
Abstract
Activins and inhibins, which belong to the TGFβ family, are composed of different combinations of α-, βA-, and βB-subunits, resulting in inhibin A (αβA), inhibin B (αβB), activin A (βAβA), activin B (βBβB), and activin AB (βAβB). They regulate several cell functions, acting as paracrine/autocrine factors. Their actions, which depend on binding to specific receptors, are also modulated by follistatin. Gastroenteropancreatic (GEP) endocrine cells and endocrine tumors (ETs) produce several growth factors, but it is not well known whether they express follistatin and the various inhibin/activin subunits. We studied their expression in 65 GEP ETs using immunohistochemistry (IHC) and in situ hybridization (ISH). The α-subunit and follistatin were not identified in normal GEP endocrine cells and were poorly expressed in ETs. A βA-subunit immunoreactivity (IR) was detected in A-, G-, EC-, and GIP-cells, while βB-chain IR was present only in D-cells. The mRNAs encoding for these molecules were poorly expressed in normal tissues. βA- and βB-subunits were identified in several ETs by both IHC and ISH: βA-subunit mainly in G-cell and A-cell ETs, and βB-subunit in D-cell, A-cell, and EC-cell ETs. Our results demonstrate a differential expression of activin/inhibin subunits among different types of GEP endocrine cells and related tumors, suggesting a role in modulation of biological functions of these normal and neoplastic endocrine cells.
Keywords
I
Activins' actions are mediated by binding to specific receptors with serine/threonine kinase activity (Mathews 1994). Specific receptors with high affinity for inhibin have not been identified (Risbridger et al. 2001), although inhibin has been found to bind to activin type II receptors (Halvorson and DeCherney 1996).
In addition to activin receptors, activin actions are also modulated by follistatin, which inhibits its functions, but with approximately one third of the potency of inhibin (DePaolo et al. 1991). Follistatin, initially isolated from porcine follicular fluid, is a single-chain peptide that does not share any structural relationship with inhibins or activins (Ueno et al. 1987) but shows structural homology with the epidermal growth factor and with a group of enzyme inhibitors of the Kazal family (Risbridger et al. 2001). As demonstrated by Shimonaka et al. (1991), follistatin blocks activin function by binding to the β-subunit. In addition to the ovary, follistatin is expressed in several tissues in both rats and humans. Using Northern analyses, Shimasaki et al. (1989) identified follistatin gene expression in rat brain and kidney. Moreover, immunoreactivity for follistatin was found in several human cells including Leydig cells, pituitary somatotrophs, pancreatic β-cells, thyroid follicular cells, cortical cells of the adrenal glands, neurons of the brain cortex, and monocytoid cells of the bone marrow (Wada et al. 1996). The biological meaning of this distribution is not yet clear, but it has been suggested that in these sites follistatin can modulate actions of inhibins and activins (Wada et al. 1996).
Gastrointestinal and pancreatic endocrine (GEP) cells belong to the diffuse neuroendocrine system and are characterized by production of several hormones or amines, whose expression allows their identification. In recent years, some investigations have demonstrated that normal endocrine cells of the digestive system, in addition to hormones, express growth factors and growth factor receptors (Bordi et al. 1994; Kuroda et al. 1995; La Rosa et al. 1998, 2001, 2003) whose biological functions are yet not clear. In addition, among various growth factors, activin A has been recently detected by IHC in specific human endocrine cell types of the gut and pancreas (La Rosa et al. 1999), and studies in rat pancreas have demonstrated the expression of the βA-subunit and activin A in some pancreatic islet cells (Yasuda et al. 1993; Ogawa et al. 1993, 1995; Furukawa et al. 1995). Although a βB-subunit immunoreactivity has been described by Ogawa et al. (1995) in endocrine cells of rat pancreatic islets, to the best of our knowledge the βB-subunit expression in human adult gut and pancreatic endocrine cells has never been reported. Follistatin expression has only been investigated in pancreatic islets (Ogawa et al. 1993, 1995; Wada et al. 1996) of rat and humans, but data concerning its localization in human gut endocrine cells are lacking.
Endocrine tumors (ETs) of the GEP system are composed of tumor cells whose morphofunctional profile reproduces in part that of normal GEP endocrine cells from which they derive (Solcia et al. 1999). Like normal endocrine cells, GEP ETs have been found to produce several growth factors in addition to their hormone secretion (Bordi et al. 1998). We have recently demonstrated that whereas the α-subunit of inhibin is expressed in rare cells of a small number of GEP ETs, the βA-subunit is expressed by several GEP ETs, including gastrinomas, insulinomas, pancreatic A-cell tumors, and intestinal EC-cell neoplasms (La Rosa et al. 1999). However, as far as we know, the expression of the βB-subunit and follistatin in GEP ETs has not been reported in the English literature. The present study was designed to localize the three subunits of inhibin/activin and follistatin in normal GEP endocrine cells and GEP ETs using IHC and ISH.
Materials and Methods
Tissues
Samples of normal pancreas and gut mucosa and of 65 well-characterized GEP ETs were collected at surgery. The main clinicopathological data of patients are summarized in Table 1. Tissues were fixed in buffered formalin (formaldehyde 4% and acetate buffer 0.05 M) for 24 hr and embedded in paraffin. Sections 5 μm thick were stained with hematoxylin-eosin (H&E), alcian blue-periodic acid Schiff (AB-PAS), and Grimelius silver stain for the histopathological examination.
Antibodies
The anti-α-subunit antibody (Serotec; Oxford, UK) was a mouse monoclonal antibody (MAb) directed against a synthetic protein corresponding to the 1–32 peptide sequence of the α-subunit of 32-kD human inhibin. The mouse MAb directed against the βA-subunit (Serotec) recognized a synthetic peptide corresponding to the 82–114 protein sequence of the βA-subunit of 32-kD human inhibin A and activin A. The anti-βB-subunit mouse MAb (Serotec) was directed against a synthetic peptide corresponding to residues 82–114 of the inhibin βB-subunit. The anti-follistatin antibody was a rabbit polyclonal antiserum recognizing the 27–43 amino acid sequence of rat follistatin (follistatin peptide FP2 of the National Hormone and Pituitary Program; Bethesda, MD), which is identical to the human amino acid sequence in this region. Normal endocrine cells and endocrine tumors were identified and classified using the antibodies and antisera listed in Table 2.
Riboprobes
The sequence of human ovarian α-subunit of inhibin (Gen-Bank accession number M13144) was used to design the primers to detect the α-subunit mRNA in tissue sections: forward primer, 5′-TGTTCCGGCCATCCCAGCAT-3′ (298–317 of sequence); reverse primer, 5′-ACTGGGTGGTCTG-GTCCGA-3′ (632–614 of the sequence). These amplified a 335-bp segment. The sequence of human inhibin/activin βA-subunit (GenBank accession number BC007858) was used to design the primers for βA-subunit detection: forward primer, 5′-GTTGGCAAGTTGCTGGATT-3′ (256–274 of the sequence); reverse primer, 5′-CTCCATAAGTTCAT-TCATTTC-3′ (580–560 of the sequence). These amplified a 325-bp segment of the gene. The sequences of human inhibin/activin βB-subunit gene for exon 1 (GenBank accession number M31668) and for exon 2 (GenBank accession number M31669) were used to design the primers for βB-subunit detection: forward primer, 5′-GAAATCATCAGCT-TCGCCGAG-3′ (1190–1210 of the exon 1 sequence); reverse primer, 5′-CGAATGCGGTGCCTGCTGTC-3′ (500–481 of the exon 2 sequence). These were used to amplify a 574-bp segment of the gene.
Main clinicopathological data and activin/inhibin subunit expression in digestive endocrine tumors a
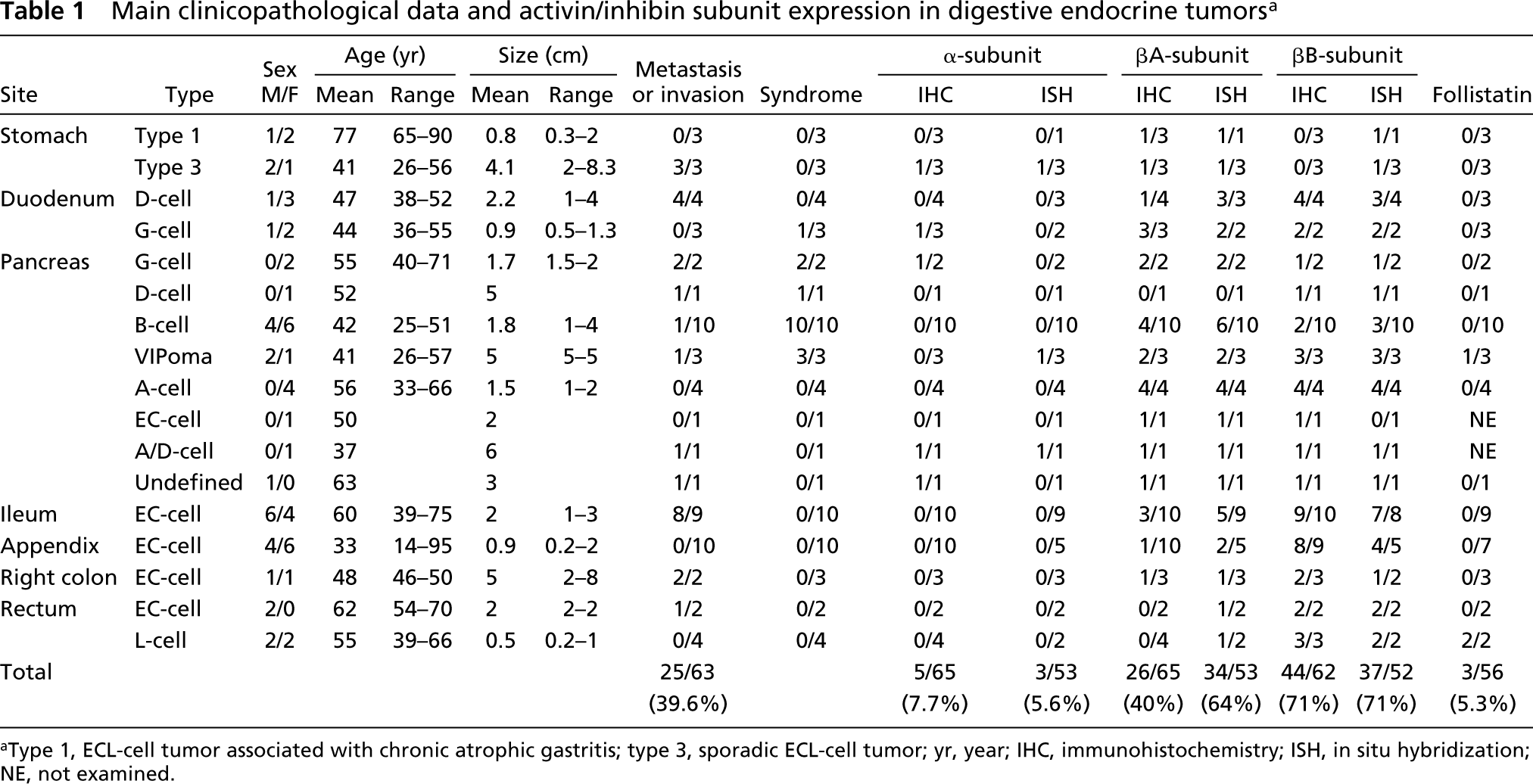
aType 1, ECL-cell tumor associated with chronic atrophic gastritis; type 3, sporadic ECL-cell tumor; yr, year; IHC, immunohistochemistry; ISH, in situ hybridization; NE, not examined.
Antibodies and antisera employed
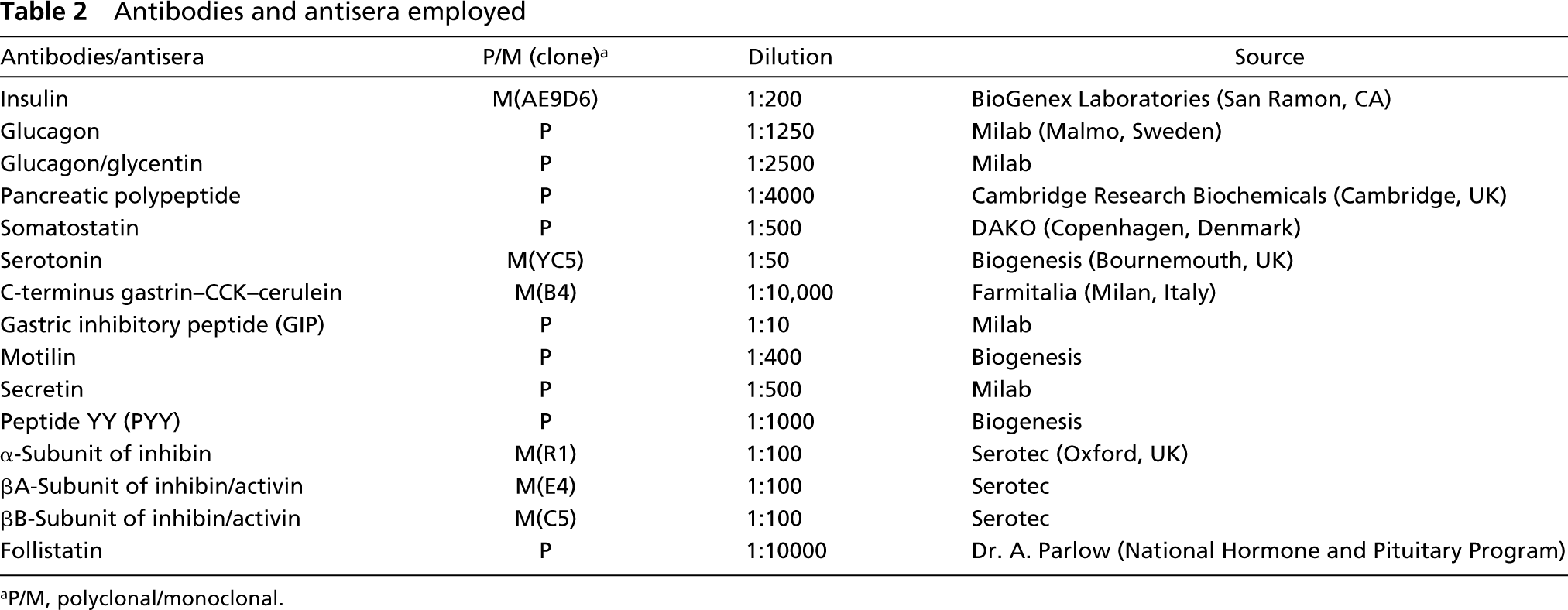
aP/M, polyclonal/monoclonal.
For α- and βB-subunits, the Stratagene ProSTAR First-Strand RT-PCR Kit (Stratagene: La Jolla, CA) was used to make cDNA using 5 μg of total RNA from normal human thyroid. Segments were PCR-amplified in a Perkin-Elmer 9600 thermocycler by the following parameters: 94C for 5 min, then 35 cycles of 94C for 1 min, 62C for 1 min, 72C for 2 min using 5μl cDNA, 1 pM each primer, 1.25 U Taq polymerase, and 25 mM MgCl2 in a 50-μl total reaction using the RT-PCR kit. For βA-subunit, the Stratagene ProSTAR First-Strand PCR Kit was used to generate cDNA from 5 μg of total RNA extracted from a normal human pituitary. The segment was amplified in a Perkin-Elmer 9600 thermocycler by the following parameters: 94C for 5 min, then 30 cycles of 94C for 1 min, 42C for 1 min, 72C for 2 min using 5 μl of the cDNA, 50 ng of each primer, 1 μl dNTP mix (2.5 mM each dNTP), 5 μl cloned Pfu buffer and 1.25 U of cloned 10X Pfu Turbo DNA polymerase (Stratagene) in a 50-μl reaction. The PCR products were ligated into the pGEM-T Easy vector (Promega; Madison, WI). Each ligation was done using 0.5–2.5μl of each PCR reaction, 5 μl 5X Rapid Ligation Buffer, 3 U T4 DNA Ligase in a 10-μl reaction volume for 1 hr at ambient temperature. Three μl of each ligation was used to transform Top 10 Ultracompetent E. coli (Invitrogen; Carlsbad, CA). Plasmids were sequenced by the Mayo Clinic Molecular Biology Core facility using the pUC/M13 primer Forward (Promega). The riboprobes were digoxigenin 11-UTP labeled using the labeling kit purchased from Boehringer Mannheim (Mannheim, Germany). The transcription reaction produces either antisense or sense RNA probe, depending on the orientation of the clonal insert.
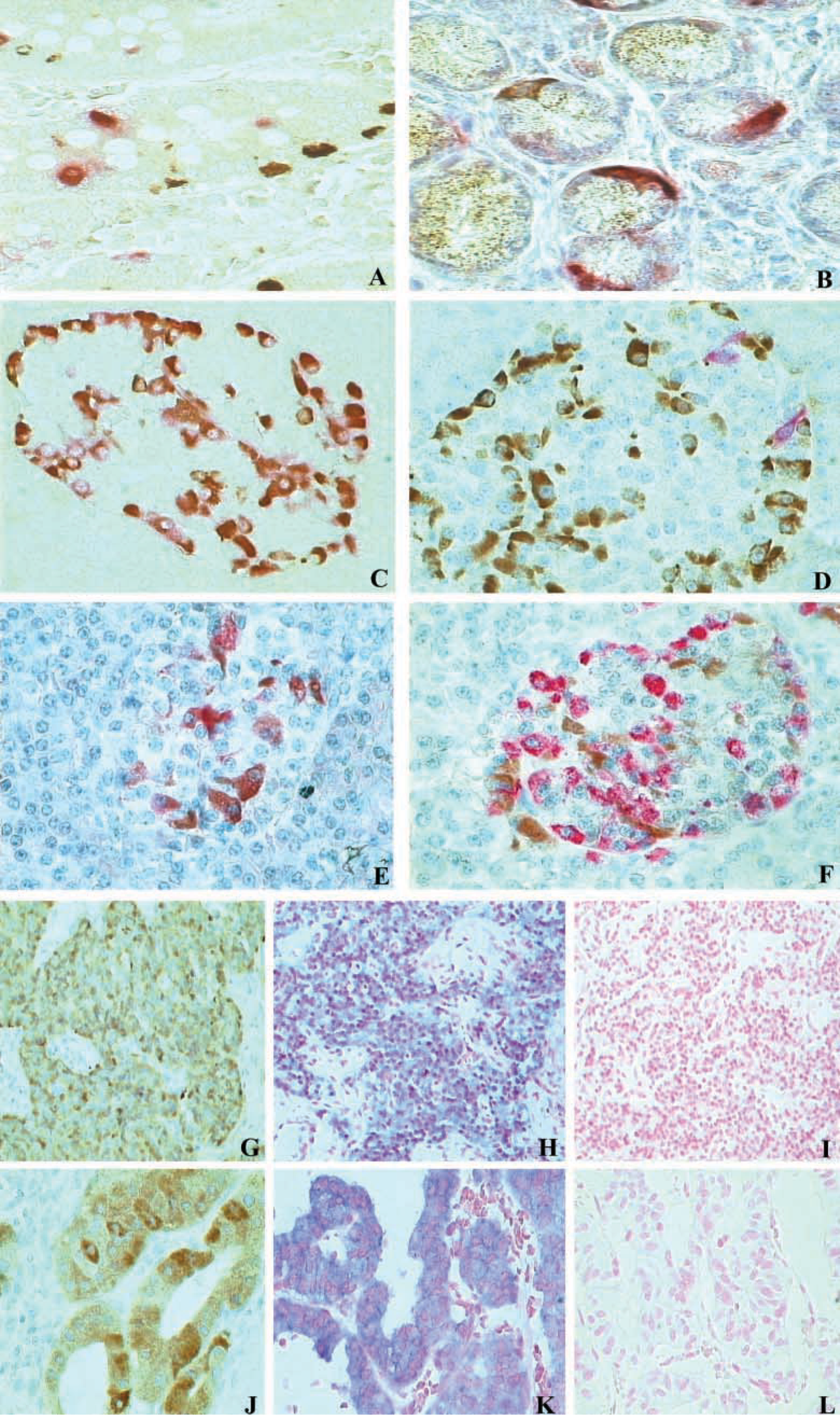
Double-label immunostaining demonstrates that the βA-subunit (red) is co-localized with gastrin (
Immunohistochemistry
For IHC staining, 3-μm-thick sections were mounted on poly-
In situ hybridization
ISH was performed as previously reported (Lloyd et al. 2001). Briefly, sections were deparaffinized and placed in a 10 mM citrate buffer, pH 6, in a microwave oven at 800 W power and then treated with proteinase K (Boehringer). After incubation in 0.2 N HCl in 0.1 M triethanolamine with freshly made acetic anhydride and in prehybridization buffer, hybridization was done at 50C for 16 hr. After RNase treatment and washing in sodium citrate and sodium chloride buffer, sections were reacted with anti-digoxigenin antibody linked to alkaline phosphatase (Roche; Penzberg, Germany), followed by incubation with nitroblue tetrazolium (NBT) and 5-bromo-4-chloro-3 indolylphosphate (BCIP). Specificity controls consisted of the omission of the antisense riboprobe, use of a sense riboprobe, and testing the antisense in tissues known to express the mRNA.
Results
Normal Tissues
Endocrine cells dispersed along the gut or present in the pancreatic islets were negative for both α-subunit and follistatin.
Intense cytoplasmic immunoreactivity for the βA-subunit was found in several endocrine cells of the gastric and duodenal mucosa and in many cells of pancreatic islets. Conversely, βA-subunit immunoreactivity was lacking in endocrine cells located in the other tracts of the gut. Double-label immunostaining demonstrated that, in antroduodenal mucosa, βA-sub-unit-immunoreactive (IR) cells corresponded to G- (Figure 1A), EC- (Figure 1B), and GIP-cells (Table 3). Owing to the rarity of βA-subunit-IR cells in the oxyntic mucosa of the stomach, it was not possible to establish which type of endocrine cell was expressing the βA-subunit. In the pancreas, βA-subunit-IR was found in cells mainly located at the periphery of the islets and also in several endocrine cells dispersed through the exocrine parenchyma. Double-label immunostaining demonstrated that βA-subunit-IR cells corresponded mainly to glucagon-producing A-cells (Figures 1C and 1D).
Immunoreactivity for the βB-subunit was mainly restricted to endocrine cells of the antral and duodenal mucosa as well as in those of pancreatic islets, but it was lacking in the other portions of the gut, with the exception of rare positive cells in the fundic and rectal mucosa (Table 3). As demonstrated by co-localization studies, βB-subunit-IR, which was intense, cytoplasmic, and granular, was localized in somatostatin-producing D-cells, both in the antroduodenal mucosa and in the pancreatic islets (Figures 1E and 1F).
Normal islet cells and normal gut endocrine cells were mostly negative for α-, βA-, and βB mRNA detection. Only in rare endocrine cells was weak positive ISH staining observed.
Immunohistochemical localization of α-, βA-, βB-subunits of inhibin/activin and follistatin in normal endocrine cells of gut and pancreas a
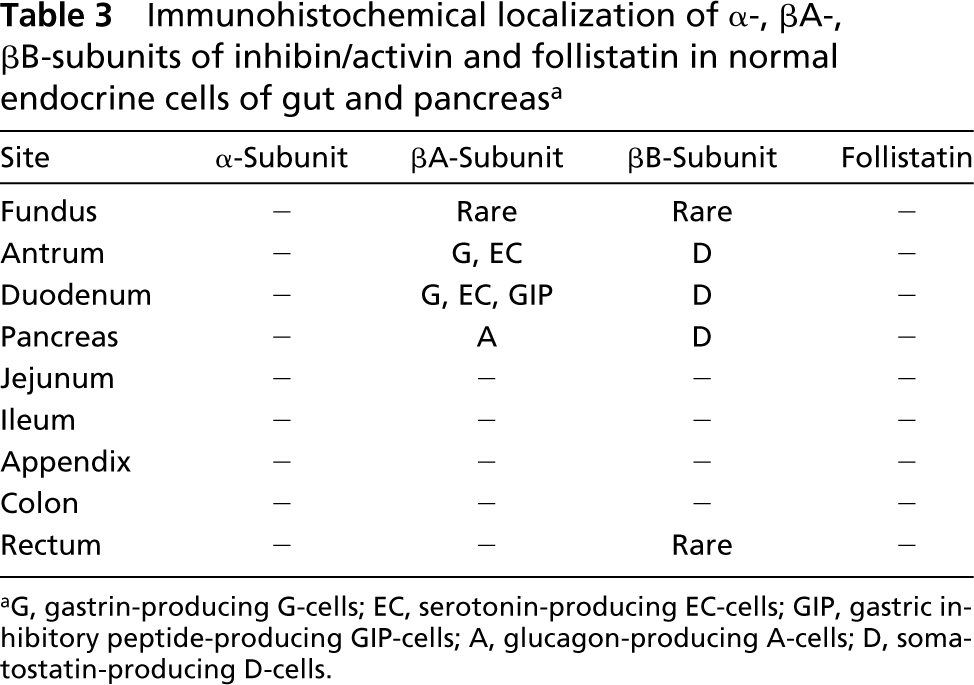
aG, gastrin-producing G-cells; EC, serotonin-producing EC-cells; GIP, gastric inhibitory peptide-producing GIP-cells; A, glucagon-producing A-cells; D, somatostatin-producing D-cells.
Endocrine Tumors
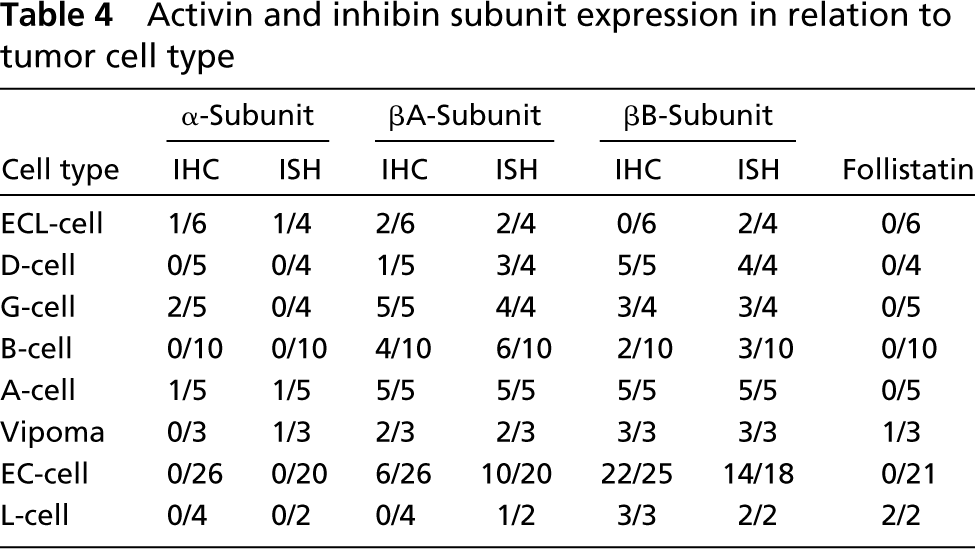
The clinicopathological profile of the 65 ETs investigated is reported in Table 1. Clinically, the majority (48/65) of tumors were nonfunctioning. The functioning neoplasms were represented by three gastrinomas (one duodenal and two pancreatic), one pancreatic somatostatinoma, 10 insulinomas, and three VIPomas, each of them associated with specific symptoms of the related syndromes. With the exception of three cases associated with the MEN 1 syndrome, all tumors were sporadic. Table 4 summarizes the expression of the three subunits of inhibin/activin and of follistatin in relation to the tumor type, independently from the site of origin.
α-Subunit immunoreactivity was found in a few ETs (5/65, 7.7%), and in these tumors the mean percentage of positive cells was 10% (range 3–30%). α-Subunit mRNA was detected by ISH in 3/53 (5.6%) cases.
Immunoreactivity for the βA-subunit was found in 26/65 (40%) ETs and was mainly restricted to G-cell and A-cell tumors (Figure 1G). However, some tumors of a different type, including four B-cell, six EC-cell neoplasms, and two VIPomas showed immunoreactivity for the βA-subunit, although this was less intense and expressed in fewer tumor cells than in G-cell and A-cell tumors. By ISH, 34/53 (64%) tumors were positive for mRNA detection and, as for IHC, A-cell (Figure 1H) and G-cell neoplasms presented stronger staining in more numerous cells than the other tumor types.
βB-Subunit immunoreactivity was observed in 44/62 (71%) ETs, including all D-cell, A-cell, L-cell neoplasms, and VIPomas, and in the majority (22/25 cases, 88%) of EC-cell tumors. In addition, other types of ETs, including two insulinomas, one tumor of undefined cell type, and three G-cell tumors presented some βB-subunit-IR cells; 37/52 (71%) tumors were positive at ISH investigation and, as shown in Table 4, there is a good agreement between ISH and IHC results (Figures 1J and 1K).
Follistatin immunoreactivity was found in only 3/56 (5.3%) ETs, represented by two rectal L-cell tumors and one pancreatic VIPoma. The mean percentage of positive cells in L-cell neoplasms was 15%, but in the VIPoma only rare cells were positive.
Activin and inhibin subunit expression in relation to tumor cell type
Discussion
In the present study we have investigated the expression of α-, βA-, and βB-subunits of inhibin/activin in normal endocrine cells and in a series of well-characterized ETs of the digestive system. In addition, we studied the IHC expression of follistatin in the same tissues. Considering the molecular homo/heterodimeric structure of inhibins and activins, comprehensive study of the expression of the three subunits composing these proteins has enabled us to identify their exact distribution in both normal and neoplastic GEP endocrine cells. The co-expression of α-subunit with βA- or βB-subunit was indicative for the presence of inhibin A or inhibin B, respectively. On the other hand, the unique immunoreactivity for βA- or βB-subunits was consistent with the presence of activin A or activin B. Finally, when βA- and βB-subunits were detected within the same cells, the presence of activin AB as well as of activin A and activin B was considered. These data, combined with the functional characterization of normal and neoplastic endocrine cells based on the detection of their hormonal production, provided a survey of the distribution of various forms of activins and inhibins in different endocrine cell types and in various ETs.
Our results indicate that follistatin is not expressed in normal GEP endocrine cells. In addition, because we did not identify any α-subunit immunoreactivity in any endocrine cell of the gut and pancreas, we suggest that inhibins, including inhibin A (α-βA) and inhibin
B (α-βB), are not expressed in these cells. On the other hand, our results have shown that activin A (βA-βA) and activin B (βB-βB) are differently expressed in GEP endocrine cells. In particular, activin A is expressed by G-, EC-, and GIP-cells of the antral and duodenal mucosa and in A-cells of the pancreatic islets, while activin B expression is restricted to duodenal and pancreatic somatostatin-producing D-cells.
Our findings concerning the βA-subunit distribution are in agreement with several recent IHC studies in which tissues of adult humans and of adult or fetal rats were investigated. We have identified activin A in gut G-, EC-, and GIP-cells, confirming our previous results (La Rosa et al. 1999). The expression of activin A in pancreatic A-cells fits well with findings reported in previous studies (Ogawa et al. 1993, 1995; Yasuda et al. 1993; Furukawa et al. 1995; La Rosa et al. 1999), although Wada et al. (1996), in their IHC investigation, observed activin A immunoreactivity only in insulin-producing B-cells of the pancreas. These different results may be explained by considering the different antibodies employed. In addition, one must consider that activin A and glucagon have been demonstrated to be pooled within the same granules (Verspohl et al. 1993), suggesting that they may have a synergistic action in the control of glucose metabolism.
The βB-subunit of inhibin/activin has been previously localized in A- and B-cells of rat pancreatic islets (Ogawa et al. 1995), but data concerning its distribution in human gut and pancreatic endocrine cells are lacking. Our study has demonstrated, for the first time, that duodenal and pancreatic somatostatin-producing D-cells are strongly immunoreactive for the βB-subunit, suggesting that this cell type expresses activin B. This finding, which is different from that observed by Ogawa et al. (1995) in rat pancreatic tissues, may be due to the difference in the species investigated or in the antibodies employed.
Our findings regarding the localization of follistatin in pancreatic endocrine cells are unlike those reported in previous studies (Ogawa et al. 1993, 1995; Wada et al. 1996). In fact, we did not observe any follistatin immunoreactivity in pancreatic endocrine cells and in gut endocrine cells. On the contrary, follistatin immunoreactivity has been reported in both human (Wada et al. 1996) and rat (Ogawa et al. 1993) pancreatic B-cells. Ogawa et al. (1995) demonstrated that rat pancreatic B-cells were positive for follistatin when tested with antibodies detecting the short form of the molecule, whereas they were negative when tested with the antibodies detecting the long form. Using a rabbit polyclonal antibody raised against a recombinant follistatin, Wada et al. (1996) observed follistatin immunoreactivity in human pancreatic B-cells. In our study, we employed an antiserum against the 27–43 amino acid sequence of follistatin, which is present in both the short and long form of the molecule. The specificity of our antiserum was demonstrated by the staining in normal tissue, including pituitary and ovary, and negative staining of the same tissues after incubation of the antiserum with both specific sequence peptide and recombinant follistatin, which abolished the positivity. The discrepancies between our results and those above described (Ogawa et al. 1993, 1995; Wada et al. 1996) may be mainly due to the different antibodies employed. The absence of immunoreactivity for follistatin that we observed in gut endocrine cells cannot be compared with other findings because of the lack of previous studies on this subject.
ISH investigation did not reveal significant mRNA expression in normal GEP endocrine cells, in contrast to IHC, which demonstrated, as discussed above, a specific distribution of the different subunits among various normal endocrine cells. The lack of mRNA in normal tissues was not due to a general mRNA degradation, because other probes that we used in our lab, such as proinsulin or myosin XVA probes (data not shown), gave strong staining in the same tissues (La Rosa et al. 2002). In addition, several peritumoral normal tissues that we investigated were negative although the adjacent tumor cells showed different degrees of ISH staining. Using Northern blotting analysis, Kleeff et al. (1998) have recently found overexpression of mRNA encoding various subunits of inhibin and activin in pancreatic cancers in contrast with adjacent normal pancreatic tissues. In this study, very low levels of βA-, βB-, and α-subunit mRNA were found in normal pancreas, in contrast with the high expression in pancreatic cancers. Studies on porcine tissues have also demonstrated that activin A and B mRNAs are not expressed at significant levels in gut mucosa (Schneider et al. 2000). The very low level of mRNA found in normal tissues reported above is well in agreement with our data. Conversely, the IHC expression of various subunits is well demonstrated by our and other investigations (Ogawa et al. 1993, 1995; Yasuda et al. 1993; Furukawa et al. 1995; La Rosa et al. 1999). Discrepancies in the localization patterns of mRNA and corresponding proteins have also been noted with members of the TGFβ superfamily, including inhibins and activins in embryonic (Akhurst et al. 1990; Jakowlew et al. 1994) and ovarian (Benhamed et al. 1993; Roberts et al. 1993, 1994) tissues. Such discrepancies may be explained by several mechanisms: (a) the level of mRNAs may be below the detection limit of the assay procedures; (b) synthesized proteins have been stored in cells for a long time and no newly mRNA synthesis is required; or (c) in tumor cells mRNA may be overexpressed because of the high metabolic activity of neoplastic cells.
The biological meaning of the different distribution of activin proteins, either activin A or activin B, and the lack of inhibins and follistatin expression, which we observed in GEP endocrine cells, is yet not clear. The localization of activin A in glucagon-producing A-cells and gastric inhibitory peptide (GIP)-producing cells, which are well-known regulators of glucose metabolism (Duprè et al. 1973; Unger and Orci 1976; Elhai et al. 1979; Creutzfeldt and Ebert 1985) suggests that this factor may participate with glucagon and GIP in the same physiological mechanism. In this context, it is worth noting that activin A has been demonstrated to induce insulin secretion from both rat (Totsuka et al. 1988) and human pancreatic islets (Florio et al. 2000). In addition, transgenic mice with mutation of the activin receptor have a lower survival rate with smaller islet area and impaired glucose tolerance (Yamaoka et al. 1998). These data suggest a role for activin in modulating islet function as a local autocrine and/or paracrine factor.
The biological role of activin B expression is less clear. Because we observed its expression in somatostatin-producing D-cells, we can hypothesize that activin B may be involved, together with somatostatin, in the regulation of some endocrine cell functions, although its role remains to be elucidated.
On the basis of our negative findings, follistatin and inhibins do not appear to be involved in the regulation of endocrine cells of the gut and pancreas. Interestingly, both these peptides have inhibitory effects, through different molecular mechanisms, on activin functions. Inhibins antagonize activin actions, having an opposite biological function on the same target cells, while follistatin inhibits activin actions by directly binding to it. It can be hypothesized that, in GEP endocrine cells, activin actions may be modulated by other systems, possibly through a specific receptor or heparan sulfate proteoglycans, which are also involved in the modulation of activin activities (Halvorson and DeCherney 1996).
In addition to normal tissues, we have investigated a large series (65 cases) of well-characterized ETs. The distribution of various subunits of inhibin/activin in GEP ETs partly reflects that observed in normal tissues. Activin A was detected in all G-cell and A-cell neoplasms and activin B in all D-cell tumors, reflecting the distribution of these factors in the relative normal endocrine cells. Activin B expression (βB-subunit immunoreactivity) was unexpectedly detected in pancreatic A-cell, rectal L-cell, and in the majority (22/25, 88%) of the intestinal EC-cell tumors. Considering that the relative normal cells did not show any βB-chain expression, this discrepancy between normal and neoplastic cells may represent a “de novo” expression of activin B in tumor cells or, more likely, an overexpression of this peptide in tumors from low level, poorly detectable, present in normal cells.
We have not found any relationship between activin expression and malignancy, suggesting that it does not have a role in ET aggressiveness. This is in contrast to the data recently reported by Salmenkivi et al. (2001), who observed an inverse relationship between activin B expression and malignancy in adrenal pheochromocytomas.
In conclusion, in this study we have demonstrated that activins are specifically expressed by various endocrine cells of the GEP system, suggesting that they may participate in the modulation of physiological functions of these cells. In addition, ETs tend to express the same type of activin identified in their putative cells of origin. These findings suggest that activins may have a role in the biology and pathogenesis of ETs of the GEP system.
Footnotes
Acknowledgements
Supported in part by a grant from the University of Insubria, Varese (Italy).
We thank Jill Bayliss and Dr Long Jin for technical assistance and Dr A.F. Parlow (NIDDK's National Hormone & Pituitary Program) for the anti-follistatin antibody.