
Abstract
A resurgence of research has begun to systematically examine the relationship between psychedelic use and mental health and well-being. Although preliminary findings examining the therapeutic value of these substances show promise, the mechanisms through which psychedelic use may predict reduced mental distress remain poorly understood. To this end, we surveyed a community sample of individuals (n = 159) who endorsed lifetime psychedelic use to examine relationships among psychedelic use and self-reported spirituality, difficulties in emotion regulation, and symptoms of mental health issues. Results revealed a pathway through which classic psychedelic use predicted greater spirituality, which in turn predicted better emotion regulation, ultimately predicting lower levels of anxiety, depressed mood, and disordered eating. These results contribute to our understanding of potential mechanisms of change with respect to psychedelics and mental health. They also add to the growing body of literature pointing to the healing effects of the cultivation of spirituality and emotion regulation as separate and related constructs.
The group of substances commonly described as classic psychedelics include serotonin (5-HT2A) agonists such as lysergic acid diethylamide (LSD), psilocybin, mescaline, and N,N-dimethyltryptamine (DMT), the active ingredient in the Amazonian plant-based tea ayahuasca. Recent increases in the interest of psychedelics represent Western medicine’s curiosity in what are long-standing Indigenous technologies. The effects of psychedelics are diverse and varied but most are described as inducing altered perception of time and space, a feeling of interconnectivity and oneness, and affective introspection (Griffiths et al., 2006; Johnson et al., 2008; Vollenweider & Kometer, 2010). Plant-based psychedelics have been used for spiritual and healing purposes for millennia (Diaz, 1977; Haviland & Haviland, 1995; Tupper, 2002), and these and other psychedelic substances have reemerged as an object of serious inquiry in medicine (Tupper et al., 2015). Despite substantial obstacles with conducting clinical research, preliminary studies point to the potential of these substances in the clinical treatment of mental health conditions. For example, epidemiological, qualitative, and laboratory-based studies point to lower rates of psychological and behavioral dysfunction among individuals with a history of psychedelic use (Hendricks et al., 2015; Krebs & Johansen, 2012; Lafrance et al., 2017; Thiessen et al., 2018; Walsh et al., 2016). Clinical trials have also examined the anxiolytic and antidepressive effects of psychedelics among terminally ill patients, individuals with treatment-resistant depression, and those struggling with problematic substance use (dos Santos et al., 2016). For example, two double-blind, randomized active placebo studies reported long-term decreases in anxiety following a course of psychedelic psychotherapy for individuals with life-threatening diseases (e.g., various types of cancer) that involved two separate administrations of either LSD (Gasser et al., 2014) or psilocybin (Grob et al., 2011). Results of a small open-label study of psilocybin for treatment-resistant depression also revealed significant and sustained symptom reduction, with a substantial number of patients achieving full remission (Carhart-Harris et al., 2016). Most recently, a double-blind randomized placebo-controlled trial was conducted to test the antidepressant effects of ayahuasca among 29 patients with treatment-resistant depression over 1 week (Palhano-Fontes et al., 2019). Patients received a single dose of either ayahuasca or placebo. Compared with the placebo group, significant antidepressant effects of ayahuasca were noted at all measurement points (1, 2 and 7 days after dosing), suggesting that ayahuasca holds promise as a rapid-onset antidepressant. The ancillary effects of psychedelics are also apparent. For example, participants experienced a sustained increase in openness to experience after taking a high dose of psilocybin (MacLean et al., 2011), while others with a history of psychedelic use reported a stronger connection with nature (Kettner et al., 2019).
Mechanisms of Change
Given this renewed attention to the healing potential of psychedelics, there has been increasing interest in identifying variables that can explain the ways through which psychedelics may be related to improved mental health. Although a number of biochemical, neurobiological, and psychological variables have been proposed, the role of spirituality continues to emerge across numerous studies. Psychedelic substances have been reported to induce increases in overall levels of spirituality, as well as profoundly life-changing mystical experiences (e.g., Griffiths et al., 2006, 2011; Hasler et al., 2004; Horgan, 2003; Shanon, 2003; Strassman, 2001). Presumably because of such effects, plant psychedelics such as psilocybin mushrooms, peyote, and ayahuasca have been central to the traditional spiritual and healing ceremonies of some indigenous cultures of the Americas. Even today, these substances can be used legally if for religious purposes in certain countries, including in Canada and the United States (e.g., Gonzales v. O Centro Espírita Beneficente União do Vegetal, 546 US 418, 2006; Health Canada, 1999).
Increased capacity for emotion processing, including regulation, has also been theorized as a variable of interest in contemporary research, and empirical studies have explored its role in the mediation of positive outcomes related to psychedelic use (Stroud et al., 2018; Thiessen et al., 2018). For example, using a dynamic facial emotion recognition task, Stroud and colleagues assessed individuals with treatment-resistant depression before and after two separate doses of psilocybin. Compared with healthy controls, the experimental group improved in the processing of emotional faces, and this change correlated with reduced anhedonia (Stroud et al., 2018). More recently, a population-based study examining the relationship between psychedelic use and intimate partner violence found that male psychedelic users had decreased odds of perpetrating violence against their current partner, and that this relationship was mediated by an increased capacity for emotion regulation (Thiessen et al., 2018).
A qualitative study conducted among cancer patients with treatment-resistant depression who participated in psilocybin-assisted psychotherapy also explored participant perspectives with respect to mechanisms of action (Watts et al., 2017). Their analyses revealed two main change processes. The first related to a process through which participants reported having evolved from feeling disconnected to connected to self, others, and the world, including a deeper connection to spirituality. The second identified a change process involving shifting from an avoidant style of emotion processing to sustained increases in their capacity to connect with emotions, including in the context of relationships (Watts et al., 2017). The importance of spirituality and emotion regulation have also emerged from qualitative analysis of interviews obtained from individuals who participated in ceremonial ayahuasca use in the context of addiction (Loizaga-Velder & Verres, 2014) and eating disorders (Lafrance et al., 2017). In these studies, increases in spirituality and the capacity for emotion processing were identified as integral components of the healing experience.
Although both spirituality and emotion regulation have been identified as potential mechanisms between psychedelic use and mental health, no research to date has examined the extent to which these two variables together account for this relationship. We propose that one possible pathway is that spirituality may predict a greater capacity to confront life’s challenges and regulate emotional pain. Consistent with this notion, the effects of spirituality on overall health are thought to be primarily mediated via the effect of emotion regulation (Watts, 2007), including effects on physiological processes. For example, increased spirituality has been found to enhance emotion processing capacity by helping to reduce negative arousal, leading to decreases in inflammation and subsequently in overall morbidity (Aldwin et al., 2014; Levenson & Aldwin, 2013). We believe that this mechanism may account for at least part of the relationship between psychedelic use and mental health outcomes, particularly in emotion-based disorders.
The Current Study
In this study, we tested a model whereby we examined the associations between frequency of psychedelic use, self-reported spirituality, and difficulties with emotion regulation in a community-based sample. We also measured symptoms of anxiety, depressed mood, and disordered eating. It was predicted that psychedelic use would be linked to greater spirituality, which in turn would predict a higher capacity for emotion regulation. A higher capacity to manage stress and distress would then be linked to lower levels of depressed mood, anxiety, and disordered eating (see Figure 1). In other words, we hypothesized that both spirituality and emotion regulation would mediate the relationship between psychedelic use and symptoms of depressed mood, anxiety, and disordered eating. Finally, because some work suggests that dose may influence psychedelic use and mental health, with larger mental health benefits being obtained at higher (vs. lower) doses (Griffiths et al., 2016; Roseman et al., 2019), we examine individual differences in frequency of use.
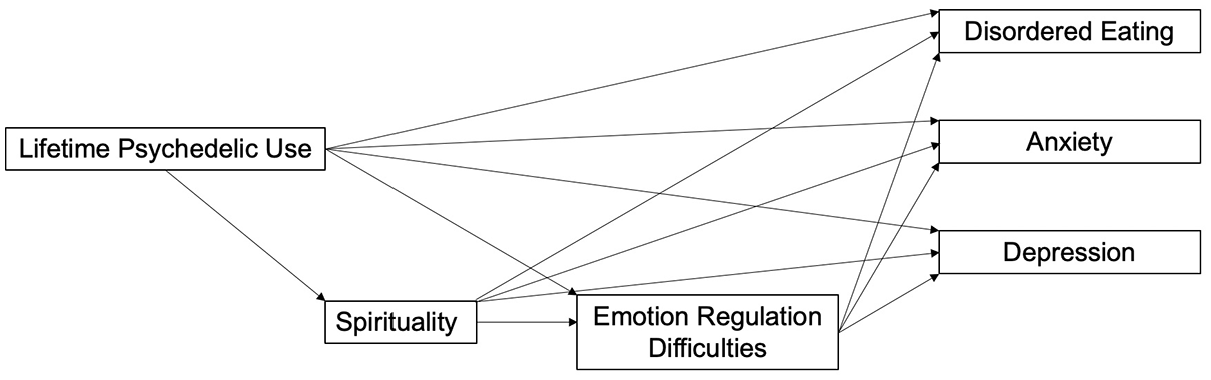
Proposed Mediation Model.
Methods
Participants
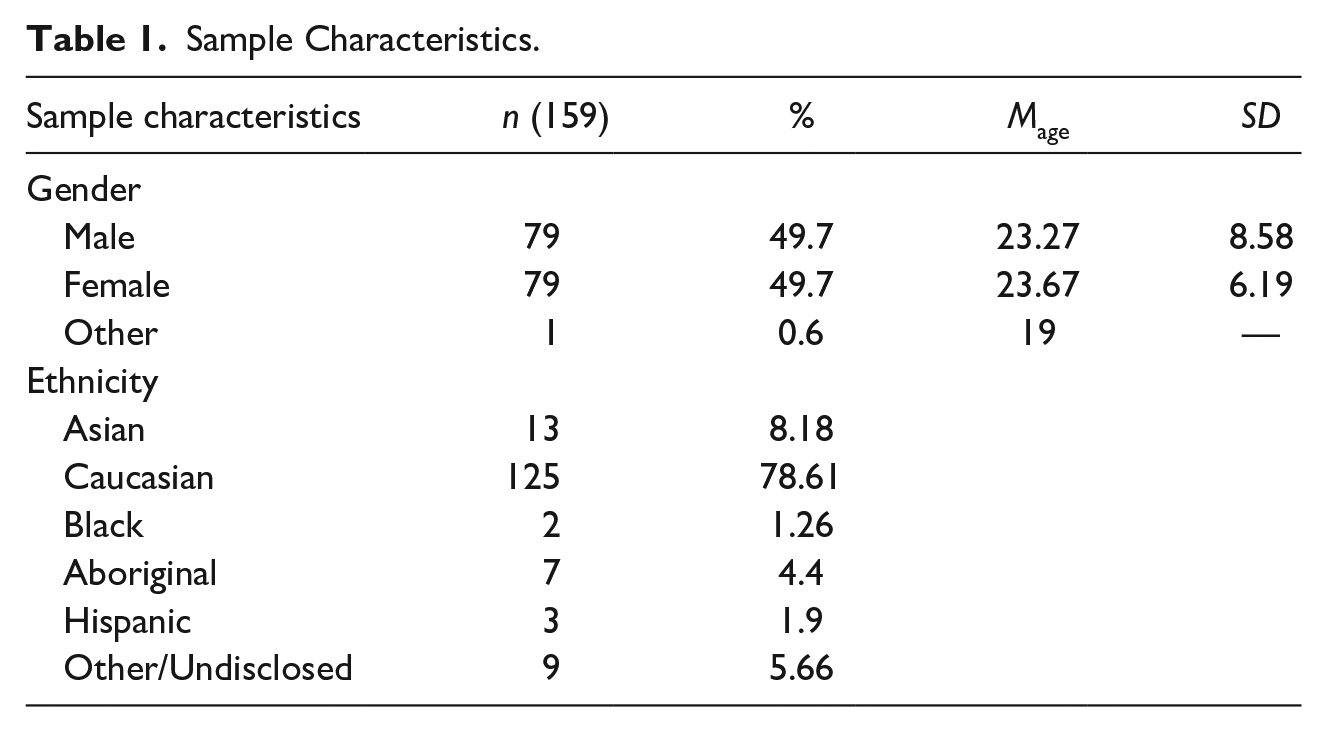
As part of a larger study, 461 participants were recruited from undergraduate psychology classes from two Canadian universities, online from Reddit forums (e.g., r/psychedelic studies, r/psychedelic medicine, r/drugs), and via Amazon’s Mechanical Turk (AMT)—an internet crowdsourcing marketplace. Those who could not read English were excluded from participating. Participants were paid, compensated with course credits, or entered into a draw for a gift card. Participation in the study was voluntary and completed online at the respondents’ discretion. This study was approved by the Research Ethics Boards of The University of British Columbia and Laurentian University, and conducted in accordance with the ethical principles of the Declaration of Helsinki. For this study, a subset of 159 participants who had used psychedelics (32.3% of the total sample) were included in the subsequent analyses to examine how individual differences in frequency of use related to mental health. The participants ranged from 18 to 69 years of age (Mage = 23.44, SD = 7.44); additional sample characteristics are presented in Table 1. Following a process of informed consent, participants were invited to complete an online questionnaire relating to their history of psychedelic use, as well as self-reported ratings of spirituality, difficulties in emotion regulation (DERS), and symptoms of mental health issues. Specific measures are detailed below.
Sample Characteristics.
History of Psychedelic Use
Respondents rated their lifetime psychedelic use on a 5-point Likert-type scale, ranging from 1 (never) to 5 (more than 10 times). Participant scores were summed with higher scores indicating greater lifetime use of one or more of the following substances: LSD, psilocybin, mescaline, DMT, and ayahuasca.
World Health Organization Spirituality, Religiousness, and Personal Beliefs (WHOQOL-SRPB)
The WHOQOL-SRPB is a 32-item questionnaire that measures various aspects of quality of life, with a focus on spirituality, religiousness, and personal beliefs (World Health Organization, 2002). Sample items include “To what extent do you find meaning in life?” and “To what extent do you feel inner spiritual strength?” Questions are presented using Likert-type scales ranging from “1 = not at all/very dissatisfied” to “5 = an extreme amount/extremely/completely/very satisfied,” with possible scores ranging from 32 to 160.
DERS
The DERS is a 36-item self-report measure designed to evaluate patterns of emotion regulation (Gratz & Roemer, 2004). Participants respond to questions on a five-point scale ranging from “0 = almost never” to “5 = almost always” that represent different facets of emotion processing, including lack of emotional awareness and clarity, nonacceptance of emotional responses, difficulty with impulse control, and engaging in goal-directed behavior; and limited access to emotion regulation strategies. Higher scores on this scale represent greater emotion regulation difficulties, with possible scores ranging from 36 to 180.
Beck Anxiety Inventory (BAI)
The BAI is a self-report measure of current generalized anxiety symptoms (Beck & Steer, 1990). The measure has 21 items on which participants rate the severity of each symptom on a 4-point Likert-type scale ranging from “0 = not at all” to “3 = severely.” Total anxiety scores range from 0 to 63, with higher scores indicating greater symptoms of anxiety.
Center for Epidemiologic Studies Depression Scale Revised (CESD-R)
The CESD-R is a 20-item screening test for depression and major depressive disorder (Eaton et al., 2004). This measure asks participants to rate each item on a 5-point Likert-type scale ranging from “0 = rarely or none of the time” to “4 = most or all of the time.” The total CESD-R score is calculated as a sum of responses to all 20 questions, with higher scores indicating greater symptoms of depressed mood.
Eating Disorders Examination Questionnaire (EDE-Q)
The EDE-Q is a 30-item questionnaire designed to measure the range and severity of eating disorder characteristics and behavioral symptoms (Fairburn & Beglin, 1994). The measure includes questions relating to disordered eating thoughts and behaviors within the past 28 days and requests that the participants rate the frequency of engagement with each symptom using the scale: “0 = no days” to “6 = every day.”
Analytic Approach
Descriptive statistics were conducted for all variables included in this study. As an initial test of the links in the proposed model, a series of regression analyses were conducted. To test the model as a whole, AMOS Graphics 20.0 structural equation modeling software was employed.
Results
Descriptive Statistics
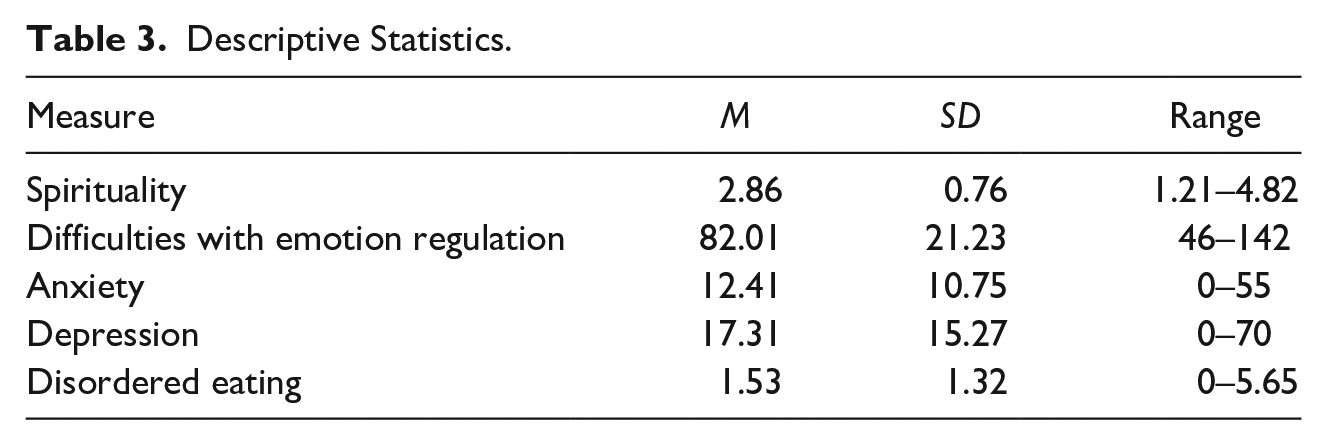
Approximately 96% (n = 152) of the sample reported past use of psilocybin, and a third of individuals (n = 52) reported using more than one type of classic psychedelic (see Table 2 for psychedelic use). Descriptive statistics for spirituality, emotion regulation, anxiety, depression, and eating disorder symptoms are presented in Table 3.
Psychedelic History.
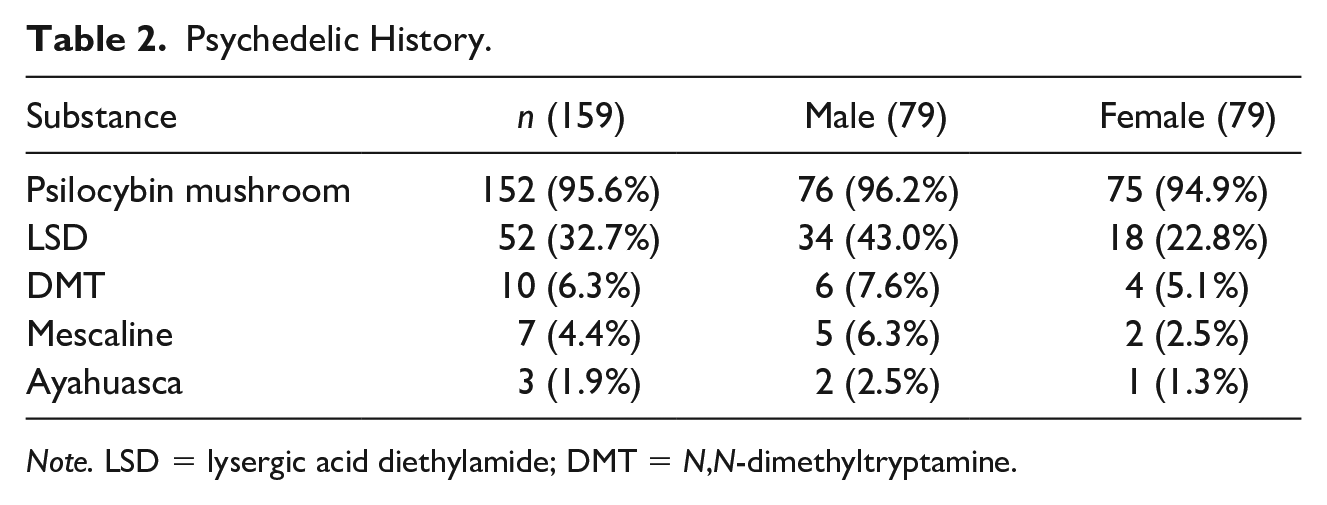
Note. LSD = lysergic acid diethylamide; DMT = N,N-dimethyltryptamine.
Descriptive Statistics.
Links Between Psychedelic Use and Spirituality
We predicted that higher psychedelic use would be linked to higher levels of spirituality; in other words, we expected that our independent variable (IV) would predict our first mediator. To test this hypothesis, we ran a simple regression analysis testing whether psychedelic use predicted spirituality. We found support for our hypothesis: Participants who reported more frequent use of psychedelics reported higher levels of spirituality, b = .155, t = 1.95, p = .052, R2= .024.
Link Between Spirituality and Emotion regulation
We hypothesized that higher levels of spirituality would be related to fewer difficulties with emotion regulation. That is, as spirituality increased (our first mediator), participants’ capacities in regulating their emotions (second mediator) would also increase. To test this prediction, we ran a simple regression analysis testing whether spirituality predicted DERS. We found support for our hypothesis: participants who reported higher levels of spirituality reported an increased capacity for emotion regulation (indicated by less emotion regulation difficulties), b = −.395, t = −5.38, p < .001, R2= .156. Thus, the first mediator predicted the second mediator in our model.
Links Between Emotion Regulation and Anxiety, Depressed Mood, and Disordered Eating
We then conducted regression analyses to test whether DERS predicted levels of self-reported anxiety, depressed mood, and disordered eating. In other words, we tested whether the second mediator predicted the three dependent variables (DVs) in our model. We conducted three separate regression analyses to test these predictions. In the first regression analysis, we found that DERS positively predicted endorsement of symptoms of anxiety, such that the more difficulty participants had regulating their emotions, the more anxiety they experienced. In the second regression analysis, we found that DERS were also linked to the endorsement of symptoms of depressed mood. The more participants reported difficulties with emotion regulation, the higher their rate of depressed mood. Finally, we found that DERS positively predicted disordered eating. That is, the more participants reported difficulties with emotion regulation, the more eating disorder symptoms they reported (see Table 4 for regression findings). Thus, we found that the second mediator predicted all three DVs in our model.
Multiple Regression Results for Anxiety, Depression, and Disordered Eating.
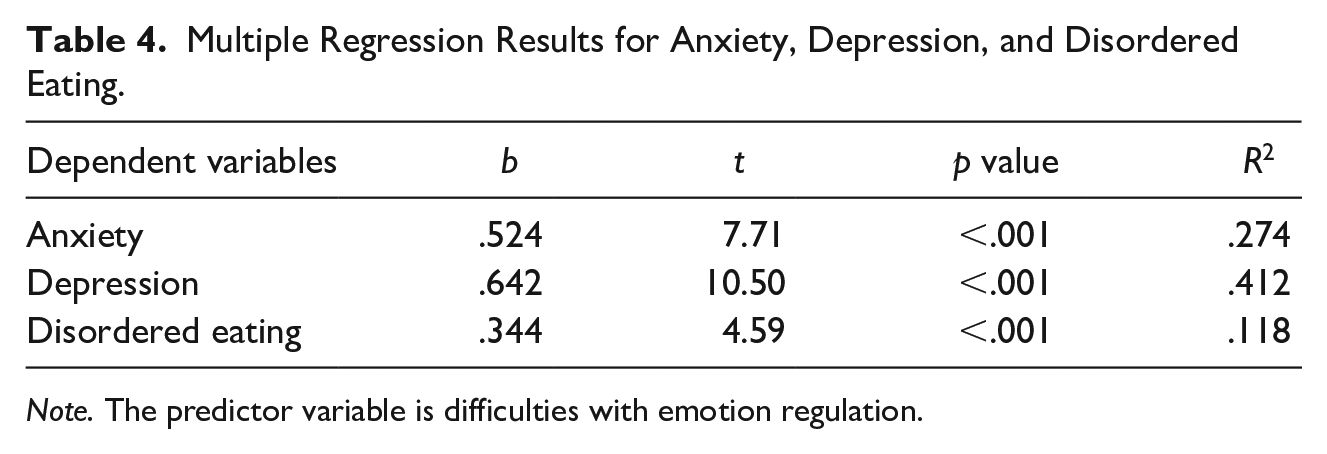
Note. The predictor variable is difficulties with emotion regulation.
Test of Mediation Model
Examination of the distribution of psychedelic use scores revealed that this variable was highly positively skewed with most participants reporting lower frequency of use. As a result, the psychedelic use variable was log-transformed (using a base of 10) resulting in a distribution of scores that more closely approximated a normal distribution. Because the scaling of the instruments used to address the key variables in our proposed model differed drastically (see methods for more detail), all measures were mean centered, including the log-transformed psychedelic use variable, prior to running the main model. We predicted that psychedelic use (IV) would predict spirituality (Mediator 1), which in turn would predict capacities for emotion regulation (Mediator 2), which in turn would predict the three DVs: anxiety, depressed mood, and disordered eating. To test our predictions, we used AMOS Graphics 20.0 structural equation modeling software. We entered psychedelic use as the IV, spirituality as the first mediator, emotion regulation as the second mediator, and anxiety, depressed mood, and disordered eating as the three DVs. The errors of all three DVs were allowed to correlate, and 95% confidence intervals (CIs) for the indirect effects were estimated using bias-corrected bootstrapping based on 1,000 samples. See Figure 2 for the final model with standardized estimates (n = 159). As can be seen in Figure 2, there was a significant indirect effect of psychedelic use on anxiety, 95% CI = [−.08, −.009], p = .015, depressed mood, 95% CI = [−.09, −.01], p = .016, and disordered eating, 95% CI = [−.05, −.005], p = .014. Because the CIs do not include 0, one can conclude that the indirect effects were significant at p < .05. Furthermore, the direct effect of psychedelic use on anxiety, depressed mood, and disordered eating were all nonsignificant. Thus, we found support for our proposed path model: Spirituality and emotion regulation together accounted for a portion of the relationship between psychedelic use and the three dependent measures of anxiety, depressed mood, and disordered eating.
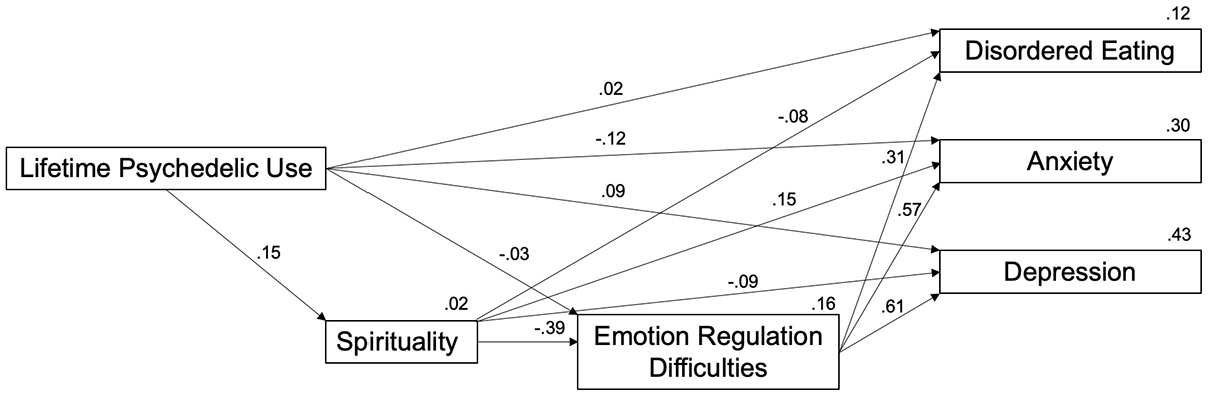
Path Analysis Using Structural Equation Modeling.
Discussion
While spirituality and emotion-processing capacity have each been linked to psychedelics and mental health outcomes, no study has examined their combined pathways of influence. The present findings demonstrate a possible pathway from psychedelic use to mental health, wherein more frequent psychedelic use is related to higher reported spirituality, which predicts higher emotion regulation, ultimately predicting better mental health across different domains. These results provide initial evidence of the synergistic role of both spirituality and emotion-processing capacity for mental health and well-being.
Previous research has found that following psychedelic use, higher scores on the Mystical Experience Questionnaire and a measure of emotional breakthrough predict increases in well-being in a dose-dependent manner (Roseman et al., 2019). Specifically, higher estimated psychedelic doses were associated with the greatest change in mystical experience and emotional breakthrough, leading to greater well-being. To the degree that peak spiritual experiences and emotional breakthrough follow from higher doses of psychedelics, it could be hypothesized from this study that more substantial dosing could also lead to greater changes in one’s ability to regulate emotions. There is also the possibility of a ceiling effect, including the influence of factors that limit therapeutic use and effects. To clarify this question, and given that deficits in emotion regulation are relevant for the development and maintenance of various mental health disorders (Berking & Wupperman, 2012), the therapeutic value of higher doses of psychedelics will be an important consideration for future work. In line with this proposal, a recent controlled trial found that high doses, but not low doses of psilocybin, were responsible for decreases in anxiety and depression (Griffiths et al., 2016). As others have noted, however, the degree to which higher doses of psychedelics predict therapeutic benefit will also depend on context (Hartogsohn, 2016), such that greater benefit is likely to be achieved when done in a psychologically supportive environment (Carhart-Harris & Goodwin, 2017). Psychotherapy provides such psychological support, and therefore, the consideration of using psychedelics at various doses with different forms of psychotherapy, such as the third wave behavior therapies (Walsh & Thiessen, 2018), will likely be a key research area for future work.
The present findings also contribute to the resurgence of research on the therapeutic potential of psychedelics. Despite promising results from early work in the 1960s, political pressures and legislative changes led to a slowing and eventual halt of experimental research in 1970. The increase in research over the past decade has once again shown promising results in finding, for example, that psychedelics can significantly reduce symptoms of depression, anxiety, and substance use (see Reiff et al., 2020, for review). More research using rigorous controlled trials will be required to determine how these substances can potentially be used in nonresearch clinical contexts, and the nature of the results presented here and elsewhere suggests that this is a worthwhile endeavor. Indeed, granting agencies and researchers appear to be slowly embracing the importance of this work (Reiff et al., 2020).
It is also important to note that although psychedelic psychotherapy is a relatively young area of scientific inquiry, connection with the spiritual world via nonordinary states of consciousness has been facilitated in Indigenous communities across the world for millennia (Michaels et al., 2018). Calls highlight the need for increased representation of communities from which these technologies come (e.g., Black, Indigenous, People of Color) in contemporary psychedelic psychotherapy. As these inequities are addressed, more communities will hopefully benefit, once again, from the increased spiritual connection that psychedelics can foster.
The results of this study also have important clinical implications outside of psychedelic medicine. While the importance of targeting emotion processing skills in psychotherapy is becoming widespread, the appropriateness of religion and spirituality in the context of psychotherapy remains controversial (Brown et al., 2013). However, our study suggests that the degree to which individuals cultivate spirituality may influence their capacities to manage stress and distress, and therefore improve their mental health functioning. In other words, a focus on spirituality appears to be a powerful catalyst for the transformation of emotion processing difficulties which are thought to underlie most emotion-based disorders, including mood, anxiety, and eating disorders. Although the extent that increasing a focus on spirituality in the context of psychotherapy (with or without psychedelic use) predicts positive mental health outcomes will require future research, our preliminary test of the model suggests that it can be useful for clinicians to support their clients in cultivating a greater connection with self, others, the natural world or with spirit, and/or greater involvement with ceremonial or religious practices, as appropriate. For clinicians who were trained to avoid such topics unless directed by the client, a focus on this dimension may feel foreign and possibly uncomfortable, and therefore, more training may be required to do so in a manner that is ethical, client-centered, and ultimately effective. We believe this to be a worthwhile investment, given the ever-present need to find ways of increasing the effectiveness of therapeutic interventions for individuals suffering from treatment-resistant emotion-based disorders (Mennin, 2006).
Limitations
This study is not without limitations. First, no causality can be inferred from this study due to the cross-sectional method employed, and as a result, the findings, particularly those from the path model, should be interpreted with caution. This allows us to estimate the extent to which the relationship between psychedelic use and identified mental health outcomes (depression, anxiety, and disordered eating) is accounted for by spirituality and emotion regulation together, assuming these two variables are mediators of these relationships. However, it does not show unequivocally that these variables are true mediators (Fiedler et al., 2011). Given that approximately 1% of Canadians indicate past year hallucinogen use (Government of Canada, 2012), it is likely that psychedelic users share unique characteristics not found in the general population, and it is therefore possible that an unmeasured factor explains the reported findings. Because of the inherent difficulty with experimentally manipulating psychedelic use, correlational research, such as this study, is an invaluable step in the research process, as it allows us to identify processes that can be tested with experimental protocols. Future research should employ longitudinal and experimental designs to attempt to replicate the current findings, rule out third variables, and confirm the causal direction of the proposed relationships.
Second, although effort was made to recruit a diverse sample of individuals, the majority of psychedelic users came from the university sample, and therefore, the sample lacked diversity. Furthermore, psilocybin mushrooms were the most frequently endorsed psychedelic, and therefore may be exerting more of an influence on the model than the other substances. The small number of individuals endorsing usage of other psychedelics precluded the testing of individual psychedelic substances, which may be an important consideration for future research. Studies with more diverse samples and that examine a wider range of psychedelics are necessary to test the generalizability of the current findings. In addition, frequency of use was relatively low for most participants in the current sample, as evidenced by a positively skewed distribution of psychedelic use scores, and thus, it will be necessary to collect data from samples with greater variation in the frequency of psychedelic use. Future research should also test whether the main model generalizes when users versus nonusers are compared directly.
Third, self-reports of substance use and mental health are susceptible to social desirability bias, which may have reduced the accuracy of responses. Additional research should aim to utilize experimental manipulations of psychedelic use and observational measures of mental health to help demonstrate the robustness of these relationships. Finally, with the correlational design of this study, it may also be that individuals with better distress tolerance are better able to tolerate the powerful experiences that may accompany the use of psychedelics. This, in and of itself, would be a novel and important finding to help maximize the therapeutic potential of psychedelics.
Despite these limitations, this study provides preliminary evidence to suggest that spirituality and emotion regulation may be mechanisms through which psychedelic use relates to improved mental health variables, including anxiety, depressed mood, and disordered eating behavior.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Zach Walsh is in a paid advisory relationship with Numinus Wellness and EntheoTech regarding the medical development of psychedelics and provision of psychedelic psychotherapy.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Research Ethics Boards of The University of British Columbia and Laurentian University and conducted in accordance with the ethical principles of the Declaration of Helsinki.
Author Biographies