
Abstract
P63 is essential for the differentiation of normal urothelium and is also expressed in transitional cell carcinoma (TCC) of the bladder. We investigated p63 immunoreactivity in upper urinary tract TCC (n = 53) and in renal-cell carcinoma (RCC; n = 188) using a tissue microarray technique. P63 expression was detected in 51/53 (96.2%) TCCs, showing decreased expression in high-stage (pT1 and pT2 100%; pT3 90.9%) and poorly differentiated (G1 and G2 100%; G3 92%) tumors. All RCCs were negative for p63. P63 proved to be a helpful tool, even in poorly differentiated and undifferentiated renal malignancies, to distinguish TCC from RCC.
Keywords
D
P63 comprises at least six different protein isoforms with homology to the tumor suppressor protein p53, which are generated from a single gene by two promoters and alternative splicing of the primary RNA transcript. Certain isoforms (TAp63) are capable of transactivating p53 target genes and inducing cell cycle arrest and apoptosis, and are mainly associated with the fully differentiated phenotype. Other isoforms (DeltaNp63), however, act as dominant-negative factors, inhibiting transcriptional activation by both p53 and TAp63 isoforms and are mainly associated with stem/reserve-cell populations. These findings show a switch in expression of p63 isoforms during normal cell differentiation and indicate that individual p63 isoforms may have different roles in neoplastic transformation (Nylander et al. 2002).
A strong nuclear p63 expression in normal human tissues has been reported in the basal-cell layers of stratified and transitional epithelia and in the basal/reserve-cell population of the respiratory tract, prostate, and breast tissue (Di Como et al. 2002; Nylander et al. 2002; Urist et al. 2002). Although mutations of p63 in human cancer cell lines are uncommon (Hagiwara et al. 1999), frequent alterations and loss of p63 expression have recently been described in advanced stages of human bladder carcinomas (Park et al. 2000; Urist et al. 2002). Thus far, p63 immunoreactivity of nonneoplastic renal tubule and collecting duct epithelium has not been investigated systematically, and reports on p63 expression in human malignancies, including RCCs, are limited due to the small number of cases investigated and the lack of information concerning histological subtypes (Kaufmann et al. 2001; Di Como et al. 2002).
Formalin-fixed and paraffin-embedded material of upper urinary tract TCCs (n = 53) and RCCs (n = 188) was selected from the files of our institute to investigate the expression of p63 and to assess the value of p63 for differential diagnosis in poorly differentiated and undifferentiated renal malignancies. In the RCC group, 66 (35.1%) tumors were in stage pT1a, 29 (15.4%) in pT1b, 13 (6.9%) in pT2, 39 (20.7%) in pT3a, and 41 (21.8%) in pT3b. Six (3.2%) were G1, 99 (52.7%) G2, 79 (42%) G3, and 4 (2.1%) G3-4 tumors. Histological subtypes (main component) were as follows: clear-cell (conventional) in 133 (70.7%), papillary in 20 (10.6%), chromophobe in 23 (12.2%), granular cell in 8 (4.3%), and spindle cell in 4 (2.1%). In the TCC group, 22 (41.5%) tumors were in stage pT1, 9 (17%) in pT2, and 22 (41.5%) in pT3. A total of 28 (52.8%) were G2 and 25 (47.2%) were G3 tumors. Neither stage pTa nor grade 1 tumors were found among the TCC group. Two specimens of nonneoplastic renal tissue were analyzed for comparison.
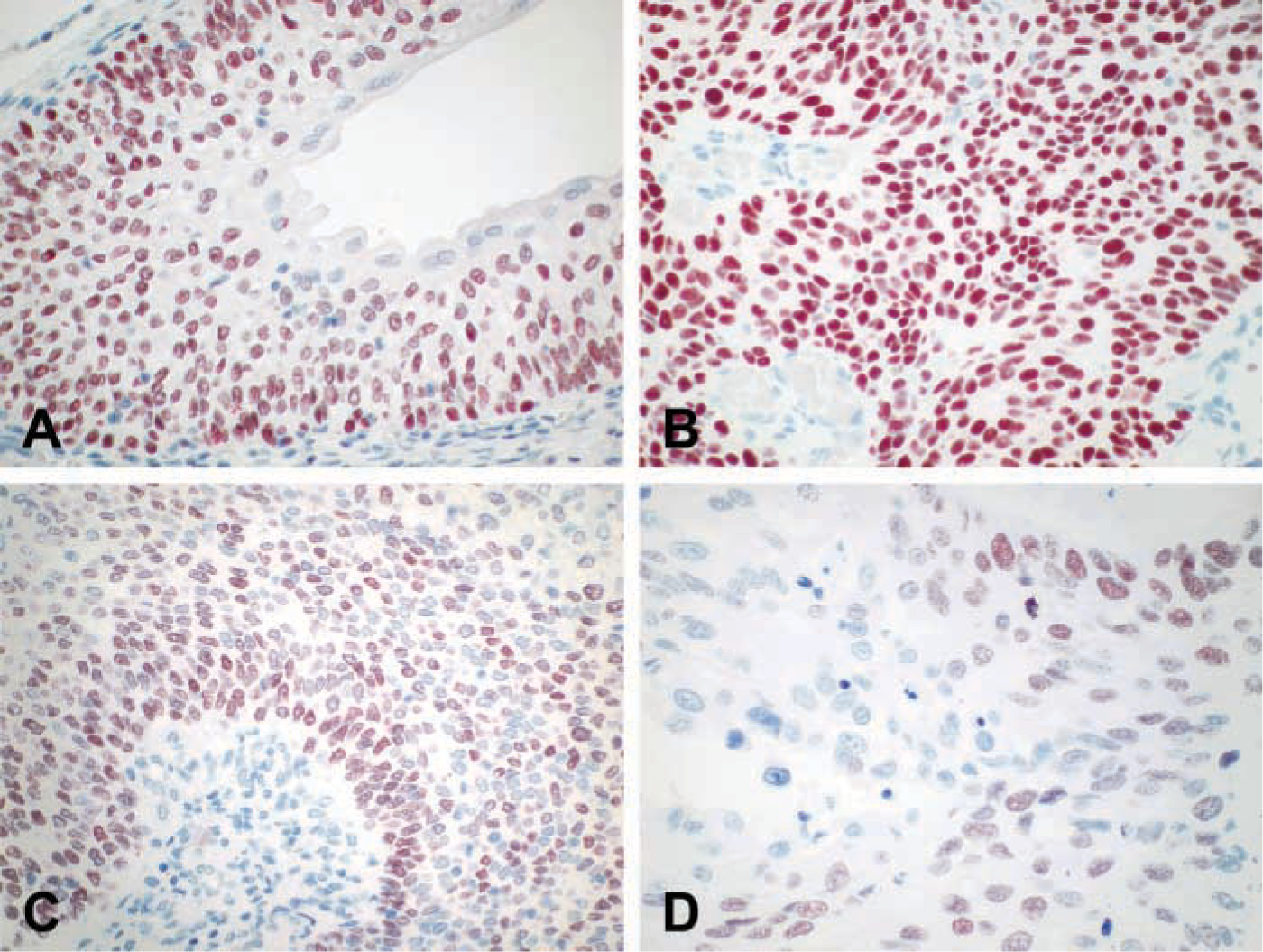
P63 expression in non-neoplastic pelvic urothelium (A) and upper urinary tract transitional-cell carcinoma (B-D). Note diffuse staining (B) and accentuation of immunoreactivity at the periphery of tumor nests with a decreasing gradient to the central zone (C) in moderately differentiated tumors. Marked heterogeneity of staining without a zonal pattern in a poorly differentiated tumor is shown in D. Original magnifications: A-C × 100; D X200.
For immunohistochemical evaluation, a tissue microarray technique (at least three cylindrical core biopsies 0.6 mm in diameter taken from different sites of each tumor; Kononen et al. 1998) and an automated immunostainer (DAKO-Autostainer, Universal Staining System; DAKO, Glostrup, Denmark) were used. Briefly, after microwave epitope retrieval (30 min. 160 W in Tris-HCl, pH 9.5 + 5% urea) sections were incubated for 30 min with the monoclonal mouse antibody Ab-4 (1:200; NeoMarkers, Fremont, CA), which recognizes all known isotypes of p63. Binding of the primary antibodies was assessed by the DAKO LSAB2 System detection kit. Immunoreactivity was analyzed semiquantitatively and documented in categories as follows: 0, no reactivity; 1, less than 10% of cancer cell nuclei positive; 2, 10–25% positive; 3, 25–50% positive; 4, 50–75% positive; 5, 75–90% positive; and 6, more than 90% of tumor cell nuclei positive for p63.
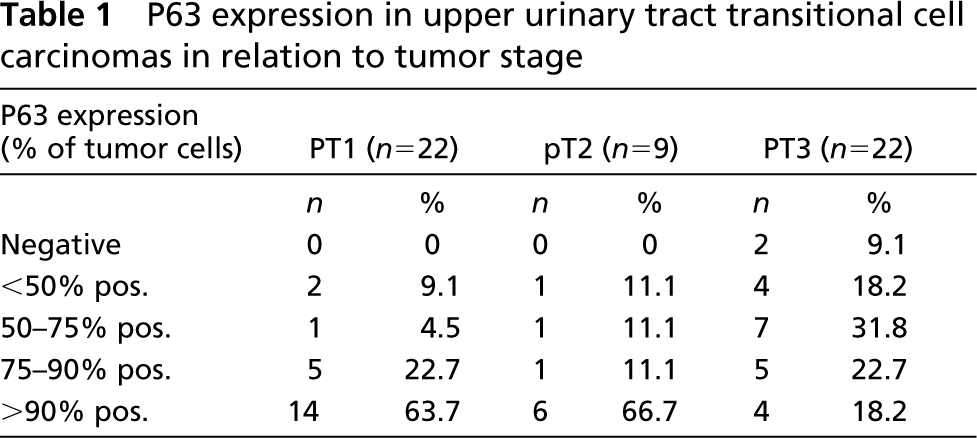
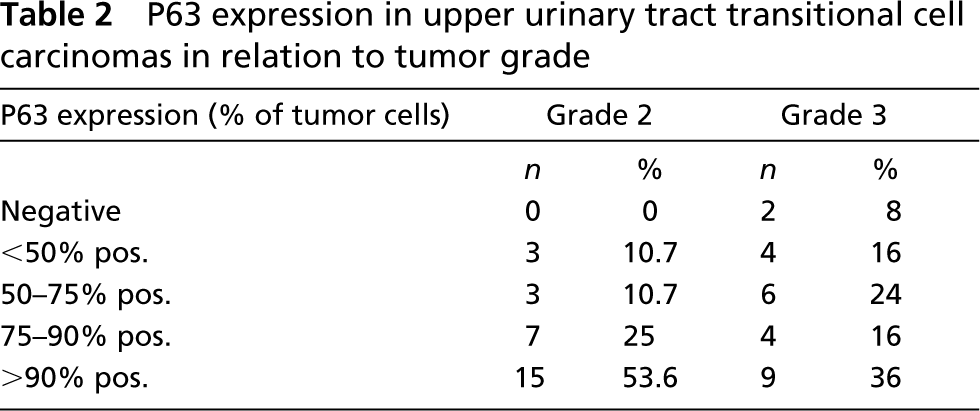
Non-neoplastic pelvic urothelium showed nuclear immunoreactivity with a slightly decreasing gradient from basal to luminar cells; superficial umbrella cells remained unstained (Figure 1A). Normal renal tubule and collecting duct epithelium and stromal cells lacked p63 expression. Tumor tissue sufficient for a reliable evaluation of p63 immunoreactivity was present in 184/188 (97.9%) RCCs and in all 53 TCCs. In the RCC group, all tumors regardless of histological subtype, grade, and stage were negative. In the TCC group, p63 was negative in 2/53 (3.8%) cases. P63 expression of less than 50% of tumor cell nuclei was found in 7/51 (13.7%), 50–75% in 9 (17.6%), 75–90% in 11 (21.6%), and more than 90% in 24 (47%) cases (Figure 1B). With regard to pT stage and tumor grade, a decrease of p63 expression in pT3 and G3 tumors was observed. Details are listed in Table 1 and 2. In moderately differentiated TCCs, staining was sometimes accentuated at the periphery of tumor nests with a decreasing gradient to the central zone, thus mimicking non-neoplastic transitional cell maturation (Figure 1C). In poorly differentiated TCCs a marked heterogeneity was noted (Figure 1D).
To our knowledge, this is the first study analyzing the expression patterns of p63 in a large number of RCCs and upper tract TCCs. The absence of immunoreactivity in non-neoplastic tubule and collecting duct epithelium, which are known to lack proliferative activity, is in accordance with the supposed function of p63 in the maintenance of a stem-cell population, regulating epithelial cell proliferation and differentiation (Nylander et al. 2002). All our RCCs were negative for p63. Even in poorly differentiated tumors and tumors with sarcomatoid transformation, no evidence of p63 expression was noted despite increased mitotic activity. These results are in line with previous reports from Di Como et al. (4/4 clear-cell RCCs negative; Di Como et al. 2002) and Kaufmann et al. (1/13 RCC positive, no histological subtype mentioned; Kaufmann et al. 2001). On the other hand, strong expression of p63 was detected both in normal pelvic urothelium and TCCs. The staining pattern of p63 in normal pelvic urothelium is identical to that of bladder mucosa (Di Como et al. 2002; Urist et al. 2002), and the decreased p63 immunoreactivity in pT3 and G3 tumors also resembles bladder TCCs (Urist et al. 2002). This indicates that, with respect to p63, upper tract TCCs are comparable to bladder cancer. Recently, a decrease of TAp63 and an increase of DeltaNp63 in bladder TCCs compared to normal urothelium were detected by quantitative PCR analysis. Regarding patient survival, the altered TAp63 expression reached borderline significance (Park et al. 2000). Therefore, we are now investigating whether p63 immunoreactivity is related to prognosis in patients with TCC.
P63 expression in upper urinary tract transitional cell carcinomas in relation to tumor stage
P63 expression in upper urinary tract transitional cell carcinomas in relation to tumor grade
Despite the altered nuclear immunoreactivity in high-grade (G3) cancers, only 2/53 (3.8%) TCCs did not show any nuclear staining for p63 in our series. These results clearly demonstrate that p63 is a reliable marker for the immunohistochemical distinction of upper tract TCC from RCC, which may be difficult in standard H&E sections but is essential for treatment and follow-up. Whether p63 might also serve as a prognostic marker in upper tract TCCs is now under investigation.