
Abstract
While the potential of serotonergic psychedelics and related substances as adjuncts in substance-assisted psychotherapy (SAPT) has been investigated for the treatment of several disorders, evidence for the appropriate therapeutic conduct in administration sessions is sparse. In this article, we discuss the current evidence for best therapeutic practice during administration sessions with serotonergic psychedelics and entactogens as adjuncts to psychotherapy. We conducted a systematized review of the literature following PRISMA guidelines. PsycINFO, MEDLINE, and Cochrane Library databases were searched. Clinical trials, treatment manuals, study protocols, qualitative studies, case studies, descriptive studies, opinion papers, reviews, book chapters, and conference proceedings published until February 1, 2022 were retrieved. The final synthesis included k = 82 sources. Information about substances, dosages, number of administration sessions, issues that are common for clients, different types of experiences, music, and therapeutic conduct was summarized, compared, and critically discussed. The effects different therapeutic models, methods, techniques, and more complex interventions each have on the therapeutic outcome have not been investigated by means of rigorous research. Most of the available evidence we retrieved was anecdotal limiting any conclusive statements regarding appropriate therapeutic conduct during administration sessions. Consequently, essential components of therapeutic interventions remain largely tentative, necessitating systematic investigation.
Keywords
It is suggested that people have consumed psychedelics for at least 5,700 years (El-Seedi et al., 2005). The use of psychedelics in the general population is increasing (Krebs & Johansen, 2013) and the contexts these substances are currently consumed in range from ritualistic, shamanistic, and indigenous contexts (Metzner, 1998), to recreational use in festival settings (Palamar et al., 2016), to underground therapy (Sessa & Fischer, 2015) and clinical studies with and without psychological support and/or psychotherapy (Rucker et al., 2018; Thal et al., 2021). Evidently, the field is experiencing a surge of interest, and with it a growing need for guidance. However, there are limited data to draw firm conclusions about how to handle administration sessions. In the current article, we aim to summarize the reported suggested practices during administration sessions of substance-assisted psychotherapy (SAPT) to date, to inform subsequent work and to offer practitioners an overview of common practices in the field.
Following the resumption of research into the therapeutic application of psychedelics, various substances have been investigated as potential adjuncts in SAPT. Serotonergic or “classic” psychedelics, which were mainly used in the treatment of alcohol dependence (Krebs & Johansen, 2012; Mangini, 1998), have now also been effectively used for the treatment of existential anxiety (e.g., Griffiths et al., 2016; Grob et al., 2011), tobacco dependence (Johnson et al., 2014, 2017), alcohol dependence (Bogenschutz et al., 2015), obsessive-compulsive disorder (Moreno et al., 2006), and treatment-resistant depression (e.g., Carhart-Harris et al., 2021; Palhano-Fontes et al., 2019). Meanwhile, 3,4-methylenedioxymethamphetamine (MDMA), ibogaine, and ketamine have been used for the treatment of opioid dependence (e.g., Alper et al., 1999; Krupitsky et al., 2007), depression (Diazgranados et al., 2010; Murrough et al., 2013), post-traumatic stress disorder (Mithoefer et al., 2011, 2018; Oehen et al., 2013), and social anxiety disorder (Danforth et al., 2018).
The mechanisms responsible for the effectiveness of these substances in therapeutic settings across psychiatric disorders are not fully understood (Thal et al., 2021). Therapeutic outcomes are affected by the psychopharmacological effects of the substance (see Carhart-Harris & Friston, 2019; Preller et al., 2019), the client’s dispositions (Haijen et al., 2018; Studerus et al., 2012, 2021), their subjective experience (Carhart-Harris, Erritzoe et al., 2018b; Roseman et al., 2018), emotional breakthroughs during the administration sessions and psychological insights after the experience (Peill et al., 2022), and the successful integration of the experience into their lives (Gorman et al., 2021; Malone et al., 2018).
Some of the acute substance-induced subjective experiences that may be linked to positive outcomes include ego dissolution (Mason et al., 2020; Tagliazucchi et al., 2016), mysticomimetic experiences (i.e., mimicking mystical experiences; Davis et al., 2021; Ross et al., 2016), and death transcendence (Schmid & Liechti, 2018). Challenging experiences, or more precisely, their quality, intensity, and duration may also mediate the therapeutic outcome (Carbonaro et al., 2016; Romeo et al., 2021; Roseman et al., 2018). Furthermore, different psychotherapeutic approaches (Thal et al., 2021) and therapy-related variables, as well as contextual factors (see Thal et al., 2022), are thought to influence the outcome of the SAPT.
The course of SAPT may be divided into three stages (Van Rhijn, 1967): the preparatory stage, the administration stage, and the integration stage. Careful consideration of all aspects constituting each of these stages is important as preparation before administration of the substances, the shared interpersonal experience between client and therapist (Adamson & Metzner, 1988; Cosimano, 2021), and subsequent integration of the experience (Garcia-Romeu & Richards, 2018; Richards, 2017) may affect the outcome of SAPT. In this article, we review the current evidence for best therapeutic practice during administration sessions with classic psychedelics and entactogens as adjuncts to psychotherapy.
This article is the third in a series of papers reviewing the literature on Western psychotherapeutic paradigms of SAPT that have been developed and employed since the 1950s. The first paper in this series (Thal et al., 2021) outlined the appropriate preconditions for conducting SAPT including ethical considerations, the spiritual emphasis of the therapeutic approaches, different concepts of psychological mechanism of action and therapeutic effects of SAPT, and similarities between models, approaches, and potential mediators for therapeutic effects. The second paper (Thal, Wieberneit et al., 2022) discussed best practice measures for appropriate therapeutic conduct in preparation sessions to provide a basis for future investigations and training programs for therapists. This included current safety and screening procedures; set and setting; contextual-, physiological-, and psychological preparation; prerequisites of the therapists; and the importance of the therapeutic relationship. The purpose of the current review is to identify, analyze, and discuss current literature to inform therapeutic conduct during the administration stage of SAPTs. Thereby, we aimed to extract details regarding (a) substances that are used as adjuncts in SAPT, (b) dosages that are used in SAPT, (c) number of administration sessions that are used across different models of SAPT, (d) common issues for clients and therapists, (e) common types of experiences, and (f) therapeutic conduct during administration sessions in SAPT.
Method
We followed PRISMA 2020 guidelines (Page et al., 2021) and conducted a systematized review of the literature (Grant & Booth, 2009). We did not consider quantitative analyses informative since the objective of this review was to extract qualitative study details to describe current best-practice methods. We systematically searched the MEDLINE (OVID), PsycINFO (OVID), and Cochrane Library databases and included papers that were published before February 1, 2022. We published detailed information about the search strings for the respective databases on the project’s Open Science Framework (OSF) page (https://osf.io/usgeb/). We scanned references of retrieved articles and consulted experts in the field to supplement our search. Finally, we imported the literature into EndNote 20.
Eligibility Criteria
We selected broad inclusion criteria because we expected the literature outlining administration of psychedelics to be sparse. We included studies that (a) used classic psychedelics or MDMA in SAPT, (b) used a type of psychotherapy or therapeutic techniques as part of an intervention, (c) described the methods and/or theories used for administration and to guide the conduct of therapists, and (d) recruited participants diagnosed with psychiatric disorders according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994), Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013), or International Classification of Diseases (10th Revision; ICD-10; World Health Organization, 1993) criteria. We excluded studies if they (a) involved in vitro research, (b) involved animal research, (c) described indigenous and ritualistic use, (d) the administered doses in the intervention condition were subperceptional, (e) the full text was unavailable via institutional access or through direct correspondence with the authors, or (f) were written in any language other than English or German. After reviewing the literature, we decided to also include studies with healthy participants (i.e., who did not have a psychiatric diagnosis) that explicitly investigated the effects of different doses of substances to provide a complete picture of the dosages that are currently used in clinical research. We limited our review to individual and couples therapy but aimed to synthesize applicable and valuable insights from literature regarding group therapy. We further disregarded the use of combinations of two or more psychoactive substances (Eisner, 1964; Schmid et al., 2021). Detailed information regarding excluded studies is outlined on the project’s OSF page (https://osf.io/mu8hp/). The final sources consisted of clinical trials and follow-ups, treatment manuals, study protocols, case studies, qualitative studies, descriptive studies, theoretical papers, reviews, book chapters, and conference proceedings. We expected that not every resource would provide information relevant to all aspects that we hoped to cover in this review to an equal degree.
Selection Process
Two independent reviewers (S.B.T. and T.W.) screened the retrieved literature for the initial search on July 1, 2019. Good interrater reliability was reached (κ = 0.72; Cicchetti & Sparrow, 1981) for the title and abstract screening. In a subsequent full-text review, good interrater reliability was reached (κ = 0.66; Cicchetti & Sparrow, 1981). We conducted a second search with an identical search string on February 1, 2022. Two independent reviewers (S.B.T. and M.W.) screened the title and abstract reaching good interrater reliability (κ = 0.76; Cicchetti & Sparrow, 1981). In the subsequent full-text review, excellent interrater reliability (κ = 0.90; Cicchetti & Sparrow, 1981) was reached. If sources were identified as suitable for inclusion by one reviewer but not the other in either search, the suitability of the literature was discussed with the other co-authors until a consensus was reached.
Data Collection and Analysis
We extracted data from eligible studies including details on the type of clinical target, study design, therapeutic framework, substance administered, dosage administered, and number of administration sessions. We then synthesized the retrieved information regarding current best-practice approaches in administration sessions.
Terminology
The terminology used in the literature varies widely. Phelps (2017) identified the term “therapist(s)” to be the preferred terminology by psychedelic scholars used for the person(s) conducting the session(s). Consequently, we use this expression in this article. Furthermore, we use the term “client” to maintain a professional reference and avoid pathological connotations.
Results
The first search resulted in 3,932 hits. In addition, 45 records were identified through secondary sources. After preliminary analysis of the titles and abstracts, a total of 390 duplicates were removed and 136 sources were identified for further full-text analyses. In the initial search, 88 sources were included through consensus. The subsequent search resulted in 6,619 hits. The EndNote 20 software was used to remove 447 duplicates. The remaining 6,172 sources were screened by title and abstract. Consequently, 5,948 sources were exclusions, and 224 full-text publications were identified for full-text analysis by two independent reviewers (S.B.T., M.W.). Afterward, 22 additional articles and book chapters were included. In addition, one article was included after the peer review with the result that 82 papers, and book chapters were included in the final results (see Figure 1). As expected, not every resource was able to speak to each issue discussed below.
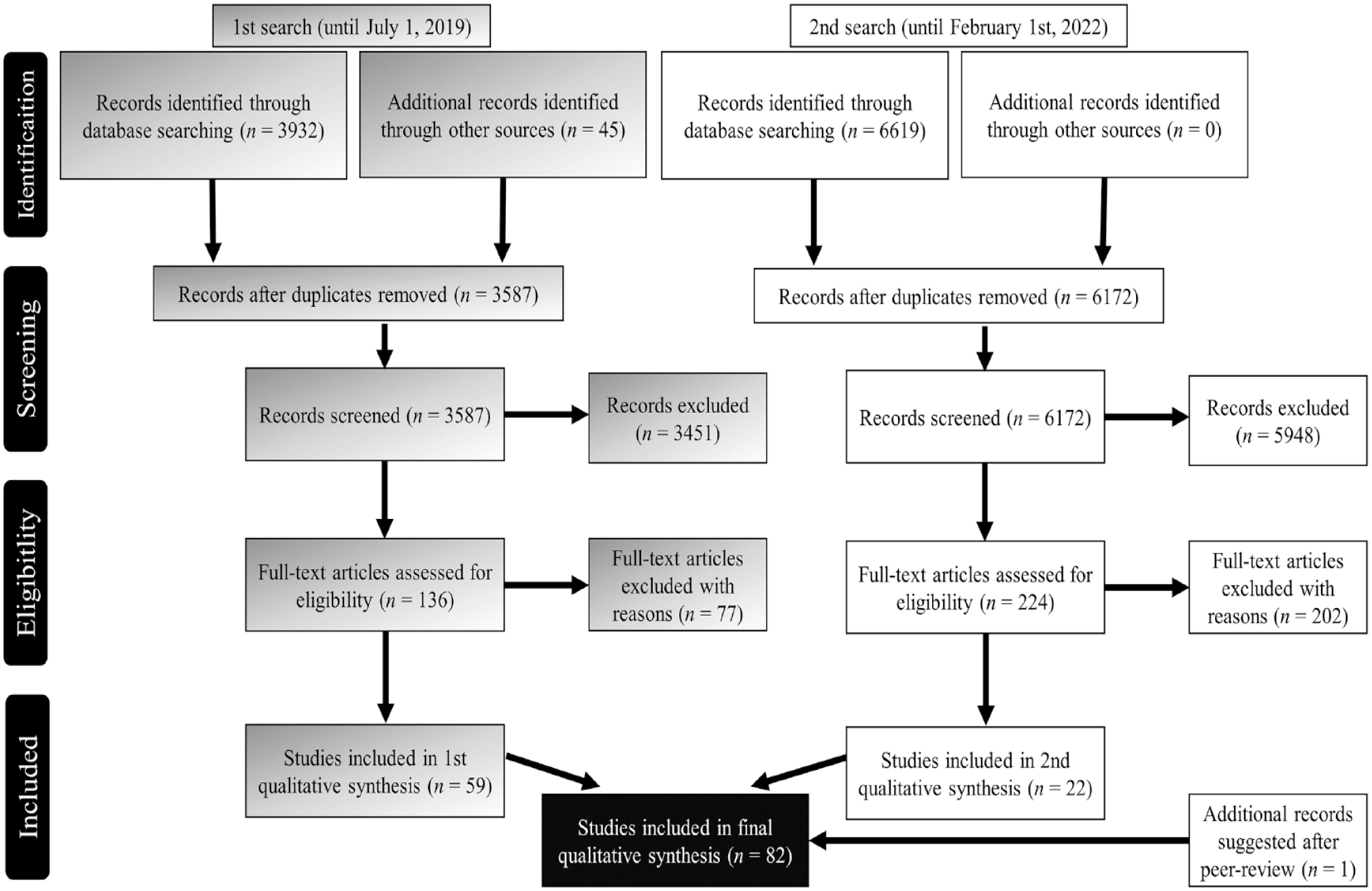
Visualization of the Literature Search.
Characteristics of Included Studies
The details of the publications included in the final qualitative synthesis can be found in Supplemental Appendix A. The 82 publications included 31 clinical trials, one follow-up analysis, four treatment manuals, two study protocols, three quasi experiments, two case studies, three qualitative investigations, three descriptive studies, one time-series study, 14 opinion papers, 11 reviews, and seven books and book chapters.
Substances and Dosage
Psilocybin is considered a classic psychedelic and is found in more than 200 species of mushrooms. The effects of psilocybin are usually noticeable 10 to 40 min after ingestion, and last 2 to 6 hr depending on the dose and individual metabolism (Passie et al., 2002). Doses of psilocybin in recent clinical trials ranged from 1.75 to 30 mg with 21 mg being the median dose used (based on an average body weight of 70 kg; see Supplemental Appendix A). A post hoc analysis of 10 studies with 288 participants showed that, on average, participants who received 20 mg/70 kg reported moderately high scores for mystical experiences and intensity and low to moderate scores for challenging experiences. Participants who received 30 mg/70 kg reported, on average, high scores for mystical experiences and intensity and low to moderate scores for challenging experiences. The same study showed no advantage of adjusting the dosing of psilocybin to the bodyweight of participants over fixed dosing (Garcia-Romeu et al., 2021).
Lysergic acid diethylamide (LSD) is a lysergamide derived from alkaloids of a group of fungi known as ergot (Nichols, 2004). The effects of LSD may last up to 12 hr (Schmid et al., 2015). In the past doses have ranged from 20 μg (Greiner et al., 1958) to 1,500 μg (MacLean et al., 1961). The only recent clinical study administered a dose of 200 μg (Gasser et al., 2014). Some authors consider optimal therapeutic effects be achieved in the range of 100 to 200 μg (Passie et al., 2008) among healthy adults, with 100 μg being considered an “intermediate” or “good effect” dose (i.e., a good combination of positive subjective effects and medium levels of ego dissolution with minimal negative subjective effects), and 200 μg being considered a “high” or “ego dissolution” dose (i.e., substantial ego dissolution, similar positive subjective effects but increased negative subjective effects; Holze et al., 2020; Li et al., 2021). Sex and bodyweight do not seem to affect the plasma concentration or subjective strength of effects for LSD in healthy participants (Dolder et al., 2014; Holze et al., 2019, 2020).
Ayahuasca is commonly prepared (McKenna et al., 1984) by combining Psychotria viridis and Banisteriopsis caapi (Riba et al., 2003). Its effects last for 4 hr (Riba et al., 2003). The ayahuasca used in the only clinical study to date (Palhano-Fontes et al., 2019) contained 0.36 mg/mL of N,N-dimethyltryptamine (N,N-DMT), 1.86 mg/mL of harmine, 0.24 mg/mL of harmaline, and 1.20 mg/mL of tetrahydroharmine and participants received ayahuasca adjusted to contain 0.36 mg/kg of N,N-DMT.
MDMA is usually classified as an entactogen (i.e., producing feelings of empathy and connection; Nichols & Oberlender, 1990). Subjective effects commonly peak after 2 hr and last around 4 hr (Cole & Sumnall, 2003; De La Torre et al., 2004). Doses administered in clinical studies ranged from 50 to 125 mg (usually with a booster of 50% of the initial dose offered after 2 hr) with 110 mg being the median dose (see Supplemental Appendix A). The best predictor of the subjective strength of MDMA’s effects is plasma MDMA concentration, which is significantly dependent on the dose per body weight someone receives (Studerus et al., 2021). Thus, it has been recommended to consider dose adjustments for bodyweight (Studerus et al., 2021; Vizeli & Liechti, 2017).
The dosage of the substance(s) affects the strength of the subjective effects of the experience (Liechti & Holze, 2021). It was suggested that the ideal dosage should be determined considering the recommended amounts for a specific substance, the client’s intentions, and the client’s past reactions to the substance (Meckel, 2019). Substances and doses employed in current clinical trials are outlined in detail in Supplemental Appendix A.
Number of Sessions
Historically, a high-dose single-session Psychedelic model was preferred (for review see Bogenschutz, 2013). Alternatively, multiple sessions with escalating doses were used, or a booster dose was offered a few hours after the initial dose was administered (MacLean et al., 1961; Rolo et al., 1960). In the case of the low-dose Psycholytic model, up to 80 substance-assisted sessions were conducted throughout the course of therapy (Grof, 1980), although some therapists argued that psychoactive substances be used as sparingly as possible as adjuncts to psychotherapy (Cutner, 1959).
The number of administration sessions that have been used in recent clinical studies has ranged between one and four sessions with a median of two sessions (see Supplemental Appendix A). The number of administration sessions may depend on the model that is used for the treatment (see Thal et al., 2021).
Commencing Administration Sessions
Information about proper preparation and safety measures is outlined in our earlier article (Thal et al., 2022). On the day of the substance-assisted session, protocols usually have the therapist(s) check-in with the client to briefly assess their overall mood and well-being (e.g., Mithoefer, 2017; Sloshower et al., 2020; Watts, 2021). If the client reports feeling unwell or exhibits signs of a potential illness, the session might be canceled or postponed. A certain degree of pre-emptive anxiety and excitement may, however, be normal and widely reported (Fadiman, 2011). Expectations and intentions might be reviewed and clients may be shown the location of the bathroom and the restroom procedure (Sloshower et al., 2020).
Current treatment protocols suggest that the rationale behind the therapeutic approach, the range of experiences, and strategies and techniques for potentially challenging experiences should be reviewed before the substance is administered. Questions, fears, and doubts can be addressed prior to administration (Sloshower et al., 2020; Watts, 2021). The client may further be reminded of the agreements made during preparatory sessions regarding physical contact, self-harm, and harm to others and property (Garcia-Romeu & Richards, 2018; Mithoefer, 2017; Sloshower et al., 2020). The appropriate dose and substance for the session may also be reassessed and discussed with the client. Anecdotal reports, self-reports, and treatment protocols suggest that silence, meditation, or even prayer before the administration of the substance can assist clients in their surrender to the experience. Some authors take the view that these preparatory activities aid in reducing anxiety prior to administration, throughout the session and afterward (Greer & Tolbert, 1998; Mithoefer, 2017; Nicholas et al., 2018; Stolaroff, 2004). Some current treatment protocols suggest offering the substance to the client in a designated vessel and instructing clients to take it of their own accord to promote active engagement and self-efficacy. After ingesting the substance, clients are usually invited to lie down and focus inward (Sloshower et al., 2020; Watts, 2021). Fadiman (2011) advises therapists should trust their intuition and refuse to conduct the session if they do not feel certain about it.
Music
Music is a consistent feature reported in SAPT studies (e.g., Barrett et al., 2018; Horton et al., 2021), used for guidance and support (Bonny & Pahnke, 1972; Eisner & Cohen, 1958). It is usually delivered through headphones and may significantly affect the subjective experience and the therapeutic outcome (Kaelen et al., 2015, 2016, 2018; Preller et al., 2017; Swift et al., 2017; Watts et al., 2017). There are also some reports that music may facilitate peak experiences, emotional release, and autobiographical processing (Kaelen, 2021) and it is associated with mystical experiences and insights during administration sessions (Kaelen et al., 2018). Music may also reduce distraction from environmental stimuli and the urge to partake in verbal interactions (Johnson et al., 2008). Furthermore, it may be a source of support and reassurance (Kaelen et al., 2018). Some consider music a source of nonverbal direction allowing for deep immersion into the experience. For the client, songs may become immersive worlds, and music may be experienced as a profound, highly personal, and dynamic element of the administration session (Kaelen, 2021).
Kaelen et al. (2018) conducted semi-structured interviews with 19 participants who received psilocybin for treatment-resistant depression and found that music had both welcome (i.e., effects described as accepted, appreciated, and wanted) and unwelcome (i.e., effects described as rejected, unappreciated, and unwanted) effects on participants’ subjective experience. Welcome influences included a sense of guidance, a sense of safety and calm, the evocation of therapeutically useful and personally meaningful emotions and mental images, perceived openness, and positive intensification of the experience. Unwelcome influences included perceived misguidance and resistance, the evocation of unpleasant imagery and emotion, and negative intensification of the experience. It is thus evident that music may have positive and negative influences on the subjective experience.
Clinical guidelines often emphasize the importance of (Western classical) music during SAPT. Usually, it is recommended that the structure and time course of an administration session should match music sequencing (Bonny & Pahnke, 1972; Eisner, 1997; Johnson et al., 2008). An early study with 49 participants found no significant differences in effects across no music, familiar music, and unfamiliar music conditions in people receiving LSD in the treatment of alcohol use disorder (Gaston & Eacle, 1970). More recently, overtone-based music (i.e., music in which instruments with a particularly strong overtone signature were prevalent) was found to elicit higher mystical experience scores and slightly higher treatment response compared with Western classical (similar to the music most commonly used in curated playlists in SAPT) music in a small sample of participants receiving psilocybin for tobacco smoking cessation (Strickland et al., 2021). Barrett et al. (2017) conducted an anonymous online survey with 10 individuals with extensive experience in administering psilocybin in therapeutic and/or research conditions. They identified 24 recommended musical stimuli that support the onset or pre-peak period of psilocybin effects and 24 recommended musical stimuli that may support peak effects of psilocybin based on the survey. Compared with pre-peak music, peak music comprises formulaic, regular, and predictable phrase structure and orchestration, a slowly building feeling of continuous forward motion, and lower perceptual brightness. Based on these findings, 27 titles for pre-peak and 27 titles for peak periods of administration sessions were recommended. It is currently not established whether curated playlists (as used by Davis et al., 2021; Palhano-Fontes et al., 2019; Sloshower et al., 2020), personalized playlists (as used by Carhart-Harris et al., 2021; Watts, 2021), or specific genres of music offer therapeutic advantages.
According to Kaelen (2021), six key criteria should be considered for the effective use of music in SAPT, including (a) type of direction provided by the music, (b) adaptation of the music to the session, (c) adaptation of the music to the current personal process of the client and potential musical resistance, (d) understanding and consideration of the role of silence, (e) preparation of an open mindset, (f) appropriate technical specification for the music delivery.
Common Issues for Clients
Diverse effects of psychoactive substances on the client were described, ranging from a feeling of complete alienation to a feeling of recalling and reuniting with a very familiar state of mind (Fadiman, 2011). It might be challenging to encounter these altered states and to accept the corresponding positive or difficult feelings without acting on them (Möckel Graber, 2010). The potential for adverse physiological reactions can depend on the substance and dose (see, for example, Nichols, 2016). Adverse psychological effects can generally include anxiety, panic, dysphoria, paranoia, isolation, dissociation, confusion, and delusion (Barrett et al., 2016; Carbonaro et al., 2016; Grinspoon & Bakalar, 1979; McCabe, 1977; Pahnke et al., 1971; Strassman, 1984). These effects may even result in transient, and if handled inappropriately potentially permanent, psychological crisis (Twemlow & Bowen, 1979). The previously mentioned pre-emptive fear may lead to attachment behaviors and dependence on the therapist(s) and/or the substance. For personal growth and positive treatment effects, self-regulation, staying with, and observing these fearful reactions are thought to be essential (Buckman, 1967; Richards, 2014; Rodger, 2018; Russ & Elliott, 2017).
As in regular psychotherapy, it is suggested that some clients may produce and talk about the material that they think is expected from them (Buckman, 1967). This may be emphasized by certain substances (such as LSD) that can enhance suggestibility in clients (Carhart-Harris et al., 2015). Due to the strong psychological effects of the substances used as adjuncts, memories may surface, and clients may experience emotional catharsis with the potential for abreaction and subsequent relief and remission. Preliminary and anecdotal evidence suggests that the risk of a traumatic experience may be avoided by clients gaining new perspectives and correcting patterns of emotional responses through previously inaccessible positive associations. It has been suggested that a prerequisite for this corrective process could be the client’s ability to surrender to the experience and witness the resurfacing of difficult memories (Frecska et al., 2016; Pahnke, 1969).
Common Experiences
There was a common understanding across sources that the effects of psychoactive substances in SAPT may be difficult to predict. Garcia-Romeu and Richards (2018) note that the mere description of these typologies may impact subsequent experiences through expectations and suggestions (Carhart-Harris et al., 2015). These authors further discourage valuing certain experiences over others and advise to equally acknowledge and accept the vast potential of different experiential encounters.
Garcia-Romeu and Richards (2018; cf., Buckman, 1967 for alternate taxonomy) outline the following classes of experiences for low to medium doses of serotonergic psychedelics: sensory-aesthetic, psychodynamic-autobiographical, cognitive-intellectual, and symbolic-archetypal, challenging, and mystical experiences for high doses.
Sensory-aesthetic experiences include perceptual changes across all senses. The role of these experiences in treatment outcomes has not been adequately examined since these experiences might be altered in clinical settings due to the common use of eyeshades, music, and the minimization of interpersonal communication.
Psychodynamic-autobiographical experiences include recollection, reemergence or revisiting, and reflections on negative experiences regarding significant past or present autobiographic events and relationships. There is preliminary qualitative evidence that these experiences contribute to therapeutic efficacy (Gasser et al., 2015; Watts et al., 2017).
Cognitive-intellectual experiences refer to alterations of baseline cognitive patterns and thinking. While models of SAPT do not leverage these as part of the therapeutic process, some authors take the view that alterations of cognitive patterns and novel perspectives might challenge maladaptive schemas and allow spontaneous cognitive reframing (Clark & Beck, 2010; McCusker, 2001). However, this has not been empirically examined.
Symbolic-archetypical experiences are sometimes referred to as “visionary experiences” and involve symbolic content like historical imagery, gemstones, and encounters with deities and universal qualities such as beauty, truth, or love (Richards, 2002; Richards et al., 1977). There is anecdotal evidence for the therapeutic value of these experiences through reduced client anxiety and the rich material they can offer for continuous integration processes (Garcia-Romeu & Richards, 2018; Richards et al., 1977).
Challenging experiences include fear, anxiety, panic, paranoia, confusion, disorientation, grief, isolation, and physical discomfort are generally linked to psychotomimetic reactions (i.e., psychotic experiences such as delusions) and a persistent fear of dying or going insane (Barrett et al., 2016; Carbonaro et al., 2016; Garcia-Romeu & Richards, 2018; Pahnke et al., 1971). Extensive preparation, adequate set and setting, social support, and a good therapeutic relationship all reduce the likelihood of challenging experiences (see Thal et al., 2022). Regardless, clients may benefit from these experiences (Carbonaro et al., 2016; Garcia-Romeu & Richards, 2018) provided the therapist(s) remains calm, reassuring, present, emotionally responsive, and is able to assist the client integrate afterwards. Watts (2021) recommends that the experience of the client should be validated, and the client should be reminded that they are safe and that the experience is temporary, normal, and related to the effects of the substance. Guided imagery or breathing exercises (the therapist(s) may breathe together with the client; Watts, 2021) and changes in music can be used to provide structure and containment. In doing so, it is hoped that clients will cease to resist and reject the experience, and instead accept and surrender to it. In extreme cases, anxiolytics and antipsychotics can be administered (Johnson et al., 2008). Subsequent to a challenging session, the therapist(s) must monitor the client’s emotional state. Intensive and timely recapitulation, reflection, and integration are considered especially important for the contextualization and meaning-making of the experience (Garcia-Romeu & Richards, 2018).
Mystical experiences—also called peak or transcendent experiences, or ego dissolution—comprise a transcendence of time and space, intense positive mood, the feeling of unity, sacredness, ineffability, and a perception of ultimate truth and reality (i.e., the noetic quality; Griffiths et al., 2006; Pahnke, 1969; Pahnke & Richards, 1966). These experiences can be reliably occasioned with classic psychedelics provided the set, setting, client, and therapist(s) are well-prepared (Bogenschutz et al., 2015; Griffiths et al., 2006, 2016; Johnson et al., 2014; Palhano-Fontes et al., 2019; Ross et al., 2016). As outlined above, mystical experiences have been linked to persisting personality changes, and anxiolytic, antidepressant, and antiaddictive effects in several randomized controlled trials (Davis et al., 2021; Griffiths et al., 2016; Mason et al., 2020; Ross et al., 2016; Tagliazucchi et al., 2016). Mystical experiences may thus be a mediating factor for the therapeutic efficacy of SAPT (Garcia-Romeu & Richards, 2018). However, these experiences can also pose challenges to the study of psychedelics that are outlined elsewhere (Johnson, 2021).
Therapeutic Conduct in Administration Sessions
The literature revealed several issues that may present challenges to the therapist’s skill and resources (Buckman, 1967). This includes reports that the intensity and duration of the session can be quite exhausting for therapists, and over-exhaustion or feeling drained of energy, perspective, and compassion is unhelpful. It is suggested that this can be prevented by making the session as comfortable as possible for the client and the therapist(s) (Greer & Tolbert, 1998). Using a co-therapist team can also ease exhaustion (Mithoefer, 2017). In most contemporary studies, a mixed-gender co-therapist team is used (see Thal et al., 2022).
Non-Directiveness and Support
Most reviewed sources described that the therapist(s) must ensure the physiological and psychological safety of the client and minimize the potential for difficulties and adverse reactions (Johnson et al., 2008; Sloshower et al., 2020; Watts, 2021). This may in turn create the conditions for the emergence of transcendent, transpersonal, and mystical states. Most sources recommend that the therapist(s) avoids intruding into the client’s process and allows room for the effect of the substances to unfold, sometimes subtly reminding clients of their goals and focus: to go inside, surrender to the experience, trust, and let go (Sloshower et al., 2020; Tai et al., 2021; Watts & Luoma, 2020). If previously agreed upon with the client, the therapist(s) might guide the client toward the core themes (e.g., their index trauma) of their therapeutic processes (Mithoefer, 2013, 2017). Even though many recent studies applied therapeutic frameworks to SAPT that were not nondirectional, per se (k = 11 explicitly used nondirectional/supportive frameworks; see Supplemental Appendix A), there is usually very limited verbal (psychotherapeutic) interaction in administration sessions across frameworks. Moreover, it has been noted that being present can often be of more value to clients than verbal exchange (Tai et al., 2021). Across all sources, there was a consensus that therapists should let the transpersonal experience unfold during the session to let the client stay with their own realizations, encourage them to collect and remember their experiences, offer reassurance, and save the discussion for later review and reflection instead of offering interpretation and suggestions or intrude on the client with their ideas or opinions during the session (Buckman, 1967; Cutner, 1959; Garcia-Romeu & Richards, 2018). The therapist(s) may both construct and retain the framework for the session and avoid trying to excessively control its course (Möckel Graber, 2010; Tai et al., 2021). The therapist(s) may assist the clients to the bathroom, help them with the ingestion of liquids or food, or change the music for them (Johnson et al., 2008; Mithoefer, 2017; Sloshower et al., 2020; Watts, 2021).
Self-Awareness, Presence, and Responsiveness
Tai et al. (2021) suggest that the therapist(s) remains responsible for their own feelings, stance and attitude, the client, and what happens in the shared space. This includes their own potential feelings of anxiety, fear, or boredom while modeling an open attitude and interest toward clients. Moreover, the therapist(s) may pay attention to their intuition, motivation, behavior, and mindset. Maintaining a patient, thorough, and friendly attitude is thought to be helpful (Buckman, 1967; Möckel Graber, 2010).
The importance of the presence of the therapist(s) has been consistently alluded to in the literature that was retrieved for this article (Mithoefer, 2017; Phelps, 2017; Tai et al., 2021). Therapeutic presence may be defined as a state of being nonjudgmental, receptive, gentle, and compassionate to the experiences of the client (Geller & Greenberg, 2002) and is closely linked to a person-centered approach and Roger’s idea of the importance of presence, congruence, positivity, acceptance, and empathy from the therapist(s) in the context of psychotherapy, outlined above (Rogers, 1957, 1966). Therapeutic presence is thought to be essential for effective therapeutic relationships, independent of the approach or theoretical orientation of the therapist(s) (Geller, 2013a, 2013b; Geller et al., 2012; Geller & Greenberg, 2012; Tannen & Harry Daniels, 2010). Nevertheless, the concept of therapeutic presence has not yet been qualitatively or quantitatively assessed and investigated in the context of SAPT.
Some consider the therapists’ emotional and physical responsiveness and alertness crucial due to the potential sudden shifts in the mental states of the client and the content of their experiences (Fadiman, 2011). Meanwhile, the therapists’ presence may maintain a nonintrusive quality (Sloshower et al., 2020). Watts (2021) recommends that therapists be constantly present; if clients appear to be engaged, they may do nothing. If clients are not engaged, they may communicate with them and check for potential resistance. While the therapist(s) may respond to the physical and emotional needs of the client and, if requested, may offer perspective (Greer & Tolbert, 1998; Mithoefer, 2017), significant psychotherapeutic work is generally avoided until the effects of the substance have ceased (Horton et al., 2021).
Some clients may become demanding, especially during regressive processes, while others may grow distrustful and paranoid. The therapist(s) must be able to work with a variety of emotional responses and not react to or engage with clients in an unhealthy way (Buckman, 1967; Grof, 1980). Physical contact and touch might be helpful and supportive—some have even described it as essential (Spencer, 1963)—if previously discussed and agreed upon with the client. However, it is noted that the potential for gross exaggerations of the client’s imagination during the session requires careful awareness of intended and unintended physical contact from the therapist (Buckman, 1967; Fadiman, 2011; Grof, 1980; Mithoefer, 2017). Twemlow and Bowen (1979) explicitly stress that if the client’s experience is negative and there are obvious signs of anxiety or distress, therapists should empathize with the situation of the client to conduct effective crisis intervention. This is not always straightforward due to the bizarreness, vastness, and swiftly changing nature of the experience and requires sustained attentiveness and presence from the therapist(s).
Techniques, Methods, and Interventions
The reviewed literature revealed a nondirective and supportive therapeutic framework is most commonly used during substance-assisted sessions (e.g., Mithoefer, 2013, 2017; Sloshower et al., 2020; Watts, 2021; Watts & Luoma, 2020). Preparation and integration sessions have more frequently incorporated therapeutic techniques and frameworks from motivational enhancement therapy (e.g., Bogenschutz et al., 2015), or cognitive behavioral therapy (CBT; for review, see Horton et al., 2021; Thal et al., 2021).
Anecdotal evidence suggests that initially, verbal communication may distract the client and could thus have fewer beneficial effects than expected in traditional talk therapy (particularly if high doses are administered; Walsh & Grob, 2006). Therapists may instead observe the client’s facial expression and body language. If clients want to engage with the therapist(s), supportive listening and appropriate empathic responses are generally advised in the literature. After a few minutes, the therapist(s) may need to suggest the client resume an inward focus. If the suggestion is met with resistance, continued support and compassion may be offered until clients are ready to focus inward again. Resistance to an inward focus may represent experiential avoidance that should be discussed during integration sessions (Sloshower et al., 2020). In current studies with psilocybin, conventional psychotherapeutic techniques are usually not implemented until the last hour of the administration session (Horton et al., 2021). During later parts of the session, openness and receptiveness to the application of various therapeutic, meditative, breathwork, and bodywork methods may be increased (i.e., after peak effects of the substance begin to subside; Sloshower et al., 2020).
During challenging parts of the experience, reassurance, support, comfort, and connection through physical contact (i.e., reassurance by holding hands) may be initiated, if necessary, appropriate, and previously agreed on, after communication with the client (Johnson et al., 2008; Mithoefer, 2017; Watts, 2021). The therapist(s) may talk to the client through difficult parts of the experience and assess and acknowledge their emotions (Buckman, 1967; Mithoefer, 2017; Sloshower et al., 2020; Spencer, 1963; Watts, 2021). Therapists ought to stay calm and reassure clients that they are safe and secure and that their current state of mind is the result of psychoactive substances that will wear off with time. Intense and unpleasant aspects of the experience should be acknowledged to convey empathy for the client; clients may be reminded to accept and surrender to the experience. Repeated suggestions and unconditional acceptance of the client’s negative feelings in the substance-assisted session may challenge conditioned feelings of rejection and foster general acceptance (Spencer, 1964). Attempts to distract the client from the intensity of the situation are likely to be counterproductive. If appropriate, certain techniques might be used to ease the tension and support the client: During times of heightened anxiety, several containment techniques can be borrowed from different therapeutic approaches, including relaxation techniques taught in CBT and Prolonged Exposure Therapy, and mindful diaphragmatic breathing (Mithoefer, 2013). In their manual for psilocybin for depression using acceptance and commitment therapy (ACT), Sloshower et al. (2020) offer scripts for several grounding techniques including abdominal breathing, therapeutic touch, and body awareness exercises that are closely followed when participants experience distress. Generally, the client is encouraged to confront rather than avoid painful, difficult, or challenging affective states. In the case of further escalations, anxiolytic or antipsychotic medications may be administered, or, as a last resort, the client may be transferred to an emergency department (Johnson et al., 2008; Strassman, 1984; Watts, 2021). Research regarding different responses and interventions for challenging experiences is currently lacking.
To conclude the session, clients might draw or paint as they desire (Cohen & Eisner, 1959). Alternatively, guided imagery has been used in later parts of the administration sessions in some studies (Carhart-Harris et al., 2016; Johnson et al., 2014). Gucker (1963) suggested that external symbolization might be used in the form of play therapy. By working through material that prompts internal conflicts, unconscious processes might be discharged in the form of hallucinations, and additional physical abreactions might occur. All emerging materials should be properly and continuously integrated (Gucker, 1963). The efficacy of these techniques and methods has not yet been investigated in rigorous studies.
Projection, Transference, and Countertransference
Grof (1980) suggests that in SAPT transference aspects of the therapeutic relationship and strong emotional projections can be more pronounced than in regular psychotherapy. The intensity of transference may be proportional to resistance against facing the issues at hand. It is unclear whether transference situations in SAPT can or should be handled similar to transference in conventional psychotherapy. Due to the hallucinatory effects of some substances and the psychodynamic-autobiographical experiences and symbolization, the usual misidentification (on the conceptual level) in transference may become amplified to complete identification (on the perceptual level) of the therapist(s) with different persons or entities (Cattell, 1957). There have not been any investigations into whether the development and analysis of transference is essential for therapeutic progress in SAPT (Grof, 1980).
It is suggested that the subjective experience of transference may vary widely (Cutner, 1959). Several authors highlight that the therapist(s) is responsible for accepting and potentially dissolving the transferences and projections that may arise. The therapist(s) should aim to support the client throughout the issues and should be aware of their own reactions and potential counter-transferences (Buckman, 1967; Cutner, 1959; Mithoefer, 2013; Möckel Graber, 2010; Spencer, 1963). Related issues may include problems of authority, sexual tension, physical touch, client demands, and client wishes that need to be handled appropriately (Möckel Graber, 2010). If therapists are persuaded to act out instead of remaining centered, clients might be prevented from gaining insights (Buckman, 1967; Savage, 1957). Therapists should seek supervision to reexamine their motivations and reactions and discuss and resolve these potential pitfalls (Buckman, 1967).
Projection, transference, and countertransference can be discussed with clients in the preparation phase (see Thal et al., 2022) and it should be agreed that negative reactions from clients toward the therapist(s) will not be taken personally in the substance-assisted session. These phenomena may be regarded as normal and might become opportunities for the processing of unconscious material. Due to the heightened sensitivity to verbal and nonverbal expression under the influence of psychoactive substances in a dosing session, honest and open discussion about related feelings should be encouraged (Mithoefer, 2013). A positive therapeutic relationship may alleviate disruptive transference reactions and facilitate working with these phenomena (Cattell, 1957; Cohen & Eisner, 1959; Hausner & Dolezal, 1963). The current evidence for the excessive occurrence of these phenomena in SAPT is anecdotal.
Therapeutic Misconduct
One of the most frequently noted therapist issues is when unresolved problems within the therapist(s) become a burden for the client. Feelings of anxiety, helplessness, powerlessness, or disorientation may manifest as the therapist(s) not remaining grounded or becoming unable to provide a holding function (Cutner, 1959; Fadiman, 2011; Möckel Graber, 2010). Likewise, there may be a risk of the therapist(s) feeling extraordinarily special, developing unhealthy grandiosity and narcissism, or adopting the role of a leader or guru instead of an equal human caretaker (Haartman, 2001; Möckel Graber, 2010; Rodger, 2018). As in conventional psychotherapy, therapists should resist any temptation to make the client dependent on them (Buckman, 1967).
Of greater concern are reported issues of sexual misconduct and unwanted sexual advances by therapists within SAPT sessions (e.g., https://maps.org/2019/05/24/statement-public-announcement-of-ethical-violation-by-former-maps-sponsored-investigators/). There is increased potential for these sexual boundary violations within SAPT sessions, due to the increased suggestiveness and vulnerability of clients under the influence of certain psychoactive substances. While experiential evidence suggests that some occasions of therapeutic touch (i.e., holding hands) can decrease clients’ anxiety and offer support during challenging experiences (Mithoefer, 2017; Sloshower et al., 2020; Watts, 2021), it is vital that any physical touch is nonsexual, used for support, and is explicitly discussed and consented to prior to administration. Therapists should remain aware of any sexual tension, but this should never be acted upon (Cutner, 1959; Fadiman, 2011; Möckel Graber, 2010).
Concluding Administration Sessions
The literature also highlighted the importance placed on concluding administration sessions. It has been suggested that the therapist(s) should facilitate a smooth transition to the everyday state of consciousness. Clients may be invited to talk about their experience and reflect on their respective emotions. The therapist(s) may take notes and focus on eliciting phenomenology (Sloshower et al., 2020). Alternatively, clients may engage in narrative writing to summarize and recollect their experiences (Johnson et al., 2014). Several authors suggest that interpretations or lengthy recollections of the experience should, however, be postponed to the first integration session, which is usually scheduled for the next day (Greer & Tolbert, 1998; Mithoefer, 2017; Sloshower et al., 2020). Some guidelines suggest that a significant other or important person can be invited to join the client for the preliminary integration process—provided that their visit would be supportive to the client and not interfere with the therapeutic process (Mithoefer, 2017; Spriggs et al., 2021). The inclusion of a partner or support person has not been common practice in all clinical trials. Aftereffects of the substances (Majić et al., 2015) and the expected course of the healing process may be discussed. Usually, physiological measures (similar to those prior to the session) are taken and stress level and mental state are assessed (see Thal et al., 2022). If residual emotional or physical symptoms are experienced, appropriate interventions may be employed; this will be explored further in a future paper. Some authors advise that only if the client is mentally and physically stable and the acute effects of the substances have subsided, the therapist(s) may depart from the side of the therapy session (Johnson et al., 2008). Clients usually stay overnight in a comfortable room with an attendant on duty. Alternatively, they may be picked up by a previously appointed and briefed companion (Sloshower et al., 2020; Spriggs et al., 2021; Watts, 2021). Clients are typically encouraged to reflect on the psychedelic experience once the therapist has concluded the substance-assisted session. They may be encouraged to write down or record creative expressions of their thoughts and the content of the session and subsequent experiences, dreams, and reflections. However, it has been noted that if the client remains severely anxious or reports suicidal intent, the therapist(s) ought to stay with the client overnight or consider hospitalization (only under extreme conditions; Johnson et al., 2008; Mithoefer, 2017; Sloshower et al., 2020; Watts, 2021).
Discussion
We conducted a systematized review and outlined information regarding appropriate conduct for therapists in administration sessions in SAPT. To the best of our knowledge, this is the first article to offer a systematic and comprehensive description of the evidentiary basis for current therapeutic conduct in administration sessions of SAPT.
There seems to be a general agreement across sources regarding the overall process of the administration session and the rather unobtrusive and supportive stance of the therapist(s). Evidently, most of the information we extracted about therapeutic conduct in administration sessions was based on anecdotal evidence and research that was conducted before the Controlled Substances Act in 1970. While this evidence is valuable, recent clinical investigations of SAPT have offered only limited details on how administration sessions are conducted. Therefore, there is a pressing need for timelier and more rigorous qualitative and quantitative investigations to evaluate how specific therapeutic conduct during the administration sessions of SAPT affects therapeutic outcomes. Such studies would help to enhance the understanding of the mechanisms involved in the therapeutic benefits of SAPTs and further develop evidence-based practices in this area.
One of the current gaps is the validation of optimal combinations of substances and doses for distinct conditions and disorders. Since the duration of the effects of the substances and their subjective effects differ dramatically, physicians and therapists need to be aware of the pharmacology and effects of different substances so they can suggest the best-suited substance and dosage for their clients based on their experience, the treatment model, and therapeutic goals. Future research should also consider ethnoracial differences regarding the metabolism, safety, and efficacy of particular doses of these substances (Fogg et al., 2021) as women, Black, Indigenous, and People of Color have been underrepresented in current investigations (Michaels et al., 2018). Data do not address the therapeutic potential of the numerous derivatives of the substances included in this review, alone or in combination (Shulgin & Shulgin, 1991, 1997). Although their acute effects can mimic the symptoms of some target disorders (Garcia-Romeu & Richards, 2018), their novel pharmacological impact might have meaningful therapeutic advantages that could be explored in future studies (Eisner, 1964; Johnson, 1969; Schmid et al., 2021; Sherwood et al., 1968).
Current research does not offer conclusive information regarding the optimal number of sessions for specific substances and disorders. Future research should investigate potential links between the number of administration sessions and therapeutic outcomes. Recently, some authors suggested the number of sessions may be adapted to the clients’ needs, the therapeutic goals, the therapeutic process, and the integration of the sessions (Brennan & Besler, 2022; Oehen & Gasser, 2022).
Although several studies explored the effects of music in SAPT, the results are not yet sufficient to form clear guidance. Most of the suggested key criteria (Kaelen, 2021) have not been investigated by rigorous research and currently lack a clear evidence base. While there was a consensus on the potential effects of music, the findings suggesting that this could be facilitative or unwelcome effects (Kaelen et al., 2018), future research is required to examine conditions that are likely to be most useful, potentially including personalized playlists.
Scientific exploration of the value of different kinds of experiences is currently lacking. The data suggested that while the effects of psychoactive substances can be manifold and difficult to predict, some experiences may be more common than others. As such, it is important not to overgeneralize these descriptions of the experiences of individual people. Each session is unique and potentially influenced by the individual’s life situation, biography, dispositions, and many other factors (see, for example, Haijen et al., 2018; Studerus et al., 2012, 2021). Qualitative studies could explore the subjective effects clients may attribute to different kinds of experiences or the value of certain therapeutic interventions to handle them. Quantitative studies may investigate the links between the occurrence and intensity of certain experiences and therapeutic outcome measures.
Rigorous research into therapists’ characteristics and skills is lacking, as well. The evidence we retrieved for this review was largely anecdotal. Future research should explore the influence of therapists’ ability to be present and responsive and the influence of their degree of self-awareness on the therapeutic relationship and the therapeutic outcome. Valid and reliable instruments to assess the perception of therapeutic presence in therapists and clients (e.g., Geller et al., 2010) and therapeutic responsiveness (e.g., Elkin et al., 2013) exist and may be used in future studies (see Thal, Engel, & Bright, 2022).
While the therapeutic techniques we identified may have positive effects in combination with a psychoactive substance, it is impossible to determine whether these effects are due to psychopharmacological effects of the substance, the therapy, or a combination of both. Most of the techniques we summarized are derived from anecdotal reports. Rigorous studies are needed to determine the efficacy of individual techniques, methods, and interventions. It has been proposed that the administration of psychedelics within nondirective and supportive contexts be compared with a structured and manualized CBT context to determine the impact of psychotherapy in SAPT (Horton et al., 2021). Others have suggested to systematically vary and compare the psychotherapy components in preparation, administration, and integration sessions (Luoma et al., 2019). In addition, it would be informative to investigate whether the use of tools such as breathwork and meditation in later parts of the session may offer any benefits (e.g., improved short-term and long-term outcome measures) compared with controls who do not receive these interventions. Above that, investigating whether certain interventions (e.g., holding hands or breathing) for phases of heightened anxiety or other adverse effects are superior/quicker than others in resolving distress in clients (and thus improve therapeutic outcome) is vital. Furthermore, future research should explore whether projection and transference pose significant challenges in SAPT and how to best navigate these situations to inform future training programs for therapists.
Reports of therapeutic misconduct, the potential perception of unequal power dynamics in the therapeutic relationship, and the fact that serotonergic psychedelics like LSD have been linked to increases in suggestibility (Carhart-Harris et al., 2015) highlight the need for a careful evaluation of current practices. Regulatory authorities must examine and, if necessary, handle professional misconduct. Supervision and peer review are important forums to reflect on challenging situations and prevent unethical behavior. Specific and repeated training must be implemented to increase therapists’ ability to offer therapeutic support through consensual and appropriate therapeutic actions while avoiding encroaching behaviors. Future research should explore the specific challenges therapists face conducting therapy in substance-assisted settings. Qualitative investigations of adverse events and challenging situations for therapists are important to inform future training and supervision.
In conclusion, it is evident that although clinical studies using SAPT for the treatment of various psychiatric disorders are steadily evolving, there has been limited research into the variables that potentially influence therapeutic outcomes. Most of the available evidence retrieved from the sources was anecdotal and based on untested philosophical and/or theoretical approaches. As a result, the effectiveness, risks, and essential components of therapeutic interventions remain largely tentative, necessitating systematic investigation to ensure optimal clinical outcomes. As such, conclusive statements regarding best practice during an administration session are not possible at this point. This comprehensive description of the current evidence base may be used to inform the baseline structures and future developments of SAPT training courses. It may also offer therapists interested in SAPT training a basis to evaluate the content of current programs. Future research should systematically investigate how specific therapeutic conduct during the administration sessions and certain experiences of the client affect therapeutic outcomes in SAPT.
Supplemental Material
sj-docx-1-jhp-10.1177_00221678231168516 – Supplemental material for Dosing and Therapeutic Conduct in Administration Sessions in Substance-Assisted Psychotherapy: A Systematized Review
Supplemental material, sj-docx-1-jhp-10.1177_00221678231168516 for Dosing and Therapeutic Conduct in Administration Sessions in Substance-Assisted Psychotherapy: A Systematized Review by S. B. Thal, M. Wieberneit, J. M. Sharbanee, P. M. Skeffington, R. Bruno, T. Wenge and S. J. Bright in Journal of Humanistic Psychology
Footnotes
Acknowledgements
The authors thank Eternity Hausen for proofreading and the linguistic revision of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is a review study. No ethical approval is required.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.