
Abstract
While everyone experiences threats, some threats are culturally specific and not universally recognized or addressed by providers. A prominent example is threat-based worry and hypervigilance in Black Americans and other minoritized individuals, which is higher due to systemic racism and increases risk for psychopathology like clinically significant paranoia. To date, there have been no adaptations of cognitive-behavioral therapies for Black Americans with psychosis, despite the long-standing history of systemic racism in the United States, and its increasingly recognized contribution to psychotic experiences. Accordingly, we present the first step towards developing an adapted cognitive-behavioral intervention for Black and minoritized Americans with psychosis. This adaptation of an empirically supported worry-based treatment for persecutory delusions was accomplished by comprehensive conceptualization and integration of how systemic racism and minoritization drive the prevalence and perception of threats. This contrasts with conceptualizing racism-related hypervigilance and cognitions as worry or ignoring these critical experiences altogether, which is invalidating and neglects optimal identification and intervention on behavioral targets. Using a validating and normalizing approach, the individual was able to identify how frequent threats related to systemic racism resulted in increased worry, vigilance, and distress. By identifying and intervening on the perception of threat and associated worry, the individual engaged in more helpful responses to the threat, which in turn increased participation in more meaningful activities and reduced worry and clinical paranoia. This case illustrates how accurate conceptualization clarifies behavioral targets and increases patient engagement, which together enhance the effectiveness of the intervention for minoritized individuals.
“[Black Americans] can’t sit back and relax at all; you have to be vigilant at all times; if you don’t you’ll be back in chains.” – Feagin and Sikes (1994)
1 Theoretical and Research Basis for Treatment
The Role of Systemic Racism and Minoritization in Persecutory Delusions
Everyone experiences psychological threats. Some events are perceived as threatening by many, like being looked at by strangers or hearing an unusual noise downstairs. Other experiences confer threat in a culturally specific fashion and may only be recognized, understood, or classified as threatening by communities with minoritized identities. Examples may include being pulled over by the police, asked about immigration status, or being monitored or addressed by a store owner. Systemic racism and minoritization are pervasive, threatening experiences in the United States among Black individuals. For Black Americans, systemic racism and minoritization promotes increased worry and attention towards threats in order to maintain safety — termed racism-related vigilance (Feagin, 1995; Hines et al., 2018). These experiences of racism not only contribute to worry, but also predict non-clinical paranoia (Combs et al., 2016).
Paranoia is a broad construct that spans more normative cultural paranoia, which is described as an adaptive psychological and behavioral response to systemic racism and minoritization, and clinically significant paranoia commonly present in psychotic disorders (Whaley, 2002). Although thought of as adaptive, cultural paranoia can lead to both helpful and unhelpful cognitions and behaviors (e.g., keeping both hands on the steering wheels during a traffic stop vs. speeding away from a police officer during a traffic stop, respectively). Cultural and clinical paranoia may occur discretely or in combination, with the combination often resulting in a more severe, intractable presentation (Whaley, 2002). Perhaps unsurprisingly, Black Americans receive psychosis diagnoses at a rate of 2–4 times that of White individuals (Olbert et al., 2018; Schwartz & Blankenship, 2014). In the UK, estimates suggested a 6-fold elevation in paranoia for Black compared to White individuals, which was specific to more severe forms of persecution (Freeman et al., 2011). While various social determinants, healthcare inequities, and biases in assessment may contribute to these disparities, a complementary theory is that systemic racism and minoritization contribute to increases in persecutory delusions in part due to a heightened vigilance to threats (to maintain safety) (Oh & Anglin, 2021; Oh et al., 2016). It is also likely that such experiences alter beliefs about the self and others that create vulnerabilities for the occurrence of paranoia. Disentangling these psychological drivers of paranoia (cultural vs. clinical) creates challenges for earnest clinicians, while failure to understand and address both driving processes may result in less effective treatment, leaving minoritized individuals, especially Black Americans, underserved by our current cognitive-behavioral approaches and therapeutic systems (cf. (Oluwoye et al., 2018)).
Broadly, research is beginning to conceptualize worry, a critical factor in cultural paranoia, as a contributory causal factor in the maintenance of clinically significant persecutory delusions (Freeman & Garety, 1999; Sheffield et al., 2021; Startup et al., 2016). In the Threat Anticipation Model, it is hypothesized that a number of psychological mechanisms, including worry, maintain the strongly held but inaccurate belief that one is under threat (i.e., the persecutory delusion) (Freeman., 2016). Worry is thought to bring threatening ideas to mind, elaborate the content, and increase the distress. Clinical trials have demonstrated the efficacy of targeting worry in the treatment of persecutory delusions (Freeman et al., 2015). Yet, the role of systemic racism and minoritization in the formation and maintenance of such delusions and integration into individualized worry models has not been directly addressed.
2 Case Introduction
James is an adult, middle-class, Black male in the South with a diagnosis of a schizophrenia-spectrum disorder characterized by paranoia, who presented to a clinical study of a worry intervention for persecutory delusions. Therapy sessions were recorded with James’ consent and in keeping with the study protocol. He presented as extremely personable and polite yet guarded about his symptoms. He often used vague or abstract language and excessive metaphors to explain his experiences. Of his volition, James was not engaged in services to address his symptoms, including psychotherapy or medication management. He ultimately consented to participate in the hopes of decreasing his worry.
3 Presenting Complaints
James’ primary concern upon entry into the study was significant worry. He also presented with persecutory delusions that “people of a certain demographic know that I know too much and therefore want to harm me or make me feel isolated.”
4 History
James received a diagnosis of schizoaffective disorder in young adulthood. At the time of the study, James was not utilizing medication management services or psychotherapy services. He reported no history of therapy for psychological concerns. James also reported a history of moderate to severe childhood emotional, physical, and sexual abuse as determined by the Childhood Trauma Questionnaire (Bernstein et al., 1998), though did not meet diagnostic criteria for a past or current trauma-related disorder.
5 Assessment
James’ Assessments Across the Intervention.
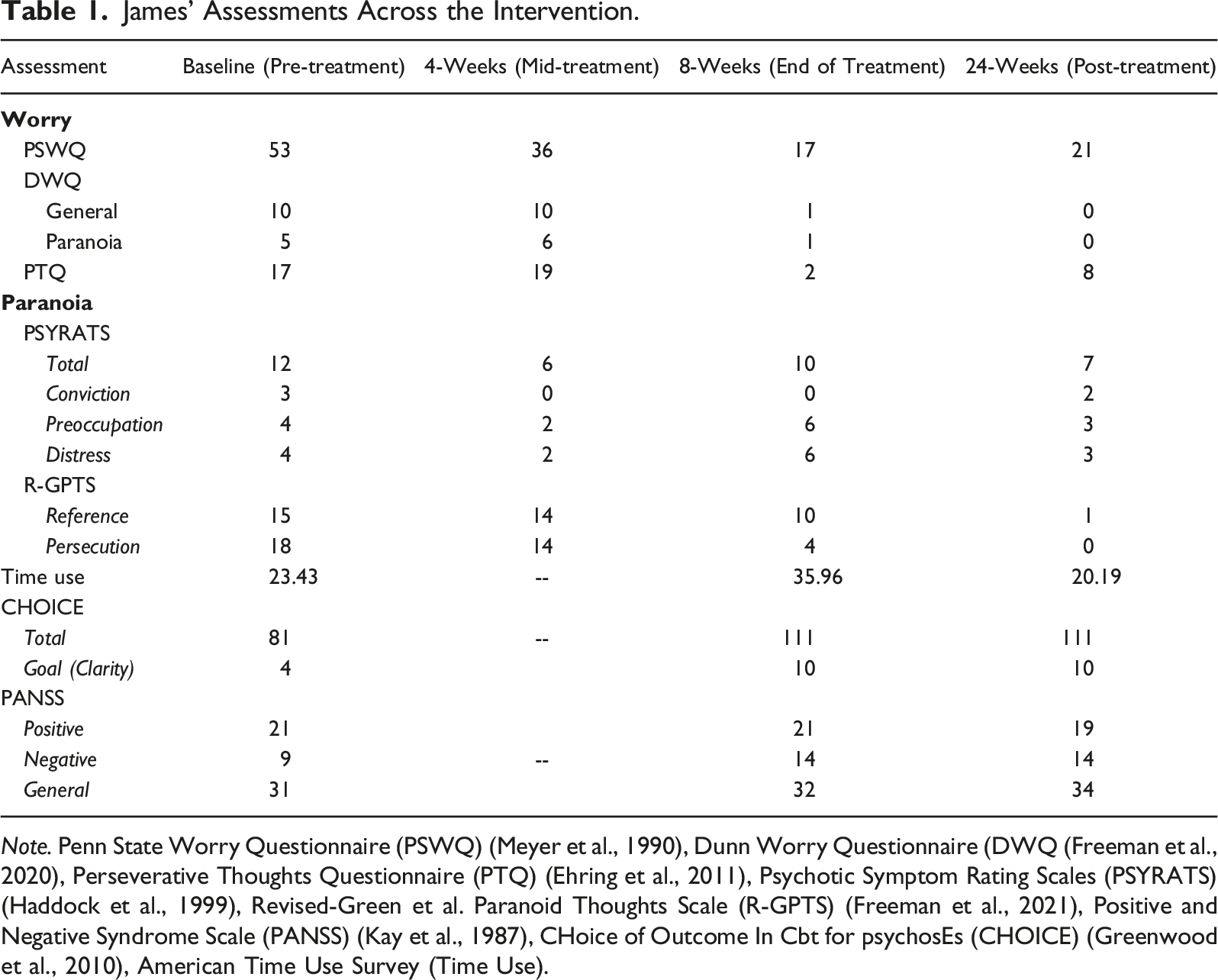
Note. Penn State Worry Questionnaire (PSWQ) (Meyer et al., 1990), Dunn Worry Questionnaire (DWQ (Freeman et al., 2020), Perseverative Thoughts Questionnaire (PTQ) (Ehring et al., 2011), Psychotic Symptom Rating Scales (PSYRATS) (Haddock et al., 1999), Revised-Green et al. Paranoid Thoughts Scale (R-GPTS) (Freeman et al., 2021), Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987), CHoice of Outcome In Cbt for psychosEs (CHOICE) (Greenwood et al., 2010), American Time Use Survey (Time Use).
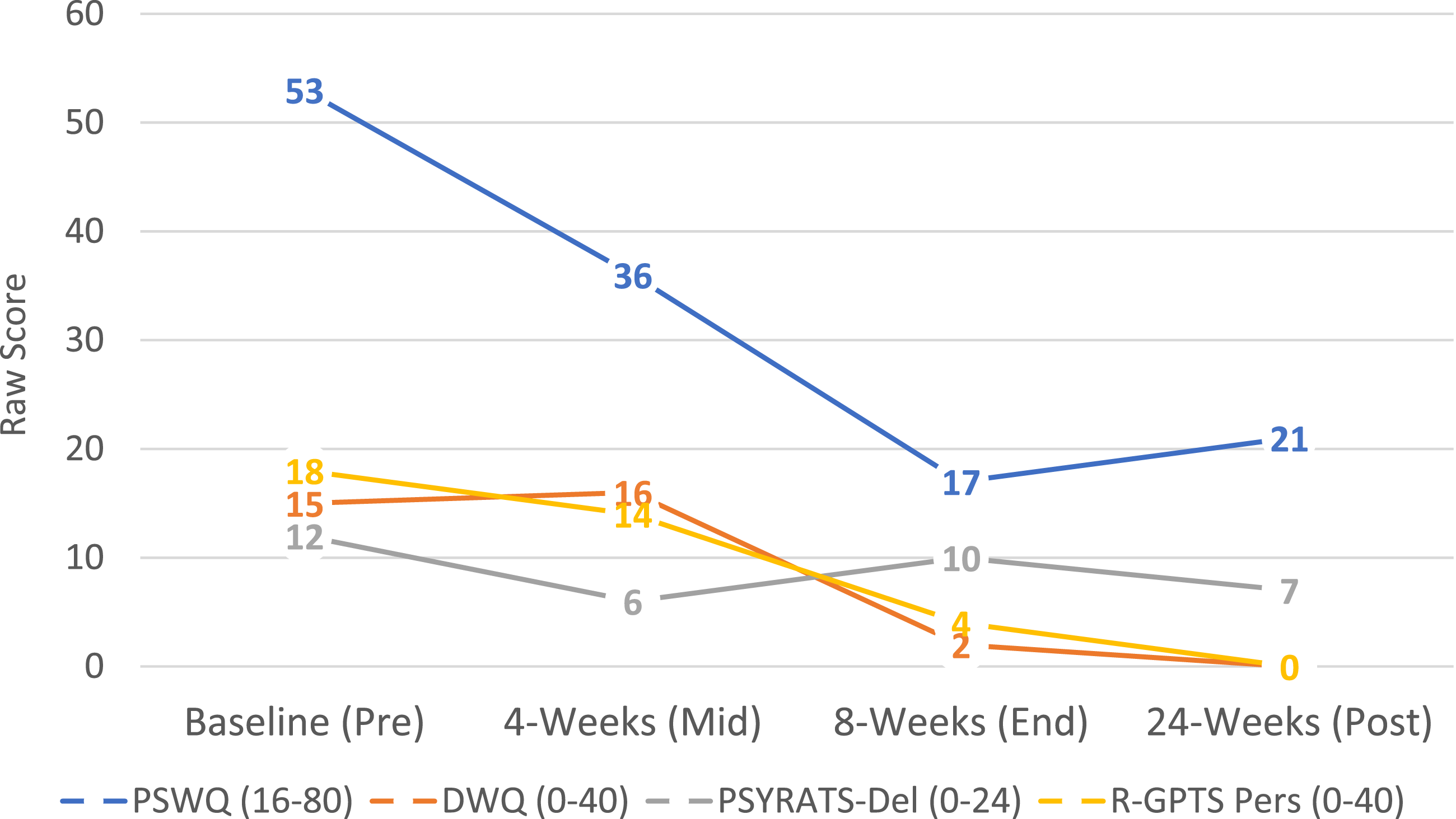
Changes in Worry and Paranoia. Note. Depiction of James’ changes in worry (Penn State Worry Questionnaire (PSWQ) and Dunn Worry Questionnaire (DWQ)) and paranoia (PSYRATS-Delusion Subscale and Revised Green et al. Paranoid Thoughts Scale (R-GPTS) persecution subscale). Score ranges for each scale are in parentheticals. James was assessed over the course of the intervention including baseline (pre-intervention), 4 weeks (midpoint of intervention), 8 weeks (end of intervention), and 24 weeks capturing post-intervention follow-up. Data show a marked decrease in worry as well as decrease in persecutory delusions. Gains were maintained post-intervention.
To assess worry, the Penn State Worry Questionnaire (PSWQ) (Meyer et al., 1990), Dunn Worry Questionnaire (DWQ (Freeman et al., 2020), and Perseverative Thoughts Questionnaire (PTQ) (Ehring et al., 2011) were administered. The PSWQ is a 16-item self-report measure of worry focused on the time and context in which worry occurs. At baseline, James endorsed a moderate amount of worry (total score = 53), suggesting his worry occurred frequently and across contexts. At both week 4 and 8, James’ worry decreased to the mild range (Reliable Change Index (RCI) = 4.59 and 9.72, respectively). His reports on the PSWQ were consistent with the DWQ, a 15-item self-report measure of general worry (subscale score = 10) and paranoid worry (related to others trying to harm oneself; subscale score = 5) and the PTQ, a 15-item self-report assessing ruminative, unproductive thinking style (total score = 17). While his PTQ scores did not meet the recommended clinical threshold, they indicated an inability to engage in thought that is meaningful and productive. This was well-aligned with the motivation for the intervention. A slight increase on the PTQ was observed at week 4 (total score = 19), which was consistent with James’ personal reports during the intervention that he was noticing his worries and times of rumination more often. By week 8, he exhibited a reliable decrease in perseveration (total score = 2; RCI = 3.82). Change on the DWQ showed a similar trend, with no improvement at week 4 (general score = 10, paranoia score = 6), then a dramatic decrease by the end of the intervention (general score = 1, paranoia score = 1).
Persecutory delusions were assessed with the Psychotic Symptom Rating Scales (PSYRATS) (Haddock et al., 1999)) and Revised-Green et al. Paranoid Thoughts Scale (R-GPTS) (Freeman et al., 2021). The PSYRATS is a clinician-rated assessment tool of which one component is assessment of delusions via six questions, including establishing a delusional statement representative of the delusional content and assessing for preoccupation, conviction, and distress associated with the delusion. James summarized his delusions as “people of a certain demographic know that I know too much and therefore want to harm me or make me feel isolated.” Regarding this delusion, he was determined to have high preoccupation (subscore = 4) consistent with his reports of worry and perseverative thinking, high distress (subscore = 4), and high-moderate conviction (subscore = 3). By week 4, his total PSYRATS score showed a reliable decrease (RCI = 4.74; total score = 6), with a marked decrease in conviction (score = 0). Change in conviction persisted to week 8, though there was little meaningful change in preoccupation or distress. As a complement, the R-GPTS measures paranoid thinking domains of ideas of reference and persecutory beliefs. James’ self-report indicated elevated ideas of reference (subscore = 15) and severe persecutory beliefs (subscore = 18). Midway through the intervention, no meaningful change occurred though there was a modest downward trend in both self-reported ideas of reference (subscore = 14) and persecution (subscore = 14). At the end of the intervention, reliable change was observed in James’ self-reported persecutory thoughts (subscore = 4, RCI = 6.04) and both subscales were now in the “average” range. The Positive and Negative Syndrome Scale (PANSS) (Kay et al., 1987), a 30-item clinician rated measure was used to assay the broad spectrum of psychosis symptoms including positive symptoms (e.g., hallucinations, delusions), negative symptoms (e.g., flat affect, alogia), and general symptoms (e.g., cognitive impairment, irritability). James evidenced significant general symptoms (subscore = 31) and more prominent positive symptoms (subscore = 21), driven by delusions. Negative symptoms were not a defining characteristic of his presentation (subscore = 9) at baseline. No meaningful change was observed by week 8 (end of intervention).
Progress towards therapeutic goals were tracked with the CHoice of Outcome In Cbt for psychosEs (CHOICE) (Greenwood et al., 2010), a 24-item self-report of intervention satisfaction broadly and related to a specific individually-chosen goal for treatment. James chose a goal of gaining more clarity. Initially, James reported moderate skills and satisfaction with the intervention and minimal efficacy in his goal (total = 81, goal subscore = 4). At the 8-week end of intervention evaluation, James scores reflected notable success with the intervention and CBT-based skills as well as self-efficacy in his goal of clarity (total = 111, goal subscore = 10).
Finally, functional engagement was assessed with the American Time Use Survey. James reported minimal engagement in meaningful or enjoyable activities (total score = 23.43). At the end of treatment, he reported more engagement in goal-directed activities (total score = 35.96), which was consistent with his reports in session including going to sporting events and spending more time with others.
A follow-up assessment was conducted at 24 weeks (post-treatment) in which the same assessments were readministered (section 10 below; Table 1, Figure 1).
6 Case Conceptualization
Assessment and evaluation suggested that James possessed entrenched paranoid delusional beliefs that caused him both worry and distress about his safety and well-being, and impacted his ability to engage in enjoyable activities. It is well-established that cognitive-behavioral approaches (e.g., CBT for psychosis, Recovery-Oriented Cognitive Therapy) are efficacious and effective forms of intervention for the symptoms of psychosis including delusions, hallucinations, and negative symptoms (Beck et al., 2020; Burns et al., 2014; Lysaker et al., 2020; Masterson et al., 2020; Mehl et al., 2015). Regarding paranoid delusions, the cognitive-behavioral approach involves the clinician (a) developing a formulation of the maintenance factors (thoughts, behaviors) of the delusion, (b) guiding an individual through identifying and evaluating the accuracy and utility of the maintaining factors, including resultant emotions, thoughts, and behaviors, and (c) identifying alternative adaptive responses (new beliefs, behaviors) to the maintaining factors.
A prominent feature of James’ delusional landscape was the role of systemic racism and his demographics as a minoritized individual in the context of a majority culture. This was both a real experience with implications to his daily activities and became delusional, making him suspicious of neighbors and strangers. Recent acknowledgement of the role of systemic racism and minoritization on stress and mental and physical health disparities has prompted an increase in cultural adaptations to our current interventions to better serve Black Americans (cf. (Zhou et al., 2022)). For cognitive-behavioral interventions, some cultural adaptations have been developed, such as inclusion of the family, infusion of identity-based content (military, sexual orientation), and language-based adaptations (Naeem, 2019). In treating psychosis specifically, effective cultural adaptations of cognitive behavioral therapy primarily come from Asia and the UK. Adaptations include content on culturally-specific beliefs about treatment, the role of family and religion, and addressing culturally-driven stigma and beliefs about psychosis (Naeem, 2019; Naeem et al., 2015, 2021; Rathod et al., 2010, 2013). To date, there have been no adaptations of these therapies for Black Americans with psychosis, a population that presents a unique case given the embedded and long-standing history of systemic racism in the United States. It was clear that James would benefit from sensitivity to these issues within the intervention and assistance with distinguishing the adaptive components of his suspiciousness (e.g., action to safety) with the less accurate recognitions of threat and less helpful outcomes (e.g., worry). Accordingly, we present the first step towards developing an adapted intervention for Black and minoritized Americans.
The following case utilized a novel empirically supported, cognitive-behavioral intervention for a subset of delusions, persecutory delusions, established by Freeman and colleagues as part of the Feeling Safe Programme (Freeman et al., 2019). The rationale for this approach is that worry (conceptualized as a behavioral process) “brings implausible fearful ideas to mind, keeps them there, and exacerbates the distress” (Freeman, 2016). For instance, an individual may believe that their ex-boyfriend breaks into their home every night and leaves clues around the house to harass and frighten them. This individual may spend hours worrying about what specifically this person might do to them and feel they are in danger. This creates a rich narrative in their mind of all the possible ‘what if’ scenarios that could result in their harm, expanding the delusional belief system and limiting other cognitive resources. Accordingly, decreasing worry will help the individual live a more meaningful life filled with preferred activities and, ultimately, undermine the delusion.
Core to this process is a model by which threats set off a cycle of unproductive worrying (Figure 2), perpetuated by the generation of new worry-based threats. While worry is colloquially used to describe a feeling, in this model and the CBT framework broadly, worry is conceptualized as a behavioral process by which one engages in effortful activity in response to unpleasant feelings. The perception of a threat (e.g., arrive home with all the lights off, in the prior example) can lead to a cognitive process by which the individual gives themselves license to worry. This is a positive belief the individual holds about worry, which may include “worry prepares me for the worst,” “worry prevents bad things from happening,” “worry helps me to avoid problems in the future,” or some other cognition that highlights the supposed benefits of worrying. With this license to worry triggered by threat, the individual engages in worry, asking “what bad thing happens next? What if?” Accordingly, as this behavior (worry) continues, the individual ends at a worst-case outcome that becomes a new threat. The process continues, resulting in dwelling on the sense of unsafety and avoidance or inaction. Systemic Racism, Paranoia, and the Worry Cycle. Note. Cycle depicts the model by which worry maintains paranoia. Threats exist broadly in our daily lives; a subset of threats are maintained by systemic racism, clinical paranoia, and cultural paranoia, which have both distinct and partially overlapping effects. Accordingly, the experience of systemic racism increases the scope of threats an individual may perceive due to increase racism-related vigilance (e.g., noticing a store owner taking notice of oneself) and increased presence of targeted threats (e.g., police officers are a threat, rather than a protection). The perception of threat activates a positive belief about the function of worry (e.g., “worry prepares me for the worst,” “worry prevents bad things from happening,” etc.). With this license to worry triggered by threat, the individual then worries. They ask, “what bad thing happens next? What if?” As this behavior (worry) continues, the individual ends at a worst-case outcome on which they dwell. This becomes a new threat. The process continues. Figure adapted with permission from Daniel Freeman, Manual developed for the Worry Intervention Trial (WIT) funded by the MRC/NIHR Efficacy and Mechanism Evaluation Programme 2011.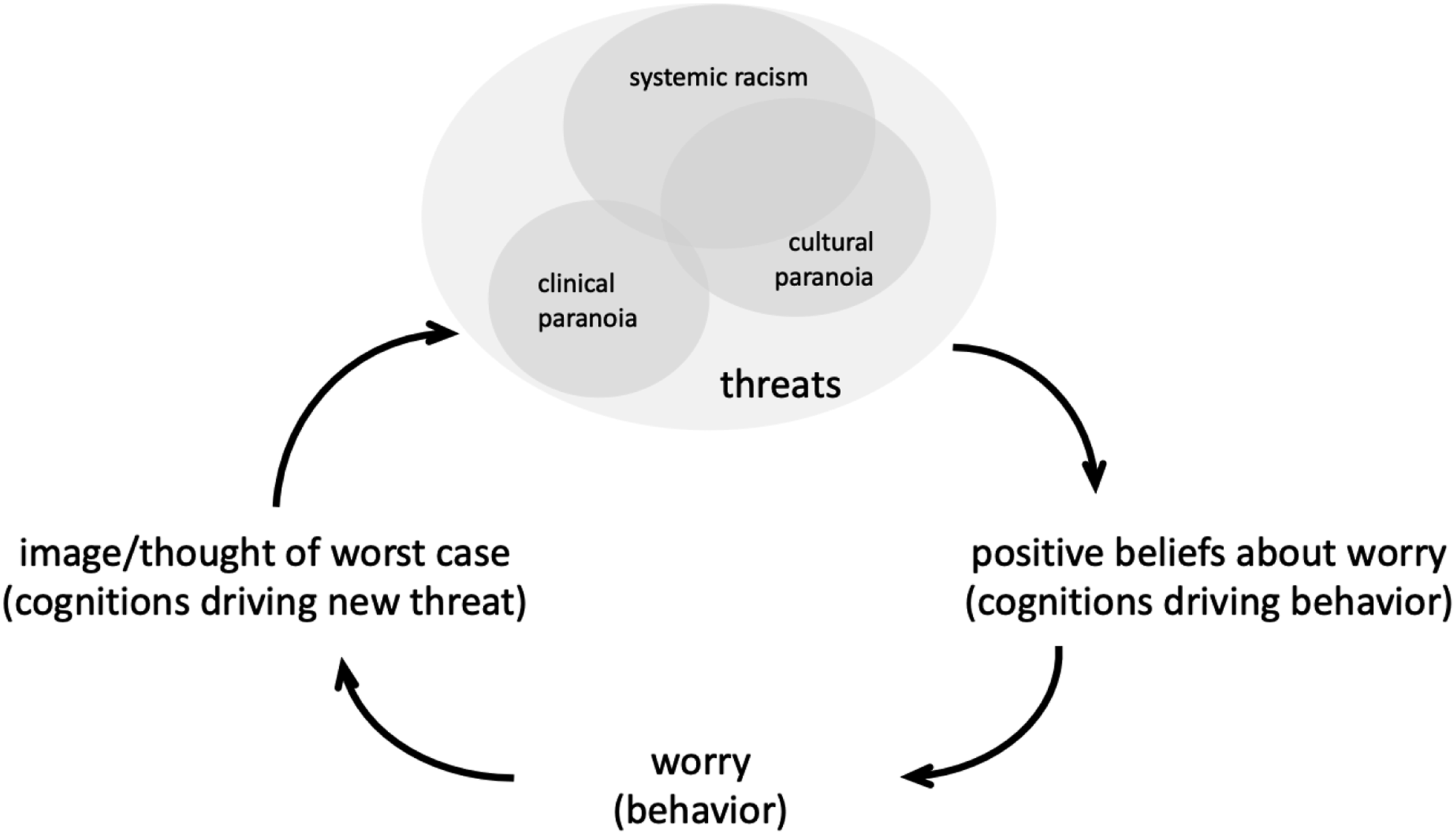
In the case of systemic racism and minoritization, the threat may be perceived due to a very real set of historical and systemic circumstances that place the individual at higher risk (frequency and severity) of danger and increase hypervigilance. Individuals monitor their external environment for threats such as being in a perceived wrong place, reactions (or perceived reactions) of others, presence of authority figures, and other system-based threats and microaggressions (cf. (Alang et al., 2022; Anglin & Lui, 2021; Freeman et al., 2001; Garety et al., 2001)). Simultaneously, individuals monitor threats through internal vigilance, such as noticing increases in heart rate, gut feelings, images/memories of past personal or second-hand racist experiences, and other internal signs of threat (Feagin, 1995; Forsyth & Carter, 2012). The worry amplifies the threats, creating a new threatening situation that increases motivation to worry, and the cycle accelerates. With each time through the cycle and each new incorporated threat, the worry gets more extreme and frightening, which may be part of the pathway to persecutory delusions. For someone under threat in the context and infrastructure of systemic racism, taking time to worry and resulting safety seeking behaviors (e.g., staring at people, behaving defensively) can elicit reactions from surrounding threats and place the individual at more risk (e.g., acute danger) than engaging in a behavior that places them in safety (e.g., problem solving).
7 Course of Treatment and Assessment of Progress
James was offered 6-8 weekly, 50-minute Worry Intervention Trial (WIT, cf. (Freeman et al., 2015)) sessions over an 8-week period. He ultimately attended 7 sessions, as detailed below. Treatment covered 5 modules, including setting up the threat-worry model, establishing a worry time, postponing worry, increasing sense of safety, and ended with a wrap-up session in which treatment was consolidated and reinforced. Between each therapy session, James was contacted via phone twice (total of 12 successful contacts) by his therapist for check-ins to follow-up on skill implementation, troubleshooting barriers, and eliciting feedback on skills. These contacts lasted on average 5 minutes. James also utilized these contacts to report insights from the week that he wanted to place on the agenda for the following session.
Session 1: Establishing the Model
Session 1 was focused on establishing the rationale for targeting worry. During this session, James initially presented with low volume of speech, poor eye contact, and was reticent to share his opinion or experiences. As the session continued, he became more audible and interactive.
The protocol uses metaphors and in-session exercises to illustrate how worry builds and that worry can occur for neutral and positive experiences, in addition to negative or threatening experiences. James was especially reticent to verbalize the worst-case scenario during the in-session exercises in which the therapist and James collaboratively worried about dropping a pen and, next, winning the lottery. Instead, James attempted to jump into the best case, frequently commented that the outcome could get “really dark,” asked to instead reflect on the scenario happening to someone else, and used indirect language (e.g., “self-harm yourself into not existing anymore”). This pattern of avoiding talking about difficult topics was a theme across therapy and addressed in session 5.
As a part of developing the model, James was directed to identify from a list of positive beliefs he holds about worry, including “worry keeps me safe, “I have to worry in order to remain organized,” and “worry prepares me for the worst.” He also was able to identify negative beliefs he has about worry, such as “my worrying could make me go mad” and “I would be a stronger person if I worried less.”
With these foundational concepts, much of the session was dedicated to establishing the worry cycle, the model by which threats activate our positive beliefs (license to worry) about worry, which set off the behavior, ending with a worst-case outcome that poses as a subsequent threat. James walked the therapist through his own example of this model: Therapist: “Tell me more about what it meant or what the threat was that this person moved to another side of the street”
Session 2: Setting Up Worry Time and Worry Postponement
James entered this session having not done any of his daily worry tracking. As the therapist and James began to troubleshoot barriers, James reported worrying about tracking his worry due to the threat that he “might be more worried about it than I think I am.”
The therapist and James explored this by diagraming a particularly worrisome day for James, including his various activities, and identifying all the times at which he is worrying. James maintained a rigid interval schedule (i.e., different activity every hour, 3–4 hour sleeping bursts throughout the day). Through this exercise, it was discovered that James spent nearly all his waking hours (12 hours) worrying or engaging in some sort of activity to try to negate worry. James reported being surprised by how much time he spent worrying; he acknowledged that this limits his ability to be present and effective in a given moment.
With an investment in reducing his time spent worrying to increase his ability to engage in enjoyable activities, James and his therapist set up the concept of worry postponement, in which worry in the moment is postponed and saved for a brief, scheduled period later in the day. An initial postponement strategy was established in which James made a silly sound when he noticed himself worrying to pull him out of the worry and back into the moment. Worry was induced in session, during which James worried about what to worry about, and James practiced his postponement strategy. A 15-minute evening worry period was established during which James could freely worry about the worries he saved up from the day.
Session 3 and 4: Boosting Worry Postponement
Sessions three and four were focused on boosting James’ worry postponement skills, including troubleshooting past skills, and establishing new postponement skills. In session 3, James learned how to do problem solving. This skill was collaboratively chosen by James and the therapist due to continued avoidance of therapy homework, specifically worry tracking. At the end, the therapist helped James to generalize the use of problem solving to threatening situations in which he may be experiencing racial threats to keep himself safer. An example included a recent situation in which James walked by a car that looked like one he saw in a police report (threat). He reported concerns that the police may drive by and think he was affiliated with the crime (systemic racism and minoritization based threat), resulting in being jailed or convicted (worst case). The therapist and James discussed how his worry made him tense, experiencing chest tightness, and hypervigilance, looking around erratically. Therefore, worry was leading to behaviors that might make him appear more suspicious to police.
In session 4, James learned another postponement strategy: five senses grounding. Notably, James’ worry ratings were higher during this session. He attributed this to being more mindful of his worry, which allowed him to notice and “process” the worry. He described how this activity of “processing” (worry), caused him to get to conclusions he would have never worried about (worst case) and reinforced the threat. The therapist helped James conceptualize this “processing” as part of the worry cycle. James was able to identify how worrying about these threats does not get him closer to changing current or future outcomes.
To practice postponing this urge to “process,” the therapist and James walked in a busy area outside, noticing their minority status to induce worry. James reported experiencing chest tightness. James used grounding and reported experiencing no worry and being focused on the walk and nature. James described how this activity gave him “permission to experience.” James and therapist repeated worry induction and postponement to reinforce that James had control over his worry.
Session 5: Increasing Safety
Worry postponement strategies are useful in limiting worry once the cycle has started. Throughout the session, it was clear that James was hypervigilant to threats. For example, James reported looking at uplifting videos on Instagram and thinking about a positive future for himself, then noticed that he began to worry about the past and how it might negatively impact his future. He talked around “the past;” part of session was spent helping James to name his experiences. James had worries about the potential for him to perpetuate generational physical abuse and the objectifying of humans (starting from slavery). He was particularly aware of times when he treated others, such as past romantic partners or family, as “objects.” His experience could be conceptualized as a perception of threat for a benign incident (“objectifying someone” by watching them on Instagram) connected to a larger threat or worst-case (White views of humans as objects, instantiated by slavery).
To address this hypervigilance to threats, Session 5 was dedicated to a strategy of increasing an individual’s sense of safety, lowering the threshold by which a threat triggers the cycle. James created a mental image of walking in a wooded park with a waterfall. The therapist walked him through the 5 senses to increase the salience of the imagery. James reported that this induced a sensation of weightless and childlike wonder, which made him feel safe.
Session 6
This session was skipped at the request of James due to conflicting family responsibilities and lack of transportation.
Session 7: Differentiating Postponement Strategies
Now that James had established a toolkit of postponement strategies, session seven was used to increase his understanding of situations in which certain strategies were more or less helpful. James and the therapist walked outside in a crowded area. James immediately attempted to walk on the side closest to the road. The reader will recall that this chivalrous act of walking on a particular side of the sidewalk was a prominent event in James original threat-worry cycle from session 1. The therapist used this opportunity to process this worry cycle around chivalry by intentionally standing on the side closest to the road and traffic. James described the possibility of the person he is with being hit by a car (threat), which lead him to ruminate about the various threatening scenarios that may occur (worry, e.g., people seeing James and thinking he was not honorable). He reported worrying about this less frequently since engaging in daily practice of his safe space imagery (i.e., the wooded area visual). He reported that when it does come up, grounding is the most effective strategy to stop his worry, allowing him to go about his day or be mindful and attentive in his interactions with his walking partner.
Session 8: Consolidation of Worry Tools
In the final session, James and writer consolidated the various skills he learned over the course of the intervention and prepared for future setbacks. The therapist and James diagrammed his most worrisome day of the past week, as done in session 2. James reported spending roughly 6 hours worrying (50% decrease from session 2) that was specific to unstructured time. He reported his time engaged in enjoyable activities as more effective and meaningful.
8 Access and Barriers to Care
James was attending therapy in the context of a research study. He was not seeking care outside of this context by personal choice. No difficulties or concerns emerged regarding access and/or barriers to care.
9 Complicating Factors
Two complicating factors were addressed during the application of the worry intervention. First, James often used abstract language and talked around topics (circumstantiality), which initially made it difficult to fully understand his experience (i.e., understanding why the woman on the street was threatening, identifying the threat of generational trauma). Therapist: “can we name things?” James: “abuse… abuse” Therapist: “what was it like to name the thing” James: “it feels like there’s more… it’s big” Therapist: “if you can’t touch it you can’t address it… that keeps you stuck”
Simultaneously, James’ language allowed him to capture beautifully the spirit of the intervention and its goals (e.g., being caged by worry, diverting a cognitive river, the dulled knife of worry). In accordance with best treatment practices, developing a common language with James bolstered his ability to effectively understand the model and apply the intervention, increasing his investment in intervention strategies.
Second, James feared the consequence of engaging in homework, specifically daily worry tracking. When addressed in session, James reported hesitancy to write down the things that worry him because (1) it was difficult to accept how much time he actually spent worrying and (2) he was worried about the things he worried about (e.g., abuse, generational trauma), reporting that writing things down made them more real. These experiences in which James was actively worrying about completing the worrying ratings were able to be used in session as personal examples and rationale for various postponement strategies. Although James never got to a place of completing these ratings, he did exhibit increased awareness of the presence of his worrying, situational factors that triggered his worry, and had a clear sense of which strategies were helpful to reducing his worry in various situations.
10 Follow-Up
By the end of treatment, James exhibited a clinically meaningful reduction in worry that persisted to follow-up. His scores on the PSWQ decreased 60% from his baseline assessment (score = 21 at week 24; RCI = 8.64), with similar improvement on both subscales of the DWQ (subscale scores = 0) and the PTQ (total score = 8; RCI = 2.29). James also exhibited enduring improvement in delusional content per his self-report on the R-GPTS (at week 24 reference subscale score = 1; persecution subscale score = 0, RCI = 7.77) and the clinician-rated PSYRATS (at week 24 total score = 7; RCI = 3.95) with distress, conviction, and preoccupation all trending downward. Over the course of treatment, James reported a strong working alliance with his therapist, including working towards the same goal and that his therapist understood him. This was supported by sustained reports of self-efficacy and treatment satisfaction on the CHOICE. No meaningful change was observed on the PANSS and time use survey.
11 Treatment Implications of the Case
Conceptualizing and integrating the role of systemic racism and minoritization into our models of treatment, particularly for psychosis, is critical for effective, comprehensive treatment especially for minoritized individuals such as Black Americans. Targeted interventions for paranoia, like the worry intervention, provide a clear opportunity to address the reality of these threats to our minoritized community members and the role everyday unsafety plays in increasing clinical symptomology, particularly persecutory delusions.
Fundamental to this model is that the entrenched framework of systemic racism and minoritization in everyday life constitutes an unsafe environment for certain groups that increases the probability of threat. This in turn increases hypervigilance to external threat cues, internal responses, and outcomes that are unproductive to the individual (Coogan et al., 2020; Lipscomb et al., 2019; Peters et al., 2011; Wheeler et al., 2011). The role of threat in delusion formation and maintenance for Black Americans and other minoritized individuals highlights a possible sand trap in these interventions. This occurs because the threats experienced by Black Americans and other minoritized individuals may be misclassified as worry or, on the extreme end, clinical paranoia, when in fact these experiences are sustained real-world threats. Alternatively, appreciation of these real-world threats can be a powerful inroad for more accurate conceptualization of their paranoia, enhancing working alliance and treatment outcome. Clinicians armed with an accurate model of systemic racism and minoritization as threatening experiences can address the resultant worry that is increasing distress and negative outcomes within the paranoia framework. As clinicians and researchers, accurately conceptualizing where the threat of systemic racism falls along the road to worry and paranoia is important for (1) clearly identifying targetable behaviors, (2) validating and understanding the client’s experience, and (3) helping the client move towards productive rather than potentially harmful actions.
The clinician with an accurate conceptualization of systemic racism as a threat provides motivation to change the response to the threat. Worry (rather than problem solving) may result in greater acute danger or unproductive outcomes (e.g., in the case of James, staring at the woman who crossed the street and making her more uncomfortable, perhaps prompting a confrontation or call to police). Unfortunately, the involvement of law enforcement rather than understanding or pathways to healthcare for Black Americans is staggering and results in more harm to the individual (Faber et al., 2023). The clinician employing a strategy based on an accurate conceptualization reduces the factor (worry) that puts the patient at increased risk by shifting engagement to productive behaviors (e.g., problem-solving, refocused activity). With the reclaimed mental space that was seized by worry, the individual can return to preferred life activities and pursuit of ambitions. Ultimately, this also undermines a core function of racism, to seep into and overrun a persons’ mental space, rendering them less engaged and effective in their own life (Carter et al., 2021; Williams, 1999).
Worry is not the crux on which the effects of systemic racism rest. General levels of stress have been linked to worsening delusions and paranoia in all individuals (Freeman et al., 2011; Lincoln et al., 2009; Moritz et al., 2011). Systemic racism and minoritization can be conceptualized as a chronic social stressor (Berger & Sarnyai, 2015). Stressors of this type induce long-term changes in stress response systems, such as the HPA-axis and neural regions responsible for the perception (increased hypervigilance), processing (increased salience), and response (dysregulation of top-down control, emotion regulation) to threats including the prefrontal cortex, hippocampus, amygdala and anterior cingulate cortex (Berger & Sarnyai, 2015). Accordingly, anxiety and mood disorders which have similarly implicated stress systems are also elevated in Black Americans (Berger & Sarnyai, 2015) and exhibit within-group increases as a function of higher race-based stress (Hudson et al., 2016). Black individuals experience higher rates of trauma and often meet criteria for PTSD at higher rates than White individuals, a well-established risk factor of psychosis (Faber et al., 2023). Elevations in stress hormones also result in changes to bodily functions, including hypertension, compromised immunity, etc. with their own long-term health consequences. Lack of treatment for medical and other psychiatric conditions (e.g., mood and anxiety) effectively increase rates of more severe psychopathology (e.g., psychosis) and inhibit proper engagement (access, maintenance) with healthcare services due to various biases and bureaucratic hassles (Faber et al., 2023). We therefore note that stress is a critical underlying aspect of worry and persecutory delusions that may increase risk for more severe persecutory delusions in Black Americans. This further highlights the need for racially-sensitive treatments, that can appreciate minoritization as a stressor that can exacerbate worry and delusions.
A recent study developing a novel measure for the assessment of racial trauma identified three core components — Lack of Safety, Negative Cognitions, and Difficulty Coping — that were elevated in minority groups and associated with psychopathology and trauma (Williams et al., 2022). These domains highlight the value of the entire Feeling Safe programme, allowing the provider to address other areas in which systemic racism has deleterious effects that contribute to paranoia. For example, systematic racism impacts formation and maintenance of self-confidence. Individuals internalize the negative messages and reduce pursuit of their valued activities, leading to more time and focus on dangers in the world. Additionally, minoritized individuals are likely to avoid going out into the world due to the ongoing perceived threats. Avoidance of going out provides more reinforcement for the dangers in the world and fewer opportunities to relearn safety. Finally, sleep disturbances can become amplified and instantiated by hypervigilance and worry, while also cyclically reinforcing more hypervigilance and paranoia due to inability to consolidate and refresh cognitive resources through sleep. Each of these factors associated with paranoia can be misunderstood or, hopefully, accurately conceptualized as sequelae of systemic racism and minoritization.
It is important to recognize the difference between when someone has perceived a threat as the result of a constellation of experiences resulting from systemic racism (e.g., being asked “are you going to buy that” at a store) versus when someone is in acute danger of harm. For example, if an individual was in a contentious situation in which a white man with a gun was accusing a black man of a slight, this would be a dangerous situation and would warrant a pause in the intervention to engage in targeted safety planning and process the experience. In that moment, the clinician should validate the real threat of racism and clearly label it as such. The clinician should also validate the impact these experiences have on the individual’s mental space, engagement, and effectiveness. The clinician can offer strategies within the individual’s control (e.g., safely exiting the situation, obtaining appropriate help, problem solving, alternate activities (Carter & Forsyth, 2010)). The clinician should emphasize the importance of meaningful engagement as a method of reclaiming the individual’s life, with focused work on determining the true safety of any strategies developed in therapy. The therapist should not suggest the individual enter an unsafe situation and should not diminish experiences of true danger. Instead, work should be focused on identifying safe and meaningful experiences that feel personal and fulfilling.
12 Recommendations to Clinicians and Students
This case clearly demonstrates how the experience of systemic racism and minoritization can be addressed through our current intervention models, especially if the clinician is aware and attentive to the dynamic. Sensitivity and intentionality validating an individual’s experiences of these threats pave a fruitful avenue for intervention. Such an approach moves the individual towards more productive strategies to manage discriminatory situations and resulting worry, while also decreasing clinical symptomology (persecutory delusions in this case). The individual can then increase engagement in meaningful and enjoyable activities.
Clinicians should prioritize acknowledging and talking about race, minoritization, and minority-related discrimination including systemic racism in the context of the intervention. A major factor identified through focus-groups in prior adaptations (Naeem, 2019) included the perception that therapists were avoiding or unaware of culturally specific drivers or outcomes of racism. Addressing this concern must begin with internal work by the clinician. Clinician discomfort or their own biases and assumptions can maintain barriers (cf. (Knox et al., 2003; Sue et al., 2007)). Practicing cultural humility is a clear step in support of this goal. Cultural humility is a process by which an individual reflects on their own cultural experiences and biases, approaching others with non-judgmental curiosity of their experiences to update and refine one’s own beliefs about the world, others, and our place within it (Mosher et al., 2017). In some cases, patients do not feel comfortable disclosing their experiences on their own, especially in race-incongruent dyads (Chang & Yoon, 2011). The clinician should recognize the developmental nature of identity formation — e.g., identifying with the majority culture while rejecting the minority culture (“pre-encounter”); immersion and curiosity about their own culture; etc. (Jackson III, 2012) — and meet individuals where developmentally indicated (Greig, 2003; Scottham et al., 2008). Open curiosity and expression from the clinician in a culturally humble way can facilitate this process. The clinician might slowly increase the focus to the presence of systematic racism: 1. 2. 3. 4.
By openly exploring the threat with the patient and putting forth questions about race in the context of the proposed intervention, the clinician can stimulate these discussions and provide a safe, contained place to address race-based concerns that the patient may have. Moreover, direct adaptations to the examples, phrasing, and rationale within the treatment workbook may provide embedded acknowledgement and context of the role of systemic racism and minoritization in worry, paranoia, and its treatment. A standardized framework in the treatment materials may improve provider comfortability with discussing these topics and increase patient confidence that the provider and system finds these issues to be valid and important in their treatment.
Clinicians should take time to accurately identify the threat, as well as how it may be perceived. If too hasty in conceptualization, the clinician may misidentify the true threat and, even worse, may misattribute an experience of systemic racism and minoritization as worry. The clinician should look at the situation and consider whether the fear described is common to that situation (e.g., Black man being accused of a crime near a car; Black man being accused of harassing a White woman). If unsure, asking the individual provides a collaborative approach to identifying racism as the threat and shows openness of the therapist to understand the individual’s experience. If the therapist does not seek understanding, the alliance with the patient may be ruptured by invalidating their real lived experience, leading to an incorrect internal model and worsening maladaptive behavioral and cognitive strategies. If the clinician notices the individual avoiding or retreating from the intervention, reexamine the worry and consider that it might be an actual threat. Accordingly, clinicians should take time to understand how systemic racism is shaping their clients’ beliefs/behaviors and may be leading to unhelpful or risky situations (cf. (Brown et al., 2021)).
In sum, the current case report provides a promising first step in developing a cultural adaptation to a worry-based, empirically supported intervention for persecutory delusions in psychosis. We do so by thoughtfully and intentionally disentangling driving factors of cultural and clinical paranoia to ensure that both are addressed, thereby strengthening the overall comprehensiveness and impact of the intervention. Examples in this case highlight subtle modifications that clinicians can begin to make to improve accurate conceptualization (e.g., asking about race dynamics) and for targeting the intervention when used with minoritized individuals. Moreover, this work identified some changes that can be made to intervention materials, such as the workbook, to support both patient and clinician in representing these dynamics in the therapeutic dyad and treatment. Ultimately, these adaptations will improve effectiveness of this intervention for Black Americans, who are uniquely impacted by systemic racism and often underserved or ignored by our mental health systems.
Footnotes
Acknowledgments
We wish to acknowledge our research participants and their families. We also thank other colleagues in the Oxford Cognitive Approaches to Psychosis (O-CAP) team at Oxford University, especially Louise Isham, Felicity Waite, and Rowan Diamond for training and support in implementing the Worry Intervention for Persecutory Delusions, part of the Feeling Safe Program. We acknowledge the contributions of the Vanderbilt University Medical Center Department of Psychiatry and Behavioral Sciences Psychosis research team who collected data used in this study and assisted with recruitment, including Kristan Armstrong, Kendall Beals, and Lauren Hall. We also thank Beshaun Davis for his review and thoughtful comments on earlier versions of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is the result of work supported with resources and funding provided to Julia Sheffield for completion of the Worry Intervention Study Evaluating the Updating of Persecutory beliefs (WISEUP) clinical trial by the Vanderbilt University Medical Center Department of Psychiatry and Behavioral Sciences.