
Abstract
This study investigates whether local social capital (neighbor networks and norms of trust/reciprocity) buffered the impact of mixing/mobility restrictions on psychological distress during the COVID-19 pandemic. It draws on two nationally representative panel surveys: the UK Household Longitudinal Study (UKHLS) Mainstage survey (n = 31,805 person-observations) and UKHLS COVID-19 survey (n = 22,933 person-observations), a subsample of the Mainstage survey respondents followed during the pandemic. Individual-level and (prepandemic/peripandemic) contextual-level local social capital indicators are tested. Longitudinal fixed-effects analyses indicate that distress increased with the onset of mixing restrictions, and peripandemic psychological distress increased more in areas experiencing greater spatial immobility (measured using Google spatial mobility data). However, increases in distress were significantly smaller among individuals reporting both higher individual and contextual social capital. Differences in social contact or neighborhood social support did not explain social capital’s buffering role. Results suggest social capital be considered a key element of crisis preparedness.
Extensive research has documented the negative impact of the COVID-19 pandemic on mental health (Bueno-Notivol et al. 2021). One pandemic stressor thought to be particularly detrimental for mental health is the restrictions on social mixing and reduced spatial mobility, especially via the impact they had on social isolation, loneliness, and stresses associated with confinement (Bierman and Schieman 2020; Chan et al. 2024; Laurence and Kim 2021). However, although extensive research has examined how the pandemic impacted mental health, less is known about what factors may have cushioned its impact on mental health.
“Stress buffering” (or “protective”) characteristics are those factors that cushion the negative impact of adverse life events on mental well-being (Cohen and Wills 1985). One factor that may have been especially effective for protecting mental health during the pandemic is social capital. Broadly speaking, social capital comprises “social networks [a structural component] and norms of reciprocity and trust [a cognitive component] that arise from them” (Putnam 2000:19; see also De Silva et al. 2005). Research documents the mental health benefits accrued from social capital (De Silva et al. 2005), such as social support, advice, and resources from networks (Kawachi and Berkman 2000), or a sense of group membership and self-esteem from its cognitive dimensions, such as belongingness or trust (Han and Chung 2023; Kawachi and Berkman 2000). Social capital has also been found to protect mental health from personal experiences of adversity (Aminzadeh et al. 2013; Zeng and Wu 2022) and cushion the harm caused by large-scale crises, such as natural disasters or recessions (Aldrich and Meyer 2014; Lindström and Giordano 2016).
Drawing on this work, this study explores the potential stress-buffering role of social capital during the COVID-19 pandemic, in particular, how far it protected individuals’ mental health from the impact of mixing/mobility restrictions and through what pathways any stress buffering operated. I suggest that local social capital—that is, networks and prosocial norms among neighbors—may have been especially effective for cushioning the impact of mixing/mobility restrictions. In addition, I argue that individuals’ own local social capital (e.g., how connected they are to their neighborhoods) and the stocks of local social capital in their wider residential community (e.g., average levels of neighbor connectivity in an area) should both evidence important stress-buffering properties. Drawing on two nationally representative UK panel data sets and applying both individual-level and (prepandemic/peripandemic) contextual-level indicators of local social capital, I investigate how far local social capital cushioned (a) prepandemic to peripandemic changes in mental health following the onset of mixing restrictions and (b) peripandemic changes in mental health in response to changing levels of local spatial mobility (measured using high-frequency Google spatial mobility data). In doing so, the study seeks to contribute to the sociological literature on mental health by robustly testing the stress-buffering role of local social capital during large-scale crises; providing novel insights into the relative importance of stocks of both individual-level and contextual-level local social capital for protecting mental health; and exploring the mechanisms through which any stress buffering operates.
Background
Local Social Capital as a Stress Buffer during the COVID-19 Pandemic
Social capital (networks and norms of reciprocity/trust embedded within them) can emerge from multiple (sometimes overlapping) sources, for example, schools, workplaces, families, online, or faith communities (Moore and Kawachi 2017; Putnam 2000). One source of social capital that has been shown to be both an important driver of positive mental health (Kawachi and Berkman 2000; Zangger 2023) and a buffering factor against stressors (Aminzadeh et al. 2013; Nakagomi et al. 2021) is social capital within neighborhoods, that is, social networks among neighbors and norms of reciprocity and mutual trust between them (henceforth termed “local” social capital) . Such local social capital is suggested to emerge from both formal ties, derived from associational involvement in local civic and social organizations, and informal ties, emerging from social connectivity among neighbors (Li, Pickles, and Savage 2005; Putnam 2000).
Several pathways are posited to account for the stress-buffering role of local social capital (Laurence 2025). Neighborhood social ties can provide access to instrumental, emotional, and informational support to manage the impact of adverse experiences on mental health, deemed efficacious, in part, due to their spatial proximity (Cohen and Wills 1985; Larnyo et al. 2024; Unger and Wandersman 1985). Indeed, research on natural disasters has shown that networks of trust/reciprocity among neighbors ameliorate harm and facilitate recovery during crises by providing “information, aid, financial resources, and child care along with emotional and psychological support” (Aldrich and Meyer 2014:256; see also Jung 2019; Lê et al. 2013; Lindström and Giordano 2016). Local social capital may also cushion mental health by increasing the likelihood that individuals get involved in providing support to others (Dederichs 2023), which can protect mental health by fostering a sense of purpose and identity, providing structure for people’s time, and generating greater social contact (Wang et al. 2022). Local social capital is also believed to cushion stressors via opportunities for sustained social interactions or brief, positive interactions (“daily uplifts”; McCullough, Huebner, and Laughlin 2000), which protect mental health through feelings of safety, belongingness, and stress reduction (Berkman et al. 2000; Thoits 2011).
Although social capital among neighbors is not the only source of social capital that likely mattered during the COVID-19 pandemic, it may have become particularly important for buffering the impact of restrictions on mixing and wider mobility. Public health measures, such as stay-at-home orders, physical distancing, and prohibitions on traveling outside of local areas, compounded by wider fears of infection, significantly reduced people’s social contact and their ability to access social and institutional support at a time of significant need (Kovacs et al. 2021; Long et al. 2022). This was likely a key driver of worsening mental health during the pandemic via increased loneliness, social isolation, and separation from social support (Bierman and Schieman 2020; Chan et al. 2024; Kovacs et al. 2021; Laurence 2025).
In response to such restrictions, local social capital may have become a key stress-buffering resource. First, given that restrictions on mixing separated people from their wider, nonlocalized networks, for many people, neighbors became one of the primary sources of in-person social support outside of their households; for example, neighbors could help those struggling with care work/homeschooling, shop to shield vulnerable people, or check in on neighbors at risk of isolation (Laurence and Kim 2021; Zangger 2023). Similarly, wider restrictions meant that neighbors were one of the only groups to whom people could provide support during the pandemic. In fact, during the first UK lockdown, help from neighbors was the second most frequent source of support (10% of people received help from neighbors), behind help from adult children (13%), and neighbors were the second most frequently helped group (17% reported helping neighbors), behind providing help to parents and/or grandparents (26%; University of Essex, Institute for Social and Economic Research 2021). Local social capital may thus have cushioned the impact of mixing restrictions via access to and opportunities to provide social support (Laurence, Russell, and Smyth 2024).
Second, as noted, a key pathway through which mixing restrictions likely harmed mental health is via reduced social contact, leading to social isolation and loneliness. However, both the network dimension (e.g., neighbor ties) and cognitive dimension (e.g., sense of neighborhood belonging) of local social capital can reduce loneliness (Bello et al. 2024; Laurence 2025; Nyqvist et al. 2016). Under restrictions on wider social mixing, where individuals’ lives were largely constrained to their local areas, neighbor connectivity may have become a vital compensatory form of social contact, providing some of the only social interactions available to reduce social isolation and loneliness, cushioning the impact of mixing restrictions on mental health.
What is less clear from the literature is the scale at which any stress-buffering role of social capital might have operated: at the individual-level or contextual level (Laurence and Kim 2021; Poortinga 2006). Some studies focus on social capital from a micro, or egocentric network, perspective, measuring it at the individual-level, under which it essentially forms a “private good,” where the health/stress-buffering benefits attributed to social capital are accrued by individuals based on self-reported levels, for example, how connected people are to their neighbors—henceforth labeled “individual” social capital (see e.g., Gilbert et al. 2013). Other studies conceive of social capital as a contextual resource (measured at the contextual level), which forms a “public good,” where the health/stress-buffering benefits are accessible to all members of the contextual unit (e.g., average connectivity among neighbors in an area)—henceforth labeled “contextual” social capital (Aminzadeh et al. 2013; Nakagomi et al. 2021). I suggest that during the COVID-19 pandemic, both individual and contextual local social capital may have buffered the impact of mixing restrictions on distress. Individuals with more trusting, reciprocal local ties are more likely to have had access to/opportunities to provide social support and greater opportunities for social contact. However, less connected individuals may still have benefited from living in areas with higher stocks of local social capital. For example, areas with denser, more trusting/reciprocal networks may have been better able to mobilize residents to check up on those more socially isolated neighbors or set up local support groups to provide help to all residents regardless of how connected they are.
Based on the aforementioned literature, I formulate three key hypotheses. First, the impact of social mixing restrictions and attendant patterns of reduced spatial mobility on psychological distress will be weaker among individuals with higher local social capital (Hypothesis 1). Second, I predict that both higher individual-level local social capital (e.g., individuals’ own degree of connectivity to local residents) and contextual-level local social capital (e.g., average levels of connectivity among residents in an area) will independently cushion the impact of mixing restrictions and reduced spatial mobility on psychological distress (Hypothesis 2). Third, individuals with higher (individual-/contextual-level) local social capital will experience a weaker impact of reduced spatial mobility on their mental health because they received/gave more neighbor social support (Hypothesis 3a) and because they experienced comparatively more social contact (Hypothesis 3b).
Evidence on the Role of Local Social Capital during the Pandemic
Research provides initial evidence that individual-level local social capital may have protected mental health during the pandemic. However, there are limitations with this work. Peripandemic cross-sectional studies identify positive associations between social capital and mental health as evidence of a cushioning role (Chen, Zou, and Gao 2021; Mannarini et al. 2022). However, without a comparable prepandemic estimate of the social capital/mental health relationship, it is difficult to determine whether it reflects a cushioning role of local social capital following the onset of pandemic stressors.
Stronger evidence comes from longitudinal studies showing that people with higher prepandemic individual-level local social capital experienced smaller negative changes in mental health over the pandemic (Han and Chung 2023; Laurence et al. 2024; Sato, Kondo, and Kondo 2022; Vacchiano and Valente 2023). However, using values of social capital fixed at their prepandemic level could bias analyses given that they may not reflect levels of social capital during the pandemic itself, especially given evidence that social capital declined during the pandemic (Bierman and Schieman 2020; Borkowska and Laurence 2021). Using fixed prepandemic values of social capital may also increase bias from unobserved time-invariant heterogeneity, such as personality traits.
Another issue is what pandemic-related stressors local social capital may have cushioned. Most longitudinal studies model the impact of the pandemic using period effects and imply that social capital cushioned the harm of social restrictions (Mannarini et al. 2022; Sato et al. 2022; Vacchiano and Valente 2023; Zangger 2023). However, the pandemic triggered multiple stressors, many of which local social capital could theoretically be cushioning. Where studies directly test if local social capital cushioned mixing restrictions, these tend to be self-reported measures of social withdrawal using cross-sectional data, potentially problematic because poorer mental health may have led to social withdrawal (Chen et al. 2021; Laurence and Kim 2021; Mannarini et al. 2022). In addition, most studies have focused on measuring the stress-buffering role of individual-level local social capital. It is therefore unclear at what level any apparent local social capital stress-buffering effect operated and whether contextual-level local social capital may also be important. Lastly, to my knowledge, no pandemic research has examined the pathways through which any stress-buffering role of local social capital worked. I aim to address these limitations.
Current Study
This study tests whether individual-level and contextual-level local social capital buffered the impact of social mixing restrictions and attendant reductions in spatial mobility on mental health during the COVID-19 pandemic. I take two complementary approaches to testing this question. The first approach examines whether local social capital cushioned prepandemic to peripandemic changes in mental health following the onset of mixing restrictions. I draw on two prepandemic waves and one peripandemic wave of the United Kingdom Household Longitudinal Study (UKHLS) Mainstage data and leverage temporal and spatial variance in the onset of indoor/outdoor mixing restrictions across UK areas (local authority districts [LADs]) to test how the onset of mixing restrictions shaped prepandemic to peripandemic changes in mental health, whether local social capital cushioned the impact of restrictions on mental health (Hypothesis 1), and whether individual- and contextual-level social capital exerted independent stress-buffering roles (Hypothesis 2).
Focusing on whether local social capital cushioned prepandemic to peripandemic changes in mental health with the onset of restrictions provides a strong test of its potential stress-buffering role. However, the onset of restrictions is a relatively coarse (binary) measure. Furthermore, research demonstrates how lockdowns often reduced mobility at their outset but mobility began recovering even while lockdowns were still in place (Joshi and Musalem 2021). In addition, fear of infection may have curtailed mobility outside of periods of restrictions. The second approach thus examines how far local social capital cushioned the impact of wider patterns of spatial immobility on mental health during the pandemic itself. To do so, I turn to a second data set, comprising three waves of the UKHLS COVID-19 study, which followed a subsample of individuals from the UKHLS Mainstage data during the pandemic, and apply high-frequency data from Google Community Mobility Reports on the duration of time people spent at home in an area. With this, I can test how changes in spatial immobility are linked to changes in mental health during the pandemic, whether local social capital cushioned the impact of increasing spatial immobility (Hypothesis 1), and whether individual-level and contextual-level social capital exerted independent stress-buffering roles (Hypothesis 2). In addition, I use this data set to test two potential explanatory pathways: whether any stress-buffering role of local social capital can be accounted for by greater social support among neighbors (Hypothesis 3a) or higher levels of social contact (Hypothesis 3b).
This dual approach helps address several issues with the current literature. I draw on longitudinal data, containing contemporaneous measures of local social capital in every wave, allowing me to account for time-invariant unobserved heterogeneity. I apply two external (non-self-reported) measures of mixing restrictions. I also test both individual-level and contextual-level indicators of local social capital together and directly test posited stress-buffering mechanisms.
Data and Methods
Data
The first data set employed was the longitudinal UKHLS Mainstage data (University of Essex, Institute for Social and Economic Research 2023), a nationally representative household panel survey, which recruited 40,000 households to take part in 2009, tracking the same individuals from Wave 1 (2009–2010) to Wave 13 (2021–2022). Interviews occurred over a two-year period (e.g., participants in Wave 12 were interviewed between January 2020 and December 2021). The UKHLS had an attrition rate of ≈50% between Waves 1 and 13 (the most recent wave), higher among younger people, ethnic minorities, and those with lower income or no qualifications (Cabrera Alvarez and Lynn 2023). This study used Waves 6, 9, and 12 of the Mainstage data, in which social capital indicators were included. Wave 12 (interviews conducted January 2020 to December 2021) captured the pandemic period. Wave 6 (January 2014 to December 2015) and Wave 9 (January 2017 to December 2018) captured two prepandemic waves. Longitudinal sampling weights were applied. Listwise deletion of missing data resulted in a final analytic sample of 31,805 person-observations over three waves.
The second data set was the UKHLS COVID-19 Study web survey (University of Essex, Institute for Social and Economic Research 2021). This data set tracked a subsample of participants from the UKHLS Mainstage survey over the COVID-19 pandemic. All panel members who participated in Waves 8 or 9 of the Mainstage survey were invited to take part in the COVID-19 study. The response to the initial April 2020 survey was around 48%, with 28% attrition between Waves 1 and 9 (the last wave). I used Waves 3 (June 2020), 6 (November 2020), and 8 (March 2021), during which social capital was measured. Longitudinal weights were applied, and listwise deletion of missing data resulted in a final longitudinal analytic sample of 22,933 person-observations. Several factors predicted whether Mainstage respondents participated in the COVID-19 study: Nonparticipants were more likely to be male and non-White, have lower qualifications, be younger, be in rented accommodation, not be living as a couple, and be unemployed. Longitudinal weights went some way toward accounting for differential nonresponse across groups. Additional robustness tests to account for bias from missingness were undertaken, yielding substantively similar results as outlined in the results section.
Both data sets contained identifiers of the LADs (average population ≈ 160,000 residents) in which respondents lived at the time of the interview. I matched additional data sources to the survey data sets at the spatial community (LAD) level (for details, see “Measures” section). Information on whether respondents were living in a LAD under mixing restriction ordinances at the time of interview were compiled from Institute for Fiscal Studies (2022) data. Information on LAD levels of spatial immobility were derived from Google Community Mobility Reports (Google LLC 2021). LAD-level covariate measures (e.g., socioeconomic disadvantage) were based on UK census data. LAD-level COVID-19 case data were based on UK government test data. 2 The study drew on two data sets to capture contextual (LAD level) local social capital. Prepandemic contextual social capital was measured using the UK Social Fabric Index (Tanner et al. 2020). Peripandemic contextual social capital was captured using publicly available data on the location of local pandemic support groups. 3
Measures
Pandemic impact and social restrictions
I took two approaches to measuring the impact of social mixing restrictions on mental health. The first approach tested the presence/absence of governmental ordinances restricting indoor/outdoor mixing in hospitality venues. I leveraged the fact that interviews in Wave 12 (the peripandemic wave) of the UKHLS Mainstage were conducted over a 24-month period (January 2020 to December 2021) and that government restrictions on mixing were in place at different times during this period. Mixing restrictions also differed across space given that the tier system of restrictions put in place by the government meant that outside of national lockdowns, restriction severity/timing also differed across spatial regions (LADs). Figure 1 shows the distribution of Wave 12 (pandemic-period wave) interviews by whether they fell on a period/in an area in which mixing was prohibited (0 = no indoor/outdoor mixing restrictions, 1 = indoor/outdoor mixing restriction in place). Mixing ordinances data were matched to respondents based on their interview date/LAD.
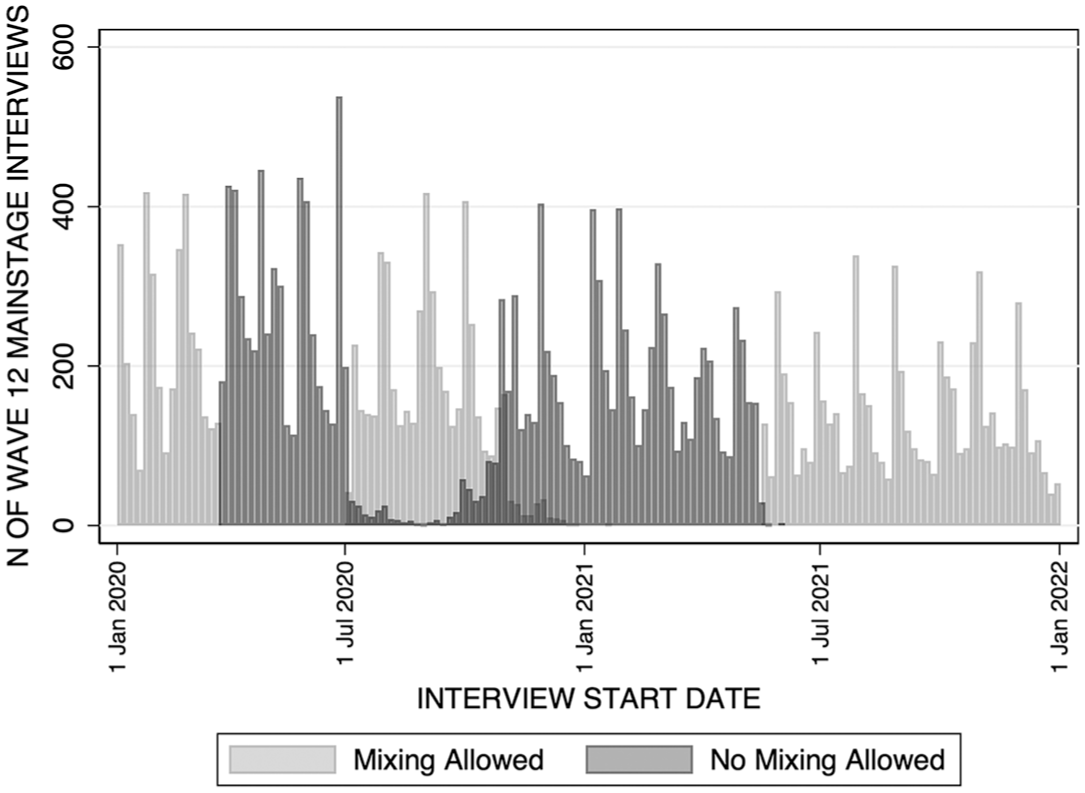
Distribution of United Kingdom Household Longitudinal Survey Mainstage Wave 12 Interviews That Fall within and outside of Periods of Social Restrictions.
The second approach drew on spatial mobility data from Google Community Mobility Reports (Chan et al. 2024; Google LLC 2021), which used data collected from devices connected to the internet with “location history” enabled. The data provided estimates of how much time people were spending at home during the pandemic in an area (LAD). For each day, they calculated the percentage change in the amount of time people spent at home compared to an equivalent pre-COVID-19 baseline day. 4 Separate daily estimates were available for each spatial region (LAD). For each day/region, I calculated rolling averages of change in spatial immobility based on the previous seven days. Given that these data were only collected during the pandemic, the mobility data were matched to respondents in the UKHLS COVID-19 study data based on respondents’ interview date/LAD of residence. The mobility data had limitations in that they were only gathered from people with internet-connected devices using Google products with “location history” turned on. This may bias the mobility data toward some demographic/socioeconomic groups.
Mental health
Mental health was measured using the General Health Questionnaire-12 (GHQ-12), capturing nonpsychotic psychological distress (Chandola et al. 2022; Lundin et al. 2016). Participants reported the extent to which they experienced 12 symptoms in the past few weeks, such as depression or anxiety (e.g., “been feeling unhappy and depressed,” “lost much sleep over worry”), using a four-category Likert response scale. I employed the Likert scoring method, which summed participants’ scores across all 12 items (ranging = 0–36), which has performed strongly in general populations (Lundin et al. 2016).
Individual and contextual local social capital
In the UKHLS Mainstage analysis, individual-level local social capital was captured using six self-report items from the Buckner (1988) scale of cohesion. This included dimensions of attachment to the neighborhood (“I plan to remain a resident of this neighborhood for a number of years”), degree of neighborhood interactions (“I borrow things and exchange favors with my neighbors,” “I regularly stop and talk with people in my neighborhood”), and psychological sense of community (“I think of myself as similar to the people that live in this neighborhood,” “I feel like I belong to this neighborhood,” “I would be willing to work together with others on something to improve my neighborhood”). These measures are frequently employed to capture individual-level local social capital (e.g., Johnston, Kung, and Shields 2021). Factor analysis demonstrated that the items loaded onto a single index (minimum factor loadings > .55; eigen value = 2.65; α = .82).
The UKHLS COVID-19 study contained two items from the aforementioned list (“I think of myself as similar to the people that live in this neighborhood” and “I regularly stop and talk with people in my neighborhood”) and three different items: “People in this neighborhood can be trusted,” “People around here are willing to help their neighbors,” and “People in this neighborhood generally don’t get along with each other” (reverse-coded). Factor analysis demonstrated that the items loaded onto a single index (minimum factor loadings > .55; eigen value = 2.38; α = .81).
I employed two largely external measures of contextual-level local social capital. The first measure was the “local relationships” dimension of the UK Social Fabric Index, which captures the degree of neighborliness and associational involvement in an area (Tanner et al. 2020). This index was composed of multiple indicators, measured at the LAD level, including per capita rates of community-owned shops or pubs, amateur sports clubs, charities and membership organizations, or neighborhood watch or residents’ associations. These data were taken from administrative data sources, such as the Department for Revenues and Customs, the Charity Commission, and Business Counts. The index also included indicators from the UKHLS Mainstage data, aggregated to the LAD level, including share of people who participate in a local organization, attend religious services, locally volunteered in the last year, and reported higher neighborliness (e.g., who agree that “this is a close-knit neighborhood”; Blagden and Valentin 2023). This index captured prepandemic contextual-level social capital based on 2018–2019 data.
This measure evinced good face and content validity, capturing both cognitive and structural dimensions of social capital (De Silva et al. 2005). In particular, measures of local civic/social engagement form key indicators of social capital (Putnam 2000), and the index was also composed of aggregate key indicators of neighborliness from the Understanding Society data. In addition, the indicators were focused specifically on the locality. Most indicators composing the index (e.g., density of civic/social organizations, frequency of local volunteering) also featured in more established measures of contextual social capital (e.g., Putnam’s [2000] social capital index). Although the UK Social Fabric Index itself has not been validated, other measures of contextual-level social capital containing similar indicators show good validity across a range of dimensions (Lee and Kim 2013). The index was also constructed using UK administrative data records, providing an important external measure of local social capital to help reduce endogeneity bias.
Given that the pandemic may have impacted levels of contextual-level social capital (e.g., prohibitions on mixing affecting civic/social engagement), the measure of prepandemic contextual social capital may not fully capture peripandemic levels of contextual social capital. Accordingly, I also applied a peripandemic-specific measure of contextual-level social capital that aimed to pick up expressions of local social capital relevant to the pandemic itself. To do so, I looked at the density of pandemic support groups set up by local residents (2020–2021). This measure was aligned with the concept of local social capital given that setting up local pandemic support groups and reaching individuals in need is predicted to be a key outcome of local social capital during crises, requiring both local networks and norms of reciprocity/mutual support (Aldrich and Meyer 2014). There was some evidence suggesting that density of pandemic support groups was an efficacious measure of peripandemic contextual-level local social capital. First, it was relatively strongly correlated with the prepandemic indicator of contextual-level local social capital, r = .55, suggesting that areas richer in social capital before the pandemic were more likely to come together to set up support groups. Second, research shows that although helping behaviors and local social capital more generally declined during the pandemic, a good predictor of whether individuals did engage in helping behaviors or maintained (or even increased) their local social capital was their levels of prepandemic social capital (Dederichs 2023; Zangger 2023). This further suggested that the emergence of pandemic support groups likely occurred more in areas with higher local social capital.
Pandemic support group data were available online, gathered from sources including social media, webpages, and self-submission. The data were not a complete list of all groups but remained the best possible source of information. Using the location of the support groups, I calculated the number of mutual aid groups per 10,000 people in an LAD. Data on contextual-level social capital measures were only available at a single point in time. Their levels were therefore fixed across all waves of the panel data (time invariant).
Explanatory pathways of social capital stress buffering
Two potential social capital stress-buffering pathways were examined. The first set of pathways looked at whether social capital may have cushioned the impact of the pandemic via higher levels of social contact. Respondents were asked: “In the last 4 weeks, how often have you met in person with friends and family who do not live with you?” (a seven-category Likert scale of “never” to “daily”). They were also asked, “In the last 4 weeks, how many different friends and family members from outside your household have you deliberately met up with?” (count variable).
The second set of pathways looked at whether social capital may have cushioned the pandemic via opportunities to give/receive material social support to/from neighbors (e.g., shopping, driving, cleaning). Respondents were asked: “Thinking about the last 4 weeks, did you provide help or support to family, friends, or neighbors who do not live in the same house/flat as you” and “Thinking about the last 4 weeks, did you receive support from family, neighbors, or friends who do not currently live in the same house/flat as you?” Respondents who answered “yes” were then asked if this help was from/to a “neighbor.” This provided binary (no/yes) measures of “received help from neighbors” and “provided help to neighbors.”
These two sets of measures were only available in the UKHLS COVID-19 study. In addition, social contact measures were only available in Waves 3 and 6, and social support measures were only available in Waves 1 and 6. I therefore interpolated Wave 3 support values using Wave 1 values (one and a half months between Waves 1 and 3).
Covariates
UKHLS Mainstage data models accounted for respondents’ sex, ethnicity, whether they were born in the United Kingdom, age, disability status, tenure, number of children in the household, whether they were living in a couple, marital status, employment status, household income, subjective financial situation, and highest qualification. A more limited number of covariates was available in the UKHLS COVID study data. This included age; employment status; living with a partner; number of household members ages 0 to 4, ages 5 to 15, and ages 70+ (excluding respondents); and whether they had COVID-19 symptoms.
Models also adjusted for community-level variables, including urban/rural location, COVID-19 case rate per 1,000 at the time of interview (LAD level), LAD-level measures of the proportion ages 65+, and two indices of socioeconomic disadvantage: an index of economic disadvantage (percentage in social housing, percentage unemployed, percentage female, lone-parent households) and an index of social disadvantage (percentage without degrees, percentage not in managerial and professional roles). 5 Apart from case rates, repeated LAD covariate data were not available at a frequency that I could match onto different waves of the panel data sets. These variables were therefore fixed at the same level across waves (time invariant).
All models also contained period dummy variables and LAD fixed effects. For distributions of variables in the data, see Appendices S.2 and S.3 in the online version of the article.
Analysis Plan and Estimation Strategy
I undertook three sets of analyses. The first set used UKHLS Mainstage data to test how the onset of ordinances against indoor/outdoor mixing shaped GHQ-12, employing interaction terms between individual-level/contextual-level local social capital and mixing ordinances to test for stress-buffering processes. Linear individual fixed-effects models accounted for time-invariant unobserved heterogeneity. Given that contextual-level local social capital was fixed across waves (time invariant), its direct effect dropped out of fixed-effects models, but mixing restrictions/contextual-level local social capital interaction terms tested whether the impact of restrictions on GHQ-12 differed by levels of contextual local social capital.
The second set of analyses tested the cushioning role of local social capital during the pandemic itself using the UKHLS COVID-19 Study data, 6 testing the impact of changes in spatial immobility (LAD level). An interaction term between LAD spatial immobility and individual-level/contextual-level local social capital examined the posited stress-buffering role of social capital. Linear individual fixed-effects models were employed. I applied two measures of contextual-level local social capital: prepandemic neighborliness/associational involvement and peripandemic density of mutual aid groups. The third set of analyses tested whether social contact and neighbor support accounted for any observed stress-buffering role of social capital during the pandemic (restricted to Waves 3 and 6 of the UKHLS COVID-19 Study). Quadratic terms for social capital were tested given evidence of nonlinear social capital/mental health relationships (e.g., Kirkbride et al. 2014) . Table 1 summarizes the data sets used, time periods covered, and details of the measures applied for each set of analyses.
Summary of Data and Measures of Analytical Approach.
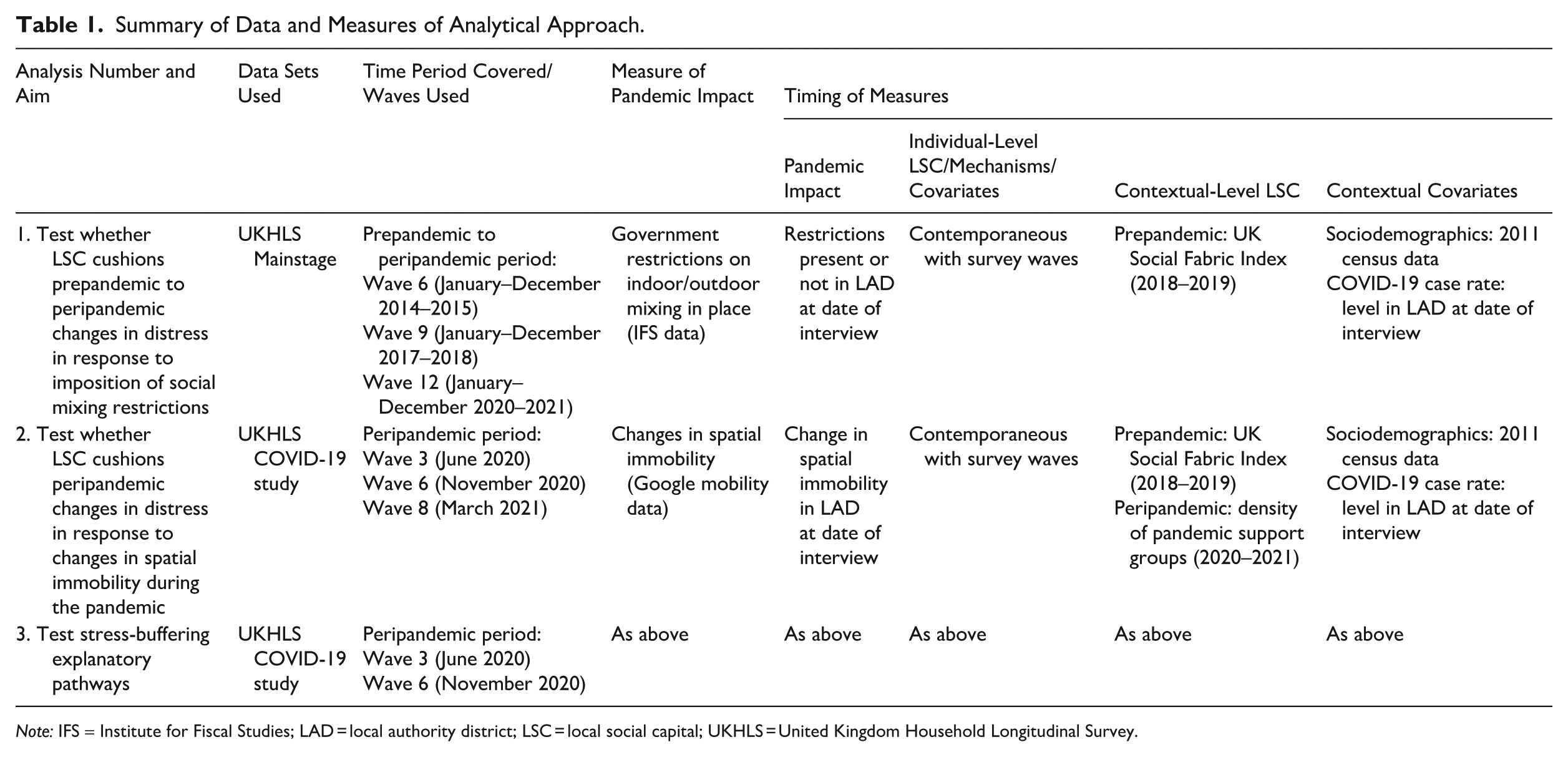
Note: IFS = Institute for Fiscal Studies; LAD = local authority district; LSC = local social capital; UKHLS = United Kingdom Household Longitudinal Survey.
Results
Mixing Restrictions, Mental Health, and the Role of Local Social Capital
The first analytic stage uses the UKHLS Mainstage data to directly test the impact of prohibitions on meeting indoors/outdoors on prepandemic to peripandemic changes in GHQ-12. As mentioned, I leverage the fact that UKHLS Wave 12 interviews were conducted between January 2020 and December 2021 and that during this period, social restrictions varied across time/space. Table 2 shows the results of linear fixed-effects regression models (for full results, see Appendix S.4 in the online version of the article).
Fixed-Effects Linear Modeling of Relationships between the Onset of Mixing Restrictions Ordinances, GHQ-12, and Individual-/Contextual-Level Local Social Capital.
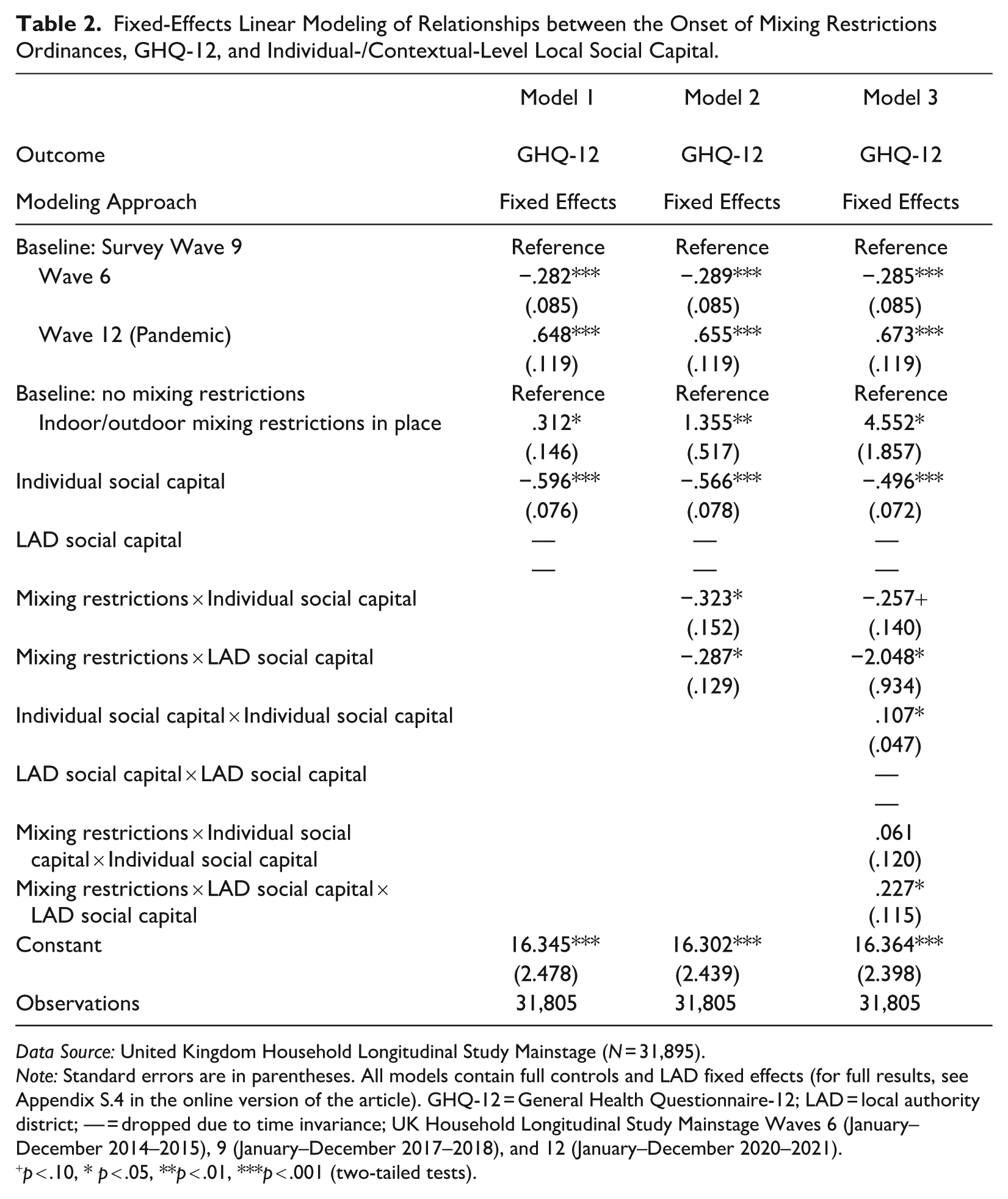
Data Source: United Kingdom Household Longitudinal Study Mainstage (N = 31,895).
Note: Standard errors are in parentheses. All models contain full controls and LAD fixed effects (for full results, see Appendix S.4 in the online version of the article). GHQ-12 = General Health Questionnaire-12; LAD = local authority district; — = dropped due to time invariance; UK Household Longitudinal Study Mainstage Waves 6 (January–December 2014–2015), 9 (January–December 2017–2018), and 12 (January–December 2020–2021).
p < .10, * p < .05, **p < .01, ***p < .001 (two-tailed tests).
Examining first the overall trends in GHQ-12, Model 1 period effects demonstrate that mental distress was significantly higher in the pandemic period (Wave 12: January to December 2020–2021) than in the prepandemic period (Wave 9: January to December 2017–2018). 7 In addition, the prepandemic to peripandemic increase in GHQ-12 (Wave 9 to Wave 12 change: +.648 points) represents a larger increase in GHQ-12 than the prepandemic, Wave 6 to Wave 9 trend in GHQ-12 (January to December 2014–2015 to January to December 2017–2018: +.282 points), suggesting that the pandemic period increase is not simply a continuation of an upward trend.
Turning to local social capital and the impact of mixing restrictions, Model 1 demonstrates that increases in individual-level local social capital are associated with decreases in GHQ-12 scores and that the onset of mixing restrictions is associated with a significant increase in GHQ-12 scores (+.312 points), even after accounting for period trends. Model 2 then tests whether social capital may have cushioned the impact of mixing restrictions via interaction terms between restrictions and individual-level or contextual-level local social capital. Regarding individual-level social capital, the interaction term is significant and negative, suggesting that the onset of restrictions had a significantly weaker positive association with GHQ-12 among individuals with higher individual-level local social capital (Model 2). Model 3 tests whether this moderating association is nonlinear (interaction between a quadratic term for individual-level local social capital and mixing restrictions), which is nonsignificant. Figure 2 plots the marginal effects of mixing restrictions across 11 percentiles of individual-level local social capital (5th to 95th; based on Model 2, Table 2). At low levels of local social capital, mixing restrictions have a significant positive association with GHQ-12. However, as local social capital increases, this positive association weakens until the 40th to 50th percentiles, above which the onset of mixing restrictions no longer has a significant association with GHQ-12.
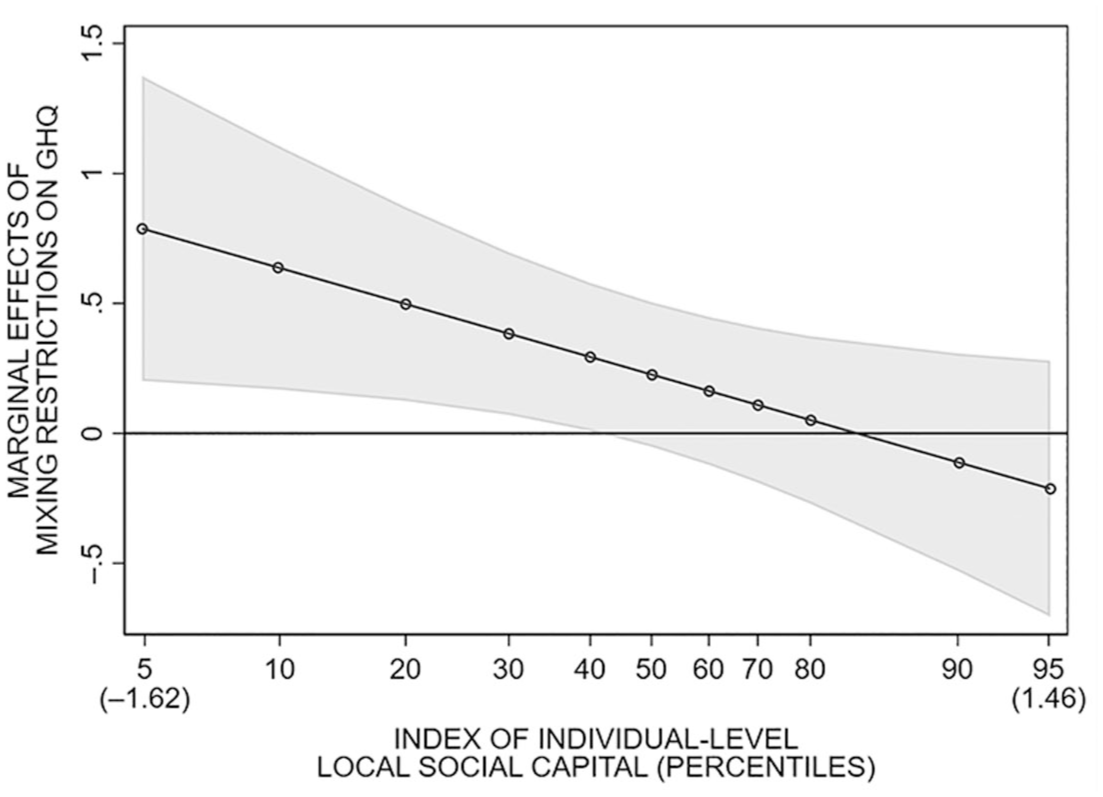
Marginal Effects of Social Mixing Restrictions on GHQ-12 by Level of Individual-Level Local Social Capital.
Turning to contextual-level local social capital, Model 2 demonstrates that the interaction term between mixing restrictions and contextual-level social capital is also significant and negative (i.e., the positive association between mixing restrictions and GHQ-12 is weaker among respondents living in LADs with higher prepandemic contextual-level local social capital). Model 3 then tests whether the moderating role of contextual-level social capital is nonlinear via an interaction between a quadratic contextual-level social capital term and mixing restrictions. This interaction term is significant and positive, whereas the negative linear contextual-level social capital/mixing restrictions interaction term becomes stronger and more significant. Figure 3 explores this nonlinear moderating relationship, plotting the marginal effects of mixing restrictions across 11 percentiles of contextual-level local social capital (5th to 95th; based on Model 3, Table 2). At low contextual-level social capital, mixing restrictions have a strong, significant positive association with GHQ-12. This association then decreases up to the 30th/40th percentiles of contextual-level social capital, after which it becomes nonsignificant.
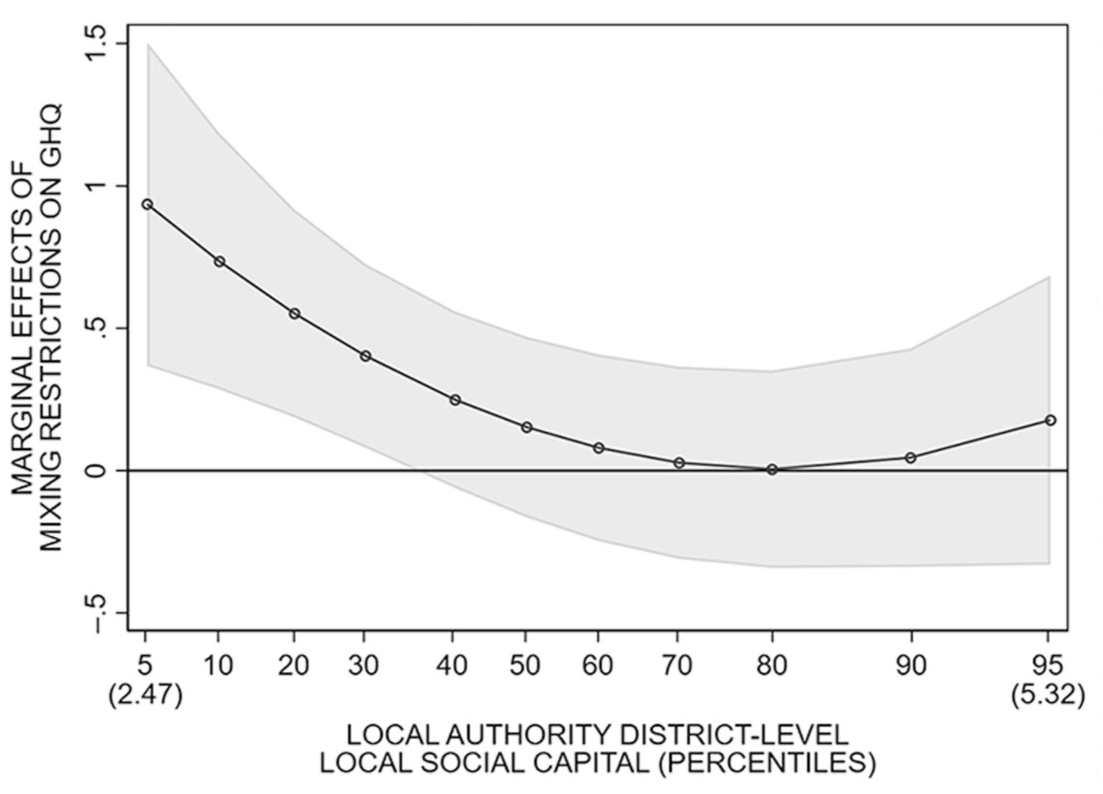
Marginal Effects of Social Mixing Restrictions on GHQ-12 by Level of Contextual-Level (Local Authority District) Local Social Capital.
Taken together, these findings suggest local social capital appeared to cushion the impact of mixing restrictions (evidence for Hypothesis 1) and that both individual- and contextual-level local social capital exerted independent stress-buffering roles (evidence for Hypothesis 2). Testing shows that the significant interactions between mixing restrictions and individual-/contextual-level social capital remain even after including interaction terms between mixing restrictions and all other individual- and LAD-level covariates, including time-invariant covariates (results available on request due to number of models). In addition, Model 1 (Table 2) was rerun but using individual-level local social capital as the outcome and GHQ-12 as the moderator. However, the mixing restrictions/GHQ-12 interaction term was not statistically significant (see Appendix S.5 in the online version of the article).
Spatial Immobility, Mental Health, and the Role of Local Social Capital
The second analytic stage turns to the UKHLS COVID-19 Study data to test how changes in spatial immobility in an area during the pandemic itself are associated with changes in GHQ-12 (using Waves 3, June 2020; 6, November 2020; and 8, March 2021). Spatial immobility is measured using Google Community Mobility Reports, capturing the seven-day rolling average change in the duration of time people in an LAD spent at home.
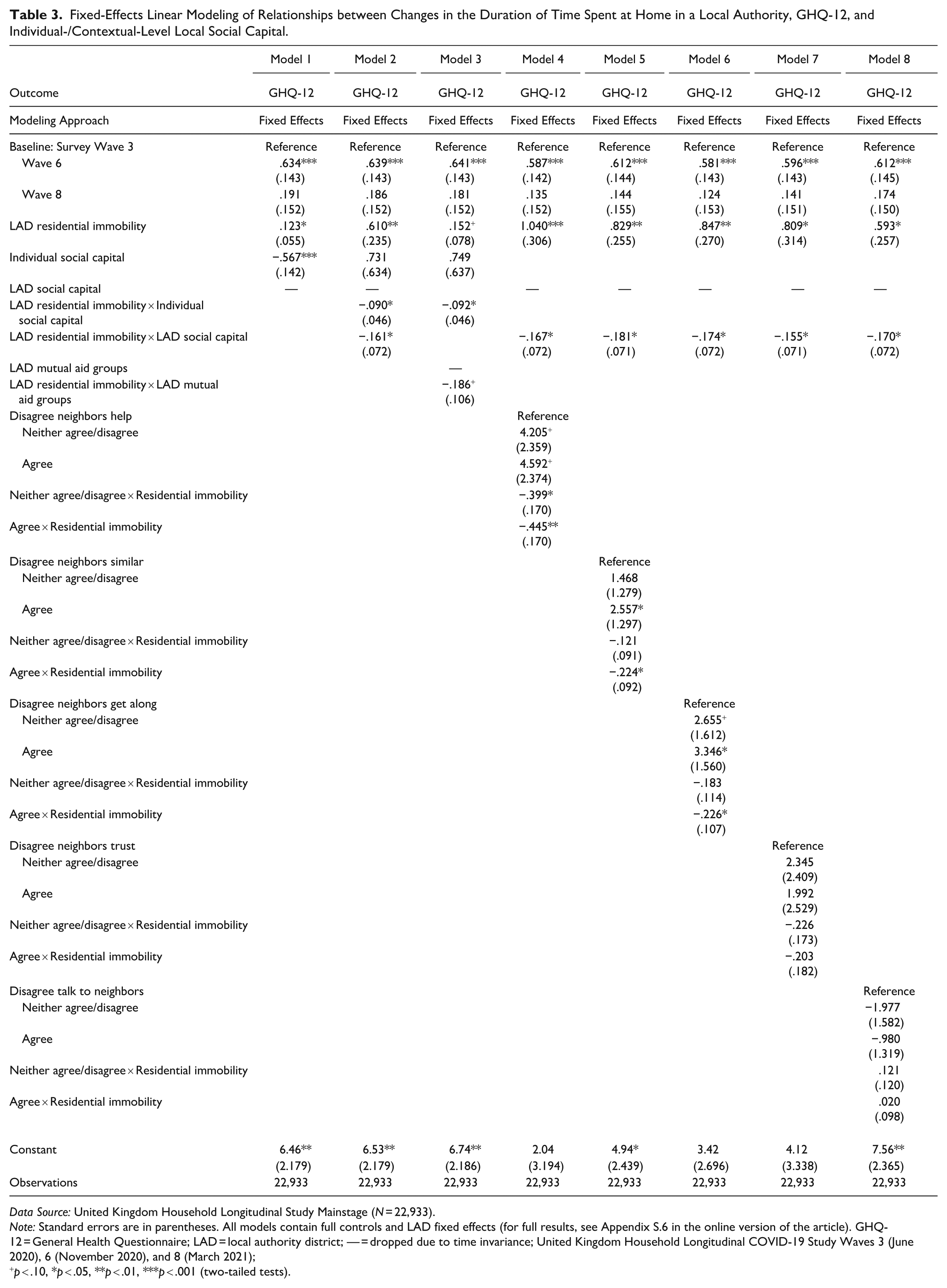
Table 3 shows the results of linear fixed effects regression models (for full results, see Appendix S.6 in the online version of the article). Model 1 (Table 3) demonstrates that increases in spatial immobility are associated with increases in GHQ-12. Model 1 also demonstrates how individual-level local social capital has a significant and negative association with GHQ-12, suggesting that even across the pandemic itself, increasing individual-level local social capital is associated with decreasing GHQ-12. Model 2 then tests whether the association between spatial immobility and mental health may be moderated by individual-/contextual-level local social capital. The interaction terms between spatial immobility and both individual- and (prepandemic) contextual-level social capital are significant and negative, suggesting that spatial immobility had a weaker positive association with GHQ-12 among individuals with more individual-/contextual-level social capital. Tests for whether this moderating relationship was nonlinear were nonsignificant.
Fixed-Effects Linear Modeling of Relationships between Changes in the Duration of Time Spent at Home in a Local Authority, GHQ-12, and Individual-/Contextual-Level Local Social Capital.
Data Source: United Kingdom Household Longitudinal Study Mainstage (N = 22,933).
Note: Standard errors are in parentheses. All models contain full controls and LAD fixed effects (for full results, see Appendix S.6 in the online version of the article). GHQ-12 = General Health Questionnaire; LAD = local authority district; — = dropped due to time invariance; United Kingdom Household Longitudinal COVID-19 Study Waves 3 (June 2020), 6 (November 2020), and 8 (March 2021);
p < .10, *p < .05, **p < .01, ***p < .001 (two-tailed tests).
Model 3 substitutes the measure of prepandemic contextual-level social capital for a measure of peripandemic contextual-level social capital (LAD density of mutual aid groups). The interaction term with residential immobility is negative and significant (at the p < .1 level). 8 Despite the weaker statistical significance, this result is substantively important. 9 Taken together, these results provide evidence that even across the duration of the pandemic, local social capital appears to have cushioned mental health from the impact of reduced spatial mobility (evidence for Hypothesis 1) and that both individual- and prepandemic/peripandemic contextual-level social capital played important stress-buffering roles (evidence for Hypothesis 2).
Models 4 to 8 explore which dimensions of individual-level local social capital have the strongest moderating association with spatial immobility, testing the role of each dimension separately. How far individuals agree/disagree (a) that “people in their area are willing to help their neighbors,” (b) that they “feel similar to the people that live in their neighborhood,” and (c) that “people in their neighborhood generally get along with each other” exhibit the strongest moderating associations (Models 4–6). Whether people agree that “people in their neighborhood can be trusted” exhibits a similarly sized moderating association, although this difference is not statistically significant at the p < .05 level (Model 7). 10 Model 8 demonstrates no significant difference in the spatial immobility/GHQ-12 association across how much individuals “regularly stop and talk with people in my neighborhood.”
Figure 4 plots the marginal effects of increases in spatial immobility among those who agree, neither agree nor disagree, and disagree with each local social capital indicator (based on their corresponding Models 4–8, Table 3). Figure 4 shows how spatial immobility has no significant association with GHQ-12 among individuals who agree that their neighbors are willing to help one another, that their neighbors get along, and that they are similar to their neighbors. Spatial immobility also has a weaker, positive association with those who neither agree/disagree with these statements about their neighborhoods. However, spatial immobility has a strong and significant positive association with distress among those who disagree that their neighbors help, get along with one another, or that they are similar to their neighbors. There is a similar pattern for neighbor trust, although the differences are not statistically significant, but little difference across those who agree/disagree they regularly talk to their neighbors.
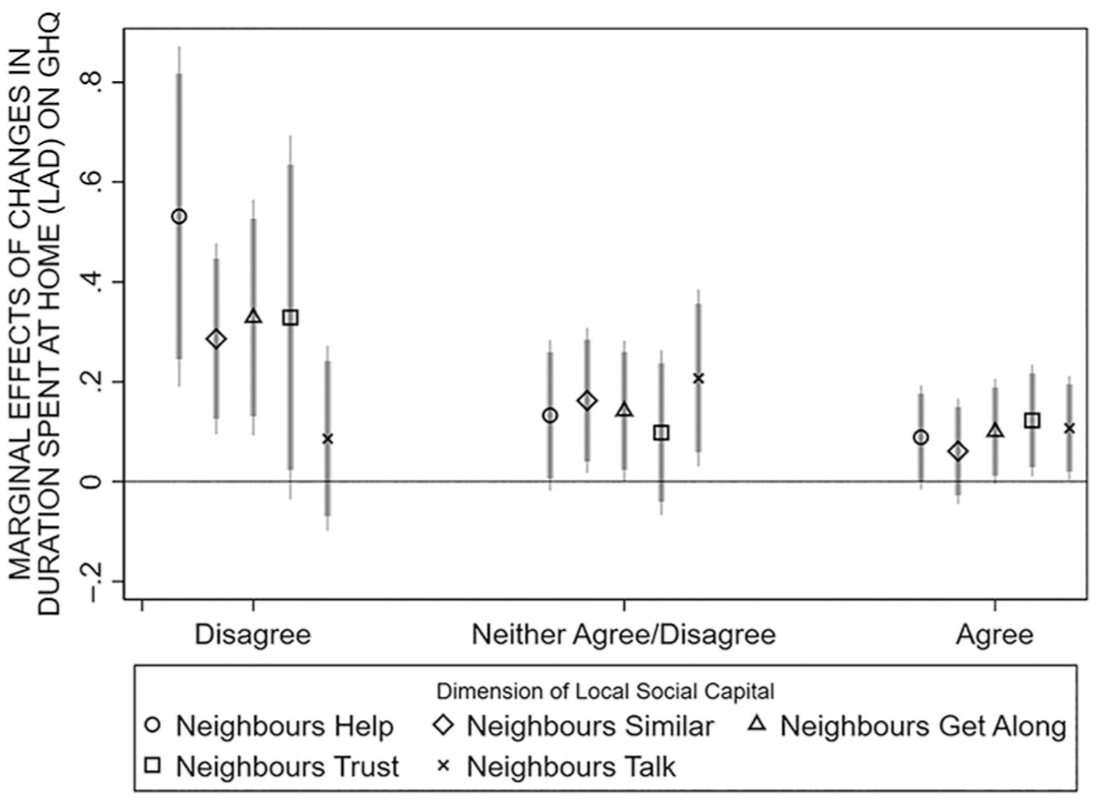
Marginal Effects of Changes in Duration Spent at Home in Local Authorities on GHQ-12 by Level of Individual-Level Local Social Capital.
There is no evidence that the moderating roles of individual-/contextual-level social capital were being driven by other time-variant/invariant characteristics (results available on request). In addition, there was no evidence that the findings were driven by mental health buffering the association between spatial immobility and local social capital (see Appendix S.7 in the online version of the article).
Explaining the Stress-Buffering Role of Local Social Capital
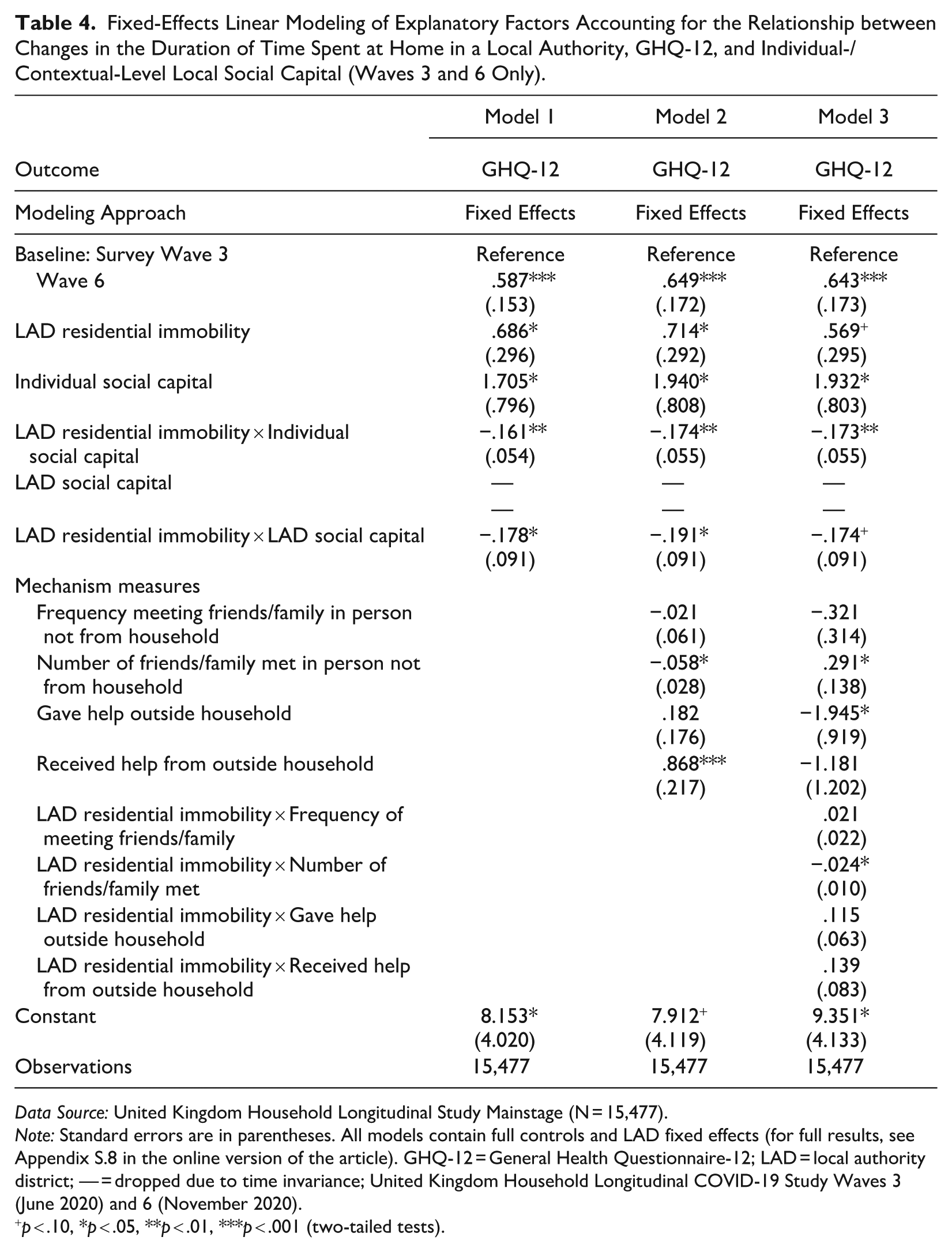
The proceeding section explores what pathways might explain the apparent stress-buffering role of local social capital. This analysis is restricted to UKHLS COVID-19 Study Wave 3 (June 2020) and Wave 6 (November 2020). Table 4 shows the results of linear fixed-effects regression models (for full results, see Appendix S.8 in the online version of the article).
Fixed-Effects Linear Modeling of Explanatory Factors Accounting for the Relationship between Changes in the Duration of Time Spent at Home in a Local Authority, GHQ-12, and Individual-/Contextual-Level Local Social Capital (Waves 3 and 6 Only).
Data Source: United Kingdom Household Longitudinal Study Mainstage (N = 15,477).
Note: Standard errors are in parentheses. All models contain full controls and LAD fixed effects (for full results, see Appendix S.8 in the online version of the article). GHQ-12 = General Health Questionnaire-12; LAD = local authority district; — = dropped due to time invariance; United Kingdom Household Longitudinal COVID-19 Study Waves 3 (June 2020) and 6 (November 2020).
p < .10, *p < .05, **p < .01, ***p < .001 (two-tailed tests).
Model 1 (Table 4) reestablishes the main model demonstrating how individual-/contextual-level social capital moderate the association between residential immobility and GHQ-12. Model 2 tests whether the weaker spatial immobility–mental health association among respondents with higher local social capital is because they had more social contact with friends/family or gave/received more neighbor support by including these measures in the model. Individuals who met up with a higher number of contacts outside the household during the pandemic reported lower GHQ-12, although seeing friends/family more frequently was not associated with GHQ-12. Meanwhile, people who provided help to neighbors saw no difference in GHQ-12, whereas those who received help from neighbors saw higher GHQ-12. However, the individual-/contextual-level social capital moderating associations remain significant.
Another mode by which contact/support may explain the stress-buffering role of social capital is that people with higher individual-/contextual-level local social capital had more social contact/neighbor support and that it is greater contact/neighbor support that moderates the spatial immobility–GHQ-12 relationship. Model 3 includes interaction terms between residential immobility and each contact/support measure. The interaction between immobility and nonhousehold friends/family contact is significant and negative, suggesting that social contact with friends/family also cushioned the impact of residential immobility; none of the remaining interactions are significant. However, the individual-/contextual-level social capital moderating relationships remain largely unchanged. Taken together, this provides evidence against Hypothesis 3a/3b.
Robustness and Causal Identification
Several further robustness tests were conducted. Multiple imputation was used to address missingness, and bespoke longitudinal weights were tested, which account for differential attrition by local social capital and mental health (see Appendices S.9a and S.9b in the online version of the article). Broadly consistent results were returned. Alternative indicators of disadvantage were applied (e.g., income, health, crime, access to services; see Appendix S.10 in the online version of the article), as was access to green spaces (see Appendix S.11 in the online version of the article). The substantive findings remained unchanged. Measures of contextual-level local social capital based on aggregating individual-level local social capital responses to the LAD level were also tested but were nonsignificant (see Appendices S.12a and S.12b in the online version of the article).
There remains the risk that reverse causality accounts for the findings, especially the individual-level local social capital–mental health relationship. To explore further evidence that at least part of the individual-level local social capital–mental health association emerges from the former affecting the latter, I employed a two-step system generalized method of moments (Arellano-Bond) estimator, which can help address endogeneity stemming from reverse causality (Arellano and Bond 1991; Leszczensky and Wolbring 2022). The results provide some further evidence that individual-level local social capital likely affects mental health (see Appendix S.13 in the online version of the article). However, challenges remain, preventing strong claims of causal identification.
Discussion
This study aimed to examine the protective role of individual- and contextual-level local social capital for mitigating the potential harm of mixing restrictions and attendant spatial immobility on psychological distress during the COVID-19 pandemic. I observe that psychological distress increased substantially during periods of restrictions on social mixing and in areas when the amount of time people spent in residential settings increased. These associations were significant even after adjusting for pandemic period effects, suggesting mixing restrictions acted as one complementary pathway through which the pandemic harmed mental health. However, both individual- and contextual-level local social capital appeared to buffer these negative impacts.
First, prepandemic to peripandemic, psychological distress increased much less with the onset of mixing restrictions among individuals with higher individual-level local social capital and those living in areas with higher contextual-level local social capital. Second, during the pandemic itself, changes in spatial immobility in an area had a weaker positive association with distress among those with higher individual- and (prepandemic or peripandemic) contextual-level local social capital. The study tested two potential explanatory pathways: social contact and neighbor social support. Although more contact with friends/family during the pandemic was associated with decreasing psychological distress and also appeared to cushion the positive association between spatial immobility and distress, neither social contact nor neighbor support could explain the stress-buffering roles of local social capital.
The study makes several important contributions. It provides robust insights into the protective role of individual-level local social capital during crises, adding to studies demonstrating its protective role during the pandemic (Han and Chung 2023; Laurence et al. 2024). It also shows how contextual-level local social capital (both prepandemic neighborliness/associational involvement and peripandemic density of mutual aid groups) played a buffering role, even after accounting for people’s individual-level local social capital. This contributes to the literature highlighting the importance of contextual-level social capital for protecting mental health during other types of large-scale crises (Jung 2019; Lê et al. 2013; Lim and Laurence 2015; Lindström and Giordano 2016). Together, these findings suggest that local social capital as a property of both individuals and wider contexts can simultaneously play important stress-buffering roles (Laurence and Kim 2021).
The study also suggests how contextual-level social capital is measured shapes our understanding of its role, especially whether measures are constructed from aggregating individual survey responses to the local level (e.g., Sato et al. 2022) or using external indicators of social capital, such as the density of civic groups (e.g., Laurence and Kim 2021). I find that although external measures of contextual social capital evidence stress-buffering roles, the aggregated survey responses measure did not.
Some insights can also be derived into the pathways through which local social capital protected mental health. Neighbor social support is often cited as a key stress-buffering pathway. However, giving/receiving support to/from neighbors (e.g., shopping for someone, providing lifts with the car) did not account for the buffering role of local social capital. Indeed, respondents who received help from neighbors reported higher psychological distress (potentially driven by more distressed people requiring more support). One possibility is that the neighbor support measures applied largely capture instrumental support and not more emotional/psychological support and that the quality of this crisis meant that material support (often a key need in natural disasters) was potentially somewhat less important than emotional support (Aldrich and Meyer 2014; Larnyo et al. 2024). Furthermore, I still show that the strongest moderating component of individual-level local social capital during the pandemic was whether respondents believed “people in their area are willing to help their neighbors” and that density of pandemic support groups also protected mental health (Figure 4). This suggests that all forms of material and non-material social support may not be currently captured in the models. Alternatively, it may be that perceiving that support is available, even when not necessarily needed, is critical for cushioning the impact of stressors. In this way, networks/norms of reciprocity and support among neighbors may act as a form of “informal insurance” that people feel that they can access, even if they do not need draw on it, which might contribute to people’s sense of security, certainty, and control over life, which would further protect people against depressive symptoms, especially during the pandemic (Aldrich and Meyer 2014; Han and Chung 2023; Laurence 2025:409).
Another posited pathway was greater social contact. However, meeting up with friends/family outside of the household did not account for the apparent cushioning role of local social capital. In addition, frequency of interacting with neighbors alone did not appear to cushion the impact of spatial immobility on mental health (Figure 4), even though talking to neighbors more frequently was associated with lower psychological distress. These results suggest that the network dimension of local social capital alone does not buffer adversity but that cognitive components, such as norms of reciprocity, are an important stress-buffering component of local networks.
Although these findings cannot empirically identify the pathways through which local social capital cushioned mental health, they suggest that exploring different forms of social support (e.g., emotional/psychological) and other psychological resources posited to emerge from local social capital, such as resilience (Laurence 2025; Zhang, Brown, and Rhubart 2023), might help better understand the pathways of stress buffering. Interestingly, these findings also demonstrate that other forms of social capital, namely, friend/family networks, also appeared to cushion the impact of mixing restrictions but that social capital embedded in people’s local areas (local social capital) continues to operate alongside these broader networks, highlighting the independence of different forms of social capital for stress buffering.
The study also sheds light on which groups/areas might be less protected from the impact of crises on their mental health due to lower local social capital. Socioeconomically disadvantaged groups are generally found to have lower individual-level social capital. However, factors broadly related to life stage also appear important, with retirees, those with more children, older age groups, those in owned homes, living with a partner, and living in areas with a higher share of over 65-year-olds all reporting higher individual-level social capital. Some of these groups also suffered larger declines in social capital over the pandemic, including younger age groups, residents of disadvantaged areas, and lower skilled workers (Borkowska and Laurence 2021). The findings therefore suggest that investing in society’s social infrastructure, particularly among people/places with lower local social capital and who are more at risk to its erosion during crises, is critical in preparations for future crises (Aldrich and Meyer 2014; Borkowska and Laurence 2021).
Despite these insights, there are several limitations. First, although the modeling approach accounted for time-invariant unobserved heterogeneity, time-variant unobserved heterogeneity may continue to bias the estimates of individual social capital. Relatedly, data on contextual-level social capital were only available at a single point in time (time invariant), increasing the risk of bias from unobserved time-invariant heterogeneity. The contextual social capital measures were also only available at the LAD level, and there is likely to be heterogeneity in levels of local social capital across smaller areas within LADs.
Bias from reverse causality also remains a key issue. Testing suggested that it is not the case that the results are simply picking up how mental health moderated the impact of the pandemic on social capital. However, the direct association between individual-level indicators of social capital and mental health could be solely a result of reverse causality. Additional modeling using the Arellano-Bond estimator provides some stronger evidence that at least part of the association may result from individual-level local social capital driving mental health. In addition, the use of a more exogeneous measure of contextual-level local social capital (based largely on administrative data) also provides some evidence that the stress-buffering role of local social capital is not solely a product of reverse causality. Ultimately, I do not claim to have identified a causal effect of social capital, only somewhat stronger evidence in favor of it relative to prior pandemic studies. Lastly, the study was limited in the explanatory pathways that it was able to test. Although providing some insights into what, at least, does not solely explain the apparent stress-buffering role of local social capital, further research is needed. For example, integrating the role of collective efficacy alongside social capital is important, especially investigating the conditions under which the latter does/does not lead to the emergence of the former.
In sum, the study provides important insights into the protective role local social capital played during the pandemic and could play in future crises. Efforts to support/grow local social capital might therefore not only provide a protective factor from the stressors of everyday life but also protect people during future major crises.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465251368341 – Supplemental material for Did Social Capital Protect Mental Health from Social Mixing Restrictions and Spatial Immobility during the COVID-19 Pandemic? A Longitudinal Analysis of Individual- and Contextual-Level Local Social Capital
Supplemental material, sj-docx-1-hsb-10.1177_00221465251368341 for Did Social Capital Protect Mental Health from Social Mixing Restrictions and Spatial Immobility during the COVID-19 Pandemic? A Longitudinal Analysis of Individual- and Contextual-Level Local Social Capital by James Laurence in Journal of Health and Social Behavior
Footnotes
Acknowledgements
I thank participants of the Institute for Social Sciences, University of Tokyo, seminar series for their comments on this research.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Economic and Social Research Council (Grant No. ES/W00349X/1).
Supplemental Material
Appendices S.1 to S.13 are available in the online version of the article.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.