
Abstract
Examination of cause of death patterns among disabled people is shrouded by death patterns in the general population. To remove this shroud, we focus on multiple causes of death (MCOD) comorbidity patterns between decedents with and without Down syndrome with Alzheimer’s disease or unspecified dementia. Using 2005 to 2019 U.S. MCOD data, we examined comorbidity profiles of adults with (N = 7,936) and without (N = 4,593,118) Down syndrome using the broadest International Classification of Diseases (ICD-10) “List of 113 Selected Causes of Death” (selected cause groups) of death classification scheme as well as the ICD-10 “Specific Conditions” (specific causes). Comparison of these classification schemes revealed that the use of selected cause groups veiled comorbidities common among adults with Down syndrome—choking-related deaths, seizures and hypothyroidism. Results from this study underscore the necessity to change cause of death classifications schemes and/or the reporting of this information to account for differences and to mitigate data inequities.
Introduction
Life expectancy among people with Down syndrome increased substantially over the past 70 years due to improvements in medical care, social supports, and intervention efforts (Bittles and Glasson 2004; Torr et al. 2010). Despite this improvement, adults with Down syndrome still die on average 15.7 years younger than the general population (Landes, McDonald, et al. 2021). As more people with Down syndrome survive beyond age 40 years, researchers document a high prevalence rate of Alzheimer’s disease and/or unspecified dementia (AD/UD) in this population. According to the National Down Syndrome Society (2024), amyloid plaques and tangles in the brain, indicators of Alzheimer’s disease, exist in nearly all persons with Down syndrome by age 40, although onset of manifestations are estimated to be between 48 and 56 years (Head et al. 2012). According to a recent report on Down syndrome and associated Alzheimer’s disease in the United States, the prevalence of Alzheimer’s disease is roughly 6 times higher in adults with than without Down syndrome who are age 65 years and above (Weden et al. 2023), with survival between 4.6 years and 6.7 years (Lai and Williams 1989; Prasher et al. 2010).
Alzheimer’s disease is challenging to diagnose in the general population (Dilworth-Anderson et al. 2008; Poole et al. 2020) due to stigma and fear of a dementia-related diagnosis among patients, normalization of symptoms and lack of perceived need by patients and their carers, and the attribution of symptoms to the aging process (Knopman, Donohue, and Gutterman 2000; Parker et al. 2020; Swaffer 2014). Diagnosing Alzheimer’s disease proves a more formidable task for adults with Down syndrome due to additional challenges in the screening process. Preexisting cognitive limitations, having Alzheimer’s-related symptoms mistakenly associated with preexisting intellectual impairment, medication behavioral side effects, or difficulty differentiating this disease from other comorbidities, commonly referred to as diagnostic overshadowing, can all cloud the diagnostic process (Fortea et al. 2021; Marsack-Topolewski and Brady 2020; Nieuwenhuis-Mark 2009). Given diagnostic challenges and evidence that nearly all adults with Down syndrome develop Alzheimer’s disease neuropathology by age 40 (Antonarakis et al. 2020; Snyder et al. 2020), it is plausible that the actual prevalence of Alzheimer’s disease among adults with Down syndrome is higher than reported.
Research in the general population reports that Alzheimer’s disease and age are positively associated in the United States, with Alzheimer’s disease occurring in one in nine people age 65 years and older (Alzheimer’s Association 2024). Average duration (years lived after diagnosis) is between four and eight years among adults in the general population age 65 years and older (Alzheimer’s Association 2023). The three most common risks for Alzheimer’s disease in the general population include older age, genetic predisposition, and family history (Alzheimer’s Association 2024). Related to comorbidities, there is a high prevalence of cardiovascular diseases in general (Keene et al. 2001; Newman et al. 2005) as well as hypertension and diabetes specifically (Chen et al. 2017; Wang et al. 2018). Studies have further identified comorbidities that may be risk factors, those that may be sequelae of dementia, and risks that may be modifiable (Alzheimer’s Association 2024; Bauer et al. 2014).
Research on Alzheimer’s disease among adults with Down syndrome has primarily focused on predictors of disease, prevalence rates and survival, clinical presentation, and neuropathological trends (McGlinchey, McCallion, and McCarron 2020; Snyder et al. 2020). There has recently been more attention to the increasing knowledge of comorbidities, health care needs, and hospitalizations among adults with Down syndrome in general (Chenbhanich et al. 2019; Chicoine et al. 2021). Less attention has been provided to understanding the particular comorbidity patterns among adults with Down syndrome who have AD/UD. Yet understanding comorbidity patterns, particularly those that lead to mortality, can improve health care in adults with Alzheimer’s disease (Doraiswamy et al. 2002; Wang et al. 2018). In studies focused only on adults with Down syndrome, a higher volume of comorbidities and a higher prevalence of epilepsy, hypothyroidism, and respiratory diseases were reported among those with compared to those without Alzheimer’s disease (Bayen et al. 2018; McCarron et al. 2005).
Although it is important to understand comorbidity patterns solely among adults with Down syndrome and AD/UD, it remains unclear whether these patterns differ by Down syndrome status among adults with AD/UD. Differences are likely because those with Down syndrome are known to have higher numbers of comorbidities in general (Baksh et al. 2023; Kinnear et al. 2018), a much earlier age of dementia onset with shorter duration, and a higher prevalence of Alzheimer’s disease. For instance, respiratory diseases are not commonly reported as comorbidities among the general population with Alzheimer’s disease (Rajamaki, Hartikainen, and Tolppanen 2021; Santiago and Potashkin 2021). Because respiratory diseases are reported at overall higher rates among deaths of those with Down syndrome (Landes, Stevens, and Turk 2020; Santoro et al. 2021; Torr et al. 2010), it could be reasonably postulated that respiratory diseases would appear in comorbidity patterns of those with Down syndrome and Alzheimer’s disease.
It is also unknown if certain comorbidities vary by age group between decedents with and without Down syndrome, which is important given differences in age of onset. There is research indicating that age matters when observing comorbidities, such as differing numbers of comorbidities by age in adults with Down syndrome and dementia (Bayen et al. 2018). There is also research on the general population indicating that the association between certain comorbidities, such as hypertension, and risk of dementia are significant in adults at middle age but not at older ages (Corrada et al. 2017; Walker et al. 2019). There appears to be no research to date comparing comorbidity profiles at the time of death between adult decedents with and without Down syndrome who have Alzheimer’s disease. Without a clear picture of whether Alzheimer’s-related comorbidity profiles are similar or different for adult decedents with and without Down syndrome, it is possible that health care providers may conclude that medical comorbidity patterns observed in the general population also occur among adults with Down syndrome.
Ensuring quality health care for adults with Down syndrome and Alzheimer’s disease requires a clearer picture of possible differences in medical comorbidity profiles of adults with Alzheimer’s disease with and without Down syndrome. Currently, there is insufficient comparative U.S. data on comorbidity patterns among adults with and without Down syndrome with Alzheimer’s disease. Eventually, this may be possible through data collected by research projects such as the National Institutes of Health’s (2025) INCLUDE (INvestigation of Co-occurring conditions across the Lifespan to Understand Down syndromE) Project. Until that occurs, comparisons can be examined using multiple causes of death (MCOD) data (Landes, Finan, and Turk 2023). Research demonstrates the benefit of examining MCOD data because it avoids underestimating conditions contributing to death but not counting as the underlying cause of death (Piffaretti et al. 2016; Redelings, Sorvillo, and Simon 2006).
Yet although helpful, the way in which MCOD is schematically organized and examined potentially shrouds cause of death patterns among adults with Down syndrome. Death certificates and MCOD data provide a unique opportunity for surveillance and research. Death certification is the basis for state, national, and international mortality statistics reporting. The Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) centrally administers this program and database system and analyzes and reports statistics on leading causes of death in the United States for adults, infants, and children. The certificate is composed of Part I, listing the chain of events directly causing death, and Part II, listing diseases or conditions that contributed to death (where disability conditions commonly are considered). The World Health Organization (WHO) has established the International Classification of Diseases coding that is now in the 11th revision (ICD-11), although not implemented in the United States, which is currently using the 10th revision (ICD-10).
For consistency in mortality analysis and reporting, the NCHS established nine Mortality Tabulation Lists for death certification completion based on WHO lists (CDC and NCHS 2020). The “List of 113 Selected Causes of Death” is the classification scheme most commonly used when examining and reporting mortality patterns and ranking leading causes of death. It is inclusive of 113 causes and two additions in 2006 (enterocolitis due to clostridium difficile) and 2020 (COVID-19). The “113 Selected Causes of Death” list is central to reporting on causes of death in the United States (Curtin, Tejada-Vera, and Bastian 2024). However, it is important to understand that the “113 Selected Causes of Death” list classification scheme is based upon comorbidities that have “broad appeal and acceptance in the public health community” (Curtin et al. 2024). Because people with Down syndrome account for only .07% of the population (de Graaf, Buckley, and Skotko 2022), it is reasonable to question whether the “113 Selected Causes of Death” list is representative of their MCOD patterns.
Fortunately, there is a second list, formally called the “Each Cause List.” Although rarely used, the “Each Cause List” provides a table of all valid ICD-10 codes that can be used for underlying cause of death classification or co-occurring conditions at the time of death. Analysis of these and other lists to determine the complexity of multiple conditions and diseases in causing death composes MCOD reporting (Bishop et al. 2023).
Disability Data Justice
Medical sociology has historically neglected to include disabled people in our understanding of health and illness. Recently, Mauldin and Brown (2021) issued a call to bring the sociology of disability into robust dialogue with medical sociology. Although efforts to do so are growing (Bixby 2023; Carr and Namkung 2021; Landes, Stevens, and Turk 2022), more is needed. One area where the dialogue between the sociology of disability and medical sociology must consistently occur is within disability data justice. A disability data justice approach demands that the collection, analysis, and use of disability data is accurate, inclusive, and aimed at combatting the ableism embedded in our public health systems (Swenor 2022; Valdez and Swenor 2023).
At a baseline level, including the perspectives and experiences of disabled people in our understanding of health and illness requires the accurate collection and analysis of data on this population. Simply put, it is not possible to understand and address health inequities among disabled people without accurate data. One area where more work is needed to achieve disability data justice is in the analysis of cause of death data. Disability must be intentionally considered when using data to combat ableism. Although rarely discussed, this aim applies to the use of the National Vital Statistics System to understand cause of death patterns. One way that medical sociology can better include people with disabilities in our understanding of health and illness is by ensuring that data inequities do not hinder researchers and clinicians from understanding cause of death patterns among disabled people. We do so in this article by focusing on differences between adults with and without Down syndrome.
Removing the Shroud
Disability data justice requires that we attend to the potential structural ableism perpetuating data inequities. This concept refers to the system of discriminatory processes, institutions, and policies that perpetuate inequities where able-bodied people benefit and experience positive outcomes while neglecting disabled people (Keefe 2022; Lundberg and Chen 2024). Early efforts to address structural ableism in cause of death data focused on topics such as postmortem diagnostic overshadowing. This occurs when intellectual or developmental disabilities are inaccurately reported as the underlying cause of death on the death certificate, threatening the usefulness of underlying cause of death data for understanding health outcomes (Landes, Stevens, and Turk 2022; Landes, Turk, and Bisesti 2021; Landes, Turk, and Finan 2022). This was an important first step. But much more work is needed to address ableism built into the cause of death reporting practices. Beyond preventing intellectual and developmental disabilities from being inaccurately labeled as the underlying cause of death, it is important to identify and excavate the potential structural ableism within the larger coding system for cause of death conditions.
Some conditions of the “113 Selected Causes of Death” list are grouped (e.g., diseases of the heart include ICD-10 codes I00–I09, I11, I13, and I20–I51), whereas others are more discrete (e.g., acute bronchitis and bronchiolitis include ICD-10 codes J20 and J21). The decision-making related to the selected cause groups is not provided federally or internationally. Although there are instructions for cautions in completion related to elderly and infant decedent certification, there is no advisory related to disability conditions that often are listed as the direct cause of death (Landes, McDonald, et al. 2021; Landes, Stevens, and Turk 2019). It is possible that normative cause of death classification schemes that are based on the general population, which includes more nondisabled than disabled people (Varadaraj et al. 2021), may hide important cause of death patterns among decedents with Down syndrome. In other words, cause of death patterns among decedents with Down syndrome may be “shrouded” compared to cause of death patterns among decedents without Down syndrome. If so, we would have to conclude that the use of these classification schemes to understand comorbidity patterns among decedents continues the reach of structural ableism postmortem. This must be addressed in order to better understand comorbidity patterns among people with Down syndrome, who, as with other disabled people, are a health disparity population (Baksh et al. 2023; Reynolds 2024). In order to determine if and which conditions are shrouded, examining multiple causes of death using both the “113 Selected Causes of Death” list and ICD-10 “Specific Conditions” is an appropriate strategy.
The purpose of this study is to examine the comorbidity profiles associated with AD/UD in decedents with and without Down syndrome using MCOD data that encompassed both Part I and Part II of the death certificate. Our immediate concern is to advance knowledge of the different comorbidity patterns between adults with and without Down syndrome with AD/UD reported on their death certificates. Our long-term concern is to mitigate the data inequity that may be producing a severe lack of knowledge among researchers and clinicians regarding the health and health care needs of people with disability, in this case, those with Down syndrome.
Hypotheses
Data and Methods
Data
The 2005 to 2019 U.S. MCOD data were used to examine comorbidity patterns among adult decedents ages 18 and above with (N = 7,936) and without (N = 4,593,118) Down syndrome who had Alzheimer’s disease (ICD-10 code G30.9) or unspecified dementia (ICD-10 code F03), abbreviated here as AD/UD, reported on the death certificate. MCOD data included any ICD-10 diagnosis reported on the death certificate in either Part I of the death certificate, the diseases or injuries identified as part of the causal sequence leading to death, or Part II, other conditions present at the time of death but not indicated as having contributed to the causal sequence leading to death. Down syndrome was identified when ICD-10 code Q90.9 was reported in either Part I or Part II of the death certificate. The year 2005 was selected as a starting point for this study to ensure consistency and comparability because all U.S. states adopted the revised standard death certificate to align with the WHO’s ICD as of that year. Of note, there were changes in the coding and documentation of Down syndrome as the underlying cause of death that occurred over the study period. Instructions on documenting the underlying cause of death for people with Down syndrome who died from AD/UD were revised in 2013 so that Down syndrome is reported as the cause of death rather than Alzheimer’s disease or unspecified dementia. This acts as further justification for using MCOD data as opposed to underlying cause of death data.
Measures
Comorbidities were analyzed for six age groups: 18 to 49, 50 to 54, 55 to 59, 60 to 64, 65 to 69, and 70 and over. The top 10 AD/UD comorbidities for adults with and without Down syndrome using both the selected cause groups categories and the specific causes reported on the death certificates were identified. All comorbidities used for analysis were coded dichotomously. The abbreviations and shortened names of the most common comorbidities of AD/UD between those with Down syndrome and those without Down syndrome are reported in Table 1. Because they were the variables used for comparison, Down syndrome, unspecified (Q90.9); Alzheimer disease, unspecified (G30.9); and unspecified dementia (F03) were not included in the comparison of MCOD. Because intellectual disability (F70–F79) is a disability, not a disease, and indicative of Down syndrome for most individuals with this condition, it was not included in comparisons. For clarification, one of the selected cause groups, pneumonitis due to solids and liquids (J69), combines the specific causes of pneumonitis due to food and vomit (J69.0) along with other pneumonitis due to solids and liquids (J69.1–J69.8). However, of note in this study, there were only cases of pneumonitis due to food and vomit (J69.0) for adults with Down syndrome. Therefore, the percentages reported for the selected cause group of pneumonitis due to solids and liquids and the specific cause of pneumonitis due to food and vomit were the same.
Abbreviations and Shortened Names of Several of the Most Common Comorbidities of AD/UD between Those with Down Syndrome and Those without Down Syndrome.
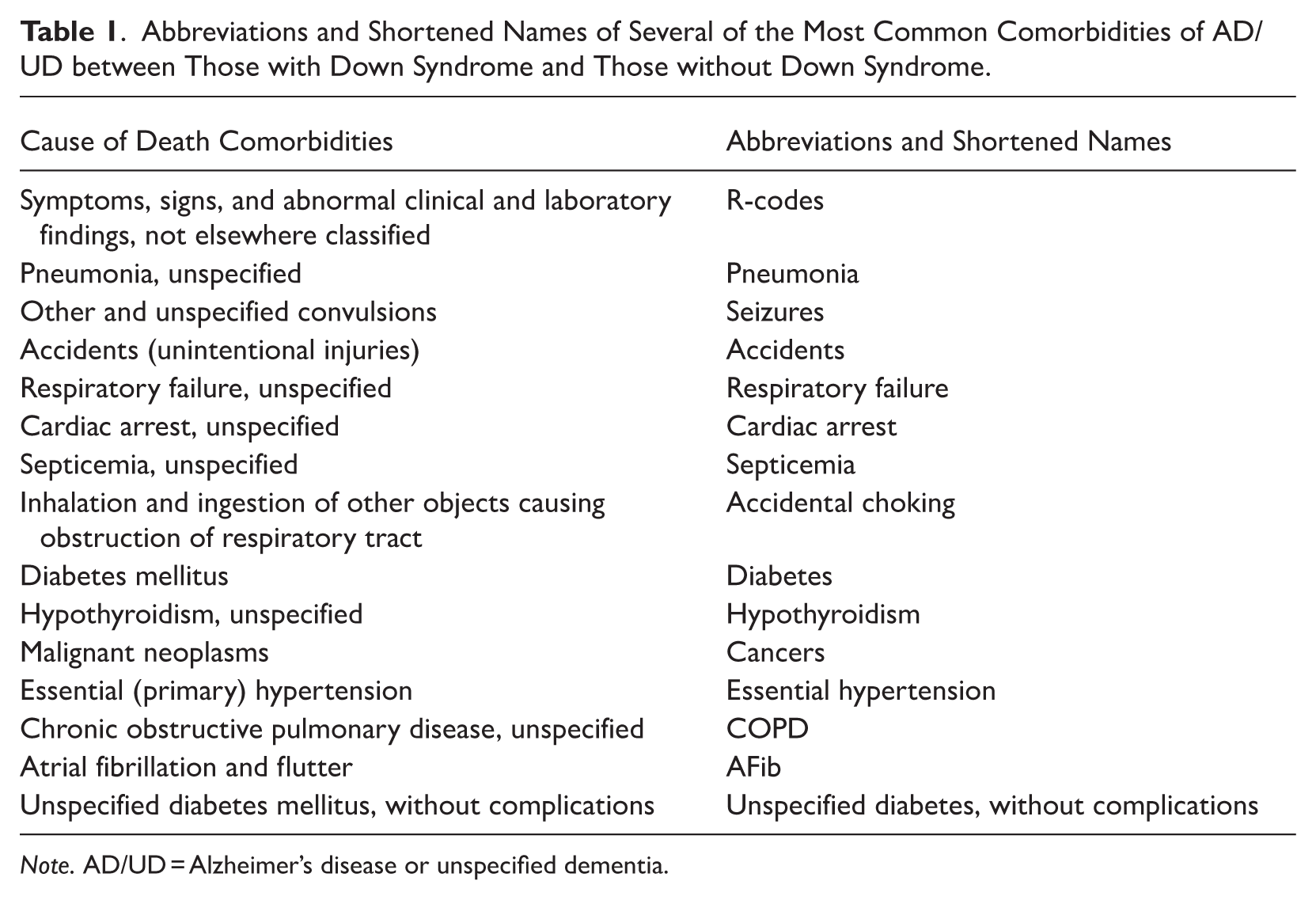
Note. AD/UD = Alzheimer’s disease or unspecified dementia.
Analytic Plan
To test our first hypothesis, we used two classification strategies to examine comorbidity patterns of adults with and without Down syndrome who had AD/UD reported on the death certificate. Our first strategy was to use the ICD-10 113 selected cause groups of death category list. Our second strategy was to use the entire list of ICD-10 specific conditions from the “Each Cause List” (referred to hereafter as specific causes) listed on the death certificate. Thus, for this strategy, we did not use any groupings, instead examining each specific cause of death listed on the death certificates used for the study. Comorbidities could have been reported on either Part I or Part II of the death certificate. Using both classification strategies allowed us to test our second hypothesis and determine whether the reach of ableism extends postmortem. Specifically, we examined whether marginalization is occurring within the comorbidity classifications schemes that health researchers use to understand the health of the population.
First, the most common AD/UD comorbidities were examined using the selected cause groups. Next, comorbidities were examined using the specific cause list. To test this study’s first hypothesis, the ranked 10 most common comorbidities for adults with and without Down syndrome were reported separately. To provide a point of comparison, conditions that appeared in the top 10 list only for one group were also listed and provided a rank order for the other group. To test this study’s second hypothesis, the ranked 10 most common comorbidities in each group were compared by classification scheme to determine any clear differences of using the selected cause groups or the specific cause list. Finally, the risk ratios of having the selected cause groups and specific causes as an AD/UD comorbidity for adults with compared to adults without Down syndrome were reported. General linear models were used to calculate the risk ratios, which were analyzed by age category. Analyzing risk ratios between decedents with and without Down syndrome by age group eliminated bias due to the difference in average age of death between the two groups. By taking age into account in this analysis, we avoided assuming that our current knowledge on AD/UD comorbidities and age-related disease patterns in the general population also reflect comorbidity profiles of people with Down syndrome. Analyses were conducted with Stata 18.0 (StataCorp 2023).
Results
The AD/UD rate among the study population was 28.44% for decedents with Down syndrome and 11.97% for decedents without Down syndrome. The average age of death for decedents with Down syndrome and AD/UD was 59.10 years, and the average age of death for decedents without Down syndrome with AD/UD was 86.50 years. The rankings of the top 10 most common comorbidities for AD/UD among adults with and without Down syndrome are reported in Table 2. For decedents with Down syndrome, the 1st through 10th most common selected cause groups in rank order were R-codes (34.02%), major cardiovascular diseases (20.67%); pneumonitis due to solids and liquids (18.18%); influenza and pneumonia (15.52%); other diseases of respiratory system (11.76%); accidents (6.35%); septicemia (6.26%); diabetes (2.95%); nephritis, nephrotic syndrome, and nephrosis (2.90%); and chronic lower respiratory diseases (2.07%). For decedents without Down syndrome, the 1st through 10th most common selected cause groups in rank order were major cardiovascular diseases (49.79%); R-codes (25.73%); diabetes (8.84%); influenza and pneumonia (8.29%); nephritis, nephrotic syndrome, and nephrosis (8.14%); chronic lower respiratory diseases (7.06%); other diseases of respiratory system (6.96%); cancers (5.96%); pneumonitis due to solids and liquids (4.88%); and accidents (4.52%). On the death certificate, R-codes are used for causes of death involving “symptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified.”
Comparing Rank Orders of the 10 Most Common Multiple Causes of Death with AD/UD between Those with Down Syndrome (N = 7,936) and Those without Down Syndrome (N = 4,593,118).
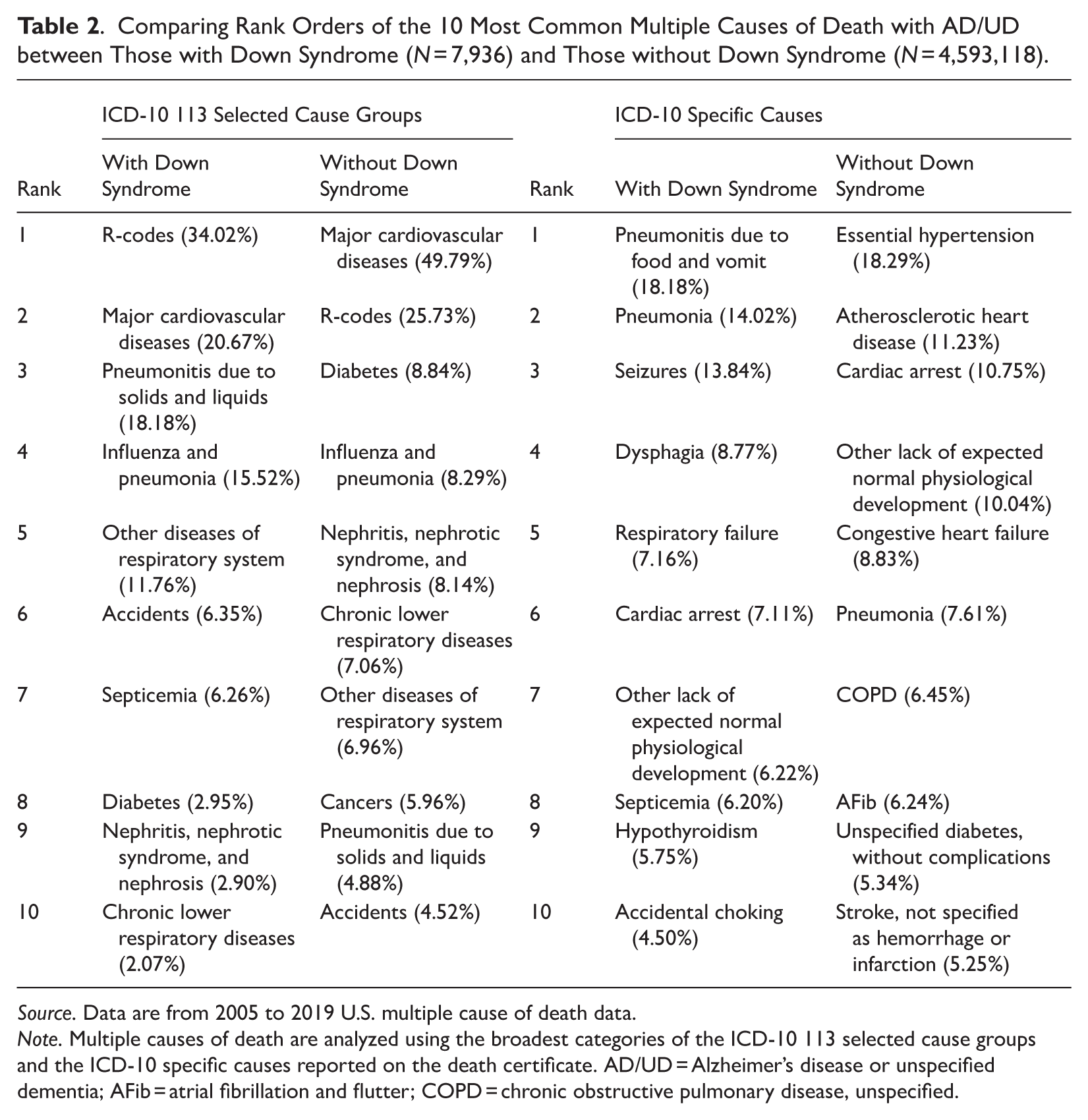
Source. Data are from 2005 to 2019 U.S. multiple cause of death data.
Note. Multiple causes of death are analyzed using the broadest categories of the ICD-10 113 selected cause groups and the ICD-10 specific causes reported on the death certificate. AD/UD = Alzheimer’s disease or unspecified dementia; AFib = atrial fibrillation and flutter; COPD = chronic obstructive pulmonary disease, unspecified.
For decedents with Down syndrome, the 1st through 10th most common specific causes in rank order were pneumonitis due to food and vomit (34.02%), pneumonia (14.02%), seizures (13.84%), dysphagia (8.77%), respiratory failure (7.16%), cardiac arrest (7.11%), other lack of expected normal physiological development (6.22%), septicemia (6.20%), hypothyroidism (5.75%), and accidental choking (4.50%). For decedents without Down syndrome, the 1st through 10th most common specific causes in rank order were essential hypertension (18.29%); atherosclerotic heart disease (11.23%); cardiac arrest (10.75%); other lack of expected normal physiological development (10.04%); congestive heart failure (8.83%); pneumonia (7.61%); chronic obstructive pulmonary disease (COPD; 6.45%); atrial fibrillation (AFib; 6.24%); unspecified diabetes, without complications (5.34%); and stroke, not specified as hemorrhage or infarction (5.25%).
Differences in Comorbidity Patterns Using Selected Cause Groups
There were differences in the rankings and frequencies of the observed selected cause group comorbidities between adults with and without Down syndrome. Among the selected cause groups, pneumonitis due to solids and liquids and other diseases of the respiratory system were relatively more common in adults with Down syndrome, and cancers and major cardiovascular diseases were relatively more common in adults without Down syndrome. There were also differences in the rankings and frequencies of the observed specific causes between adults with and without Down syndrome. Four of the top five specific causes for adults without Down syndrome were heart-related conditions: essential hypertension, atherosclerotic heart disease, cardiac arrest, and congestive heart failure—none of which appeared in the top five conditions for adults with Down syndrome.
Table 3 shows the risk ratios of having each comorbidity on the death certificate for adults with AD/UD compared to without Down syndrome. These risk ratios are sorted by age groups, first presenting the most common selected cause groups comorbidities and then presenting the most common specific causes.
Risk Ratios of Having a Certain Condition as a Comorbidity of AD/UD for Adults with Down Syndrome (N = 7,936) Compared to Adults without Down Syndrome (N = 4,593,118) by Age Groups.
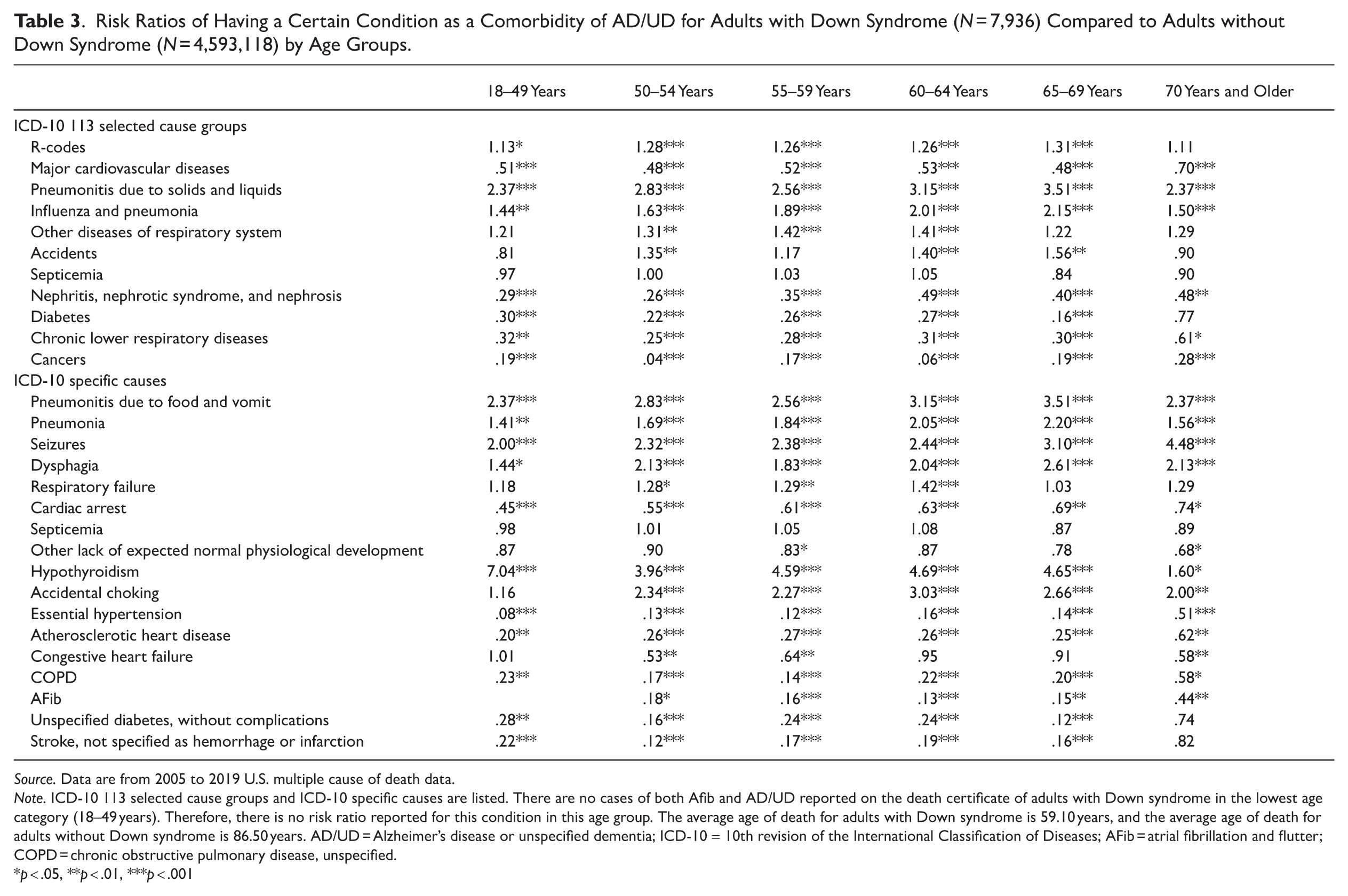
Source. Data are from 2005 to 2019 U.S. multiple cause of death data.
Note. ICD-10 113 selected cause groups and ICD-10 specific causes are listed. There are no cases of both Afib and AD/UD reported on the death certificate of adults with Down syndrome in the lowest age category (18–49 years). Therefore, there is no risk ratio reported for this condition in this age group. The average age of death for adults with Down syndrome is 59.10 years, and the average age of death for adults without Down syndrome is 86.50 years. AD/UD = Alzheimer’s disease or unspecified dementia; ICD-10 = 10th revision of the International Classification of Diseases; AFib = atrial fibrillation and flutter; COPD = chronic obstructive pulmonary disease, unspecified.
p < .05, **p < .01, ***p < .001
Examining the selected cause groups, the risk ratios of major cardiovascular diseases as a comorbidity were significantly lower for adults with than without Down syndrome across age groups. Risk ratios were much higher for adults with than without Down syndrome for pneumonitis due to solids and liquids, and this was statistically significant across all age groups, with the risk ratio over 2 times as high at ages 18 to 59 years and age 70 and older and 3 times as high at ages 60 to 69. Risk ratios of nephritis, nephrotic syndrome, and nephrosis; diabetes; chronic lower respiratory diseases; and cancer were lower for adults with than without Down syndrome, and this difference was most pronounced at younger ages. Meanwhile, the risk ratios of influenza and pneumonia and other diseases of the respiratory system were higher for adults with than without Down syndrome.
These risk ratios and their significance levels across age groups help show the real differences in AD/UD comorbidity profiles between those with and without Down syndrome. Comorbidity profiles significantly differ between those with and without Down syndrome even when stratifying for age, suggesting that this factor should not be considered as a sole reason for these differences. Although certain risk ratios, such as hypothyroidism, were higher at the youngest age group, risk was still higher for people with Down syndrome at every age, presenting an actual difference from the general population.
Differences in Comorbidity Patterns Using Specific Causes
Differences between decedents with/without Down syndrome were more apparent when examining the specific causes. Although within the top 10 most common specific cause comorbidities for both groups, pneumonia was relatively more common in adults with Down syndrome. Most importantly, there were common comorbidities for adults with Down syndrome that were completely shrouded when solely using the selected cause groups. There were three choking-related causes of death in the specific cause top 10 list for adults with Down syndrome: pneumonitis due to food and vomit, dysphagia, and accidental choking; none of these appeared in the specific cause top 10 list for those without Down syndrome. However, when using the selected cause groups, only one choking-related comorbidity appeared in the top 10 list for adults with Down syndrome: pneumonitis due to solids and liquids, which did appear in the selected cause groups top 10 list for those without Down syndrome. Therefore, use of the selected cause groups not only shrouded the prevalence of choking-related deaths for adults with Down syndrome, but it also hid the higher percentage of adults with Down syndrome dying with a choking-related death such as dysphagia or accidental choking compared to adults without Down syndrome (a combined 31.45%). Other important and completely missed comorbidities for adults with Down syndrome when observing the selected cause groups were seizures and hypothyroidism.
Comparing rank order (see Appendix A in the online version of the article) of the 10 most common ICD-10 specific causes only among those with Down syndrome between decedents with AD/UD (N = 7,936) and without AD/UD (N = 19,972) showed variation in MCOD when AD/UD was present. There were elevated rates of choking-related deaths, particularly dysphagia, ranking 4th (8.77%) among those with AD/UD and ranking 8th (5.35%) among those without AD/UD. Pneumonitis due to food and vomit ranked 1st among those with AD/UD (18.18%) and 2nd for those without AD/UD (16.14%). Conditions ranking for those without AD/UD that do not appear in the 10 most common comorbidities list for those with AD/UD include congestive heart failure (8.06%) and acute respiratory failure (5.26%), and conditions ranking for those with AD/UD that do not appear in the ranked list for those without AD/UD include other lack of expected normal physiological development (6.22%) and accidental choking (4.50%). Of note, cardiac arrest ranked higher for those without AD/UD (13.73%) than those with AD/UD (7.11%). In addition, there were higher percentages of seizures and hypothyroidism among those with AD/UD (13.84% and 5.75%, respectively) than without (10.25% and 4.94%, respectively).
Examining the risk ratios for specific causes (Table 3), risk ratios of pneumonitis due to food and vomit, pneumonia, seizures, dysphagia, and hypothyroidism were higher for adults with than without Down syndrome, and these were statistically significant across all age groups. Risk ratios of accidental choking were also higher for adults with than without Down syndrome, and these were statistically significant at age 50 years and above. Risk ratios were lower among adults with than without Down syndrome for cardiac arrest; essential hypertension; atherosclerotic heart disease; COPD; unspecified diabetes, without complications; and stroke, not specified as hemorrhage or infarction across age groups, with the risk ratios lowest at ages under 70 years. The conditions with risk ratios most similar between adults with and without Down syndrome include septicemia and other lack of expected normal physiological development. There were no adults with Down syndrome and AD/UD in the youngest age group (18–49 years) who had AFib reported on the death certificate, so there is no risk ratio for this condition for this age group.
When focusing on the risk ratios of the comorbidities shrouded by the selected cause groups, substantial differences between adults with and without Down syndrome were observed. Risk ratios for MOCD for choking-related comorbidities, seizures, and hypothyroidism were higher for adults with than without Down syndrome. Risk ratios for dysphagia were significantly higher for all age groups, and accidental choking reached about 3 times as high for adults with than without Down syndrome between 60 and 64 years of age. Seizures and hypothyroidism, two additional comorbidities not identified when using the selected cause groups, were much higher for adults with than without Down syndrome. Risk ratios for seizures were significantly higher for all age groups, being over 4 times as high for the oldest age group. Risk ratios for hypothyroidism were also high in those with Down syndrome, being about 7 times as high at the youngest age group—the largest risk ratio for any comorbidity.
Discussion
Results from this study provide evidence supporting Hypothesis 1 because there were distinct differences in MCOD comorbidity patterns between adult decedents with and without Down syndrome. Results also demonstrate that differences in comorbidity patterns in adults with and without Down syndrome with AD/UD depend on how cause of death is classified, providing evidence in support of Hypothesis 2. Sole reliance on the selected cause groups of death classification shrouds critical differences in MCOD comorbidities among adults with Down syndrome. This study demonstrates that MCOD tell a different story for adults with Down syndrome depending on classification scheme.
Relying solely on the selected cause groups to understand comorbidity patterns in adults with AD/UD on their death certificates heavily caters to the general population, perpetuating structural ableism postmortem. Although use of the selected cause groups shrouded the actual specific causes of death for adults with Down syndrome, this was not the case for adults without because the mortality burden of heart-related causes remained clear when using both schemes. The decision to only use the selected cause groups to analyze and report cause of death data further marginalizes people with Down syndrome from public health surveillance, reinforcing data inequities.
The most striking example of this shrouding is choking-related cause of death morbidities. The selected cause groups do not group pneumonitis due to food and vomit, dysphagia, and accidental choking as choking-related risk conditions, instead separating these causes of death into three distinct categories. For this reason, although choking-related causes of death combined (pneumonitis, dysphagia, accidental choking) are a highly prominent comorbidity for people with Down syndrome (31.45%), the presence of this potentially preventable cause of death is shrouded when using the selected cause groups classification scheme.
The higher risk of choking-related comorbidities was only apparent when using the specific causes coding scheme. Although this critical information about the cause of death comorbidities among adults with Down syndrome is hidden when relying on the selected causes, unshrouding this information is not a surprising finding because these conditions are more prevalent in general among adults with Down syndrome compared to those without Down syndrome (Cooper et al. 2020; Robertson et al. 2018). They are often identified early in life and are generally unrelated to AD/UD, with dysphagia tending to progress with age regardless of AD/UD status (Sanders et al. 2024). They may also partially explain higher rates of pneumonia in this population (Chicoine et al. 2021; Santoro et al. 2021). The high percentage of choking-related deaths among those with Down syndrome observed in this study likely reflects both the underlying prevalence of dysphagia and increased recognition of swallowing impairments. Additionally, dysphagia and gastroesophageal reflux have been shown to have a significant association with multiple hospitalizations among adults with Down syndrome (Chenbhanich et al. 2019).
Although not surprising that a high rate of choking-related comorbidities were unshrouded when using the specific causes, this finding provides crucial information on the population of adults with Down syndrome. Based on these findings, it is imperative for medical providers who are caring for adults with Down syndrome and AD/UD to assess for clinical signs of dysphagia, aspiration, and gastroesophageal reflux disease and when present, implement appropriate assessment and interventions addressing oral-motor skills, positioning, appropriate diet, and necessary supports and adaptations for meals (Lazenby 2008; Manduchi, Fainman, and Walshe 2020; Smith, Teo, and Simpson 2014). Dysphagia is typically progressive as AD/UD symptoms advance and requires monitoring and periodic assessments. Clinicians who are not aware that adults with Down syndrome manifest symptoms and conditions commonly seen in an older population at much younger ages and that the pathology may progress may miss an opportunity for early recognition of onset or change and treatment of these conditions.
It is also not surprising that use of the selected causes revealed that R-codes are more common on the death certificates of people with Down syndrome. This finding likely reflects uncertainty regarding underlying causes of death among certifiers for decedents with intellectual and developmental disabilities (Landes et al. 2019, 2023; Landes, Turk, and Finan 2022). Uncertainty surrounding death is associated with intellectual or developmental disabilities being inaccurately reported as the underlying cause of death, obscuring cause of death patterns.
Epilepsy is a medical condition associated with Alzheimer’s disease that affects adults with and without Down syndrome, yet it is not well represented when using the selected cause list. Related to Down syndrome, previous studies have reported an association between clinical dementia and epilepsy among adults with Down syndrome (Bayen et al. 2018; McCarron et al. 2017), yet this condition only appeared in the ranked 10 most common comorbidities when using the specific cause list. In Down syndrome, seizures are commonly diagnosed early in life, and later onset is often a prodrome for an AD diagnosis (Bayen et al. 2018); presence of seizures has been implicated in declining cognition in those with Down syndrome (Lott et al. 2012). Promoting use of the specific cause list could elevate assessments and possibly treatment for seizures for those with Down syndrome. For adults without Down syndrome, epilepsy was not found in either of the classification schemes despite the association of seizures with poor cognitive and functional performance and the strong association with the underlying neuropathology (Vöglein et al. 2020). In this instance, clinicians may not recognize the strong association of seizures with poor performance and may therefore either not consider listing seizures as a contributing cause of death or not understand how to complete the certification process.
The vast amount of literature on Alzheimer’s disease rightly characterizes it as most common among older adults and also accompanied by comorbidities indicative of older age. This overall assessment holds true for the general population. However, it is important to realize that comorbidities among adults with Down syndrome and AD/UD are quite distinct from those of an aging general population with AD/UD. Physicians unaware of this distinction may not assess adults with Down syndrome for these comorbidities based on their understanding that AD/UD is often associated with diseases typical of older age. It is also important to note that prior research has identified conditions that are common in those with Down syndrome in general, such as sleep apnea, and conditions commonly mistaken for AD/UD, such as depression and hearing loss (Bayen et al. 2018; Capone and Chicoine 2022; Fortea et al. 2021; Jensen and Bulova 2014; McCarron et al. 2005). Unless clinicians receive medical education throughout their training that is inclusive of disability knowledge and skills, in this case, of common medical condition profiles of adults with Down syndrome with and without AD/UD symptomatology, diagnostic overshadowing, delayed diagnosis, and delayed management may continue to contribute to younger mortality. In addition, although unintended, clinicians may incorrectly generalize patterns seen in the general population when treating patients with Down syndrome and AD/UD.
To ensure that these misunderstandings do not occur, data equity is necessary through a disability data justice approach (Swenor 2022). As evidenced by this study, the method of classifying and reporting causes of death data influences knowledge of comorbidity profiles for adults with Alzheimer’s disease with and without Down syndrome. Use of the selected cause groups based upon the health profile of the overall general and largely nondisabled population introduces an element of bias to results that does not ensure equitable health outcomes for disabled people. Examining structural ableism and identifying the ways in which it acts and interferes with our understanding of health disparities, even when not intended, is a necessary step toward ensuring disability data justice (Jain 2025; Swenor 2022; Valdez and Swenor 2023). Given the evidence of postmortem diagnostic overshadowing on death certificates, examining structural ableism in cause of death coding schemes would further highlight how health inequities between disabled and nondisabled people are maintained through structural forces.
Our findings of structural ableism in death certificate coding systems contribute to medical sociology by highlighting ways to make the field more inclusive of disabled people. A disability data justice approach is essential to achieving data equity, and it is crucial that we consider disability in every aspect of how we observe and identify health disparities (Mauldin and Brown 2021). A requirement to complete specific training on death certification completion or an advisory on listing or including underlying disabilities may be one way to improve the database used to explore comorbidity profiles.
As with all studies using death certificate data, there are some clear limitations. First, there are no assurances that all decedents with Down syndrome have this disability reported on their death certificate. There is also difficulty with diagnosing AD in people with disabilities in general, with poor recognition of symptoms, missed diagnoses, overshadowing of other diagnoses, and only recent assistance from a clinical guideline about best diagnostic practices, published in 2020 (Cipriani et al. 2018; Tassé et al. 2016). Although unable to completely address this limitation, including unspecified dementia may partially address this issue. Second, comorbidity profiles relate to the known health conditions at the time of death, either within the sequence of causation or as a known comorbidity, and relies on accurate listing by those completing the certificate (Stevens and Landes 2021). Consequently, not all known health conditions may be listed (e.g., arthritis, vision impairments), and there may be unrecognized conditions. Additionally, selection bias is possible if AD/UD is more likely to be recorded in severe cases. Finally, although this study uses MCOD data, comorbidity prevalence estimates may differ if certifiers are more likely to record certain comorbidities for decedents with Down syndrome. The conditions identified in this study provide at least some evidence of comorbidities leading to or present at the time of death.
Conclusion
There were distinct profiles of mortality-associated comorbidities for people with AD/UD with and without Down syndrome. Adults with Down syndrome and AD/UD showed higher risks of respiratory conditions, seizures, and dysphagia, which are common comorbidities among adults with Down syndrome in general. Choking-related incidents were especially common in those with Down syndrome and AD/UD, although these comorbidities were shrouded when using the selected cause groups rather than the specific causes. Among adults with AD/UD but without Down syndrome, the comorbidity profiles showed a predominance of cardiovascular comorbidities. It is important that clinicians recognize these distinct patterns and increase identification of other treatable health conditions that may mask or mimic dementia.
Given the different comorbidity patterns presented in adults with and without Down syndrome in addition to the clear differences in those patterns depending on coding scheme, our concern is that continued use of a coding scheme biased to the nondisabled population further marginalizes people with Down syndrome by reinforcing data inequities. The manner in which these systems of coding were originally organized along with the continued sole reliance on these systems produce a structural system that necessarily shrouds critical information about adults with Down syndrome. The question that lingers is whether the same occurs regarding adults with other disabilities. To ensure that clinicians recognize these distinct health profiles, this study’s results suggest that medical sociologists and health researchers need to reconsider the role data inequities play in our understanding of health profiles and patterns. This includes consideration of how current cause of death classification schemes are influencing our perception of health and mortality disparities.
The continued use of the selected cause groups despite knowing that it hides the prominent causes of death among adults with Down syndrome amounts to an ableist practice. Using the selected cause groups to analyze general population trends may be useful, but improving the monitoring of health trends for subpopulation groups, such as adults with Down syndrome, will require researchers and public health professionals to analyze cause of death trends at the specific cause level. It will be especially important to pay particular attention to the specific MCOD conditions reported on the death certificate rather than solely relying on the 113 selected cause of death groupings. Lifting the shroud on important differences in comorbidities can inform resource allocation and health policy decisions.
By integrating disability into every aspect of how we observe and identify health disparities, a disability data justice approach will help to mitigate the influence of structural ableism on our understanding of health differences between adults with and without Down syndrome. It is important not to assume that data from the general population are representative of all individuals in the population. Our findings suggest that normative assumptions are not sufficient to describe cause of death patterns for all individuals. A disability data justice approach requires moving beyond these assumptions and recognizing and documenting meaningful differences among individuals (Jain 2025; Lundberg and Chen 2024; Valdez and Swenor 2023). The findings of this study highlight the harms of relying on coding schemes that obscure meaningful differences in cause of death data. When disability is not accounted for in analytic strategies, structural ableism can be reinforced. Ensuring that disability is explicitly incorporated into medical sociology’s conceptualization of health and illness is essential for accurately observing health patterns across all subpopulations rather than just granting greater visibility to those without disabilities.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465261450455 – Supplemental material for Removing the Shroud: Revealing Cause of Death Patterns among Adults with Down Syndrome and Alzheimer’s Disease
Supplemental material, sj-docx-1-hsb-10.1177_00221465261450455 for Removing the Shroud: Revealing Cause of Death Patterns among Adults with Down Syndrome and Alzheimer’s Disease by Julia M. Finan, Scott D. Landes and Margaret A. Turk in Journal of Health and Social Behavior
Footnotes
Author Contributions
Julia M. Finan was a contributor to the conceptualization, data curation, formal analysis, investigation, methodology, visualization, writing of the original draft, and the review and editing of the manuscript. Scott D. Landes was a contributor to the conceptualization, data curation, funding acquisition, investigation, methodology, writing of the original draft, and the review and editing of the manuscript. Margaret A. Turk was a contributor to the conceptualization, methodology, writing of the original draft, and the review and editing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.