
Abstract
Many support schemes in current autism clinical services for children and young people are based on notions of neuro-normativity with a behavioral emphasis. Such neuro-disorder approaches gradually undermine a person, restrain authentic self-expression, and fail to address the impact of a hostile world on autistic well-being. Furthermore, such approaches obscure attention from a fundamental challenge to conceptualize an alternative humanistic informed framework of care for staff working with diagnosed or undiagnosed autistic children and young people. In this article, we offer an appreciation of the lifeworld-led model of care by Todres et al. We discuss how mental health practitioners can adopt an experience-sensitive framework of health care by incorporating the eight dimensions of care into practice. This neuroinclusive approach creates a culture of respect, honors the sovereignty of the person, prioritizes personalization of care based on collaborative decision-making, and enables practitioners to support well-being from an existential, humanistic view, grounded in acceptance of autistic diversity of being. Without a fundamental shift toward such neurodivergence-affirming support with practitioners being willing to transform their understanding, real progress cannot happen to prevent poor mental health outcomes for autistic people across the lifespan. This shift is needed to change practice across research, clinical, and educational contexts.
To reflect the language preferences of the majority of the autistic community (e.g., Bury et al., 2023; Kenny et al., 2016), this article uses identity-first language, that is, “autistic” and “autistic child or young person,” as opposed to person first language, that is, “child with Autism / with Autism Spectrum Disorder.”
Introduction
Many support schemes for autistic children and young people are designed to support them to fit in and conform with idealized notions of neuronormativity, “with the autistic lifeworld being invaded by a never-ending tide of interventions that try to eradicate autistic styles of diversity” (Milton, 2017). Rather than caring for the young person in a way that accepts and develops their individuality, these kinds of support often tacitly take neurotypical behavior as the standard to aim at and lead the autistic child or young person to mask their autistic traits and repress their atypical sensory and emotional reactions. While in the short term, it can lead to measurable improvements in adaptation to society and higher achievement, in the long term, it can lead to an increased mental strain, alienation from one’s authentic self, depression, and a higher suicide risk. Thus, we see the need for an approach to supporting autistic children and young people that is, by principle, grounded in acceptance of the autistic diversity of being and informed by autistic experience, which we elaborate on in this article.
The neuronormative interventions often stem from a neuro-disorder narrative that justifies targeting core traits by framing them as pathological (Yang, 2019). The consequence of a cultural narrative of tragedy, epidemic, and othering has resulted in the proliferation of interventions that have been justified as remedies, aimed at reducing the health, education, or economic “burden” of autism (Baxter et al., 2015).
Almost 100 years after Sukhareva, in 1925, described children with “autistic tendencies,” specifically social/affective differences, stereotyped mannerisms, and sensory sensitivities (Sher & Gibson, 2021), the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013) criteria maintained the disorder framing of autism as “persistent deficits in social communication and social interaction across multiple contexts as well as the presence of restricted and repetitive patterns of behavior.” In the intervening years, Kanner (1943) defined “infantile autism” as a rare condition. Asperger (1944) described autistic psychopathy. He recognized the social value and potential for social integration for his patients who were of “high intellect,” whereas those labeled “feeble-minded” or “mentally inferior” were segregated (Pearson & Rose, 2023). Unfounded accusations of “refrigerator parents” (Bettelheim, 1967) left a legacy of parental blame that still proliferates (Clements & Aiello, 2021). While previously mothers were held responsible for causing autism, they are now held responsible for a lack of remediation from it (Douglas, 2014). Psychogenic theories of autism were refuted, with evidence of a neurodevelopmental condition that was treatable (Rimland, 1964) and subsequent treatments for autism followed (e.g., Schopler & Reichler, 1971). Lovaas (1987) reported 47% “recovered” children, who made substantial improvements in IQ and adaptive and social skills following intensive behavioral treatment, which involved “treating autistic children during most of their waking hours for many years.” Autistic children have been subjected to a vast range of “pseudo treatments” such as “packing,” holding therapy, secretin, hyperbaric oxygen, fecal transplants, oxytocin, and injections of stem cells (Pukki et al., 2022). The search for explanations for an autistic person’s existence, even cures, has perpetuated the dehumanizing autism narrative.
The work of Wing and Gould (1979) led to autism being described as a “triad of impairment” with a continuum of functioning from “socially impaired” to “sociable severely retarded,” and autistic interaction given pathologizing descriptors, such as “aloof,” “passive” and “odd.” Cognitive theories propagated further notions of impairments, proposing that autistic children lacked a theory of mind (Baron-Cohen et al., 1985), could not “get the gist,” (Frith, 2003), and had executive functioning deficits (Ozonoff et al., 1991). None of these theories satisfactorily explained autism but they continue to influence research and practice which focuses on neuronormative skill development (e.g., Fridell et al., 2023; Holopainen et al., 2019). However, these skill development programs can teach or normalize masking—the camouflaging of autistic traits. Yet masking has been shown to result in increased feelings of thwarted belonging, which in turn is correlated with suicidal thoughts and behaviors (Cassidy et al., 2020), with suicide being a leading cause of death in autistic people (Hirvikoski et al., 2016). The products of the disorder narrative of stigma and prejudice have rendered society ignorant of autistic forms of thriving and what a good autistic life would look like (Chapman & Carel, 2022). The predominance of research produced by non-autistic researchers, taking an outsider view of autism, has impeded clinicians from reflecting on and developing support based on the insider perspectives and voices within the autistic community.
The deficit model fails to address the impact of a hostile world on autistic well-being. Autistic people experience minority stress, being exposed to more stressful life situations, including acts of discrimination, social exclusion, victimization, and internalized stigma, due to being a neurominority. This leads to diminished well-being and increased psychological distress (Botha & Frost, 2020). Crane et al. (2019) found that 80% of young autistic people with co-occurring mental health problems were less likely to seek help due to high levels of stigma associated with both autism and mental health problems. Shaw et al. (2023), building on results from previous studies looking at health care barriers encountered by autistic people, found that patient–provider communication challenges and sensory issues contributed to self-report adverse outcomes. Even with the increase in autism specialists and neurodevelopmental pathways, services remain unlikely to meet demands; therefore, a responsive and universal framework of care, offering personalized and meaningful support, could ensure a more effective and less traumatic journey navigating health care.
The dominating “autism as disorder” narrative limits professionals in their understanding of diverse ways of being and ways of responding to distressing life events. The pathologization of autism means that health care professionals can often reduce all poor mental health outcomes, such as anxiety or self-harm, to “symptoms” of autism itself. The lack of holistic thinking, or tendency to treat all negative outcomes as evidence of autistic pathology, can serve as an additional barrier to help-seeking for autistic people. The belief that distress is part of being autistic regardless of the cause, that it is something the person must tolerate, or learn to live with rather than have support to reduce can have potentially dire outcomes. Something has to change (Crane et al., 2019) so that autistic people receive affirming and therapeutic support for their needs which addresses their distress.
Shifting From Disorder to Neurocognitive Difference and Disability
The emancipatory aims of the neurodiversity movement and the neurodiversity paradigm (Walker, 2021) have led to a positive shift in attitudes toward autism. Autistic-led and co-produced research along with a variety of biographical accounts of autistic experience is changing the narrative, centering autistic perspectives and priorities, and this is contributing to the paradigm shift from disorder to neurocognitive difference or disability. This now paves the way for creating a society where autistic people flourish (Chapman & Carel, 2022). Realize moving from neuro disorder to neuro inclusive practices humanistic values in clinical practice an experience-sensitive framework of health care will guide clinicians to draw on non-deficit-oriented concepts defined by autistic scholars and embraced by the autistic community such as the “double empathy problem” (Milton, 2012) and monotropism (Murray et al., 2005) will help professionals understand the autistic experience better and make their practice more neurodivergence-affirmative. The “double empathy problem” refers to a breakdown in mutual understanding between any two people; yet it is more likely to occur when people of very differing dispositions attempt to interact (Milton et al., 2022). Rather than an “empathy deficit” located solely within the autistic individual, this frames the social disjuncture as a result of “cross-neurotype” differences in communication and lifeworlds. Monotropism is a theory that describes how autistic people’s attention is pulled to focus on one or few interests at any time. This core characteristic of autistic cognition influences information processing and communication styles. These autistic-led theories enable systems of support to see autistic people in both agency and vulnerability positions (Pavlopoulou, 2020) and draw attention to the social determinants that significantly limit their participation and impact their health and well-being. Rather than defaulting to treating “deficits,” the clinician is enabled to adopt an experience-sensitive approach, viewing the child or young person as an expert in their own experience, supporting them and/or their family members, to co-create plans of support, and addressing barriers and stressors in the environment.
At present, micro traumatic relating pervades autistic lives and silences, excludes, and marginalizes (Golan et al., 2022; Rumball et al., 2021). Here, we refer to the seemingly benign, almost invisible, hurtful everyday messaging that communicates impairment and otherness. Being seen as a risk to be controlled or as something in need of fixing inflicts damage habitually, gradually undermining a person and can (re)traumatize and/or further restrain self-expression. Too often autistic young people’s unique, expert knowledge is cast aside, and the child or young person becomes exhausted trying to convince clinicians of their perspective, defending against expertise based on preconceived, erroneous medicalized, or neuronormative ideas. It is therefore essential that from the earliest opportunity, something “over and above” the all-knowing approaches of objectification and medicalization are offered as these take power over and likely increase distressed behavior (Quinn, 2018). Practitioners must bring their humanity, abandon any aloofness in their persona, and learn to see beyond otherness. Adopting a stance of unknowing, rather than knowing, supports practitioners to encounter the person “in a very personal and profoundly human way” (Lietaer, 2001, p. 47). Something qualitatively different can occur for autistic children and young people when practitioners enter a relationship without expectation and shift their focus from “treating autism” to focusing on the autistic child or young person and their unique lived experience. By practitioners being genuinely curious about autistic perspectives and freeing themselves of normative ideals, autistic children and young people might feel more able to meet without masks or feel safe to begin processing or relating more authentically. Teams that embed the social model of disability and a neurodiversity-affirming approach can create a culture of respect, honor autistic ways of being, prioritize personalization of care based on collaborative decision-making, and in doing so, promote epistemic agency (Chapman & Botha, 2023). That is, they can honor autistic children and young people’s ability to tell their own stories and control their narratives in ways that are meaningful for them.
An Experience-Sensitive Framework of Health Care as a Neurodiversity Affirming Approach
Shifting practice from looking at behavior to understanding someone’s experience fits within a neuro-inclusive approach, by supporting well-being from an existential, humanistic view. In this article, we offer an appreciation of the lifeworld-led model of care by Todres et al. (2009) and conceptualize an alternative humanistic informed framework of care for staff working with diagnosed or undiagnosed autistic children and young people; the experience-sensitive framework of health care. Although our conceptualization is not new, we believe that it is timely to re-consider clinical care from this existential view of well-being to provide a direction for neuro-affirming care and practice for diagnosed and undiagnosed autistic children and young people, recognizing that many enter the system without a diagnosis and are delayed in accessing formal diagnosis (Crane et al., 2016; Malwane et al., 2022). We echo the critiques of the neurodiversity paradigm in current policy and practice as expressed in many behaviorally oriented clinical competencies, for example, PBS Clinical Competence Framework (2015). Our critique focuses on how the behavioral emphasis in many current autism clinical services obscures attention from an essential challenge to conceptualize an alternative humanistic/existential informed framework of care. A fundamental mind-shift is needed to change practice across research, clinical, and educational settings. Without this, real progress cannot happen to prevent poor outcomes for autistic people across the lifespan (McVey et al., 2023).
The lifeworld care model forms the basis of a value-based theoretical framework for considering the spectrum of possibilities in providing potentially humanizing through dehumanizing care and interactions (Todres et al., 2009). The humanizing framework, underpinning the experience-sensitive framework of health care, is compatible with the social model of disability and places individuals at the center of care and considers how support can uphold the key aspects of what it means to be human, as outlined by the eight dimensions of care. Embedded within these dimensions are some essential principles for practice; a collaborative approach, flexibility, accessible communication, and personalization of support based on a deep understanding of the person and their circumstances. The experience-sensitive framework of health care has broad application, promoting a good practice that creates a culture of respect; honors the sovereignty of the person; enhances dignified, individualized, and meaningful care or support (Hemingway et al., 2012); and enables practitioners to support wellbeing from an existential, humanistic view, grounded in acceptance of autistic diversity of being. The “experience sensitive approach” (Pavlopoulou, 2020) promotes a sense of agency and identifies strengths, barriers, and needs to support well-being and to create opportunities for the person to flourish authentically, living their best life, according to their own norms.
As a group of neurodivergent experts by science and experience, we describe how the eight dimensions could be incorporated into community mental health services by practitioners.
Insiderness/Objectification
The dimension of insiderness recognizes that we each have a personal world that carries a sense of how things are for us. Only the individual themself can be the authority on how this inward sense is for them. This authority may be tentative and unspoken in children and young people as they develop language and concepts to make sense of their inner world, including those areas not yet explored. Objectification treats someone as lacking in subjectivity, or as a tool or object lacking agency, to be used (LaCroix & Pratto, 2015) and can occur when the young person is reduced to a label, a list of symptoms, a diagnostic category, or is seen as a risk because of their diagnosis, or another “case” or statistic. Objectification denies the inner subjectivity of a child or young person, removing their full humanness or agency, while treating their inner world as thin or non-existent. Objectification from others can result in self-objectification or dehumanization (Calogero et al., 2011).
Practitioners are encouraged to be intentional about cultivating compassion, connection, and curiosity. The practitioner must humbly seek and value the subjective experiences of the individual, starting with seeking an understanding of the young person’s hopes, fears, and struggles. Being facilitated by an interested other to express one’s own experiences and having those validated is essential to building a collaborative therapeutic relationship. Through conversations or interactions that center on the child or young person’s experiences, emotional safety is cultivated, and the child or young person can feel seen, heard, and understood. To avoid assumptions and misunderstanding, practitioners must recognize their own biases and lack of understanding when they seek the young person’s views, such as, “What is your view on this experience?” “Why do you think it was that way?” and “How did that make you feel?” Acknowledging that each individual may be imagining or experiencing things differently and being curious about the other’s view can build a bridge for both to cross, for example, “I am imagining it like this, and I wonder how that compares to what you have in mind. Can you help me to see in the way you do?”
Importantly, we should also acknowledge that part of what a child or a young person holds inside is their interpretation of how others see them on the outside, so they will come up with stories about how they think we or others see them that in turn have an impact on how they feel they can or should act or how they are expected to act. This may create masking as a trauma response (Pearson & Rose, 2021). Practitioners should check with the child or young person regarding their understanding of why they have come to the service if in fact they had been consulted at all and check that matches with the expectations of the practitioner. Assumptions from both parties can be examined while confirming that the child or young person’s motivations arise from their needs and desires and are not due to external pressure to “fix” their autism or please others by trying to normalize autistic core traits. Autistic young people may be used to being blamed for what is a mutual breakdown in understanding or reciprocity and have internalized other people’s push toward “fixing” themselves as an antidote to this breakdown in communication. Take time to explore how asking for help is understood, and what that looks like for the child or young person and what they hope for in receiving it. Use a personalized approach to support a child or young person to describe their experiences such as identifying sensory needs and difficulties, and using alternative modes of communication, as necessary—this inherently acknowledges their subjectivity. Being creative and patient is key as there is no one-size-fits-all strategies or toolboxes that will work for all.
This approach will span all points of collaboration, from initial identification to specific support as required or requested. Post-diagnostic support could focus on moving from the context of medicalized aspects of diagnosis to arrive at a collaborative formulation that promotes the individual in their self-discovery of their neurodivergence. This could also be extended to engagement with the young person’s family, to support a broader neuro-affirmative approach which may create environments that are more receptive to autistic ways of being.
Agency/Passivity
Being human involves being able to make choices and to be generally held accountable for one’s actions. Having a sense of agency is closely linked to a sense of dignity. Agency affords the possibility of freedom to be and act within certain limits. In contrast, passivity is created by internalized or imposed attitudes and practices that make the young person a passive recipient of support or treatment, leading to a diminished sense of personhood, a loss of hope and/or increased feelings of distress.
Agency is promoted within a therapeutic relationship approach when autonomy is facilitated, and support and advocacy are proactively offered. Individualized supports are offered instead of the unthinking application of a standard “treatment” program or “off the shelf” strategies. The practitioner makes space for the individual to express their wishes as far as they are able, including those occasions when the young person does not yet know, without imposing a perceived but not shared understanding. Feeling safe to not know may create a more secure path toward self-discovery. The child or young person is invited to express what they need to feel comfortable in the clinical space, such as where they sit, having options to stand and move, and having access to anchoring objects or activities or the presence of an anchoring person. Addressing difficulties in the environment that affect the child or young person can create a sense of empowerment and safety. For some, this will reconceptualize the “therapy context.” The clinical room itself can create inaccessible barriers for those who feel more able to connect with their feelings and experiences when in nature. Walking and talking may enable easier communication. Accessible communication increases opportunities for agency and self-advocacy. Communication styles and preferences are valued, for example, verbally, pen and paper, or asynchronous formats. The practitioner listens earnestly to what the person has to say, takes care to interpret tentatively, and checks for understanding. The child or young person’s views are accepted as significant. Informed consent is essential. The young person’s “voice” is in each piece of work. This is in contrast to activities or assessments that are completed in a “tick box” approach, similarly, diminishing engagement and understanding for children and the professionals working with them. At a service level, the agency is increased through co-production to shape service development.
Uniqueness/Homogenization
To be human is to actualize a self that is unique. Each person’s uniqueness is a product of their relationships and their context. Recognizing the child and young person’s characteristics, attributes, and roles (e.g., age, gender, ethnicity, class, friend, son, and student) honors and supports them in their journey toward a flourishing life and is essential for well-being. Homogenization erodes identity by focusing on conformity and norming. The individual’s strengths are overlooked in favor of the demands to do things in the same way as others. Homogenization risks the autistic child falling into the role of “good patient” and becoming susceptible to an unchecked power dynamic that limits creativity and reduces the likelihood of achieving a synergistic therapeutic relationship.
For a child or young person to grow in the rich and varied aspects of their identity, they need environments where they are accepted and receive unconditional positive regard and genuine empathy. By developing an understanding of the young person’s experiences and by accepting their emotions as valid, practitioners develop a greater capacity for compassion and empathy. The young person’s reports of distress are understood in context and accepted even if their expressions do not match with the practitioner’s expectations. Information is personalized and represents a young person’s evolving cultural and social identity in full, including, for example, their gender identity, support plans, an affirming post-diagnostic letter, or a communication passport. The young person is supported to build self-knowledge and self-understanding while building toward and supporting self-advocacy. Autistic communication and processing styles are recognized, accepted, and accommodated, affirming an important aspect of the individual’s uniqueness. The practitioner is curious about the young person’s life and interests. Conversations should be initiated with the awareness that, for some young people, question types may need significant adaptation and for others, too many questions may be experienced as threatening or uncomfortable. When the right questions are asked but do not result in the desired effect, the responsibility may once again be attributed to the child for not engaging, starting with the presence and relational depth as defined in Quinn et al. (2023) and allowing time to adjust and trust. Being prepared to take it slow and making engagement itself the priority rather than what is talked about is an invaluable expression of the clinician’s interest in the young person rather than the procedures to be followed. Use of photos, pre-recorded voice notes, and drawing or sand tray or simply doing activities, like LEGO or kinetic sand while talking, may help some children and young people to self-regulate. Reducing the normative communication demands, such as maintaining eye contact and providing opportunities for soothing repetitive or sensory experiences to be naturally integrated may reduce the complexity of the interpersonal and cognitive demands and help the child or young person to retain a degree of control. Tailored support programs can be developed and adapted in response to feedback and the progress or lack of progress achieved, according to the child or young person’s perspective.
Togetherness/Isolation
A person’s uniqueness exists in relation to others and in community with others. Through relationships, practitioners and the children and young people they work with have the opportunity to learn more about themselves, through both commonalities and differences. Inclusive practices nurture a sense of belonging and connection. Togetherness is experienced through building bridges of understanding and empathy to validate the young person’s suffering, struggles, strengths, and perspectives. Creating a safe place for the young person to share their worries and joys is important to allow them to reflect on their impact across different contexts of their life. Isolation occurs when the young person’s everyday social connections are disrupted or severed. A child or young person may experience alienation and othering in environments when the support they need is not offered, is offered in a way that stigmatizes them, or restricts their freedom to be authentic or express themselves. Restrictive practices, such as seclusion and restraint, common in services that operate an institutional culture, significantly risk health and well-being and impact a sense of human belonging for both the young people and the staff involved.
Practitioners use a relational and compassionate approach to curate a sense of acceptance and belonging. This is always important, and especially so when supporting those who have been subjected to restrictive and traumatic practices. Trauma frequently happens interpersonally and its impact has the greatest potential to be revisited and healed in safe, reparative relationships. Practitioners should work to create a sense of safety and trust, through consistency, transparency, and practice of “power-with” strategies, empowering the child or young person’s voice and ensuring meaningful choice through a collaborative process. This work in partnership will help both to discover ways that help the young person to regulate their nervous system individually and interpersonally.
Delivery of effective clinical plans relies on understanding the child or young person’s life experiences; exploring experiences of home life, friendships and school with the young person, and, importantly, what they need to access the human experiences of privacy, human connectedness, and intimacy; and acknowledging the layers of marginalization (gender, sexuality, race, and class) that may have affected their experiences of diagnostic and post-diagnostic supports and interactions with professionals. Autistic young people who have other marginalized identities may benefit from access to community members, organizations, groups, or information where they can find peer support, acceptance, and validation, for example, LGBTQIA+ youth groups, autistic-led mentoring programs, Chinese Autism (an autism support group for the Chinese community). Practitioners should ensure that they and the young person have a range of ways to learn about autistic experiences, culture, and communication. Difficulties in relationships may require perspective-taking work for the autistic young person and their family members or other relevant people/professionals in their life, offering an opportunity for all to reduce the double empathy gap without the assumption that the autistic young person is responsible for all social or relationship discord simply because they are autistic. Prompt resolution of access barriers that fail to consider language or literacy needs, or the ability to use a telephone to book appointments, can help young people and their families who use the service feel welcome. Interpreters and translation of documents should be provided whenever required to facilitate the child or young person’s and parent/carer’s involvement and understanding.
Sense-Making/Loss of Meaning
Sense-making involves a motivation to find meaning and significance in things, places, events, and experiences. The child or young person is viewed as the nascent storyteller and storymaker of their own life. Autistic ways of being and perceiving are understood as intrinsically meaningful and help formulate a view of the young person’s lifeworld, their health, well-being, and identity. Listening openly to autistic interpretations of experiences in a relational way supports the young person to make sense of their world so they can define their experiences and reflect on how these experiences have shaped them. When sense-making is obstructed in varying degrees, the young person can experience a sense of dislocation and meaninglessness. This can happen when the individual has inaccurate or misleading stories told about them by other professionals or family members which shape their understanding of themselves. When advice is given or treatment models are shared without contextual understanding, or with little relevance to the young person’s life and circumstances, a disconnect can occur resulting in disengagement or loss of trust in the professional. When human beings are reduced to numbers and statistics, the sense of the individual is lost in the system and the standardized practice is not experienced as care.
Practitioners can deepen their understanding through careful exploration of the young person’s sensory experiences and recognition of stimming as a valid way to process and regulate emotions. Ensuring that adequate space and privacy are provided will help to create an environment in which children and young people can feel safe enough to express themselves, their needs and preferences, and to reflect on their past experiences without normative pressures.
Physical space is complemented by the emotional space created by supportive silence in exchanges to build connection and allow time to process even if this time might seem inordinate or uncomfortable to practitioners who may not be used to extended silences. Meaningful and accessible modes of communication can also be used to help with sense-making, such as photo stories, objects, music, movement, or media. In a collaborative process of sense-making, practitioners accept the communicative value and seek to understand all forms of expression, from swearing, to partially constructed sentences, and to unfamiliar or unexpected body language.
Humanizing language is used in report writing, case discussions, and support plans, with full knowledge that the child or young person may be exposed to what is written about them, and regardless deserve to be respected even if they never are. Practitioners explain the therapeutic plan and rationale so that the child or young person understands their situation, and options, and has the opportunity to ask clarifying questions.
Personal Journey/Loss of Personal Journey
To be human is to be on a journey. Understanding how we are at any moment requires the context of the past, present, and future, and ways of bringing each of these parts together into a coherent or appreciable narrative. A child or young person can and should be able to simultaneously feel secure in connections to the past while moving into the unfamiliarity and uncertainty of the future. Every child and young person, and their family, entering mental health services embarks on a journey that involves uncertainty and often worries for the future. The personal journey is diminished if health professionals fail to pay attention to the child or young person’s history and or future goals and hopes, relying instead on assumptions based on a “snapshot” of the young person’s life at present. This can risk excessive focus on how the young person is, not who they are or what they want to achieve. Furthermore, discontinuity between care can mean that the child or young person is asked to endlessly repeat their history to each new person. This builds a cumulative impression that they are never heard, or that they are stuck in the past, making the repeated telling not only futile labor but feeding a sense of hopelessness or even retraumatizing them.
Children and young people accessing mental health services will often find themselves in unfamiliar situations at a time when their anticipated life has been interrupted. Staff should be sensitive to the need to acknowledge and value the child or young person’s concerns and help them to adapt to the new environment without the pressure of gratitude from the child or young person. Practitioners should recognize and facilitate individual pathways of support and discuss aspirations, interests, and passions to co-create plans for the child or young person’s next steps, with an acknowledgment that the child or young person may not yet be able to articulate their past or future cohesively. Regardless, professionals should make attempts to co-construct a stepped plan with the young person where they can begin to identify their own goals; and should validate the young person’s hopes for their future (however rapidly they shift or evolve). Questions that promote attention to the personal journey and reflective understanding during an episode of care include: What would you like to get out of these sessions? What are your goals or aims right now, in 6 months, or in the future? Do you have ideas on what you need to achieve that goal?
It is important that transitions are supported thoughtfully. Moving between services and changes of professionals should be carefully planned and explained with enough time to process prior to the change. Start with clarity around the time limitations of the support and provide information throughout the therapy journey regarding time scales. The end of therapeutic support can be seen as the beginning of a new chapter in the personal journey, with the creation of a network of support to help with the move to the next step. Services should be cognisant of the emotional impact of a history of multiple journeys through health care services, and the likelihood of repeated distress in services where needs were not met or where the young person was offered “more of the same” standardized treatments or blamed for a lack of positive outcomes. Listening to those experiences and taking action to not repeat history may restore a sense of trust, where trust has been lost.
Sense of Place/Dislocation
To feel “at home” is not just about coming from a physical place, it is where the young person finds meaning and feels welcome, safe, and connected. Security, comfort, familiarity, and continuity are important factors in creating a sense of place. Dislocation is experienced when the child or young person is in an unfamiliar, unknown culture where the norms and routines are alien to them. The space, policies, or conventions do not reflect their identity or needs. Dislocation can be physical (to be removed from home or community settings that are familiar), or emotional (to be removed from families, peers, or communities and other psychological and social connections). This is especially true in a day and age where a lot of sense of place or people is generated in online or virtual spaces.
Practitioners should ask, in age-appropriate ways and taking account of language needs, about what creates a sense of home and place for the individual. Exploring what inclusion means personally to the young person may involve looking at how their access needs are honored and understanding the attitudes of their supporters. Questions to explore the young person’s views on a sense of place: What do the words “included,” “welcome,” and “belonging,” mean to you? Where do you feel included/not included? Who makes you feel included? Do you take part in any activities or clubs? What makes it difficult for you to feel comfortable there? What gets in the way? What makes this feel right for you? If you have felt safe before, what can we do to help you feel that kind of safety here? Some children and young people will need support from a parent/carer to help explore these topics.
Culturally sensitive health care practices are required to welcome the diverse range of people who attend for support. Information should be provided in the young person’s chosen language or in culturally appropriate pictorial form for younger children. Health care practices should intentionally strive for a sense of homeness, safety, and familiarity. This could be achieved through the provision of visual information in advance about the setting, ensuring privacy in open spaces, considering the sensory and social set up of waiting rooms and eating spaces, offering objects or tasks that comfort, and having a degree of flexibility around visiting times or appointment times. Guidelines and policies should be reflected upon and updated to prevent a stagnancy in culture which makes the place of care too rigid or bureaucratic to be homely.
Regarding those deemed “hard to reach” or who “did not engage,” practitioners should reflect on access barriers that may have contributed to a sense of dislocation and subsequent difficulties engaging with the service. What would practitioners change if the focus was shifted to practitioners being hard to reach and difficult to engage? What would they change to make autistic young people feel like their service was a safe place to belong, a place that was welcoming and included them?
Embodiment/Reductionist View of the Body
Being human means living within the limits of our human body. Embodiment relates to how we experience the world, and this includes our perceptions of our context and its possibilities, or limits. A child or young person’s experience of the world is influenced by the body’s experience of being in the world, feeling joy, playfulness, excitement, pain, illness, and loss of function. Embodiment views well-being as a positive quality while also acknowledging struggles and the complexities of living (Todres et al., 2009). The young person’s social, environmental, psychological, or spiritual needs are recognized so that the young person’s experience of living and being goes beyond a narrow definition of themselves based on deficits and disabilities which are instilled in a lot of autistic young people along with a deep sense of shame or loss. A reductionist view uses the medical model approach and exposes the young person to potentially excessive tests and reduces them to a list of symptoms and deficits to be “fixed.”
Practitioners relate to young people as people first and avoid making assumptions or value judgments. They presume competence and provide augmentative and alternative communication modes. A total communication approach ensures the inherent communicative value in autistic body language and nonverbal methods of expression is honored. Autistic ways of being and/or disability are explored without defaulting to a deficit narrative, thereby enabling personal development, growth, or reflection without the stigmatizing gaze of an ableist society. The practitioner may facilitate two-way sharing of information about autism and autistic experiences, on a one-to-one basis or in peer group sessions with mindfulness that children and young people might have stark differences in how they are, or where they are in their understanding of autism. Furthermore, they might have immediate social circles with contrasting levels of information or feelings toward autism and autistic young people. The practitioner seeks to understand experiences and feelings around their challenges and disability, for example, How does this make you feel? Why do you think you couldn’t do that? Do you want support to improve this or find a workaround? The young person is supported to identify what they need to do and what they want to do. The Spoon Theory (Miserandino, 2003) or energy accounting may be a practical support for supporting well-being and understanding and advocating for one’s needs.
The practitioner may explore how ableism and internalized ableism impact the young person. Personal struggles and challenges are not minimized but neither is the contribution of a hostile society. The dynamic nature of an individual’s disability is acknowledged, and compassion and support are freely given according to the needs at the moment, especially at times of crisis when the young person expresses thoughts of life not worth living. At these times, when the young person or their family member reaches out for help, their courage and vulnerability are recognized, and the practitioner responds empathetically and with positive steps of action. Drawing, also, on the dimension of togetherness, the practitioner will be prepared to stand alongside the young person amid their distress. This may require services reviewing policies and practices which limit practitioners in their offer of care emphasizing the dimension of togetherness.
Within current constraints where austerity, limited resources, and overstretched services mean that care often comes during immense crises is rarely preventive, and where there is a resurgence of the idea of the “deserving or undeserving disabled” (Geiger, 2021), compassionate care always treats the child or young person as worthy of receiving care and intervention. Autistic people are often painted as being a financial and social drain on societal resources (Baxter et al., 2015), and these attitudes can be perpetuated within neoliberal approaches to care, regular access to or reliance on services can be criminalized, especially where suicidality, or self-harm play a role, based on resource wasting. Compassionate, humanizing care challenges this rhetoric in a way that reminds the child or young person that prevention, slow recovery, and collaborative intervention are all possible.
Practical Applications of the Eight Dimensions in Times of Crisis/Suicidality
Here, we use a specific example to explore how this framework can facilitate support for autistic people in crisis, basing it on a personal recollection of one of the present authors about self-harm and suicidality. The example demonstrates how the clinician might explore the dimensions with the individual. The dimensions naturally overlap and complement each other to produce an individualized, person-centered model of care and support.
Dimensions of Uniqueness and Embodiment: Check whether self-harm could be a side effect of psychiatric medication. Some autistic people have atypical reactions to medication (e.g., hyper- or hyposensitivity). Professionals should recognize and validate the individual experience of the autistic person, even if it stands in contrast with their prior knowledge and assumptions.
Dimensions of Embodiment, Uniqueness, and Sense of Place: Be curious whether self-harm is being used to meet sensory needs and is instead being labeled as “behaviours of concern.” Seek to understand the subjective experience of why and how something is happening for the child or young person, and do not assume that as a practitioner you can apply subjective meaning (why the person is self-harming or what might help) from unexplored objective facts (the person is self-harming).
Dimensions of Togetherness/isolation, Sense-making, Agency/Passivity: Check whether there is a communication mismatch with the young person. Rely on subjective accounts as a starting place of genuine curiosity, even when you do not understand the connection between the autistic person’s verbal communication and their body language. Ways of expressing and showing distress are subjective, exist in flux and fluidity, and attempts to reach out should not be minimized as disingenuous. Approaching with cynicism (“it’s attention seeking”), skepticism (“they don’t seem distressed, they could be lying”), or aggression (“you will be put into seclusion, lose privileges, or be denied access to X if you do not comply”) will always do more damage to the therapeutic relationship than approaching with openness and curiosity.
Dimensions of Isolation, Sense of Place, Sense-making/Loss of Meaning: Assess whether self-harm could be caused by relational disconnection, isolation, or loneliness. There is a lingering assumption in the general perception of autism that all autistic people want isolation and don’t desire relationships. While it may be true for some, many do have a need for meaningful human connection, which often remains unmet and leads to an exacerbation of mental health difficulties. Research shows that autistic children as well as adults tend to report higher loneliness than their non-autistic and neurotypical peers (Grace et al., 2022; Hymas et al., 2024). The notion that autistic people do not desire human interaction is damaging and misleading. Most people have a need for belonging and togetherness. Check if this need is not neglected in the child or young person, even if it is not communicated in an obvious way.
Dimensions of Uniqueness, Insiderness, and Sense-making: What can be seen as alarming for the family or professionals working with the child or young person may in fact be their way to cope with difficult life events or situations, “When I started researching death processes, I was trying to make sense of my brother’s death. I wasn’t actually planning to die.” Monotropism can be a useful concept to understand this. The world can be chaotic, especially when going through a traumatic experience, and a deep intellectual dive into what caused the stress can be a way of processing it and creating a sense of order and security. The professional should find out what effect an intense (or morbid) interest has on the young person without prior assumptions, whether it signifies rumination or is actually a positive way of coping with hardships. A more holistic view of the autistic child’s life can be beneficial in different scenarios. One common example of a surface-level understanding of the child is seeing video games as a cause for isolation or mental health difficulties, rather than a way to cope with an often chaotic, unpredictable, and isolating school experience. Games can give the young person a creative outlet, a sense of control and achievement, and access to communities of shared interests. It can be the only safe space they have available in their lives.
Dimensions of Togetherness, Sense-making, Embodiment, and Personal Journey: Not feeling that others are trustworthy, not belonging, and having to mask the real self is associated with suicide among autistic people (Cassidy et al., 2020). Tackling suicidality has been recognized by NHS England (2022) and the UK Government (2023) as a priority, but it is impossible to do so if we don’t improve the way we connect with autistic people. Accepting the autistic young person as they are and, if necessary, helping them reconnect with their authentic self are crucial elements of good therapy.
Conclusion
The experience sensitive approach is a coherent, neuroinclusive framework that promotes a dignified, respectful, personalized approach to care, which has potential for universal application across health care (Figure 1).
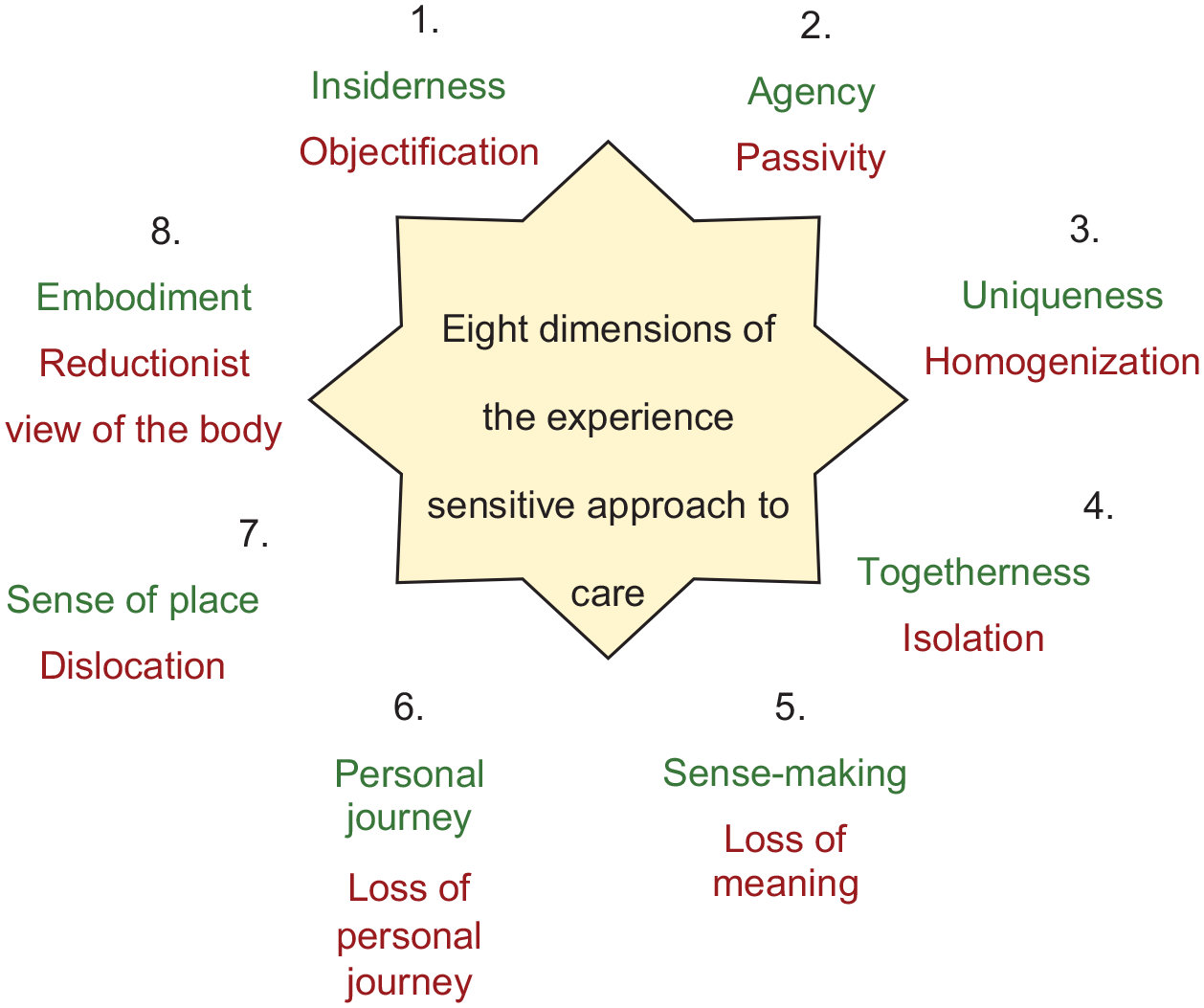
The 8 dimentions of the experience sensitive approach to care, adapted from Galvin, K., & Todres, L. (2013). Caring and well-being: A lifeworld approach. Routledge.
The approach moves practitioners to pay attention to the individual’s experiences and needs in the context of their own lives. This approach can improve the poor experiences of autistic people accessing mental health care, something which is an urgent need given the disproportionately high incidence of mental health difficulties and suicidality.
It is common for practitioners to consciously support “positive,” usually non-autistic patterns of thought or behavior at the expense of so-called less desirable (perhaps autistic) traits. In addition, when practitioners focus on promoting growth and change, parts of autistic people are likely to remain unacknowledged even when warmth and acceptance are extended to other parts. However, well-intentioned, objectification, expectation, and desire results in the person no longer being free to experience, neglecting their totality.
A reduction in stance toward autistic people as “other” where practitioners operate from a position of unknowing can support the conveyance of acceptance and non-judgment. These qualities are required to embrace the totality of autistic people, enabling less defended self-expression and supporting the movement toward self-determination. The aim must not be about finding answers or creating change. Rather, gentle and respectful curiosity should facilitate personal explorations and re-authoring of internalized neuronormative, objectifying narratives. Honoring the sovereignty of the person in this way requires a determination to maintain a relationship of mystery and a willingness on the part of practitioners to transform their understanding.
The respectful and non-judgmental character of this approach is something that is not only relevant to supporting young autistic people. The many dimensions described here can characterize good therapy in general, as well as more broadly, respectful human interactions. Autistic young people, however, are more likely to face self-diminishing interactions on an everyday basis, with some having virtually no available person to safely “unmask” with. In such cases, having a neurodivergence-affirming support at hand can serve almost as an oasis that allows the young person to flourish in a desert of adversity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: G.P is director of National Autism Trainer Programme (NATP) at Anna Freud, commissioned by NHS England. R.M, K.R, E.M and A.Q have been involved in NHS funded autism train-the-trainer model activities. R.M, K.R, E.M often delivery paid lectures/trainings as independent trainers M.B. Is often a paid speaker on topics relating to autistic peoples mental health, and a paid advisor to Donaldsons trust (a service for neurodivergent young people) and Information autism.