
Abstract
As humanity has been utilizing psychedelic substances for millennia, much knowledge has already been accumulated about the exploratory potential and therapeutic power of the psychedelic-induced nonordinary states of consciousness (NSC). However, we still have only a limited understanding of the process that unfolds in mind and the brain. Only recently have systematic investigations become possible, as the myths about psychedelics are abating and the legal strictures gradually loosening. With the availability of brain imaging techniques, exciting findings have been made about the associated dynamic brain processes. Our prospective observations of spontaneously generated NSC, major mood disorders, have been elucidating another dynamic aspect, the oscillatory brain processes. The findings indicate that the NSC’s propensity is markedly increased at the peaks of the oscillatory brain activity and that the NSC entirely unfolds when the oscillations exceed their normal range. The observation that neurobiological correlates of experientially opposite NSC, melancholy and mania, appear qualitatively the same is compatible with the concept that the experiential content is emerging from nonlocal consciousness. Psychedelic experiences are triggered by the administration of the psychedelic drug. However, they are influenced by nondrug factors and molded, in particular, by the individual’s mental set and the setting of the session. The transformative process can be utilized psychotherapeutically for healing and profound inner restructuring.
Introduction
We know much about the profound experiences they induce, and there is evidence about psychedelics’ therapeutic potential and the involvement of neurotransmitters. Thanks to brain imaging and neuroscience, we have recently learned about some dynamic processes in the brain’s connectivity and the default mode network’s involvement. However, many important questions about the underlying process remain unanswered.
For example, why is every psychedelic experience unique? With other substances, the typical pharmacological reactions are usually quite predictable. Why does the intensity of psychedelic experiences fluctuate from session to session, even if the same dosage is used every time? Why do the peak, breakthrough, and mystical transformative experiences come at a particular time but not at other times, even when the circumstances are similar? These are some examples of questions that cannot be answered from the present knowledge.
As with many complex phenomena, better understanding of the processes might be obtained by creating a composite picture from different perspectives. Experiences induced by the administration of psychedelic substances are an example of nonordinary states of consciousness (NSC) that can also be experienced under different circumstances. For instance, they can be induced physiologically in Holotropic Breathwork (by combining guided relaxation, speeded breathing, and evocative music) or developed spontaneously during major mood disorders. Better understanding of oscillatory brain processes’ contribution to psychedelic experiences could be obtained by observing prospectively recurrent major mood disorders.
First, such observations suggest that the oscillations taking place in the brain at the time of the substance’s ingestion significantly influence the intensity and oscillatory unfolding of the psychedelic experience. Second, the propensity for the NCS is markedly increased at the peaks of the oscillatory brain activity and the NCS fully unfold when the oscillations exceed their ordinary range. Third, the observation that all the investigated neurobiological processes during manic and depressive states are qualitatively indistinguishable is compatible with the interpretation that psychedelic experiences’ experiential content may be emerging from nonlocal consciousness.
Past and Present
Humans have utilized psychedelic substances for millennia. The earlier documents date about 40,000 years ago (S. Grof, 2019). Later paintings, for example with one showing a shaman holding a magic mushroom, are about 5,000 years old (S. Grof, 2019). They may have had a significant effect on human mental and cultural development, particularly in Greece and Egypt. Eleusian mysteries took place in Greece from 1500 BC to 500 AD, and ergot-like substances similar to LSD were used. Some of the most prominent Greek intellectual leaders such as Plato, Aristotle, and Plotinus allegedly took part. During many centuries Greek cultural heritage had a profound influence on the development of European culture.
During the 20th century, the use of many substances with psychotropic effects has been greatly misunderstood, psychedelics in particular. Most of these substances have been judged by society according to how they were abused, not by their most valuable potential for treatment, healing, personal growth, and spiritual advancement. The way these substances were evaluated during the 20th century is one of the particularly bizarre stories in human history (Blevins, 2014).
Rather than recognizing that there is a place for the judicious, careful use of psychedelic substances for their potential healing and transformative effects, they were aggressively suppressed. Hundreds of billions of dollars have been wasted in “the War on Drugs,” yet paradoxically, the abuse actually increased, driven by the black market. During the 1960s the use of psychedelics mushroomed but, for political reasons, it was forced underground and made illegal. The illegal status of psychedelic substances made it impossible to test their therapeutic potential properly.
Many people have an intense and legitimate desire to have access to them to improve their emotional state, enter spiritual domains, or pursue personal growth. We now live during the psychedelic Renaissance. The initial impetus came from the realization that the substances such as ketamine, psilocybin, and marijuana have significant medicinal use. They can be helpful even in situations where mainstream medicine failed. With the involvement of academia, psychedelics are now slowly achieving greater public acceptance and improving public perception. The corresponding legal adjustments are gradually becoming more appropriate.
For the first time in history, mind-expanding substances are becoming available to many, not just for religious and spiritual purposes but also for treatment, healing, and recreational use. Ketamine and psilocybin are also arriving via medical use, and ayahuasca, after years of pressure on politicians, is becoming legitimately available for spiritual purposes.
NSC Induced by Psychedelics
The term psychedelic is a derivative of the Greek words psyche and delein; psyche meaning mind or soul and delein to manifest. It was coined initially by the British psychiatrist Humphry Osmond. In native communities, there is a long history of the use of psychedelics in physical and mental healing and spiritual and religious ceremonies. For example, Native North American practitioners have used mescaline-containing cacti, Mazatec practitioners routinely use psilocybin mushrooms for healing divination, and ayahuasca is widely employed in Brazil and Peru.
Pharmacologically, psychedelic substances can be divided into three major classes: serotonergic agonists, serotonin releasers and NMDA ( N-methyl-D-aspartate) antagonists that are related to glutamate function. Serotonergic psychedelics comprise LSD, psilocybin, mescaline, DMT, and ibogaine. The serotonin receptor 2A agonism is suspected to be the pharmacological trigger of the psychedelic experience (Carhart-Harris, 2019). This explanation is based on the observation that ketanserin, a selective 5-HT2A receptor antagonist, can entirely block the effects of LSD. Serotonin releasers or “empathogens” are phenethylamine derivatives such as MDMA and MDA. NMDA antagonists include ketamine.
5-HT2A receptor agonism is known to be the pharmacological trigger of the “psychedelic experience.” The administration of psychedelics is accompanied by a marked increase of the brain activity and characterized by increased connectivity of neuronal networks and the suppression of activity in the neuronal Default Mode Network (Carhart-Harris, 2019). The observed effects of psychedelic substances depend on the dosage of psychedelic drug and can be described in broad terms such as enhanced emotional activity, augmented mental and psychodynamic processes and perceptual changes.
The pharmacological effect is an essential trigger of the psychedelic experience, but it is the non-drug factors such as set and setting and individual characteristics of the subject and the supporting therapist that play great importance in determining the nature of psychedelic experience. The subject’s life situation at the time of the session, his or her expectations, beliefs, the relevant physiological, emotional, intellectual and spiritual problems are very important. The content of the experience the subject describes has a definite predilection for material that carries a strong emotional charge.
Another important variable is the therapist’s approach to the session, his personality makeup, the therapeutic relationship with the client. It often seems that during the session the participant intensely perceives the emotions of persons present.
The setting of the psychedelic session is also a very significant variable. Different settings activate different elements from the unconscious of the subject. Similarly, various stimuli from the surroundings, particularly the people involved, play an essential modulating role. These influences differ not only from subject to subject but usually also vary considerably from session to session in the same subject. The effects of archetypal forces from the collective unconscious have also been investigated (Tarnas, 2006). It appears that they may be captured by archetypal astrology.
Mind-expanding substances can trigger a variety of mind states: desirable positive from euphoria to deep mystical experiences; undesirable negative from despair and anxiety to the hellish dark night of the soul. But similar NSC can also come without a trigger by a substance, spontaneously, in spiritual emergence or clinical states of depression or mania. Whether they are used intentionally or emerge on their own, they all teach us about how the mind functions.
NSC and Major Mood Disorders
NSC integrate transpersonal, psychosocial and biological factors. They can emerge spontaneously as they do in connection with major mood disorders or they can be induced, for example by psychedelics. To understand better complex phenomena such as NSC, scientists have often found it helpful to integrate observations from several disciplines.
Our observations of oscillatory processes that appear pertinent to psychedelic experiences took place during long-term research of another type of NSC, major mood disorders. Half a century of prospective investigations of major mood disorders contributed to understanding better the dynamic nature of psychedelic states, their timing and variable intensity.
Since 1960, the clinical courses of more than 2,000 patients with major mood disorders have been observed prospectively for periods stretching from 5 years to 50 years. For a significant proportion lifelong data are available. Patients investigated prior to 1970 were treated only during the acute episodes and no effective maintenance medications were available or administered. In such patients, the absence of effective stabilizing treatment was a major advantage for observing spontaneously emerging recurrences unadulterated by medication. Such cohort data cannot be obtained any more.
The most useful source for understanding the process of emerging NSC were observations from bipolar disorders of the classical manic-depressive type. Their major plus was that the patients had clearly demarkated episodes of illness and were returning to full, psychopathology free remissions. These free intervals were also demonstrated by normal profiles on psychological testing (P. Grof et al., 2009).
The classical manic-depressive type of bipolar disorder was originally described by Kraepelin (Kraepelin, 1921) and characterized by recurrent and episodic, fully remitting course, clustering in families and infrequent psychotic symptoms.. In these patients, the changed oscillatory activity takes place in the frontal parts of the brain (Buszaki, 2006) and the patterns appear relatively fixed, nonadaptive. One can extrapolate some observations from patients with classical bipolar type to patients with other types from bipolar spectrum only with caution. The recurrences of the latter patients are on the average less frequent and more reflecting the patients’ psychosocial influences.
Bipolar depressions and manias tend to recur throughout lifetime. The unfolding of recurrences is usually highly individual and appears unpredictable. We tried to analyze and explain the capricious patterns for three decades unsuccessfully. Finally, it became clear (Lat et al., 1981) that the major drivers of recurrence are the oscillatory processes in the brain and that we humans share the oscillatory patterns with other mammals.
NSC and the Brain Oscillations
The human brain is a powerful multioscillating system (Buszaki, 2006). With over 15 billion neurons and trillions of interconnections, the brain functions as a complex system. It maintains stability by oscillating its activity, within an individual range. Oscillatory processes take place at different levels of the brain, from neuron to brain regions and neuronal networks.
The brain both human and animal can be viewed and understood as a complex system of oscillators functioning at all levels from subcellular to various brain components.
When the oscillating waves exceed their usual range, they are associated with a large variety of nonordinary experiences of the mind: spontaneously occurring NSC during mood disorders such as depression and mania; physiologically induced NSC emerging, for example, during Holotropic Breathwork; NSC triggered by psychedelics or other psychotropic drugs, such as antidepressants or stimulants; common spontaneously occurring state bordering on NSC such as falling in love or spiritual emergence.
The experience on psychedelics is unlike taking nonpsychedelic drugs where the effect usually persists until the drug is metabolized and then the effect stops. Psychedelics initiate and for a while maintain such an oscillating experience but even after the substance is fully metabolized, the continuing oscillatory process may continue to bring NSC periodically to awareness. What the subject then experiences on psychedelics is more a process of learning about activating and expanding one’s mind rather than a specific, predictable effect of a drug.
From the observations in mood disorders one can assume that the underlying oscillatory activity is relevant for psychedelic experiences in two ways, influencing in particular the experience’s intensity during acute sessions and timing of new sessions. First of all, acutely, when an individual ingests a psychedelic substance the underlying oscillatory activity gets magnified, desinhibited by the effect of the substance on inhibiting neurotransmitter systems. The experience of nonordinary states usually builds up gradually in waves of increasing intensity, with progressively shorter intervals in-between, until eventually, for a limited time, the individual is fully immersed in the nonordinary experience. Later the experiences usually abate in a decelerating oscillatory pattern. Finally, isolated “flashbacks” may keep emerging for some time, reflecting the gradually lessening oscillating processes. All these phenomena are common expressions of an oscillating process.
Most participants who have taken a psychedelic such as LSD notice that the nonordinary experiences evolve in a fluctuating pattern, in oscillations. Wave after wave, the subject enters nonordinary states of mind. While monitoring the brain activity regularly, we have seen unfolding of other NSC experiences around the oscillatory peaks. The oscillating waves created predispositions for a variety of nonordinary experiences from falling in love, and spiritual emergence, to episodes of depression and mania. Similarly, as these oscillatory processes in the brain are ubiquitous, the oscillatory peaks are times when the mind-expanding substances act particularly strong.
NSC During the Course of Bipolar Disorders
How does this process unfold in bipolar disorders? The pattern of bipolar recurrences over lifetime is individually very variable. For most bipolar patients, the course appears capricious, driven by a complex interactive process. Acute episodes of depression and mania appear to result from the interplay between the brain’s oscillatory processes and neurobiological and psychosocial factors. In patients with severe, classical manic-depressive type of bipolar disorders, the adaptivity of oscillations to external circumstances appears lost, the oscillatory patterns become relatively fixed and therefore predictable, as long as one can identify the underlying oscillatory patterns.
As an example, on Figure 1 oscillatory process is shown of one of our participants measured monthly using dexamethasone suppression test as a proxy for the level of centrencephalic activity. The values are averaged. This is a representative 4-year cut out of a 43-year follow-up. This lady has bipolar disorder, with depressions and manias. At the peaks of the oscillations she is prone to experiencing NSC.
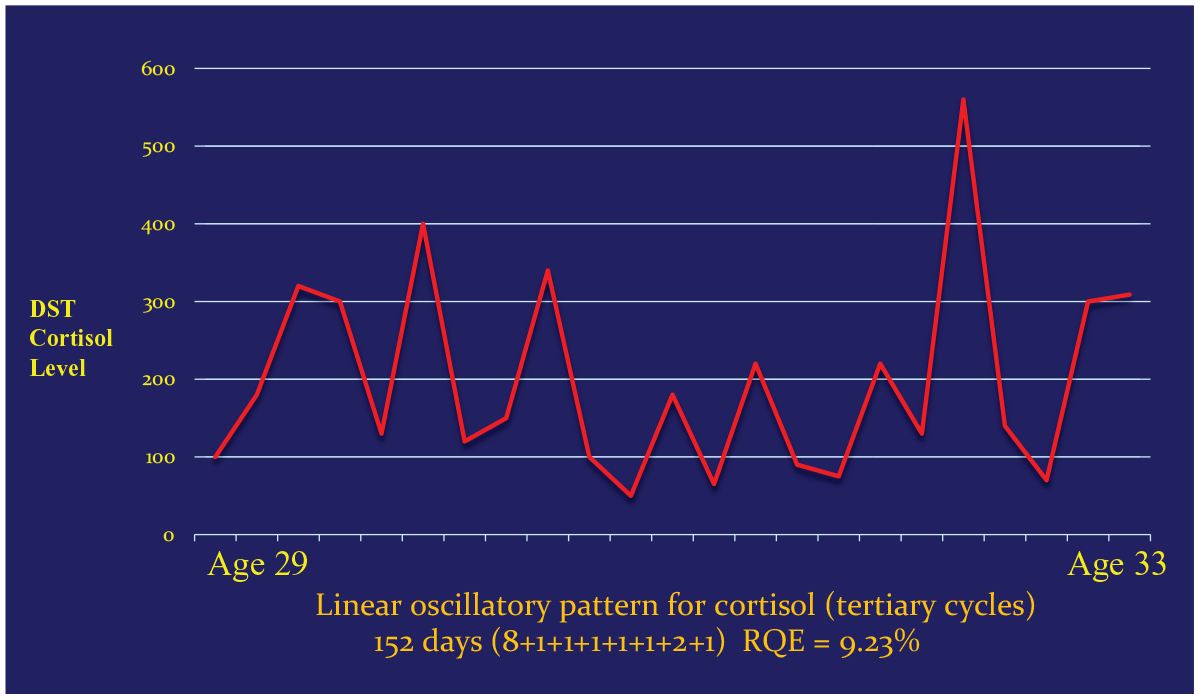
Bipolar disorder, oscillatory activity (4 years example).
Figures 2 and 3 are examples of natural courses of bipolar illness that was treated only during the acute episodes; free of any maintenance treatment in between. The patient on Figure 2 was initially suffering from four episodes of depression before a manic episode took place and bipolar diagnosis was confirmed. The analysis identified an underlying linear course of illness with episodes emerging above the threshold that was gradually rising. The patient on Figure 3 suffered from a severe, classical manic-depressive illness. To a naked eye, the recurrence appeared capricious but there was an underlying exponential pattern, gradually accelerating and then decelerating. The acute episodes of illness corresponded the peaks of the oscillations. Such conversion of all oscillatory peaks into acute episodes takes place only in the most severe illness cases. However, the patient appeared protected when the oscillatory peaks took place during pregnancy. The patient eventually died suddenly at age 52.
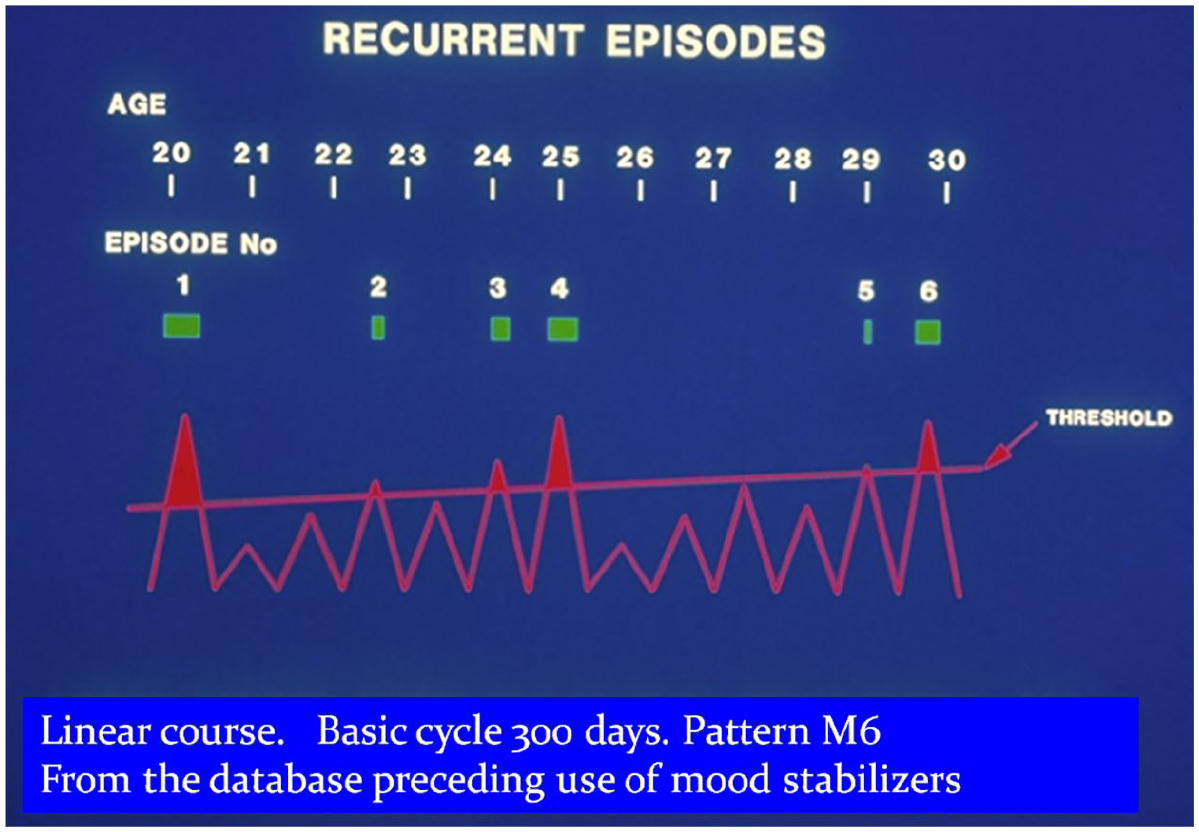
Natural course of bipolar disorder example of linear course.
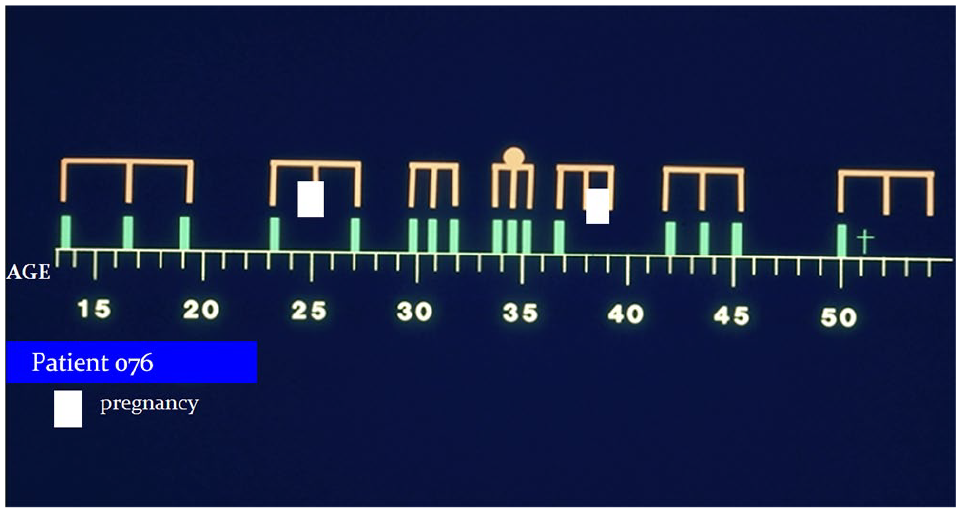
Natural course of bipolar disorder Example of exponential pattern (with secondary cycles).
Our prospective findings indicate that people are highly prone to nonordinary experiences at the peaks of these oscillatory activities. Nonordinary states are initiated when the oscillations exceed the ordinary range. This step outside the range can start naturally in clinical mood disorders, initiated either by a weakness in the oscillation regulatory processes or stressful events. In neurobiological investigations of these patients—including our cohort—weaknesses in serotonergic systems have been identified, even during remissions, and genetic differences, related mainly to G protein transduction (Nunes et al., 2021). A similar disruption can presumably be initiated by the ingestion of psychedelic substances.
The investigations of patients with recurrent mood disorders in our programs contributed, first of all, to the understanding of when the nonordinary experiences likely to take place and how intense they will be. This predictability of recurrence risk in the classical, episodic bipolar disorder makes a safe intermittent lithium treatment possible (Figure 4). When the disorder is severe, all peaks of the oscillations convert into the episodes of illness, as long as the patient does not receive an effective preventative treatment. The recurrence then appears to be driven fully by the oscillatory peaks. In most patients, however, there is an interplay of the underlined oscillatory rhythm and inner and outer psychobiological influences. Only some of the peaks then convert into acute episodes of mania or depression which make seem the overall course of illness looking capricious. Conversely, no recurrences have been seen whenever no oscillatory peaks are present.
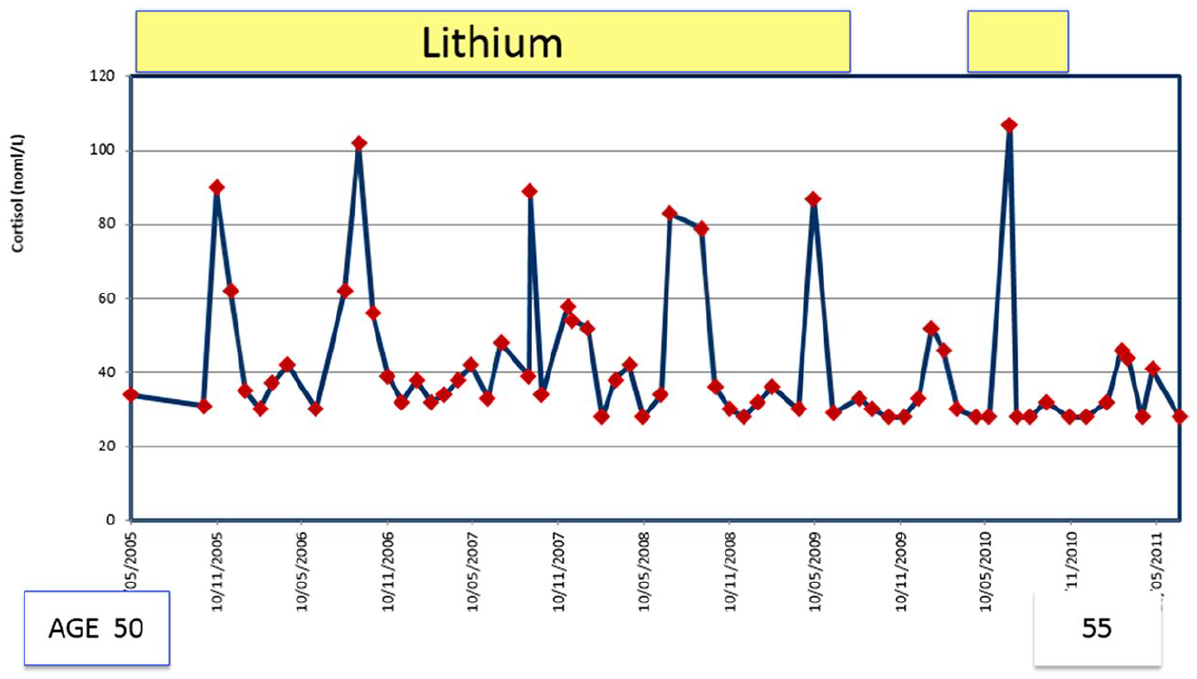
Intermittent lithium treatment.
On the two final figures I offer a simplified schema of how oscillatory processes may maintain balance during ordinary states (Figure 5), and then during NSC resulting from the administration of psychedelics (Figure 6). These schemas reflect our prospective research.
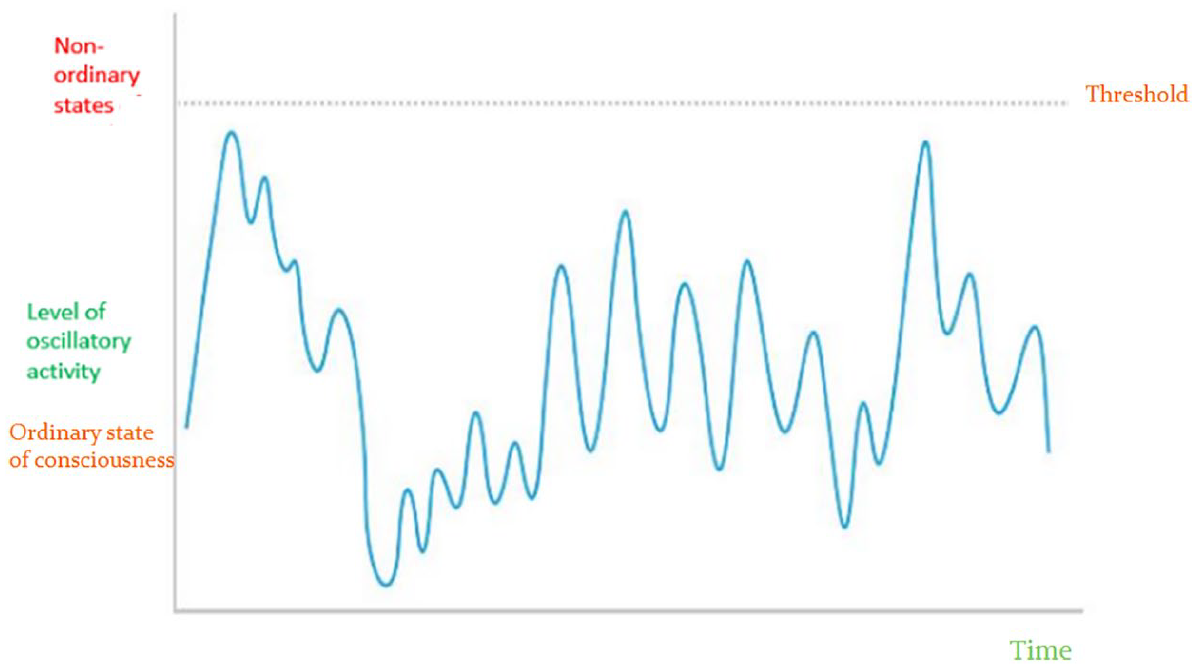
Schema of what happens under ordinary circumstances.
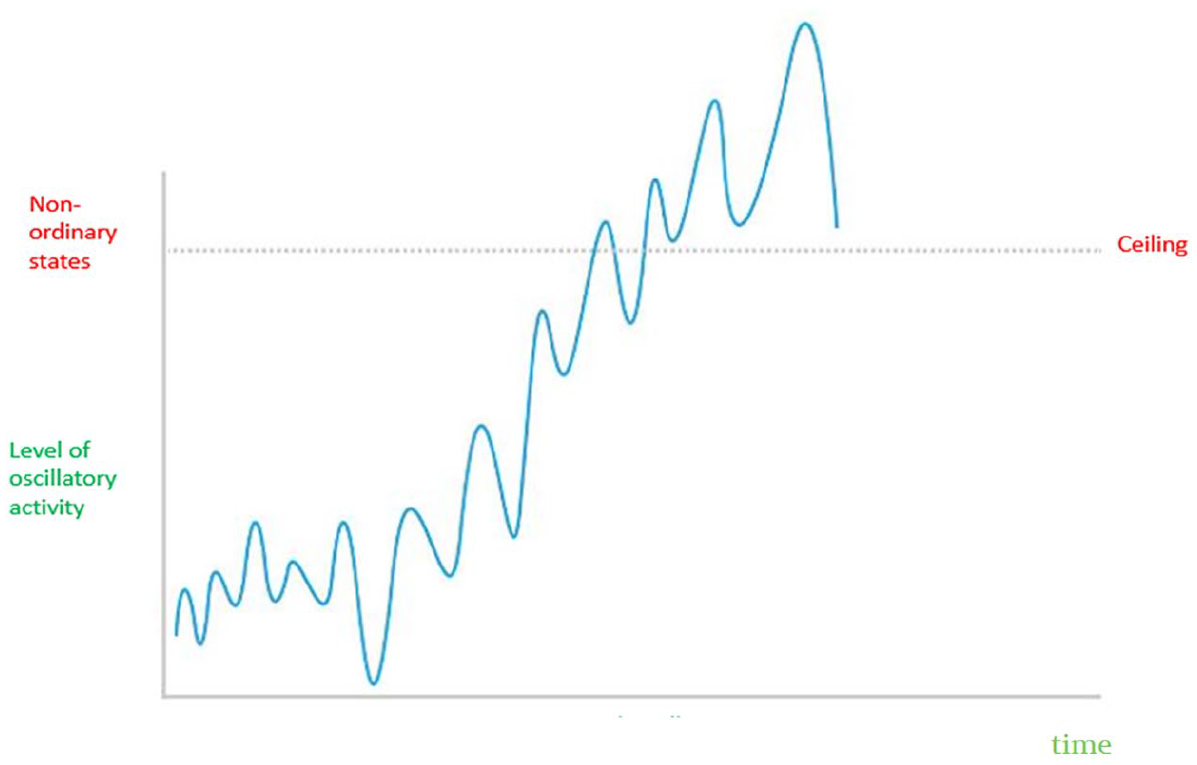
Schema of NCS unfolding.
Most people with the propensity for mood disorders become only mildly or moderately ill, and then only some of the oscillatory peaks convert into the episodes of illness. The development of an episode of NOS then depends on the interplay between the oscillating propensity for such a state and the stressful psychobiological events the person will experience at that particular time. Therefore, it often becomes difficult to correctly predict the timing of future episodes of illness even in the patients suffering from the classical type of bipolar illness.
Physiologically Induced NCS
We have made some useful observations in patients with bipolar disorders during Holotropic Breathwork (S. Grof & Grof, 2010). The safety of this approach was ensured by special arrangements. A trained team was available for 3 days after each session in case some experiential material needed to be fully integrated. We also arranged an access to a hospital bed in my Unit but it was never needed. The sessions took place once a month for more than two years and the group included usually 20 patients (P. Grof, 2013).
In each session only two or three of the group’s participants had deep, intense peak experiences. Usually, these were different individuals every month but they reexperienced breakthroughs later again in a pattern that was suggesting that an oscillatory rhythm was determining their propensity for profound experiences.
Five of the patients from this group participated also in a project that monitored their brain activity once a month. The profound transformative breakthroughs took place at the times when the monthly monitoring indicated a high oscillatory peak. The intensity of the experience during a session appeared distinctly higher when the oscillatory activity of the brain was closer to the ceiling of the range. When working with the group for more 2 years, one could observe how the peak experiences kept shifting from person to person depending on the underlying oscillatory rhythms. These observations were presented at the ITA conference in Manaus, Brazil, 1999.
Oscillations During Intermittent Lithium Treatment
Intermittent lithium treatment has made it possible to test the hypothesis of tight association between NSC and oscillatory peaks experimentally (Figure 4). To classical bipolar disorders lithium offers a unique stabilizing ability. Once stabilized, however, some patients have been requesting to keep lithium treatment to a minimum and for a clinician it is imperative to administer the minimum effective amount in order to limit the adverse effects of long term treatment on the patients’ kidneys. This side-effect becomes particularly worrisome after decades of continuous, uninterrupted maintenance with lithium as it leads to a demonstrable reduction of glomerular filtration and the ability of the kidneys to get rid of waste. Occasionally but fortunately rarely the result has been a kidney failure.
Since Kraepelin, we know that the natural course of the classical bipolar disorders is episodic, with full remissions. Therefore, the illness lends itself to intermittent treatment if we can identify the minimum risk time. Using each patient’s oscillatory patterns, we identified minimum risk periods in 31 such patients and have been treating them intermittently, with success.
Intermittent lithium treatment is a clinical experiment that happens to test prospectively the validity of the relationship between the high risk for NSC around the oscillatory peaks and a low risk in the oscillatory valleys. When a patient requests it and it is possible to identify the underlying oscillatory rhythm of the patient, we have been administering lithium intermittently. These patients have a history of excellent lithium responder and when they are on lithium during the period of risk, they do not experience recurrences. Similarly, when the risk is very low, they remain well without lithium. As long as the patients return to taking lithium as instructed, during the high-risk times, they remain well. On the other hand, if they do not resume taking lithium as they were advised, they become ill again, during the high-risk peak. When they forget to follow the instruction, the recurrence returns as they used to. Fortunately, these patients have been responding reliably to the reinstitution of lithium. Naturally this approach must be considered experimental and suitable only for specialized set ups.
Experiential Content of NSC
In his extensive life-long research, Stan Grof identified three broad categories of experiences that emerge during psychedelic sessions: biographical, perinatal, and transpersonal. The descriptions of the experiences have been extricated from the observations of more than 30,000 sessions; with NSC induced either by a psychedelic or by a Holotropic Breathwork. All these types of experiences are also captured in Stan Grof’s books, for example, The Realms of the human unconscious (S. Grof, 1975), Holotropic mind (S. Grof & Bennett, 1992), and LSD psychotherapy (S. Grof, 1994).
Here I will only offer the briefest summary. The biographical material includes in particular emotionally highly relevant events from the subject’s life. They may stretch from early childhood to the present time and usually share the same emotional quality, as if some program tied together memories with the same emotional attribute. The traditional approach of remembering and reconstructing the repressed biographical events is not helpful enough. To be effective, the therapeutic work with the client must reach deeper than just the biographical dimension. It must release the traumatic material from the level where it is strangulated. Perinatal experiences fall into four different matrices corresponding to the four stages of human birth.
Transpersonal experiences pose a particular challenge to the verbal description because they expand beyond the traditional linear space time boundaries. During the sessions, the participants usual mental abilities may be able to reach outside the usual ranges, for example, to ancestral, fetal, perinatal, or precognitive experiences. The brain obviously cannot not generate any transpersonal information that it did not previously receive through its sensory channels. Thus, transpersonal experiences definitely, and perinatal and prenatal personal experiences possibly, must come from some other, nonlocal source.
Such experiences are presumably based on information the mind obtains intuitively, outside of the person’s sensory channels. Time and space in transpersonal experiences are congruent with the ideas of quantum physics but they cannot be explained within the contemporary mechanistic concept of the human mind.
Stan Grof reported radical discoveries about NSC. His findings propose where the nonordinary experiences come from, what determines the content and how they can be used in a fundamentally new way, for self-exploration and emotional healing. While working prospectively with patients with major mood disorders we have made some observations that appear compatible with his findings and are relevant for the source of the NSC’s content.
One set of our observations came from long-term studies of families of bipolar probands, several of them as large as 110 family members. The initial impetus for a systematic investigation of the bipolar families was the hope to uncover the contributing genetic factors. Mood disorders are clustered densely in the families of classical bipolar disorders. After 35 years of search, this effort recently culminated in the identification of gene set significantly associated with the response of patients to lithium stabilization (Nunes et al., 2021). With the employment of artificial intelligence techniques, Nunes et al. identified the predictive set of genes and also confirmed our earlier finding that the response to lithium stabilization can be successfully forecasted from the comprehensive clinical profile of each patient.
Interesting clinical observations in these large families show that the affected members present findings indicating that affected family members share the same neurobiological reactivities, while at the same time they exhibit a substantial variety of presenting syndromes and meet diagnostic criteria for a variety of Diagnostic and Statistical Manual of Mental Disorders–Fifth edition (DSM 5) disorders. Same type of the course of illness, stabilized on the same medications, failed on the same medications and the emotional problems clustered markedly in those large family. Yet their psychopathological manifestations—the types of their NSC—varied greatly. Each proband had a bipolar disorder but over the years they brought many others family members for assessment and, if indicated, for treatment. Despite the same clinical and neurobiological abnormalities, they had a large variety of emotional problems.
In other words, their experiential contents are not linked to their neurobiological reactivities. These observations were compatible with the interpretation that the content and form of their NSC were arising from somewhere else then their brains.
The second set of finding has come from observing over 25 years the evolution of psychiatric disorders in the offspring of bipolar parents; children and the grandchildren of the probands (Duffy et al., 2019). The psychopathological presentations were dependent on the age at which the symptoms occurred. If the first symptoms emerge in childhood, they are rather nonspecific and include sleep disorders, various manifestations of anxiety disorders and adjustment disorders. The onsets in adolescence usually present with isolated depressive symptoms and syndromes. The full presentations of the classical type bipolar disorder usually take place in early adulthood, with the average around 30 years. So, this set of prospective observations again indicates that while we are dealing with the same underlying and resulting dysfunction, the same individual may live through a variety of experiential content and may receive a number of DSM-5 diagnoses.
The third relevant set are neurobiological observations carried out by us and many others in bipolar disorders. During the past five decades the majority of research in bipolar disorders was neurobiological. However, the focus kept changing as the new neuroscience techniques were developed. In neurochemistry, for example, the emphasis moved from neurotransmitters to neuropeptides, neurohormones and cellular metabolism. Details are captured in the literature. Perhaps the most comprehensive representation of these studies is in two comprehensive, voluminous books by Goodwin and Jamison (1990; Goodwin et al., 2007). Recently, brain imaging was added to favorite techniques. A very large body of observations has confirmed that there are clear, reproducible neurobiological abnormalities when people experience major depressions and manias. They differ significantly from controls and, whenever possible, also from the patients in remission.
For four decades, we were also searching in the brain for a culprit causing depressions and mania and found a large number of biological abnormalities. What is striking however is that the neurobiological changes are qualitatively in the same direction in conditions as experientially different as depressions and manias. The findings in melancholia and mania may be different quantitatively, with mania associated changes being at times more intense. But in both conditions the neurobiological abnormalities are qualitatively the same. The abnormalities during depressions and manias move qualitatively in the same direction regardless of whether the patients are experiencing what they would describe as “Hell” or “Heaven.” This statement only does not apply to those findings that are directly related to the different levels of physical activity in mania and depression.
These findings are again congruent with the interpretation that the brain’s oscillatory activities play a role in the propensity and intensity but not in the content of nonordinary states. What is not yet known is whether the neurobiological changes are directly involved in the generation of dynamic abnormalities of NSC such as increased connectivity, changed oscillatory patterns and suppressed default mode network, or conversely, whether they are perhaps all one of the expressions of the dynamic abnormalities.
It appears that during major mood disorders—that is, these types of NSC—neurobiological abnormalities are not likely to generate the content of the experiences. Contrary to the assumptions underlying the biological theories of mind, the brain does not seem to play a role in the content of the nonordinary experiences. The neurobiological activities influence the timing and intensity of NSC but not the experiential content. These observations resonate with a concept that psychedelic experiences emerge out of rich, complex interplay of dynamic brain processes with nonlocal consciousness fields
Taken together, these findings seem compatible with the concept that the NSC experiences do not come directly from the brain but from another source. Of the available candidates, nonlocal consciousness seems to be the likely generator. The concept of nonlocal consciousness is captured comprehensively in the writings of the internist and surgeon Larry Dossey (2013), the philosopher of science Ervin Laszlo (2016), and investigator Lynne McTaggart (McTaggard, 2011). This model is also reflected in books of Dean Radin (2006) and Charles Tart (2009).
Footnotes
Acknowledgements
I am very grateful to all clients who have participated in the related research over the past five decades
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.