
Abstract
Relationships with children are often highly salient to older adults and can be characterized by both social support and strain. Although research suggests that social support and strain are linked to older adults’ cognitive functioning, few studies have considered reciprocal effects or examined potential explanatory mechanisms. This study uses data from the Health and Retirement Study (N = 7,639) to examine longitudinal, bidirectional relationships between social support and strain in relationships with children and cognitive functioning among older U.S. adults. Results from dynamic panel models suggest that higher social support from children predicts modestly better later cognitive functioning and that strain from children is negatively linked to subsequent cognition. Older adults with higher cognitive functioning report less later strain in relationships with children. Depressive symptoms and receipt of children’s help with functional limitations play modest roles in helping to explain associations between social support and strain from children and cognitive functioning.
As the proportion of the U.S. population that is in older adulthood grows, understanding and addressing cognitive decline is a public health priority (U.S. Department of Health and Human Services 2022). An estimated 6.9 million U.S. adults are currently living with Alzheimer’s disease or related dementias, a number that is expected to nearly double by 2050 (Alzheimer’s Association 2024). Uncovering social and environmental factors linked to cognitive health as adults age is important not only for improving knowledge about contexts in which cognitive decline arises but also for identifying mechanisms that may help slow its progression. Predictors of cognitive functioning that may be amenable to intervention, such as the quality and content of older adults’ social relationships, offer promise as a means to help support cognitive health as the U.S. population ages.
Parent–child relationships are among the most enduring and meaningful social ties throughout the life course (Fingerman, Huo, and Birditt 2020; Silverstein and Bengtson 1994; Suitor et al. 2022; Umberson 1992). As underscored by theory and research on intergenerational ambivalence (Luscher and Pillemer 1998), they are also often complex and simultaneously experienced as supportive and strained (Fingerman et al. 2020; Pillemer and Suitor 2004; Spitze and Gallant 2006). A handful of prior studies provide limited evidence that social support or strain from children are linked to cognitive functioning (Okabayashi et al. 2004; Thomas and Umberson 2018; Wilkinson et al. 2023; Zahodne et al. 2019). However, potential pathways through which relationships with children might impact cognition are underexplored. In addition, because older adults with declining health often require increased help from close family (Liao et al. 2018; Spitze and Gallant 2006; Van Tilburg and Broese Van Groenou 2002), which over time may impact how they experience these relationships, it is important that studies consider the reciprocal, longitudinal effects of cognitive functioning on social support and strain in parent–child relationships.
Drawing on theory and research about intergenerational ambivalence, the life course, and social stress, this study adds to previous research exploring the meaning of family relationship quality for older adults’ health by examining bidirectional, longitudinal associations between social support and strain from children and older adults’ cognitive functioning. It also considers whether three potential mechanisms—depressive symptoms, receipt of children’s help with functional limitations, and in-person contact and coresidence with children—help explain links between social support and strain in relationships with children and cognitive functioning. The analyses highlight the salience and complexity of intergenerational ties as predictors of health and well-being for adults in later life.
Background
Social Support and Cognitive Functioning
A rich body of research shows that supportive social relationships predict better mental and physical health, including cognitive functioning (Fratiglioni, Paillard-Borg, and Winblad 2004; House, Landis, and Umberson 1988; Seeman et al. 2001; Umberson, Crosnoe, and Reczek 2010; Umberson and Karas Montez 2010). Explanations for the positive association between social support and cognition often draw on the stress process model (Pearlin and Schooler 1978; Thoits 1995). As highlighted by stress process research, dimensions of social support include emotional support, through which network members provide each other a sense of value and acceptance; informational support, or advice on and help making sense of stressful events or situations; and instrumental support, which involves offering material assistance or resources (e.g., Cohen and Wills 1985). Engagement in supportive social networks may help maintain cognitive functioning by supporting cognitive ability and by helping buffer against and cope with the detrimental effects of social stress, which is associated with numerous negative mental and physical health outcomes linked to cognitive functioning (Lupien et al. 2007; Marin et al. 2011; Pearlin, Menaghan, and Lieberman 1981; Pearlin et al. 2005; Sabia et al. 2009). Friends and family also encourage healthy behaviors and discourage unhealthy behaviors in one another (House et al. 1988; Umberson 1987), with beneficial implications that may extend to cognitive health.
Health and cognition may, in turn, shape how people evaluate and experience their social relationships. Older adults experiencing cognitive decline typically need and receive greater help with instrumental activities of daily living (IADLs), such as managing finances and health conditions, from close network ties (Jekel et al. 2015; Liao et al. 2018; Seltzer, Lau, and Bianchi 2012; Van Tilburg and Broese Van Groenou 2002). They may thus perceive these relationships as supportive due to feelings of gratefulness and appreciation and increased relationship intimacy. However, relatively few prior studies have examined impacts of cognitive health on self-reported social support. Of those that do, most find no relationship (Luo et al. 2021; Xu, Thomas, and Umberson 2016; Zahodne et al. 2019), and one (Liao et al. 2018) suggests that older adults with better cognitive functioning report greater instrumental social support.
Social Strain and Cognitive Functioning
Although social support enhances well-being, strained relationships with close network members can increase risk for negative health outcomes through multiple pathways (House et al. 1988; Koropeckyj-Cox 2002; Umberson 1992; Umberson, Crosone, and Reczek 2010). Studies typically find that experiences with social strain predict poorer cognitive functioning (Chen et al. 2019; Kotwal et al. 2016; Lindert et al. 2022; Luo et al. 2021). However, other evidence suggests that the association between strain and cognitive function may be more complex, finding some positive links between them (Thomas and Umberson 2018; Xu et al. 2016). The “use it or lose it” theory of cognitive aging argues that engagement in cognitively stimulating social interactions helps preserve cognitive functioning over time (Fratiglioni et al. 2004; Hultsch et al. 1999; Seeman et al. 2001). Following this theory, even relationships that are challenging may carry benefits for cognition. In addition, family and friends often act to control negative behaviors and support positive health behaviors among declining older adults, perhaps by nagging (Birditt and Antonucci 2008; Cornwell, Goldman, and Laumann 2021). Although these “irritating” behaviors may introduce strain to relationships (Birditt and Antonucci 2008; Warner and Adams 2016), they may ultimately help maintain health.
Cognitive functioning may also have reciprocal negative impacts on relationship quality, leading to greater perceptions of strain. Loss of the ability to function independently and conflicts over health behaviors may cause conflict in relationships (Birditt and Antonucci 2008; Kaufman and Uhlenberg 1998; Pearlin et al. 1990; Warner and Adams 2016). Individuals experiencing cognitive decline may additionally have compromised resources and ability to maintain frequent and reciprocal social interactions (Gurung, Taylor, and Seeman 2003; Washburn, Sands, and Walton 2003). Consistent with the possibility that poorer cognitive health can lead to declines in some aspects of relationship quality, the same study finding that adults with better cognitive function report greater instrumental support suggests that they perceive less emotional support over time than those with poorer cognitive functioning (Liao et al 2018).
Relationships with Adult Children and Older Parents’ Health and Cognition
Relationships between parents and children are among the most valued and enduring throughout the life course (Fingerman et al. 2020; Silverstein and Bengtson 1994; Suitor et al. 2022; Umberson 1992). The life course theory principle that individuals’ lives are “linked” in lifelong processes of development (Elder 1994; Elder, Johnson, and Crosnoe 2003) underscores that the structure and content of intergenerational relationships evolve alongside the needs of family members. As adults enter later life, retire, and experience bereavement and health declines, children may grow in importance as sources of social support (Kaufman and Uhlenberg 1998; Milkie, Bierman, and Schieman 2008; Silverstein and Bengtson 1994; Umberson, Pudrovska, and Reczek 2010). A variety of research shows that supportive relationships with children are linked to better mental and physical health among older parents (Silverstein and Bengtson 1991, 1994; Suitor et al. 2022)
However, as emphasized by theory on intergenerational ambivalence, parent–child relationships are often complex and may simultaneously be experienced as profoundly rewarding and stressful (Fingerman et al. 2020; Luscher and Pillemer 1998; Pillemer and Suitor 2004; Suitor et al. 2022). Relationships that encompass different stages of life and are difficult to disengage from even when they are problematic, such as those between parents and children, may be especially likely to be perceived as negative and demanding (Offer 2020; Offer and Fischer 2018; Rook et al. 2007). As with other social ties, studies on the “dark side” of relationships with children tend to show that strain and negative interactions take a toll on parents’ well-being (Koropeckyj-Cox 2002; Milkie et al. 2008; Umberson 1992).
Although many studies highlight the importance of relationships with children for older adults’ health generally, little previous research has examined impacts of support or strain in these sometimes affectively complex intergenerational relationships on cognitive functioning. The four prior studies we uncovered provide limited evidence that both may positively impact the cognitive health of some groups of older parents (Okabayashi et al. 2004; Thomas and Umberson 2018; Wilkinson et al. 2023; Zahodne et al. 2019). Specifically, a cross-sectional analysis showed that support from children predicted better cognitive functioning among widowed Japanese parents (Okabayashi et al. 2004), and a longitudinal study of U.S. adults found that strain in relationships with children was linked to slower cognitive decline as fathers (but not mothers) aged (Thomas and Umberson 2018). However, only two of the four studies considered reciprocal impacts of cognitive functioning on child relationship quality (Thomas and Umberson 2018; Zahodne et al. 2019), and just one accounted for number of and coresidence with children (Thomas and Umberson 2018), two important structural contexts that may shape both parents’ health and reports of support and strain from children. To date, no prior research has examined potential mediators of the relationship between social support and strain from children and cognitive functioning.
Depressive Symptoms, Help with Functional Limitations, and Contact Frequency as Potential Mediators
Although unexplored in previous research, many mechanisms may help explain links between support and strain from children and older adults’ cognitive functioning. Our analysis examines three potential mediators: depressive symptoms, help with functional limitations, and coresidence and other in-person contact with children. These mediators represent diverse emotional, instrumental, and relationship structure-based mechanisms through which overall evaluations of social support and strain from children and cognitive functioning may be linked.
First, as highlighted by the broader literature on family relationships, stress, and health across the life course, mental health is one key mechanism through which social relationships impact overall health. Supportive relationships with adult children can provide companionship and a critical source of purpose in life, which may reduce risk for depression (Rook and Charles 2017; Silverstein and Bengtson 1994; Umberson, Pudrovsak, and Reczek 2010), a risk factor for cognitive decline (Boss, Kang, and Branson 2015; Donovan et al. 2017; Jajodia and Borders 2011). At the same time, conflict and strain in relationships with children can increase depressive symptomatology (Koropeckyj-Cox 2002; Milkie et al. 2008; Umberson 1992). Alternatively, depression, which can result in a loss of interest in and importance placed on social life (Rizvi et al. 2016; Watson et al. 2020), may dampen impacts of support and strain on cognitive functioning. Depressive symptoms may also mediate or help explain potential impacts of cognitive functioning on social support and strain. Older adults experiencing early cognitive decline are susceptible to negative mood changes (Jajodia and Borders 2011; Yates, Clare, and Woods 2013), which may result in less positive or more negative evaluations of their social relationships (Hussenoeder et al. 2021; Nezlek, Imbrie, and Shean 1994; Roberson et al. 2018).
Day-to-day help provided by children, a type of instrumental support, is a second pathway through which overall evaluations of how supportive or strained relationships with children are may impact parents’ cognition. As underscored previously, children are an important source of instrumental support as older parents’ health worsens (Kaufman and Uhlenberg 1998; Silverstein and Bengtson 1994; Umberson, Pudrovska, and Reczek 2010). Parents with more supportive and less strained relationships with their children may be more likely to receive day-to-day help from them (Schwarz et al. 2005), and that help may sustain cognitive functioning by maintaining independence. However, studies also suggest that dependency on others can lead to further deterioration in health if it lessens engagement in cognitively stimulating daily and self-care activities (Hultsch et al. 1999). Receiving help with functional limitations may also help explain reciprocal impacts of cognitive functioning on social support and strain. As noted, adults experiencing cognitive decline may especially need help with IADLs, such as remembering to take medicines and managing finances (Jekel et al. 2015; Lau et al. 2015). Receiving regular help with daily activities may result in parents with poorer cognitive functioning perceiving their children as supportive. However, most research indicates that the role reversal that takes place when children care for parents can cause strain in parent–child relationships (Kaufman and Uhlenberg 1998; Liao et al. 2018; Pearlin et al. 1990; Spitze and Gallant 2006).
Third, the frequency with which parents and children interact could further explain links between parents’ reports of support and strain from children and cognitive functioning. Adults with more positive relationships with their children may be more likely to meet and interact with them (Lawton, Silverstein, and Bengtson 1994). Frequent social interaction can help to maintain cognitive functioning organically by stimulating brain activity (Hultsch et al. 1999; Seeman et al. 2001). Thus, older adults who have more supportive and less strained relationships with children may have better cognitive functioning in part because they often interact with them. Contact with children may also mediate impacts of cognitive functioning on support and strain in relationships with children. Parents experiencing cognitive decline may need to interact with their children more frequently and perceive greater support from them partly for this reason. Conversely, because relationships with those who we interact with often are frequently more fraught than relationships with more distant network members (Birditt et al. 2017; Offer and Fischer 2018; Suitor et al. 2022), increased contact with children may result in greater strain in these relationships.
Research Questions
Drawing on theory and research on the life course perspective, the stress process, and intergenerational ambivalence, our study adds to the literature on social relationships and cognitive functioning by examining the following research questions.
Research Question 1: How are social support and strain from children related to older adults’ cognitive functioning over time?
As underscored by the concept of intergenerational ambivalence, social support and strain often coexist in parent–child relationships. Literature highlighting that social support predicts better health and that relationship strain can be a source of stress suggests that social support from children will be positively linked and strain negatively linked to parents’ subsequent cognitive functioning. However, strained relationships with children may still be cognitively stimulating, and strain may arise in relationships where children act to control health behaviors. Thus, an alternative possibility is that strain from children is unrelated or even positively linked to later cognitive functioning.
Research Question 2: How is older adults’ cognitive functioning related to subsequent social support and strain from children?
The literature also supports different possibilities regarding reciprocal effects of cognitive functioning on social support and strain from children. Although individuals with poorer health may need and perceive more social support from children, receiving help from and feeling dependent on children may introduce relationship strain.
Research Question 3: Do depressive symptoms, receipt of children’s help with functional limitations, and coresidence or in-person contact with children help to explain longitudinal links between social support and strain from children and cognitive functioning?
As described previously, these three constructs represent diverse potential pathways through which social support and strain and cognitive functioning may be linked. Depressive symptoms may be impacted by both support and strain from children, leading to changes in cognitive health over time. Parents with more supportive and less strained relationships with children may receive more help with functional limitations from them, helping them maintain cognitive health over time. Last, coresidence and frequent in-person contact with children could mediate the social support/strain and cognition link because frequent interaction in supportive relationships helps maintain cognitive functioning.
Data and Methods
Data and Sample
Data came from the 2006 to 2020 waves of the Health and Retirement Study (HRS). The HRS is an ongoing, biennial panel survey of over 20,000 U.S. adults age 50+ and their spouses conducted by researchers at the University of Michigan and supported by the National Institute on Aging and the Social Security Administration (Juster and Suzman 1995). The first wave was collected in 1992 among 12,654 adults born from 1931 to 1941. Seven new cohorts of adults age 50+ have been added since. A self-administered, leave-behind psychosocial and lifestyle questionnaire including questions about perceived social support and strain in relationships was added to the HRS in 2006 (Smith et al. 2017). One random half of HRS respondents were first given the leave-behind questionnaire in 2006, and the other half was first given the questionnaire in 2008. The leave-behind questionnaire is provided to each alternating half of the sample every other survey wave, resulting in a gap of four years between leave-behind questionnaires. Thus, for this study, the baseline time point (T1) was either 2006 or 2008, T2 was 2010 or 2012, T3 was 2014 or 2016, and T4 was 2018 or 2020.
The base sample for these analyses was HRS respondents who had been born before 1954 and joined the study by 2004, answered a baseline leave-behind questionnaire and at least one of the three follow-up leave-behind questionnaires, reported at least one child or stepchild over age 18 at every wave, and had normal cognitive functioning scores in 2004 or 2002 (N = 8,668). To achieve the same analytic sample across the various analyses, we excluded respondents who were missing data on non-time-varying covariates and without at least two waves of data on time-varying covariates, producing an analytic sample size of N = 7,639. The analytic sample differed from the sample excluded due to missing data across several characteristics, including that they were on average in better health, more likely to be White and married, higher income, and reported more social support and less strain in relationships with children. However, analyses including respondents with missing data produced substantively identical results (abbreviated results for main models shown in Table S1 in the online version of the article).
Variables
Cognitive functioning
Cognitive functioning was assessed with an adapted version of the Telephone Interview for Cognitive Status (TICS), a widely used tool to screen for cognitive impairment in individuals who cannot be assessed in person (Brandt, Spencer, and Folstein 1998; Crimmins et al. 2011; Ofstedal, Fisher, and Herzog 2005). A variety of studies show that the TICS has high test-retest reliability and is a valid predictor of cognitive functioning when compared to in-person exams in diverse older adult populations (e.g., Desmond, Tatemichi, and Hanzawa 1994; Knopman et al. 2010; Moylan et al. 2004). It provides a global measure of cognitive function that encompasses memory, executive functioning, and attention by including the following components: (1) ability to recall 10 words both immediately after they are read and after a brief delay (0– 20 points), (2) ability to subtract 7 from a given starting number five times (0–5 points), and (3) ability to count backwards from a given number (0–2 points). Total TICS scores ranged from 0 to 27. Scores of 0 to 6 indicated likely dementia, scores of 7 to 11 suggested cognitive impairment without dementia, and scores of 12 to 27 were interpreted as in the normal cognition range (Crimmins et al. 2011).
Social support and strain from children
The HRS leave-behind questionnaire included three questions measuring social support from children and four measuring strain in relationships with children. These items were from scales developed by Walen and Lachman (2000) and were designed to be combined to provide continuous estimates of social support and strain from network members. They measured perceptions of social support and strain, which have consistently been found to be more important for health indicators than objective exchanges (Cohen, Underwood, and Gottlieb 2000). For brevity, we refer to them as “social support” and “strain.” The three support items asked how much respondents feel that their children understand the way they really feel, that they can rely on them if they have a serious problem, and that they can open up to them if they need to talk about their worries. The four strain questions asked how much respondents feel that their children make too many demands on them, criticize them, let them down when they are counting on them, and get on their nerves. Response categories included a lot (coded 3), some, a little, and not at all (coded 0). Social support scores ranged from 0 to 9 (high support), and strain scores ranged from 0 to 12 (high strain). Cronbach’s alpha at baseline in 2006 was .83 for the social support items and .78 for the strain items, indicating good internal reliability.
Depressive symptoms
Depressive symptom scores were measured with eight items from the Center for Epidemiologic Studies–Depression scale (Radloff 1977). The items asked whether respondents felt depressed, felt that everything was an effort, had restless sleep, were happy, felt lonely, enjoyed life, felt sad, or could not get going during much of the prior week. Positive items were reverse-coded, producing scores that ranged from 0 to 8.
Receipt of children’s help with functional limitations
HRS respondents who indicated that they have any difficulty with a series of activities of daily living (ADLs; getting across a room, dressing, bathing, eating, getting into or out of bed, using the toilet) or IADLs (preparing a hot meal, shopping for groceries, making a phone call, taking medications) due to a health or memory problem were asked whether anyone ever helps them with those activities. If they received help, they were asked to identify who helped them. We created time-varying dummy variables identifying respondents who (1) had ADL limitations and did not receive help from children, (2) had ADL limitations and received help from children, (3) had IADL limitations and did not receive help from children, and (4) had IADL limitations and received help from children. The comparison category for these variables was respondents who did not have IADL/ADL limitations. We measured help with ADL and IADL limitations separately because IADL limitations often appear early in the trajectory of cognitive decline and require less intensive care and support than ADL limitations (Jekel et al., 2015; Lau et al., 2015).
Coresidence and weekly in-person contact with children
We identified the presence of coresident children from household rosters. HRS respondents were also asked how often on average they meet up with any of their children that do not live with them, including chance and arranged meetings. From these data, we created mutually exclusive time-varying dummy variables identifying respondents who (1) did not live with children but met with children at least weekly, (2) lived with children but did not meet non-coresident children weekly, and (3) both lived with children and met non-coresident children weekly. The comparison category was respondents who neither shared a home with nor had weekly in-person contact with any child.
Other covariates
Non-time-varying analytic variables included age in years at T1, race-ethnicity (Black, Hispanic, and non-Hispanic White), foreign-born, female, and years of education. Other time-varying covariates included household income quartile, employment status, and marital/partnership status. We also included time-varying covariates for number of children and whether at least one non-coresidential child lived within 10 miles, both of which may impact respondents’ opportunities to perceive support or strain from children.
Analytical Approach
Multivariate analyses showed results from linear dynamic panel models leveraging the command xtdpdml in Stata (Moral-Benito, Allison, and Williams 2019; Williams, Allison, and Moral-Benito 2018). These models nest observations at different time points within individuals, helping to account for unobserved, time-invariant heterogeneity and supporting the investigation of within-individual change in an outcome (e.g., cognitive functioning) over time as predicted by independent variables (e.g., social support and strain in relationships with children). A type of structural equation model, they also accommodate lagged predictor and outcome variables, helping adjust for reverse causality between outcomes and predictors. This method is especially useful for modeling relationships where prior values of the independent and dependent variables are theorized to impact later values of the outcome, as was the case in our study. We also included contemporaneous measures of predictor variables in the dynamic panel models to achieve a fuller picture of how predictors and outcomes were linked not only over time but also at the same point in time. The xtdpdml command simplified the specification of dynamic panel models, allowed for the inclusion of time-invariant predictor variables, and supported Stata’s full-information maximum likelihood approach for missing data.
We also drew on findings from cross-lagged structural equation models to assist with interpreting longitudinal mediation effects (Demirer et al. 2021; Newsom 2015). These analyses estimated indirect effects of predictors at T1 on outcomes at T3 through depressive symptoms, help received from adult children, and contact with adult children at T2.
Results
Bivariate Analyses
Bivariate differences between those in the top and bottom tertiles of social support and strain from children scales at T1 are presented in Table 1. Overall, these results suggest that those reporting lower levels of both support and strain in relationships with children were in better health, more likely to be men, and less likely to live near children than those indicating higher levels of support and strain. In addition, older and nonworking parents were more likely to report high levels of support and lower levels of strain in their relationships with children. Parents reporting low levels of support from children also had fewer years of education and lower household incomes than those indicating higher levels of support. Descriptive statistics for the whole sample with bivariate analyses comparing characteristics of those who were and were not cognitively impaired by T4 are available in Table S1 in the online version of the article.
Descriptive Statistics across Social Support and Strain from Children Groups in Percentage or Mean (SD; N = 7,639).
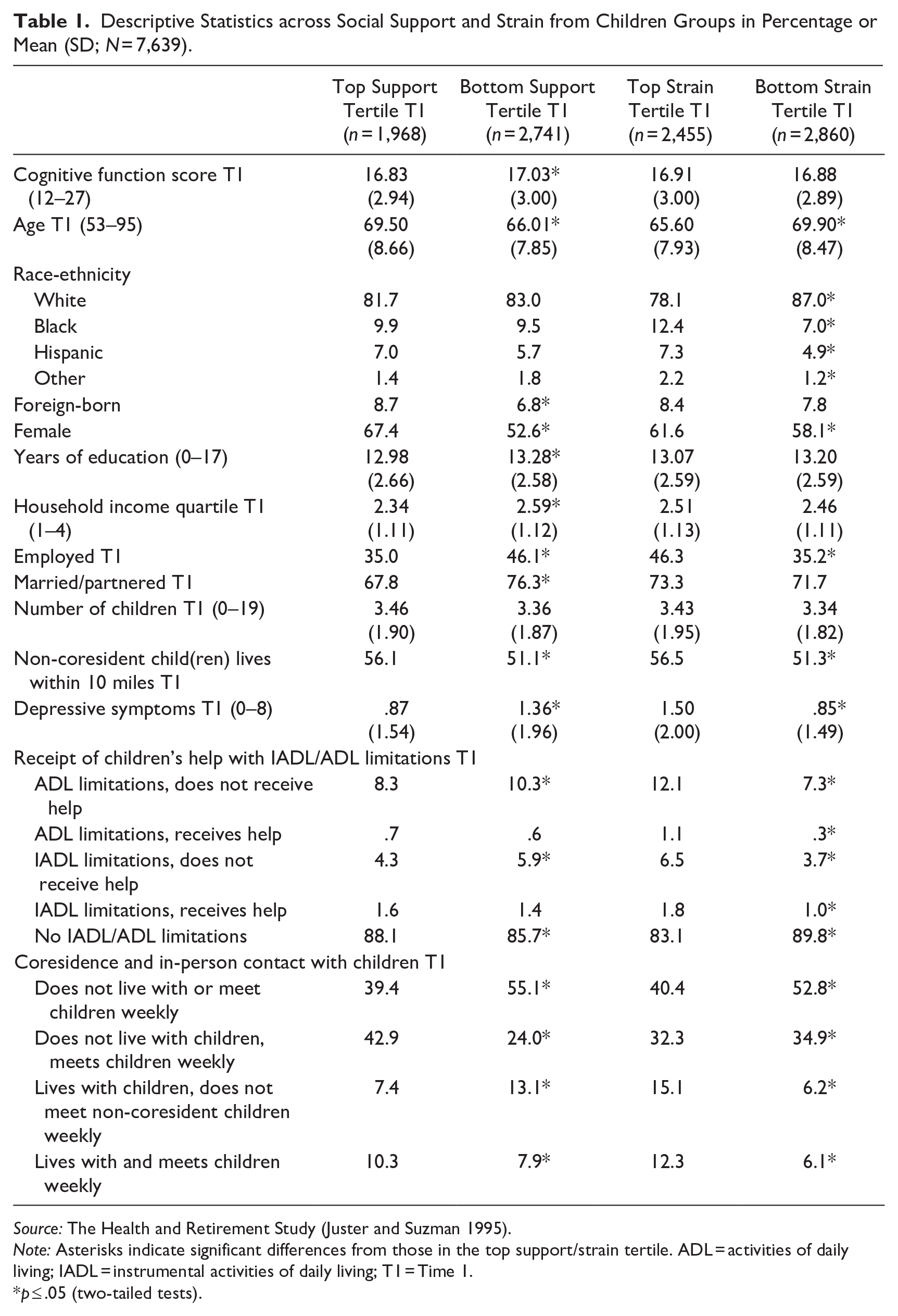
Source: The Health and Retirement Study (Juster and Suzman 1995).
Note: Asterisks indicate significant differences from those in the top support/strain tertile. ADL = activities of daily living; IADL = instrumental activities of daily living; T1 = Time 1.
p ≤ .05 (two-tailed tests).
Social Support and Strain in Relationships with Children and Later Cognitive Functioning
Table 2 shows coefficients from linear dynamic panel models regressing cognitive functioning on social support (Models 1–4) and strain from children (Models 5–8). T1 is represented in the first lagged variables, and coefficients are interpretable as the average effect of predictors on cognitive functioning from T2 to T4 accounting for prior cognitive functioning scores. Model 1 shows that lagged cognitive functioning scores from four years prior were strong predictors of later cognitive functioning. Contemporaneous social support from children was not a significant predictor of cognitive functioning, meaning that perceiving higher support from children was not related to parents’ cognitive health in the same year. However, a 1-point increase in support from children (range 0–9) four years earlier predicted later cognitive functioning scores that were significantly but modestly higher (by an average of .077). Model 1 also shows that average cognitive functioning scores decreased with age, increased with years of education, and were higher among White and female respondents than racial-ethnic minority and male respondents.
Results from Linear Dynamic Panel Models Regressing Cognitive Functioning on Social Support and Strain from Children, T2–T4 (N = 7,639).
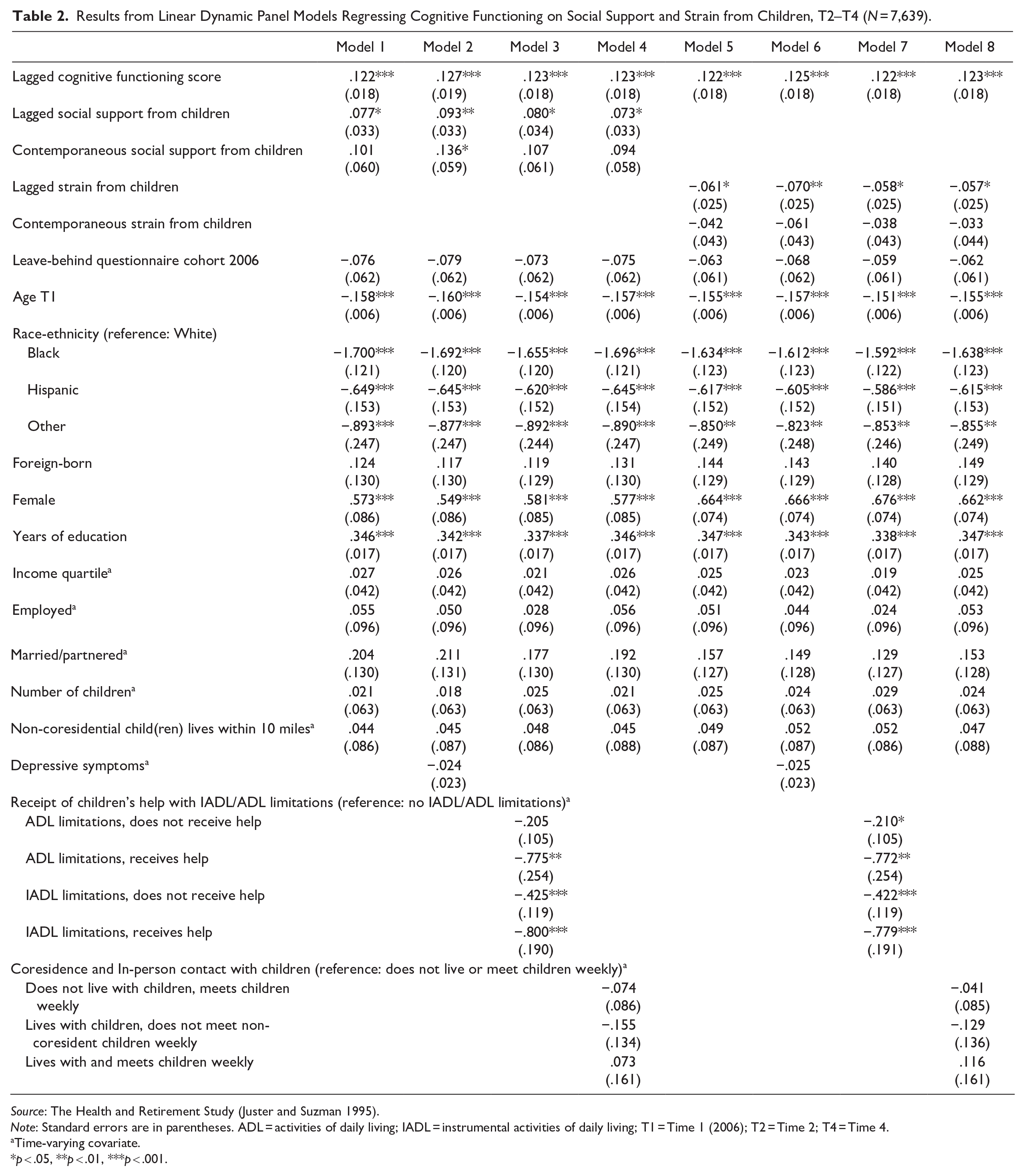
Source: The Health and Retirement Study (Juster and Suzman 1995).
Note: Standard errors are in parentheses. ADL = activities of daily living; IADL = instrumental activities of daily living; T1 = Time 1 (2006); T2 = Time 2; T4 = Time 4.
Time-varying covariate.
p < .05, **p < .01, ***p < .001.
Added in Model 2, depressive symptoms were not related to cognitive functioning in these models controlling for prior cognition. However, the coefficient for lagged social support from children became stronger, and the positive coefficient for contemporaneous social support became marginally significant, suggesting that the presence of depressive symptoms may suppress positive effects of social support from children on cognitive functioning. In addition, mediation analyses (Model 1 of Table 4) show that social support had a significant positive indirect effect on cognitive functioning through depressive symptoms. Consistent with expectations, this suggests that social support predicts better cognitive functioning in part by reducing depressive symptoms.
Model 3 added receipt of children’s help with functional limitations related to health or memory problems. Having and receiving children’s help with either ADL or IADL limitations was a strong predictor of poorer cognitive functioning, as was having IADL limitations without receiving help from children. However, help with functional limitations did not explain any part of the links between social support from children and cognition, and mediation analyses in Model 1 of Table 4 indicate it was not an indirect pathway from social support to cognitive functioning. Counter to expectations that increased interaction with children helps maintain cognition, Model 4 shows that coresidence and in-person contact with children were unrelated to cognitive functioning and did not impact links between social support and cognitive functioning. Model 1 of Table 4 again shows that social support did not impact cognition through indirect effects on coresidence and contact with children.
Model 5 shows that strain in relationships with children four years prior predicted later cognitive functioning scores that were modestly lower after accounting for cognitive functioning at the prior time point. Each 1-point increase in strain predicted a .061 decrease in respondents’ cognitive functioning scores. However, as with social support, contemporaneous strain in relationships with children was unrelated to cognitive functioning in the same year. In Model 6, controlling for depressive symptoms, the relationship between strain and later cognitive functioning became stronger. Mediation analyses in Model 2 of Table 4 indicate that social strain had a negative indirect effect on later cognitive functioning through depressive symptoms. Similar to findings for social support, these findings suggest that depressive symptoms may have suppressed the negative cognitive functioning impacts of strain in relationships with children and that strain exerted a negative impact on cognitive functioning in part by increasing depressive symptoms. Links between strain from children and cognitive functioning remained unchanged when accounting for receipt of help with functional limitations and coresidence and in-person contact with children in Models 7 and 8. Model 2 of Table 4 also shows that strain did not negatively impact cognitive functioning through its effects on either of these child relationship contexts.
Cognitive Functioning and Later Social Support and Strain in Relationships with Children
Results of analyses regressing social support (Models 1–4) and strain (Models 5–8) in relationships with children on cognitive functioning are presented in Table 3. Prior levels of social support and strain from children were strong predictors of later levels, as indicated by the lagged outcome variables. Model 1 shows that neither lagged nor contemporaneous cognitive functioning scores were significant predictors of social support from children from T2 to T4. Social support from children increased with age, and women and unpartnered respondents reported greater support from children than men and respondents who were married or partnered.
Results from Linear Dynamic Panel Models Regressing Social Support and Strain from Children on Cognitive Functioning, T2–T4 (N = 7,639).
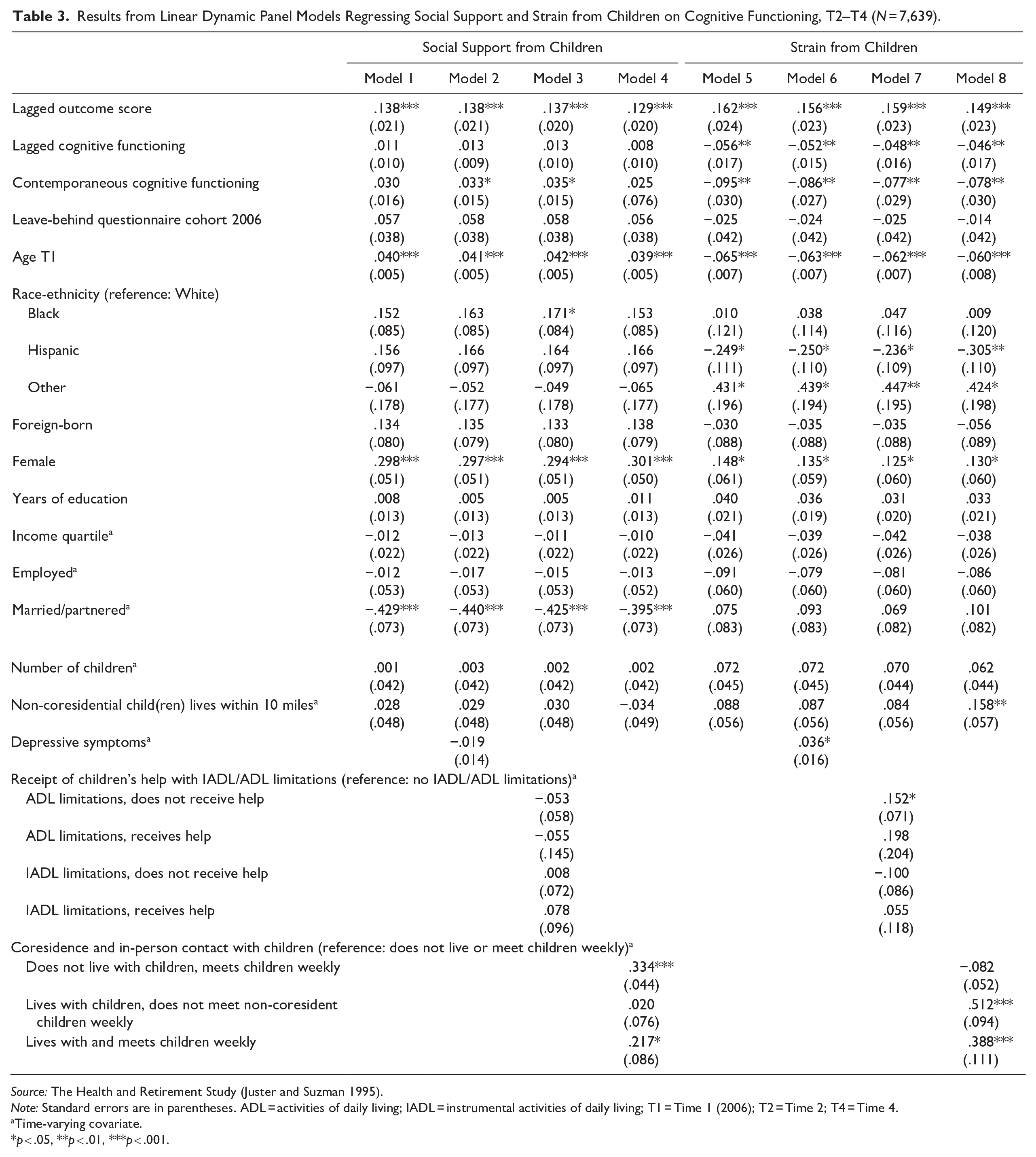
Source: The Health and Retirement Study (Juster and Suzman 1995).
Note: Standard errors are in parentheses. ADL = activities of daily living; IADL = instrumental activities of daily living; T1 = Time 1 (2006); T2 = Time 2; T4 = Time 4.
Time-varying covariate.
p < .05, **p < .01, ***p < .001.
Models 2 and 3 show that depressive symptoms and receipt of help with functional limitations from children were not significantly associated with social support from children. However, the relationship between contemporaneous cognitive functioning and social support became marginally significant in these models, highlighting the potential roles of depressive symptoms and functional limitations in suppressing or masking positive links between support and cognitive functioning. In addition, mediation analyses in Model 3 of Table 4 show that cognitive functioning had positive indirect effects on social support through both depressive symptoms and functional limitations. In other words, higher cognitive functioning may predict higher subsequent perceptions of social support in part by reducing the odds of depressive symptoms and functional limitations. In Model 4, meeting with children weekly was a positive predictor of social support from children, especially for respondents who did not share a home with a child. The coefficient for contemporaneous cognitive functioning weakened some in this model and became again nonsignificant, suggesting that cognitive functioning did not impact social support through coresidence and contact with children. Consistent with this interpretation, Model 3 of Table 4 shows that coresidence and in-person contact with children was not an indirect pathway between cognitive function and social support.
Estimated Indirect Effects of Predictors on Outcomes from Cross-Lagged Structural Equation Models (N = 7,639).

Source: The Health and Retirement Study (Juster and Suzman 1995).
Note: Standard errors are in parentheses. All models include controls for age, leave-behind questionnaire cohort, race-ethnicity, foreign-born, gender, years of education, income, employment status, marital sttus, number of children, and non-coresidential children living within 10 miles of respondent. ADL = activities of daily living; IADL = instrumental activities of daily living; T1 = Time 1 (2006); T2 = Time 2; T3 = Time 3.
p < .01, ***p < .001.
In models with strain from children as the outcome, higher cognitive functioning four years prior and in the same year predicted lower strain (Model 5). Strain in relationships with children also decreased with age, was lower for Hispanic and higher for other race-ethnicity respondents than for White respondents, and was higher for women than men. Depressive symptoms were positively linked to strain from children in Model 6. Model 7 shows that respondents with ADL limitations who did not receive help from children reported higher levels of strain than peers who were not functionally limited, and Model 8 shows that respondents who lived with children reported more strained relationships with them. The explanatory variables in Models 6 to 8 did not impact the direction or significance of the cognitive functioning–strain link. However, Model 4 of Table 4 reveals negative indirect effects cognition on strain through depressive symptoms and functional limitations. In other words, mediation analyses suggest that better cognitive functioning reduced strain in part by lessening the impacts of depressive symptoms and functional limitations.
Discussion
In this study, we drew on theory and research about the life course, social stress, and intergenerational ambivalence to investigate bidirectional links between social support and strain from children and older adults’ cognitive functioning over 12 years. We also examined three potential pathways through which cognitive functioning and social support and strain in relationships with children may be linked. Table 5 provides a summary of the findings.
Summary of Findings for Relationships between Cognitive Functioning and Social Support and Strain in Relationships with Children (N = 7,639).

Source: The Health and Retirement Study (Juster and Suzman 1995).
Note: + = positive relationship between outcome and predictor/mediator; − = negative relationship between outcome and predictor/mediator; ADL = activities of daily living; IADL = instrumental activities of daily living.
p < .05, **p < .01, ***p < .001.
The results showed that earlier social support was positively related to later cognitive functioning and that strain was negatively related to later cognitive functioning. Accounting for these earlier effects, social support and strain from children were not related to parents’ cognition in the same year, further suggesting that the time ordering of these associations may reflect a causal link. Other steps we took to improve inference about causal ordering include beginning with a sample of adults with normal cognitive functioning, using models that estimate within-individual change in cognition, and including controls for previous levels of cognitive functioning. Thus, although associations are not large, we believe that our findings provide notable support for hypotheses that both social support and strain from family can impact cognitive health.
These findings are consistent with a rich body of research showing that supportive social ties can benefit health and well-being and that strain can be a source of stress with negative health implications (e.g., Fratiglioni et al., 2004; Seeman et al., 2001; Umberson, Crosnoe, and Reczek 2010). They also resonate with theory on the life course and intergenerational ambivalence. In line with the life course perspective focus on the dynamic interplay between individual lives over time (Elder 1994; Elder et al. 2003), our study suggests that how aging parents experience and evaluate relationships with their children has meaningful implications for their cognitive health. Reflecting the theory on intergenerational ambivalence (Fingerman et al. 2020; Luscher and Pillemer 1998; Pillemer and Suitor 2004; Suitor et al. 2022), it also highlights that parent–child relationship experiences and their impacts on the health of older parents can be both positive and negative. Future research may examine joint effects of social support and strain from children to further unravel implications of intergenerational ambivalence for older adults’ cognitive health.
Drawing on theory and research on the stress process (Cohen and Willis 1985; Pearlin and Schooler 1978; Thoits 1995), we explored three potential emotional, instrumental, and relationship structure-based pathways through which social support and strain from children may impact cognitive functioning: depressive symptoms, receipt of children’s help with functional limitations, and coresidence and in-person contact with children. Together, the findings suggest that depressive symptoms play a modest but complex role in shaping the impacts of social support and strain from children on cognitive functioning. Consistent with expectations, mediation analyses indicate that they act as a pathway through which social support and strain partially exert their impacts on cognitive functioning. At the same time, the presence of depressive symptoms may suppress or mask the benefits of social support and the costs of social strain for cognitive functioning. One possible interpretation of these findings is that depression, which can have profound negative impacts on how people experience life and may dull perceptions of the importance of social interactions, somewhat negates both the positive and negative cognitive health effects of relationships. Neither help with functional limitations from children nor coresidence and in-person contact with them appeared to help explain links between social support and strain from children and subsequent cognitive functioning. Other potential mechanisms consistent with the stress process to investigate in future research include parents’ health and lifestyle behaviors and additional psychosocial constructs, such as purpose and meaning in life.
Another contribution of our study was to explore whether cognitive functioning played a role in shaping later social support and strain in relationships with children. Cognitive functioning was negatively related to both contemporaneous and later strain in relationships with children, consistent with research indicating that experiencing health declines can introduce stress to social relationships (Kaufman and Uhlenberg 1998; Liao et al. 2018; Pearlin et al. 1990). In addition, cognitive functioning predicted modestly higher contemporaneous social support from children in models controlling for depressive symptoms and functional limitations, suggesting that the presence of mental and physical health problems may suppress or mask positive concurrent links between cognition and social support. Furthermore, mediation analyses indicated that impacts of cognition on later social support and strain from children were explained partly through depressive symptoms and help with functional limitations. Together, these findings resonate with expectations that links between cognitive decline and poorer mental and physical health may lead to more negative and less positive evaluations of relationships with close family members. Investigating other potential explanatory mechanisms, such as feelings of dependency and compromised ability to maintain relationships as cognition declines, is a task for future research.
As the population continues to age, these insights about the dynamic links between social support and strain in relationships with children and cognitive functioning may prove valuable to researchers and public health scholars searching for ways to help maintain older adults’ cognitive functioning. Families continue to be central to the care and support of older adults in the United States. Our findings suggest that policies and programs to enhance intergenerational social support and limit strain—such as educational programs that foster better communication between parents and their adult children and supports for family caregivers—may have significant, if modest, cognitive health benefits for older adults. In addition, our study underscores the importance of mental health and to a lesser extent, instrumental support with functional limitations as pathways between intergenerational social support and strain and cognitive functioning. Screening and treating for depression and enhancing adult children’s ability to help parents with declining health may help maximize the positive effects of intergenerational social support and minimize the negative effects of strain on cognitive health. In turn, reductions in the pace of cognitive decline could improve how older parents experience their relationships with their adult children.
One important limitation of our study is that the social support and strain measures included in the HRS ask about all children broadly. We thus were unable to explore whether support and strain in relationships with some children, such as those who are older, female, or provide health support to or live with parents, is more strongly related to cognitive functioning than support and strain from other children. Similarly, child contact questions referred to all respondents’ children. Future studies leveraging data providing contextual information about specific children that can be linked to support and strain in relationships with those children are important to shed further light on these links. Another limitation is the four-year gap between waves of data on child relationship quality. Changes in cognitive functioning, relationships with children, and the link between the two that occurred within those time periods are thus not fully captured by this analysis.
Although there is a need for further research to better understand mechanisms, this analysis contributes to research on health, aging, and the family by showing that social support predicts higher cognitive functioning and that strain from children is reciprocally linked to older parents’ cognitive functioning over time. In line with prior theory and research on family, intergenerational ambivalence, and the life course, the findings thus highlight that both positive and negative aspects of how we experience intergenerational relationships can have complex implications for our health and that health can impact how we experience our close relationships.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465251335039 – Supplemental material for Examining Longitudinal Relationships between Social Support and Strain in Relationships with Children and Older Adults’ Cognitive Functioning
Supplemental material, sj-docx-1-hsb-10.1177_00221465251335039 for Examining Longitudinal Relationships between Social Support and Strain in Relationships with Children and Older Adults’ Cognitive Functioning by Jennifer Caputo, Linda Waite and Kathleen A. Cagney in Journal of Health and Social Behavior
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the National Institute on Aging (R03AG072235). The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (Grant No. NIA U01AG009740) and is conducted by the Institute for Social Research at University of Michigan.
Supplemental Material
Supplemental Table S1 and S2 are available in the online version of the article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.