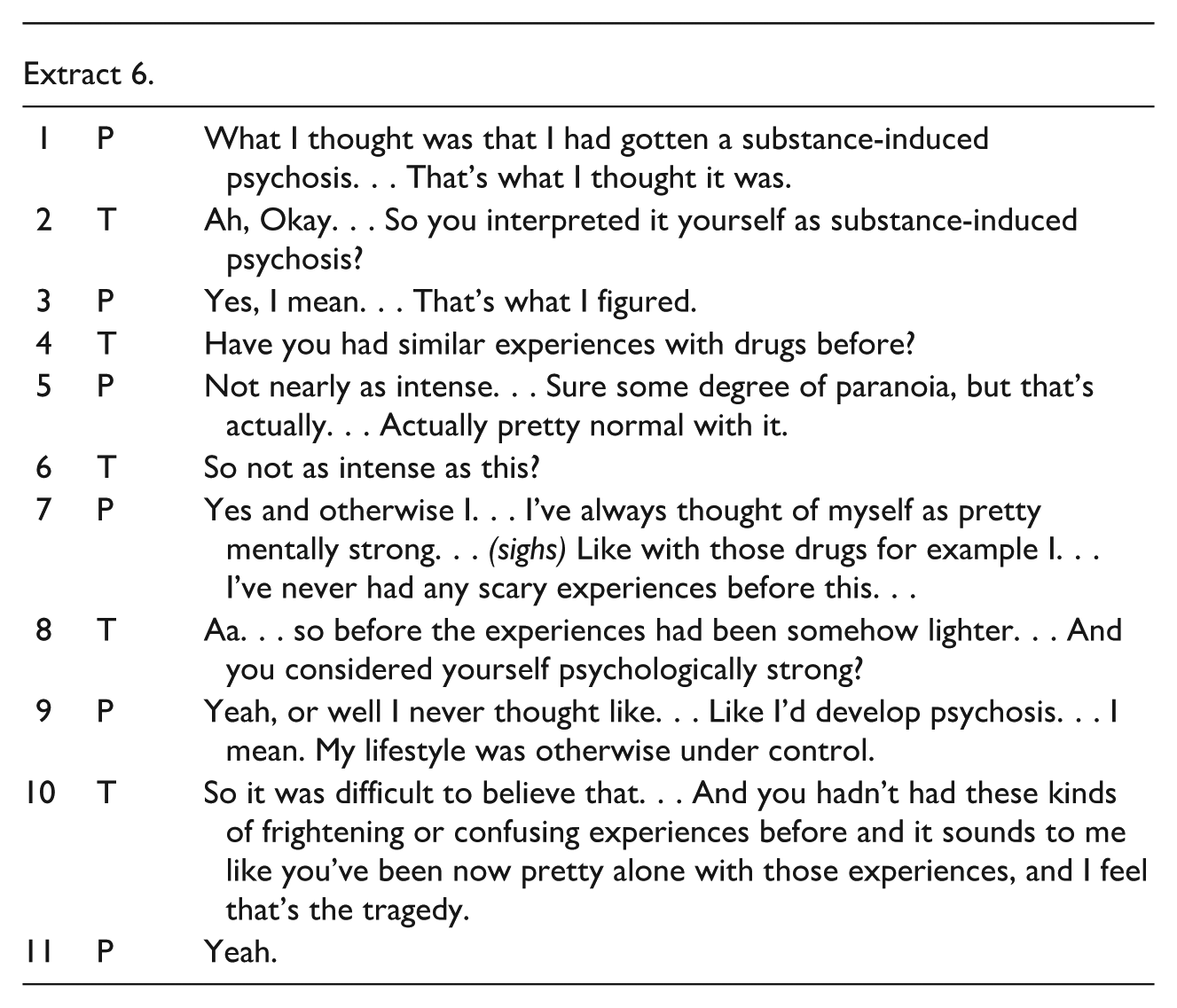
Whereas in earlier moments (e.g., Extracts 2–4), Jack narrated his experiences with high emotional immediacy and from a first-person, immersed perspective, here he begins to contextualize the episode within a broader explanatory framework (Extract 6, line 1).
The therapist does not challenge or confirm this, but instead follows Jack’s meaning-making by offering open, validating, and clarifying questions (Extract 6, lines 2 and 4). As the dialogue progresses, Jack contrasts this experience with previous, more familiar and less intense reactions to drugs (Extract 6, line 5), thereby positioning the current episode as qualitatively different.
In line 7, Jack introduces a narrative of psychological resilience, emphasizing his previous belief in being “mentally strong”, especially in the context of drug use. This introduces a rupture in self-narrative: the Jack who once trusted in his mental stability is now confronted with an experience that contradicts that belief. The therapist supports this reflective process by repeating Jack’s wording in line 8. Jack responds in a sad tone, saying he never thought he would develop psychosis, emphasizing the gap between his self-perception and current reality. Then the therapist offers an emotionally resonant reflection, emphasizing its subjective nature through the phrasing “it sounds to me”—a formulation that leaves space for Jack to disagree.
The therapist’s reflection highlights that the tragedy lies not only in the frightening nature of the experience itself, but also in the isolation in which it has unfolded (Extract 6, line 10). However, this reflection does not introduce a new thematic direction or increase polyphony of conversation (Extract 6, line 11). More generally, as illustrated also in the previous extracts, in the session under study the interaction tends to shift into an interview-like format rather than evolving into a polyphonic dialogue where multiple perspectives are openly explored. This may be attributed to both the one-on-one setting, therapist minimal use of reflections and Jack’s guarded stance at the beginning of treatment. Nevertheless, the emotional tone of the session became more relaxed toward the end, as shown in Extract 7.
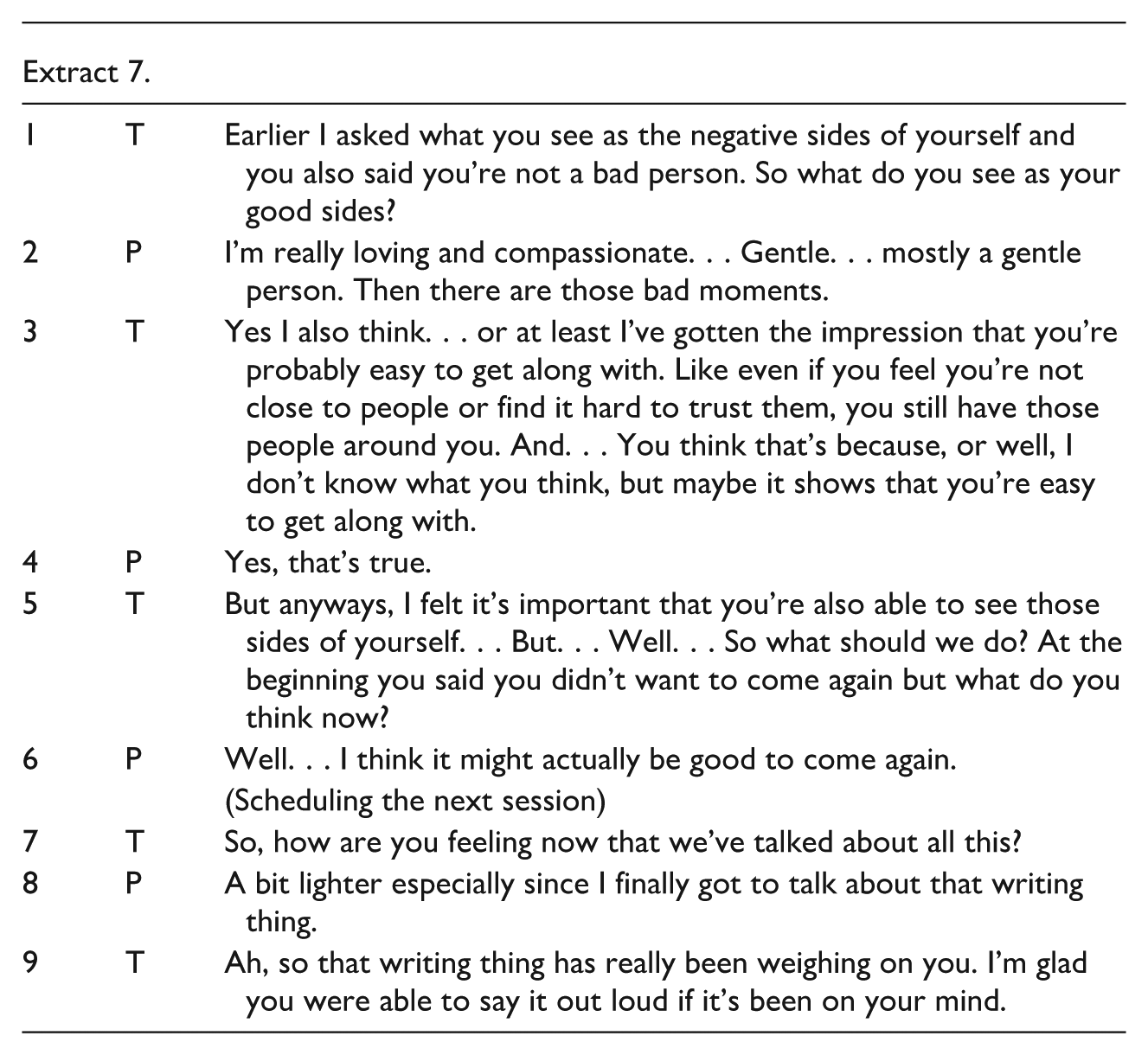
This closing sequence illustrates a moment of shared reflection. After previous segments focused on shame, fear, and isolation, the therapist now reorients Jack toward self-recognition by explicitly inviting positive self-assessment (Extract 7, Line 1). Jack responds with emotionally resonant descriptors which signal a reconnection to valued identity traits, even while acknowledging the presence of “bad moments.”
The therapist then introduces a relational reframing, noting that Jack is likely easy to get along with, and uses this as indirect validation of Jack’s social worth despite his mistrust of others. The therapist avoids over-interpretation by acknowledging the limit of his own understanding (Extract 7, Line 3) while still offering an affirming reflection on Jack’s previous statement—one that Jack affirms in his response (Extract 7, Line 4).
The therapist validates this shift (Extract 7, Line 5), reinforcing the significance of being able to acknowledge both negative and positive aspects of the self. The therapist also checks in on Jack’s emotional state (Extract 7, Line 7), inviting affective reflection here and now moment. Jack reports a sense of lightness—an embodied indicator that emotional relief has occurred.
The therapist revisits a statement from the beginning of the session in which Jack expressed not wanting to return (Extract 7, Line 5). Jack’s response (Extract 7, Line 6) shows a shift in stance, indicating openness to further dialogue.
Discussion
This study explored the psychotherapy session between a young adult with experiences interpretable as psychosis and a clinician with professional and academic background in dialogical approaches to psychosis. Using a conversation analysis-informed case analysis of a single post-hospitalization psychotherapy session, the findings highlight how key interactional mechanisms supporting dialogical conversation—such as reflective formulations, non-directive open questions, and affective attunement—can support the emergence of meaning, emotional regulation, and more reflective self-positioning, even in a single session with a person who has previously been interpreted as having limited understanding and difficulties engaging with the treatment offered.
The analysis revealed several moments where Jack shifted from emotionally charged and fragmented narratives to more integrated reflections. These changes were facilitated not by confrontation or theoretical reframing, but by the therapist’s consistent use of non-pathologizing language, epistemic humility, and relational validation.
Throughout the session, dialogical rhythm was maintained through the therapist’s open-ended questions, which showed interest in Jack’s experiences. In contrast, disruptions often followed closed or interpretive questions, especially when they limited Jack’s opportunity to elaborate. The therapist’s use of open-ended questions related to the ongoing topic, along with repetition, reflection, and summarizing, helped restore the conversational flow and support shared meaning-making. Although dialogical approaches emphasizes flexible, need-adapted responses, the consistent use of such interactional techniques may offer a practical framework for fostering dialogue across diverse clinical situations.
As noted in previous conversation analyses on OD network treatment meetings (Ong et al., 2021, 2024), reflections and repetitions seemed to serve multiple functions. This also reflected the fact that, while the idea of dialogism emphasizes the reduction of power asymmetries and the unconditional acceptance of otherness, the therapist nonetheless plays an active role by choosing what to highlight, reflect upon, and repeat. This was evident also in this session through the therapist’s use of repetition, reflection, and open-ended questions that focused on topics and interpretations aligned with a more neutral epistemic positioning and openness to multiple perspectives.
It is notable that similar interactional practices drawn from OD network meetings appeared to support more egalitarian interaction and reflective self-positioning, even within a one-on-one setting. However, despite these efforts, the session still lacked clear polyphony, and the interaction frequently shifted toward an interview-like, monological format. This suggests that maintaining an open, dialogical stance may be more challenging in individual therapy, where the absence of multiple voices can more easily lead to a directive therapeutic approach. These findings underscore the importance of involving a broader social network to sustain a truly dialogical process, which in turn may facilitate shared understanding and meaning-making in actual relational contexts.
Although this study focused on a single case, and the one-on-one format limited the presence of polyphony, the findings offer insight into why interactional mechanisms supporting dialogism may be therapeutically effective. In the analyzed session, even subtle signs that Jack’s beliefs were being challenged often led to defensive or rigid responses that could reinforce a narrative interpretable as psychotic. This highlights the risk of a circular dynamic, wherein Jack feels compelled to repeatedly justify his experiences. Such justifications may then be perceived by clinicians as further evidence of “psychosis,” prompting more psychoeducation or correction, which in turn increases the person’s frustration and reduces engagement.
The ability to return to a dialogical stance after ruptures highlights the importance of sensitive and collaborative methods—especially during acute crises, when more confrontational approaches may jeopardize the therapeutic alliance. The session also illustrates how dialogical engagement can open space for deeper themes, such as shame, low self-worth, and vulnerability. While these themes could be addressed within conventional therapeutic models, they may remain inaccessible if the circular dynamic described earlier takes hold. In this sense, dialogical practice does not replace structured approaches but serves as a vital entry point for meaningful therapeutic engagement.
Overall, the findings suggest that the core interactional practices that promote dialogue in the treatment of situations diagnosable as psychosis—together with an emphasis on the therapeutic relationship, a not-knowing stance, and active rupture repair—may not differ substantially from those found in other relational psychotherapy approaches. Recognizing these similarities may support the broader implementation of dialogically informed practices and thus foster a more holistic way of engaging with individuals and their social networks in everyday clinical settings.
Strength and Limitations
This study has several strengths. Most notably, it presents an ecologically valid example of a real-life therapy conversation with a person who met the diagnostic criteria for severe psychosis, including stereotypical symptom expression and course. The data also provide valuable insight into how dialogical treatment can at least partially unfold in a one-on-one therapy setting—beyond the more commonly studied OD network meetings. This is particularly relevant, as in everyday clinical practice, service users may refuse the involvement of family members. Building trust and collaboration in individual sessions may lay the groundwork for involving the social network later in treatment, which was in fact also the case with Jack. Moreover, while existing literature on dialogical approaches has shown promising outcomes, few studies have closely examined how experiences diagnosed as psychosis are actually discussed and shaped within real-time dialogical interaction.
Nevertheless, this study has several limitations. First, it is based on a single therapy session with one case, which affects generalizability of findings. Another limitation is the potential for researcher bias. As the research was conducted as part of the author's formal psychotherapy training thesis, the author served as both therapist and analyst. Even though this dual role itself enabled a rare analysis of a routine psychotherapy session involving a participant who is typically difficult to reach in research, it likely also influenced which aspects of the interaction were attended to and emphasized in the interpretation. To mitigate this, the session recording was independently reviewed by a supervision group, with general agreement on the main analytic observations and interpretations.
To mitigate potential researcher bias, the analysis prioritized observable interactional evidence in the extracts, using dialogical concepts as sensitizing tools rather than as a fixed, theory-driven coding scheme. This approach was supported by the inclusion of extensive transcript excerpts, enabling readers to independently evaluate the interpretations. Importantly, Jack himself reviewed and agreed with the main findings and conclusions. However, the possibility of social desirability bias remains, as he was aware that the therapist would hear his feedback.
Finally, therapist's dual role and expertise in dialogical work can also be considered a strength, as it allowed for nuanced and clinically informed interpretations during the analysis phase.
Conclusion
This study demonstrates that interactional practices supporting dialogism can create meaningful therapeutic opportunities in the treatment of psychosis, even within a one-on-one setting. Rather than provoking defensiveness or reinforcing experiences commonly interpreted as psychotic, these interactional practices fostered engagement and reflective self-awareness. Although individual sessions carry a risk of reduced polyphony and a shift toward monological interaction, the development of a therapeutic alliance may increase the service user’s trust and openness to involving social network members later in the treatment process. In this way, dialogue can serve not only as a therapeutic method but as a foundation for meaningful and more holistic treatment process of situations diagnosable as psychoses.
Footnotes
Acknowledgements
I sincerely thank Jack for his openness and courage in allowing this session to be analyzed and published. While he continues to disagree with interpreting his experiences as symptoms of psychotic disorder, he supported the publication, appreciating the value of the interaction.
Ethical Considerations
Before the session, the Chair and Secretary of the Ethics Committee of the University of Jyväskylä reviewed the study plan and concluded that it did not require ethical review under the guidelines of the Finnish National Board on Research Integrity (Statement on the need for an ethical review: 583/13.00.04.00/2025).
Consent to Participate
Prior to the session, Jack provided signed, informed consent for the psychotherapy sessions to be recorded for training supervision. He also consented to the use of material from the recordings in an author’s integrative psychotherapy training thesis and in scientific journal publications.
Consent for Publication
Jack has read the manuscript and was given the opportunity to comment on it, request changes, or decline its publication. After reading and commenting the manuscript, written informed consent for publication was obtained from Jack.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The full, non-pseudonymized transcription is not available due to the sensitivity of the topic and because informed consent for publication was obtained only for the use of pseudonymized and translated extracts included in the paper.