
Abstract
Sleep is a critical health behavior that often varies by gender, and most partnered adults sleep with a significant other. Despite growing research on sleep health, little is known about how daily sleep within couples shapes marital dynamics, especially across same- and different-sex relationships. This study uses dyadic diary data from 378 mid- to later-life couples in the United States (N = 756) to examine how respondents’ and partners’ daily sleep quality are each associated with daily marital strain and whether these associations vary by gender and couple type. Respondent sleep quality predicts lower marital strain for all couple types except for men married to women. Spousal sleep quality is also associated with reduced strain but only for women in different-sex marriages. These women appear uniquely affected by both their own and their partner’s sleep, highlighting the importance of dyadic and gender-relational perspectives in understanding links between sleep and relationship dynamics.
“Sleep divorce” has recently surged into headlines as a modern remedy for marital bliss. Media coverage suggests that sleeping apart can improve sex lives (Pearson 2025), rescue strained marriages (Beddington 2023; Khan 2025), and keep long-term relationships alive (Adams and Stanley 2024). Despite its popularity, most married individuals continue to share a bed. In the United States, 82% of partnered adults sleep in the same bed, and 60% sleep with a significant other (National Sleep Foundation 2013). This may help explain why, when disrupted, sleep becomes an important yet often overlooked source of tension in intimate relationships. Poor sleep is a significant public health concern, associated not only with cardiovascular, immune, and neurodegenerative conditions (Decker, Fischer, and Gunn 2022) but also with strained relationship functioning (Troxel et al. 2007).
Sleep is shaped not only by biological rhythms but also by the structure and demands of daily life. Parenting, employment, and caregiving significantly impact adults’ sleep health, particularly among women (Frazier and Brown 2023). Married women work less and thus may have more flexible sleep schedules, but their sleep is more likely to be interrupted due to nighttime caregiving and emotional labor (Burgard and Ailshire 2013; Maume, Hewitt, and Ruppanner 2018; Walker et al. 2012). This may, in turn, diminish relationship well-being by increasing daily strain and reducing emotional availability within the couple.
A growing body of research, particularly in psychology and health sciences, has examined how partners’ sleep affects marital quality and individual well-being (Andre, Lovallo, and Spencer 2021; Gunn et al. 2015; Troxel 2010; Troxel et al. 2007). For example, a recent study found that poor sleep quality predicted more negative partner interactions for both partners (Xie, Lemay, and Feeney 2025), whereas others find notable gender differences, with only women reporting more positive marital interactions following nights of better sleep quality (Yorgason et al. 2018). However, most of this research is based on small or community samples of exclusively different-sex couples. Given sleep’s gendered patterns and its clear implications for marriages, there is a need for more sociological research that centers the dyadic and relational dimensions of sleep, especially across diverse couple types.
Same-sex marriages offer a relational context to understand how gender shapes sleep and marital dynamics. Sexual-minority individuals tend to experience more sleep problems than the heterosexual population (Chum, Nielsen, and Teo 2021; Dai and Hao 2019); however, we know very little about how sleep influences the quality of same-sex marriages. The gendered dynamics may likely vary for same-sex and different-sex couples, while at the same time, stressors unique to sexual-minority couples may introduce burdens that complicate these patterns. Examining these dynamics across a broader range of couple types can shed light on how gender operates within and across relationship contexts.
To add to the literature, we work from the gender-as-relational perspective to examine how sleep shapes marital dynamics in same- and different-sex marriages. This approach suggests that men and women may “do” gender differently depending on whether they are interacting with a man or a woman in their relationship (Connell 2012; Springer, Hankivsky, and Bates 2012). Prior research comparing diverse couple types, for instance, finds that daily marital strain is linked to poorer well-being for all spouses, especially so for women married to men (Garcia and Umberson 2019). Thus, gender effects vary by the gender compositions of the couples. We use 10 days of dyadic diary data (N = 378 couples; N = 756 individuals) to examine (1) whether respondent and spousal daily sleep quality are associated with respondents’ daily marital strain and (2) how these associations vary by gender (men and women) and by gender compositions of marriages (i.e., same-sex and different-sex).
Background
Sleep as a Social and Shared Experience in Marriages
Sleep is often viewed as a biological necessity, but it is also a social and shared behavior, particularly in the context of marriage. Scholars increasingly recognize sleep as a socially embedded practice, even calling it “a time of social interaction” (Meadows 2005:240). Sleep is rarely solitary; it is organized around gendered expectations and work–family obligations and the rhythms of shared life (Ailshire and Burgard 2012). Adults’ sleep behaviors change as they age, and those in midlife who are employed and care for others experience diminished sleep (Frazier and Brown 2023). As a form of periodic remission, sleep restores individuals from daily pressures (Schwartz 1970). When compromised, managing daily life becomes overwhelming and marital relationships can suffer.
Sleep as a shared experience, then, has tremendous implications for marriage and health (Chen, Waite, and Lauderdale 2015; Waite and Gallagher 2001). Married individuals sleep alongside their spouses, and sleep disturbances often co-occur with relationship problems (Rosenblatt 2006). A growing body of interdisciplinary research has shown that sleep is interdependent across partners and closely tied to both individual well-being and relationship functioning. Daily marital interactions likely shape sleep experiences, which in turn may affect how couples engage with one another the next day (Troxel 2010; Troxel et al. 2007).
Evidence from small samples of different-sex couples suggests that poor sleep may contribute to more negative partner interactions (Gordon and Chen 2014; Hasler and Troxel 2010; Yorgason et al. 2018). In a study of 29 couples, men who experienced uninterrupted sleep reported fewer negative partner interactions the next day, such as feeling let down or disappointed by their spouse. This effect was not observed for women, suggesting greater interpersonal resilience or emotional regulation despite poor sleep (Hasler and Troxel 2010). In another study of 191 older couples, women reported more positive marital interactions and higher satisfaction after nights of better sleep, whereas better sleep quality but not duration was linked to greater marital satisfaction for men (Yorgason et al. 2018).
Other studies highlight how sleep affects not only the individual but also their partner. One study of early-stage couples found that poor sleep increased next-day conflict frequency and reduced empathic accuracy, the ability to understand one another during conflict, for both partners (Gordon and Chen 2014). Another recent study of 238 long-married adults found that poor sleep quality predicted more negative and fewer positive partner interactions the following day for both partners, with no gender differences (Xie et al. 2025).
Taken together, prior studies provide mixed evidence on the relationship between sleep quality and next-day relationship dynamics. Much of this rich work relies on relatively small, heterosexual samples, limiting our understanding of whether these patterns generalize across different couple contexts. However, the findings also point to meaningful asymmetries by gender and suggest the presence of dyadic effects, both of which warrant further investigation across more diverse couple types. The present study builds on this work by examining how daily sleep quality is associated with marital strain and whether these associations differ for men and women in same- and different-sex marriages using dyadic diary data from a large and diverse sample of couples.
Gendered and Relational Contexts of Sleep Quality
Women negotiate their time around work–family, often prioritizing their partner’s and children’s sleep over their own (Hislop and Arber 2003; Maume and Ruppanner 2017; Meadows 2005). Women’s sleep, already walking a tightrope, is usually disrupted, particularly in different-sex couples, where work–family demands are unevenly distributed (Frazier and Brown 2022; Hislop and Arber 2003; Venn et al. 2008). Broader cultural norms around sleep further disadvantage women. Men tend to devalue sleep as a biological necessity for productivity and may not recognize how their poor sleep may affect their partners (Meadows et al. 2008). Furthermore, men may move more frequently during sleep, leading to sleep disturbances for women (Andre et al. 2021; Pankhurst and Home 1994). These factors may increase sleep-related marital strain for women in different-sex relationships.
We also expect sleep quality and marital strain to vary by couple type. The gender-as-relational perspective conceptualizes gender as a dynamic and relational process shaped by interactions between partners (Connell 2012; Springer et al. 2012; Umberson et al. 2015). This approach moves beyond static gender roles and instead emphasizes that gender is constructed within the context of relationships. Prior research using this framework shows that women in same-gender relationships reported receiving more positive support and fewer unsupportive responses from their partners than women in different-gender relationships (Wang and Umberson 2023). One study found that daily marital strain undermined the well-being of women and men in both same-sex and different-sex couples, but the association was stronger for women married to men (Garcia and Umberson 2019). These findings point to the importance of the gender composition of the couple.
The gender-as-relational perspective is a useful lens to understand sleep, a behavior that is both relational and gendered and may vary depending on whether individuals are partnered with someone of the same or different gender. Compared to different-sex couples, same-sex couples may have more similar sleep patterns or a more equal gender division of labor, which is likely to shape their marital outcomes. First, women generally move less during sleep, and this reduces sleep disruption for their partners (Dittami et al. 2007). Similarly, men in same-sex couples may benefit from improved sleep quality because men tend to wake less frequently than women (Andre et al. 2021; Pankhurst and Home 1994).
There is also some evidence that health behaviors among same-sex couples are more concordant than among different-sex couples, including behaviors such as smoking or drinking (Holway, Umberson, and Donnelly 2018). Because such behaviors are known to affect sleep quality and duration, greater alignment may create more favorable conditions for shared sleep. As a result, same-sex couples may experience better sleep quality when sharing a bed with their partners (Andre et al. 2021), potentially leading to a weaker link between sleep quality and marital strain.
Moreover, the collaborative approach to caregiving that characterizes many same-sex relationships, especially in contrast to the gendered imbalances common in different-sex couples, may help buffer marital conflict and negative communication stemming from poor sleep. Egalitarian approaches to caregiving in same-sex relationships compared to those in different-sex relationships may offer relief from the cognitive and emotional toll that accumulates before bedtime (Downing and Goldberg 2011; Goldberg, Smith, and Perry-Jenkins 2012). Same-sex partners tend to engage in more equal and effective forms of dyadic coping when confronting daily or health-related stressors. For example, long-term same-sex spouses often take an active role in each other’s health management, such as reminding a partner about medical appointments or accompanying them to visits (Reczek et al. 2018). They also work together to address problems and provide mutual emotional responses, coping strategies shown to mitigate the adverse effects of stressors on relationship quality (Wang and Umberson 2023).
Yet same-sex couples may face individual- and couple-level minority stress that puts them at higher risks of poor sleep (Chen and Shiu 2017; Dai and Hao 2019; Fredriksen-Goldsen et al. 2017; McKay et al. 2023; Patterson and Potter 2019) and relationship strains (LeBlanc, Frost, and Wight 2015). Individual-level minority stressors, such as experiences of discrimination, fear of stigmatization, identity concealment, and internalized homophobia, contribute to mental health burden for the sexual-minority population (Baams, Bos, and Jonas 2014; Cao et al. 2017; Frost and Meyer 2009; Hsu and Mernitz 2024, 2026; Meyer 1995, 2003; Puckett et al. 2015). Same-sex couples can also experience couple-level stressors, such as relationship invalidation and stigma, which are linked to lower relationship quality and mental well-being (LeBlanc and Frost 2020). This may have great implications for same-sex couples’ sleep and marital strain. Minority stressors are associated with increased sleep disturbances, often through heightened levels of stress and generalized anxiety (Gibbs and Fusco 2023). Women in same-sex relationships report similar sleep duration but feel less rested after seven hours of sleep compared to women in different-sex relationships; no differences were observed among men (Martin-Storey, Prickett, and Crosnoe 2018). Poor sleep may thus have a disproportionately large impact on relationship functioning in same-sex couples because they occur within a broader context of individual- and couple-level minority stress.
The Present Study
Building on prior evidence, we first expect both respondents’ and spouses’ better sleep to be associated with lower levels of respondent marital strain. Prior studies discussed previously have shown mixed results regarding gender differences in this association. Thus, we continue to explore the gender difference. We expect the association between sleep quality and marital strain to be stronger for women married to men than other couple types because they are expected to take up the caring responsibilities, and their spouses may not provide sufficient care when they are sleep deprived for stress, childcare, or other family- and work-related reasons.
We also expect the association between spousal sleep quality and marital strain to be stronger for women married to men than other couple types because they are expected to be more attuned to their partners’ needs (Rao 2017; Umberson et al. 2020) and thus may be more affected by their spouse’s sleep quality.
Working from the gender-as-relational perspective, same-sex couples may benefit from greater concordance in sleep behaviors and a more egalitarian approach to family and work responsibilities and how they cope with stressful daily events in more collaborative ways. Their collaborative approach may buffer the adverse effects of inadequate sleep on marital strain for same-sex couples. Therefore, we expect the negative association between sleep quality and marital strain to be weaker for same-sex couples, especially when compared to women in different-sex marriages. The minority stress perspective, however, provides a different prediction. Chronic minority stressors can compromise both sleep quality and relationship functioning, potentially magnifying the adverse effects of poor sleep on marital strain. We extend these expectations to both respondent and spousal sleep quality, anticipating similar patterns in how each partner’s sleep may shape marital strain across couple types.
Data and Methods
Sample
This study utilized publicly available data from the Health and Relationships Project (HARP), a study of how marital dynamics influence health and well-being among midlife U.S. women and men in long-term same-sex and different-sex marriages (Umberson 2022; N = 419 couples). HARP was designed to advance understanding of how gender and couple type shape relationship processes and health outcomes during midlife (ages 35–65), a life stage characterized by accumulated relationship histories and increasing health risks. All study procedures were approved by the Institutional Review Board at the University of Texas at Austin.
Sample recruitment happened between October 2014 and September 2015. Initially, Massachusetts vital records were used to identify gay and lesbian couples who met the age requirements and had been married between 2004 and 2012. These couples were invited via mail. Massachusetts was selected as the research site because it was the first U.S. state to legalize same-sex marriage in 2004, which facilitated access to a sizable population of legally married gay and lesbian couples. Participating couples were also asked to refer both same-sex and different-sex couples from their social networks with no geographic restrictions. Additional different-sex couples were recruited via mailings to areas with large numbers of same-sex participants, identified using publicly available city-level demographic data.
Approximately 70% of same-sex couples were recruited from vital records and 30% via referrals; about two-thirds of different-sex couples were recruited through referrals. Although recruitment began in Massachusetts, a substantial proportion of participants lived in other U.S. states at the time of data collection (55% of gay couples, 62% of lesbian couples, and 51% of different-sex couples). Of the 419 couples initially recruited, 415 completed the baseline survey and were included in the analytic sample. The sampling procedure was designed to make married same- and different-sex couples comparable with respect to relationship length, age, and geographic location.
The resulting sample of 415 couples (168 female same-sex, 123 male same-sex, and 124 different-sex couples) was not nationally representative; however, the demographic characteristics of the sample were consistent with nationally representative data comparing same-sex and different-sex spouses in midlife on several key characteristics (Behler, Donnelly, and Umberson 2019; Gates 2014, 2015). For example, comparisons with 2015 American Community Survey data for married midlife couples (ages 35–65) showed that the HARP sample matched national averages on age, household income, and the presence of children under 18 (Behler et al. 2019). The sample was more highly educated and less racially and ethnically diverse than the general population; however, relative differences across couple types mirrored national trends, with same-sex couples more likely to be highly educated and less likely to include racial or ethnic minorities than their different-sex counterparts (Behler et al. 2019).
Data for the present analyses came from two components of HARP: a baseline survey and a 10-day daily diary study. After completing the baseline survey, each couple selected a convenient period to complete the diary portion together. All questionnaires were completed online, with each spouse responding separately. The baseline survey took approximately 45 minutes, and the diary entries took 5 minutes to 10 minutes per day. Each respondent received a $50 gift card as compensation for completing the survey. To be included in the analytic sample, both spouses were required to complete at least 6 of the 10 daily diary entries; 90% completed all 10 days. The final analytic sample comprised 378 couples (N = 756 individuals), including 106 male same-sex, 157 female same-sex, and 115 different-sex couples.
Measures
Dependent variable
Marital strain (respondent) was measured using four daily diary items adapted from previous measures assessing strain in relationships (House 2018). The respondents were asked: “Over the past 24 hours, how much did your spouse (1) let you down and (2) act inconsiderate towards you?” and “Over the past 24 hours, how much did you (3) feel bothered or upset with your spouse and (4) want your spouse to listen to you more than they did?” Response options ranged from 1 (not at all) to 5 (a great deal). Responses to each item were averaged to form a composite daily marital score, with higher values indicating higher strain (range = 1–5, α = .78). Only five cases (.07%) were missing. We imputed them using each respondent’s mean across nonmissing diary days. Results were unchanged when we excluded these (available on request).
Independent variables
Daily sleep quality was assessed each day by asking participants, “How would you rate your overall sleep quality last night?” Answers ranged from 1 (poor) to 5 (excellent), with higher scores indicating better sleep quality. Only nine cases (.12%) were missing and were imputed using each person’s mean across diary days. Results remained consistent when these cases were excluded (available on request).
Because sleep quality can vary both between individuals and within individuals across 10 days, we used person-mean centering to isolate the association between daily fluctuations in sleep quality and marital strain, minimizing the influence of stable, between-person differences (e.g., chronic sleep disorders; Allison 2005; Bolger and Laurenceau 2013). Similarly, we included each respondent’s grand-mean-centered person average to account for between-subject variation.
Covariates
We controlled for factors that may be associated with both sleep quality and marital strain. Respondent’s daily sleep duration was independently reported by each spouse and was measured in self-reported hours (range = 0–13, top-coded). Including sleep duration allowed us to examine whether it was the amount of sleep, the perceived quality, or both that drove variations in marital strain. There was a moderate between-person correlation between sleep duration and sleep quality (r = .43); although these two measures were related, they captured distinct dimensions of individuals’ sleep experiences.
We included a daily stress measure derived from seven questions adapted from the Daily Inventory of Stressful Events (Almeida, Wethington, and Kessler 2002), capturing both the frequency and severity of nonmarital stressors. Respondents were asked whether in the past 24 hours, they had (1) an argument or disagreement with someone other than their spouse, (2) experienced another stressful event, (3) faced housework or home demands, (4) encountered work demands, (5) experienced financial concerns, (6) had a health problem, or (7) reported that their spouse experienced a problem or difficulty (coded 1 = yes). Respondents also rated how stressful the events were on a scale from 1 (not at all stressful) to 5 (extremely stressful) if they answered yes to any of the stressors. If no event occurred, the stress rating was coded as zero. Responses were averaged and standardized to form a composite daily stress score (α = .81).
We also controlled for time-invariant demographic and relationship characteristics from the baseline survey, including respondent age (in years), education (college degree or higher vs. less), and employment status (currently working vs. not). Relationship duration measures the total number of years the couple has lived together, accounting for differences in legal access to marriage among same-sex couples. The number of children under age six in the household was measured as a continuous variable (range = 0–4; M = .49, SD = .87). Given the midlife age range of the sample, most participants had no young children, but variation was retained to capture differences in caregiving demands across couple types. Race-ethnicity was included as a binary indicator (non-Hispanic White vs. all other racial-ethnic groups) due to small cell sizes when cross-classified by gender and couple type. The full sample was 86% non-Hispanic White, 4% Black, 4% Hispanic, 3% Asian, <1% Native American, 2% multiracial, and 1% other. Finally, we controlled for diary day (1–10) to account for temporal variation across the 10-day study period.
Analytic Strategy
To examine variation in daily sleep quality and marital strain the next day across same-sex and different-sex couples, we employed the factorial method (Kroeger and Powers 2019; West, Popp, and Kenny 2008), an extension of the actor-partner interdependence model, via mixed-effects multilevel modeling with crossed random effects (mixed in STATA). This approach combined fixed and random effects to assess between-person differences in sleep quality on marital strain while accounting for the nested structure of dyadic diary data. This way, the modeling strategy allowed random variation at both dyad and day levels (Bolger and Laurenceau 2013). The factorial method allowed us to assess three gender effects: (1) respondent gender, (2) spouse gender, and (3) the interaction between respondent gender and spouse gender (i.e., whether one is in a same- or different-sex marriage).
We estimated a series of interaction models, each assessing a gender effect on the marital strain intercept, and the final model included a three-way interaction among respondent gender, spouse gender, and sleep quality. These models were run separately for respondent and spousal sleep quality to explore how the gender of the respondent, the gender of their spouse, and the gendered relational context of the marriage may have affected the association between respondent and spousal sleep quality and marital strain. Estimates were then used to calculate predicted coefficients for the association of daily sleep quality with marital strain. Postestimation pairwise comparisons tested differences across four union types: (1) men married to men, (2) men married to women, (3) women married to men, and (4) women married to women. All analyses were conducted using STATA (Version 18.0).
Results
Descriptive Results
Table 1 summarizes the descriptive characteristics of the sample. On average, the respondents are 48 years old, with relationships averaging 15 years. Over half of the sample held a postgraduate degree (50.8%). Racial and ethnic diversity is limited, with only 14.8% of respondents identifying as non-White. Over 80% of respondents are employed outside the home. There is variation in the presence of children in the household, with 61% of individuals in different-sex marriages reporting children compared to 12% of men married to men and 38% of women married to women.
Descriptive Statistics by Gender Composition of the Couple (N = 756 Individuals; N = 378 Couples), Health and Relationships Project, 2014–2015.
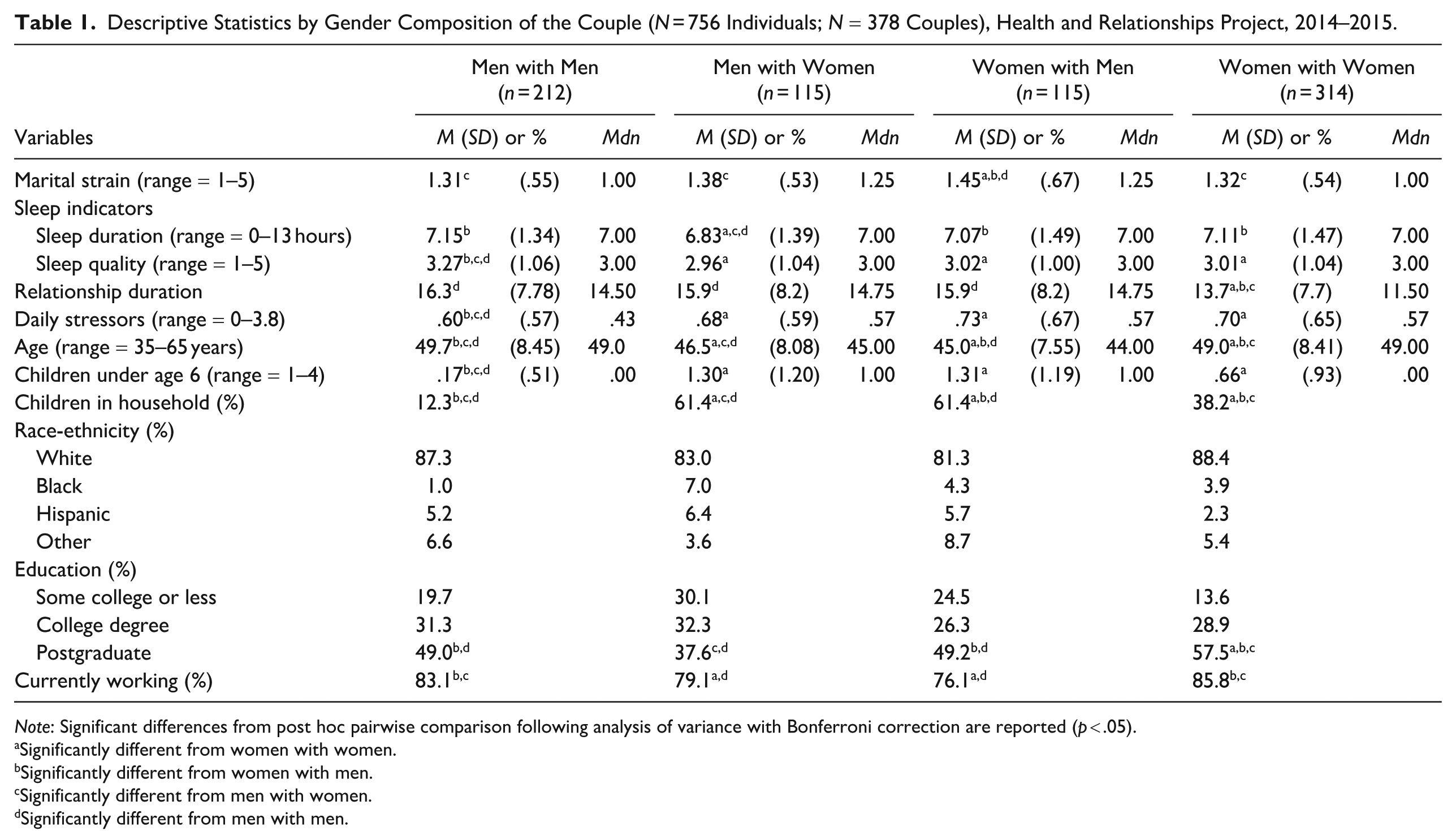
Note: Significant differences from post hoc pairwise comparison following analysis of variance with Bonferroni correction are reported (p < .05).
Significantly different from women with women.
Significantly different from women with men.
Significantly different from men with women.
Significantly different from men with men.
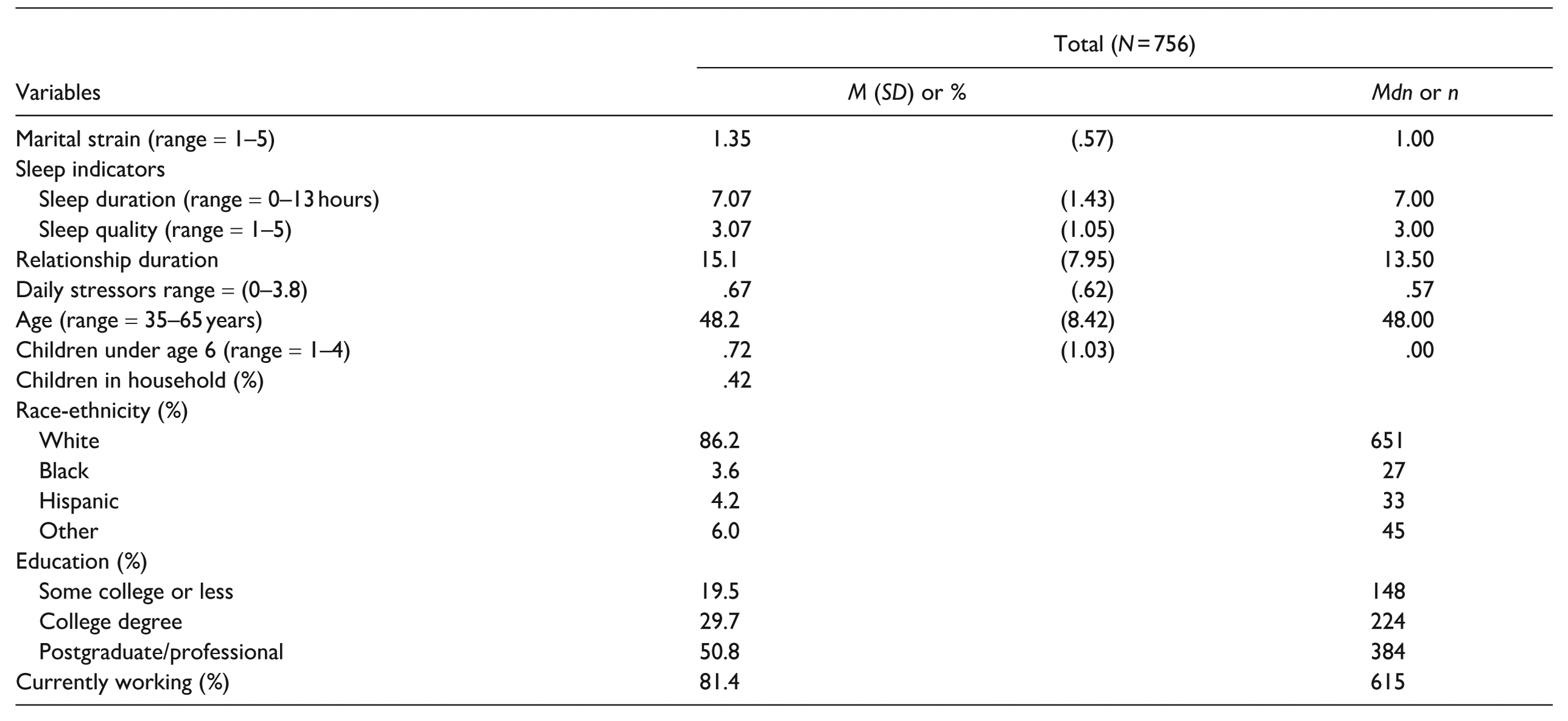
The average marital strain for the whole sample was 1.35 (range = 1–5). Daily sleep quality averaged 3.07 (range = 1–5). Daily sleep duration was 7.1 hours. Daily stressors are, on average, .67 (range = 0–3.80). To explore the significant differences among the four groups, we performed post hoc pairwise comparisons using analysis of variance with the Bonferroni correction. Results show that women married to men reported significantly more daily marital strain than all other groups (1.45). Men married to men reported significantly better sleep quality than the other groups (3.27). Men married to women reported sleeping significantly less than the other three marital groups (6.8 hours). Men married to men reported significantly fewer daily stressors than the other three marital groups (.60).
Association between Daily Sleep Quality and Daily Marital Strain across Same-Sex and Different-Sex Couples
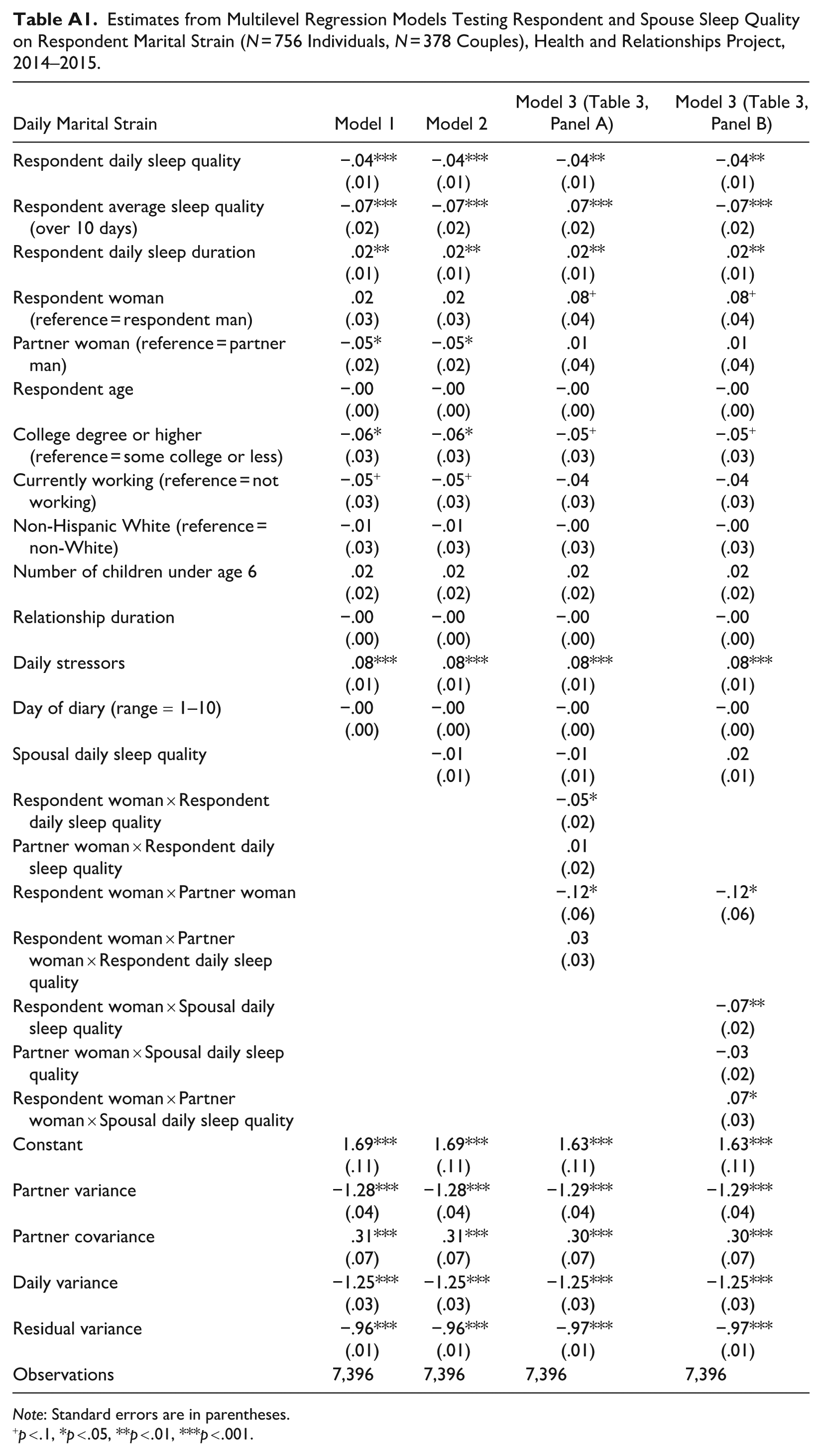
We examine how the respondent’s and the spouse’s daily sleep quality were associated with the respondent’s marital strain (Table 2), adjusting for the respondent’s sleep duration and daily stressors. The multilevel regression results from Model 1 reveal clear baseline patterns: Better daily sleep quality is linked to lower marital strain (b = −.04, p < .001), and better sleep quality on average across days predicts lower overall strain (b = −.07, p < .001), holding other factors constant. Additionally, sleep duration had a weak positive association with marital strain (b = .01, p < .05), and daily stressors show a strong positive association with marital strain (b = .08, p < .001). Respondents married to women report significantly lower marital strain than those married to men (b = −.05, p < .05) net of individual and relationship characteristics.
Estimates from Multilevel Regression Models Testing Respondent- and Spouse-Reported Daily Sleep Quality on Respondent Marital Strain (N = 756 Individuals, N = 378 Couples), Health and Relationships Project, 2014–2015.
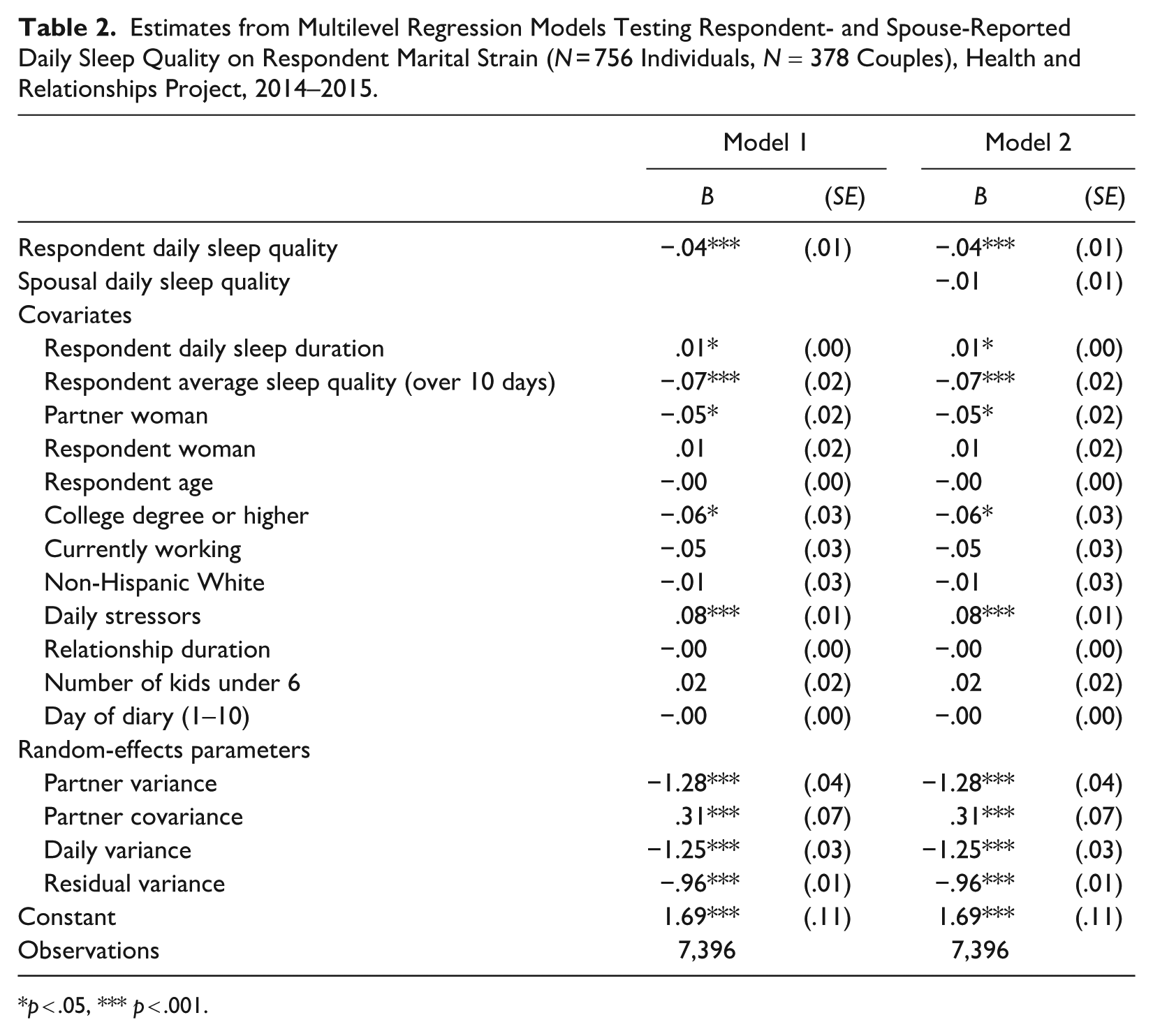
p < .05, *** p < .001.
In Model 2, the association between the respondent’s own sleep quality and marital strain remains significant after we fitted spousal sleep quality. However, the link between spousal sleep quality and marital strain is not statistically significant. Overall, these findings indicate that Hypothesis 1 was partially supported, with respondent sleep quality significantly associated with reduced marital strain.
Gender Differences in the Role of Daily Sleep Quality
Next, we examined whether the associations between respondent and spousal daily sleep quality and marital strain vary by union type (Table 3). Model 3 determines whether these associations were moderated by respondent gender, spouse gender, and the interaction of respondent sleep quality (Table 3, Panel A) and spousal sleep quality (Table 3, Panel B).
Estimates from Multilevel Regression Models Testing Respondent and Spouse Daily Sleep Quality on Respondent Marital Strain (N = 756 Individuals, N = 378 couples), Health and Relationships Project, 2014–2015.
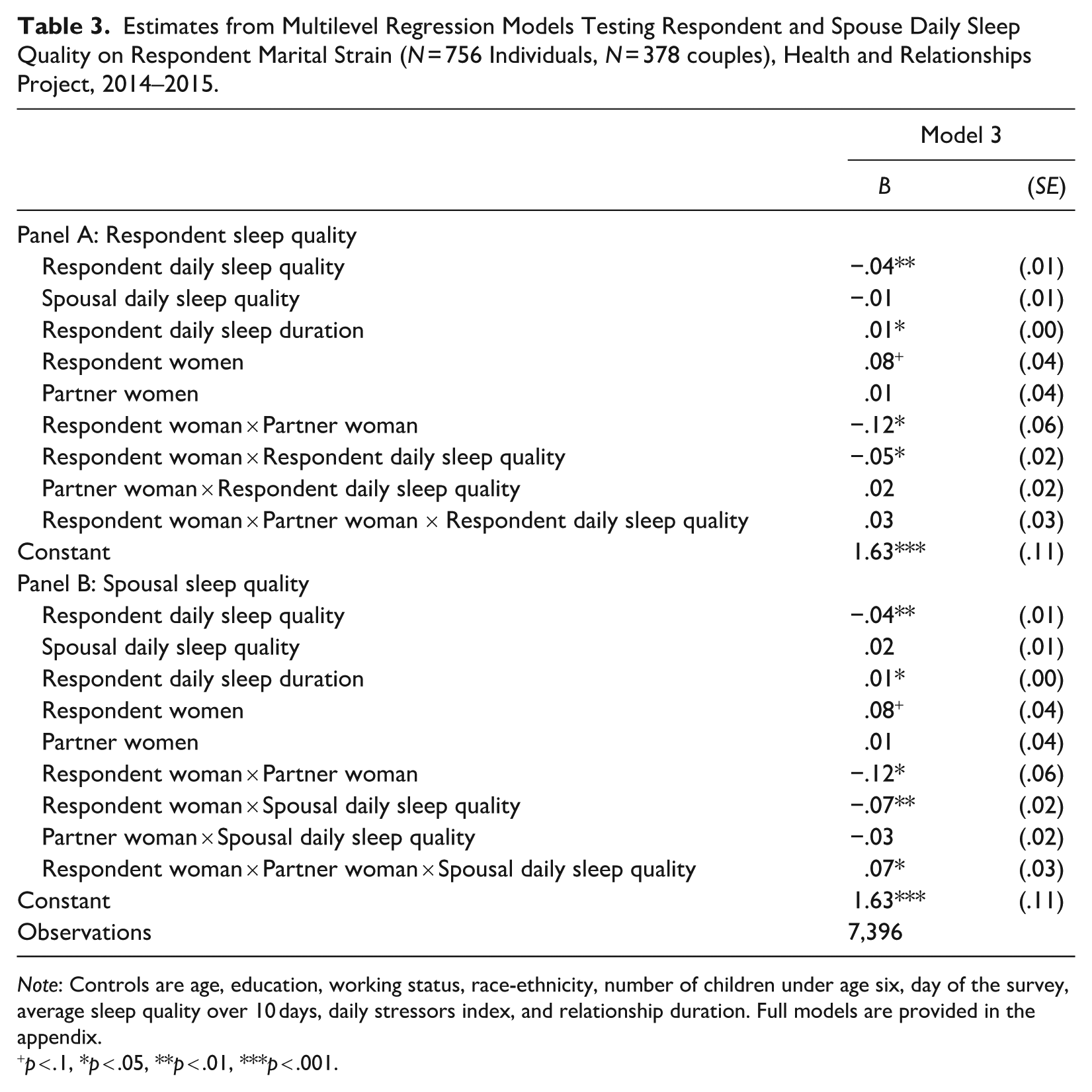
Note: Controls are age, education, working status, race-ethnicity, number of children under age six, day of the survey, average sleep quality over 10 days, daily stressors index, and relationship duration. Full models are provided in the appendix.
p < .1, *p < .05, **p < .01, ***p < .001.
Respondent sleep quality
In Model 3, a series of interaction terms were added. Here, men married to men serve as the reference category for union groups. The main effect of respondent sleep quality applies to them (b = −.04, p < .01), and all comparisons are made accordingly. The significant interaction between respondent gender and sleep quality indicated a stronger association between sleep quality and marital strain for women married to men compared to men married to men (b = −.05, p < .05). The nonsignificant interaction between spouse gender and respondent sleep quality suggests that the effect was similar for men in same- and different-sex couples. The nonsignificant three-way interaction between respondent gender, spouse gender, and respondent sleep quality indicates that a dyadic gender effect did not exist. That is, couple gender composition (i.e., same- vs. different-sex) did not illustrate the variation. Thus, although gender matters, it is the respondent’s gender rather than the couple’s gender configuration that drives the observed differences.
We visualized the results of Model 3 (Table 3, Panel A) in Figure 1, with the estimated coefficients for the association between respondent sleep quality and marital strain across four union types. The association was significantly negative for all groups except men married to women, and magnitudes varied. It was strongest for women married to men (b = −.08, p < .001), followed by men married to men (b = −.04, p < .01) and women married to women (b = −.03, p < .01). Postestimation pairwise comparisons confirmed that the daily sleep and marital strain link was significantly stronger for women married to men compared to all other groups. These contrasts are also visualized in Figure 1 by gender and couple type.
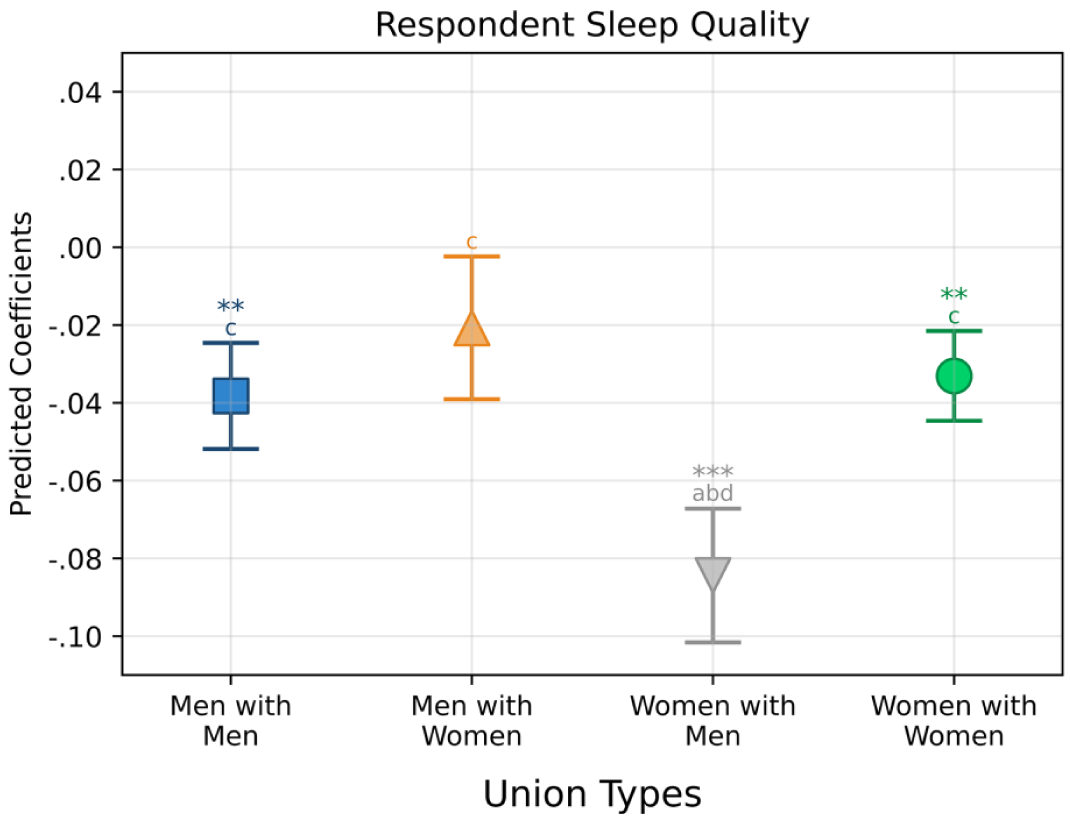
Adjusted Predicted Coefficients for the Association of Respondent Daily Sleep Quality with Marital Strain by Union Types (N = 756), Health and Relationships Project, 2014–2015.
Predicted slopes based on Model 3 (Table 3, Panel A) are further illustrated in Figure 2. The slope for women married to men declines most sharply, indicating a strong link between better daily sleep and reduced marital strain. The slopes for men married to men and women married to women are also negative but less steep. The slope for men married to women is notably flatter, and the association is not statistically significant.
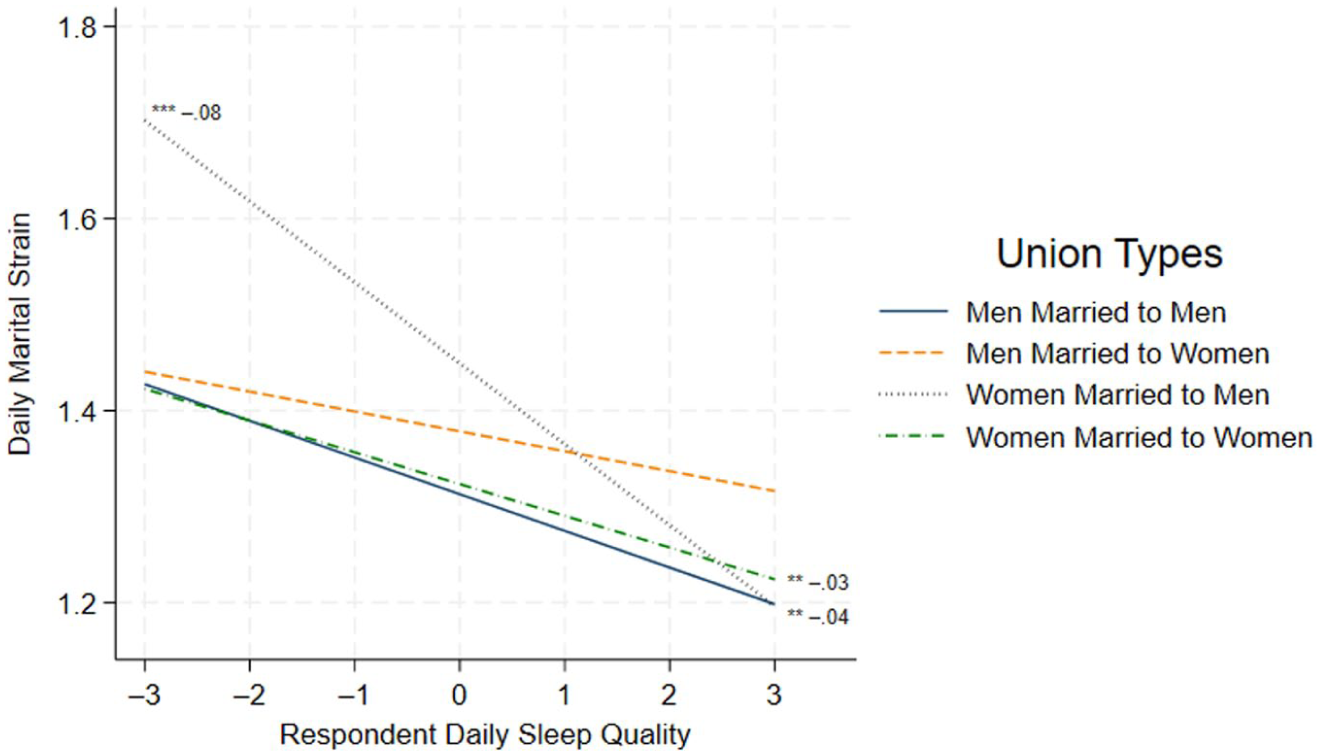
Estimated Effects of Respondent Daily Sleep Quality on Marital Strain (N = 756), Health and Relationship Project, 2014–2015.
These results strongly support Hypothesis 2a: The negative association between respondent sleep quality and marital strain is significantly stronger for women married to men than for men married to women. Furthermore, Hypothesis 3 was supported: The negative association between respondent sleep quality and marital strain varied significantly across couple types. Specifically, we found strong support for Hypothesis 3a: The negative association was significantly weaker for men and women in same-sex marriages than for women married to men, who showed a powerful association. However, we found no support for Hypothesis 3b.
Spousal sleep quality
In Table 3, Panel B, we examined whether spousal daily sleep quality predicted respondent marital strain. We first observed a significant interaction between respondent gender and spousal sleep quality (b = −.07, p < .01). This interaction indicates that the relationship was stronger for women married to men compared to men married to men. However, there is no strong evidence that the association is substantially stronger for women married to men than for men married to women, providing no support for Hypothesis 2b. Second, the significant three-way interaction among respondent gender, spouse gender, and spousal sleep quality indicates a dyadic gender effect (b = .07, p < .05), with associations varying by couple gender composition (i.e., same-sex vs. different-sex).
Figure 3 presents estimated coefficients from Model 3 (Table 3, Panel B), illustrating how better spousal daily sleep quality is associated with lower respondent marital strain across groups. The results indicated that the association of spousal sleep quality with marital strain was only significant for women in different-sex couples, and the association is stronger compared to men in same-sex marriages based on pairwise comparisons. Here, we conclude that our third hypothesis found partial support. We found that the negative, inverse association between spousal sleep quality and respondent marital strain varies significantly across couple types but only between men in same-sex marriages and women married to men. Thus, we conclude that we still found some support for Hypothesis 3a and no evidence for 3b in the spousal sleep quality case.
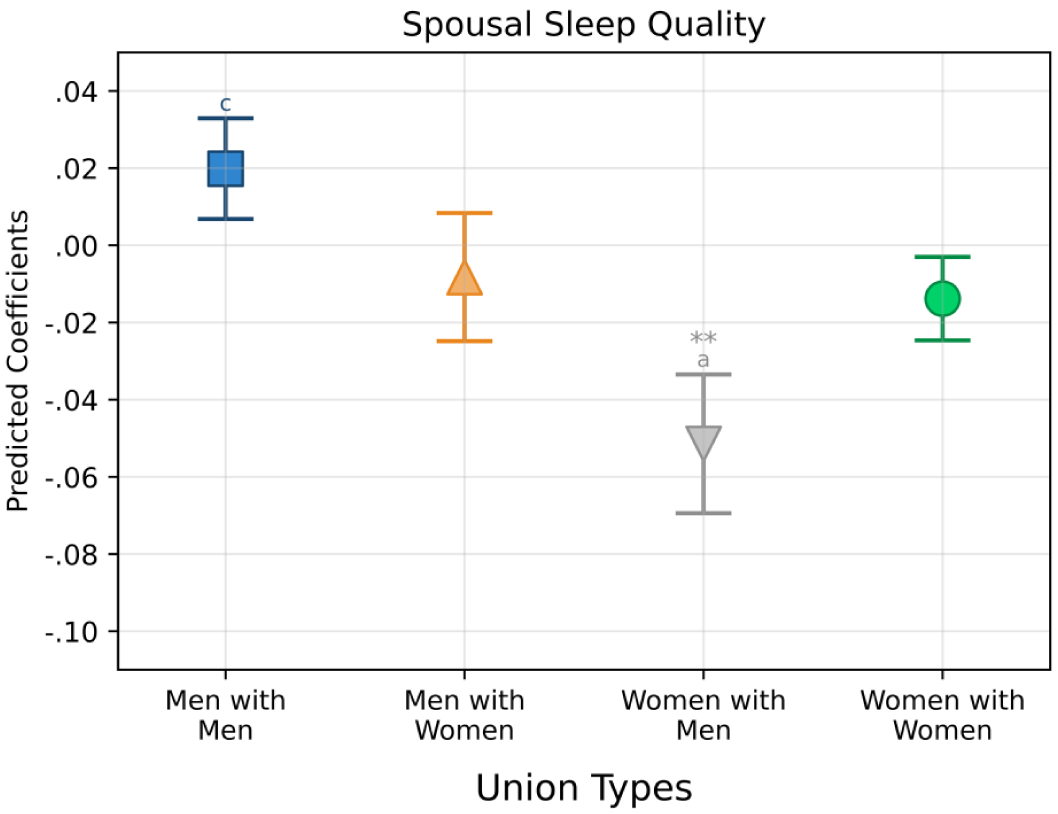
Adjusted Predicted Coefficient for the Association of Spousal Daily Sleep Quality with Marital Strain by Group (N = 756), Health and Relationships Project, 2014–2015.
We visualize results in Figure 4. The slope of the association between spousal sleep quality and marital strain is steepest for women with men, indicating that women may experience greater relief from marital strain when their partner sleeps well. By contrast, the solid line for men married to men slopes upward, yet the association is insignificant. Figures 2 and 4 both illustrate that women married to men report the highest levels of marital strain when partner experiences poor sleep quality. However, as sleep quality improves for both partners, differences in marital strain diminish.
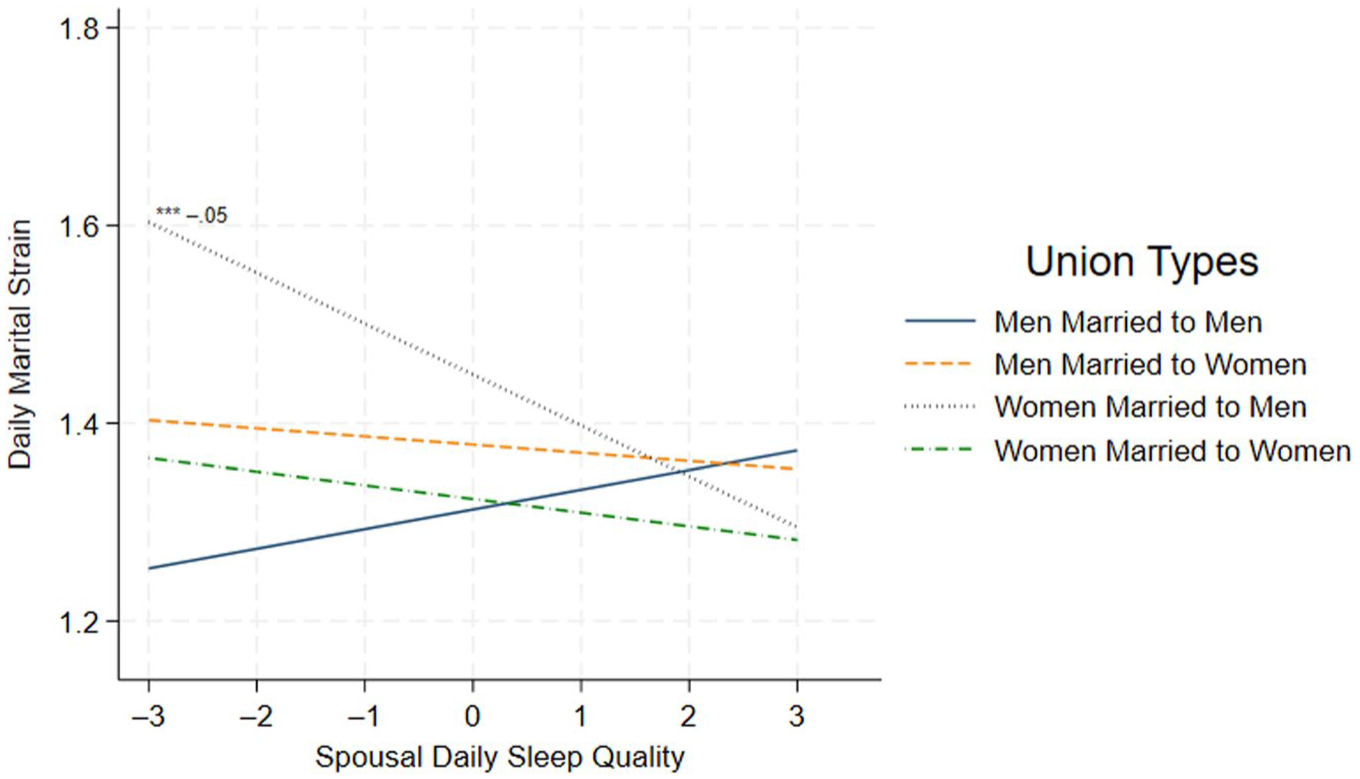
Estimated Effects of Spousal Daily Sleep Quality on Marital Strain (N = 756), Health and Relationship Project, 2014–2015.
Discussion
Sleep is a biological need, a health indicator, and a social behavior influenced by social patterns and demands of daily life. Marital relationships often serve as the primary context for individuals’ sleep experiences. Because many couples share a bed, their dynamics significantly impact sleep (Troxel et al. 2007) and, in turn, relationship outcomes (Hasler and Troxel 2010). Women’s sleep is often disrupted, particularly in different-sex couples, due to the gender-related responsibilities they face, such as transition to motherhood (Cavanagh and Saydam 2025; Frazier and Brown 2022; Hislop and Arber 2003; Venn et al. 2008). Most prior studies of sleep and relationship quality have focused exclusively on different-sex couples, leaving unanswered questions about whether these gendered sleep patterns also exist or vary within same-sex relationships. To contribute to this literature, this study examines sleep as a couple-level health behavior through the lens of a gender-as-relational framework (Springer et al. 2012; Thomeer, Umberson, and Reczek 2020). It explores how sleep shapes marital strain similarly or differently for men and women in same- and different-sex relationships. To the best of our knowledge, this is the first study to examine how sleep quality is associated with marital strain in same- and different-sex couples.
First, we find that daily sleep quality could play a role in shaping daily marital strain. Better sleep quality is consistently associated with lower marital strain among women and among individuals in same-sex marriages, supporting our Hypothesis 1, even after accounting for sleep duration and other covariates. However, this association does not hold for men married to women, suggesting that the benefits of restorative sleep for relational well-being may depend on gendered dynamics in different-sex marriages. Notably, at high levels of sleep quality, differences in marital strain across couple types diminish, indicating that good sleep benefits everyone and may buffer against relationship stress even among men in different-sex relationships. These results highlight that it is not merely the number of hours slept but also how restorative and satisfying that sleep feels that matters for relationship quality. Sleep quality is linked to couples’ capacity to regulate emotions, communicate effectively, and respond to stress, all of which are critical for daily communication and interactions in marriages but may operate differently across relationship contexts (Gordon and Chen 2014; Maranges and McNulty 2017; Marini et al. 2020). These findings support a growing body of research that positions sleep as a vital but often overlooked component of relationship health (Chen et al. 2015; Troxel et al. 2007; Xie et al. 2025).
Second, we find that the relationship between respondent sleep quality and respondent marital strain is more pronounced for women in different-sex relationships, supporting Hypothesis 2a. In other words, when women in a different-sex marriage report poor sleep quality, their levels of marital strain rise more sharply than those of individuals in other couple types. Poor sleep quality can impede an individual’s ability for both cognitive and emotional functioning on a daily basis (Mauss, Troy, and LeBourgeois 2013; Nebes et al. 2009), potentially giving rise to frustration and miscommunication. Compared to men or women in same-sex couples, women in different-sex marriages likely have fewer opportunities to compensate for or recover from disrupted sleep, reflecting enduring gender expectations that they maintain for the smooth functioning of family life.
Moreover, because the couples in our sample are in midlife, women in different-sex marriages often navigate an especially dense set of familial obligations, including paid work, childrearing, and caregiving for aging parents. This accumulation of responsibilities may heighten the impact of poor sleep on daily functioning and make sleep-related disruptions more likely to spill over into relationship strain (Arber et al. 2007; Frazier and Brown 2023). In this way, poor sleep or the lack of it may both reflect and reproduce gendered strains in intimate relationships, consistent with prior research linking sleep disruption to broader patterns of gender inequality (Burgard and Ailshire 2013; Frazier and Brown 2023; Hislop and Arber 2003; Maume et al. 2018).
Third, we also found that the associations between spousal sleep quality and marital strain were significant for women in different-sex relationships, consistent with spousal component of Hypothesis 1. This might suggest that women in different-sex marriages are more attuned to their partner’s sleep quality and daily stress. Prior research demonstrated that women are often the emotional and health care manager in the family (Reczek et al. 2018) and experience greater emotional reactivity (Garcia and Umberson 2019), and gendered expectations about caregiving make women in different-sex couples more attuned to signs of partner distress or well-being, such as sleep quality. This aligns with the cost of caring, where women often absorb the emotional burdens of those around them and are expected to manage and respond to others’ needs during times of family stress (Rao 2017; Taylor 2015; Thomeer, Reczek, and Umberson 2015). By contrast, the nonsignificant association for women in same-sex couples may point to greater mutual responsiveness, which could buffer the link between partner sleep quality and marital strain. These findings support the idea that gender composition shapes not only sleep quality but also how it is linked to relationship quality, highlighting a particular risk for women married to men. Still, these findings warrant further exploration in future research.
Finally, we also find that the pattern linking spousal sleep quality and marital strain among women in different-sex relationships contrasts significantly from the pattern observed for men in same-sex unions, offering partial support for Hypothesis 3a. When examining men in different- and same-sex marriages, we see no meaningful differences in the association between their own or their partner’s sleep quality and marital strain. Although we did not hypothesize specifically regarding men across couple types, the absence of results points to an important gap in the literature. It may be that the mechanisms linking sleep quality to relational strain operate differently for men or are less shaped by the gender composition of their relationship. Men may also be less emotionally reactive to their partners’ sleep, potentially because they view sleep in more functional terms rather than as a relational process (Meadows et al. 2008). These possibilities can be important directions for future research.
Limitations and Future Directions
There are some limitations to note. First, the results of this study cannot be generalized to the broader U.S. married population because the sample is relatively socioeconomically privileged, with most respondents being racialized as White, college-educated, cisgender, and middle-class. Therefore, the findings should be interpreted with caution. Second, in our analysis of sleep and marital strain, we only identify associations rather than making causal inferences. It may well be that couples who retain lower levels of marital strain have better sleep quality and sleep-sufficient nights (Chen et al. 2015; Hasler and Troxel 2010). Besides, the results mainly reflect day-to-day fluctuations among couples experiencing relatively low levels of strain. Future work could examine whether these patterns look different in samples with clinically elevated or chronic marital distress. Third, although our analyses focus on within-person changes in daily sleep quality, which help account for stable factors such as chronic sleep disorders, other unobserved characteristics, such as cosleeping arrangements and bedtime routines, may still influence the observed associations. We do not know whether partners share a bed or have aligned sleep schedules. Yet according to national data from the National Social Life, Health, & Aging Project almost 80% of married older adults sleep in the same bed (Lauderdale et al. 2014), and the absence of cosleeping information does not significantly affect the validity of the dyadic sleep measures (Chen 2017). In addition, although regional factors, such as time zone alignment, environmental conditions, and cost of living, may shape sleep and relationship dynamics, geographic identifiers were unavailable due to confidentiality restrictions. Future research can explore this direction further.
Sleep duration and time use may vary across weeks (Basner et al. 2007; Hale 2005; Mireku and Rodriguez 2021), and sleep quality may as well. We were unable to examine potential differences between weekdays and weekends in our data. Future research should aim to tease out these variations more clearly. Lastly, because sleep quality was reported retrospectively at the end of the day, responses may be subject to recall bias. Prior research suggests that longer recall periods are associated with greater recall bias and reduced data accuracy (te Braak et al. 2023). However, participants still completed each diary within a limited time window in order to remain in the study, which likely helped reduce recall bias.
Conclusion
This study contributes to the growing literature on sleep and marriage by applying the gender-as-relational perspective (Connell 2012; Springer et al. 2012) to examine the associations between sleep quality and marital strain across same- and different-sex couples. To our knowledge, this is the first study to compare these associations across couple types. Our findings demonstrate that sleep is not just an individual health behavior but also a dyadic experience shaped by individual gender and gendered contexts. In different-sex marriages, women appear particularly vulnerable to the effects of both their own and their partner’s poor sleep, highlighting how gendered expectations may amplify daily relationship strain.
Practices such as “sleep divorce” may serve as temporary or situational coping strategies for managing sleep-related relationship stress. However, these individualized solutions are unlikely to address more fundamental, structural inequalities that shape sleep itself and, by extension, relationship dynamics. In couples under a roof, sleep-related tensions may reflect broader imbalances in caregiving, household and emotional labor, and paid work that disproportionately burden women, particularly in different-sex relationships. These implications reiterate the necessity of addressing sleep as a gendered, relational process and emphasize the need for support in intimate relationships as a key to improving both sleep and relationship quality. Our study advances this perspective by emphasizing how gender and couple type shape sleep, positioning sleep not only as a health outcome but also a window into relational equity and emotional well-being.
Footnotes
Appendix
Estimates from Multilevel Regression Models Testing Respondent and Spouse Sleep Quality on Respondent Marital Strain (N = 756 Individuals, N = 378 Couples), Health and Relationships Project, 2014–2015.
| Daily Marital Strain | Model 1 | Model 2 | Model 3 (Table 3, Panel A) | Model 3 (Table 3, Panel B) |
|---|---|---|---|---|
| Respondent daily sleep quality | −.04***
(.01) |
−.04***
(.01) |
−.04**
(.01) |
−.04**
(.01) |
| Respondent average sleep quality (over 10 days) | −.07***
(.02) |
−.07***
(.02) |
.07***
(.02) |
−.07***
(.02) |
| Respondent daily sleep duration | .02**
(.01) |
.02**
(.01) |
.02**
(.01) |
.02**
(.01) |
| Respondent woman (reference = respondent man) | .02 (.03) |
.02 (.03) |
.08
+
(.04) |
.08
+
(.04) |
| Partner woman (reference = partner man) | −.05*
(.02) |
−.05*
(.02) |
.01 (.04) |
.01 (.04) |
| Respondent age | −.00 (.00) |
−.00 (.00) |
−.00 (.00) |
−.00 (.00) |
| College degree or higher (reference = some college or less) | −.06*
(.03) |
−.06*
(.03) |
−.05
+
(.03) |
−.05
+
(.03) |
| Currently working (reference = not working) | −.05
+
(.03) |
−.05
+
(.03) |
−.04 (.03) |
−.04 (.03) |
| Non-Hispanic White (reference = non-White) | −.01 (.03) |
−.01 (.03) |
−.00 (.03) |
−.00 (.03) |
| Number of children under age 6 | .02 (.02) |
.02 (.02) |
.02 (.02) |
.02 (.02) |
| Relationship duration | −.00 (.00) |
−.00 (.00) |
−.00 (.00) |
−.00 (.00) |
| Daily stressors | .08***
(.01) |
.08***
(.01) |
.08***
(.01) |
.08***
(.01) |
| Day of diary (range = 1–10) | −.00 (.00) |
−.00 (.00) |
−.00 (.00) |
−.00 (.00) |
| Spousal daily sleep quality | −.01 |
−.01 |
.02 |
|
| Respondent woman × Respondent daily sleep quality | −.05*
|
|||
| Partner woman × Respondent daily sleep quality | .01 |
|||
| Respondent woman × Partner woman | −.12*
|
−.12*
|
||
| Respondent woman × Partner woman × Respondent daily sleep quality | .03 |
|||
| Respondent woman × Spousal daily sleep quality | −.07**
|
|||
| Partner woman × Spousal daily sleep quality | −.03 |
|||
| Respondent woman × Partner woman × Spousal daily sleep quality | .07*
|
|||
| Constant | 1.69***
|
1.69***
|
1.63***
|
1.63***
|
| Partner variance | −1.28***
|
−1.28***
|
−1.29***
|
−1.29***
|
| Partner covariance | .31***
|
.31***
|
.30***
|
.30***
|
| Daily variance | −1.25***
|
−1.25***
|
−1.25***
|
−1.25***
|
| Residual variance | −.96***
|
−.96***
|
−.97***
|
−.97***
|
| Observations | 7,396 | 7,396 | 7,396 | 7,396 |
Note: Standard errors are in parentheses.
p < .1, *p < .05, **p < .01, ***p < .001.
Acknowledgements
We thank Kim McErlean, Mieke Beth Thomeer, Michael Garcia and Dan Powers for their helpful feedback on earlier versions of this article. We also thank our audience for their feedback at the Population Association of America 2025 Annual Conference. We are also grateful to Debra Umberson for her guidance and support.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institute on Aging of the National Institutes of Health (R37AG076057 and P30AG066614) and the Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant No. P2CHD042849), awarded to the Population Research Center at The University of Texas at Austin. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.