
Abstract
In recent decades, naturalization rates among U.S. immigrants have surged as many seek citizenship to regain lost rights and protections. However, the impact of naturalization on immigrants’ life outcomes, such as health, remains underexplored in academic research. Challenges arising from selection processes complicate the interpretation of any observed health disparities between naturalized citizens and noncitizens. To address this gap, we link restricted-use data from the 2000 U.S. census to individual Social Security records on citizenship change and death, enabling a 20-year observation of naturalization and mortality. Results from discrete-time hazard analysis of mortality risk reveals a significant protective health effect from naturalization, which increases in magnitude among long-term naturalized citizens. The effect is particularly strong across older ages and among groups with lower education, refugee entry status, Hispanic origin, and health limitations. These findings suggest that naturalization represents an important but stratifying source of institutional support for socially vulnerable immigrants.
Keywords
In recent decades, there has been a notable increase in U.S. immigrants pursuing “defensive” or “protective” naturalization in response to an increasingly anti-immigrant policy climate in the United States (Aptekar 2016; Gilbertson and Singer 2003; Massey and Pren 2012; Ong 2011; Van Hook, Brown, and Bean 2006). This trend is characterized by immigrants seeking U.S. citizenship through naturalization to regain certain rights and protections that are revoked from noncitizens, including equal access to public assistance and health care (Nam and Kim 2012; Van Hook et al. 2006). Prior research reveals that naturalization improves health care access (Prentice, Pebley, and Sastry 2005; Sanchez et al. 2017), social and political integration (Hainmueller, Hangartner, and Pietrantuono 2015, 2017), and socioeconomic mobility (Bratsberg, Ragan, and Nasir 2002; Pastor and Scoggins 2012). These have direct and indirect implications for immigrant health, prompting the question: Does naturalization improve U.S. immigrants’ long-term health outcomes? Although some research has begun exploring the consequences of naturalization on health (Guadamuz et al. 2022; Minsart, Englert, and Buekens 2013), addressing selection into naturalization remains a challenge. Using longitudinal data from linked U.S. administrative records, this study aims to systematically evaluate the relationship between naturalization and mortality risk, which serves as a common indicator of health (Parrish 2010).
Drawing from the rich array of theoretical frameworks concerning the social origins of health disparities (Braveman, Egerter, and Williams 2011; Diderichsen, Evans, and Whitehead 2001; Glass and McAtee 2006; Krieger 1994; Link and Phelan 1995; Marmot 2005), it is evident that social conditions can shape health outcomes by differentially providing opportunities, imposing constraints, and directing resources in manners that affect the rates of health risks across social groups. Immigration scholars engaging with this literature have argued that the immigrant experience—especially the policies that shape these experiences (Castañeda et al. 2015; National Academies of Sciences 2018; Perreira and Pedroza 2019), particularly for those who are unauthorized and racialized (Asad and Clair 2018; Hagos and Hamilton 2024)—can limit resources and opportunities and alter the effects of other social conditions in ways that elevate health risks. Leveraging this prior theoretical work and bolstered by empirical evidence indicating that naturalized citizenship augments rather than restricts opportunities, resources, and choices, one could reasonably anticipate that naturalization would exert a positive influence on health, with its effects magnifying over time.
Yet this expectation faces challenges from different selection processes that highlight a different direction and nature to the naturalization–health relationship. The first challenge stems from varying rates of selection into naturalization based on a host of social conditions, including sociopolitical contexts (Bloemraad 2006; Mossaad et al. 2018; Nam and Kim 2012; Woodrow-Lafield et al. 2004), individual attributes (Le and Pastor 2023), and even present health conditions (Gubernskaya, Bean, and Van Hook 2013). This selection process can lead to patterns of disparate health outcomes between naturalized citizens and noncitizens that resemble the effects of influence. Although longitudinal data could help disentangle influence and selection processes, the dominant mode of research investigations thus far has been cross-sectional in nature.
A second challenge stems from institutional barriers that essentially select unauthorized immigrants out of naturalization. These immigrants also face elevated health risks due to persecutory legislation (Asad and Clair 2018; Cheong and Massey 2018; Martinez et al. 2015; Ornelas, Yamanis, and Ruiz 2020). Consequently, it becomes unclear whether any observed health disparities between naturalized citizens and noncitizens are attributable to naturalization improving citizens’ health or unauthorized status worsening noncitizens’ health. To isolate the effects of naturalization, it is necessary to compare the health of naturalized citizens only to noncitizens eligible for naturalization. However, making this distinction has proven to be challenging in prior research due to the sensitive nature of such information (Brown et al. 2019a) and concerns about the accuracy of self-responses (Van Hook and Bachmeier 2013).
This study makes a significant contribution by overcoming current research limitations to investigate the relationship between naturalization and health to the extent that mortality is tied to poor health. We link restricted-use data from the 2000 U.S. census survey responses to Social Security records tracking citizenship changes and deaths from 2000 to 2020. Our analytical sample includes only respondents who, in the 2000 survey, were noncitizens authorized to work (effectively excluding unauthorized immigrants) and had lived in the United States for a minimum of five years. Using discrete-time hazard analysis, we compare the mortality risks between those who naturalized and those who did not while adjusting for baseline social conditions. This research design enables us to mitigate selection effects stemming from these social conditions and from unauthorized status. We focus on mortality risk, which directly impacts life span, as our outcome of interest because it is an externally validated metric for assessing health outcomes. Additionally, mortality does not directly lend itself to selection given that death precludes naturalization.
This research also extends beyond the prevailing focus of immigrant health research, which typically centers on the health and mortality advantage experienced by immigrants in comparison to the native-born population (Markides and Eschbach 2011; Markides and Rote 2015; Mehta and Elo 2012; Riosmena, Kuhn, and Jochem 2017). Our study reveals significant mortality disparities within the U.S. immigrant population between citizens and noncitizens. Specifically, our results indicate a protective effect of naturalization on mortality risk that becomes more pronounced among long-term, naturalized citizen, older adults and individuals with lower education, refugee entry status, Hispanic origin, and health limitations. The findings underscore the role that naturalized citizenship, as a form of credential, may play in stratifying immigrants’ health trajectories over time. We discuss in detail the broader implications of these findings.
Background
Naturalization in the U.S. Context
Naturalization is the legal process by which an individual born outside of the United States and its territories to non-American parents acquires U.S. citizenship. Historically, only free White noncitizens were eligible for naturalization, and those who filed a “declaration of intention” to naturalize gained many rights akin to citizens (Motomura 2006). Declarants, as highlighted by Chin (2020), were granted the ability to vote in many state elections, own land in the United States, be employed by state governments, and join unions for labor protection prior to naturalization. These rights essentially gave White noncitizens a critical advantage over noncitizens of color, who were not eligible to naturalize. U.S. immigration and naturalization statutes eventually became race neutral in 1952. Today, noncitizens who hold legal permanent residence status in the United States for five years or more typically qualify for naturalization, although we note shorter residency requirements for those who are married to a U.S. citizen or have offered up their military service. We refer to this group hereafter as “eligible noncitizens.” 1
In recent decades, the contrast in legal treatment between citizens and noncitizens has grown, even as, or perhaps because, race-based laws are now relegated to the American past. The rights once extended to (White) noncitizens who declared their intention to naturalize disappeared with the removal of racial barriers to immigration and naturalization (Chin 2020), which has led to a burgeoning population of new immigrants from Latin America and Asia. Starting in the 1990s, the U.S. government enacted a series of laws that have further curtailed the rights of noncitizens. These laws, for example, created more obstacles for eligible noncitizens to sponsor family members to the United States, restricted their access to public assistance, and made deportation possible for those who hold a criminal record (Massey and Pren 2012).
As U.S. laws grow increasingly more hostile toward noncitizens, there has been a notable surge in eligible noncitizens seeking naturalization to safeguard their rights (Aptekar 2016; Massey and Pren 2012; Ong 2011) despite the soaring legal fees associated with the process (Pastor et al. 2013). One steep surge occurred after the 1996 welfare reform that complicated eligibility for public assistance, including Medicaid, among noncitizens (Nam and Kim 2012; Van Hook et al. 2006). Over time, the benefits of U.S. citizenship have grown as the costs of noncitizenship have multiplied. Presently, some advantages naturalized citizens hold over noncitizens include priority in sponsoring family members to the United States, immunity from deportation due to criminal records, unrestricted access to public assistance (including health care), voting rights, and federal job prospects. Consequently, naturalization rates have continued to rise. In the following section, we discuss how naturalized citizenship, as a form of credential, may directly and indirectly impact health by providing access to these legal benefits and protections.
Naturalization as a Social Condition Influencing Health
Given the current hostile U.S. reception toward noncitizens and the recent erosion of their rights, naturalization could hold significant consequences for millions of U.S. immigrants beyond the immediate legal benefits they receive. However, the relationship between naturalization and immigrants’ life outcomes, particularly their long-term health, remains inadequately researched. This study first establishes the theoretical grounds for anticipating a positive influence of naturalization on health and, in doing so, synthesizes the state of prior research. Naturalized citizenship functions similarly to other credentials, such as education, by conferring legitimacy on its holders and disproportionately granting them access to opportunities and resources (Collins 2019; Pager 2003). We formulate and test our hypotheses to uncover new insights into the relationship between naturalization and health.
Multiple theoretical frameworks have been developed that aim to understand how social conditions interact with individual biology and genetics to influence health outcomes. These include, for example, fundamental cause theory (Link and Phelan 1995), ecosocial theory (Krieger 2001), risk regulator model (Glass and McAtee 2006), and the social determinants of health approach (Braveman et al. 2011; Marmot 2005, Solar and Irwin 2010), among others. From this extensive literature, we can distill two basic principles that shed light on the relationship between naturalization and health. First, social conditions can exert an upstream or distal influence on health by patterning groups’ exposure and susceptibility to disease risk factors (Braveman et al. 2011; Phelan, Link, and Tehranifar 2010). Second, the effects social conditions have on health may operate cumulatively over the life course (Glass and McAtee 2006; Smith 2003).
Based on the first principle, the effects of naturalization on health likely operate by widening individuals’ opportunity structure and access to resources across the life course, much like other forms of credential (Pager 2003; Rivera 2011). One direct way this occurs is through the improvement of access to public assistance. Long-term legal permanent residents (LPRs) may not qualify for Medicaid, the Children’s Health Insurance Program, or Temporary Assistance for Needy Families (cash assistance for low-income families with children) if they live in certain restrictive states (Urban Institute 2022). Additionally, to qualify for Supplementary Security Income (SSI), LPRs generally must have worked for about 10 years in the United States. Enrollment in SSI is crucial for becoming eligible for other assistance programs (Lacarte, Gelatt, and Podplesky 2024). It is also worth noting that many LPRs who qualify may not apply due to confusion about noncitizens’ eligibility stemming from the 1996 welfare reform (Fix and Passel 1999; Hagan et al. 2003; Potocky-Tripodi 2004).
Studies conducted in U.S. cities (Prentice et al. 2005) and focusing on the Latinx population (Sanchez et al. 2017) have shown that naturalized citizens are more likely to have health insurance and use health care facilities compared to LPRs. According to a 2023 national health survey, naturalized citizens are 3 times less likely to report being uninsured compared to authorized noncitizens (LPRs and visa holders) and 10 times less likely compared to unauthorized noncitizens (Schumacher et al. 2023). They are also less likely to report postponing or forgoing needed care compared to both groups of noncitizens. Health insurance enables health care utilization. It is reasonable that naturalized citizens who have these advantages are better able to mitigate their health risks to improve their long-term health.
Naturalization may enable more distal health benefits by enhancing social and civic engagement, which are positively associated with health (Nelson, Sloan, and Chandra 2019). As noted, citizenship offers immunity from deportation and voting rights, which may improve one’s sense of social belonging and political enfranchisement. In their quasiexperimental studies in the Swiss context, Hainmueller et al. (2015, 2017) compared the integrational outcomes of otherwise similar immigrants who narrowly won versus lost their naturalization referendums and found enhanced social integration among those who won. Naturalized citizens also exercised their rights to vote and felt more politically enfranchised (Hainmueller et al. 2015). Although these studies were conducted on Swiss immigrants, it is reasonable to assume that the integration process operates similarly among U.S. naturalized immigrants, with positive health implications.
Finally, economists argue that naturalization directly improves socioeconomic status by providing access to public sector jobs, many of which require or prefer citizenship and offer better paid and benefits. Having U.S. citizenship may also incentivize long-term investment in U.S.-specific human capital, resulting in greater socioeconomic returns (Bratsberg et al. 2002). Indeed, studies have revealed a positive effect of naturalization on earnings (Bevelander and DeVoretz 2008; Bratsberg et al. 2002; Sumption and Flamm 2012). Pastor and Scoggins’s (2012) research demonstrates an earning differential as high as 7.9%, favoring naturalized citizens over noncitizens.
Evidence of enhanced health care access and utilization, along with increased social, political, and socioeconomic integration among naturalized immigrants, highlights several pathways through which the credential of citizenship may positively impact immigrant health. These pathways are especially important for disadvantaged groups who face greater health vulnerabilities and economic hardships, such as older adults, individuals with lower education levels (Braveman et al. 2011; Marmot 2005), and refugees (Reed and Barbosa 2017). Hispanic-origin immigrants are especially vulnerable as noncitizens due to heightened racialization (Sanchez et al. 2017). The potential for naturalization to help immigrants meet their health care and resource needs informs our first hypothesis.
Hypothesis 1: Naturalized citizenship is associated with a reduction in mortality risk among immigrants.
The second principle, concerning cumulative effects, suggests that if a health advantage exists for naturalized citizens, this advantage should strengthen over time. A long research tradition has explored cumulative (dis)advantage, which refers to how the benefits or drawbacks of one’s social position create ripples through one’s life course, accumulating and intensifying in their effects (Dannefer 2003; Ferraro and Kelley-Moore 2003; Smith 2003; Willson, Shuey, and Elder 2007). Mirowsky and Ross (2005) note that the effects of education on health accumulate over the life course, fostering health-promoting changes from the socioeconomic level down to the behavioral and cellular levels.
The effects of citizenship status on immigrant health may accumulate or “snowball” in similar ways. For instance, naturalized citizens’ enhanced access to health care and more consistent utilization may improve their health in the short term while also reducing the likelihood of major health issues in the future. This, in turn, can lower financial costs and psychological distress over the long run. To our knowledge, this study is the first to investigate whether naturalization has a cumulative effect on health, where longer citizenship lengths lead to greater divergences in health outcomes between citizens and noncitizens. If a cumulative effect exists, it suggests that studying the effects of naturalization only in the short term or through cross-sectional analyses might underestimate its true significance.
Hypothesis 2: Time since naturalization boosts the effect of naturalized citizenship on mortality risk reduction.
Challenges from Selection Effects
Although there is theoretical support and circumstantial evidence for the potential health benefits of naturalization, the presence of selection effects complicates this expectation by offering an alternative explanation to the naturalization–health relationship. Selection effects refer to processes that determine who are likely to naturalize, which may be related to health directly or indirectly. Figure 1 illustrates a path diagram outlining common sources of selection into naturalization (blue arrows) and how these may relate to health. One source of selection stems from general social conditions (Figure 1: selection1) that themselves influence health (Figure 1: influence1). Empirical evidence suggests that a combination of individual attributes (e.g., age, ethnoracial background, and education level), assimilation measures (e.g., length of stay, English ability, and legal status of family members), and context-based attributes (e.g., class of legal entry and context of reception) affect both naturalization odds (Bloemraad 2006; Jones-Correa 2001; Le and Pastor 2023; Liang 1994; Logan, Oh, and Darrah 2012; Mossaad et al. 2018; Riosmena et al. 2015; Van Hook et al. 2006; Woodrow-Lafield et al. 2004; Yang 1994) and health outcomes in both positive and negative directions (Akresh and Frank 2008; Cutler, Deaton, and Lleras-Muney 2006; Golub et al. 2018; Gutin and Hummer 2021; Khuu 2024; Lara et al. 2005).
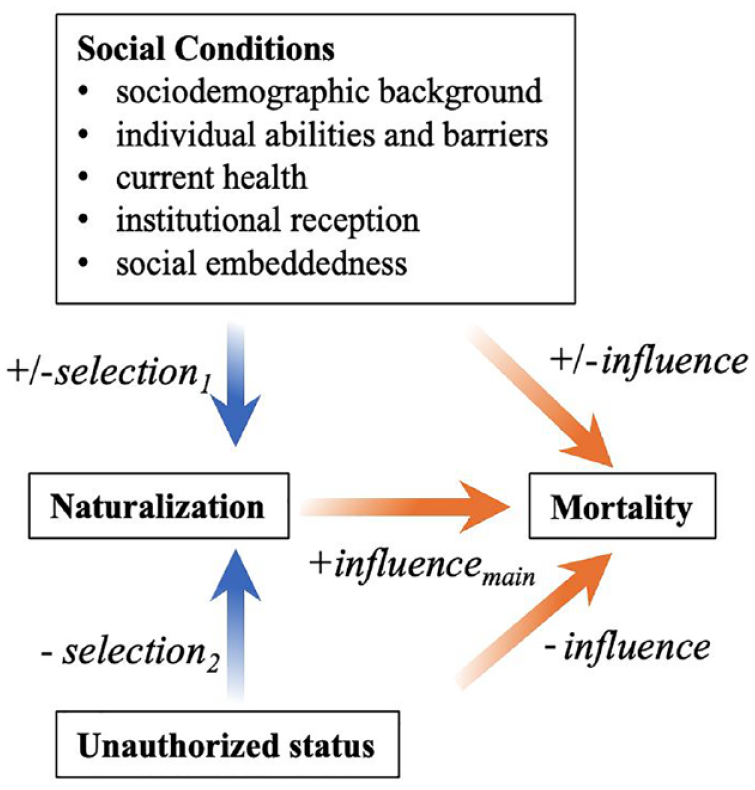
Path Diagram of Sources of Selections and Influences to Consider in the Dynamic Relationship between Naturalization and Mortality.
Current health conditions may also influence naturalization decisions. Healthier individuals may find it easier to naturalize, whereas those in poorer health might be more motivated to naturalize to gain better access to public health assistance (Gubernskaya et al. 2013; Van Natta et al. 2019). Based on the existing literature, we focus on four types of social conditions that may affect both the odds of naturalization and mortality: sociodemographic background, individual abilities and barriers, institutional reception, and social embeddedness. Overall, selection effects may manifest a positive association between naturalization and health, aligning with the anticipated outcome of the influence process we are investigating (Figure 1: influencemain). Thus, although some cross-sectional studies have linked naturalization to lower rates of psychological distress (Gee et al. 2016), older age functional limitations among early arriving immigrants (Gubernskaya et al. 2013), and mortality itself (Riosmena et al. 2015), it remains uncertain whether these findings point to a positive effect of naturalization on health or health-related selection into naturalization. Longitudinal research that could more clearly disentangle influence from selection is notably lacking in the existing research literature, limiting insights into the nature of the naturalization–health relationship.
The complete exclusion of unauthorized immigrants from naturalization represents a second distinct selection effect (Figure 1: selection2), adding greater complexity to the systematic analysis of naturalization and health. Unauthorized immigrants, unlike eligible noncitizens, lack legal authorization to reside in the United States and do not have a pathway toward citizenship. Essentially, they are perfectly negatively selected out of naturalization. With approximately 11 million unauthorized immigrants currently in the United States (Van Hook, Gelatt, and Ruiz Soto 2023), they constitute a significant proportion of the noncitizen population, outnumbering the estimated 9 million eligible noncitizens (Miller and Baker 2023). Facing heightened surveillance and punitive measures, unauthorized noncitizens often encounter barriers to health care access (Hacker et al. 2015; Tuohy 2020) and experience elevated risks of psychological distress and mental illnesses (Arbona et al. 2010; Martinez et al. 2015) and worse health outcomes (Cheong and Massey 2018; Van Natta et al. 2019). Emerging research suggests that unauthorized noncitizens who legalized through the unique opportunity offered by the 1986 Immigration Reform and Control Act (IRCA) subsequently experienced better health care access (Sudhinaraset et al. 2024) and lower mortality (Baker 2010). However, since IRCA, there have been no additional opportunities for unauthorized immigrants to legalize. Hence, they have no pathway to citizenship. Their perpetual noncitizen status coupled with significantly elevated health risks (Figure 1: influence2) raise reasonable concerns that any health advantage observed among naturalized citizens compared to general noncitizens may stem from the effects of unauthorized status.
Hence, to better evaluate the impact of naturalization on health, it is essential to focus on the noncitizen population eligible for naturalization and compare outcomes between those who naturalize and those who choose not to while accounting for other relevant social conditions. Because unauthorized noncitizens are indefinitely ineligible for naturalization and often face additional health disadvantages, excluding them from comparative analysis is imperative. However, prior research comparing the health of naturalized citizens and noncitizens has struggled to identify unauthorized immigrants among noncitizens.
Current Study
This study makes a contribution by systematically addressing selection effects from various social conditions linked to health outcomes, including present health conditions and unauthorized status, to explore two questions that have received limited research attention: Is there a positive impact of naturalization on immigrant health? Do immigrants who have been naturalized citizens for longer periods experience a more pronounced positive health effect? Our study offers several clear advantages for addressing these questions. We used a nationally representative sample of foreign-born respondents from the 2000 U.S. census survey, focusing specifically on noncitizens at the time of the survey. The census survey offers extensive data on individual attributes, which we used to establish baseline social conditions prior to any naturalization or death. This approach enables us to account for selection effects to the extent that they are reflected in these measures. In addition, our data on naturalization and mortality are longitudinal, allowing us to observe subsequent discrete changes in citizenship and mortality statuses over time. Our comparison includes only initial noncitizens who were eligible for naturalization and possessed comparable levels of institutional embeddedness, thereby mitigating negative selection out of naturalization due to unauthorized status and other potential institutional factors. Finally, we use externally validated measures of the main independent (naturalization) and dependent (mortality) variables obtained from Social Security administrative records, thus eliminating potential self-reporting errors or biases.
Data and Methods
The data set used in this study consisted of responses to the long form of the 2000 U.S. census survey (17% of the U.S. population). Respondents were subsequently linked to the Numerical Identification Files (NUMIDENT) using person-unique protected identification keys. The NUMIDENT comprises individual records from the U.S. Social Security Administration for all individuals who have applied for a Social Security number (SSN) since 1936. An SSN is generally required to work in the United States, receive Social Security benefits, and apply for government-administered social services. All U.S. citizens and noncitizens eligible to work are thus eligible and incentivized to apply for an SSN (Brown et al. 2019a). The linkage from the census survey to the NUMIDENT enabled the incorporation of administrative data records, detailing census survey respondents’ date of birth, date of death (if applicable), foreign-birth indicator, current and past citizenship/immigration status, and year of citizenship change (if applicable).
Figure 2 illustrates how our data were structured to better disentangle selection and influence. We first refined our analytical sample to include only noncitizens who were eligible for naturalization in 2000. Eligibility was determined based on whether respondents were classified as a “U.S. citizen” or “legal alien authorized to work” in the NUMIDENT and whether they reported having lived in the United States for at least five years. We excluded those with statuses not certain to have a pathway toward citizenship (i.e., “legal alien not authorized to work,” “other,” “alien student,” and “conditionally legalized alien”). 2 Figure 2 outlines the four hypothetical scenarios involved in our comparative analysis: noncitizens who later naturalized and either died or survived and noncitizens who never naturalized and either died or survived. Regardless of naturalization, it was evident that all respondents were firmly embedded in U.S. legal institutions, having enrolled in the U.S. Social Security system and actively participated in government-administered surveys. This ensured that the comparison groups of this study—those who naturalized and those who did not—shared comparable levels of institutional integration.
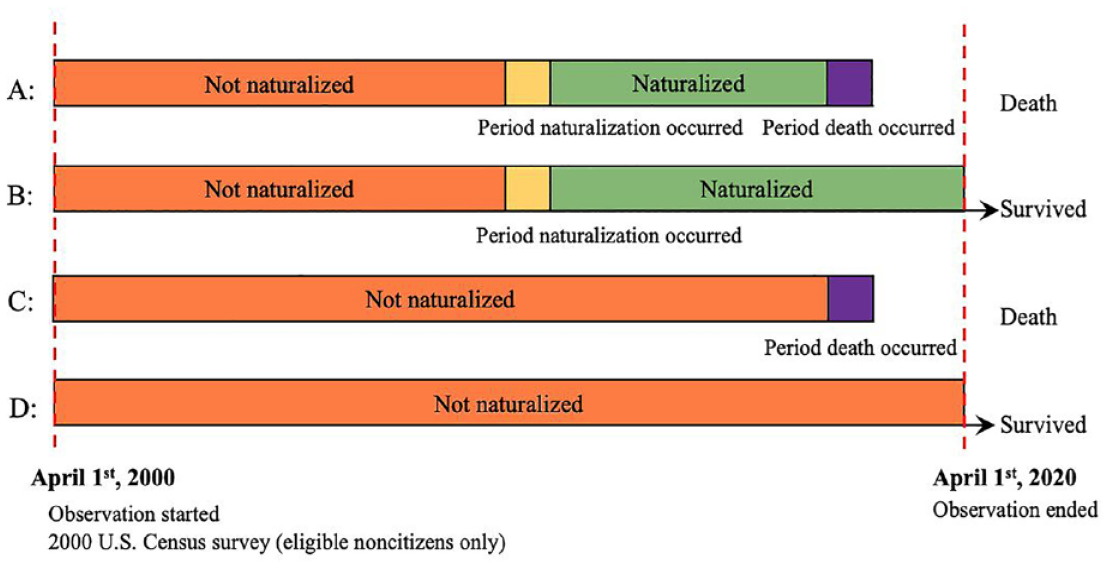
Data Structure Illustrating Four Sequences of Event for Observing Naturalization and Death among Noncitizens Eligible for Naturalization.
We further refined our analytical sample to include only foreign-born respondents who immigrated on or after 1980, were 18 years or older upon immigration, and were working-age noncitizens (25–65 years old) at the time of survey. To reduce potential biases arising from excess deaths due to the COVID-19 pandemic, we censored our data. Hence, we set the observation of citizenship change and death to begin on April 1, 2000, coinciding with when the 2000 census survey was conducted, and to end on April 1, 2020. We drew from the census survey to establish our measurements of baseline social conditions, including health.
Variables
Mortality status
Death was the main dependent variable, a conventional and unequivocal negative health measure (Parrish 2010). The NUMIDENT reported the verified day, month, and year of a respondent’s death. We segmented the span of our observation of death into 20 discrete periods, each equating a year’s length and beginning in April of each calendar year between 2000 and 2020. For each respondent, we used the date of death to code their mortality status for each discrete period: 0 indicates survival, and 1 indicates death, after which point, observation for that respondent ends. For those whose deaths were not observed, their mortality status remains at 0 throughout the 20 discrete periods.
Naturalization
The primary independent variable was naturalization status. The NUMIDENT provided validated information on the timing (year) of citizenship change from the Social Security Administration, constituting a key advantage of these data. Prior studies have demonstrated considerable rates of misreporting of naturalization in self-response surveys (Caron, McAvay, and Safi 2023; Passel and Clark 1997; Van Hook and Bachmeier 2013). With governmental records of naturalization, misreporting was less of a concern in our study.
More specifically, we coded the discrete time periods as follows: Periods when respondents were noncitizens were coded as 0, periods covering the calendar year of naturalization were coded as 1, and periods when they were naturalized citizens were coded as 2. Note that the precise timing of respondents’ naturalization could occur in either of any two contiguous discrete periods that together covers the entire reported calendar year of citizenship change. 3 Our coding scheme for naturalization status distinguished these periods when naturalization occurred as separate from periods when they were noncitizens and when they had already become naturalized citizens because respondents were significantly less likely to pass away during the same periods in which they naturalized, if only because the act of naturalization necessitated that respondents be alive. We also created a continuous variable for naturalization status to indicate the numbers of periods respondents had spent as a naturalized citizen. When employing the continuous variable in our analysis, we also introduced a dummy variable to again distinguish the periods when naturalization occurred from 0 (noncitizen).
Sociodemographic factors
We included sociodemographic background as controls, including respondents’ self-reported gender, ethnoracial background (i.e., non-Hispanic White, Asian, Black, other, and Hispanic), age (at survey), and length of U.S. residence, all of which were derived from information reported in the 2000 census.
Abilities and barriers
We also used data from the 2000 census to account for baseline measures of abilities and barriers, factors that could impact both the odds of naturalization and of death. Baseline ability and barrier measures included individual-level health, years of education, employment status, family income, and English usage at home. Indicators of health included self-reported functional limitations of the following types: work, self-care, independent living, cognitive, mobility, and vision/hearing.
Institutional reception
The kind of institutional reception respondents experienced as immigrants also had impacts on their naturalization propensity and health. We included three variables to account for institutional reception: class of entry, public assistance recipiency, and state-level inclusive policies. For class of entry, we used an estimation method that has been commonly employed in prior research (Capps et al. 2015; Evans and Fitzgerald 2017; Khuu 2024; Khuu and Bean 2022; Tesfai 2023). We categorized respondents as “refugees” if they reported immigrating during a year and from a country where the refugee flow to the United States constituted at least 75% of the total immigration flow. Those who immigrated during a country-year combination where the refugee flow constituted less than 5% of the total immigration flow were categorized as “nonrefugee.” We labeled the residual category as “mix-stream” because it encompasses significant proportions of both refugees and nonrefugees. Statistics on refugee and total immigrant flows came from the 1980 to 2000 U.S. Yearbook of Immigration Statistics (Office of Immigration Statistics 1980).
Public assistance recipiency was a dichotomous variable indicating whether respondents reported receiving SSI or welfare income in the previous year. Finally, we included a count variable indicating the number of inclusive policies adopted by the respondent’s state of residence (0–3), sourced from the Urban Institute (2022). LPRs generally cannot apply for public assistance during their first five years of residence, after which time, eligibility depends on their state of residence. The count variable reflected whether the state provides long-term LPRs with (a) Temporary Assistance for Needy Families, (b) Medicaid and Children’s Health Insurance program, and (3) SSI replacement for those who remain ineligible for SSI due to a shortage of work years (Urban Institute 2022). Although state of residence is rooted in respondents’ 2000 census responses and does not capture subsequent residential changes, the variable is time-varying, reflecting changes in the number of inclusive policies adopted by the states themselves over time.
Social embeddedness
Immigrants who had more social ties in the United States may feel a stronger sense of belonging and thus opt to naturalize, and such ties may also impact mortality risk. Thus, we included respondents’ marital status and the number of children living in their household. Both measures came from the 2000 census.
Analytical Strategy
We employed discrete-time hazard models to conduct our analysis. Discrete-time hazard models are statistical tools commonly applied to person-period data sets to predict the hazard or risk of an event occurring during a particular time interval given that it has not occurred before. In this study, the time intervals were delineated by 20 year-length discrete periods. The events of interest were naturalization and death. Another advantage of discrete-time hazard models is their capacity to accommodate time-varying effects, which was necessary for assessing Hypothesis 2.
Our analytical strategy involved several steps. After describing the data, we initially employed a discrete-time hazard model to predict the risk of naturalization based on social conditions and health measured via the 2000 census. This step helped ascertain whether these conditions indeed act as sources of selection by affecting respondents’ odds of naturalization. Next, we employed a set of discrete-time hazard models to predict the risk of death as a function of naturalization after adjusting for these baseline conditions. This step assessed the influence of naturalization on mortality, addressing Hypothesis 1. Finally, a third set of discrete-time hazard models was used to examine the time-varying effect of naturalization. For this set of models, naturalization status was coded as a continuous variable, representing the number of periods spent as a naturalized citizen. This analysis aimed to determine whether the expected positive impact of naturalization on mortality strengthens with longer durations since naturalization, thereby testing Hypothesis 2.
Results
Table 1 presents descriptive statistics of the analytical sample (N = 740,000) divided into two groups: the never-naturalized group (n = 439,000), consisting of respondents who did not naturalize throughout the observation period, and the naturalized group, consisting of respondents whose naturalization was observed (n = 301,000). It is important to note that all reported statistics, including sample sizes, adhere to U.S. census rounding rules for its disclosure avoidance procedures. Comparing the two subsamples, the never-naturalized group experienced proportionally twice as many deaths (.10) as the naturalized group (.05).
Descriptive Statistics by Naturalization Status.
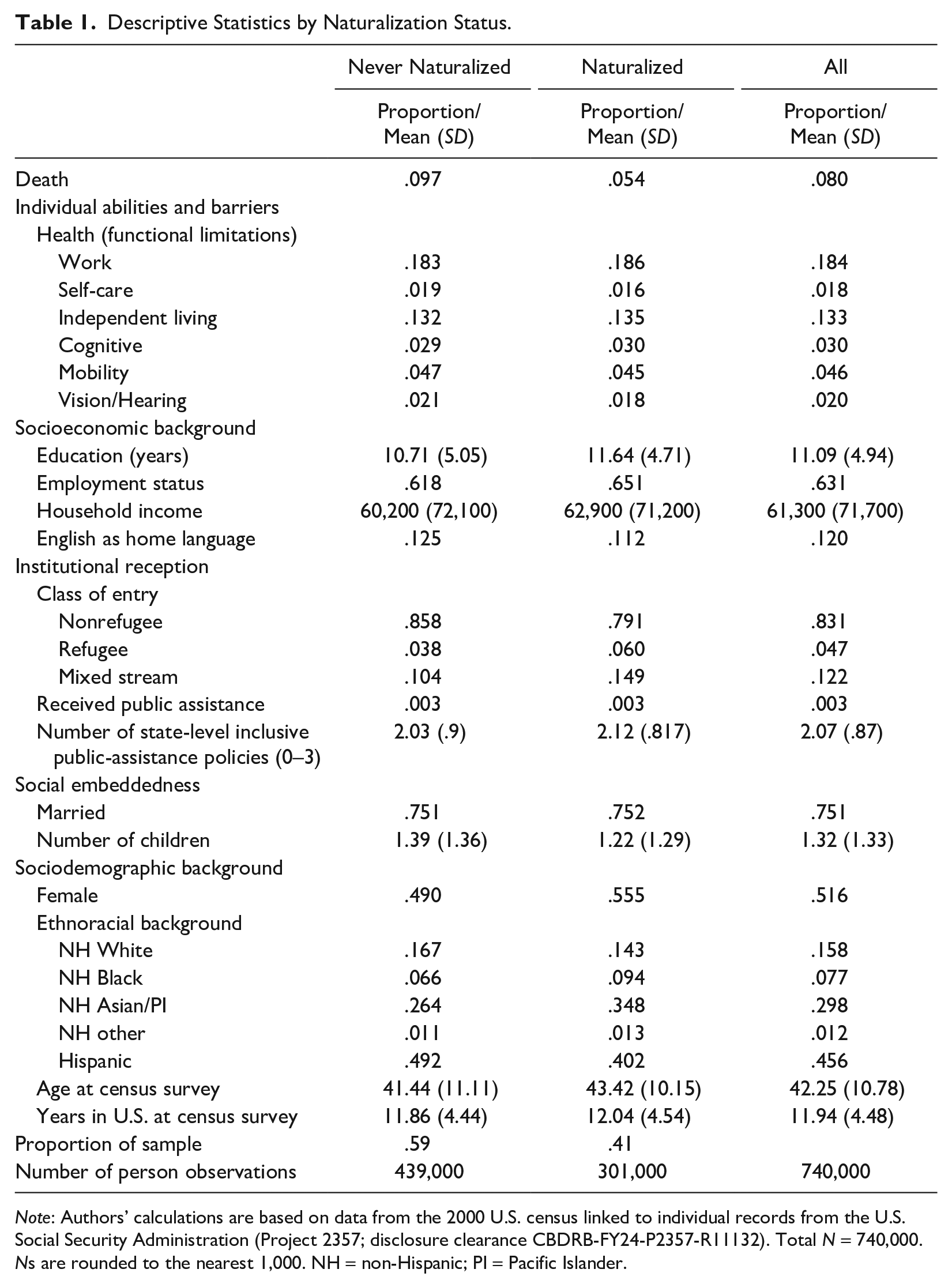
Note: Authors’ calculations are based on data from the 2000 U.S. census linked to individual records from the U.S. Social Security Administration (Project 2357; disclosure clearance CBDRB-FY24-P2357-R11132). Total N = 740,000. Ns are rounded to the nearest 1,000. NH = non-Hispanic; PI = Pacific Islander.
Both groups exhibited comparable baseline health, with similar rates of functional limitations, but differed in socioeconomic background. The naturalized group reported approximately one more year of education (M = 11.6, SD = 4.7) than the never-naturalized group (M = 10.7, SD = 5.1), slightly higher employment rate (.65 vs. .62), and a mean annual income that was $2,700 higher. Differences in institutional reception mainly manifest in class of entry, with nonrefugees being more highly represented in the never-naturalized group than in the naturalized group (.86 vs. .79). The mean number of inclusive policies in the state of residence is also slightly lower for the never-naturalized group (never naturalized: M = 2.0, SD = .90; naturalized: M = 2.1, SD = .92).
In terms of sociodemographic background, the naturalized group comprises proportionally more individuals of Asian and Pacific Islander origin (.35 vs. .26), whereas the never-naturalized group comprises proportionally more individuals of Hispanic origin (.49 vs. .40). The naturalized group is also slightly older than their counterpart (M = 43.4, SD = 10.2 vs. M = 41.4, SD = 11.1). Overall, the comparative descriptive patterns align with expectations. In particular, the direction of the bivariate association between naturalization and death is consistent with the direction predicted by our hypothesis.
Naturalization Risk
Before proceeding to model mortality risk to test our hypotheses, we model naturalization risk to gauge the selection effects of the baseline social conditions. To accomplish this, we conducted a discrete-time hazard analysis where naturalization is the event of interest. The results presented in Table 2, reported in log-odds coefficients and odds ratios, indicate that variables related to sociodemographic background; individual abilities and barriers, including baseline health; institutional reception; and social embeddedness all exert significant influence on the risk of naturalization. All racialized minorities are more likely to naturalize than non-Hispanic White individuals, and each additional year of residence in the United States increases the log-odds of naturalization by .02 (SE = .00).
Estimates from Discrete-Time Hazard Analysis Predicting Naturalization as a Function of Other Social Conditions.
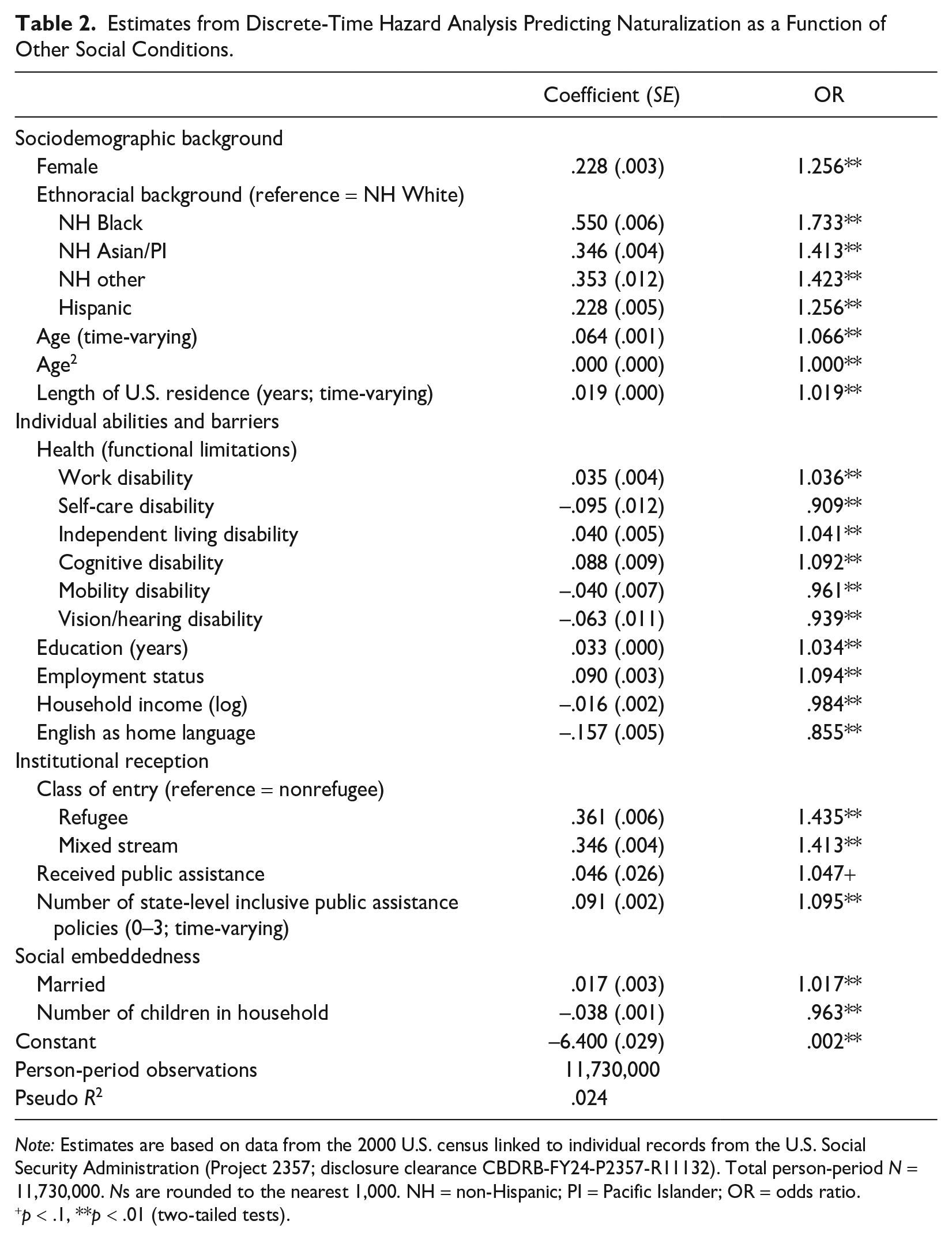
Note: Estimates are based on data from the 2000 U.S. census linked to individual records from the U.S. Social Security Administration (Project 2357; disclosure clearance CBDRB-FY24-P2357-R11132). Total person-period N = 11,730,000. Ns are rounded to the nearest 1,000. NH = non-Hispanic; PI = Pacific Islander; OR = odds ratio.
p < .1, **p < .01 (two-tailed tests).
Baseline health, as measured by different types of functional limitation, has significant effects on the risk of naturalization. However, the direction of the effects varies depending on the type of limitation, suggesting that health can exert both positive and negative selection effects (refer back to Figure 1: selection2). Self-care, mobility, and vision/hearing disabilities, which pose challenges to physically undergo the process of naturalization, are associated with decreased odds of naturalization, whereas work, independent living, and cognitive disabilities are associated with increased odds.
Similar variability exists for other social conditions, with effects showing mixed directions. For example, among variables measuring individual abilities and barriers, education increases the odds of naturalization (b = .03, SE = .00), but household income decreases it (b = –.02, SE = .00). With regard to social embeddedness, being married is associated with increased odds of naturalization (b = .02, SE = .00), but number of children is associated with a decrease (b = –.04, SE = .00). The direction of selection is clearer for institutional reception, with enhanced institutional support (i.e., refugees or mixed stream immigrants vs. nonrefugees, recipiency of public assistance, more state-level inclusive policies) associated with significantly increased odds of naturalization. The effect is particularly strong for class of entry (refugee: b = .36, SE = .01; mixed stream: b = .35, SE = .00). Nevertheless, the overall small pseudo r2 (.024) of the model suggests that the strength of the relationship between these baseline conditions and naturalization is weak, indicating that the model’s ability to capture the propensity to naturalize is small.
Mortality Risk
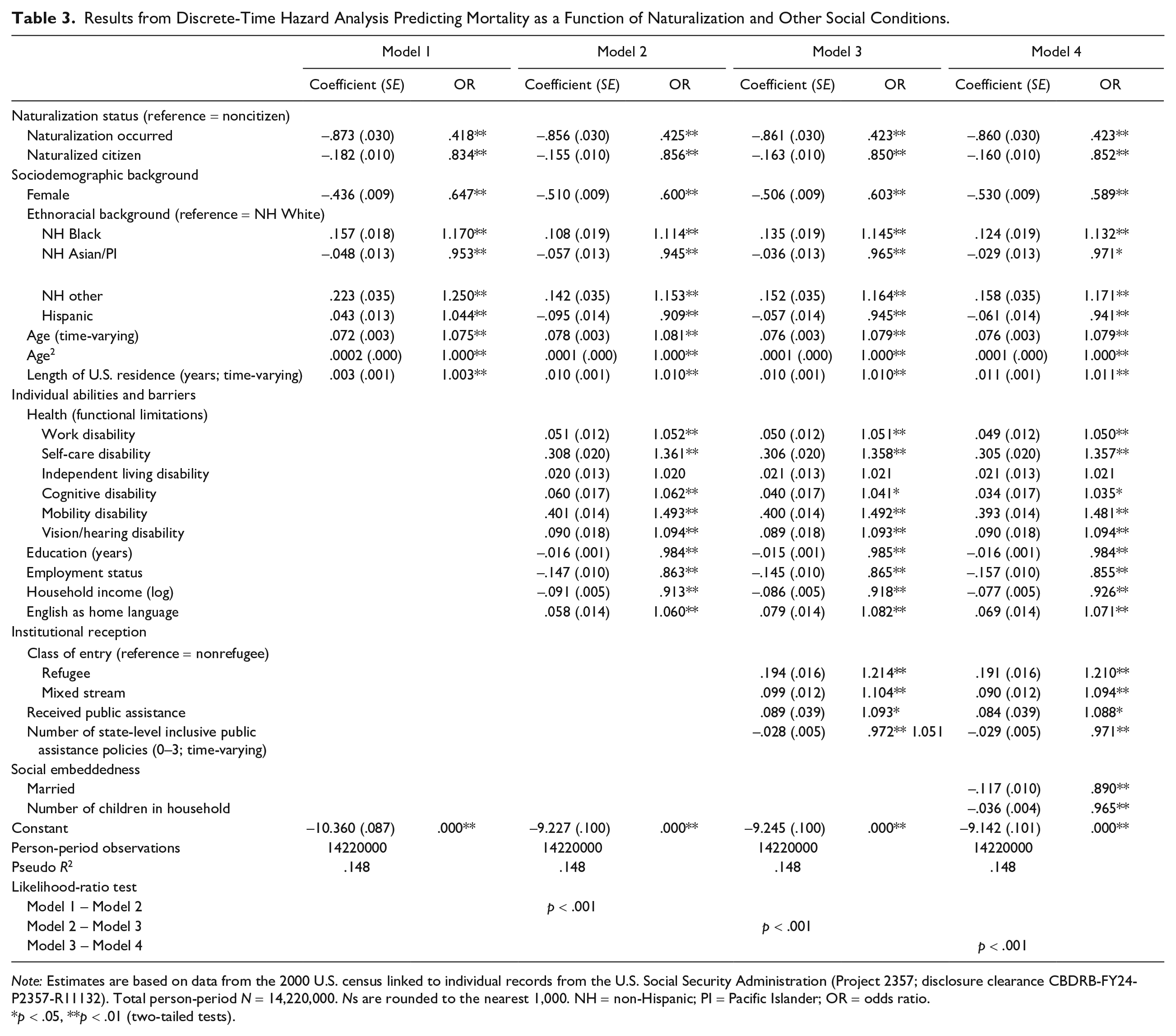
We now present the results of a set of discrete-time hazard models in Table 3 for the purpose of assessing Hypothesis 1, which predicts that naturalization is associated with a reduction in mortality risk. We treated naturalization status as a time-varying variable in the models, meaning that for each discrete period, naturalization status can take on one of three values: (1) noncitizen, (2) naturalization occurred in the time period, or (3) naturalized citizen. Model 1 of Table 3 predicts mortality risk as a function of naturalization status and sociodemographic background. For each successive model, we included additional variables measuring individual abilities and barriers, including health (Model 2), institutional reception (Model 3), and social embeddedness (Model 4). Results from likelihood-ratio tests indicate that the goodness of fit significantly improved for each successive model (p < .001), suggesting that the addition of each type of baseline condition is important for predicting mortality risk. From henceforth, unless noted otherwise, we discuss results based on the fully specified Model 4.
Results from Discrete-Time Hazard Analysis Predicting Mortality as a Function of Naturalization and Other Social Conditions.
Note: Estimates are based on data from the 2000 U.S. census linked to individual records from the U.S. Social Security Administration (Project 2357; disclosure clearance CBDRB-FY24-P2357-R11132). Total person-period N = 14,220,000. Ns are rounded to the nearest 1,000. NH = non-Hispanic; PI = Pacific Islander; OR = odds ratio.
p < .05, **p < .01 (two-tailed tests).
Regarding the main outcome of interest, we observe a significant negative effect of naturalization on mortality risk. The consistency in the magnitude of the naturalized citizen effect across the models (b = –.18, SE = .01 in Model 1 to b = –.16, SE = .01 in Model 4) suggests that the observed association between naturalization status and health is unlikely to stem from selection into naturalization based on the included baseline conditions. In the fully specified model (Model 4), being a naturalized citizen is linked to a 14.8% reduction in the odds of death compared to being a noncitizen [(1 – exp(–.16)) × 100]. Notably, the magnitude of the mortality risk reduction associated with being a naturalized citizen surpasses that of attributes such as being Hispanic origin (b = –.06, SE = .01) or married (b = –.12, SE = .01), both of which are empirically known to be linked to reduced mortality risk (Johnson et al. 2000; Kaplan and Kronick 2006; Markides and Eschbach 2005, 2011). Overall, these results offer support for Hypothesis 1, suggesting that naturalization is associated with a reduction in mortality risk, and its effect is substantial.
Apart from the effects of naturalization, we find expected associations between other social conditions and mortality risks. Before discussing these associations, it is important to note that there is an especially large reduction in mortality risk (b = –.86, SE = .30) during periods when naturalization occurred, indicating, unsurprisingly, that individuals are not likely to die during the year they naturalize. Additionally, longer lengths of U.S. residence are associated with increased mortality risk (b = .01, SE = .00). This finding aligns with prior research indicating a common association between mortality risk and length of residence (Riosmena et al. 2015). Generally, having a functional limitation (except for independent living) significantly raises one’s mortality risk, whereas higher socioeconomic status, in terms of education (b = –.02, SE = .00), employment (b = –.16, SE = .01), and household income (b = –.08, SE = .01), significantly lowers risk. Additionally, being a refugee (b = .19, SE = .02) or a mixed stream migrant (b = .09, SE = .01) increases mortality risk, whereas more state-level inclusive policies decrease risk (b = –.03, SE = .01). These findings are consistent with prior research on the effects of socioeconomic status and institutional context on immigrant health (Gutin and Hummer 2021; Khuu 2024; Perreira and Pedroza 2019).
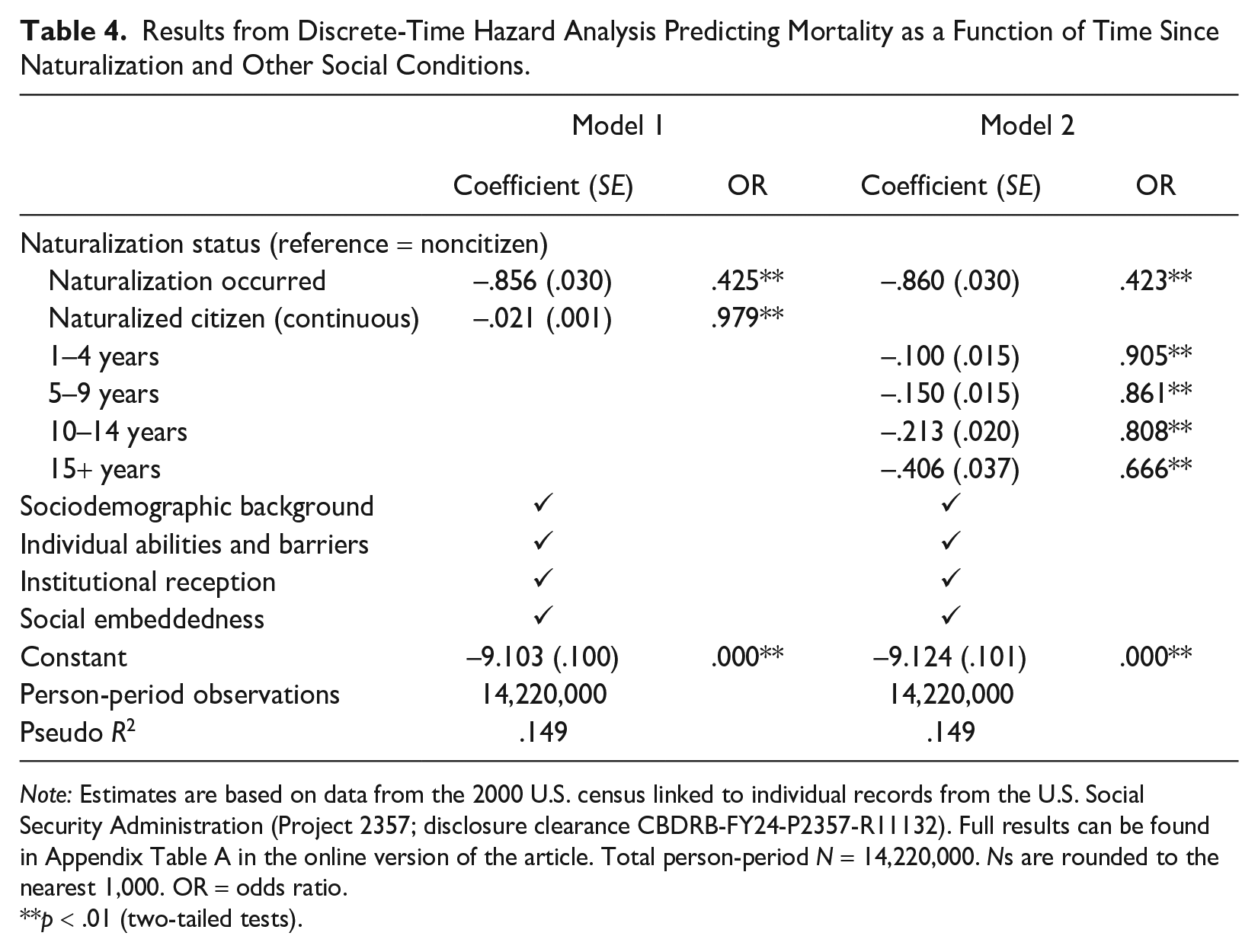
In the next set of models, as shown in Table 4, we explore how the effect of being a naturalized citizen varies over time. This allows us to test Hypothesis 2, which predicts that the longer an individual has been a naturalized citizen, the greater the reduction in their mortality risk compared to a noncitizen. In Model 1, we recode naturalization status to indicate the number of year-length periods the respondent had spent as a naturalized citizen (0 indicates noncitizen). The effect of naturalization is found to be negative and significant (b = –.02, SE = .00), indicating that for each additional year an individual spent as a naturalized citizen, they experienced a 2.1% reduction in the odds of death [(1 – exp(–.02)) × 100]. This finding indicates a cumulative effect of naturalization on mortality risk reduction.
Results from Discrete-Time Hazard Analysis Predicting Mortality as a Function of Time Since Naturalization and Other Social Conditions.
Note: Estimates are based on data from the 2000 U.S. census linked to individual records from the U.S. Social Security Administration (Project 2357; disclosure clearance CBDRB-FY24-P2357-R11132). Full results can be found in Appendix Table A in the online version of the article. Total person-period N = 14,220,000. Ns are rounded to the nearest 1,000. OR = odds ratio.
p < .01 (two-tailed tests).
Model 2 of Table 4 provides a nonlinear approach to modeling the time-varying effects of naturalization. Again, the results demonstrate a substantial and consistent reduction in mortality risk as the time interval spent as a naturalized citizen increases. Holding all else constant, an individual who has been a naturalized citizen for 1 to 4 years experiences a 9.5% reduction in the odds of death [(1 – exp(–.10)) × 100] compared to someone who has not naturalized. This reduction increases to 13.9% for those with 5 to 9 years of naturalized citizenship, 19.2% for those with 10 to 14 years, and 33.3% for those with 15-plus years. These findings offer evidence in support of Hypothesis 2, suggesting that the health benefits of naturalization accumulate over the life course, leading to a substantial mortality advantage over time.
To better understand the mortality advantage of naturalization, we use estimates from Model 2 of Table 3 to graph the predicted marginal probability of death by naturalization status, holding other variables at the mean. Figure 3 shows hypothetical individuals who entered our observation in 2000 with 10 years of U.S. residence. Because mortality risks are minimal among younger adults, the graph focuses on individuals ages 40 or older in 2000. It contrasts the predicted marginal probabilities of death between those who naturalized immediately and those who remained not naturalized across observation years. Figure 3 shows a notable disparity in the predicted probability of death across all initial age groups between individuals who naturalized immediately and those who did not naturalize. This gap widens over time, with individuals of older age groups experiencing a faster rate of increase in this gap over time. For instance, among individuals age 40 in 2000, a slight yet significant disparity in the marginal probability of death by naturalization status emerges after 11 years of observation. However, for those age 70 in 2000, the gap is immediately apparent after Year 1 and exacerbates considerably over time. These results suggest that the benefits of naturalization not only increase with longer periods spent as a naturalized citizen but also are more pronounced for populations that are more vulnerable to adverse health outcomes.
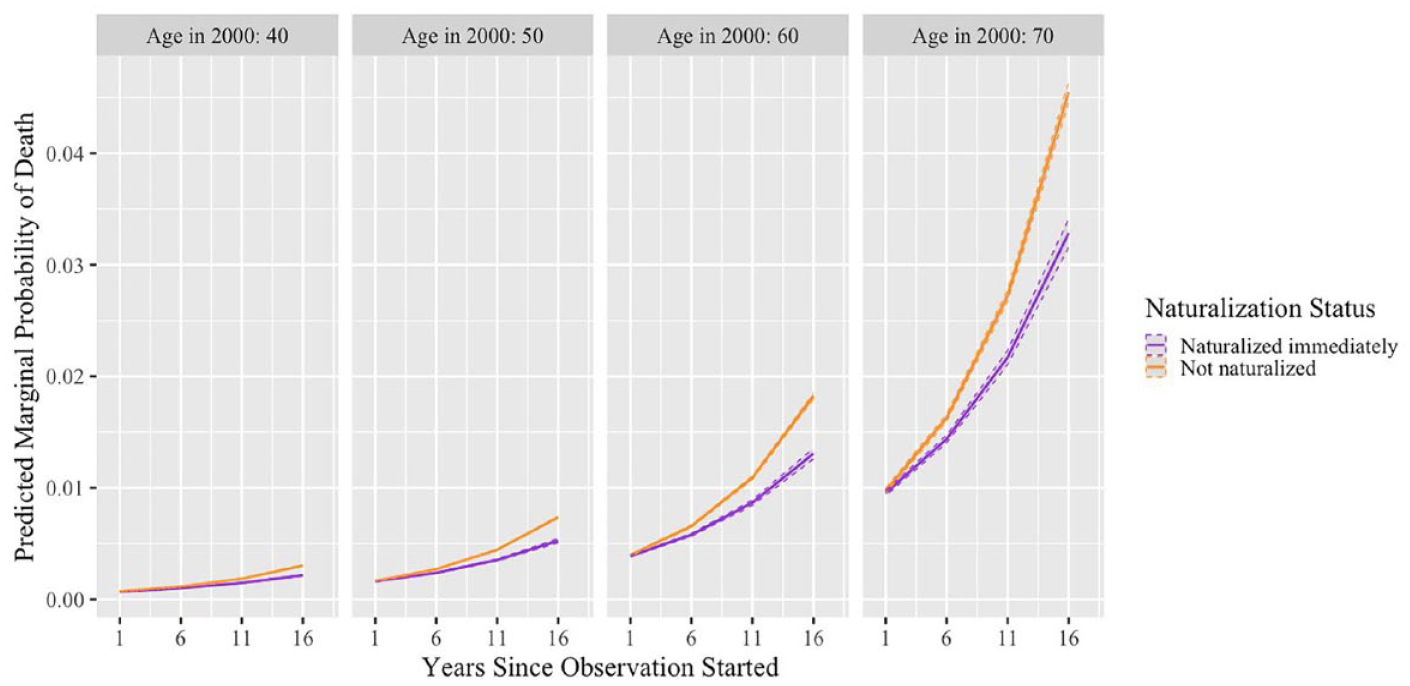
Predicted Marginal Probability of Death by Naturalization Status across Observation Year and Age of First Observation, Based on Estimates from Model 2, Table 3.
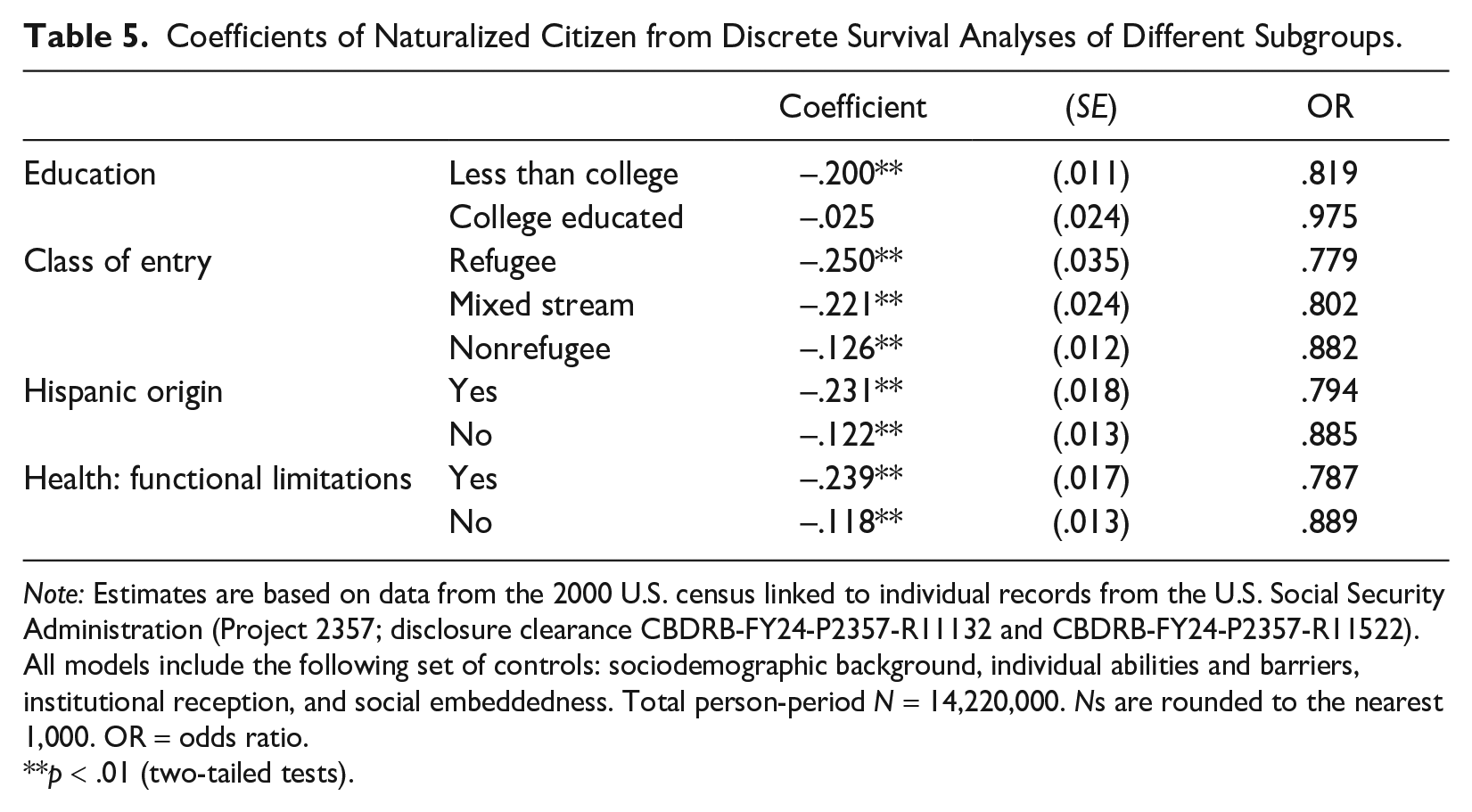
To indirectly test the mechanisms through which naturalization impacts health, we explore whether its impact varies among vulnerable groups who are more likely to use naturalization to improve health care access and resource acquisition. These groups include individuals without a college education, likely refugees upon entry, Hispanic-origin individuals, and people with functional limitations. Results show that compared to their peers without these attributes, individuals belonging to these groups experience a more pronounced effect of naturalization on their mortality risk (see Table 5). In fact, for education level, naturalization significantly reduces mortality risk only among individuals without a college degree (less than college: b = –.20, SE = .01). These findings suggest that more vulnerable and economically disadvantaged groups are positioned to leverage the resource benefits that naturalization brings.
Coefficients of Naturalized Citizen from Discrete Survival Analyses of Different Subgroups.
Note: Estimates are based on data from the 2000 U.S. census linked to individual records from the U.S. Social Security Administration (Project 2357; disclosure clearance CBDRB-FY24-P2357-R11132 and CBDRB-FY24-P2357-R11522). All models include the following set of controls: sociodemographic background, individual abilities and barriers, institutional reception, and social embeddedness. Total person-period N = 14,220,000. Ns are rounded to the nearest 1,000. OR = odds ratio.
p < .01 (two-tailed tests).
Discussion
In recent decades, there has been a notable surge in the rate of eligible noncitizens who choose to naturalize to protect or regain their rights in the United States (Gilbertson and Singer 2003; Massey and Pren 2012; Ong 2011). Although the immediate legal benefits of naturalization are apparent, its impact on immigrants’ long-term health remains unclear. This research fills this gap by assessing the relationship between naturalization and mortality risk using linked administrative data. We discuss the important findings of this research in the following paragraphs.
Results from this research support the proposition that naturalization yields a protective health effect, to the extent that lower mortality risk is indicative of better health. The magnitude of the effect is substantial, surpassing that of other known determinants of health, such as ethnoracial background and marital status. Furthermore, the study reveals a cumulative advantage of naturalization: The reduction in mortality risk intensifies over time, reaching a notable 33.3% decrease in odds of death among naturalized citizens with 15 or more years of citizenship.
These findings highlight the role of naturalization as a determinant of health, aligning with research that emphasizes the importance of immigration policy in health studies (Castañeda et al. 2015; National Academies of Sciences 2018; Perreira and Pedroza 2019). Extant research has established a clear link between unauthorized status and adverse health (Cheong and Massey 2018; Martinez et al. 2015; Ornelas et al. 2020), with unauthorized noncitizens improving their health outcomes upon gaining legal status through IRCA (Baker 2010; Sudhinaraset et al. 2024). This research builds on this body of work, further illustrating how legal status functions as a credential that shapes health outcomes, even within the authorized immigrant population, by providing greater access to resources and opportunities.
The analysis of selection into naturalization reveals that socially disadvantaged groups are opting for naturalization at higher rates, with the exception being those without a college education compared to their more educated peers. All else equal, older adults, refugees, those of Hispanic origin, and individuals with health limitations are more likely to naturalize. They also benefit more from naturalization, showing more pronounced reductions in mortality risk after naturalizing. These findings suggest that naturalization helps immigrants, especially those who are socially vulnerable, better address their health and resource needs.
Policy Implications
The policy implications of this research are complex. On the one hand, promoting more naturalization seems logical given its demonstrated benefits, offering noncitizens a potentially vital means of health protection. With approximately 9 million eligible noncitizens yet to naturalize, efforts could be made to facilitate their access to citizenship, especially considering the rising costs associated with naturalization (Pastor et al. 2013). On the other hand, recent benefits of citizenship have stemmed from the retraction of rights and protections for noncitizens, raising ethical questions about the continued exclusion of noncitizens ineligible for naturalization from the institutional support it affords. Addressing existing disparities in treatment between citizens and noncitizens is complex yet necessary for mitigating health disparities among the U.S. immigrant population.
Limitations and Future Directions
There are a few limitations to consider in this research. First, although we have endeavored to systematically account for selection effects based on baseline health and other measurable social conditions, our ability to do so comprehensively is limited. Factors not easily observable, such as a strong sense of belonging or a desire to make a long-term investment in living in the United States, may motivate individuals to pursue naturalization and could potentially correlate positively with health outcomes. Unfortunately, these aspects are challenging to quantify or measure directly. It is also possible that the baseline conditions included in our study changed between 2000 and the time naturalization occurred, which could create unobserved selection effects.
This research focuses on naturalization in the last two decades, a period marked by significant changes in U.S. immigration policies and attitudes toward noncitizens. Although it offers timely insights into the experiences of today’s immigrants, it remains important to consider whether the observed effects of naturalization on health vary over different time periods. Also, mortality, serving as a key health indicator determining life span, is central to this study; however, it is important to expand this research to examine naturalization’s relationship with other health indicators. Existing studies consistently show an immigrant advantage in mortality outcomes compared to the U.S.-born population (Markides and Eschbach 2011; Mehta and Elo 2012; Riosmena et al. 2017), but this advantage is less consistent across other health measures, such as comorbidity and disability rates (for a review, see Markides and Rote 2015). Along the same vein, although our findings indicate that naturalized citizens exhibit lower mortality risks than noncitizens, this alone does not fully capture their overall health, warranting further investigations into a broader range of health indicators.
Conclusion
Overall, this research produces evidence suggesting that naturalization is associated with a significant reduction in mortality risk among U.S. immigrants today, even after we have systematically accounted for selection effects in innovative ways. Additionally, it is the first study to demonstrate a cumulative advantage of naturalization on health and show more pronounced health benefits from naturalization among more vulnerable populations. We conclude that naturalized citizenship is a form of legal credential that provides critical access to resources within the U.S. immigrant population, with complicated implications for immigrant health and health inequality.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465241310347 – Supplemental material for Living with(out) Citizenship: The Impact of Naturalization on Mortality Risk among U.S. Immigrants
Supplemental material, sj-docx-1-hsb-10.1177_00221465241310347 for Living with(out) Citizenship: The Impact of Naturalization on Mortality Risk among U.S. Immigrants by Thoa V. Khuu, Jennifer Van Hook and Kendal L. Lowrey in Journal of Health and Social Behavior
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Russell Sage Foundation and the Population Research Institute at Penn State University, which is supported by an infrastructure grant by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (P2CHD041025). We thank James Bachmeier, Cheyenne Lonobile, and Ashton Verdery for their valuable feedback on earlier drafts. This research uses data from the U.S. Census Bureau. Any views expressed are those of the authors. The Census Bureau has reviewed this data product to ensure appropriate access, use, and disclosure avoidance protection of the confidential source data used to produce this product. This research was performed at a Federal Statistical Research Data Center under FSRDC Project Number 2357 (CBDRB-FY24-P2357-R11132; R11522; R11594).
Supplemental Material
Appendix Tables A and B are available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.