
Abstract
Immunohistochemical (IHC) examination is frequently necessary for a histological differential diagnosis of tumors. To simplify IHC examination, we have developed a novel device called a “multiplex-immunostain chip (MI chip).” The chip is a panel of antibodies contained in a silicon rubber plate that consists of 50 2-mm-diameter wells. A tissue section slide is placed on the plate and is fastened tightly with a specially designed clamp. The plate with the slide is then turned upside down, which applies the antibodies to the section. This technology allows IHC staining of a tissue section with 50 different antibodies in a single experiment, reducing the time, effort, and expense of IHC analysis. In addition, it enables pathologists to compare expression of multiple antigens on a tissue section simply by changing microscopic fields on a single slide. These features are unique to the MI chip technology. The method requires no expensive instruments. This device can be used in various applications in differential diagnosis of tumors and the field of cell biology.
Keywords
E
Tissue microarray (Kononen et al. 1998) and cell array (Oode et al. 2000) systems, which are high-throughput technologies, allow comprehensive assessment of expression of a single antigen across many tissues and cells, respectively, in a single experiment. However, pathologists want to survey expression of multiple antigens for a tumor at one time rather than the expression status of a single antigen for many tumors. Here, we report development of a novel high-throughput technology that allows IHC examination of a tissue section with 50 different antibodies in a single experiment.
Materials and Methods
Multiplex-immunostain Chip (MI chip)
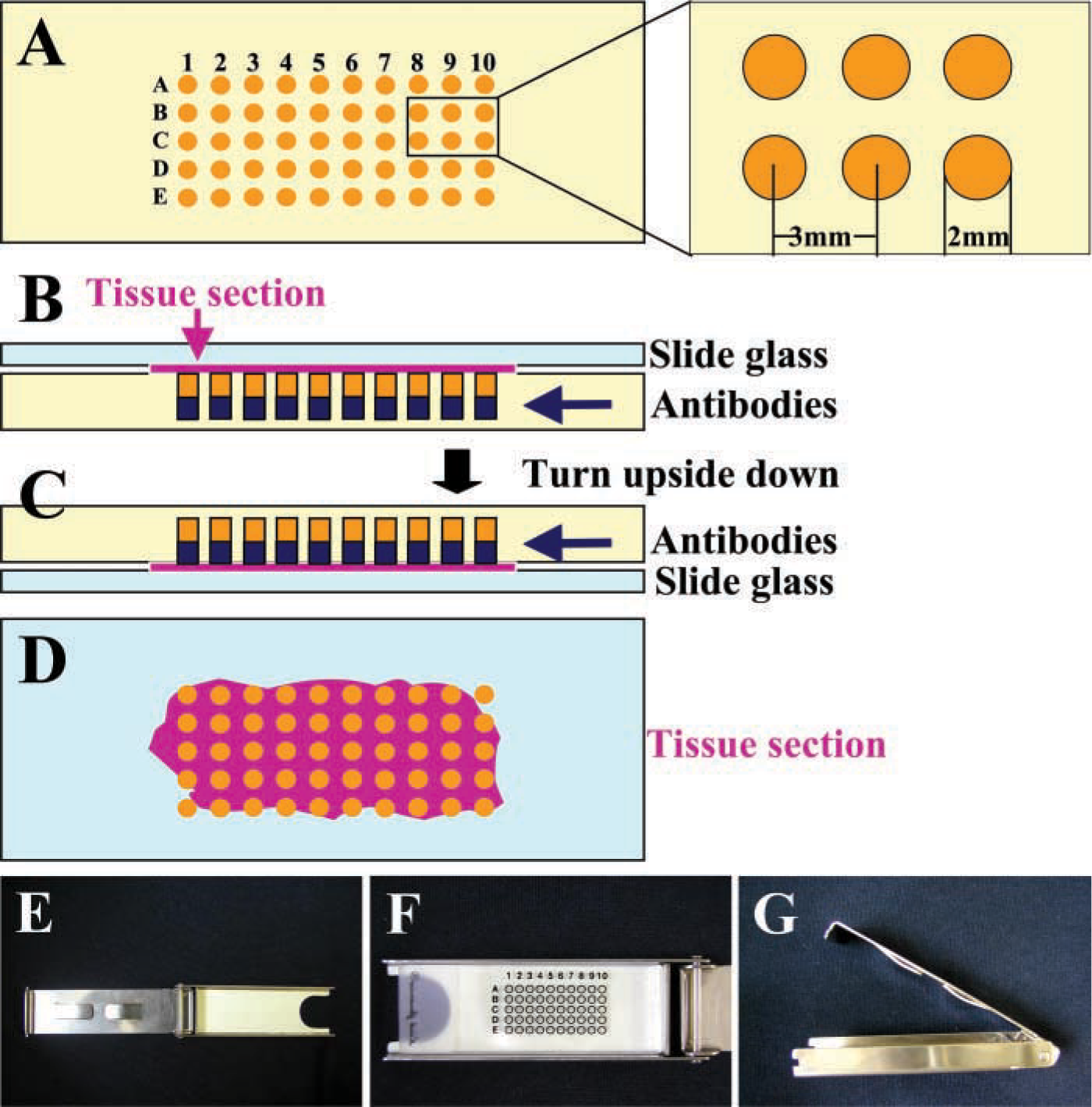
MI chips, which are the same size as glass slides, are fabricated from 5-mm-thick silicon rubber. Each chip contains 50 (5 × 10) wells that are 2 mm in diameter and 3 mm in depth (Figure 1A). The wells are arranged at 1-mm intervals and contain 4 μl of optimally diluted antibody solution. When each well is allotted different antibodies, the device allows simultaneous examination of 50 different antigens on a single tissue section.
Tissue Sections
The MI chip technology was applied to 4-μm-thick tissue sections of formalin-fixed, paraffin-embedded diffuse B-cell lymphoma and advanced gastric adenocarcinoma.
Cultured Cells
PC-14 cells, a human lung adenocarcinoma cell line (purchased from Riken Cell Bank; Tsukuba, Japan), were grown on a glass slide in Dulbecco's modified minimum essential Eagle's medium (DMEM; Nissui, Tokyo, Japan) supplemented with 10% fetal calf serum (FBS) in an incubator containing 5% CO2 at 37C. The slides were rinsed in PBS, dried well, and then fixed in 70% ethanol at room temperature (RT) for IHC.
Multiplex-immunostain chip. (
Immunohistochemistry
Each deparaffinized tissue section was treated with 0.3% H2O2 in 100% methanol to inhibit endogenous peroxidase activity and then incubated with normal goat serum for 20 min at RT. In the first experiment, one well in the center of the MI chip contained normal mouse serum; all remaining wells contained the antibody (4 μl) against leukocyte common antigen (CD45; DakoCytomation, Glostrup, Denmark) (Figure 2A). In brief, the slide was placed on the silicon rubber plate containing the serum and antibody and fastened tightly with the specially designed clamp (Figures 1E-1G). The slide and MI chip were then inverted (Figures 1B and 1C), allowing the antibody to contact the specimen, and incubated for 1 hr at RT. The section was incubated with universal immunoperoxidase (or alkaline phosphatase) polymer, anti-mouse and anti-rabbit (Histofine Simplestain Max PO or Histofine Simplestain Max AP; Nichirei, Tokyo, Japan) for 30 min at RT. Immunoreactivity was visualized with 3–3′-diaminobenzidine (DAB; Nichirei) and Fast Red (Nichirei) for peroxidase and alkaline phosphatase, respectively. Finally, sections were counterstained with Mayer's hematoxylin for nuclei. In the other experiments, two different antibody panels were applied to sections of malignant tumors (Tables 1–3). The IHC procedure was performed as described above.
(
Panels of Antibodies
Three different antibody panels were used to assess the usefulness of the MI chip. The first panel contained a single antibody against CD45 (DAKO), as mentioned above. This panel was applied to a section of B-cell lymphoma. The second panel consisted of nine different antibodies against lymphocyte markers, including CD45 (DAKO), CD20 (DAKO), CD45RO (DAKO), TdT (Novocastra; Newcastle upon Tyne, UK), CD22 (Novocastra), CD5 (Novocastra), CD10 (Novocastra), CyD1 (Novocastra), and CD3 (DAKO), and was also applied to a section of B-cell lymphoma for subclassification of the lymphoma (Tables 1 and 2). The third panel contained 11 different antibodies for detection of epithelial membrane antigen (EMA; DAKO), cytokeratin (AE1/3; DAKO), cytokeratin (MNF116; DAKO), vimentin (Nichirei), desmin (Nichirei), α-smooth muscle actin (α-SMA; Novocastra), CD45 (DAKO), neuron-specific enolase (NSE; Novocastra), S-100 (DAKO), HMB-45 (Enzo; Farmingdale, NY), and CD34 (Nichirei) (Tables 1 and 3). This panel was used to stain the gastric adenocarcinoma section and the cultured cell preparation.
Antigens examined in this study a
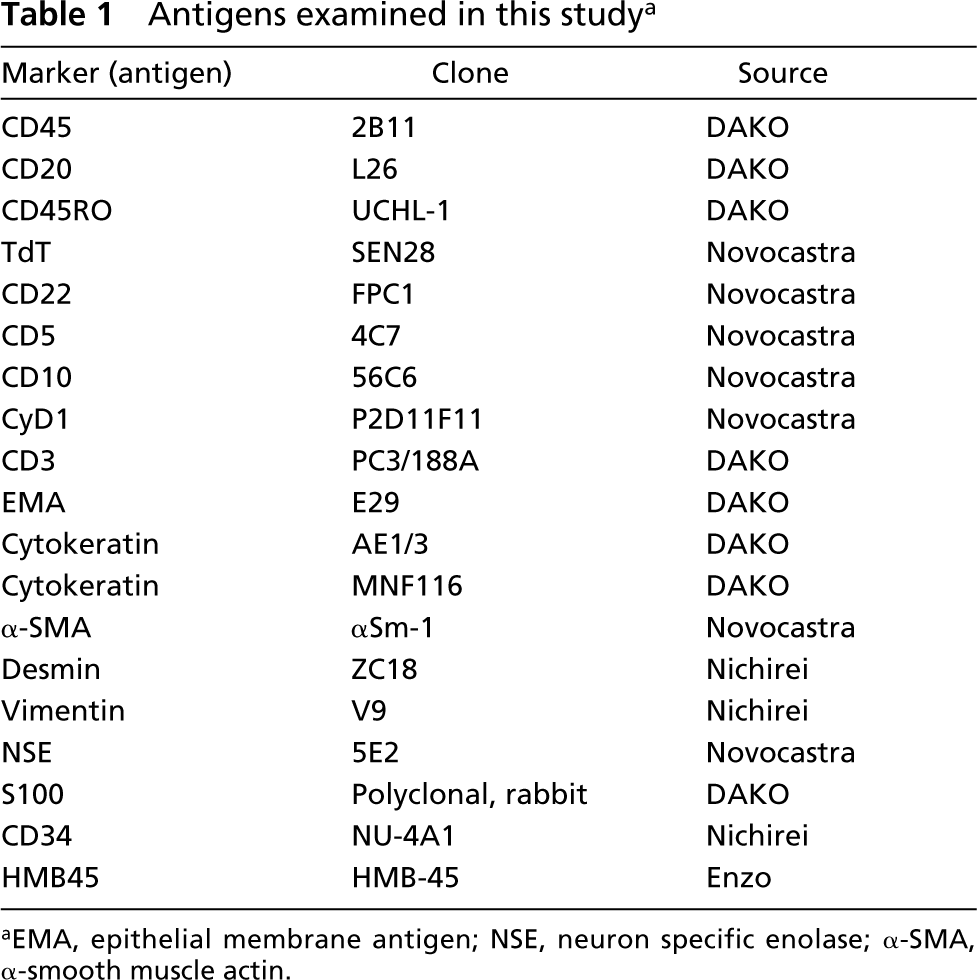
aEMA, epithelial membrane antigen; NSE, neuron specific enolase; α-SMA, α-smooth muscle actin.
Antigen Retrieval
Microwave exposure was done before IHC. The MI chip technology was also applied to sections of gastric adenocarcinoma that were heated at 100C for 20 min in 10 mM sodium citrate buffer (pH 6.0) in a plastic pressure cooker with a microwave oven (650 W). This method is generally effective for antigen retrieval for the antibodies used in this study (data not shown). Immunohistochemical staining of the sections exposed to microwaving was performed as described for the sections without microwave exposure.
Results
Immunostaining of Tissue Sections with an Antibody Against CD45
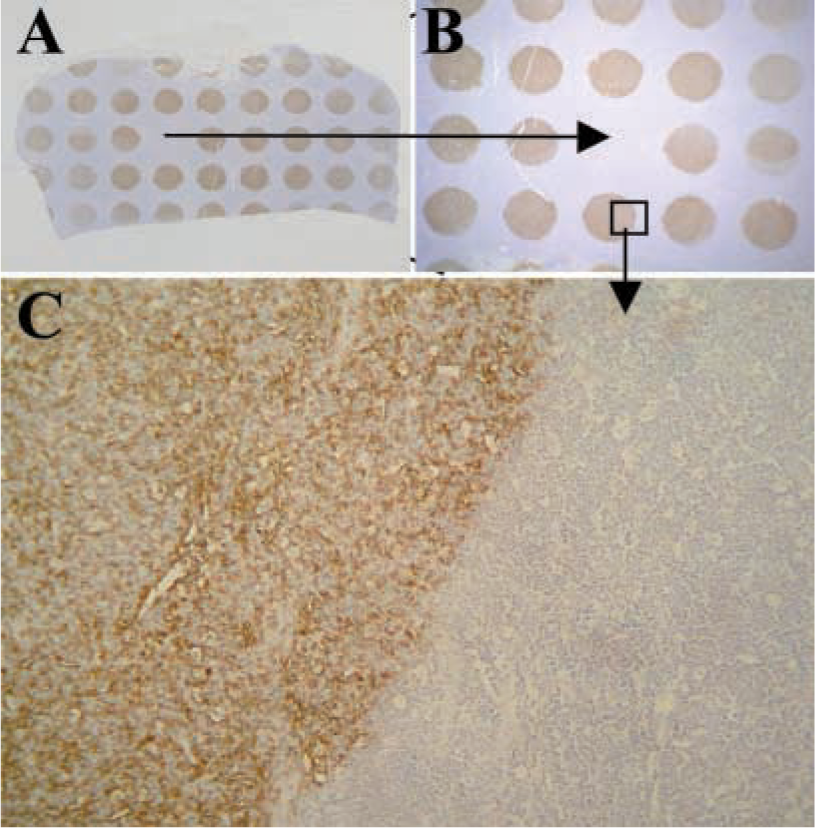
There were 49 macroscopically visible 2-mm brown spots corresponding to the wells containing the anti-CD45 antibody on the tissue section (Figure 2A). No brown DAB staining was visible on tissue surrounding the wells (Figures 2B and 2C). Microscopically, immunoreactivity was present in both normal and neoplastic lymphoid cells (Figure 2C). No other tissue components displayed immunoreactivity. The centrally located spot corresponding to the well without the antibody to CD45 and the surrounding tissue were indistinguishable (Figure 2B). Application of the MI chip did not affect specimen morphology.
Immunostaining of Tissue Sections with Panels of Different Antibodies
The lymphoma tissue section stained with the panel of nine different antibodies showed distinct spots, including lymphoma cells reactive with antibodies against CD45 and CD20. In contrast, spots corresponding to other antibodies were light in color macroscopically (Figure 3A). Microscopically, neoplastic lymphoid cells were positive for CD45 and CD20 but negative for other antibodies (Figures 3B and 3C). Antibodies other than CD45 and CD20 reacted with infiltrating non-neoplastic lymphocytes but did not react with tumor cells (Figures 3D and 3E). These IHC findings led to a diagnosis of B-cell lymphoma for this case.
Sections from a gastric adenocarcinoma specimen stained with 11 different antibodies showed spots containing cancer cells reactive with antibodies against EMA, AE1/3, and MNF116, all of which are epithelial markers (Figure 4A). In contrast, immunoreactivities for α-SMA, vimentin, desmin, and NSE were detected in original stromal tissue elements but not in cancer cells. CD45 was expressed exclusively by infiltrating leukocytes.
Influence of Antigen Retrieval
Antigen retrieval had no adverse effect on IHC. However, the tissue occasionally detached from the slide at areas in direct contact with the silicon rubber plate (data not shown).
Application to Cultured Cells
We applied the MI chip to cultured PC14 lung cancer cells grown on glass slides. The panel of antibodies applied to the cultured cells was the same as that used for analysis of gastric adenocarcinoma (Table 2). PC14 cells showed immunoreactivity only with the epithelial markers EMA, AE1/3, and MNF116 (Figures 5A and 5B).
Layout of antibodies (to antigens) on MI Chip for lymphoma a

aCyD1, cyclin D1; CDs, lymphocyte surface markers; TdT, terminal deoxynucleotidyl transferase.
Layout of antibodies (to antigens) on MI Chip for gastric adenocarcinoma and PC14 cells a

aEMA, epithelial membrane antigen; AE1/3, cytokeratin AE1/3; α-SMA, α-smooth muscle actin; NSE, neuron-specific enolase; Des, desmin; Vim, vimentin.
Discussion
MI chip technology is ideal for rapid and efficient tumor classification. With a single chip, a tissue specimen can be tested simultaneously for immunoreactivity with 50 different antibodies. Although the MI chip technology appears similar to tissue microarray (Kononen et al. 1998) and cell array (Oode et al. 2000) systems, it is very different. MI chip technology permits analysis of expression of as many as 50 antigens by a single tissue, whereas the other technologies permit analysis of a single antigen across a number of different tissues. Therefore, the MI chip is useful for the histopathological differential diagnosis of tumors that is done routinely in a typical pathology department. Cell arrays, tissue arrays, and MI chips can be used together for detailed analysis of antigen expression.
Both patient prognoses and treatment paradigms for different types of cancer depend on identification of specific antigens (Baars et al. 1999; Jones and Dorfman 2001; Chi 2002; Li 2002). Therefore, histopathological diagnosis is a prerequisite for optimal treatment of cancer patients. However, it is not always easy for trained pathologists to diagnose poorly differentiated tumors precisely in conventional tissue sections (Singer et al. 2000). Pathologists occasionally encounter tumors in which differentiation between carcinoma and sarcoma is difficult. The MI chip permits screening of such tissue specimens by IHC with multiple diagnostically relevant antibodies, leading to a more precise diagnosis. For example, the wells in a single MI chip can contain antibodies against both epithelial and non-epithelial markers for differentiation between carcinoma and sarcoma. Another panel of antibodies can be prepared for typing hematopoietic tumors.
Whether or not MI chip technology can adequately address heterogeneity in levels of antigen expression in tumors may be of concern because the area of specimen treated with antibody is small in comparison to that with conventional IHC methods. With the MI chip, one spot covers 3.1 mm2, which is large enough to evaluate the immunoreactivity of tumor cells. The specimen area in tissue microarray analysis is smaller than that in MI chip analysis. When two or three spots for the same antibody are distributed randomly on a chip, the problem of intratumor variation in immunoreactivity is reduced. In the clinical setting, pathologists make histological diagnoses from small biopsy specimens as well as large ones. With small tissue specimens, it is recommended to mount several sections from the same specimen on the same glass slide to approximate the size of a large section.
As shown in the present study, MI chip technology is an efficient and effective tool for evaluating expression of multiple antigens and is valuable for both routine histopathological examination and basic biological research.
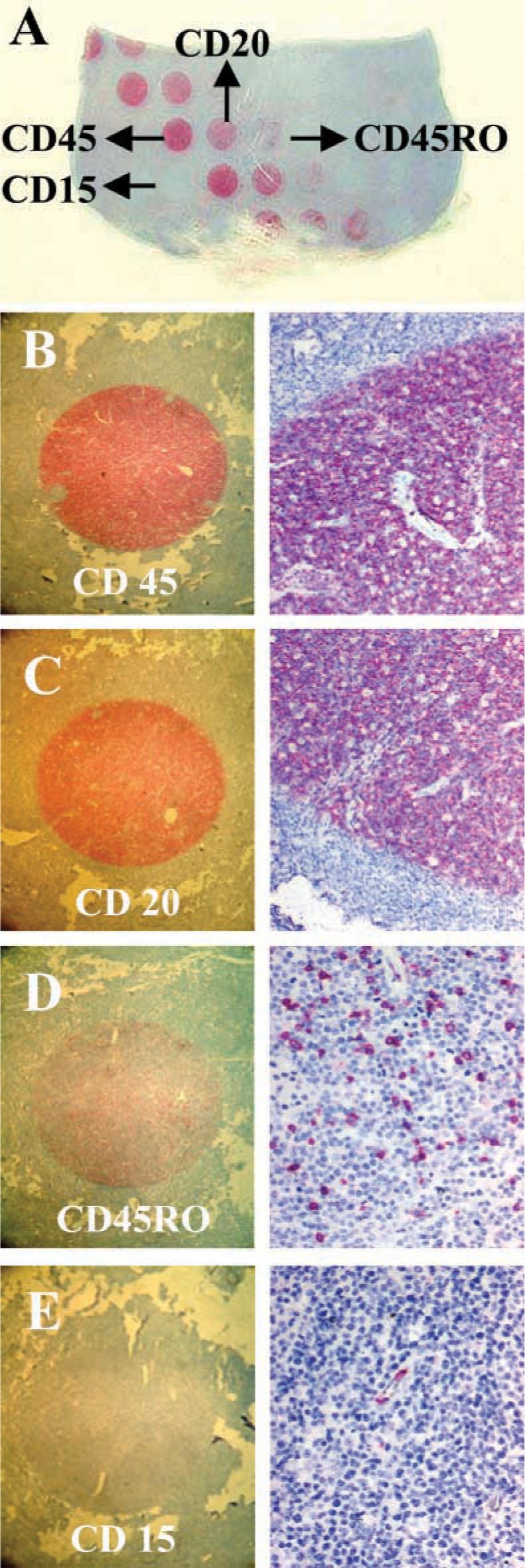
IHC staining of a tissue section from malignant lymphoma (B-cell type) with a panel of nine different antibodies in the MI chip (Table 2). Every five wells are allotted the same antibody. (
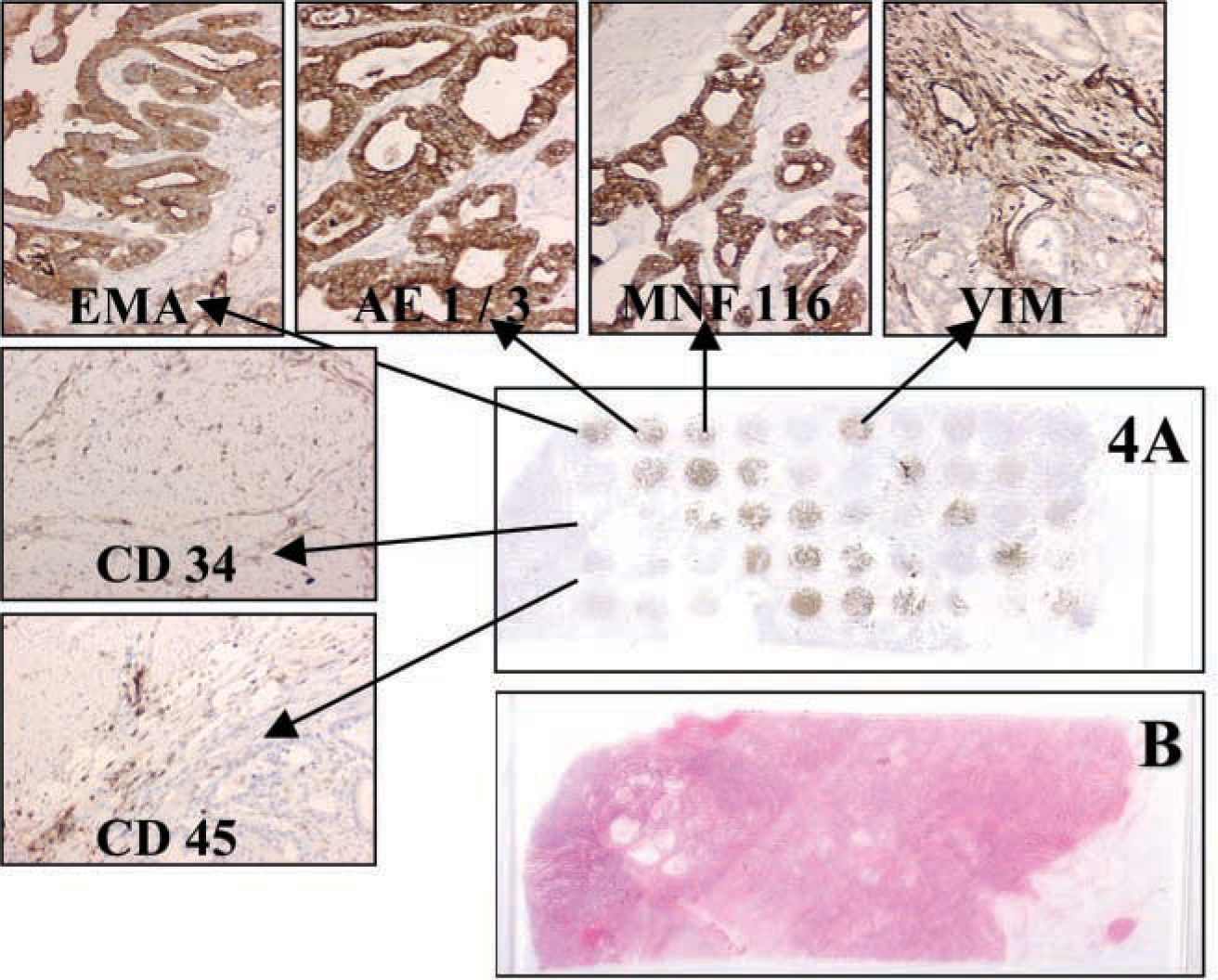
Immunostaining of a section of advanced gastric adenocarcinoma with MI chip containing 11 different antibodies and normal serum in quintuplicate (Tables 1 and 3). (
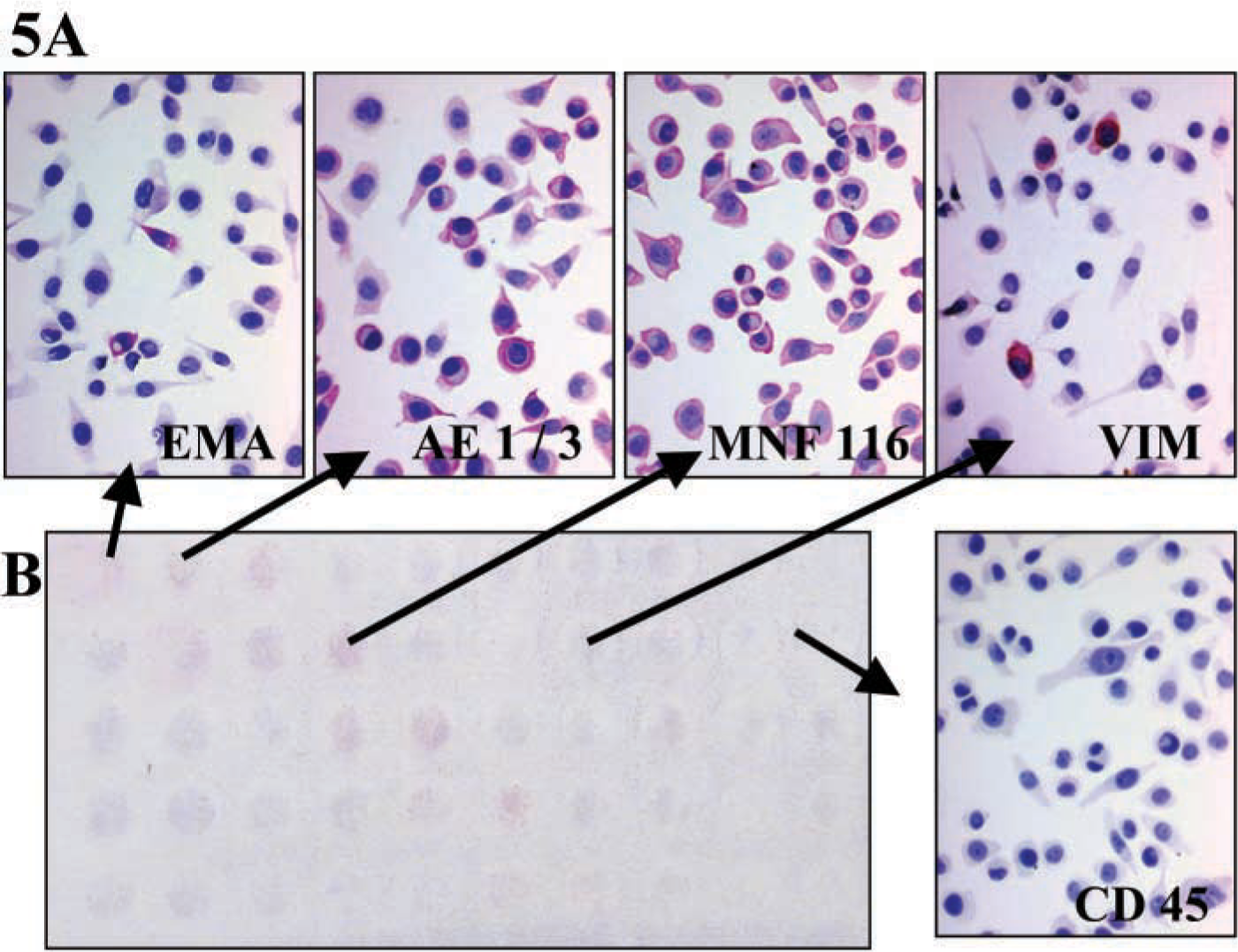
Immunostaining of cultured cell line PC14 with 11 different antibodies against EMA, AE1/3, MNF116, vimentin, desmin, α-SMA, CD45, NSE, S-100, CD34, and HMB35. (
Footnotes
Acknowledgements
Supported by Grants-in-Aid (nos. 14370071 and 13877027) from the Ministry of Education, Culture, Sports, Science and Technology.