
Abstract
Higher education can expose young people to various health challenges, yet potential disparities in health across academic disciplines remain underexplored. This study analyzes panel data on self-rated health of 14,022 German university students across nine subject groups employing both random- and fixed-effects regression models to examine selection and potential causal mechanisms. The results show that students of medicine and health sciences reported consistently good health throughout their studies. By contrast, law students exhibited the highest initial health scores but experienced the steepest decline over time. Students in arts and humanities started with the lowest health scores, but no significant change was observed during their studies. Although initial health inequalities suggest selection effects, the observed within-change heterogeneity raises the possibility that academic majors influence student health trajectories. Field specialization could represent an important dimension of health inequality in higher education, potentially extending into later life stages.
Keywords
Over recent decades, participation in higher education has risen sharply, with over 235 million students and 40% of school leavers worldwide enrolled in tertiary education programs in 2022 (UNESCO 2022). Life course research highlights this stage as a critical turning point, where both positive and negative experiences can have profound and lasting effects on future outcomes (Shanahan 2000). On the one hand, university graduates enjoy many advantages over their lower educated counterparts, including higher earnings, greater job security, healthier working conditions, and longer life expectancy (Mirowsky and Ross 2017; OECD 2023). By contrast, students tend to be more vulnerable to certain health issues when compared to the general population, with studies reporting high prevalence rates of depression, generalized anxiety disorders, and alcohol and substance use among university students (Auerbach et al. 2018; Ibrahim et al. 2013). 1
Although students may benefit from advantages such as flexible schedules and opportunities for personal and intellectual growth, they also face significant health challenges linked to the demands of academic life. These can include a wide range of stressors, such as heavy workload, exam pressure, social isolation, competitiveness, uncertainty about the future, and financial difficulties (Robotham and Julian 2006). Many students also find themselves separated from their families for the first time, needing to adapt to a new social environment in a different city or country. Some students have to fund their studies by working part-time, which further adds to their workload. These challenges can trigger stress responses, potentially leading to health problems and in some cases, study dropout—both of which may have lasting consequences for later life outcomes (Pascoe, Hetrick, and Parker 2020). Therefore, understanding the underlying risk factors contributing to students’ health challenges is crucial.
Existing research has tended to view university students as a relatively homogeneous population, overlooking potential differences in their experiences based on the characteristics of their study programs. One important aspect could be a student’s major subject. Academic disciplines structurally differ in terms of the organization of the study, the particular profile of knowledge and skills, and the potential labor market returns (Borgen and Mastekaasa 2018). These aspects might also translate into different influences on health. For example, studying subjects with higher failure rates or that are considered more difficult may be more stressful for students. In addition, study subjects can contribute to job insecurity and fear, most notably if the skills and competences acquired are of little relevance to the labor market. Conversely, some subjects may benefit health because they come with higher returns to education or impart health-relevant knowledge that positively influences a healthy lifestyle.
A number of cross-sectional studies suggest an association between field of study and student health. A survey of undergraduates in the United States found that students in medical disciplines were less likely for mental health problems, whereas an increased prevalence was found among students in the humanities, arts, and design (Lipson et al. 2016). Similarly, a study with postgraduate students from the United States confirmed that those in creatively oriented fields (humanities, arts, architecture) are more likely to screen positive for depression compared to students in other fields (Posselt 2021). An online survey of Irish students found that unhealthy behaviors, such as physical inactivity, smoking, alcohol consumption, or drug use, were more common among males studying social sciences, law, humanities, and arts than among students of medicine and health sciences (Murphy et al. 2019). Recently, a survey of Czech and Slovak students during the COVID-19 pandemic showed above-average prevalence of somatic and mental health issues in students of informatics, mathematics, and information and communication technologies (Gavurova et al. 2022).
Existing research suggests a relatively consistent pattern wherein students in subjects with a strong emphasis on creativity tend to report more health problems and those in health-related disciplines, such as medicine or health sciences, exhibit better health. However, because prior research is solely based on cross-sectional data, it remains unclear whether the observed health disparities across disciplines reflect an impact of the study program itself. Although prevalence studies are informative for descriptive purposes, they do not allow us to determine if, for instance, studying medicine keeps students healthy or if studying arts makes individuals sick. Alternative explanations could be that the health status before the study affects the likelihood of enrolling in a particular study subject (health selection) or that students of different subjects vary in terms of other characteristics correlated with health (confounding). Such characteristics can be age, sex, parental education, or aspects more difficult to measure, such as personality or motivation. To better estimate potential causal effects, longitudinal data are necessary that help to establish a temporal order between fields of study and health, thereby minimizing bias from health selection. Moreover, longitudinal data allow one to investigate intraindividual changes in health that are not biased by time-constant confounding factors.
This study will be the first to use longitudinal panel data to investigate the relationship between academic discipline and student health. In doing so, it will address two further key limitations of previous research. First, existing studies have often compared only a selective number of academic disciplines, whereas this investigation will examine the health impacts of a representative range of subject groups. Second, the available research has predominantly come from a limited number of countries, primarily the United States. However, the organization of higher education can vary significantly between countries. This study will therefore focus on the situation in Germany, where most students are enrolled in public-funded universities (Hüther and Krücken 2018). This likely removes some ambiguity when comparing students across different disciplines that may charge varying levels of tuition fees. Another particularity in Germany is that students of law, medicine, and sometimes teaching graduate with a state examination rather than a bachelor’s and master’s degree (Hüther and Krücken 2018). State examinations generally provide access to lucrative professions but are often criticized for their intensive workload. It is also worth noting that in Germany, the vocational education and training system offers an alternative to higher education. Comparisons of different school-to-work transitions in Germany have found that university students generally experience better trajectories of overall self-reported health than apprentices but less favorable trajectories of mental well-being (Reuter et al. 2022). In the following, I outline more precise theoretical assumptions about the different pathways linking study major and health that will be considered in the empirical analyses.
Background
Educational Processes and Health
Medical sociologists have long been interested in understanding the pathways by which education shapes health outcomes. As a key dimension of socioeconomic position, education consistently correlates with better health and longer life spans (Mirowsky and Ross 2017). This relationship is driven by several interrelated mechanisms that come along with higher education, including access to economic resources, intellectual abilities, social environments that promote healthier lifestyles, and advantages in terms of social-psychological burdens and resources (Cockerham 2005; Link and Phelan 1995; Pampel, Krueger, and Denney 2010; Ross and Wu 1995). From a life course perspective, the years spent in education represent a critical period because the attainment of educational degrees often initiates a cumulative process of advantages that shape subsequent stages of life (Shanahan 2000). Most importantly, higher levels of education provide access to higher paying jobs and safer work environments while lowering the risk of unemployment (OECD 2023; Reuter et al. 2023).
In recent years, sociological research has shifted beyond treating education solely as a vertical dimension of social stratification—defined by levels of attainment, such as years of schooling or highest degree earned—to also consider horizontal dimensions, such as characteristics of educational institutions and field specialization in higher education (Gerber and Cheung 2008).
Although field specialization has been recognized as a strong predictor of economic returns and labor market opportunities (Borgen and Mastekaasa 2018), its relationship with health remains largely underexplored (Zajacova and Lawrence 2018).
Pathways between Field of Study and Health
Field specialization places individuals into distinct academic environments while often being driven by preexisting individual characteristics (Gerber and Cheung 2008). As a result, three key mechanisms are likely to shape the relationship between university major and student health (Figure 1). First, a causal connection is possible, where specific features of a given field of study can be beneficial or detrimental for health. Second, the relationship could be explained by health selection, with individuals of good health enrolling in different subjects compared to those with poor health. Third, the relationship might be confounded through social selection if both field of study and health are influenced by factors prior to the study, such as family background or personality. Notably, causal and selection mechanisms are not mutually exclusive, and all three pathways may be important. However, it is crucial to distinguish these pathways given that the primary aim of this study is to assess the potential influence of academic discipline on student health while seeking to minimize the role of health selection and confounding.
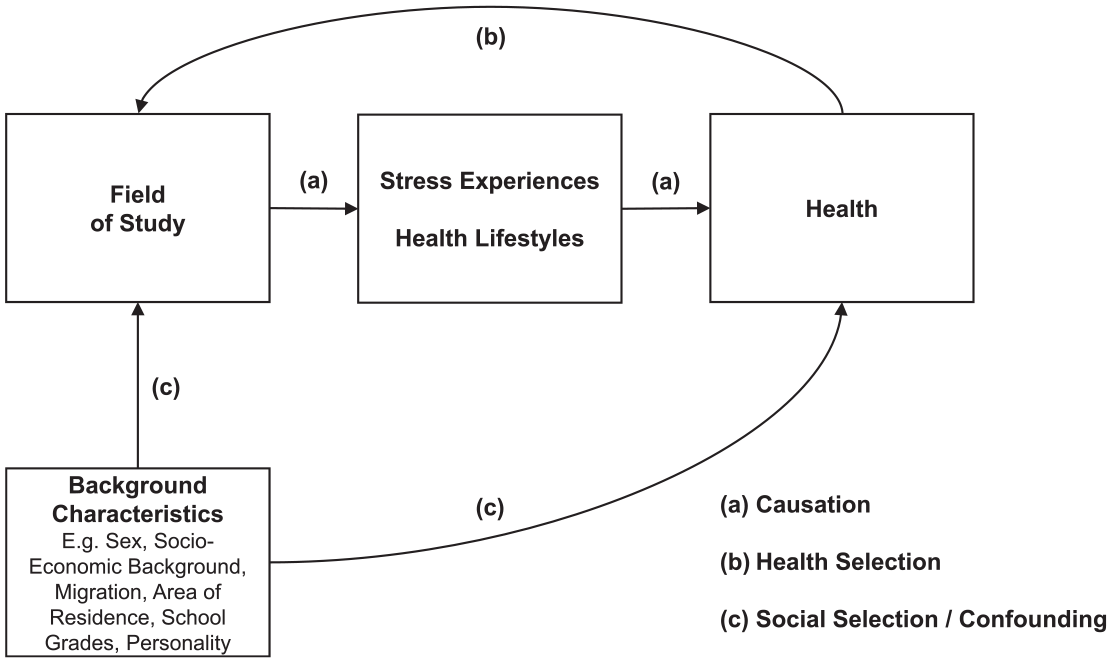
Theoretical Pathways between Field of Study and Health.
Causation
Link and Phelan’s (1995) theory of fundamental causes posits that education exerts a causal influence on health by shaping economic, social, and cultural resources that protect health and reduce exposure to risk. Although students who are still in the education system may not yet benefit from the long-term returns of their chosen field, enrollment in a specific major can shape their exposure to distinct learning environments, the types of knowledge they acquire, and their anticipation of future labor market opportunities (Gerber and Cheung 2008). I argue that these structural differences can have both potential positive and negative implications for students’ health, most importantly driven by two key mechanisms: (1) stress experiences due to academic demands and unclear career paths and (2) the promotion of health-related lifestyles.
Variation in students’ stress experiences across academic majors can be understood through the lens of two stress theories. Karasek’s (1979) demand-control model links stress to environments combining high demands (e.g., workload, deadlines) with low autonomy (e.g., no influence on when and how to do tasks). Majors such as law, medicine, and engineering often involve heavy workloads, high-stakes exams, and limited flexibility (Dahlin, Joneborg, and Runeson 2005), particularly in law, where students in most countries face rigid and highly standardized examinations (Bergin and Pakenham 2015; Heublein, Hutzsch, and Schmelzer 2022; Larcombe et al. 2020; Soonpaa 2003). By contrast, disciplines such as arts and humanities may involve lower demands and greater autonomy, such as the ability to complete assignments in flexible formats, such as essays or projects.
The transactional stress theory (Lazarus and Folkman 1984) complements this perspective by emphasizing the role of cognitive appraisal and coping resources. Although high academic demands are inherently challenging, the perceived severity of these demands is heightened when failure is seen as a likely or realistic outcome. This is particularly evident in fields such as law, where career goals depend on program completion and dropout rates are high (Heublein et al. 2017). By contrast, humanities or social science students may face less pressure, given lower dropout rates and more adaptable career paths (Heublein et al. 2022). In addition, collaborative fields, such as teaching and health sciences, may foster stronger peer support and coping resources (Topping 2005).
A related source of stress concerns the anticipation of labor market returns. From an economic perspective, education is an investment in human capital and future monetary returns (Harmon, Oosterbeek, and Walker 2003). Instead of working full-time, students accept forgone earnings, invest time and effort, spend money on tuition fees, and may even take out a student loan, all of which is expected to be compensated in the future by higher income and lower unemployment risks. However, there is a high level of heterogeneity in returns to education depending on the field of study, with medicine and economics clearly at the top and creative arts even showing negative returns to education (Walker 2020). Although these outcomes are long-term consequences, anticipation effects may become particularly relevant as students approach the end of their studies. Fields with less direct or uncertain pathways to stable employment, such as arts, humanities, and some social sciences, may expose students to higher levels of insecurity compared to fields such as medicine, law, or engineering, where career prospects are often more defined and secure.
Another aspect concerns differences in field-specific cultures, social norms, and curricular content. Drawing on Cockerham’s (2005) theory of health lifestyles, patterns of health behavior emerge from the interaction between structural life chances and individual life choices. Academic majors serve as environments in which students often share similar socioeconomic backgrounds, are exposed to comparable curricula, and internalize norms associated with their discipline (Gerber and Cheung 2008), which can influence their health behaviors as part of their emerging professional identities. For example, students in health-related fields, such as medicine, sports sciences, and nursing, often exhibit healthier behaviors, including regular physical activity, balanced diets, and lower rates of smoking or binge drinking (Keller et al. 2008). Similarly, disciplines such as sports and agricultural sciences often incorporate practical training that promotes physical fitness and active lifestyles. By contrast, students in high-stress disciplines, such as law, were found to be more prone to physical inactivity and unhealthy coping mechanisms, such as increased alcohol use and smoking (Coe et al. 1982). Meanwhile, students in creative disciplines, such as arts and humanities, may prioritize flexibility and creativity, which can disrupt health-related routines, including sleep and diet.
Academic majors group students into distinct environments that expose them to varying learning cultures, group norms, and career pathways. Although all disciplines involve both positive and negative elements, the combination of high demands, low autonomy, and limited coping resources in fields such as law may contribute to less favorable health trajectories. By contrast, majors such as medicine, teaching, and health sciences could promote positive health outcomes through more predictable educational returns, health-promoting norms, and supportive environments. Arts, humanities, and some social sciences present a mixed picture, combining more uncertain educational returns and disruptive health behaviors with benefits such as moderate demands and greater autonomy. If causal mechanisms are involved, health trajectories would be expected to differ by major, with law students experiencing more negative outcomes compared to medical students.
Health Selection
Although education is often regarded as a causal determinant of health (Link and Phelan 1995), the selection perspective suggests that healthier individuals are more likely to pursue and succeed in education. For instance, longitudinal studies demonstrate that poor childhood health significantly reduces the likelihood of attaining higher levels of education and occupational status (Haas 2006; West 1991). Grossman’s (1972) health capital model explains this as healthier individuals face fewer interruptions in education and lower opportunity costs and anticipate greater returns from education. In addition, for health problems such as mental illness, chronic conditions, or disability, structural barriers (e.g., inflexible assessment criteria) and forms of discrimination (e.g., biased treatment and evaluation) can amplify these effects (Hamilton, Hulme, and Harrison 2023).
Health selection is particularly relevant in higher education when poor prestudy health limits access to certain subjects or influences decisions about which majors to pursue. The need for good physical health to study sport is an obvious example. Moreover, early health problems in adolescence can impair school performance and subsequently restrict access to subjects with strict eligibility criteria (Mikkonen et al. 2021). For instance, in Germany, the medical degree program has a rigorous selection process favoring students with excellent grades, and this could result in medical students being healthier than other students. Health selection may also be relevant in terms of health problems that later limit access to desired professional positions. For example, teachers, judges, prosecutors, and doctors, who often work as civil servants, are subject to health screening during the recruitment process. Young people with physical or mental health problems may strategically choose a different field of study to avoid labor market disadvantage later on. This likely contributes to an overrepresentation of relatively healthier individuals in certain subjects.
Social Selection and Confounding
The likelihood of enrolling in a specific major is strongly influenced by several background factors, such as individual interest, ability, or socioeconomic origin (Kirkeboen, Leuven, and Mogstad 2016). If one or more of these characteristics are simultaneously correlated with health, the association between field of study and health may be biased by confounding. For instance, children from families with high parental education are more likely to enroll in health-related subjects, arts, humanities, and social sciences, and those from high-income families are more likely to study business and law (Hällsten and Thaning 2018). Simultaneously, parental intellectual and financial resources are strong predictors of health throughout the transition from adolescence to adulthood (Reuter et al. 2024). Academic fields are also segregated by sex, with females being underrepresented in engineering, mathematics, and natural sciences and overrepresented in humanities, social sciences, law, and health (Charles and Bradley 2009). Directly observable factors, such as sex, ethnicity, residential area, or family background, can be statistically controlled for in analyses, thus ruling out bias stemming from these social selection processes. However, more latent characteristics, such as personality or motivation, are often not directly observable or measured in surveys, but they are nonetheless important predictors of the field of study. For instance, certain personality traits, such as creativity, that have been found to be correlated with mental illness (Carson 2019) could explain higher likelihoods of health problem in arts students without necessarily indicating a negative influence of the field of study itself.
Subgroup Differences
Potential impacts of study majors on health may be systematically moderated by further factors. First, students from nonacademic families receive less economic, cultural, and social capital from their parents (Bourdieu 1986), which could lead to greater difficulties and fewer stress-coping resources among “first-generation” students. Second, due to the systematic underrepresentation of women in certain subjects, women studying male-dominated science, technology, engineering, and mathematics (STEM) subjects could experience gender discrimination. Additionally, they could also expect lower returns to education at the end of their studies due to the gender pay gap. Consequently, the moderation of parental education and sex is tested.
Research Aims
This study examines the link between academic majors and student health using longitudinal data from German first-year students. It addresses two questions:
Research Question 1: To what extent does student health differ between academic majors in the first year of the study (between-person differences)?
Research Question 2: How does student health change over the course of the study depending on academic major (within-change heterogeneity)?
The first question explores initial health disparities driven by selection, and the second examines potential impacts of academic majors on health over time. Insights from this study can inform the design of health interventions in higher education and guide stakeholders seeking to effectively improve study conditions where most needed. Furthermore, comprehending the health implications of academic subjects can extend previous models of life course research given that the period of school-to-work transition is a highly sensitive life stage where health adversities are likely to be transmitted into later life stages (Reuter et al. 2022). Additionally, academic subjects constitute a scarcely investigated horizontal dimension of education that may complement medical sociological theory on health inequalities.
Data and methods
Data
Data were used from the National Educational Panel Study (NEPS), which is carried out by the Leibniz Institute for Educational Trajectories in Germany in collaboration with a nationwide network (Blossfeld and Roßbach 2019). NEPS employs a multicohort design, where each starting cohort (SC) focuses on a specific stage of the educational process, from early childhood education to school, vocational training, and adult learning. For this article, I drew on data from SC5, which concentrates on educational choices and outcomes in higher education (NEPS Network 2024). I used the latest version (19.0.0) of the data set, which consisted of 12 survey waves, with one survey per year from 2011 to 2022. NEPS SC5 is a representative sample of German first-year students who started their study in the winter semester 2010–2011. The sample is representative of students who enrolled for the first time at a higher education institution in Germany to study for a bachelor’s degree, state examination (Staatsexamen), diploma, or master’s degree. A two-stage stratified cluster approach was used, first sampling higher education institutions (public universities, public universities of applied sciences, private higher education institutions) and then subjects within a given higher education institution (e.g., medicine, law, pharmacy, social sciences). Individuals were surveyed using computer assisted telephone interviews.
Study Sample
The original sample consisted of 17,909 individuals, contributing 114,295 person-years of observation. The study sample was derived through a stepwise process. First, 550 individuals born before 1980 with 3,520 person-years were excluded because senior students do not face the lifelong consequences of educational processes in the same way as young students. Second, 33,169 person-years during which individuals were not enrolled in university were excluded. These periods included spells of employment, parental leave, or unemployment, which were captured in the study follow-up but are not relevant to this analysis. Third, to maintain a focus on undergraduate experiences, postgraduate studies, such as master’s and doctoral programs, were excluded. 2 This step removed 67 individuals and 10,414 person-years. Fourth, to ensure that the analysis captured both the beginning and end of students’ trajectories in higher education, the sample was refined to include only two person-years per study episode: the first year and last year. Study episodes were defined as the unique combination of a degree program (bachelor’s, master’s, or state examination), a field of study, and a study outcome. Possible study outcomes were either successful completion or dropout. Incomplete study episodes, where students were lost to follow-up before completing their studies, were coded as “ongoing.” This refinement excluded 2,982 individuals and 36,992 person-years, resulting in a well-balanced sample with 2 person-years per study episode.
Focusing solely on the entry and exit time points of study episodes offered two advantages over modeling yearly trajectories. It enabled comparison of study episodes of varying lengths because many students did not complete within the standard time frame. For instance, study episodes leading to dropout were generally shorter, and those culminating in state exams were longer than bachelor’s or master’s programs. Second, study entry and exit mark relevant time points because variations in health were most likely attributable to the study itself. By contrast, looking at the time of labor market entry would likely be influenced by factors beyond the study. However, because longer study periods may result in steeper health decline due to aging effects, age was statistically controlled for in the main analyses. Finally, individuals with missing information on variables of interest (age, sex, migration, living municipality, household composition, parental education, side jobs, and health) were excluded, leading to the removal of 246 individuals and 542 person-years.
The final study sample consisted of 14,022 individuals with 29,658 person-years or 14,829 study episodes. Obviously, the number of study episodes was slightly higher than the number of individuals because I allowed multiple studies per person but controlled for within-person dependency in the statistical analyses. A detailed overview of the steps that were taken to create the study sample and their impact on the sample size can be found in the Appendix (e-Table 1) in the online version of the article.
Variables
Health
At each survey wave, participants rated their overall health by responding to the question “How would you describe your general health?” on a 5-point Likert scale where 1 = very poor, 2 = poor, 3 = average, 4 = good, and 5 = very good. The original scale was treated as a quasi-metric, with higher scores indicating better health. Self-rated health is a widely used and validated survey instrument that reflects current morbidity and future mortality in samples of young adults (Burström and Fredlund 2001; Idler and Benyamini 1997).
Fields of study
Major subjects were coded based on the classification system of the Federal Statistical Office of Germany (Statistisches Bundesamt 2022). Related subjects were grouped into broader study areas, which were then further consolidated into nine subject groups: (1) economics and social science; (2) mathematics and natural sciences; (3) linguistic and cultural studies; (4) engineering sciences; (5) medicine, sport, and health sciences; (6) arts, art science; (7) law; (8) teaching profession; and (9) agricultural, forestry, nutrition. The analysis focused only on major subjects. Minor subjects were not considered to simplify the research design. An overview about the study areas and the subjects behind each category is available in the Appendix (e-Table 2) in the online version of the article.
Covariates
Further variables were considered as potential moderators (sex, parental education) or time-varying confounders (age, residential area, household composition, study success, student jobs). Additional variables were used to describe individuals (migration background, school-leaving grade) or study episodes (study duration). The school-leaving grade referred to the final grade attained at the end of postsecondary education (in German: Abitur), which qualifies students for university admission. A migration background was given if either the respondent or at least one of the parents were not born with German citizenship.
Statistical Analysis
A series of analytical steps were taken to examine the relationship between field of study and health. First, study episodes recorded for each field were described by individual characteristics and information pertaining to the study episode itself.
Second, a group-specific random-effects growth curve model was specified to examine between-person differences in self-rated health at the beginning and end of each study period by field of study, study outcome, and study program (Rabe-Hesketh and Skrondal 2005). Growth curve models are multilevel regression models that include a function of time and an interaction between time and a time-constant factor variable and allow modeling how average levels of an outcome evolve in different groups of individuals. The random-effects model for self-rated health was specified as follows:
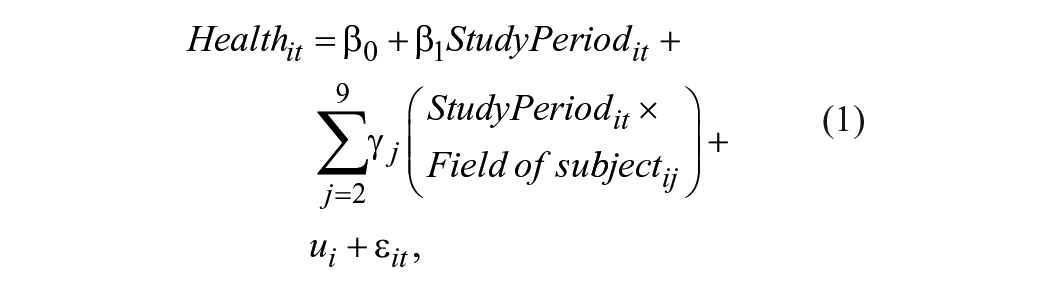
where i denotes individuals, t indicates time points (t = 1, 2), Healthit is the self-rated health of individual i at time t,
Third, to estimate the effect of a particular field of study on health, fixed-effects regression analysis was used (Allison 2009). As discussed previously, health selection and confounding might distort the estimation of effects of academic discipline on health. Fixed-effects regression models are not biased by selectivity and time-constant confounding, because only intra-individual variation is analyzed. To ensure temporal homogeneity, meaning no aging or period effects that differ between individuals due to variation in study lengths, age was added as a covariate to the regression model. By adjusting for age, a within-estimation with a control group was employed. This allowed for individual health changes to be subtracted from the average health changes observed across the whole sample (difference-in-differences approach). The main analytical approach was to test for effect heterogeneity by field of subject. Therefore, an interaction term between field of subject and study period was introduced. More precisely, the fixed-effects regression model was specified as follows:
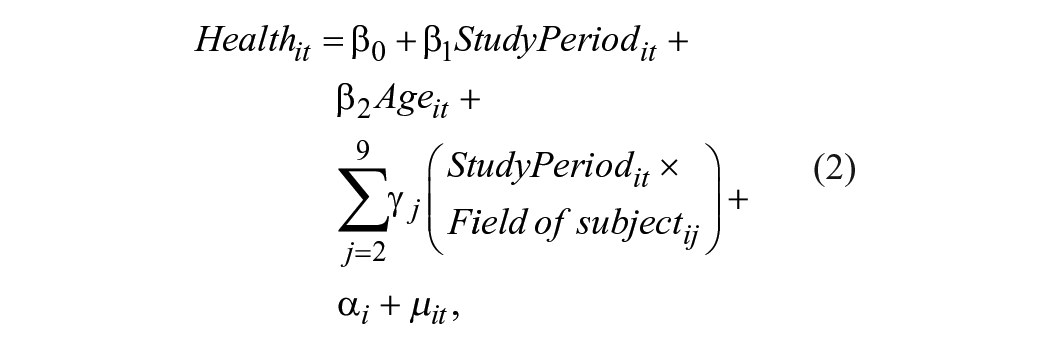
where, in deviation to the random-effects model,
To evaluate whether differing success rates across fields of study account for differences in health effects, a second model was estimated that included study outcome as a time-dependent covariate. Furthermore, to test for subgroup differences, I calculated separate fixed-effects models for men and women and for children from parents with low and high levels of education.
All regression models employed a cluster-robust variance estimation technique to account for the nested structure of the data, with multiple study periods possible within the same individual. Cluster-robust variance estimation accounts for the resulting autocorrelation and heteroscedasticity, yielding more reliable standard errors (Brüderl and Ludwig 2015). All analyses were performed using Stata 18 MP (64-bit, StataCorp LLC, College Station, TX, USA).
Results
Descriptive Statistics
According to Table 1, the most common fields of study were teaching, economics, and social sciences. The mean age at study entry was 21.3 years, with law and teaching students tending to be younger and arts students slightly older than average. 3 Students in law, arts, medicine, and health sciences more often came from academic family backgrounds. Law, medicine, and health science students achieved higher school-leaving grades. The average study duration was 3.3 years, with longer durations in law and medicine. Females were overrepresented in linguistics, culture, medicine, health, arts, and teaching but underrepresented in STEM fields. Dropout rates were above average in math, natural sciences, law, and teaching but lowest in medicine and arts. Around 17% of students had side jobs, although proportions were higher in arts and humanities.
Description of the 14,829 Study Episodes Recorded from 14,022 Individuals.
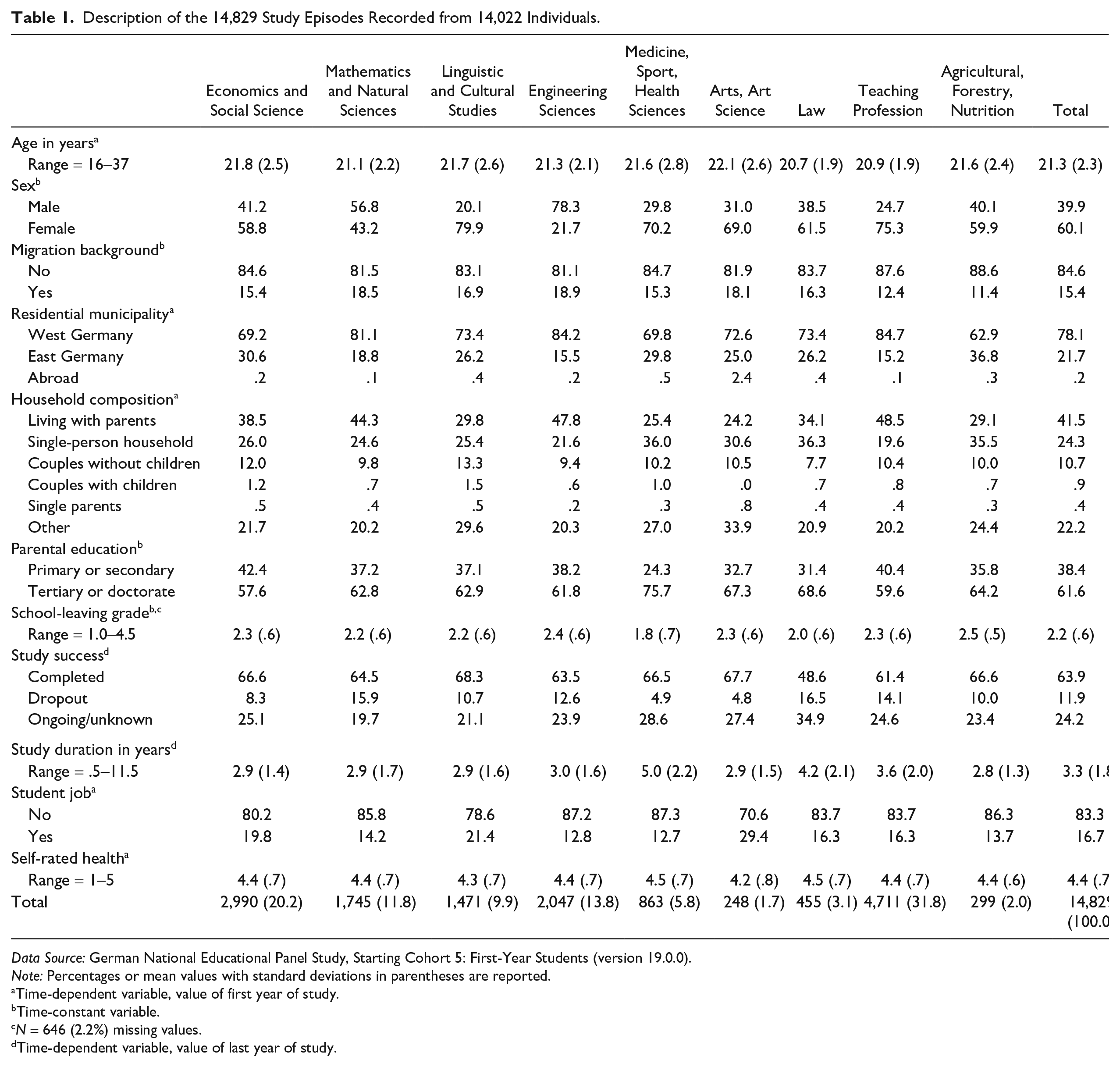
Data Source: German National Educational Panel Study, Starting Cohort 5: First-Year Students (version 19.0.0).
Note: Percentages or mean values with standard deviations in parentheses are reported.
Time-dependent variable, value of first year of study.
Time-constant variable.
N = 646 (2.2%) missing values.
Time-dependent variable, value of last year of study.
Between-Person Differences
The findings presented in Figure 2 indicate that students in the disciplines of law, engineering, medicine, sports, and health sciences reported more positive initial health compared to those in the fields of arts, linguistics, cultural studies, and agriculture. Across all majors, average health declined over time, with law students experiencing the greatest decrease and medicine, sports, and health sciences and agriculture, forestry, and nutrition students experiencing relatively little or no deterioration.
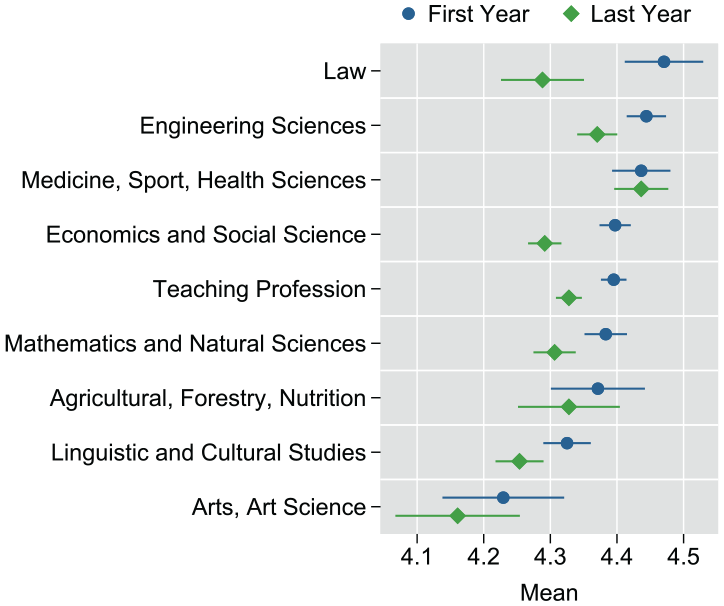
Self-Rated Health Levels Reported in the Initial and Final Years of Study by Field of Study.
Figure 3 indicates that first-year students’ health levels differed based on their eventual study outcomes. Those who completed their studies initially reported better health compared to those who later dropped out. By contrast, health decline was not steeper among students dropping out. Ongoing or unknown study episodes showed similar health levels than completed studies.
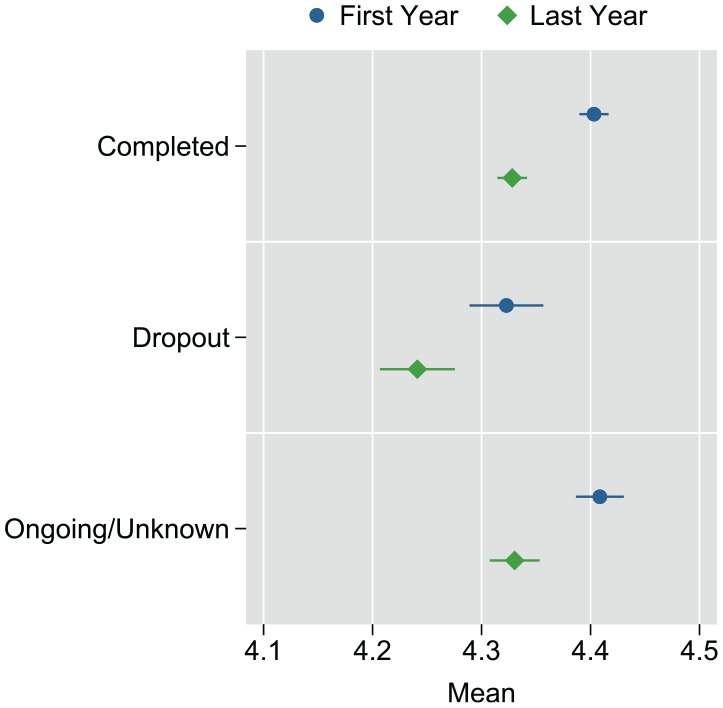
Self-Rated Health Levels Reported in the Initial and Final Years of Study by Study Outcome.
Within-Change Heterogeneity
Figure 4 depicts the results of the fixed-effects regression analysis. The effect estimates show the impact of a particular field of study compared to the sample mean effect. Statistically significant differences from the sample mean (represented as 0) are indicated by nonoverlapping 95% confidence intervals. These intervals also allow comparisons between different subjects. The first model adjusts for aging effects (dark blue dots). Notably, medicine, sports, and health sciences demonstrated positive effects on health. A positive effect was also observed for teaching and agricultural, forestry, and nutrition sciences, although not reaching statistical significance. A significant negative health effect was identified for law, where the widest spread between first- and last-year health was observed.
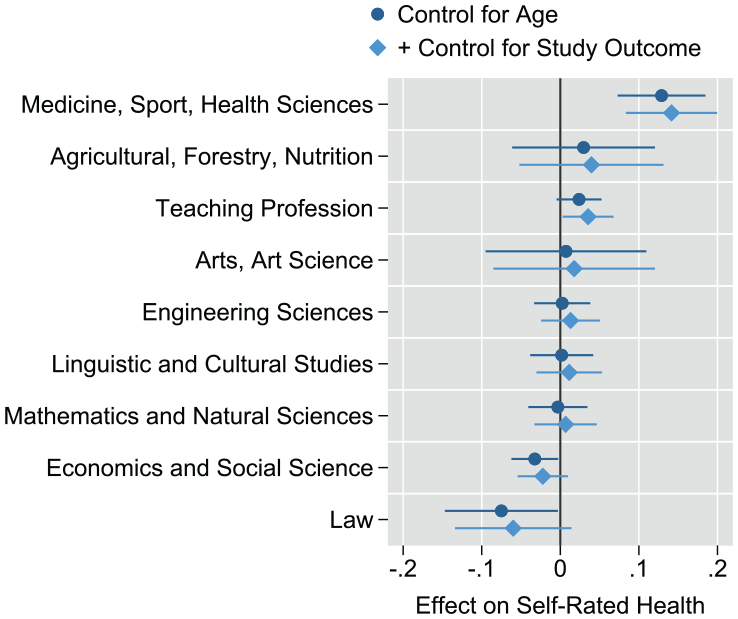
Effect of Field of Study on Self-Rated Health.
The second model additionally controlled for study outcome, thus eliminating any differences resulting from systematic variation in study dropout rates. This slightly changed the effect estimates, with positive effects increasing and negative effects being attenuated. This suggests that effect heterogeneities across fields of study were partly explained by different dropout rates. Notably, the effect for studying law was reduced and became insignificant in the second model, indicating that the higher likelihood of failure accounted for part of the negative health impact of this subject. Additionally, teaching was associated with a significant positive effect on health after accounting for dropout.
Subgroup Analyses
Figure 5 highlights the moderating role of sex in some academic fields. Law negatively impacted health only in female students, and engineering sciences were more detrimental to females but beneficial for males. Conversely, linguistic and cultural sciences were linked to more positive health outcomes for females compared to males.
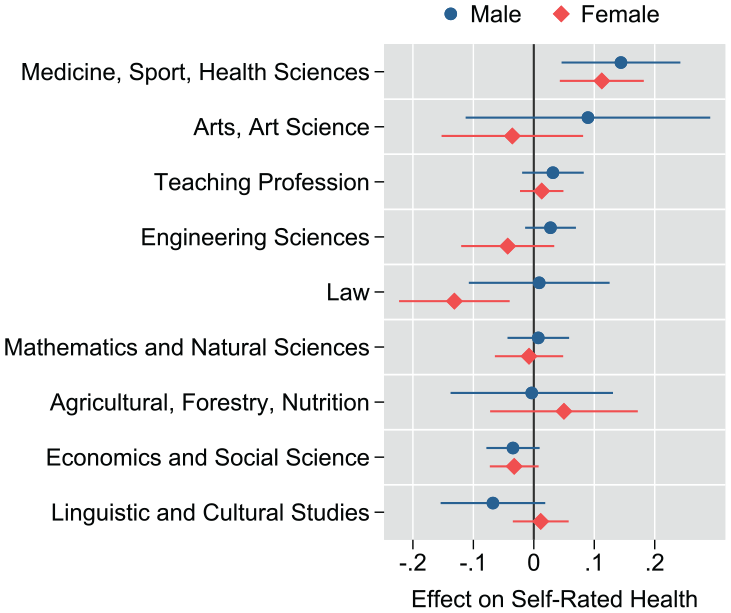
Effect of Field of Study on Self-Rated Health by Sex.
Figure 6 shows that the health effects of study majors were largely consistent between students from nonacademic and academic backgrounds. However, medical students from nonacademic backgrounds showed slightly greater health improvements over time.
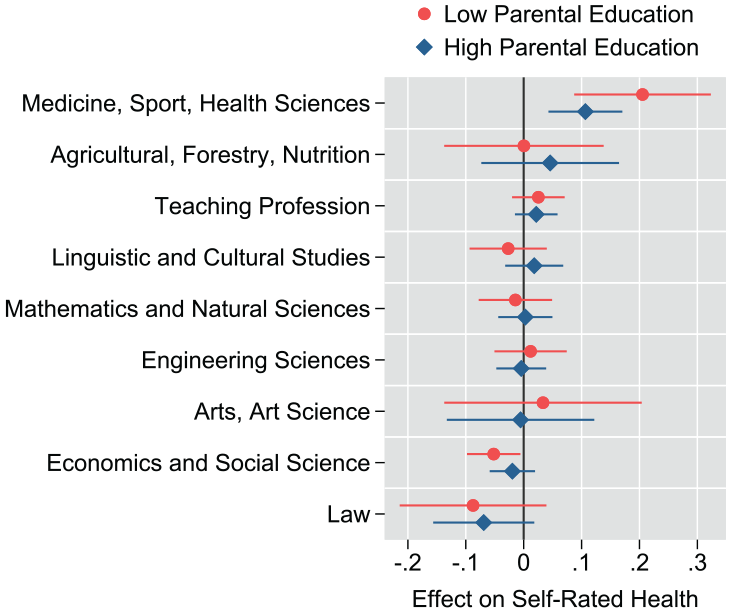
Effect of Field of Study on Self-Rated Health by Parental Education.
Sensitivity Analyses
Alternative modeling strategies were tested to assess whether the findings were robust against potential misspecification. First, a model was calculated that incorporated changes in household composition, residential area, and any side jobs undertaken while studying. Second, an analysis with only completed or unsuccessful study episodes was conducted where all ongoing episodes were dropped. Crucially, these additional modeling approaches did not alter the central findings of this study. The results of the sensitivity analyses are presented in the Appendix (e-Table 7) in the online version of the article.
Discussion
This study examined differences in self-rated health across academic majors as an important yet overlooked determinant of student health. Two key findings emerged. First, significant disparities were already present at the start of university, with higher health scores reported among students in law, engineering, medicine, and sport and health sciences and lower scores among those in the arts, art sciences, and linguistic and cultural studies. Second, health trajectories over time varied by field of study. Students in medicine, sport, and health sciences maintained consistently high health levels, and law students—despite high initial scores—experienced the sharpest decline. No significant change was observed among students in the arts and humanities.
Health disparities at study entry reveal an interesting pattern: Healthier individuals were disproportionately likely to enroll in fields such as law, medicine, and engineering—disciplines characterized by high academic demands, the need for strong school-leaving qualifications, and promising labor market returns (Dahlin et al. 2005; Heublein et al. 2017; Walker 2020). Law and medicine also had the highest proportion of students from academic family backgrounds. Such compositional differences support the theoretical assumption that health selection (Haas 2006; West 1991) and social selection (Hällsten and Thaning 2018; Kirkeboen et al. 2016) could play a role in explaining health disparities across study majors. This interpretation aligns with previous research showing that both socioeconomic background and adolescent health are strongly associated with postsecondary educational pathways (Brewer et al. 2019; Mikkonen et al. 2021; Reuter et al. 2024).
By comparison, students in arts and humanities reported the lowest self-rated health at the start of their studies, consistent with prior research indicating elevated levels of mental health problems in these fields (Gavurova et al. 2022; Lipson et al. 2016; Murphy et al. 2019; Posselt 2021). Although earlier studies have often attributed this to greater career uncertainty, the longitudinal findings in this study instead suggest that creatively oriented disciplines may attract students with preexisting vulnerabilities.
Overall, the findings suggest that organizational factors within academic programs contribute to health differences across majors. Most notably, law students, who initially reported the highest health scores, experienced the strongest health decline over time. This pattern supports stress models (Karasek 1979; Lazarus and Folkman 1984), which link negative health outcomes to environments combining high demands, limited autonomy, and heightened risk of failure. In line with this, accounting for study dropout reduced the observed health decline, highlighting examination pressure as a critical mechanism. Law programs in Germany and elsewhere are characterized by intensive workloads, rigid assessment structures, and prolonged exam periods, often associated with social isolation and reliance on external tutoring (Bergin and Pakenham 2015; Heublein et al. 2017; Larcombe et al. 2020; Soonpaa 2003).
By contrast, students in health-related fields displayed the most favorable health trajectories. Cross-sectional studies have similarly found that students in medicine and health sciences tend to report better mental health compared to students in other fields (Gavurova et al. 2022; Lipson et al. 2016; Posselt and Lipson 2016). This outcome aligns with expectations from theoretical stress models (Karasek 1979; Lazarus and Folkman 1984) because studying medicine, although academically demanding (Dahlin et al. 2005; Rotenstein et al. 2016), is often counterbalanced by positive structural factors, such as cooperative learning cultures and clear educational returns (Walker 2020). In addition, health-related fields may foster learning environments in which health-promoting behaviors are actively reinforced. From the perspective of Cockerham’s (2005) health lifestyles theory, the social context of these disciplines can shape both students’ “life chances” (e.g., by providing access to health knowledge) and “life choices” (e.g., by encouraging the adoption of healthier practices through peer interaction or institutional expectations). This interpretation is supported by prior research showing that medical students are more likely than students in other disciplines to engage in physical activity and maintain a healthy diet and less likely to smoke or drink excessively (Keller et al. 2008; Murphy et al. 2019; Polak, Pojednic, and Phillips 2015). A similar mechanism may explain the positive health outcomes observed in students of sports, agricultural, forestry, and nutrition sciences.
A notable and unexpected finding was that the health benefits of higher education did not align neatly with labor market returns. Fields such as economics, engineering, and law—known for strong employability—were not consistently associated with positive health outcomes. Conversely, arts and humanities, often linked to lower or even negative returns (Walker 2020), did not show adverse health trajectories. Instead, institutional characteristics, such as the flexibility of assessment methods and emphasis on creativity, appeared more influential.
Subgroup analyses revealed that the effects of study majors on health were broadly similar for students from academic and nonacademic families, although some differences emerged between male and female students. Female engineering students tended to face worse health outcomes than male engineering students, and female humanities students experienced more positive health outcomes than males. This could be explained by gender stereotypes about “natural ability” potentially leading to discrimination or social isolation (Leslie et al. 2015). Female law students appear more negatively affected, possibly due to the additional pressures of balancing family and career aspirations.
Taken together, the findings of this study highlight the role of field specialization in higher education for producing systematic heterogeneity in student health. Although prior research on field specialization has predominantly focused on its relationship with labor market outcomes, its potential health effects have received far less attention (Gerber and Cheung 2008; Montez et al. 2018). This study highlights a valuable avenue for future research and aligns with calls for a broader conceptualization of education—one that considers not only quantity but also the quality and context of educational experiences in shaping health inequalities (Zajacova and Lawrence 2018). For instance, medical sociological theories, such as fundamental cause theory (Link and Phelan 1995), emphasize the role of education in shaping health outcomes but focus mainly on vertical differentiation (e.g., comparisons between lower and higher education levels). The present findings suggest that not all forms of higher education confer the same health advantages and that field specialization may act as an additional structuring force. Similarly, health lifestyle theory (Cockerham 2005) treats education as a component of life chances but does not distinguish between types of higher education. These results suggest that institutional dimensions of education may play a more active role in shaping health than previously acknowledged.
Furthermore, findings of this study may have practical implications for institutional policies, particularly in the design of student support services and curricula aimed at fostering better health outcomes among students.
Strengths and Limitations
Strengths of this study are the use of panel data in combination with both random- and fixed-effects regression analysis that has allowed for a more advanced methodology compared to prior studies, most importantly to effectively preclude any selection bias and time-constant confounding. Potential time-variant confounders, such as changes in household and family circumstances, residential location, and student employment, were controlled for in sensitivity analyses to further strengthen the robustness of the findings. Second, the NEPS data, with its 12-year follow-up period, covered the crucial time window of students’ entry into and exit from higher education. The large sample size also conferred high statistical power. A further strength is the ability to analyze a representative set of academic subjects, in contrast with past research that often relied on only a few subjects or broad categories.
However, there are important limitations to consider. As with any observational study, causal claims must be approached with caution. Although the fixed-effects approach addresses time-constant heterogeneities, such as preexisting differences in health and social background, it cannot fully account for their influence on time-variant factors. For example, law and medical students—who exhibit markedly different health trajectories—may differ systematically in unobserved characteristics, such as stress resilience, which could influence their health outcomes. Medical students, for instance, may be more likely to possess traits that buffer against stress, such as a higher tolerance for high-pressure situations. Thus, although the study highlights important patterns, it cannot definitively attribute health variation across majors solely to field-specific environments.
Another limitation is the relatively low r2 values observed in the regression models, indicating that the explanatory power of academic majors for health variation is modest. Lower r2 values are not uncommon in fixed-effects models, where between-person differences are excluded (Allison 2009). Additionally, the study population comprises university students, a group characterized by youth, generally good health, and often socioeconomic advantage, reducing the prevalence of severe health issues. These characteristics combined with other potential determinants of health—such as smoking, drinking, body weight, and physical activity—may play a more substantial role in shaping health outcomes than academic discipline alone and contribute to the low explanatory power observed.
A further limitation of this study is the reliance on self-rated health as a broad health measure, which is subjective and does not allow for analysis of specific health conditions. Unfortunately, the NEPS data did not include other health indicators. It would be valuable to understand whether the findings are driven by physical or psychological health issues, which could prompt further replication studies. Additionally, due to data protection policies, the study was unable to differentiate between some subject areas that may have been interesting to explore, such as separating social sciences from economics and psychology given that these fields can vary significantly in terms of curricula and expected career outcomes.
Conclusion
The findings of this study support the assumption positing that academic majors may influence students’ health, with evidence suggesting health-enhancing factors in medical and health science programs and potentially greater health burdens associated with studying law. Future studies could explore proposed mediators, such as academic stress, healthy lifestyles, and anticipated educational returns. Overall, the findings suggest that field specialization represents a significant dimension of health inequality in higher education, potentially extending into later life stages.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465251357845 – Supplemental material for Does Your Subject Make You Sick? How Academic Majors Shape Students’ Self-Rated Health
Supplemental material, sj-docx-1-hsb-10.1177_00221465251357845 for Does Your Subject Make You Sick? How Academic Majors Shape Students’ Self-Rated Health by Marvin Reuter in Journal of Health and Social Behavior
Footnotes
Acknowledgements
I would like to thank Paul Rieger for drawing my attention to the topic of academic majors and their potential connection to student health, as well as for reading and providing valuable feedback on the first draft of this paper. I am also grateful to Dr. Alexander Patzina and Lisa Bongartz for carefully reading the initial draft and offering helpful comments.
Notes
Supplemental Material
The Appendix is available in the online version of the article.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.