
Abstract
Citizen science with particulate matter sensors at home increases awareness of pollution exposures and can inform health-protective actions, yet little research explores the emotional dimensions of sensing, especially across economic divides. This study shows that participatory air quality sensing is not emotionally neutral. We included 26 parents of asthmatic children in 10 weeks of participatory sensing with indoor and outdoor sensors to understand their exposure experiences. Drawing from weekly surveys and postproject interviews, we found that sensors often generated positive emotions (e.g., empowered, happy) across income levels, underscoring their potential as inclusive tools for asthma management. Parents less often reported negative emotions (e.g., stress, worry); when they did, those were spurred from checking outdoor readings (versus indoor) because outdoor exposures were less controllable. Parents managed emotions by creating contingent boundaries between indoor and outdoor spaces. We recommend expanding access to sensors and air purifiers to promote individual-level environmental health benefits.
Fine particulate matter pollution (PM2.5; particles 2.5 micrometers in diameter or smaller) is a serious public health concern due to its ability to penetrate deeply into the lungs and bloodstream. This pollution poses significant health risks, particularly to the respiratory and cardiovascular systems (U.S. Environmental Protection Agency [U.S. EPA] 2016). Acute exposure to unhealthy levels of PM2.5 causes asthma attacks and hospitalizations (Beard et al. 2012; Pope et al. 2008). PM2.5 also disproportionately impacts the health and well-being of vulnerable populations, such as children and individuals with respiratory conditions (Brockmeyer and D’Angiulli 2016; Madaniyazi and Xerxes 2021).
Laypeople’s use of low-cost PM2.5 sensors at home has gained popularity. These sensors, valued for their ability to detect short-term pollution spikes and fluctuations throughout the day in specific places, empower individuals to monitor indoor and outdoor PM2.5 exposures (Hubbell et al. 2018). The sensors can be networked to allow online platforms, such as PurpleAir, to publicly display near real-time data visually on maps, helping both users and nonusers (i.e., anyone living near a publicly networked sensor) stay informed about their personal exposures. People use these exposure data to engage in health-protective actions, such as reducing time spent outdoors, ventilating indoor air (e.g., opening windows), or using air cleaning measures (e.g., air purifiers; Mullen et al. 2025; Wong-Parodi, Dias, and Taylor 2018). Although the sensors provide information that individuals can use to reduce their exposures, they are not a substitute for government regulations to improve air quality, nor do they address ambient air pollution at the source, such as from factories, refineries, and freeways.
The sensors provide valuable data, but research has yet to explore how using air quality sensors for health protection, such as asthma management, might lead to distinct emotional experiences—empowerment, gratitude, concern, or fear—particularly as individuals from diverse socioeconomic backgrounds engage with real-time exposure data. The emotional impact of air quality sensing may vary by socioeconomic status (SES). For lower SES individuals, gaining access to sensors may have a more transformative impact than for others because these tools may provide a novel sense of agency and empowerment. On the other hand, the use of sensors could inadvertently harm the emotional well-being of lower SES individuals by amplifying feelings of stress or helplessness regarding exposures beyond their control. Understanding the range of emotional impacts is important as researchers and communities increasingly engage in participatory air quality sensing as a form of citizen science.
In what follows, we first review the literature on emotions associated with parenting decisions regarding environmental health risks and caring for children with asthma before reviewing the nascent literature on emotional responses to sensor use. Next, we present our contribution and the framework informing our study’s motivation and design—the exposure experience. We then describe our data and methods and present the results. We discuss our findings on parents’ emotional experiences with participatory sensing before concluding with our recommendations to enhance asthma management with improved access to sensors and air purifiers.
Background
How Parents Manage Children’s Environmental Health Risks
MacKendrick’s (2018:4) concept of “precautionary consumption” is a useful consideration when it comes to understanding individual-level actions for mitigating environmental health risks. Precautionary consumption refers to how parents attempt to protect their families from exposures through careful, informed purchases and habits. This concept builds on Szasz’s (2007) “inverted quarantine,” which refers to a reliance on personalized risk reduction strategies—buying bottled water, organic food, and ecofriendly products—as opposed to collective action for systemic change. Szasz (2007) critiques the growing trend toward privatized, individualized, and depoliticized environmental protection. Precautionary consumption highlights the personal responsibility that parents—particularly mothers—face in managing children’s exposure to environmental risks through deliberate consumer choices. In addition to reinforcing gendered burdens of care, precautionary consumption reflects class privilege because unequal access to time, financial resources, and information limit low-SES parents’ ability to fully engage in this practice (MacKendrick 2018).
Even as precautionary consumption may offer higher-income parents a greater sense of empowerment and control over threats to their children’s health compared to lower-income parents, parents of any SES can feel emotional strain stemming from the pressure to protect children from exposures (MacKendrick 2018). The pressure falls most acutely, though, on those with the increased resources and social expectations to do so, whereas lower-income parents often recognize the limits of their control over environmental risks due to structural constraints (MacKendrick 2018). Although not focused on environmental exposures, Elliott, Powell, and Brenton (2015:352) offer an exception to this trend: The lower-income Black mothers in their study engaged in key tenets of “intensive mothering” (i.e., concentrated caregiving and emotional labor behind raising children associated with good mothering) while lacking the structural supports assumed by that approach. Parents—especially mothers—feel responsible for protecting children’s health, and when they fall short of meeting pervasive standards of mothering (including health-protective care and pro-environmental behaviors), they may experience guilt or a sense of failure (Cousins 2021; Elliott et al. 2015; MacKendrick 2018).
Although parents may aspire for full control and total risk avoidance, they often settle for partial, context-dependent strategies that reflect both personal agency and its limits. MacKendrick and Stevens (2016:324) introduce the concept of “contingent boundaries” to describe how adults managed feelings of control and vulnerability toward environmental chemical exposures by creating perceived boundaries of control that encompassed the home and trusted stores but did not extend to unfamiliar, less controllable places, such as public spaces or the outdoors. Participants characterized control within the latter as weak, elusive, and emotionally taxing, and some acknowledged that they ignored certain hazards to avoid being emotionally overwhelmed or anxiousness (MacKendrick and Stevens 2016).
The literature shows that internalized strategies for controlling exposures and protecting health contribute to a range of emotional responses. Our study builds from this by exploring how the emotional impacts of individualized efforts to reduce asthmatic children’s environmental exposures (i.e., PM2.5 pollution) with air sensing are experienced across different income groups.
Environmental Injustice and the Impacts of Caring for Children Who Have Asthma
Asthma has been framed as an environmental justice issue (Brown 2007; Grineski 2009) because lower-income and minority populations are disproportionately exposed to air pollution and its associated health risks (Collins et al. 2022; Mohai, Pellow, and Roberts 2009). Grineski (2009) investigated how parents with asthmatic children of varied SES backgrounds (specifically, low-income families in central city neighborhoods vs. affluent families in the Phoenix, Arizona, suburbs) attempted to minimize environmental hazards in their daily lives. All parents engaged in strategies to reduce exposures despite feeling helpless sometimes. The difference between them was that affluent parents had a greater capacity to alter their surroundings, whereas lower-income parents had limited control over both housing conditions and ambient hazards, such as proximity to landfills. This research sheds light on the ways in which experiencing environmental injustice and asthma caregiving intersect to produce unequal levels of control and subsequent asthma burden (Grineski 2009).
Children who have asthma require daily management, and caregiving is deeply emotional. Koenig and Chesla (2004) found that parents of young children with severe asthma experience a profound sense of personal responsibility and fears of failure, which shapes how they manage daily environmental exposures—mold, dust, pollen, and tobacco smoke—and their emotional state. When parents felt they had failed to manage their child’s asthma, they experienced feelings of self-blame, guilt, or anger (Koenig and Chesla 2004). Caregiving can produce emotional stress (i.e., negative psychological experiences, including anxiety, worry, and emotional burden) even when asthma is well controlled, especially for mothers who tend to carry the mental and physical load of asthma management (Avcil et al. 2019).
It is conceivable that caring for a child who has asthma intensifies parents’ emotional responses to the task of managing environmental exposures because caregivers often feel personally responsible for protecting their child’s health. As such, air sensors may either alleviate or heighten parental stress depending on the level of health-protective support that they offer. The emotional impacts of sensing are likely shaped by broader social conditions, such as low SES and unequal environmental exposures, that may constrain parents’ abilities to act on exposure data. Our study examines how parents caring for children with asthma emotionally respond to sensor data, revealing whether sensors can support emotional well-being across income groups.
Emotional Experiences with Participatory Air Quality Sensing
From the limited number of intervention studies describing participants’ emotions during participatory sensing, we know that people generally described their experiences as positive, especially when they were able to take steps to reduce their exposures (Boso et al. 2020; Heydon and Chakraborty 2020; Wong-Parodi et al. 2018). Matz, Wylie, and Kriesky’s (2017) participants used sensors to confirm suspicions that spikes in ambient air pollution caused their illnesses (e.g., headaches, dizziness, and nausea), suggesting that sensors have the potential to validate environmental health concerns. In deSouza’s (2022) analysis of product reviews for online purchases of low-cost sensors, they found that health management was a common motivation for acquiring these devices. Purchasers frequently praised the sensor devices for their health-protective benefits, expressing satisfaction with their decision to buy them and strongly recommending them to others with health concerns.
However, air quality sensing experiences are not uniformly positive. Studies suggest that engagement with air quality sensing increases perceptions that air quality is worse than previously assumed (Boso et al. 2020; Heydon and Chakraborty 2020). Heydon and Chakraborty (2020) documented how participants who initially assumed their indoor air was cleaner and healthier than outdoor air experienced a stark shift in perception when their sensors revealed that was not always the case. This discovery shattered participants’ “home-as-haven” perceptions (Heydon and Chakraborty 2020:12), a concept that resonates with Edelstein’s (2004:93) notion of “the inversion of home.” This describes how the home, traditionally interpreted as a secure and comforting space, can become associated with danger after learning about indoor contamination. This reversal amplifies distressing emotions, such as fear and insecurity. Additionally, Heydon and Chakraborty (2020) noted that participants who adjusted their behaviors based on portable sensor readings while outdoors—such as taking alternate routes or reducing vehicle idling—yet did not observe improvements in PM2.5 levels reported feelings of powerlessness. In some cases, this led participants to disengage from their efforts to reduce outdoor exposures.
These studies begin to shed light on the complex emotional dynamics of air quality sensing. Although sensors have the potential to foster empowerment by increasing awareness and improving health experiences, their emotional impact is not universally positive. Notably, none of these studies examined how SES shaped emotional experiences. Could the use of sensors among individuals in socially marginalized and environmentally burdened communities amplify negative emotional responses—such as stress or helplessness—when the exposures that they measure feel beyond their control? Moreover, could higher-income parents—with greater access to resources and mitigation options—experience a more empowering and actionable relationship with sensor data, thereby widening emotional and health disparities between SES groups? Gaining a better understanding of emotional responses could ensure that participatory sensing research and community-level interventions are more equitable and support the well-being of all participants, particularly those from vulnerable communities.
Contribution and Framework
Despite growing interest in participatory air quality sensing, few studies have examined how sensing is emotionally experienced by parents caring for asthmatic children across different income groups. To the best of our knowledge, our study is the first to address that gap by examining how citizen science technologies influence emotional well-being in socioeconomically diverse families managing asthma.
The exposure experience framework motivated our study design to understand how parents emotionally responded to sensor readings. Rooted in medical sociology, this framework explores how laypeople understand and respond to personal exposure information—through air, dust, and urine sampling—and how it reshapes their perceptions of the extent and sources of their exposures and the associated health impacts (Adams et al. 2011; Altman et al. 2008; Judge et al. 2016). It extends the concept of illness experience, which examines the complexities of living with disease, including its social and structural dimensions (Judge et al. 2016). The exposure experience connects lived experiences with illness and contamination from chemicals or pollutants to personal exposure science, such as biomonitoring or the measurement of exposure to chemicals and pollutants, usually in people’s homes or within their bodies (Altman et al. 2008).
Exposure experience research has traditionally involved a report-back or a process wherein researchers explain personal exposure results and exposure-reduction interventions to study participants that can elicit positive emotional responses for participants (e.g., grateful to be informed and empowered to act; Brody et al. 2014; Ohayon et al. 2017). Although participants in report-back studies receive guidance from researchers to help with understanding and intervention, ordinary sensor users lack formal support in interpreting the exposure data that they collect and often determine on their own how to reduce their exposures based on sensor readings. Given the hands-off approach of our participatory sensing study (methodology explained next), our findings lend valuable insights into how families independently process the exposure data while navigating chronic illness caregiving.
We enrolled 26 asthma-impacted families from different economic backgrounds in 10 weeks of participatory sensing, weekly surveys and postproject interviews. Our research questions ask the following:
Research Question 1: How do parents of children with asthma emotionally respond to participatory air quality sensing?
Research Question 2: How do these emotional responses differ by income?
Our findings reveal that emotional responses to air quality sensing may be shaped by access to resources, caregiving responsibilities, and boundaries of control, suggesting that sensors are more than simply informational devices.
Data and Methods
All parents gave their informed, written consent for inclusion before they participated in the study. The study protocol was approved by the Institutional Review Board of the University of Utah in June 2021. We use pseudonyms for all parents to protect their identity.
Case Study Area
Salt Lake County is Utah’s largest county by area and population. Although the population is predominantly White non-Hispanic/Latinx (69.80%), 30.20% of residents are racial-ethnic minorities, with the largest share being Hispanic/Latinx (U.S. Census Bureau [USCB] 2021). Persistent PM2.5 pollution problems and subsequent negative health impacts combined with an active nonregulatory sensor network made Salt Lake County an ideal case study area for this research (Beard et al. 2012; Mullen et al. 2023; Ou et al. 2020; Pope et al. 2008).
We focused this intervention on wintertime air pollution, which has been a problem in the region for decades. This is because in winter, cold air settles in Salt Lake’s mountain valley and high-pressure systems move in, acting like a lid, trapping pollution (Silcox et al. 2012). These episodes are known colloquially as “inversions.” During inversions, the spatial distribution of peak PM2.5 concentrations is largely determined by elevation, with lower-elevation areas on the valley floor—closest to pollution emissions sources—experiencing the highest concentrations for the longest durations (Mendoza et al. 2019; Silcox et al. 2012). This unequal distribution of PM2.5 contributes to environmental injustices in the region (Collins and Grineski 2019; Mullen, Grineski, Collins, and Mendoza 2020; Mullen, Grineski, Collins, Xing, et al. 2020). Salt Lake County was considered a serious nonattainment area for PM2.5 pollution from 2009 to 2024 due to its violation of National Ambient Air Quality Standards (U.S. EPA 2024). Such persistent PM2.5 air pollution problems have led to a robust network of nonregulatory air quality sensors—such as PurpleAir and Tellus sensors—deployed by universities, schools, businesses, and individuals (Becnel et al. 2019; Mullen et al. 2023; Sayahi, Butterfield, and Kelly 2019).
Recruitment and Enrollment
From October to December 2021, we recruited 26 parents of children who have asthma. We targeted our recruitment efforts in Salt Lake County with the support of the city and county library programs, community wellness and learning centers, the University of Utah Wellness Bus Program, the Utah School Nurse Association, and three Salt Lake County school districts. Each potential participant was screened to ensure that they met the inclusion criteria: living in or very near to Salt Lake County (25 were in Salt Lake, and 1 was near the Salt Lake County line in Davis County), having a child with asthma ≤15 years, speaking English or Spanish, and not using any air sensors at the time of enrollment.
Participant Demographics
There were 25 mothers and 1 father. Ten parents had asthma, and 4 had more than one child with asthma. There were 19 White non-Hispanic/Latinx parents. One was Hispanic/Latinx White, 5 were Hispanic/Latinx multiracial, and 1 was Black non-Hispanic/Latinx. Six parents were born outside of the United States in Sweden, Mexico, Colombia, and Honduras, and 5 spoke Spanish. The average parental age was 40 (range = 25–53), and the average age among the asthmatic children was 9 (range = 2–15).
Regarding yearly household income, 3 households earned under $20,000, 5 earned between $20,000 and $49,999, 4 earned between $50,000 and $74,999, 3 earned between $75,000 and $99,999, and 1 earned ≥$100,000. We grouped parents into two groups: those earning $74,999 or less (“lower income”; n = 12) and those earning ≥$75,000 (higher income”; n = 14). We used $75,000 as the break point because it is just under Salt Lake County’s median income—$82,206 (USCB 2021). Table 1 introduces demographics of parents by income group.
Parent Demographics (N = 26).
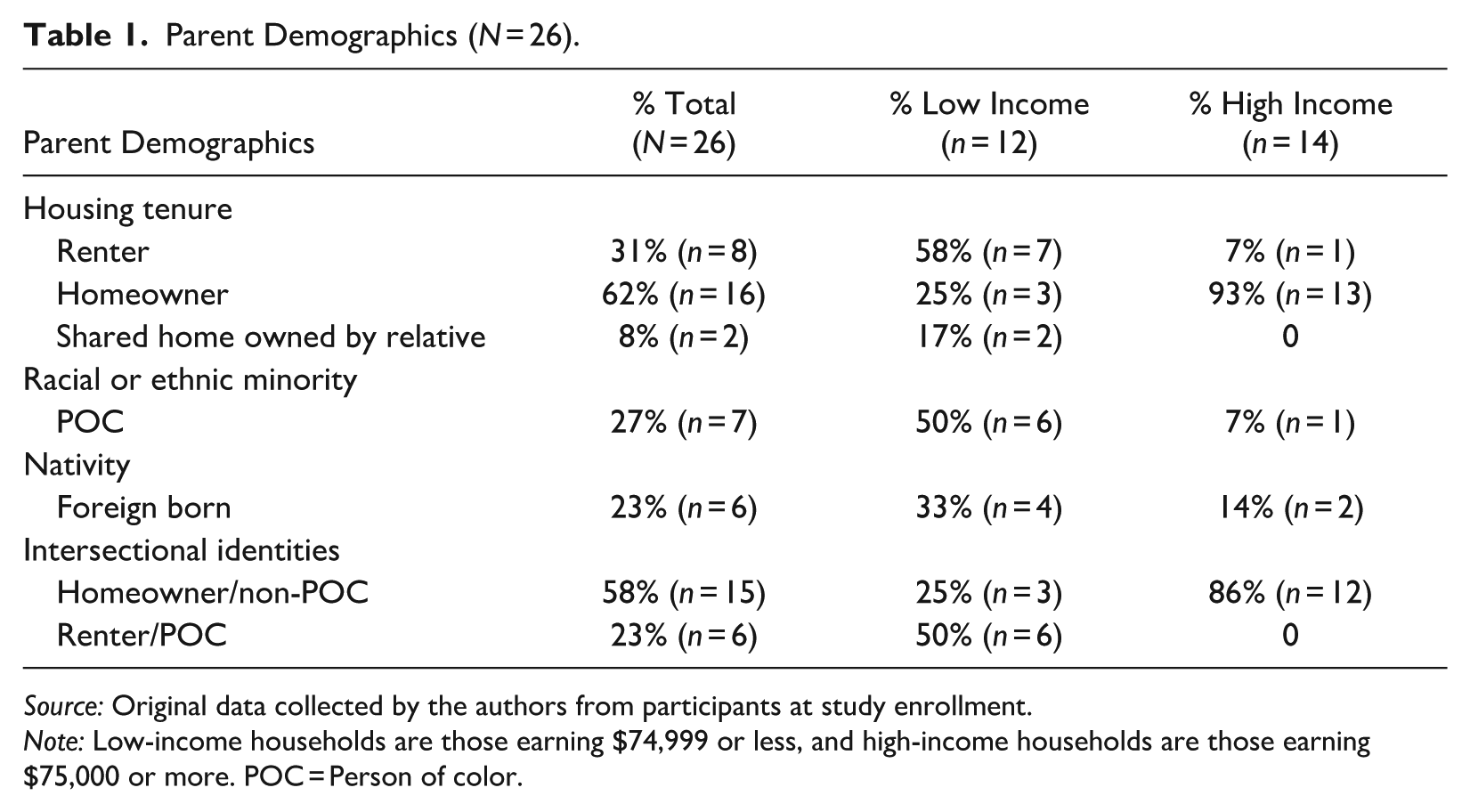
Source: Original data collected by the authors from participants at study enrollment.
Note: Low-income households are those earning $74,999 or less, and high-income households are those earning $75,000 or more. POC = Person of color.
We distributed 26 indoor and outdoor PurpleAir particulate matter sensors (i.e., the PA-I and PA-II Plantower particulate matter sensor with laser particle counters) to parents in January 2022 along with a sensor user guide that we created. The guide included information from the PurpleAir website to help parents understand the sensor technology and air quality index (AQI) readings. The families then used their sensors for 10 weeks. Although the sensors measured particles of multiple sizes using light-scattering laser-counter technology (Sayahi et al. 2019), we set up the sensors to show PM2.5. Parents obtained information about indoor PM2.5 sensor readings in two ways: by observing the sensor’s indicator light, which displayed AQI-associated colors in real time, or by checking the PurpleAir map (via the website or app) for the AQI-associated numeric value and color because the number was not displayed on the indoor sensor. To access outdoor PM2.5 readings (AQI-associated color and number), parents used the map because the outdoor sensor did not provide information directly to the user. In terms of interpreting that information for both sensors, the AQI readings and the PM2.5 24-hour average equivalent range of measurement in micrograms per cubic meter were as follows: 0 to 50 (good/green; 0–12.0 μg/m3), 51 to 100 (moderate/yellow; 12.1–35.4 μg/m3), 101 to 150 (unhealthy for sensitive groups/orange; 35.5–55.4 μg/m3), 151 to 200 (unhealthy/red; 55.5–150.4 μg/m3), 201 to 300 (very unhealthy/purple; 150.5–250.4 μg/m3), and 301 to 500 (hazardous/maroon; 250.5–500.4 μg/m3). We recommended that parents move the indoor sensor around to different locations within the home for optimal use while keeping outdoor sensors fixed to the home’s exterior.
Qualitative Data: Interview Data Collection and Analysis
Our team conducted semistructured interviews in English and Spanish 10 to 15 weeks after parents received the sensors (March–May 2022). We conducted 5 interviews face-to-face in their homes (all in English), 20 interviews over Zoom (5 in Spanish and 15 in English), and 1 interview by telephone (in English). The first author was the lead interviewer for 21 English interviews, and the third author led 5 interviews in Spanish with the first author in attendance. The interviews averaged 45 minutes (range = 30–60).
The general domains of our questions related to experiences with asthma and air pollution, participatory sensing, and health-related decision-making. The interviews included open-ended questions, created by the first author and informed by Adams et al. (2011). For example, we asked parents the following:
“How has having the sensors informed your understandings about your child’s asthma?”
“Which sensor did you refer to more often for asthma care?”
“Walk me through an experience that made you feel like having a sensor was useful” and, inversely, “was not useful.”
“Can you share examples of how you reacted to sensor readings?”
“Were you surprised by any sensor readings?”
Parents were compensated $50.00 after the interview process, and we gifted them their sensors poststudy. Each interview was recorded and transcribed.
We conducted two rounds of qualitative coding analysis using Nvivo Version 12 software. During the first round of coding, the first and third authors conducted focused coding together wherein a select number of predominant themes and patterns of interest were categorized into major topics revealed from the study (Emerson, Fretz, and Shaw 2011). During this time, we established intercoder reliability (Campbell et al. 2013). The first author conducted the second round of coding, focusing on positive and negative emotions and generating “theoretical code memos,” or summary write-ups, of the common themes and variations that occurred across the interviews (Emerson et al. 2011:641). In a third round of coding, the first author separated codes on emotional response into lower- versus higher-income categories to analyze the data for SES differences.
Quantitative Data: Weekly Survey Data Collection and Analysis
We used the web-based REDCap application to survey parents weekly between January and March 2022 for 10 weeks. We developed this survey based on previous research (Fowler et al. 2019; Grineski 2009; Utah Department of Health 2016) and a 2021 pilot study. Twenty-four parents completed at least 1 out of 10 surveys. Thirteen completed 10, four completed 9, one completed 8, one completed 7, one completed 6, one completed 5, two completed 3, and one completed 1 survey. Two lower-income parents did not complete any surveys. Each week, parents were asked the same 18 survey questions (related to their sensor readings, behavioral responses, and emotional well-being), which took about 5 to 10 minutes to complete. To gather data on parents’ emotions during participatory sensing, we asked parents to report—by selecting all that applied—if they felt “informed,” “happy,” “empowered,” “safe,” “stressed,” “sad,” “nervous,” “powerless,” “neutral,” “other,” and/or “not applicable,” generally while checking indoor and outdoor sensor readings. We aimed to measure emotions spurred by checking sensor readings. Although “informed” may be interpreted as a cognitive rather than emotional state, we included it on the survey as a driver of emotional experiences. “Happy,” “empowered,” and “safe” referred to positive emotions, and “stressed,” “sad,” “nervous,” and “powerless” were considered negative emotions.
With respect to the analysis of parents’ emotions toward sensor readings, we calculated the percentage of times that parents selected each emotion based on their total number of completed surveys, excluding “neutral,” “other,” and “not applicable” due to low counts. We then used those individual percentages to calculate the average percentage that each income group reported the emotion by sensor type—indoor and outdoor (presented in Figure 1). We used these quantitative estimations of emotions to supplement our qualitative analysis of parents’ transcripts.
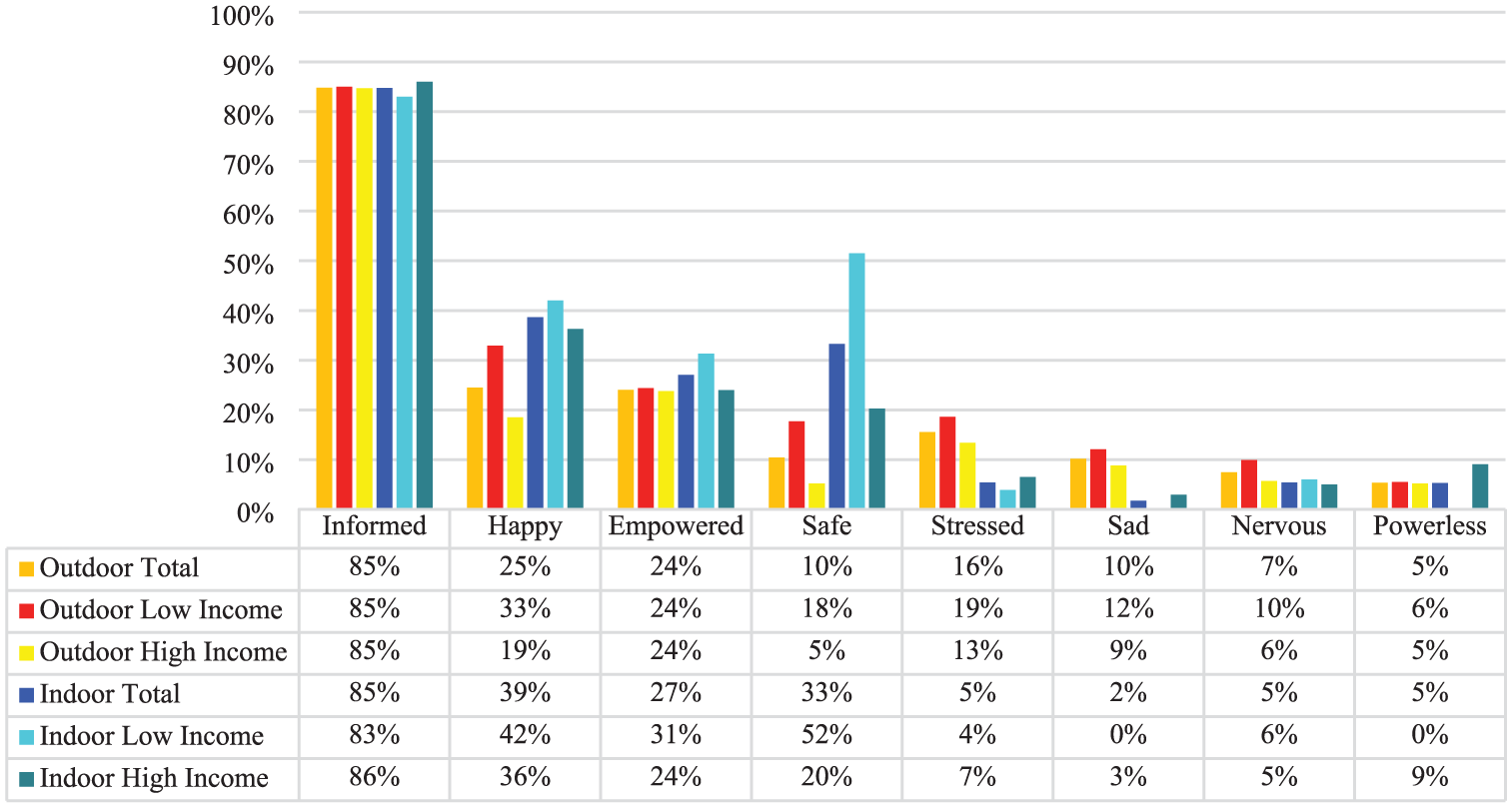
Emotional Responses to Sensor Readings by Income Group and Sensor Type.
Results
Feeling Informed
In terms of being informed, most parents reported feeling a greater sense of awareness regarding their exposure to air pollution and pollution sources through participatory sensing irrespective of their income level. Sometimes, feeling informed was associated with gaining new understandings. When we asked Penelope, a higher-income mother of a 10-year-old daughter with asthma, how her understandings about air quality evolved or changed from participatory sensing, she stated: The only thing I could think of is just being more aware of my indoor air quality. I think I was always focused on outdoor air quality. Prior to this, I didn’t worry as much about [my indoor air quality], I guess. I mean, I’m not worried now, but, you know, I guess I didn’t concern myself as much with it.
Erin, a lower-income mother of a 14-year-old son with asthma who also had asthma herself, expressed during her interview that she felt informed by both sensors because she made new connections between pollution sources and her family’s asthma experiences, which was consistent with her survey responses. She stated, “[Having the sensors] helps me to understand what’s really causing [our asthma symptoms] and be more informed.”
We found that feeling informed and empowered was described in tandem by many parents. A higher-income mother, Yvette, felt that other families should have access to air sensors due to their ability to inform and empower users. She said, “I think it’s really informative. And I think I checked ‘Empowered’ and ‘Informed’ on every single survey. It’s like to have that knowledge, I wish everybody could have it.” Often, feeling empowered signified an ability to control the exposure outcome. Parents felt empowered when an awareness of the exposures enabled them to engage in exposure-reduction action. Beth, introduced earlier as a lower-income mother, expressed a range of emotions throughout her sensing experience. Ultimately, she emphasized how the experience enabled her to connect her sensor readings with health-protective decision-making: It just was very eye opening and very beneficial for me to know [the indoor and outdoor sensor readings]. And it even made me a little bit nervous. Like in the [survey], it was like “How does it make you feel?” and when it was like “Nervous,” “Stressed?” I was like “Yes, it does! Because I’m ruining the air inside the house!” you know? Or like “Oh my gosh, my children are all breathing this terrible air outside that I’m now more aware of.” But then, after the nervousness and the stress kind of came down, it was more just like “Empowered” and “Informed” that I was feeling because here at our fingertips, I just open the app and it gives me a [sensor] reading, and then I know if I want to change any activities indoor or out.
Like Beth, a few other parents also described a shift in their emotions—from initial negative reactions to more positive ones as they engaged with participatory sensing over time. At first, they expressed feelings of nervousness and stress upon realizing the extent of their families’ PM2.5 exposures. However, as they became more familiar with the sensor data and how to use it for health-protective actions, these emotions shifted to feelings of gratitude and empowerment, with parents appreciating their ability to make more proactive decisions. One-third of parents’ surveys reflected this trend.
Another aspect of feeling informed by air sensor data was the surprise some parents felt when air quality conditions did not align with their prior assumptions. Many were particularly surprised to discover that activities such as cooking negatively impacted their indoor air quality. Some parents were surprised by the ambient air quality, expecting it to be worse than what their sensors indicated. Although these parents still perceived the outdoor air as being bad, the sensor data alleviated some of their anxieties, revealing that it was not as bad as they perceived and not as often. Charlotte, a lower-income mother with asthma, explained, “If anything, that was my biggest surprise, how good the [outdoor] air quality was. With all of the talk of bad air quality, I was like ‘Apparently it’s not that bad around our house!’” This shift in understanding may have helped reduce feelings of helplessness or stress because the sensor readings provided a clearer picture of the spatiotemporal characteristics of their air quality.
Feeling Safe Indoors
Many parents felt more secure and protected from PM2.5 exposures by knowing real-time sensor readings and taking responsive actions in the indoor environment in comparison to outdoor. Interestingly, lower-income parents reported feeling safe while checking their indoor sensor readings more than higher-income parents. In fact, “safe” was the second highest reported feeling on surveys from lower-income parents (see Figure 1).
Daisy, a lower-income asthmatic mother of three young children—one with asthma and two suspected of having asthma—and a husband with asthma, previously expressed her desire to buy a portable air purifier for her home due to her concerns that air pollution exacerbated their asthma symptoms. However, she noted that cost was a barrier. When we followed up about the air purifier, she explained, “The air sensor has showed me that our air is good inside our house. So, I don’t think that we need a whole house air purifier. . . . So that will save us a lot of money!” Daisy revealed that she was satisfied with her home’s air quality because she felt informed by the indoor sensor readings and secure. Note that her sense of reassurance was based on PM2.5 levels measured by the sensor and may not reflect the full spectrum of asthma-relevant exposures.
Descriptions of feeling safe and protected indoors tended to be associated with taking steps to ventilate and filter the air (e.g., opening windows and doors and using air purifiers). Yvette, a higher-income mother with a five-year-old daughter with asthma, spoke about how her heavy reliance on filtration led to protection indoors, reflecting what other parents reported while checking their indoor sensor readings: My thought process before [the study] was really that indoor [air quality], at least in our house, was a lot more closely linked to outside [air quality]. And I think it goes back to the fact that we’re running three or four HEPA filters [portable air purifiers] at all times, like all the rooms have everything all the time. I don’t shut the things [portable air purifiers] off. Like the huge impact that that is actually making, so that the outdoor can be really bad, but you can still be protected in your house, where I was thinking that we were not nearly as protected.
Yvette was able to confirm with her sensors that her indoor PM2.5 levels were low while outdoor levels were high due to constantly running her air purifiers. Similarly, Charlotte, introduced previously as a lower-income mother with asthma, described turning on her portable air purifier a lot more often than she had prior to her experience with participatory sensing. Being able to do so gave her positive reassurance that her indoor air was safe when outside conditions were bad: I don’t think we’ve ever run the air purifier as much as we have since we’ve had the [indoor] sensor. Because we would probably [wait to] turn it on before, until [there was] kind of a funky vibe in the house or something like that. . . . And the air purifiers are newer to our household anyway, so [our use of them] had maybe increased, but I would say it increased a whole heck of a lot since we got the sensor. A lot more often. And then it did kind of feel nice too because I’d be like “Well it’s bad outside but it’s great inside!” You know? We’re at zero [AQI inside].
Negative Emotions While Checking Outdoor Sensor Readings: Loss of Control
Overall, most parents described more positive than negative emotions during their experiences with participatory sensing. Interviews revealed a shared sentiment across income groups, with few parents expressing negative emotions regardless of sensor type. Survey responses aligned with this finding, showing minimal differences between how income groups reported negative emotions—“sad,” “stressed,” and “nervous.” Notably, feelings of powerlessness were reported the least (see Figure 1).
When we asked Ava, a lower-income mother of a seven-year-old son with asthma and asthmatic herself, if she ever felt stressed by either sensor, she stated, “Only when I was checking them and then it was bad outside. Then it made me stressed, worried, and sad because I was like, ‘Dang it this air quality! I wish we could have decent air quality!’” Sandra, a higher-income mother of a son with asthma, elaborated on why she sometimes felt worried about her outdoor sensor readings and at the same time informed and empowered: It was really interesting, like I had no idea how bad the air quality could get. Honestly, it was kind of scary like “Ah!” I mean, you knew it wasn’t good, but just to be more informed about it. . . . Usually it’s like, “I need to get these kids out!” and we would maybe not stay out[side] as long because I knew it wasn’t perfect [air quality] out there. But [it is] definitely a blessing, right? Like knowing. [Having the outdoor sensor and] knowing the [air quality conditions], you feel empowered, but then it’s also a little bit frightening too like, “Oh,” it’s worse than you think sometimes.
Although her outdoor sensor helped her assess air quality conditions and manage her family’s outdoor activity, in the same breath, Sandra revealed her anxiety surrounding the outdoor sensor readings at her home.
In a couple of notable examples, parents described heightened experiences with negative emotions when they felt constrained in their ability to address outdoor air quality or protect their families from exposure. Quinn, a lower-income mother of a son with asthma and asthmatic herself, explained her anxieties concerning outdoor sensor readings near her home in comparison to her indoor readings, which she celebrated: The one outside and then the others around us outside were the [sensors] that I relied on the most because . . . I can’t adjust outside [air pollution conditions], so I would adjust our behavior more. And they did bring you the most anxiety, though, because . . . I can’t do anything to fix that versus inside like “Oh, my indoor [sensor reading] is good,” you know? “Indoor is green, green, green! Yay indoor is clean!” But outside it was like so bad.
Quinn’s explanation characterized the attitude among other parents that although they felt generally satisfied and protected inside, by contrast, they expressed their unease with outdoor sensor readings due to their inability to control outdoor AQI levels. Conversely, Taylor, a higher-income mother of a 12-year-old son with asthma and asthmatic herself, indicated that she did not feel protected inside of her home during poor ambient PM2.5 conditions. Taylor’s historic Salt Lake home was not sealed well against outdoor air pollution, as indicated by her indoor sensor readings spiking at the same time as her outdoor sensor readings. She became highly concerned because she felt helpless in protecting her household: I was shocked by how bad the air quality in my house is because I thought we did a lot to help [with] that . . . I was under the false belief that I was safe inside my house like it was a magical bubble. And as long as we’re just in[side] we’re fine. And then realizing how bad the air quality was in my house. Because I think I felt like I had some control before in[side]—that I’ll just not go outside, or we’ll go up higher [in elevation] if we’re going to recreate. But now I just sort of thought “Well, what’s the point? It’s just as bad in my house and I can’t do anything in the moment other than the air purifier to fix that.” . . . It didn’t feel to me like there was anything I could do . . . I mean, I would turn my air purifier on, I would do that. But that is kind of what felt like all I had control over in the moment.
Taylor also shared that she felt so anxious about her indoor air quality during spikes in outdoor PM2.5 that she did not move her indoor sensor upstairs, fearing it would reveal unhealthy AQI levels her family was exposed to while sleeping. As others noted, although she could not control outdoor air quality, she sought to regain control by taking actions to reduce indoor PM2.5 levels.
Discussion
Sensors as a Tool of Empowerment and Control for Caregiving
We found that most parents—irrespective of income or sensor type (indoor vs. outdoor)—felt informed by the sensor readings. Even as parents’ emotional responses changed over time—from negative to positive—parents consistently described the participatory sensing process as reassuring because it heightened their awareness of air quality conditions. Feeling informed was closely tied to feelings of empowerment, especially when the sensor enabled them to act to reduce exposures. These positive emotional responses align with prior research on participatory air quality sensing (Boso et al. 2020; Heydon and Chakraborty 2020; Wong-Parodi et al. 2018) but are particularly noteworthy given the context of these parents’ enrollment in our study: All were caring for children with asthma (some with asthma themselves) and joined the study to access sensors as possible tools for managing illness.
This sense of empowerment is likely rooted in the physical and emotional responsibilities of caregiving. These parents undoubtedly bear the burden of the intense emotional labor of protecting children from environmental health risks and managing childhood asthma as primary caregivers (Avcil et al. 2019; Koenig and Chesla 2004; MacKendrick 2018). Thus, the sensors may have functioned as both environmental and emotional support tools—enhancing parents’ sense of control over asthma triggers like PM2.5 and affirming their efforts to reduce exposures. These benefits and positive emotional experiences were reported across income groups. This suggests that low-cost PM2.5 sensors may offer an inclusive form of support that bridges gaps in exposure awareness and action without exacerbating emotional or health disparities. This finding points to the potential for sensors to serve as accessible and empowering tools for asthma management.
Using Sensors to Navigate Contingent Boundaries
Contrary to Edelstein’s (2004) concept of the inversion of home, which posits that homes become distressing when contamination is discovered, many parents in our study reported positive feelings while checking indoor sensor readings. Most parents perceived their homes as protected spaces and felt reassured by sensor data that confirmed satisfactory indoor air quality. Parents often attributed a sense of safety to exposure-reduction measures, such as using air purifiers, and/or the observation that their homes served as a barrier from outdoor pollution. These beliefs reinforced a perception of control and were closely linked to feelings of empowerment and diminished stress (although this control extended only to PM2.5 given that their knowledge of exposures did not extend to other pollutants, such as ozone, which were not measured by their sensor).
By contrast, outdoor sensor readings underscored just how little control parents had over ambient PM2.5 pollution. Some parents were mildly surprised that the outdoor air quality was not worse than expected. These reactions were less pronounced than those documented in studies where sensors revealed unexpectedly poor conditions (Boso et al. 2020; Heydon and Chakraborty 2020). Echoing Heydon and Chakraborty’s (2020) findings, parents in our study expressed frustration about their inability to mitigate outdoor pollution and the limitations of their behavioral strategies to reduce exposures, such as limiting outdoor activity and masking. This contrasted with the control that parents felt over indoor air quality, and so their homes became a refuge—both physically and emotionally—from external environmental threats.
Rather than striving for full control over all the exposure environments they encountered, parents focused on managing air quality with the support of their sensors where they felt the most agency—in their home. This sense of selective control shaped their behaviors and emotional responses. These findings reflect the concept of contingent boundaries, which demonstrates how individuals construct emotionally manageable, discrete zones of contamination control by selectively addressing certain risks while avoiding others where they feel vulnerable to exposure (MacKendrick and Stevens 2016). In our study, this strategy allowed parents to focus their caregiving efforts within a perceived boundary of control—inside the home—while psychologically distancing themselves from outdoor conditions they felt powerless to change.
These patterns of spatially contingent control were not experienced uniformly. When we compared how lower- and higher-income parents differed in their emotional responses to indoor and outdoor sensor readings, we found that SES shaped how parents interpreted safety and their capacity to act on sensor information—sometimes in unexpected ways. Lower-income parents were more likely than their higher-income counterparts to report feeling safe indoors compared to outdoors—despite experiencing heightened indoor exposures (i.e., versus higher-income households), as we discovered in a separate analysis of these sensor data. These lower-income households experienced higher indoor PM2.5 exposures than higher-income households, with mean, median, and peak sensor readings that were 1.7, 2.9, and 2.1 times greater, respectively (Mullen et al. 2025). Although it might be expected that lower-income parents would express the most negative emotions given their heightened exposure burdens, this was not necessarily the case. One explanation may be that given the limited resources and power that lower-income families have at their disposal to reduce environmental health risks for asthma care (Grineski 2009), they may have viewed the sensors as a novel, empowering tool. Participatory sensing may have offered a new form of agency in protecting their children not available to them through other means. This interpretation aligns with MacKendrick’s (2018) concept of precautionary consumption, which suggests that consumer-based tools for exposure reduction, such as sensors and air purifiers, can foster feelings of empowerment and safety. Comparatively, it is possible that more affluent individuals, with greater access to resources, may not experience the same emotional boost from gaining access to a new protective tool, having already possessed other forms of control.
The Emotional Toll of Sensing amid Parenting Pressures to Protect
Although less common than positive responses, some parents across income groups described experiencing negative emotions, such as helplessness and anxiety, when they felt unable to control outdoor air pollution. These negative emotional reactions mirrored the experiences of other parents, documented in the literature, as they made decisions related to environmental health risks and asthma caregiving (e.g., from chemical exposures and negative experiences with illness; Avcil et al. 2019; Koenig and Chesla 2004; MacKendrick 2018). Our results similarly suggest that the pressures of caregiving coupled with the reality of uncontrollable exposures can culminate in feelings of emotional vulnerability. All parents—no matter what their income—are susceptible to the emotional consequences of falling short of idealized parenting standards when protective actions are constrained. In the case of participatory air quality sensing though, we found these feelings to be relatively rare.
We found that higher-income parents expressed greater emotional stress about their inability to protect their children from outdoor air pollution exposures than did lower-income parents. This finding among higher-income parents may appear counterintuitive given their greater access to exposure-reduction tools, such as air purifiers (Mullen et al. 2025). However, it aligns with research showing that affluent mothers often internalize ideals of intensive mothering—an expectation that good parenting requires continuous, informed, and effective risk management—contributing to heightened feelings of failure when they are unable to meet these expectations (MacKendrick 2018).
Revisiting the concept of contingent boundaries offers deeper insight into this finding. Lower-income parents in our study appeared more likely to emotionally accept what they perceived as manageable zones of control (i.e., inside the home), whereas higher-income parents—who were accustomed to leveraging interventions through precautionary consumption practices—struggled more when their efforts fell short in the face of ambient exposures that they could not mitigate. This contrast suggests that emotional responses to sensing are shaped not only by material resources but also by class-based expectations regarding caregiving responsibility.
One striking example came from Taylor, a higher-income mother, who—despite her access to resources and proactive behaviors, including using an air purifier—reported significant emotional stress when she discovered her indoor air quality mirrored poor ambient conditions. Unlike other parents in the study for whom the home functioned as a contingent boundary where control was possible, Taylor’s realization that her indoor environment was not safe dissolved that boundary and intensified her sense of helplessness (MacKendrick and Stevens 2016). Taylor had access to tools designed to help her reduce exposure, but she still felt overwhelmed when the sensor revealed that her interventions were not enough. Her story illustrates the limits of precautionary consumption as a means of health protection and emotional reassurance (MacKendrick 2018). Taylor’s decision to stop monitoring her upstairs air quality illustrates a strategic coping response, reflecting what MacKendrick and Stevens (2016) would describe as a deliberate intention to avoid distressing information once the limits of control are recognized. This case highlights how sensor use itself can become emotionally fraught, especially when information reveals the fragility of protective boundaries.
Our findings show that parents’ emotional stress emerges not simply from exposure levels but also from the interplay between caregiving responsibilities (i.e., expectations of protection and control) and the emotional consequences of encountering limits to their control. Parents—especially those socialized into ideals of intensive mothering—may experience heightened emotional vulnerability when their strategies of protection fail. For families already burdened by caregiving responsibilities, even tools designed to empower them can reveal the gaps between individual action and systemic environmental health risks. Our study findings further emphasize that environmental health tools, such as sensors, must be contextualized not only in terms of information (e.g., data) and behavioral response (e.g., exposure reduction measures) but also emotional experience.
Finally, it is essential to consider the challenges that parents face in keeping up with the increasing care demands and costs of pro-environmental and health-protective behaviors prompted by sensor use. This raises questions about the long-term sustainability of placing the responsibility for exposure reduction on individuals, particularly caretakers in low socioeconomic groups (Cousins 2021). Although it is crucial to recognize that outdoor sensor readings may evoke negative emotions, the broader issue lies in placing the burden of protection against air pollution on individuals rather than on government and policy. This misplacement of responsibility can intensify feelings of powerlessness and highlight the inadequacy of individual action to effect real change (Oksas et al. 2022). Without a broad shift toward policies that prioritize air quality at a systemic level, individual efforts will remain insufficient to address these challenges.
Limitations
Our study limitations provide insights into future research opportunities. One limitation is that some participants did not complete any of the surveys (i.e., two lower-income participants) and others completed only part of them. This restricted our ability to discern trends over time in emotional responses and SES differences. We chose to limit our discussion of the survey data to findings that could also be supported by interview data given concerns about missing data.
In our study, participants were left to interpret their sensor data independently during the 10-week intervention period, which may have led to varying levels of understanding and emotional reactions. However, it is important to note that our participants’ hands-off experiences reflect those of lay citizen scientists. Because most individuals using sensors are not part of a formal study, our findings offer valuable insights into the real-world experiences of lay sensor users. To address this limitation, one month after the study concluded, we shared informational packets with participants that included common sources of indoor and outdoor PM2.5 pollution, health-protective interventions, and opportunities for collective action, such as local environmental and health groups to connect with and methods of political advocacy. Additionally, the PM2.5 sensors that we provided to participants did not measure other pollutants that may also impact asthma symptoms and severity (e.g., ozone), and few low-cost options for measuring other pollutants exist.
This study focuses on a single case study community. Although the findings offer valuable insights, they are not necessarily generalizable to other contexts. Future research should explore the emotional implications of sensor use in other communities, especially among individuals facing everyday stressors, such as racism, stigmas, and limited resources. Although our study did not find many substantive differences in participants’ experiences by income, this does not rule out the possibility that factors such as race, ethnicity, and education level shape how individuals perceive and respond to their exposures.
Conclusion
We found that participatory sensing generally supported the emotional well-being of parents caring for asthmatic children across income levels because benefits generally outweighed drawbacks. To advance health equity in asthma management, we recommend expanding access to both low-cost air sensors and air cleaning devices, such as portable air purifiers, because this combination can empower families to make informed, timely, and sustained efforts to reduce PM2.5 exposures. Research shows that participants use sensors to identify acute spikes in pollution and assess the effectiveness of their mitigation strategies (Mullen et al. 2025). Sensors thus can support health-protective action and foster positive feelings of control, as we have shown here. We propose increasing funding for household sensor and portable air purifier distribution through existing public health infrastructure, such as the Healthy Homes Initiative, and local or state government-funded voucher programs. The United States Department of Housing and Urban Development funds grant programs to support healthy homes initiatives aimed at children and vulnerable populations; these initiatives could supply sensors and air purifiers to help families impacted by asthma. Sensors and purifiers could also be integrated into asthma management and prevention efforts, including Medicaid and other health care programs serving vulnerable populations. Federal agencies, such as the U.S. EPA, could further support these efforts through programs such as the Environmental Justice Small Grants Program and the Citizen Science Program.
Lastly, although families may use sensors in pursuit of health-protective information to reduce personal exposures, many PM2.5 exposure sources primarily arise from large-scale factors beyond individual control. Therefore, we urge policymakers and public health leaders to pair sensor distribution with structural interventions to improve air quality. Supporting a transfer of responsibility from individuals to institutions would better address the root causes of air pollution and alleviate some of the emotional burden on individuals, especially those caring for children with asthma.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants’ essential contribution to this research and extend thanks to everyone at Northeastern University’s Social Science Environmental Health Research Institute (directed by Dr. Phil Brown) for their invaluable feedback, which greatly enhanced the quality of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was supported by the National Science Foundation (Award No. 58503129), the University of Utah Sustainable Campus Initiative Fund, the National Institute of Environmental Health Sciences Research Training Grant (No. T32ES023769), and the National Center for Advancing Translational Sciences of the National Institutes of Health under Award No. UL1TR002538. The content expressed in this material is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.