
Abstract
Research demonstrates that perceived discrimination negatively impacts health. Yet there is conflicting evidence about how an individual’s definition of discrimination—separate from their experience of discrimination—shapes health disparities. Using a nationally representative survey experiment in which participants (N = 2,000) are asked to evaluate nine different scenarios of potential discrimination, we find that how a person labels these discrimination scenarios is significantly related to their self-rated health, even after controlling for sociodemographic factors. U.S. adults who are more likely to label the event as discrimination in cases where it is intentional have comparatively worse self-rated health, whereas those who are more likely to label discrimination in cases where it affects more powerful groups (White people, men, and the wealthy) have comparatively better self-rated health—even though they are not experiencing the discrimination themselves. We argue that these findings have important implications for how health researchers measure discrimination’s health effects.
Perceived discrimination negatively impacts health (Araújo and Borrell 2006; Bratter and Gorman 2011; Brown et al. 2000; Krieger et al. 2011; Lewis, Cogburn, and Williams 2015; Major, Dovidio, and Link 2018; Pascoe and Smart Richman 2009; Phelan and Link 2015; Williams et al. 1997; Williams and Mohammed 2009). These negative health effects are driven by both the structural realities of discrimination (i.e., unequal access to health-promoting opportunities and resources; Homan 2019; Krieger 2020; Phelan and Link 2015) and the perceptual appraisal process itself (i.e., avoiding, being vigilant about, and assessing potential interactions of discrimination; Clark, Benkert, and Flack 2006; Hudson et al. 2016; Jacob et al. 2022; Lewis et al. 2015; Quaye et al. 2020; Williams, Lawrence, and Davis 2019). Indeed, discrimination along the axes of race (e.g., Williams and Mohammed 2009), gender (e.g., Homan 2019), and socioeconomic status (e.g., Link et al. 2024) has been identified as a key potential mechanism driving population-level health disparities.
Yet it is very challenging to isolate and measure the health effects of experiencing discrimination from the health effects of perceiving discrimination. This is because analysts have repeatedly noted that existing measures of perceived discrimination likely capture systematically different understandings of what defines discrimination (Bratter and Gorman 2011; Grollman and Hagiwara 2019; Schmitt et al. 2002; Valentino and Warren 2025; Warren and Valentino 2025). There is thus a critical need for scholars of discrimination and health to isolate the impact of how people define discrimination to better capture the full impact of discrimination on health outcomes.
Our focus in this study is whether a person defines a given scenario as discrimination, what we refer to as a “discrimination appraisal,” as shown in the conceptual diagram in Figure 1. This focus on how people define discrimination represents a key shift from prior research’s focus on experiences of discrimination—an important tradition of work centered on measuring whether individuals report being discriminated against in various contexts (e.g., at their workplace or in a restaurant) and with various attributions (e.g., due to their race-ethnicity, their religion, etc.). Critically, a focus on definitions of discrimination allows for differentiation between the effects of the definition’s impact on whether one perceives discrimination and the effects emanating from the experience of discrimination itself.
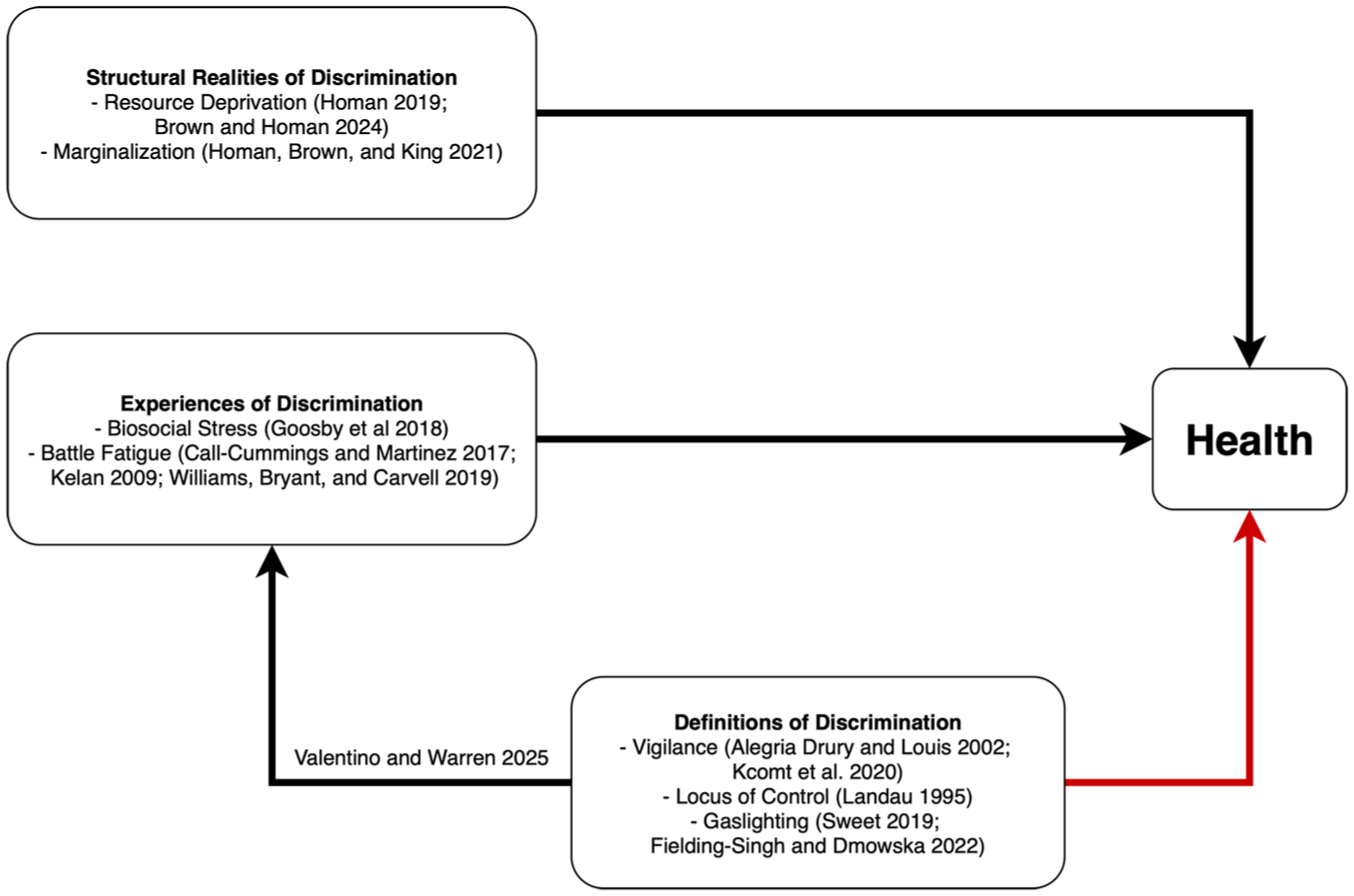
Conceptual Diagram Showing the Relationship between Discrimination, Perception, and Health.
There has been, to date, little work on the health impact of whether and how a person appraises a particular event as discrimination—even when the event did not directly impact them. This is an important gap to fill because existing work on perceived discrimination cannot distinguish between the potential health effects individuals undergo as a result of their actual experiences of discrimination and the potential health effects that occur due to having a particular definition of discrimination (Small and Pager 2020). The latter is our focus in the present study, as highlighted in red in Figure 1. This is key for scholars to understand due to its direct effects on health (our focus in the present study) and its potential impact on how often a person reports that they (or their group) has experienced discrimination (Valentino and Warren 2025), with further downstream implications for health. As we show, prior scholarship has argued that defining a given event as discrimination may be harmful or beneficial for overall health and well-being. Thus, it is urgent for researchers to resolve this paradox and understand how different definitions of discrimination relate to health.
Background
Existing work on the relationship between discrimination appraisals and health has been mixed. Some research suggests that appraising an event as discrimination likely leads to worse health outcomes, whereas other research suggests the opposite: that appraising an event as discrimination likely leads to better health. We argue that this lack of clarity about the relationship between discrimination appraisals and health is due, in part, to prior scholarship’s focus on the form of discrimination appraisals (i.e., whether they are expansive or accurate) rather than their content (i.e., how they are defined).
Appraising Discrimination Leads to Worse Health
Findings from one body of work suggest that labeling something as discrimination has a negative impact on health (Pavalko, Mossakowski, and Hamilton 2003; for a review, see Allen 2019). This perspective suggests that recognizing and naming discrimination can lead to constant vigilance and the subsequent activation of stress processes as individuals assess, encounter, and react to potential instances of discrimination around them (Himmelstein et al. 2015; Kaiser and Miller 2004). Researchers point to having an external locus of control—a sense that an individual has minimal impact over the outcomes they experience—as a major stressor (Landau 1995). Indeed, experiences of racial discrimination may clarify that there are significant factors at play beyond the control of individuals, leading to anticipatory stress as they attempt to navigate a system that feels stacked against them. For instance, those who say that they have experienced racial discrimination report being constantly on guard against racism and feeling heightened vigilance due to fear of discrimination (Alegria Drury and Louis 2002; Kcomt et al. 2020), a loss of trust in the medical system (Williams, Lawrence, Davis, and Vu 2019), and even sleep difficulty (Hicken et al. 2013).
Critically, these effects are not limited solely to individuals who experience the discrimination directly but also spill out to those in their immediate communities. For example, Colen et al. (2019) document the intergenerational transmission of discrimination, demonstrating how a child’s experiences of discrimination correlate with declines in their mother’s self-rated health during middle to late life. The vicarious negative impacts of discrimination thus underscore the important role of discrimination appraisals above and beyond the direct experience and structural reality of discrimination. Moreover, vicarious discrimination can contribute to the larger phenomenon of “racial battle fatigue” or in cases of sexism, “gender battle fatigue” (Call-Cummings and Martinez 2017; Kelan 2009; Williams, Bryant, and Carvell 2019).
Relatedly, studies examining general awareness of inequality have found that belief in and knowledge of rising inequality is correlated with lower self-rated health (Gugushvili and Reeves 2021). In fact, recent work has found that denying that one has experienced discrimination can be health protective (Napier, Suppes, and Bettinsoli 2020), further underscoring the potential negative health effects of labeling an event as discriminatory. Indeed, emerging research into the impact of structural forms of discrimination on health seeks to overcome the issue of perception by documenting how discrimination shapes health without relying on measures of individual discrimination appraisals (Brown and Homan 2022, 2024; Homan 2019; Homan, Brown, and King 2021; Hummer 2023). However, the question remains as to whether individuals see structural oppression (e.g., disparate outcomes in life chances and/or an unequal distribution of power and resources between groups) as discrimination and if so, whether perceiving this structural oppression as discrimination relates to health.
Appraising Discrimination Leads to Better Health
By contrast, findings from another body of work suggest that perceiving an event as discrimination can lead to better health. In an experimental study testing the impacts of information about discrimination on health, Carty et al. (2011) find that participants in the intervention group who were educated about racism reported better health than the control group even though they then reported higher levels of discrimination. This may occur because increased awareness about racism allows individuals to attribute the negative events they encounter to discrimination rather than to a personal failure (see Major, Quinton, and McCoy 2002; Major, Quinton, and Schmader 2003). A number of studies on perceived discrimination have demonstrated that this externalization of blame can be health protective by increasing self-esteem (Adams, Tormala, and O’Brien 2006; Crocker et al. 1991; Major, Kaiser, and McCoy 2003). Appraising discrimination may also reduce feelings of gaslighting, which was theorized by Sweet (2019:851) as a phenomenon rooted in social inequities where “the mobiliz[ation] of gender-based [or other] stereotypes and structural and institutional inequalities are used against victims to manipulate their realities.” Unsurprisingly, this sociological form of gaslighting has been shown to have negative health effects as well (Fielding-Singh and Dmowska 2022).
Specifically, among Black Americans who report experiencing racism, those who attribute blame for the negative events to systems rather than individuals experience better psychological health and reduced mortality (LaVeist, Sellers, and Neighbors 2001; Sellers, Neighbors, and Bonham 2011). Similarly, in a study of perceived discrimination among Black working-class Americans in early adulthood, Krieger and Sidney (1996) find that blood pressure is higher for those who say they have not faced racial discrimination compared to those who report that they have. They conclude that “individuals belonging to groups subjected to discrimination may be at lower risk of elevated blood pressure if they are able to articulate, rather than internalize, their experience of discrimination [italics added]” (Krieger and Sidney 1996:1376). Furthermore, recognizing an event as discrimination may also encourage individuals to seek out contextually appropriate health-promoting behaviors such as social support from members of one’s community or culturally competent mental health therapy (Carter and Forsyth 2010; Foster 2000; Jacob et al. 2022; Noh and Kaspar 2003; Shorter-Gooden 2004; but see Greer 2011).
The Need to Study How Definitions of Discrimination Impact Health
We argue that part of the reason for these mixed findings about the relationship between discrimination appraisals and health occurs because prior work has largely been focused on the form of these appraisals (i.e., how expansive people’s definitions are regarding discrimination or how knowledgeable people are about discrimination) rather than their content (i.e., how people define discrimination qualitatively). Emerging research has found that individuals appraise discrimination differently depending on their sociodemographic identity, such as their race-ethnicity, nationality, gender, education, historical knowledge, age, time period, political and religious views, and occupation, among other factors (Bonam et al. 2019; Carter and Murphy 2015; Flores-González and Salgado 2021; Fraser and Kick 2000; Greenland, West, and van Laar 2022; Kehn and Ruthig 2013; Lamont et al. 2018; Mayrl and Saperstein 2013; Nelson, Adams, and Salter 2013; Norton and Sommers 2011; Operario and Fiske 2001; Valentino and Warren 2025; Wingfield and Chavez 2020; Zell and Lesick 2021; for reviews, see Eyer 2012; Small and Pager 2020). Moreover, different situational cues and contexts—such as intentionality, magnitude of harm, presence of animus, role of individuals versus institutions, domain (i.e., the workplace vs. family), and the power and position of those affected—also shape whether people perceive an event as discrimination or not (Johnson et al. 2003; Mallett, Ford, and Woodzicka 2016; Maxwell 2015; Sommers and Norton 2006; Swim et al. 2003; Unzueta and Lowery 2008; Valentino and Warren 2025; Weinberg and Nielsen 2017; for a review, see Stangor et al. 2003). Given these developments, we expect that the impact of labeling a given event as discrimination depends on how a person defines discrimination. Our main research question is therefore: How do people’s definitions of discrimination relate to their health?
To query people’s discrimination definitions, we focus on three key dimensions of discrimination appraisals that have been found to be salient in prior research (Harnois 2023; Valentino and Warren 2025): (1) whether the action was intentional or not, (2) whether the event is a case of unequal treatment or unequal outcomes, and (3) whether the event affects someone from a traditionally less powerful group (i.e., a racial minority, woman, or poor person) or a traditionally more powerful group (i.e., a White person, a man, or a wealthy person). We do not ask people directly for their definition of discrimination because these kinds of tasks are often cognitively inaccessible and subject to issues of social desirability bias (Vaisey 2009). Instead, we use a survey experimental approach in which we ask people to rate realistic scenarios of potential discrimination faced by others. This approach allows us to control various dimensions of the discrimination scenario, understanding how these dimensions impact the likelihood that it is seen as discrimination.
To measure participants’ health, we use self-rated health, a well-validated subjective measure of generalized health that is predictive of overall mortality and morbidity risk (Harris and Hummer 2023; Idler and Benyamini 1997; Jylhä 2009). Self-rated health is often used in analyses of discrimination’s effect on health because it captures aspects of both physical and mental health. Discrimination, specifically, has been associated with better self-rated health in some studies (e.g., Carty et al. 2011) and worse self-rated health in others (e.g., Colen et al. 2018). Because self-rated health is a generalized measure, it serves as an important baseline measure of the effects of discrimination definitions on health. In addition, self-rated health is responsive to shifts in discrimination-related stress (Himmelstein et al. 2015). Objective measures of health responses to stress-related mechanisms demonstrate a clear relationship between experiences of discrimination and health (for a review, see Goosby, Cheadle, and Mitchell 2018). 1
To preview our results, data from our nationally representative survey experiment demonstrate the multifaceted relationship between discrimination appraisals and health. We observe that U.S. adults who are more likely to appraise discrimination in cases where it is intentional have worse overall self-rated health compared to those who do not rate intentional events as discrimination. However, we also find that U.S. adults who are more likely to say an event “counts” as discrimination when it happens to White people, men, and the wealthy (rather than racial minorities, women, and the poor) have better self-rated health compared to those who do not rate these events as discrimination. These findings hold even after controlling for other sociodemographic factors that are known to shape health and discrimination appraisal, such as education, political views, race, income, and age. Thus, a person’s definition of discrimination is a key factor in their overall health and well-being.
Data and Methods
We collected nationally representative survey data using a novel experimental approach to capture variations in how Americans define discrimination. We varied the components of an event to understand how different dimensions of discrimination were related to self-rated health. This research was approved by the Institutional Review Board of the authors’ university.
Experimental Design
The survey randomly varied three dimensions of discrimination while standardizing the discrimination story itself. Each participant rated nine different vignettes reflecting potential instances of racial-, gender-, and class-based discrimination. We used vignettes based on inductive interviews from Valentino and Warren (2025); these vignettes depicted real-world examples of discrimination that people may plausibly encounter or observe as third parties. This approach ensured a high degree of external validity such that the vignettes were realistic events that could occur or have occurred in real life. The racial discrimination vignettes were about a driver’s encounter with a police officer at a traffic stop, a decision about which teacher to hire at a racially segregated elementary school, and racial preferences in potential romantic partners at a speed-dating event. The gender discrimination vignettes were about gender differences in pay and promotion at the sales department of a company, a sexual confrontation between two Hollywood actors, and health care providers’ responses to a man and a woman with similar symptoms at the emergency room. The class-based discrimination vignettes were about a poor student and middle-class student dealing with their high school’s uniform policy, financial aid policies in a college admissions office, and two young men from different class backgrounds drawing on their social networks to try to obtain a job (for full text of vignettes, see Appendix B in the online version of the article).
Each of these nine stories had different versions varying the three experimental contrasts: (1) whether the situation depicted an intentional or unintentional act of discrimination, (2) whether the situation depicted a case of unequal treatment or unequal outcomes, and (3) whether the target belonged to a traditionally more powerful group or a traditionally less powerful group. Figure A1 in Appendix A in the online version of the article shows how these components were manipulated for one vignette. Participants were presented with the self-rated health question before they were asked to assess the scenarios of potential discrimination, helping to ensure that any significant results of discrimination appraisal on health are due to how participants define discrimination rather than vicarious discrimination (Colen et al. 2019; Quinn et al. 2023). Research has shown that attribution is a key part of people’s assessment when determining whether discrimination has occurred (Essed 1991); for instance, in the Everyday Discrimination Scale, respondents must report what they think the main reason is for the discrimination experience, such as their race, gender, age, religion, and so on (see Williams et al. 1997). Therefore, rather than leave the attribution ambiguous for participants to decide, which would introduce additional outside forms of variation, we instead asked them to agree with a third party’s assessment of the scenario as a particular form of discrimination (e.g., class-based discrimination in the case of the three class-focused vignettes).
Extensive pretesting included manipulation checks to ensure that the textual variation captured the intended experimental contrasts. 2 In addition to rating vignettes, participants were also asked standard questions about their policy preferences, their demographic characteristics, and their self-rated health. We discuss these variables in greater detail in the following section.
Data and Measures
We partnered with the survey firm YouGov to field the study to a nationally representative sample of 2,000 American adults. Unweighted descriptive statistics for the sample are shown in Table 1.
Sample Descriptive Statistics (Unweighted).
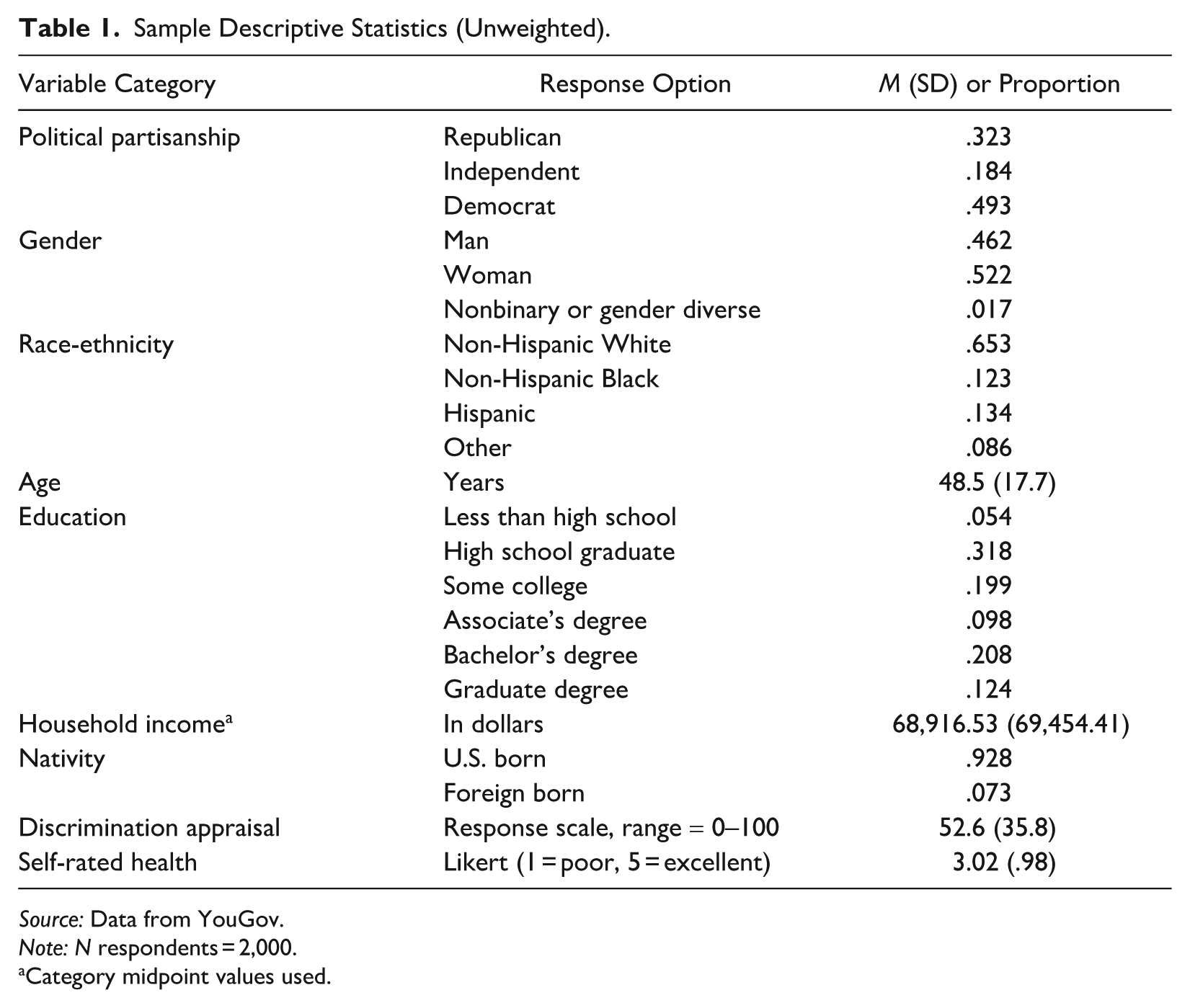
Source: Data from YouGov.
Note: N respondents = 2,000.
Category midpoint values used.
The data set included standard demographic variables and the primary variables of interest: self-rated health and discrimination appraisal. The key dependent variable, self-rated health (range = 1–5, where 1 = poor and 5 = excellent), is a well-validated proxy for overall individual health (Jylhä 2009). It has been tested in a variety of populations and captures the complex ways that mental and physical health shape each other and does not rely on official diagnoses that can often obscure disparities due to unequal health care access (Chandola and Jenkinson 2000; Idler and Benyamini 1997; Zajacova, Huzurbazar, and Todd 2017). The key independent variable, discrimination appraisal (range = 0–100, where 0 = strongly disagree that the vignette incident is discrimination and 100 = strongly agree that it is discrimination), reflected the focus of our analysis on the role of appraisal separately from the structural realities of discrimination or direct experiences of discrimination. By eliciting appraisal of a hypothetical discrimination event rather than a person’s reported experiences of discrimination, we were able isolate the role of appraisal on health rather than observing the effect of appraisal combined with the psychosocial repercussions of experiencing discrimination.
Analytic Approach
We show results from two sets of models. In the first set of models, we linearly regressed health on discrimination appraisal for each of the three experimental contrasts, including an interaction term to capture the relationship between health and the experimental condition in combination with the appraisal score. In the second set of models, we introduced sociodemographic control variables (race-ethnicity, gender, education level, age, income, nativity, and political party) because both appraisal and health are likely affected by these factors. All models included sample weights to ensure representativeness and robust standard errors clustered by participant to account for the fact that each participant rated nine different scenarios. Because income was missing from 9.55% of participants—and because income is a known predictor of both discrimination appraisal and health—we used multiple imputation with chained equations in 10 replicate data sets to account for these missing data. 3
Results
Descriptively, we observe striking variation in how people define discrimination along the three dimensions of intentionality, unequal treatment/outcomes, and power differences. As depicted in Figure 2, all six versions of the vignette were rated between 0 (the participant strongly disagreed that the event constitutes discrimination) and 100 (the participant strongly agreed that the event constitutes discrimination). Vignettes in which the action was intentional were more likely to be rated as discrimination (M = 76.16, SD = 28.12) than those where the action was unintentional (M = 66.08, SD = 30.74). Vignettes in which the action was a case of unequal outcomes were slightly more likely to be rated as discrimination (M = 44.24, SD = 34.99) than those where the action was a case of unequal treatment (M = 41.56, SD = 33.01). Vignettes in which the person affected was part of a less powerful group (a person of color, a woman, or a lower social class background) were also more likely to be rated as discrimination (M = 44.24, SD = 34.99) than those in which the person affected was part of a more powerful group (a White person, a man, or from the middle/upper class; M = 35.42, SD = 33.74). Nevertheless, the large standard deviations for these discrimination appraisals reveal broad disagreement about how discrimination is defined by American adults (for a detailed exploration of sociodemographic differences in appraisals, see Valentino and Warren 2025).
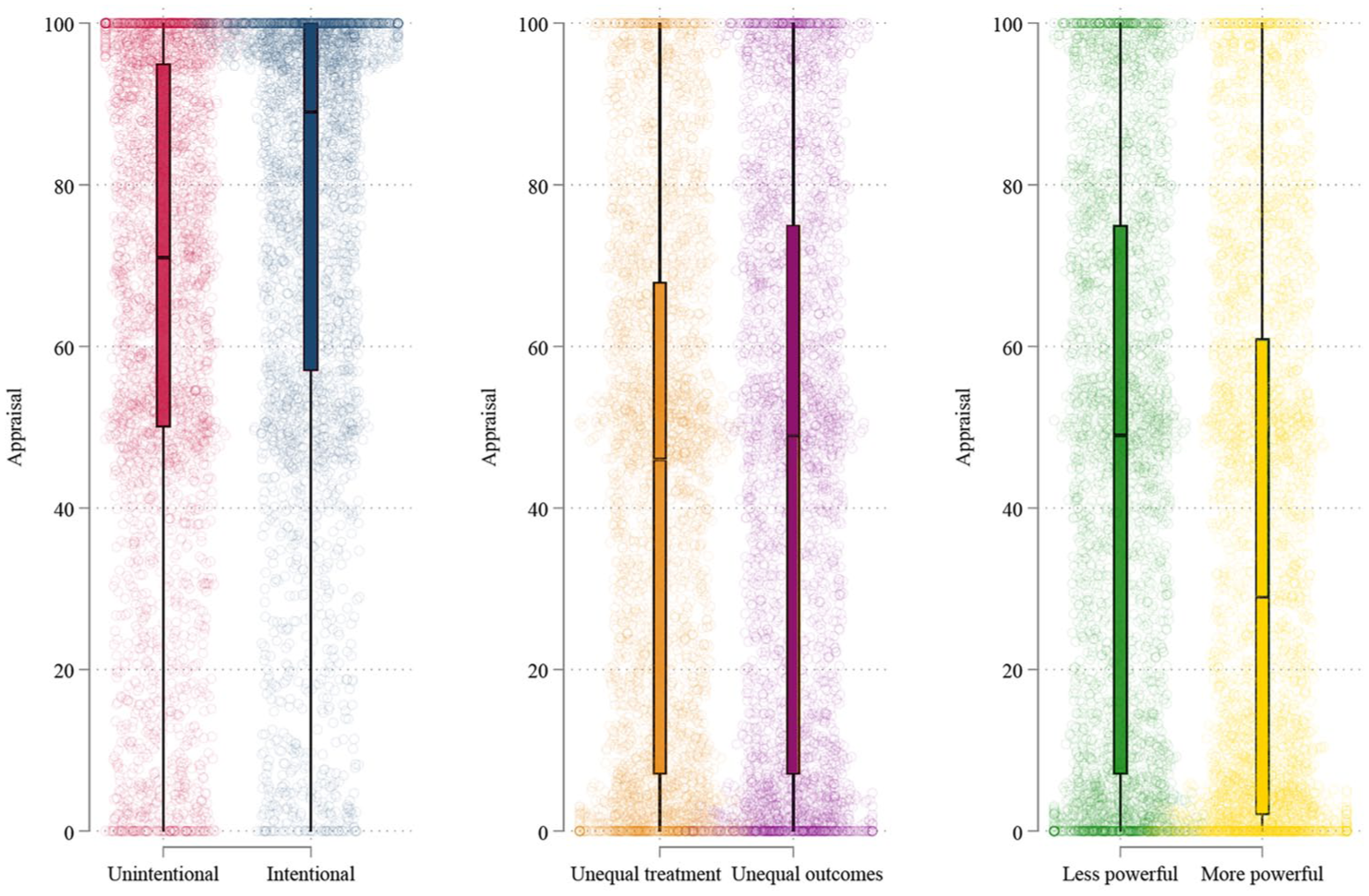
Box Plots Depicting the Distribution of Discrimination Appraisals (0 = Strongly Disagree the Event Is Discrimination, 100 = Strongly Agree That the Event Is Discrimination) for the Three Experimental Contrasts.
To understand how these varied definitions of discrimination relate to health, we linearly regress self-rated health on discrimination appraisal and then add demographic controls. Both sets of models include an interaction term to capture how discrimination appraisal is different in scenarios that are otherwise identical but for the experimental manipulation (i.e., whether it was described as intentional or unintentional). Table 2 presents the average marginal effects for these two sets of models for each of the three experimental contrasts. 4
Average Marginal Effects of Appraisal on Self-Rated Health.
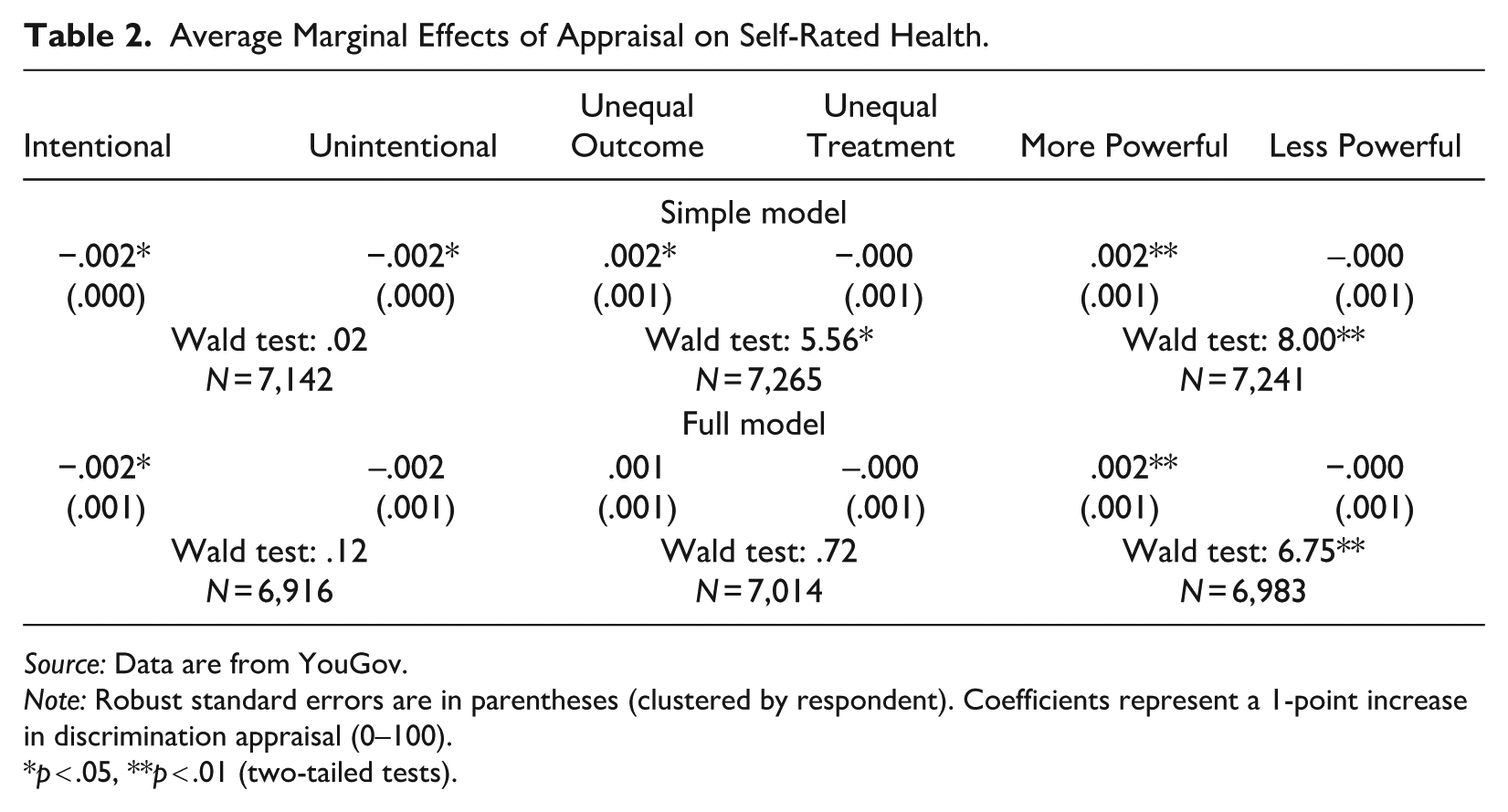
Source: Data are from YouGov.
Note: Robust standard errors are in parentheses (clustered by respondent). Coefficients represent a 1-point increase in discrimination appraisal (0–100).
p < .05, **p < .01 (two-tailed tests).
In examining the average marginal effects for the simple model (no sociodemographic controls), we find that a 1-point increase in appraisal score on the 0 to 100 scale is predictive of worse self-rated health in both the unintentional (b = −.002, p = .030) and intentional (b = −.002, p = .023) conditions. Unsurprisingly, the difference between the two coefficients is not significant, Wald test F(1, 1,979) = .02, p = .891. A 1-point increase in appraisal score for the unequal outcome condition is predictive of better self-rated health (b = .002, p = .016), whereas a 1-point increase in appraisal score for the unequal treatment condition is predictive of worse self-rated health, although the latter is not statistically distinguishable from zero (b = −.000, p = .460). The difference in these coefficients is statistically significant, F(1, 1,974) = 5.56, p = .019. Similarly, appraising discrimination when the individual in the vignette is White person, a man, or a member of the middle or upper class is predictive of better self-rated health (b = .002, p = .006), whereas appraising discrimination when the individual depicted is a racial minority, a woman, or from a lower social class background is predictive of worse self-rated health (b = −.000, p = .460). This difference is also statistically significant, F(1, 1,970) = 8.00, p = .005.
Prior work has established that individuals vary systematically in how they respond to perceived discrimination survey items, depending on their sociodemographic identity (Barkan 2018; Grollman and Hagiwara 2017, 2019; Harnois 2022; Harnois et al. 2019; Lewis et al. 2015). As expected, the inclusion of demographic controls in the models attenuates these results somewhat for all six experimental conditions; however, the directionality of the relationship between appraisal and health remains unchanged. As illustrated in both the regression results (see Appendix Table C1 in the online version of the article) and the marginal effects from the full models (shown in Table 2), the inclusion of demographic variables most substantively affects the comparison of the unequal outcome and the unequal treatment conditions such that the difference between the two are no longer significant. Thus, sociodemographic differences in appraising unequal outcomes versus unequal treatment as discrimination likely explain this variable’s relationship to health. 5 Nevertheless, in the full demographic model, results demonstrate that appraising discrimination when it is intentional continues to be predictive of worse self-rated health (b = −.002, p = .024) and that appraising discrimination when it affects more powerful individuals is significantly predictive of better self-rated health (b = .002, p = .002), even with the inclusion of sociodemographic controls. These results are depicted in Figure 3.
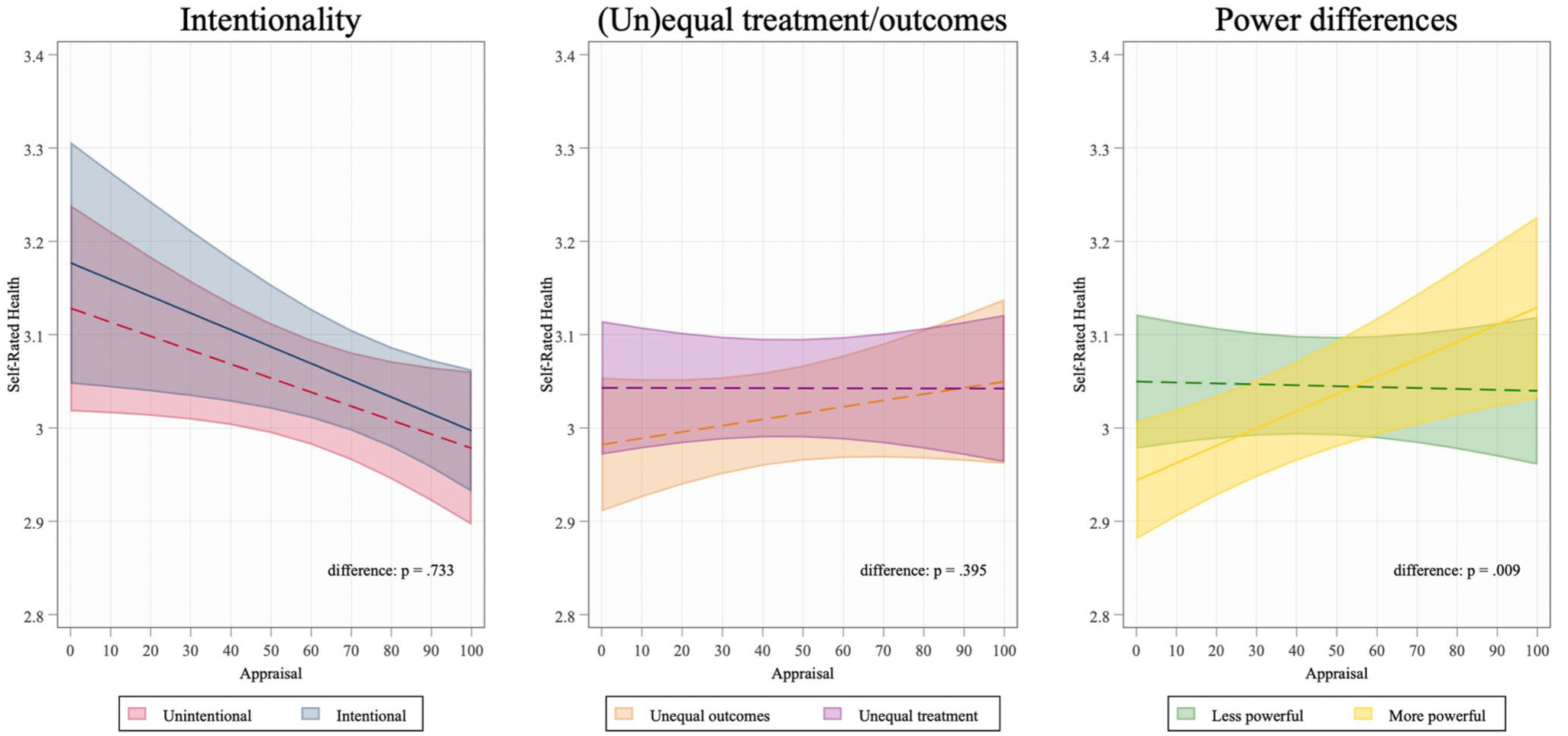
Relationship between Discrimination Definition and Self-Rated Health.
These effects are small in magnitude but substantive in impact. In the case of the intentional scenario, going from the 25th percentile in discrimination appraisal (rating it as a 15 on the 0–100 scale) to the 75th percentile (rating it as an 88 on the 0–100 scale) is equivalent to an additional 18.6 years of aging on health. In the case of the power differences scenario, going from the 75th percentile to the 25th percentile in discrimination appraisal is equivalent to an additional 19.1 years of aging on health. These estimates are based on the effect size of age on self-rated health in our sample (for results of control variables, see Table C1 in the Appendix in the online version of the article).
In the full model, we observe relationships between sociodemographic variables and health that are largely expected based on prior literature. For instance, we find that higher educational attainment is associated with better self-rated health, older individuals report worse health, and a higher income is associated with better self-rated health. Departing from prior literature, we do not observe ethnoracial differences in health in our sample, and we do not observe health differences between men and women—although gender nonbinary individuals report worse health, in line with emerging research on this population (Lagos 2019; Stacey, Reczek, and Spiker 2022). In addition, Democratic party affiliation is significantly associated with worse self-rated health across all three models, which is also consistent with earlier research (Pacheco and Fletcher 2015; Subramanian and Perkins 2010).
In summary, when we examine the relationship between self-rated health and appraisal in the full models, we find a significant negative relationship between health and appraising an event in which the discrimination was intentional. By contrast, we find a significant positive relationship between health and appraising an event in which the discrimination affects an individual from a more powerful group. Critically, these results hold even when controlling for other known sociodemographic variables that likely shape both discrimination appraisal and health (e.g., age, education, income, etc.). 6
Discussion
This study reveals the independent role of discrimination appraisals in shaping health and well-being for Americans. The present research complements findings from the large body of work showing the deep and enduring impacts of discrimination exposure and experiences on morbidity and mortality (Araújo and Borrell 2006; Bratter and Gorman 2011; Brown et al. 2000; Krieger et al. 2011; Lewis et al. 2015; Major et al. 2018; Pascoe and Smart Richman 2009; Phelan and Link 2015; Williams et al. 1997; Williams and Mohammed 2009). This study’s findings specifically underscore that the way that people define discrimination also plays a key part in shaping health. Yet our results do not neatly align with the prevailing two schools of thought regarding the impact of discrimination appraisals on health, in which appraisals are understood to either harm or protect health. Instead, we find that the relationship between discrimination appraisals and self-rated health depends on which situations a person identifies as discrimination. U.S. adults who see discrimination occurring in cases where it is intentional report worse health, whereas those who have a definition of discrimination in which more powerful individuals (White people, men, the middle and upper classes) can be discriminated against report better health.
Our first finding, regarding the negative relationship between appraisal and health for individuals who see discrimination in scenarios where it is intentional, can likely be explained by the heightened stress and vigilance associated with this definition of discrimination. These are individuals who are especially likely to agree that intentional behavior is discriminatory, such as a case where a hiring manager offers female candidates a lower starting salary because he does not like working with women. 7 People who readily identify scenarios like this one as discrimination probably notice more instances of discrimination occurring in the world around them and even their own lives, particularly compared to someone who does not as readily define these events as discrimination. As a result, they may experience more frequent activation of stress processes (Kaiser and Miller 2004) and vigilance-associated psychological fatigue (Himmelstein et al. 2015) that lead to worse overall health. Put differently, we find that those who do not label intentional events as discriminatory have comparatively better health. Ignorance, in this case, is bliss.
Our second finding, regarding the positive relationship between appraisal and health for those who see discrimination in scenarios where it affects White people, men, and the wealthy (as opposed to people of color, women, and the poor), can likely be explained by the salutary effect of endorsing, defending, and restoring the prevailing status quo of the existing power structures in the United States. By drawing attention to discrimination against the powerful, individuals can reinstate a status hierarchy where traditionally powerful groups remain on top due to their putative hard work, talent, or other meritocratic reasons. For instance, in our study, these are participants who are especially likely to see discrimination when men are underpaid relative to women despite working in the same position. They may see these scenarios as violating the status quo in which men generally do (or perhaps should) earn more than women.
Indeed, several studies have found that belief in a just world and system-justifying attitudes have palliative effects even when these beliefs are self-derogating (Harding and Sibley 2013; Napier et al. 2020; Sichel, Javdani, and Yi 2022). Wilkins et al. (2017) found that White participants experienced greater self-worth when they endorsed a belief in anti-White bias—a belief more likely to occur under conditions of racial progress (i.e., a disruption of the racial status quo). In fact, research finds that White individuals who believe in widespread reverse racial discrimination often have zero-sum beliefs, in which “they view gains for underrepresented groups as unfairly disadvantaging them” (Ballinger 2021:i). Thus, this definition of discrimination seeks to restore the status quo, ultimately justifying current inequities and power differentials. Doing so may help minimize the cognitive dissonance that occurs when inequalities occur in an ostensibly meritocratic society, thereby lowering stress and serving a health-protective function. Future research should work to unpack the mechanisms driving both of the relationships that we have uncovered in the present study.
Furthermore, our findings about the role of discrimination definition help contextualize other established patterns about perceived discrimination and gender- and race-based health disparities. For example, Schmitt et al. (2002) found that experiencing gender-based discrimination has negative effects on psychological well-being for women but not men. We would argue that this likely occurs because perceiving discrimination against traditionally more powerful (but not less powerful) groups like men can be health protective, for reasons outlined previously and because men are more likely to agree that men face discrimination. Similarly, Grollman and Hagiwara (2019) found that the relationship between perceived discrimination and health depends partly on question wording (i.e., “discrimination” vs. “unfair treatment”) and that this difference is concentrated among White individuals in particular. This is consistent with our argument that Americans define discrimination differently and that these definitions have diverging impacts on health. Last, Bratter and Gorman (2011) found that although perceived discrimination has a comparably negative impact on health for both Black and White Americans, racial awareness harms White—but not Black—individuals’ health. They note that future scholarship is needed to understand this pattern, with a focus on “the substance of thoughts about race or interactions that are perceived as discriminatory” (Bratter and Gorman 2011:378). The present study represents a direct response to this need by querying what Americans perceive to be discrimination and by examining those perceptions’ relationship to health.
Limitations
This study has three key limitations. First, the present study examined only three of the dimensions along which Americans define discrimination. Future scholarship can explore other dimensions, such as whether an individual perceives only individuals or also systems as capable of perpetrating discrimination, further building on the intersections of our findings with those of Sellers et al. (2011).
Second, it relies on a single indicator of health and well-being, self-rated health. Research has shown that self-rated health is a well-validated measure of health across populations (for ethnoracial comparisons, see Chandola and Jenkinson 2000; for gender comparisons, see Zajacova et al. 2017) and is highly predictive of morbidity and mortality outcomes (for reviews, see Idler and Benyamini 1997; Jylhä 2009). Nevertheless, there are some concerns of the long-term reliability of assessments of self-rated health within individuals (Zajacova and Dowd 2011). Given this limitation, future research should examine the relationship between various definitions of discrimination and a variety of more specific measures of health. For instance, scholars could examine the degree to which measures of mental health have distinct patterns compared to physical health (Krieger et al. 2011; Williams et al. 1997; Williams, Lawrence, Davis, and Vu 2019). Moreover, future work could examine specific health outcomes, such as chronic and acute stress biomarkers (e.g., resting heart rate, salivary cortisol, c-reactive protein levels, or blood pressure) or number of chronic health conditions or functional limitations (Warner and Brown 2011; Williams, Lawrence, Davis, and Vu 2019).
Third, our study design is cross-sectional in nature, so we are limited in our ability to make causal claims about these relationships. Some psychologists have proposed that individuals who perceive widespread discrimination and microaggressions may simply have higher levels of negative emotionality or greater race-based rejection sensitivity (e.g., Lilienfeld 2017; but see also Williams 2020). This would point the causal arrow in the other direction—suggesting that those in poorer health have higher stress levels, more negative emotions, and increased sensitivity to racist (or sexist or classist) slights, leading them to perceive more discrimination as a result. Our findings do not align with this perspective given that we find that increased propensity to label discrimination in certain scenarios (e.g., intentional cases) leads to worse health, yet labeling discrimination in other scenarios (e.g., when perpetrated against White people, men, the wealthy) leads to better health. Future work can overcome this limitation by collecting longitudinal data about the development of discrimination definitions as they impact health over the life course (for an innovative study in this vein using time diaries, see Deckard et al. 2023). Another option for future studies would be to intervene directly in people’s definition of discrimination and observe how that affects health markers such as stress or subjective well-being.
Implications
This work has key implications for research on discrimination and health. Theoretically, we have established the importance of discrimination appraisals in health and well-being, isolating these effects from those of discrimination experiences. Methodologically, our work highlights the degree to which existing measures of perceived discrimination (e.g., the Everyday Discrimination Scale, the Schedule of Racist/Sexist Events) are limited in their ability to capture the downstream consequences of discrimination on health. Emerging scholarship has demonstrated that people interpret these survey items differently (Barkan 2018; Grollman and Hagiwara 2017; Harnois 2022; Harnois et al. 2019; Lewis et al. 2012), arguing that more research is needed to better capture the multifaceted ways that people define discrimination in their lives. Our findings suggest that by better measuring how people “see” discrimination, scholars will be more equipped to understand the critical and complex impact of discrimination on health.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465251386416 – Supplemental material for Seeing Discrimination: How Different Definitions of Discrimination Relate to Health in U.S. Adults
Supplemental material, sj-docx-1-hsb-10.1177_00221465251386416 for Seeing Discrimination: How Different Definitions of Discrimination Relate to Health in U.S. Adults by Lauren Valentino and Evangeline Warren in Journal of Health and Social Behavior
Footnotes
Acknowledgements
A previous version of this work was shared at the Population Association of America’s 2023 Annual Meeting. The authors are grateful for research assistance from Julian Colbert, Chrissy Fite, Julia Grandinetti, Maya Kerr Coste, Sydney Longbottom, Grace Orians, and Heather Radcliffe. The authors wish to thank Cindy Colen, Trish Homan, and Bob Hummer for their helpful feedback on this project.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been generously supported by a Department of Sociology Seed Grant from The Ohio State University, an Institute of Population Research Seed Grant from The Ohio State University, which includes core support from the National Institutes of Health center grant P2CHD058484, awarded by the National Institute of Child Health and Human Development, and a Presidential Award from the Russell Sage Foundation (R-2111-34922).
Supplemental Material
Appendices A to C are available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.