
Abstract
Personal therapy is a common mandatory element of counseling and psychotherapy training in the United Kingdom. Previous research has established that this practice provides trainees with a unique learning space but also is associated with financial and emotional costs. Furthermore, some argue that the practice of personal therapy is ethically questionable. At the heart of many relational modalities, such as Gestalt psychotherapy, lies the relationship between client and therapist and more research is needed to explore how trainees perceive established training methods. The current study recruited 11 trainee Gestalt practitioners and conducted one-to-one semi-structured interviews to explore their experiences of engaging in personal therapy. A number of themes emerged in reflexive thematic analysis: trainees perceived personal therapy to be associated with professional and personal gains as well as financial and emotional costs; they also viewed personal therapy to be an essential component of their training but would like to be involved in discussions around how it is shaped. We recommend that training providers and professional bodies offer such a dialogic space, and that future research and practice further considers the barriers of minority clients and trainees in particular.
In the United Kingdom, the United Kingdom Council for Psychotherapy (UKCP, 2019a) and the British Association for Counselling and Psychotherapy (BACP, 2021) accredit therapeutic training offered by well over 100 providers. Accreditation is associated with an evaluation of theoretical and practice-based aspects of training and lays out both what the provider should deliver as well as the kind and amount of experience trainees are expected to gain while studying to become a therapist. In the case of the UKCP, attending personal therapy, i.e., being the client of a fully qualified psychotherapist practicing the same modality as the trainee is studying, is a requirement for completing accredited training, while in the case of the BACP, it is up to training providers to determine whether and to what extent their trainees should engage in personal therapy.
Personal therapy is often argued to be a necessary component of therapy training, offering crucial insight and personal growth which complement academic and practice-based learning and cannot be achieved quite as effectively through any other means (Murphy et al., 2018; Norcross, 2005). The research literature delivers support for these claims, reporting that personal therapy has a positive impact on therapists’ emotional well-being and perceived ability to be in service of their clients (e.g., Åstrand & Sandell, 2019; Grimmer & Tribe, 2001; Messina et al., 2018; Oteiza, 2010; Råbu et al., 2021; Rizq & Target, 2008). Conversely, it has been argued that attending personal therapy alongside training can adversely impact client outcomes as trainees become preoccupied with their own personal issues (Macran & Shapiro, 1998). Furthermore, research has reported negative impact on trainees themselves, including psychological distress, marital and family stress (Macaskill & Macaskill, 1992), as well as experiences of harm in therapy (Pope & Tabachnick, 1994). This has led some providers of therapeutic training to reject the practice of personal therapy, owing to a lack of evidence base and potentially harmful consequences (e.g., The Human Givens College). It is noteworthy, though, that most of the literature suggesting personal therapy to be associated with mainly adverse consequences is fairly dated and does not seem to reflect the current landscape of therapeutic practice. Recent studies on this topic commonly report both considerable benefits as well as costs (e.g., Ivey & Waldeck, 2014; Moller et al., 2009; Murphy et al., 2018). Furthermore, it has been found that feelings toward personal therapy may differ depending on a trainee’s background and theoretical orientation (McMahon, 2018) and that any positive impact of personal therapy on a trainee’s clinical work may be moderated by their sense of satisfaction regarding their personal therapy (Li et al., 2024). Crucially, at the heart of the controversy surrounding whether personal therapy should be mandated, lies an ethical debate (Edwards, 2018; Malikiosi-Loizos, 2013; Murphy et al., 2018), emphasizing the importance of dialoguing about it. To adopt the phrasing of the UKCP (2019b) Code of Ethics and Professional Practice, like others we question whether there is a conflict between respecting the (trainee) client’s agency and the requirement for personal therapy; or is personal therapy a justifiable intervention considering the ethical responsibility of therapists to ensure they are mentally well and competent? As noted previously, the answer to this question is likely multifaceted, including benefits and costs as well as practical considerations and their consequences. Particularly the financial burden of personal therapy is one of the highest in the case of UKCP-accredited training, significantly increasing the cost of training. This raises several concerns related to the accessibility and sustainability of training (Rizq, 2011; Sarmiento Verano, 2024). Therefore, further scrutiny of this practice, amplifying the voices of trainee practitioners, is essential for the future development of an evidence-informed and, ideally, bursary-supported psychotherapy curriculum.
Gestalt Therapy training offers an interesting case study of this debate due to the modality’s emphasis on relationality and how training is commonly offered in the United Kingdom. Gestalt Therapy is a form of humanistic psychotherapy that encourages awareness of how past, present, and expected future events affect one’s experiences of the here-and-now. This is achieved through paying attention to a client holistically, that is, to what they say, their body process, and how they make contact with their environment, including with their therapist (Perls, 1969; Perls et al., 1951; Spagnuolo Lobb, 2020). Change is thought to be a byproduct of encouraging awareness and acceptance of a client’s here-and-now experience (Beisser, 1970/2013). Although it is possible to train as a Gestalt therapist with resulting BACP accreditation in the United Kingdom, the majority of training providers offer training that can result in a full clinical membership with the UKCP (e.g., Scarborough Counselling & Psychotherapy Training Institute, The Gestalt Centre, The Metanoia Institute, The Welsh Psychotherapy Institute). As such, most (if not all) trainee Gestalt therapists in the United Kingdom attend personal therapy. Surprisingly, while some studies discussed above have included Gestalt therapists in their participant pool (e.g., Oteiza, 2010; Rizq & Target, 2008), or even focused on them specifically (Maruniakova et al., 2017), we were not able to identify a study that specifically focuses on Gestalt therapy trainees’ experiences of attending personal therapy.
In summary, mandating personal therapy is common practice associated with counseling and psychotherapy training. While the evidence for it is mixed, there appears to be a consensus in the literature that personal therapy does positively support the process of training. However, the practice is associated with a substantial emotional and financial burden, with the latter contributing to the inaccessibility of therapeutic training in the United Kingdom. Relational forms of psychotherapy may be especially relevant to consider in this context, given that personal therapy has been reported to foster relational warmth (Messina et al., 2018). The current study sought to explore Gestalt therapy trainees’ experience of attending personal therapy through individual interviews with a particular focus on the impact of the practice on trainees’ development as a relational therapist.
Method
Ethics Statement
In line with the BACP (2018) Ethical Framework for the Counselling Professions, the plans for this research were reviewed by an independent research ethics committee at King’s College London, which granted this study with full ethical approval, Ethical Clearance Reference Number: LRS/DP-22/23-34000. All participants provided informed consent through an online questionnaire.
Participants
Participants were invited to take part in this study through convenience sampling. Information was posted using the #TherapistsConnect on X (Blundell, 2021), on the message board of The U.K. Association for Gestalt Practitioners, a WhatsApp group for Gestalt psychotherapy trainees studying at The Metanoia Institute, and on the internal Moodle site for students at The Metanoia Institute.
The participants were 11 Gestalt psychotherapy trainees, all of whom were in the clinical stage of their training (i.e., second year or above) studying on UKCP-accredited courses. The age range of participants was 28 to 52 (M = 38.55, SD = 7.68), and our pool included eight females, two males, and one participant identifying as non-binary. Most participants reported to be identifying as white (n = 9; five of which White English, Welsh, Scottish, Northern Irish or British), whereas two participants reported to have a mixed identity. Other demographic characteristics of our sample are summarized in Table 1.
Demographic Sample Characteristics.
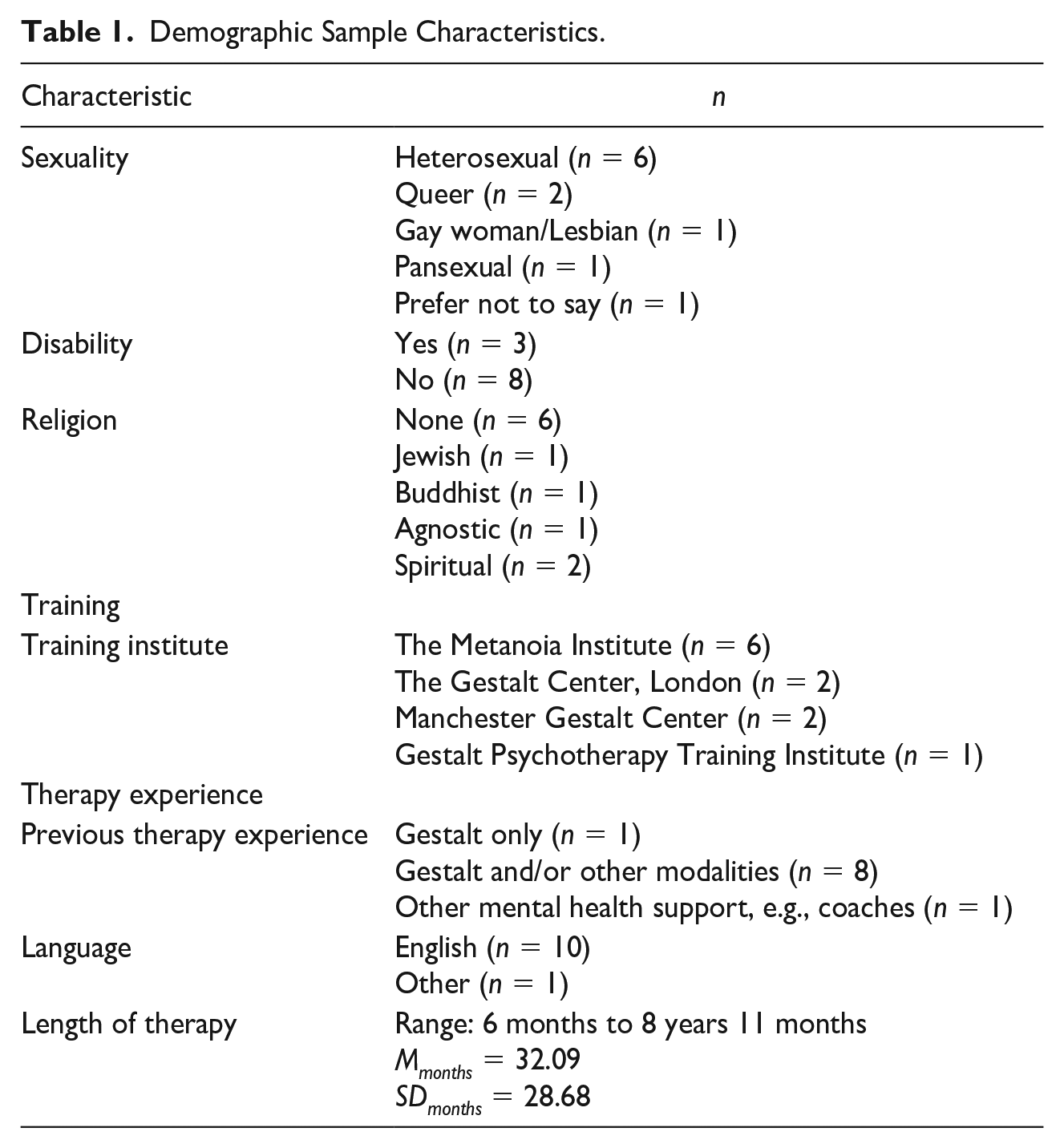
One participant was invited as a pilot participant to ensure smooth running of the study. Their data were included in the analysis reported here as the interview schedule did not change as a result of the pilot interview. All participants received £30 compensation for their time.
Researchers
The principal investigator of this research (JO) was a second-year trainee Gestalt therapists at the time the interviews took place. She was involved in designing the research, attending the pilot interview as well as a selection of other interviews, supervising the co-investigators, and preparing the final manuscript for publication. The co-investigators of this research (AC and ER) were final year undergraduate students with no formal training in counseling or psychotherapy. They were involved in designing the research, running the interviews, conducting the analysis reported here, and preparing the first version of the manuscript. Reflexivity was incorporated into the research process throughout by maintaining an open dialogue between the principal investigator and co-investigators, who had different levels of experience with psychotherapy. This was done in weekly hour-long relational supervision meetings to ensure a balanced perspective on the study design and data analysis.
Materials and Procedure
Upon contacting the principal investigator, participants were provided with a copy of the Participant Information Sheet for the study as well as the Consent Form and were offered to ask any questions they might have. Once informed consent was obtained, participants were invited to complete a short Qualtrics questionnaire (Qualtrics, Provo, UT) acquiring the demographic information presented in Table 1—this took no more than 10 min.
Interviews were scheduled at a time that was convenient for participants and led by one of the co-investigators. Sessions lasted between 30 and 60 min. All interviews took place online via Microsoft Teams, a platform which is considered to provide good data security given that appropriate precautions are taken (Jones, 2024). A further benefit is that Microsoft Teams offers automatic transcription. Transcripts were cleaned and checked for accuracy by one co-investigator following each interview; two transcripts were checked by both co-investigators. Interview recordings were deleted once this process was completed, in line with the study’s ethical clearance.
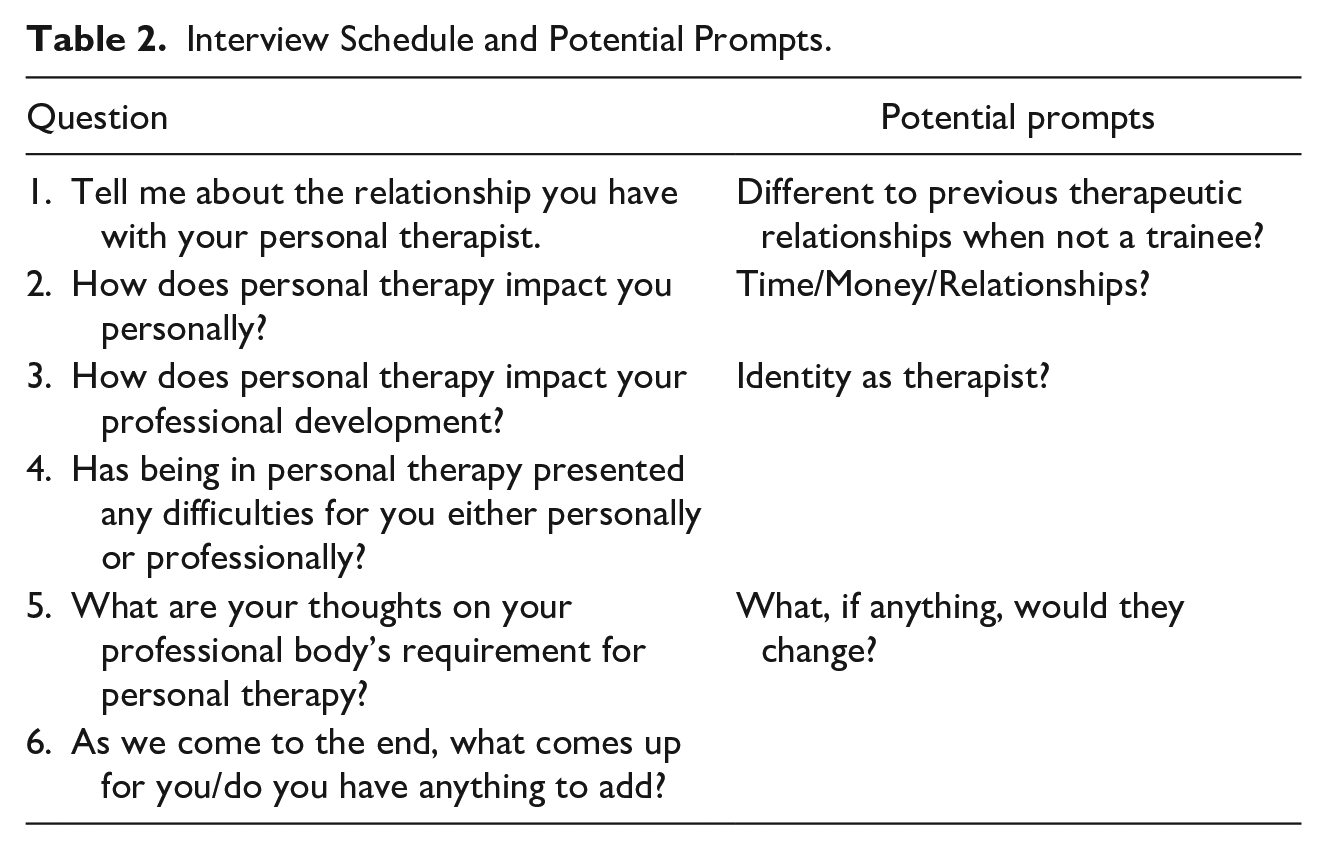
Interviews were semi-structured and followed the question catalog that is displayed in Table 2 alongside potential prompts. The questions were formulated in a manner that aimed to capture participants’ experiences holistically, informed by themes emerging from a review of the existing literature (e.g., Moller et al., 2009).
Interview Schedule and Potential Prompts.
Data Analysis
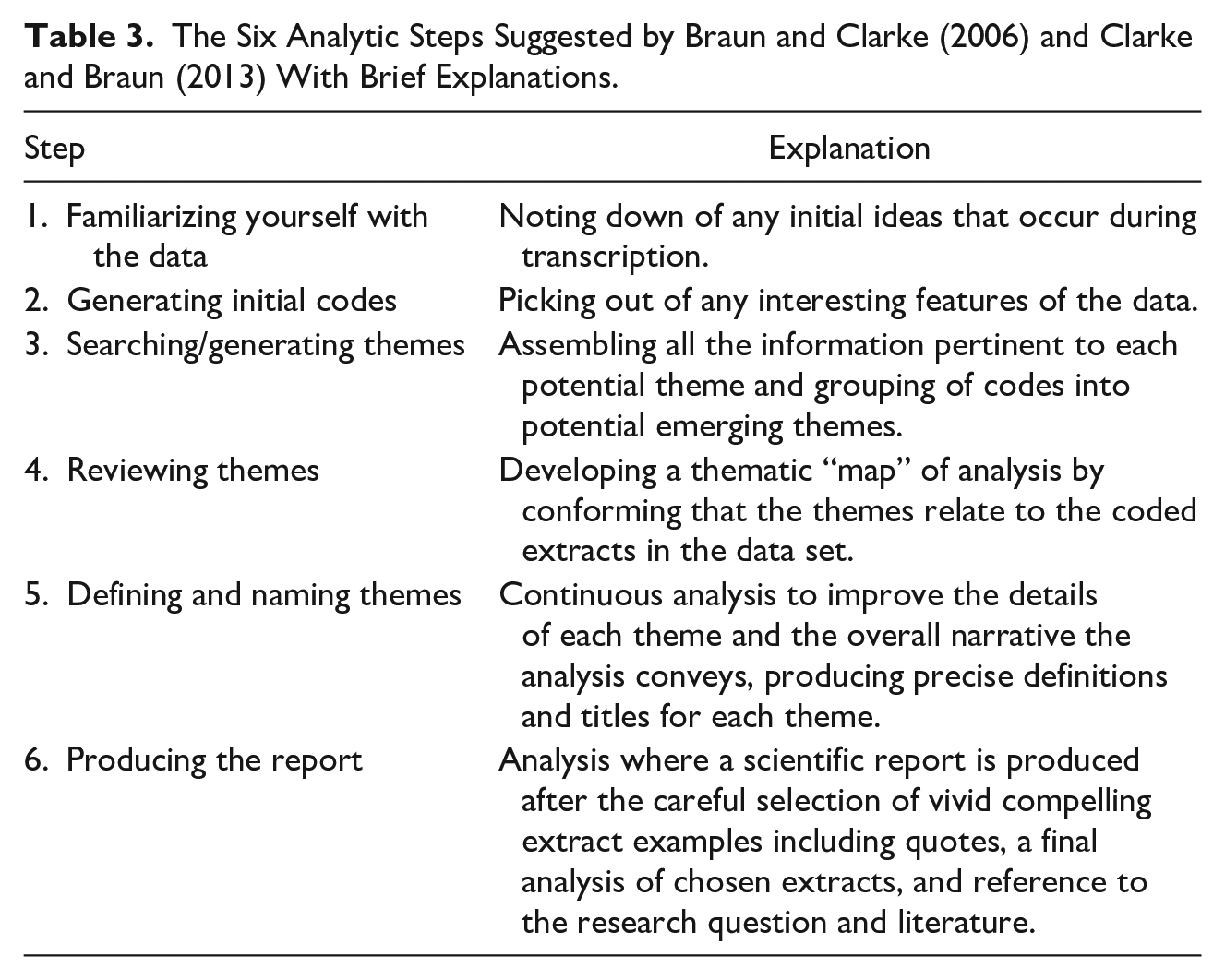
We followed Braun and Clarke’s (2006) six step guide to thematic analysis (TA) which entails going through the data set to identify themes and reoccurring patterns of shared meaning (see Table 3). More specifically, we opted for reflexive TA which values the researcher’s subjectivity as not just valid but a resource (Braun & Clarke, 2019). This is an approach which is commonly used in counseling and psychotherapy research and has been argued to particularly useful to interrogate societal structures and their implications (Braun & Clarke, 2021), which is arguably core to the research presented here. We also felt that reflexive TA aligns most closely with the Gestalt approach, which emphasizes the importance of what is co-created within the working alliance (e.g., Francesetti, 2015).
The Six Analytic Steps Suggested by Braun and Clarke (2006) and Clarke and Braun (2013) With Brief Explanations.
Being a trainee Gestalt therapist herself, the principal investigator continually reflected on the biases she brought to both the design and supervision of the investigation as well as its write-up for publication. Frequent reflective discussions were held within the research team with the aim to mitigate these biases. Co-investigators were actively encouraged to provide alternative perspectives and were put in charge of the TA of the data. These discussions allowed for a more critical engagement with the data and ensured that diverse interpretations were considered during coding and theme development. Throughout the analysis, the co-investigators’ own roles and experiences were reflected to ensure interpretations remained grounded in the participants narratives rather than imposing preconceived notions toward personal therapy (Drisko, 1997).
In the context of our study, inter-rater reliability does not concern the co-investigators’ level of accuracy regarding agreement on meaning between researchers, but rather the ability to cultivate deeper meticulous readings of the data (Maguire & Delahunt, 2017). Consistency of coding was acquired through attending the same qualitative workshops.
Steps 1 and 2 occurred during data collection as much of initial engagement with the data was completed through transcription of the interviews, before the full dataset was available. Following transcription, the co-investigators systematically coded the interviews. For each participant, code labels were coded, decoded, or even double coded. Coding can be semantic where the codes capture explicit meaning, close to participant language, or latent, more implicit or conceptual level of meaning (Boyatzis, 1998). At the beginning of the process, semantic codes were primarily used but as familiarity of the data set deepened, the use of latent codes increased.
The third step was originally referred to as “searching for themes” but is now described as “generating themes” which acknowledges the researcher’s active role in telling a latent story (Braun & Clarke, 2019). There are no hard and fast criteria on what constitutes a theme, but they are distinguished by their significance. By sorting codes into clusters of meaning, a refined set of candidate themes were generated through visual thematic mapping and continuous engagement with the data.
The initial thematic map of eight themes and 11 subthemes was modified in steps 3 and 4 to create a developed thematic map of four themes and seven subthemes. The relevant data for each preliminary theme were gathered and we reflected upon whether or not the data genuinely supported the theme. We then had to consider how well the themed fitted into the context of the full data set. In reviewing the collated data, it became evident that some of the themes were subthemes, and some subthemes were too “thin” and were either removed or integrated into other parts of the analysis.
Results
TA revealed three main themes, two of which containing multiple subthemes:
Furthermore, a theme emerged around the importance of the therapeutic relationship. While this is an important theme in the therapeutic literature more generally (e.g., Lambert & Barley, 2001; Spagnuolo Lobb, 2015), we do not believe that this theme substantially contributes to our understanding of the research aim of this paper, which is around the perceived impact of personal therapy on the training of relational therapists. We, therefore, report the analysis of this theme in the Appendix.
Personal Costs
Financial Constraint
Six trainees noted that personal therapy was financially taxing, even for those who saw their therapist at a discounted rate. Conversely, four participants stated that they were in financial positions where the cost of personal therapy did not pose any issues, and that it was “money well spent,” and two trainees expressed their awareness of the financial privilege that comes with training.
The financial pressure was reported to bring on secondary challenges, such as the potential of having to switch therapists when the financial situation changes, higher expectations for therapeutic outcomes that, if not reached, can lead to disappointment, and that paying for personal therapy sometimes took precedence over more general cost of living needs. Some trainees indicated that they would not pursue therapy outside of training due to the financial commitment: I probably wouldn’t be in weekly therapy if it wasn’t for training because it is so expensive over the course of the whole training. (Participant 7) I got an inheritance . . . and I’m using all of that to do therapy training basically, otherwise it would just be completely unaffordable for me . . . all of my savings, everything I have is going to therapy. (Participant 1)
Time Demand
Trainees discussed the challenge of balancing weekly therapy appointments with busy schedules, particularly for those working full-time outside of training: I’m also working so I have to squeeze the time into a busy schedule, and its added pressure. (Participant 6) Another trainee reflected on the impact of session timing, in that the overall amount of time spent in therapy and the time of day when sessions occur can be very demanding. We work at 8 o’clock in the morning. So that’s interesting because I often don’t feel I’m in a particular kind of emotional space in the morning. I think I’d be in a very different space at 5 o’clock you know? But that’s just the time that its most convenient to fit in. (Participant 7)
Yet, for three trainees, time demand was not a problem, especially for trainees with jobs outside of training where they have control over their own schedules. One trainee even mentioned attending more sessions if they could: . . . I do it more if I could . . . it feels like an investment in myself. (Participant 11)
Emotional Burden
Trainees described the emotional burden they experienced as both trainee therapists and clients in personal therapy. The “magnitude” of what participating trainees were learning in training while receiving personal therapy was described as “intense” and “overwhelming.” It was reported that it is “exhausting” to constantly look inwards when so many cogs and wheels are turning, especially during a time of personal difficulty. This made it difficult for the trainees to remain motivated to seek therapy: I feel like therapy has opened a can of worms and for as much as it’s amazing, it is difficult. It’s difficult to work through things. (Participant 9) I cannot for the life of me sit in another space where I have to explore things in myself, it just feels like I’m constantly turned inside out, and my nerves are on the outside and everything that touches me I have to react and explore and go in deeper in therapy. (Participant 12)
Vital Part of Training
Impact on the Self
The role of personal therapy in enabling personal growth and development of the self was identified as a significant contribution to practice by the majority of trainees. Most trainees reported a positive impact on the self as a result of “self-reflection,” “increased awareness,” and a “deeper understanding of the self.” This enabled trainees to develop the robustness and resilience required as human beings to complete the training and become excellent practitioners: Being more self-aware is fundamental to being a good therapist, and personal therapy is one way in which you can cultivate that. (Participant 7) I felt like I didn’t know who I was and now I feel like I have a much stronger sense of who I am and what I need and what I want. (Participant 4)
One trainee made a point about the significance of maintaining a balance among one’s many hats. In other words, it’s crucial to switch between receiving therapy as a client but also as a trainee, while maintaining a balance: it’s important for me to go between really treating it as therapy and then also zooming out and treating it as therapy as a trainee . . . it’s helpful for me personally to really bring myself and then bring my trainee hat self. (Participant 2)
Therapy Is Supportive
Personal therapy provided a safe space for trainees to deal with the emotional demands of their training, with the majority of trainees expressing that therapy provided them with a lot of support. It allowed trainees to reflect on their own process rather than their clients’ as typically done in training and supervision. A few of the trainees conveyed the possibility that Gestalt therapy has been more supportive than other modalities: I actually then sought out the Gestalt therapist because I was after more embodiment . . . wanting to work with someone who was able to bring me back to my sense of my own body and with the analyst . . . I found that useful but maybe not as supportive as I find my Gestalt therapist. (Participant 2) The type of program we’re on, it’s maybe more gentle than other programs. I thought I would be pushed so hard to discover myself, whereas it’s been gentler than I thought. So, in that light, personal therapy is even more important to me than I thought it would be. (Participant 1)
It was also reported that personal therapy supported personal relationships by encouraging trainees to communicate and be more honest with those around them which led to deeper but also more distanced friendships: I have a much greater degree of honesty and therefore closeness. I felt very lonely before and didn’t really feel close to the people around me, though they were there. But without that sort of honesty and emotional intimacy, and without expressing your needs, it’s really difficult to be close to people. (Participant 4) I think I can be more emotional and more open with my friends, and that helps to have deeper friendships. (Participant 1) It’s created challenges in resolving issues, that has come as a result of therapy. (Participant 6)
Integration Into Professional Practice
Trainees frequently reported that experiencing therapy as clients was crucial to their professional development, allowing them to integrate their therapists’ ways of working into their own therapeutic practice. Personal therapy provided them with a deeper understanding of therapeutic techniques and the client experience, which they could directly transfer into their work with clients: I am able to utilise Gestalt language and hear the way she [personal therapist] uses Gestalt language and to check her understanding of Gestalt terms and Gestalt theory. So that’s been really helpful professionally. (Participant 2) I think working with the Gestalt therapist and seeing how they work, you are picking up stuff as well, just through that. (Participant 7)
Trainees expressed that being on the “other side of the chair” provided this experiential knowledge that enriches therapeutic practice more than any other aspects of training. Several trainees articulated reservations about having the “resilience,” general “self-resource” and “self-support” to work effectively with clients if they had not received personal therapy: The deeper I go with my therapy, I feel the deeper I am able to work and train as a therapist . . . The deeper I go with my therapy, the deeper I feel I can resonate and offer a rich kind of richness to my being and awareness and sense of I feel like I can hold them [clients] more. (Participant 9) How can you work with someone? How can you help someone to go really deep into their journey if you haven’t done that yourself? (Participant 8)
The experience of personal therapy appeared to have directly “fed” into trainees’ skills and development and, in turn, their client work as they have picked up on their therapist’s ways of working. Accordingly, trainees stated that when considering what is beneficial to them in therapy, they “model” themselves after their personal therapist, influencing their identity as a therapist: It’s fed directly into my own skills development and seeing how a qualified professional long experience therapist is working with me, and that’s gone directly into me working with my clients. (Participant 8) It impacts my identity as a therapist, I think. I’ve noticed myself sometimes in sessions, doing kind of similar interventions or like demonstrating my presence or empathy in similar ways that he [personal therapist] does. (Participant 3)
Mandating Therapy
Overall, the notion of personal therapy as a mandated requirement of training was supported by all 11 trainees who expressed their agreement and stressed the importance of such a requirement for becoming a good practitioner, emphasizing that it is “necessary” and “essential” and becomes a matter of “mental hygiene”: I am glad it’s a mandatory requirement . . . just to see how it is to work with the Gestalt therapist and to be the client and to have that experiential reality of long-term working in the Gestalt modality, yeah, I think is invaluable. So, I think even if it were optional, I think it should be strongly encouraged. (Participant 8) I think it’s very good that it is mandated because if it wasn’t then we would have lots of therapists out there who haven’t done the work on themselves, and I don’t think that’s ideal really, not for the therapist because he will be dealing with things that will be hitting blind spots, and if he has never worked on it then what’s he going to do with the client? (Participant 3)
Around half of the trainees agreed with the hour requirement, indicating that it is a “fair” and “manageable” amount, but one participant expressed concern about taking away the choice, implying that the experience of therapy may be more negative if trainees are less willing to participate or participate solely to complete training. This was not the case for the remainder of our sample set, as the general consensus was that it should be either mandatory or strongly encouraged: I think it’s a manageable amount of hours being in personal therapy once a week. I think any more than that, it’s not an experience, well it’s not a Gestalt experience. (Participant 2) I wouldn’t certainly suggest any less, and I wouldn’t necessarily suggest any more because of the financial costs and time it takes. (Participant 9)
Professional Agency
The speed at which recruitment for this study was concluded (less than 24 hr) and the feedback from participants in general made it evident that trainee opinions on the standards set by their professional body must be taken into consideration when investigating the role of personal therapy alongside their training. There was disagreement over certain aspects of the requirements. Some trainees identified several “holes” in the system where courses contain major blind spots. The system was characterized as “disintegrated” and “confusing” for some. Numerous trainees raised possible considerations on how to improve the professional body’s requirements. For instance, the requirements could be more specifically customized to each trainee and established on a case-by-case basis, allowing for flexibility in areas like number of hours. A perceived disconnect between the duration of training and the therapy requirements imposed by the professional body was highlighted: It all depends on the person as well. I think some people are quite self-aware whereas other people are not and could probably do with a lot more therapy than they have had. (Participant 7) For a shorter course, it makes sense that they would ask for less hours I would say. So, if they do a two-year training and then maybe 80 or 100 hours should be enough. (Participant 3)
There was also a case to be made for having multiple therapists throughout training, which could expose trainees to a broader range of techniques and therapeutic styles. Trainees argued that this would enhance their professional development by providing more diverse learning opportunities: It’d be good to talk about pros and cons of that [having multiple therapists], because I think that would be distinct pros of working with two therapists for over a bit more time and seeing how they operate differently in their technique and their approach in this manner. (Participant 8)
Trainees also voiced concerns over the form of therapy, particularly the online-to-in-person ratio. Some felt that online therapy, while bringing its own challenges, was convenient and altered altered the dynamics of the therapeutic relationship positively. Others expressed a desire for more flexibility in balancing online and in-person sessions: I feel like there is a different sense of intimacy that you get from speaking online, I guess you’re kind of closer to their face. It’s a smaller surface area, you’re not seeing their whole body or what you are seeing you see more of because you’re closer. (Participant 4) There is some flexibility around online sessions which I wish was a bit more because online work actually just brings up other things and opens up different areas for exploration and it gives that feeling of actually if I want to take a break, if I want to go on holiday and I still need to make up the hours, I still have the option to log in online and have my session. (Participant 12)
These reflections reveal that while personal therapy is recognized as crucial for training, the system in place has significant gaps that hinder its full potential. The rigidity of the requirements, the lack of individualization, and the limited opportunities for exposure to diverse therapeutic practices were all identified as critical areas for improvement. As we will elaborate upon further in the discussion, the diversity of responses received corresponding to Question 5 of our question catalog (What are your thoughts on your professional body’s requirement for personal therapy?) led us to conduct further research into this particular aspect in our lab.
Discussion
Personal therapy is commonly a compulsory element of therapeutic training programs in the United Kingdom. Indeed, there is an argument to be made that relational psychotherapy emphasizing the importance of relational warmth in therapeutic work may especially benefit from personal therapy as a core component of training (Messina et al., 2018). From a theoretical standpoint, this appears to be of particular relevance to Gestalt psychotherapy training. However, it is important to acknowledge that personal therapy is not universally regarded as a useful or even ethical practice (e.g., Human Givens College, 2024) and that the requirement does contribute to the inaccessibility of counseling and psychotherapy training (e.g., Sarmiento Verano, 2024). Given the limited and rather dated research on this topic, the current study sought to amplify Gestalt trainee practitioners’ views by conducting semi-structured one-to-one interviews enquiring about their experience of attending personal therapy as part of their training.
In line with previous research, we found that personal therapy presents trainee practitioners with a kind of double-edged sword: while it is experienced to be a highly useful element of training, it also comes at a considerable financial and emotional cost (Moller et al., 2009). We, the authors including one trainee Gestalt practitioner in personal therapy at the time of writing, encourage training institutes and accreditation bodies to seriously consider the implications that these costs have on the diversity of practitioners available to clients, especially in a time of prolonged societal financial hardship. The absence of regulation around fees means that people’s spending varies significantly, and this resonates more generally with established debates around the cost and benefit of different training approaches (Frank et al., 2020). Furthermore, our findings resonate with the often-reported phenomenon of the therapeutic relationship being of key importance in psychotherapeutic work (e.g., Lambert & Barley, 2001; Spagnuolo Lobb, 2015), and that trainees must feel heard and understood in an empathetic environment for personal therapy, as an arguably unique therapeutic practice, to be perceived as useful (Horvath & Bedi, 2002; Martin et al., 2000). This may speak to a modality-specific phenomenon or, indeed, provide support for the notion that at the heart of the trainee client lies still a client in their own right. We strongly encourage future work on the importance of the therapeutic relationship in personal therapy, an area which to our knowledge has mainly been explored on a theoretical level to date (Hill & Knox, 2009). Furthermore, this highlights the need for future research focusing on other modalities.
Where our research crucially adds to the existing body of empirical writing on this topic is the very strong feelings of trainees that personal therapy, with all its positives and negatives, is essential for psychotherapeutic training. To our knowledge, this is the first study demonstrating this with overwhelming clarity. Importantly, this delivers support for a mandatory personal therapy element but still highlights that work is to be done to ensure access to it is as equitable as it can be. The diverging views of our participants regarding their professional body’s requirement for personal therapy suggest the challenges that this brings and indeed prompted further research in our lab. Based on the current study, we cautiously make the recommendation of professional bodies and training institutes to consider whether current ratios of in-person versus online therapy justify the challenges that they pose.
Throughout this discussion, we have touched upon the argument that personal therapy may contribute to the inequity of accessibility of the therapy profession and, indeed, the main limitation of our study reflects this further. While our sample size can be considered reasonable for an exploratory qualitative study (Francis et al., 2010), we reflect that the majority of our participants were white, non-disabled, cisgender, heterosexual, not religious, and English native speakers. Considering the wealth of theoretical and empirical writing around minority stress being a unique phenomenon (Meyer, 2003), it is crucial that further research in this area focuses its efforts on amplifying the voices of minority clients, including trainee clients. Furthermore, there may be concern regarding a self-selection bias in our sample in a way that only trainees who are passionate about personal therapy signing up to this study. We believe that offering fair pay for participation counteracted this potential bias and further believe that our data do not give rise to concerns around this. However, we do encourage further work in this area to strengthen these findings, including larger-scale quantitative research.
In conclusion, the research presented here adds to the existing body of evidence suggesting that personal therapy is a useful, essential even, element of counseling and psychotherapy training. While it does not support the notion that it may be detrimental to trainee therapists’ professional development, it does also highlight that this practice comes at a notable cost. We believe that our findings make a convincing argument for more dialogue between trainees, training providers, and professional bodies regarding the limitations of the current system and proposals to move forward. Crucially, this topic represents an important element of issues around accessibility of therapeutic training, and both research and practice must be mindful of this, particularly when it comes to serving minority trainees and, correspondingly, clients. Essentially, so we argue here, the debate around personal therapy in training is one that should seek to establish the balance between the two identities of every trainee within the personal therapy space, namely, the trainee client’s agency and the trainee practitioner’s responsibility.
Footnotes
Appendix
Acknowledgements
We would like to thank the 11 participants who volunteered to be part of this study, without whom this work would not have been possible. We also would like to thank Drs Caroline Catmur and Rebecca Upsher who coordinated the Research Project module for the BSc Psychology at King’s College London, the context within which this work was carried out. Special thanks to Dr Upsher for providing training to Mr Cavanagh and Ms Root in thematic analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by bench fees associated with the BSc Psychology Research Project module at King’s College London. No other funding was used to support this work.
Ethics Statement
In line with the BACP Ethical Framework for the Counselling Professions (![]() ), the plans for this research were reviewed by an independent research ethics committee at King’s College London which granted this study with full ethical approval, Ethical Clearance Reference Number: LRS/DP-22/23-34000. All participants provided informed consent through an online questionnaire.
), the plans for this research were reviewed by an independent research ethics committee at King’s College London which granted this study with full ethical approval, Ethical Clearance Reference Number: LRS/DP-22/23-34000. All participants provided informed consent through an online questionnaire.