
Abstract
Emotion regulation (ER) has been found to contribute to psychological symptoms. Previous studies have mostly examined various aspects of ER in isolation. Comprehensive knowledge regarding the relative influence of distinct aspects of ER is lacking. Also, it is not clear whether distinct aspects of ER are associated with specific psychological symptoms. This cross-sectional study aimed to explore the relative association of six ER indicators (adaptive/maladaptive regulation of negative affect [NA], adaptive/ maladaptive regulation of positive affect [PA], and adaptive/ maladaptive ER repertoire) with three psychological symptom clusters (anxiety, depression, and posttraumatic stress [PTS]). A sample of 759 university students completed measures for these ER indicators and symptoms. Results revealed that taking into account six ER indicators, maladaptive regulation of NA and PA were associated with higher levels of anxiety, depression and PTS. Adaptive regulation of NA and adaptive ER repertoire were unrelated to psychological symptoms. In addition, a larger maladaptive ER repertoire was uniquely associated with increased anxiety. Higher adaptive regulation of PA was specifically associated with less depression. These findings underscore the importance of considering different ER strategies when addressing the role of ER in different psychological symptoms.
Introduction
Most individuals encounter a wide range of adversities throughout their lives, from more subtle negative events to highly stressful challenges (Dohrenwend, 2000). Such stressful events have been found to be associated with psychological symptoms, such as anxiety, depression, and posttraumatic stress (PTS) (Davies et al., 2022; McGowan & Kagee, 2013; Mol et al., 2005; Sokratous et al., 2013). Emotion regulation (ER) is an important factor in whether individuals experience psychological symptoms after stressful events (Miu et al., 2022). According to the Process Model of Emotion Regulation, ER refers to the process of influencing emotions, including strategies to modify emotional circumstances, responses and expressions before and/or after an emotion is generated (Gross, 1998). An extension of this model has emphasised that ER is not limited to the regulation of negative affect (NA), but also includes the regulation of positive affect (PA) (Quoidbach et al., 2015). This integrated framework highlights that effective ER involves both downregulation of NA and upregulation or maintenance of PA. Within this framework, ER strategies may be adaptive or maladaptive, and individuals vary in habitual use and repertoire of these strategies. More specifically, ER strategies employed to downregulate NA, such as practising cognitive reappraisal to reinterpret negative events in a more positive light, are considered adaptive regulation of NA. Conversely, ER strategies that amplify NA, such as individuals excessively dwelling on negative thoughts, are viewed as maladaptive regulation of NA (Nelis et al., 2011). Emotion dysregulation is marked by excessive use of maladaptive ER strategies or insufficient use of adaptive ER strategies (Gross, 1998; Nelis et al., 2011). Meta-analytic reviews have indeed shown that both decreased usage of adaptive ER strategies of NA and increased usage of maladaptive ER strategies of NA were associated with elevated levels of psychological symptoms (Aldao et al., 2010; Schäfer et al., 2017).
Research has increasingly highlighted the importance of PA regulation for mental health (Boelen, 2021; Carl et al., 2013; Quoidbach et al., 2015). PA encompasses a wide range of positive feelings, such as joy, gratitude, and contentment (Nelis et al., 2011). The broaden-and-build theory posits that experiencing PA broadens the scope of attention and cognition, facilitating the building of personal resources, and thereby playing a central role in human flourishing (Fredrickson, 2001). ER strategies employed to maintain and upregulate PA, such as engaging in social sharing to prolong the pleasant of a positive event, are viewed as adaptive regulation of PA. Conversely, ER strategies that may diminish PA, such as dampening feelings of joy or tempering enthusiasm in response to positive events, are seen as maladaptive regulation of PA (Nelis et al., 2011). In their review, Carl et al. (2013) concluded that PA dysregulation occurs across different emotional disorders. Research has shown that lower levels of adaptive ER strategies for PA and increased levels of maladaptive ER strategies for PA were correlated to elevated psychological symptoms (Bijttebier et al., 2012; Boelen, 2021).
Apart from distinct ER strategies, ER repertoire may also affect psychological symptoms. ER repertoire refers to the diversity of ER strategies utilised by individuals, which can be measured by the number of distinct ER strategies reported by participants (Bonanno & Burton, 2013; Cheng et al., 2014). ER repertoire is a key element in ER flexibility research. It has been proposed that individuals with a broader ER repertoire are more capable of flexibly adapting their emotional responses to various challenges and situations (Bonanno & Burton, 2013; Cheng et al., 2014). Additionally, employing multiple ER strategies may yield a synergistic effect (Ford et al., 2019): The combination of different ER strategies may work together in complex ways that have the potential to enhance their ultimate effects. Cheng et al.’s (2014) meta-analysis indicated a small but significant positive association (r = .12) between ER repertoire and psychological adjustment. However, one empirical study found that a smaller ER repertoire was linked to higher borderline personality disorder but not depressive symptoms (Southward et al., 2018), implying variations in the association across different psychological symptoms.
A distinction can be made between adaptive and maladaptive ER repertoire (Southward & Cheavens, 2020). Adaptive ER repertoire refers to the diversity in adaptive ER strategies to regulate both NA and PA. In contrast, the maladaptive ER repertoire encompasses the diversity of maladaptive ER strategies to regulate NA and PA. Southward and Cheavens (2020) found that a larger adaptive ER repertoire was associated with better mood, while a larger maladaptive ER repertoire was associated with worse mood. However, Southward and Cheavens (2020) only had undergraduates rate their mood from 1 to 100 as the emotional outcome, without exploring the association of adaptive and maladaptive ER repertoires with different psychological symptoms.
While existing research on the association between ER and mental health has generated valuable knowledge, at least two limitations necessitate further investigation. First, previous studies have focused on specific aspects of ER in isolation, such as single ER categories (e.g., maladaptive regulation of NA), or specific ER strategies (e.g., cognitive reappraisal or suppression). It seems relevant to obtain a comprehensive understanding of the relative importance of a wider range of ER indicators, including adaptive/maladaptive regulation of NA, adaptive/maladaptive regulation of PA, and adaptive/maladaptive ER repertoire. Two meta-analytic reviews found that maladaptive ER strategies of NA were more strongly associated with psychological symptoms than adaptive strategies (Aldao et al., 2010; Kraft et al., 2023). However, these studies focused on the regulation of NA. One study indeed found that PTS was associated with maladaptive—but not adaptive—ER strategies for PA when controlling for adaptive and maladaptive ER strategies of PA (Boelen, 2021). However, the degree to which adaptive and maladaptive ER of NA and PA, as well as maladaptive and adaptive ER repertoire, are associated with different psychological symptoms is largely unknown.
Second, it is not clear whether distinct ER indicators are associated with specific psychological symptoms. For example, few studies have directly explored the relationship between ER repertoire and symptoms of anxiety. Using scripts of threatening situations, one study found that children with an anxiety disorder used greater numbers of different ER strategies to downregulate their emotions compared to children without an anxiety disorder (Carthy et al., 2010). The authors reasoned that the children felt less able to regulate NA and therefore applied other strategies to reduce NA. Notably, adaptive and maladaptive ER repertoire were not distinguished in that study. Given that anxious individuals often use maladaptive ER strategies such as emotional suppression, rumination, and avoidance (Alawadhi et al., 2023), we speculate that increased symptoms of anxiety are specifically associated with a larger maladaptive ER repertoire. Regarding depression, a key symptom of depression is anhedonia, that is, the inability to experience PA (American Psychiatric Association, 2013). In a review, Vanderlind et al. (2020) proposed that individuals with depression have a reduced desire to experience PA, which results in lower frequencies of adaptive ER strategies to regulate PA and increased use of maladaptive strategies. Empirical evidence indeed indicated that lower levels of adaptive ER strategies of PA were uniquely associated with higher levels of depression but not other psychological symptoms (e.g., PTS and prolonged grief disorder), even when controlling for maladaptive ER strategies of PA (Boelen & Lenferink, 2020; Werner-Seidler et al., 2013). However, it was unclear whether this association was strong enough to hold after controlling for other ER indicators. Finally, PTS may be associated with specific ER indicators. However, to our knowledge, no research has yet examined which ER indicators would be specific for PTS.
In summary, although different ER strategies have been found to be linked to psychological symptoms, a few issues remain unclear. We conducted a cross-sectional study among university students in order to further specify the association between specific ER indicators and specific psychological symptoms. We focused on symptoms of anxiety, depression, and PTS as these are among the most common mental health symptoms (Frazier et al., 2009; January et al., 2018). First, we examined the correlation between six ER indicators and diverse psychological symptoms. We hypothesised that lower levels of adaptive regulation of NA and PA, and a smaller adaptive ER repertoire (i.e., the number of different adaptive ER strategies used) would be associated with more psychological symptoms. In the same line, we expected that higher levels of maladaptive regulation of NA and PA, and a larger maladaptive ER repertoire would be associated with higher levels of psychological symptoms (H1). Second, we examined the relative association of the six ER indicators with anxiety, depression, and PTS, expecting variation across associations. Based on prior research indicating that increased maladaptive ER is more strongly associated with psychological symptoms than decreased adaptive ER (Aldao et al., 2010; Kraft et al., 2023), we anticipated that, when controlling for the shared variance between the six ER indicators, all psychological symptoms would specifically be related to increased maladaptive regulation of NA and PA, rather than to lower adaptive regulation of NA and PA
Method
Participants and Procedure
Data used in this study originated from an internet-based survey addressing cognitive-behavioural and ER variables in different psychological symptoms, including anxiety, depression, and PTS symptoms in students at Utrect University. Participants were recruited using convenience sampling. The original survey did not impose specific criteria for participation, except that it was exclusively accessible to students at Utrect University who were proficient in Dutch. To align with our research objectives, we introduced eligibility criteria for participants aged between 18 and 30 who had encountered negative events in the past year. The final sample for this study consisted of 759 students, with a mean age of 21.45 (SD = 1.85) years old, of whom 655 participants (86%) were females.
Upon expressing interest in participation, students were guided to a secured online platform where they accessed detailed study information, provided informed consent, and completed all designated questionnaires. Participants were compensated with course credits. The study was approved by the Ethics Committee of the Faculty of Social and Behavioural Sciences at (University’s Name) (file number 20–211).
Measures
Adversities
Life Events Scale
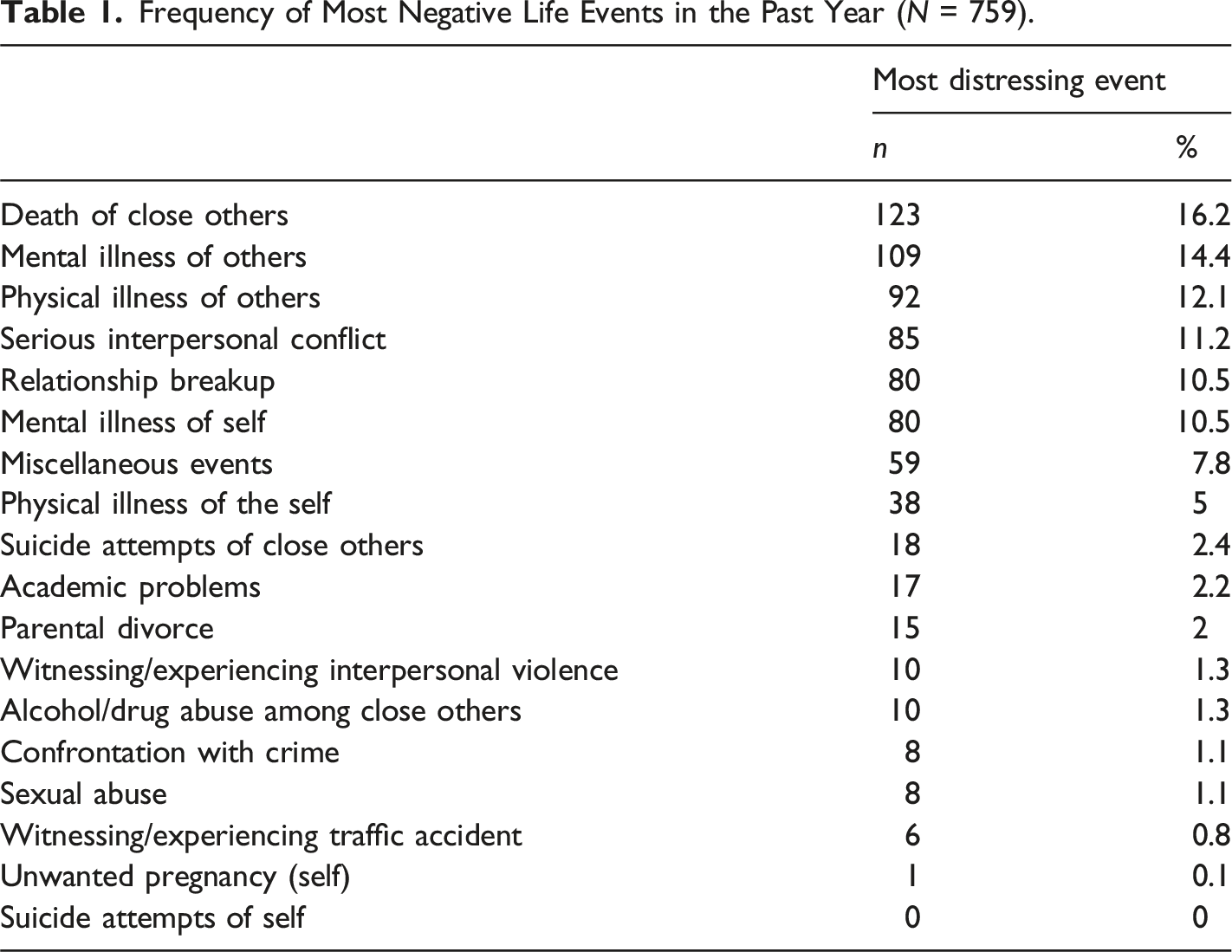
The Life Events Scale (LES), adapted from Garnefski and Kraaij (2001), assessed a range of adverse incidents, including mild to traumatic events like divorce, violence, and sexual abuse. Tailored to the student population, it also covered events like relationship breakups, conflicts, and academic challenges. Participants could also write down miscellaneous events not on the scale. Some events, such as health issues, were reported for both themselves and close relatives. Participants indicated if they experienced these events before age 16, between 16 and 1 year ago, in the previous year, or never. We focused solely on negative events within the past year, ensuring that their emotional responses were recent and relevant. After completing the LES, participants identified the most distressing event, serving as the anchor for measuring PTS.
Psychological Symptoms
Beck Anxiety Inventory
The Beck Anxiety Inventory (BAI) is a 21-item self-report questionnaire used to evaluate the severity of anxiety symptoms (Beck et al., 1988). Participants rate their experiences over the past week on a 4-point Likert scale ranging from 0 (‘not at all’) to 3 (‘severely’). Both English (Beck et al., 1988) and Dutch versions (Muntingh et al., 2011) of the BAI demonstrated adequate psychometric properties. Cronbach’s α in the current study was .92.
Beck Depression Inventory-II
The Beck Depression Inventory-II (BDI-II) is a 21-item self-report questionnaire assessing depressive symptoms (Beck et al., 1996). Each item has four statements that represent different symptom levels of depression severity. Participants pick the best match to their experience over the past two weeks. For example, in the item about sadness, they select from four statements 0 (‘I do not feel sad’), 1 (‘I feel sad much of the time’), 2 (‘I am sad all of the time’), or 3 (‘I am so sad or unhappy that I can’t stand it’). Both English (Beck et al., 1996) and Dutch versions (Van der Does, 2002) of the BDI-II have demonstrated adequate psychometric properties. Cronbach’s α in the current study was .93.
Posttraumatic Symptom Scale Self-Report Version
The Posttraumatic Symptom Scale Self-Report Version (PSS-SR) is a 17-item self-report questionnaire designed to evaluate PTS symptoms, including re-experiencing, avoidance, and hyperarousal, based on DSM-IV criteria (Foa et al., 1993). Individuals rated their experiences over the past month on a 4-point Likert scale ranging from 0 (‘not at all’) to 3 (‘five or more times per week/almost always’), focusing on the most distressing event in the past year (as indicated on the LES). Both the English (Foa et al., 1993) and Dutch versions (Engelhard et al., 2007) of the PSS-SR exhibited satisfactory psychometric properties. Cronbach’s α in the current study was .89.
Emotion Regulation
Emotion Regulation Profile Revised
The Emotion Regulation Profile Revised (ERP-R) is a vignette-based measure to assess the regulation of NA and PA (Nelis et al., 2011), involving 15 scenarios (see Figure 1 for a visual representation of ERP-R). The ERP-R includes nine scenarios describing situations that elicit NA, such as anger, sadness, and fear. Each scenario is followed by four adaptive ER strategies of NA (e.g., positive reappraisal, see Figure 1 for all ER strategies) and four maladaptive ER strategies of NA (e.g., rumination). Additionally, there are six scenarios describing situations that elicit PA, such as joy, excitation, and pride. Each scenario is followed by four adaptive ER strategies of PA (e.g., capitalising on positive experiences) and four maladaptive ER strategies of PA (e.g., inattention). Understanding the emotion regulation profile revised: A visual representation.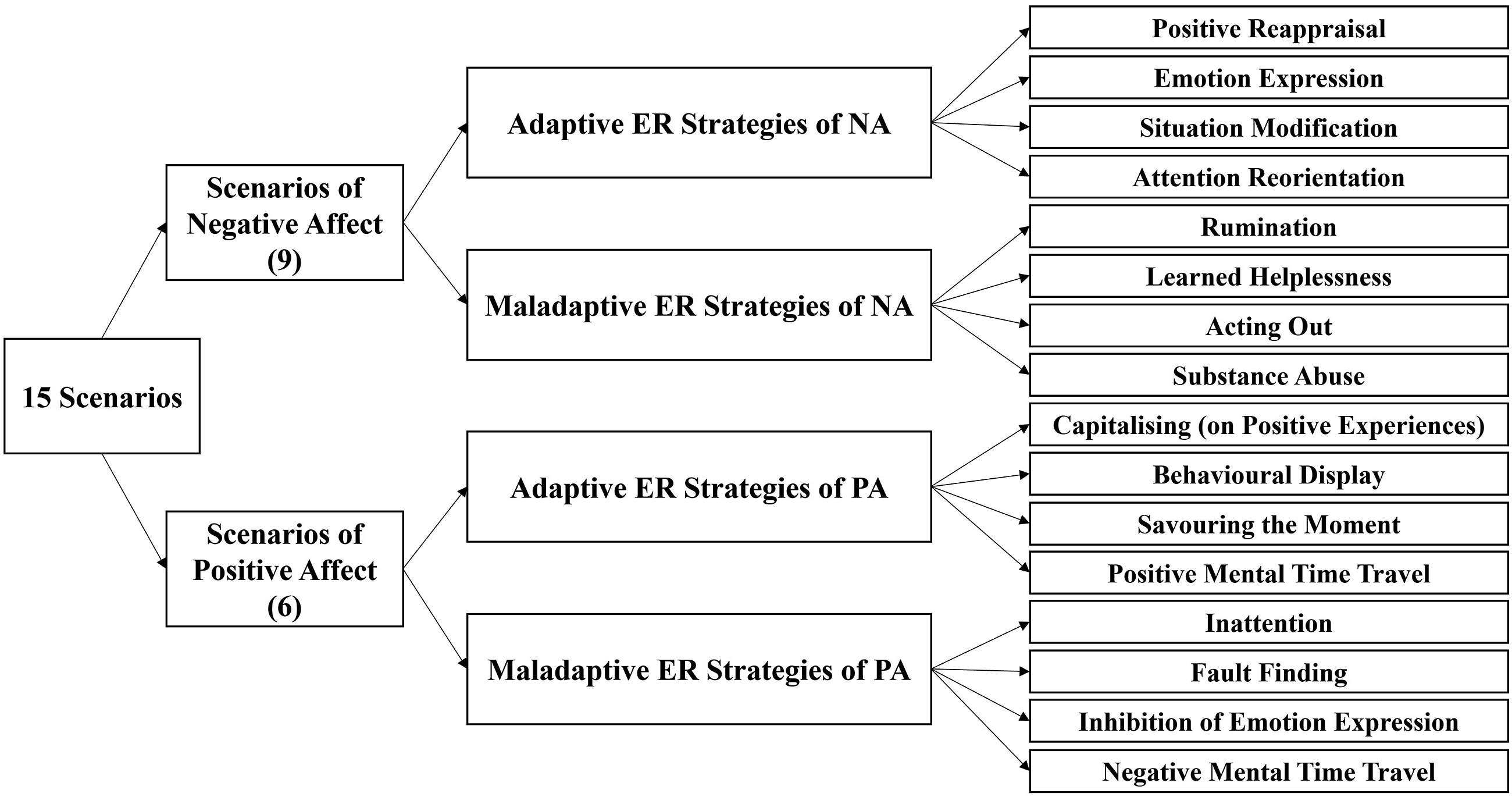
Regulation of NA and PA
Four scores were calculated as indicators of ER for NA and PA: adaptive regulation of NA, maladaptive regulation of NA, adaptive regulation of PA, and maladaptive regulation of PA. Each ER indicator score was calculated by summing the total number of times an ER strategy was chosen across the 9 negative scenarios. That is, each time a particular strategy was selected across different scenarios, this was scored as 1 point for one of the four categories (maladaptive/adaptive regulation of NA/PA). For example, the index for adaptive regulation of NA was calculated as the total number of times each of the four adaptive ER strategies was chosen across the 9 negative scenarios. In the current study, Cronbach’s α for adaptive NA regulation, maladaptive NA regulation, adaptive PA regulation and maladaptive PA regulation were .80, .80, .84, and .78, respectively.
ER Repertoire
Indices of adaptive ER repertoire and maladaptive ER repertoire were calculated by counting the unique strategies used across all scenarios. The adaptive and maladaptive ER repertoire scores were both computed as the total number of different adaptive ER strategies and maladaptive ER strategies, respectively, that were endorsed for the negative and positive scenarios (thus ranging from 0 to 8 for the adaptive and 0 to 8 for the maladaptive ER repertoire). For an example calculation of the regulation of NA, PA and ER repertoire, please see Supplemental Figure 1.
Statistical Analyses
Data were analysed using Rstudio (version 2023.06.1+524 software). There were 1.2% missing values. Little’s MCAR (missing completely at random) test showed a non-significant result (p > .05), indicating that missing data were missing completely at random. We performed multiple imputations to handle the uncertainty associated with missing data. The mice package (Buuren & Groothuis-Oudshoorn, 2011) was used to perform multiple imputations using chained equations, with 20 imputed datasets and 20 iterations. The observed and imputed data were largely similar, indicating that the multiple imputation procedure achieved its goals.
Descriptive statistics were used to map out events participants had been exposed to during the previous year. For H1, we calculated bivariate correlations to assess the relationships between the six ER indicators (adaptive/maladaptive ER of NA and PA, and adaptive and maladaptive ER repertoire) and the three outcome variables (anxiety, depression, and PTS). For H2, assumptions for multiple linear regression were assessed (Osborne & Waters, 2019), including linearity, normality, homoscedasticity, and multicollinearity. Normality was evaluated using kurtosis, skewness tests, and a Q-Q plot. When the assumption of normality was violated, the three dependent variables were transformed using the R-package bestNormalise (version 1.8.3) to ensure normality (Peterson, 2021). This automated procedure effectively transformed the input variables to approximate normality. Homoscedasticity was examined through actual residuals plotted against predicted residuals and studentised Breusch-Pagan test. Multicollinearity was assessed using Variance Inflation Factors (VIFs), with VIF values below 5 and tolerance values exceeding 0.2, indicating no multicollinearity. Next, three multiple regression analyses were conducted to explore the association of each ER indicator with symptoms of anxiety, depression, and PTS, while controlling for the shared variance of the other ER indicators. All analyses were repeated using participants without missing values (n = 632), yielding results that were approximately consistent with results obtained from multiple imputed datasets (see Supplemental Table 1 and Table 2).
Results
Frequency of Most Negative Life Events in the Past Year (N = 759).
Association Between Six ER Indicators and Psychological Symptoms
Descriptive Statistics and Correlations of all Symptoms and ER Indicators (N = 759).
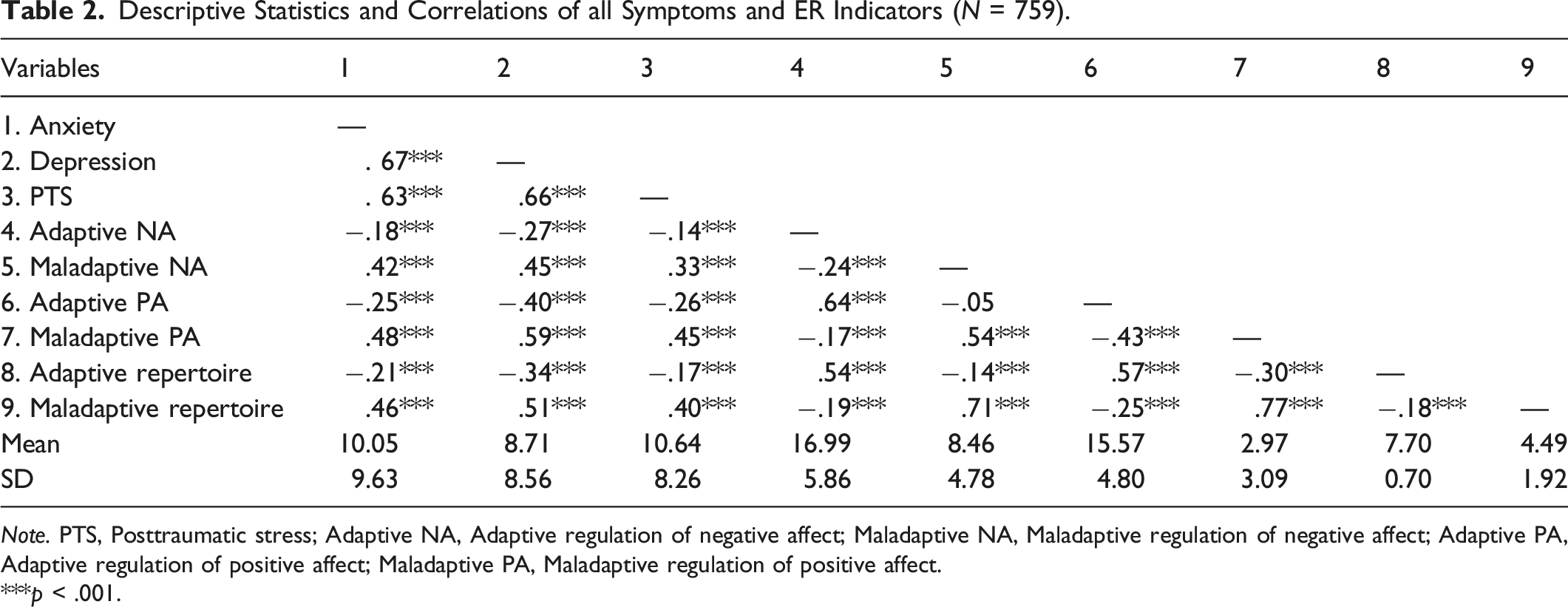
Note. PTS, Posttraumatic stress; Adaptive NA, Adaptive regulation of negative affect; Maladaptive NA, Maladaptive regulation of negative affect; Adaptive PA, Adaptive regulation of positive affect; Maladaptive PA, Maladaptive regulation of positive affect.
***p < .001.
Six ER Indicators in the Prediction of Psychological Symptoms
Results of Multiple Regression Analyses for Symptoms of Anxiety, Depression, and PTS.
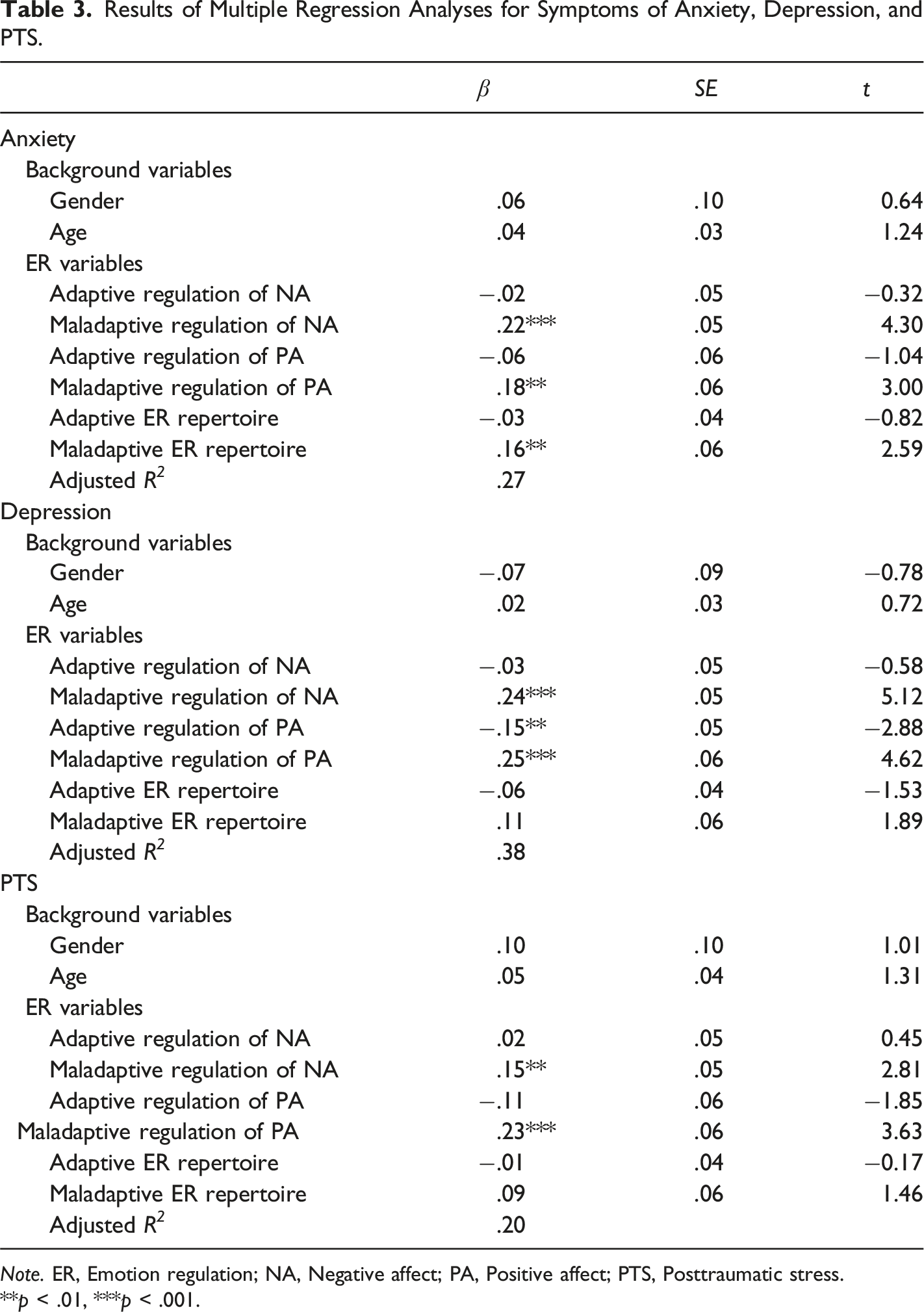
Note. ER, Emotion regulation; NA, Negative affect; PA, Positive affect; PTS, Posttraumatic stress.
**p < .01, ***p < .001.
Discussion
The present study sought to broaden our knowledge about the role of different ER indicators in symptoms of anxiety, depression, and PTS, which are among the most commonly reported psychological symptoms in student samples (Frazier et al., 2009; January et al., 2018). In line with H1, the degree to which participants endorsed adaptive ER strategies was negatively related to the severity of psychological symptoms, and the degree to which they endorsed maladaptive ER indicators was positively associated with this severity. This finding is broadly consistent with the Process Model of ER (Gross, 1998; Quoidbach et al., 2015), postulating that ER involves a series of processes through which individuals modify their emotional experiences, including the use of adaptive and maladaptive ER strategies in regulating NA and PA. Our finding also aligns with previous research suggesting that adaptive ER strategies (e.g., positive reappraisal, emotion expression) are generally protective against psychological symptoms, whereas maladaptive ER strategies (e.g., rumination, substance use) are risk factors for developing such symptoms (Aldao et al., 2010; Schäfer et al., 2017). Our study also distinguished between adaptive and maladaptive ER repertoires. As expected, a smaller adaptive ER repertoire and a larger maladaptive ER repertoire were both associated with increased psychological symptoms. Our findings were consistent with previous findings (Southward & Cheavens, 2020), which indicated that possessing a larger repertoire of adaptive ER strategies may be conducive to psychological outcomes, while reliance on broader maladaptive ER strategies may be detrimental.
Interestingly, a different picture emerged after controlling for the shared variance of the six ER indicators. That is, maladaptive regulation of both NA and PA still predicted higher levels of anxiety, depression, and PTS, but adaptive regulation of NA and adaptive ER repertoire no longer did (H2.1). This is in line with previous research, in which maladaptive ER was also a stronger predictor than adaptive ER, for both adults and youth (Aldao et al., 2010; Kraft et al., 2023). Our findings suggest that the use of maladaptive ER strategies is more critical in the development and maintenance of psychological symptoms than the absence of adaptive ER strategies. However, this does not mean that adaptive ER strategies are not relevant for psychological symptoms. They may be relevant but overshadowed by maladaptive strategies. Or alternatively, they may become more relevant in case of high levels of maladaptive ER strategies (Aldao & Nolen-Hoeksema, 2012). That is, they may buffer against the effects of maladaptive strategies or against high symptom levels.
Supporting H2.2, we found that a larger maladaptive ER repertoire was uniquely associated with higher levels of anxiety, but not with depressive or PTS symptoms. This finding is in line with one previous study, in which children with anxiety disorders used more different ER strategies compared with their non-anxiety peers (Carthy et al., 2010). We examined the ER repertoire in more detail and found that the association was specifically between maladaptive (but not adaptive) ER repertoire and anxious symptoms. There may be three possible explanations for this larger maladaptive ER repertoire in anxiety. First, as Carthy et al. (2010) suggested, anxious individuals may feel less capable of regulating and therefore switch to different ER strategies to reduce NA. Second, possibly, different ER strategies here may represent a single latent strategy, that is more frequently used in anxiety-provoking situations. Third, the maladaptive ER strategies listed in our ER measure (e.g., inattention, substance abuse, negative mental time travelling) may be typically used to reduce anxiety rather than depression or PTS. In any case, future research is needed to validate this finding.
Supporting H2.3, after controlling for different ER indicators, adaptive regulation of PA was specifically associated with lower levels of depressive symptoms but not anxiety or PTS. This finding aligns with the notion that (mal)adaptive PA regulation plays a crucial role in depressive symptoms (Vanderlind et al., 2020, 2022). Depression is characterised by anhedonia and a diminished capacity to experience pleasure, making the regulation of PA particularly relevant (Vanderlind et al., 2020). Enhancing PA through adaptive strategies such as savouring and gratitude exercises can directly counteract the deficits in PA seen in depression (Vanderlind et al., 2020). By boosting PA, adaptive regulation of PA can assist individuals facing adversities in experiencing more pleasure and finding meaning in their daily lives, thereby associated with lower depressive symptoms (Fredrickson, 2001). Our findings also suggest that this relationship may be unique to depressive symptoms, as it was not observed with anxiety or PTS.
Apart from maladaptive regulation of both NA and PA, which predicted PTS but also anxiety and depressive symptoms, no other specific ER indicators were related to PTS, after controlling for different ER indicators. Notably, one thing not covered in this study was that even though higher levels of anxiety, depression, and PTS were all associated with higher levels of maladaptive strategies, the specific ER strategies (e.g., rumination and inhibition of emotion expression) may differ among these clusters. Future research is needed to further examine if different maladaptive ER strategies and mechanisms differ among anxiety, depression, and PTS.
Limitations
Several limitations should be considered when interpreting our results. First, the cross-sectional design of our study limits our ability to establish causation or capture the intricate interplay between ER and psychopathology. It is possible that maladaptive ER contributes to the development or exacerbation of psychological symptoms, but it is also plausible that the presence of psychological symptoms influences the effect and presence of ER strategies. Longitudinal studies are needed to elucidate the temporal sequence and potential causal relationships between ER and psychopathology. Second, the sample was limited to university-aged individuals in Dutch culture, with an over-representation of females, which may raise concerns regarding the generalisability of the findings. However, our analyses did not show significant gender differences in the main effects, suggesting that the observed associations may be broadly applicable across genders. Still, future research with more representative samples is needed to further confirm whether these patterns generalise to males. Although the generalisability is limited, studying university students remains meaningful. This population face unique challenges, balancing academic responsibilities with the transitions typical of this life stage and the overall pressures of work and finances. These adversities can render them vulnerable to different psychological symptoms, warranting our careful attention and support. Moreover, ER processes are shaped by cultural values and norms. For example, in individualistic cultures like the Netherlands, people may be more inclined to express their emotions openly, whereas in collectivistic cultures, emotional suppression is often emphasised to maintain social harmony (Huwaë & Schaafsma, 2018). Our findings should therefore be interpreted within the cultural background of our sample. Third, future research may include a person-centred and context-dependent approach for the classification of ER repertoire to gain more knowledge on the individual differences in how people regulate their emotions (Chesney & Gordon, 2017; Pugach & Wisco, 2021). Finally, future studies could explore potential mediators and moderators that influence the relationship between ER and psychological symptoms. Possible mediators include maladaptive cognitions and interpersonal support. Moderators may involve cultural differences, which can influence how the adaptiveness of various ER strategies is perceived. Identifying such factors could help clarify how and for whom certain strategies are beneficial or harmful.
Implications
The findings from this study highlight several important implications for therapeutic interventions. First, given that maladaptive ER strategies (e.g., rumination and emotional suppression) are stronger predictors of psychological symptoms, interventions should prioritise reducing these strategies. Techniques such as cognitive-behavioural therapy can help individuals become aware of maladaptive thought patterns related to emotions. By challenging these thoughts, they can learn healthier ways to cope with psychological symptoms. Second, our finding that higher anxiety is associated with a larger maladaptive ER repertoire may complicate treatment, which is often aimed at reducing maladaptive ER (e.g., avoidance). Clinicians may need to identify the different ER strategies that are used, and determine whether these share common features, as well as select which specific ER strategies should be focused on primarily. Third, for individuals with high levels of depressive symptoms, interventions that specifically enhance the regulation of PA, such as taking time to savour enjoyable moments and gratitude journaling, might be particularly beneficial.
Conclusions
In conclusion, our findings indicate that maladaptive ER strategies are broadly associated with higher levels of psychological symptoms, while a larger maladaptive ER repertoire and reduced adaptive ER of PA predict specific symptoms (anxiety and depressive symptoms, respectively). Our findings underscore the importance of using a comprehensive model of ER that integrates different aspects of ER in psychopathological studies, rather than focusing solely on specific ER (e.g., maladaptive ER or regulation of NA only). Future studies may include yet other aspects of ER, such as the temporal dynamics of ER strategies and the impact of cultural factors on ER processes. Getting a more complete picture can be used to refine treatment strategies.
Supplemental Material
Supplemental Material - Adaptive and Maladaptive Regulation of Positive and Negative Affect: Specific Associations With Anxiety, Depression, and Posttraumatic Stress
Supplemental Material for Adaptive and Maladaptive Regulation of Positive and Negative Affect: Specific Associations With Anxiety, Depression, and Posttraumatic Stress by Chusi Xie, Muriel A. Hagenaars, and Paul A. Boelen in Psychological Reports
Footnotes
Author Contributions
Conceptualisation and methodology: Chusi Xie, Muriel A. Hagenaars, Paul A. Boelen. Formal analysis and writing –original draft: Chusi Xie. Investigation, project administration, resources, and supervision: Paul A. Boelen. Writing –review & editing: Chusi Xie, Paul A. Boelen, Muriel A. Hagenaars.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The Ethics Review Committee of the Faculty of Social and Behavioural Sciences at Utrecht University approved our study (approval file: 20-211). Respondents gave informed consent before starting the survey.
Consent to Participate
All participants were provided with detailed study information through an online platform. They were required to review the information and indicate their comprehension before giving informed consent. Participation was entirely voluntary, and participants could withdraw at any time without consequence.
Data Availability Statement
Data are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.