
Abstract
We present evidence from choice experiments on hypothetical triage decisions in a pandemic. Respondents have to decide who out of two patients gets ventilation. Patients are described in terms of attributes such as short-term survival chance, long-term life expectancy, and their current ventilation status. Attributes are derived from the ethical discourse among experts regarding triage guidelines during the COVID-19 pandemic and differ in the extent to which they are salient from a utilitarian or deontological perspective. Empirically, we find that although nonexperts agree with experts in prioritizing utilitarian attributes in triage decisions, nonexperts also consider the adherence to the norm of wearing face masks as particularly relevant. Furthermore, our study supports Greene and colleagues’ dual-process model of moral judgment; we find that utilitarian attributes are more decisive for respondents with a greater inclination toward utilitarianism and for respondents with a greater tendency toward reflection.
Triage is the prioritization of scarce medical resources in exceptional and catastrophic social situations, such as wars, natural disasters, and pandemics. The COVID-19 pandemic has overwhelmed health care infrastructure in many societies. Shortage and rationing of crucial resources such as intensive care beds and ventilators have become a tragic reality. Even in Western industrialized countries, such as Italy and the United States in 2020, triage decisions were observed. Many COVID-19 sufferers were left to die without adequate medical treatment (Nacoti et al. 2020). The terrible media reports and pictures of the practice of triage, especially in Lombardy, were probably the main impetus for governments worldwide to implement various nonpharmaceutical interventions, such as partial or general lockdowns, to reduce COVID-19 mortality and health care demand (Ferguson et al. 2020).
The necessity to triage limited medical resources in a catastrophic pandemic situation confronts emergency medicine specialists and physicians with an ethical dilemma: They are forced to make decisions between life and death. Against the background of the COVID-19 crisis, scientific communities, medical associations, and ethics committees are currently engaged in a controversial discourse about ethical guidelines for the practice of triage in dealing with pandemics (De Castro-Hamoy and De Castro 2020; Emanuel et al. 2020; Gelinsky 2020; Joebges and Biller-Andorno 2020; Marckmann et al. 2020; Nicoli and Gasparetto 2020). At the same time, lawyers are discussing legislation to establish legal certainty in regard to unavoidable triage decisions (Hörnle, Huster, and Poscher 2021).
Triage decisions apply to both withholding and withdrawing limited medical resources. Beyond medical aspects, triaging unavoidably involves moral choices. It is in the public interest to explicate the normative basis of the choice who will receive medical treatment and has a chance of survival and whose inevitable death will be accepted by withholding or withdrawing intensive care. The ethical values and moral principles of making such choices concern maximizing benefits, treating people equally, rewarding and promoting instrumental value for society (e.g., prioritizing health workers), and giving priority to the worst off (Emanuel et al. 2020:2052). Other criteria such as considering age or rewarding prosocial behavior have been subject to controversial discussion (Joebges and Biller-Andorno 2020). Regarding prosocial behavior, new social norms of fairness and prosociality have emerged during the COVID-19 crisis, such as the requirement to wear face masks and official vaccine recommendations to protect others and oneself from infection (Betsch et al. 2020; Diekmann 2020; Eichenberger et al. 2020; Korn et al. 2020; Krumpal 2020).
At the center of this ethical controversy is the question to what extent the application of the consequentialist principle of utilitarianism (see Mill 1863) conflicts with principles of deontology (see Kant 1797 with his famous idea of the categorical imperative). Whereas utilitarianism prescribes that the moral value of an action should only be determined by its consequences (e.g., choose the action that maximizes beneficial outcomes for the individual and society), a deontological perspective prescribes that the moral value of a choice depends on its intrinsic nature regardless of its consequences (e.g., treating the sick is a moral duty). The latter perspective implies that people are motivated by duties and unconditional moral obligations that prescribe or prohibit certain acts because they are inherently “right” or “wrong” irrespective of the outcomes (Greene 2013). Regarding triage decision, utilitarian considerations, such as maximizing chances of survival or life expectancy, conflict with deontological reasoning, according to which it is morally wrong to withdraw medical care from someone who is in need.
Our article contributes in two respects to the literature on ethical decision-making in triage situations. First, we investigate empirically the prevalent ethical orientations and moral intuitions about triage in German society. Because triage decisions could affect every citizen, it is in the public interest to inform the expert discourse with empirical evidence regarding the prevalent normative orientations in society. We report results of choice-based vignette and conjoint analysis (Auspurg and Hinz 2015; Hainmueller, Hangartner, and Yamamoto 2015; Hainmueller, Hopkins, and Yamamoto 2014; Jasso and Opp 1997; Walker et al. 2018) from three different choice experiments describing a triage scenario in which respondents were presented a series of pairs of two hypothetical patients varying in multiple attributes (e.g., age, the probability of survival, and prosocial behavior) and were asked to choose the one to be treated with the only ventilator available (paired conjoint design with forced choice; see Hainmueller et al. 2015). From a methodological point of view, conjoint analyses come with the decisive advantage of providing estimates for causal effects of attributes (Hainmueller et al. 2014, 2015). Because we implemented the criteria for triage advocated in official triage guidelines as attributes in our choice experiments, this study is informative regarding the questions of how the moral and ethical reasoning by experts encoded in official guidelines for triage converge or diverge with moral reasoning and intuition among nonexperts and how subjects simultaneously balance and weigh multiple and conflicting ethical values in moral dilemma situations.
Second, our study also sheds light on the ongoing discourse in interdisciplinary action theory regarding the theoretical and empirical merits of the dual-process perspective (Lizardo et al. 2016; Miles 2015; Vaisey 2009). In line with dual-process models in cognitive psychology (Greene 2007; Greene et al. 2001), we argue that both rational reflection on ethical principles as well as emotion and intuition play an important role in moral judgments. Former research shows that utilitarian judgments are mainly driven by cognitive processes of rational reflection, whereas deontological judgments are mainly driven by processes of emotion and intuition (Conway and Gawronski 2013; Greene et al. 2001; Tanner, Medin, and Iliev 2008). Relying on this dual-process account of moral judgment, we employ process dissociation to independently measure subjects’ inclination toward both utilitarianism and deontological principles. This technique allows to test two hypotheses derived from Greene’s (2013) dual-process model of moral judgment: first, the hypothesis that subjects’ general orientations toward utilitarianism and deontological principles affect how sensitive their triage decision-making is to attributes, which relate to either the one or the other underlying moral orientation. Second, it allows us to test the hypothesis that attributes that are salient from a utilitarian point of view weigh more heavily in the moral judgments of subjects with a tendency toward cognitive reflection.
Our results show that utilitarian and deontological principles independently contribute to the explanation of triage decisions, although considerable variation in regard to the strength of the causal effects of the single attributes can be observed. Furthermore, our findings provide evidence for a remarkably good matching of the hypothetical choices of our nonexpert respondents with triaging guidelines used by experts (Gelinsky 2020). In particular, the relative importance of attributes reflecting utilitarian principles (maximizing the probability of survival and life years) for explaining the moral choices in our hypothetical triage scenarios match the relative importance of the same attributes in guidelines on COVID-19 triage used by experts to guide actual choices in the real world. At the same time, our study also reveals that public moral reasoning and intuition on triage decisions deviate from expert ethical reasoning in one important respect. We find that subjects make treatment dependent on obeying the norm of wearing face masks, which conflicts with the principle of treating people equally (Emanuel et al. 2020:2051–53). Notably, both hypotheses derived from Greene’s (2013) dual-process model of moral judgment regarding the interaction between underlying moral orientations and the effect of attributes on the one hand and the interaction between the tendency toward cognitive reflection and the effect of utilitarian attributes on the other hand are validated by our data.
In the following section, we give a short overview of the most important ethical aspects of triaging guidelines used in various countries. Based on our review of the current discourse, we identify key attributes of our hypothetical patients. Subsequently, we introduce Greene’s (2013) dual-process model of moral judgment and derive testable hypotheses. Next, we describe the design and the implementation of our choice experiment and present our empirical findings. Finally, we discuss our empirical results, describe limitations of the current study, and hint at future directions for research.
Background
Reconstructing the Ethical Debate among Experts
Relying on the specialized literature regarding the ethics of triage in times of COVID-19 and official guidelines (Brown et al. 2020; De Castro-Hamoy and De Castro 2020; Emanuel et al. 2020; Gelinsky 2020; Joebges and Biller-Andorno 2020), it is possible to identify key attributes of patients that are considered relevant in the discourse among experts (see Table 1; for a more detailed discussion, see A1 in the Appendix in the online version of the article).
Patients’ Attributes, Moral Orientations, and Attribute Levels.
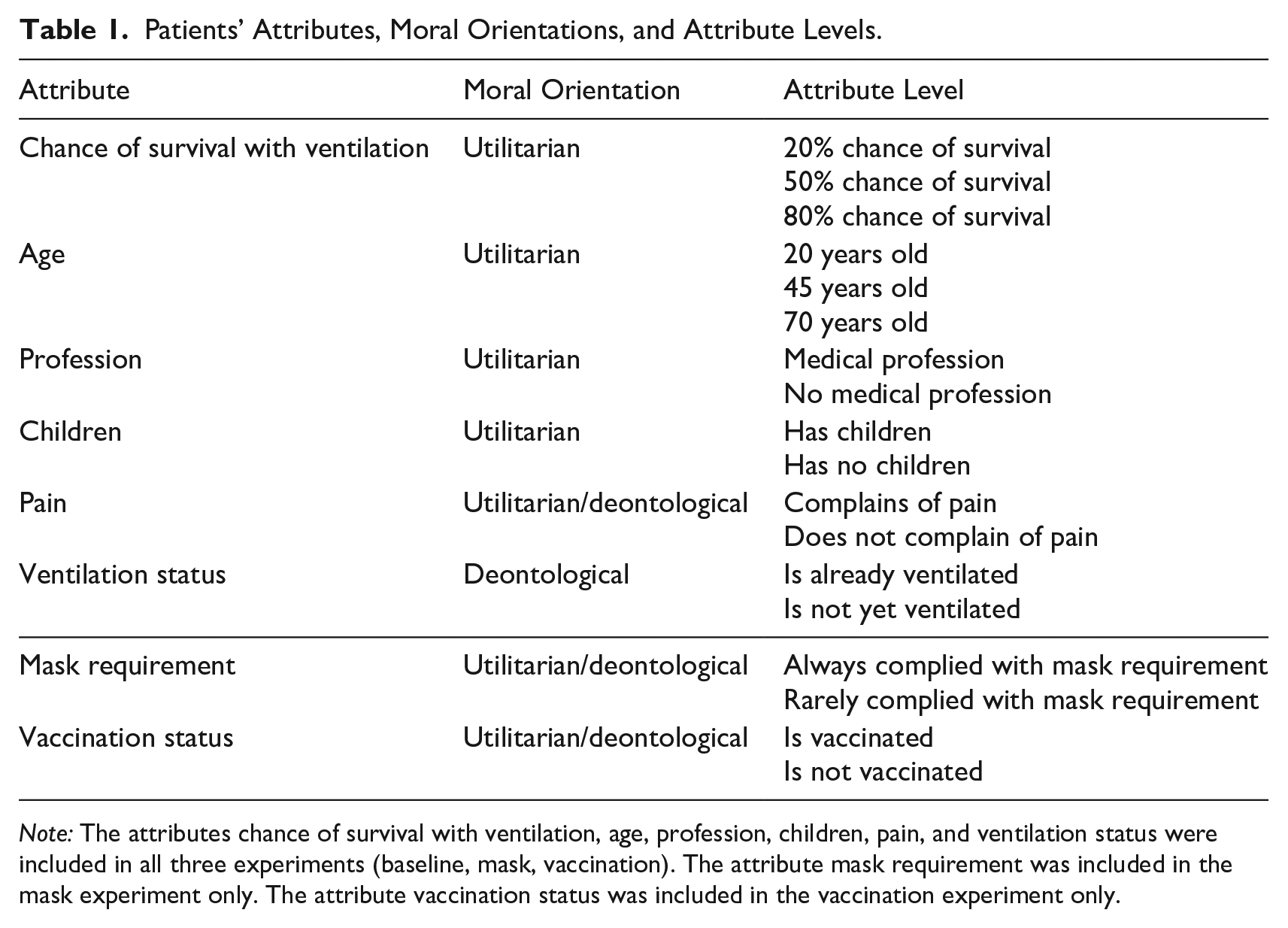
Note: The attributes chance of survival with ventilation, age, profession, children, pain, and ventilation status were included in all three experiments (baseline, mask, vaccination). The attribute mask requirement was included in the mask experiment only. The attribute vaccination status was included in the vaccination experiment only.
Many experts prioritize attributes that are salient from a utilitarian point of view. These encompass the patient’s short-term chance of survival if ventilated and age as an indicator of patient’s long-term life expectancy. 1 Additional utilitarian attributes refer to side effects of triage decisions that go beyond the welfare of the individual patient. Accordingly, patients who work in a medical profession and patients who are responsible for children should receive prioritized treatments. Both utilitarianism, with its focus on promoting experiential welfare, and deontological principles, such as “sickest first” (Emanuel et al. 2020:2052), support the idea of prioritizing patients who complain about pain. A more controversial issue in the debate among experts is the question of whether it is ethically justifiable to abandon the ongoing medical treatment of one patient in favor of the treatment of another patient. Although this is uncritical from a utilitarian point of view, a deontologist might object to this practice on the basis of the idea of the incommensurability of human lives (Brown et al. 2020).
These key attributes derived from the ethical discourse among experts are included in all three of our experimental studies (see Table 1). Furthermore, in two of the experiments, we included one additional attribute, respectively, which plays a minor or no role among experts but is interesting from a sociological point of view. During the COVID-19 crisis, new norms of prosocial behavior have emerged, such as the norm to wear face masks in the public and official recommendations to get vaccinated to protect others and oneself (Betsch et al. 2020; Diekmann 2020; Eichenberger et al. 2020; Korn et al. 2020; Krumpal 2020). Because withholding ventilation can be considered some kind of sanction, sociological and economic literature regarding punishment of norm violations (Oliver 1980; Opp 1979; Rauhut and Krumpal 2008; Simpson and Willer 2015) suggests that our respondents might condition triage decisions on patients’ adherence to the norm of wearing face masks or the norm of getting vaccinated. Note that the sanctioning of norm violations can be motivated by both utilitarian and deontological considerations. From a utilitarian point of view, sanctions are justified insofar as they contribute toward the stability of social norms that are beneficial to society. In deontological terms, sanctions are justified because norm violators breach their moral duties.
Applying Greene’s (2013) Dual-Process Model of Moral Judgment
In theorizing on ethical judgments in triage decisions, we rely on the dual-process perspective in interdisciplinary action theory. According to this approach, which has more or less independent roots in cognitive and social psychology (Evans and Stanovich 2013; Kahneman 2011), pragmatism (Dewey 1933), sociological action theories (Esser 1996, 2001; Esser and Kroneberg 2020; Kroneberg 2005, 2011; Lindenberg 2008), phenomenological sociology (Schütz 1972), theories of praxis (Bourdieu 1990; Giddens 1984; Schütz 1972), and theories of bounded rationality (Rubinstein 1998, 2013; Tutić 2020a, 2020b), human reasoning and behavior can best be understood against the background of two types of cognitive processes with qualitatively distinct characteristics. Type 1 processes typically are automatic, unconscious, associative, fast, and effortless, whereas Type 2 processes constitute the controlled, conscious, analytical, slow, and effortful part of thought. Besides lab experiments that implement decision-making under time pressure or cognitive overload (De Neys 2006; Rand et al. 2014; Rand, Greene, and Nowak 2012), evidence for two qualitatively distinct types of cognitive processes also stems from neuroscience (e.g., McClure et al. 2004). In sociology, the dual-process perspective has proven to be a fruitful action-theoretic account in theorizing on the mechanisms by which diverse forms of cultural orientations, such as internalized norms, values, and attitudes, influence overt behavior (Brett and Miles 2021; Cerulo 2010; DiMaggio 1997, 2002; Knorr-Cetina 2014; Kroneberg, Heintze, and Mehlkop 2010; Lizardo et al. 2016; Martin and Desmond 2010; Miles 2015; Moore 2017; Srivastava and Banaji 2011; Vaisey 2009, 2014; Vila-Henninger 2015).
With respect to moral judgment, the dominant dual-process model stems from Greene et al. (2001). Accordingly, two different processes contribute to moral decision-making, one slow, analytical, and capable of eliciting utilitarian judgments and the other fast and automatic, evoking deontological judgments (Greene 2007, 2013; Greene et al. 2001). Some situations engage emotional affect to a bigger extent than others. A deontological judgment is encouraged when the emotional response is strong enough and there is no motivation, time, or opportunity for cognitive deliberation. In contrast, when the given situation involves few emotional affect and the person has sufficient time and motivation to evaluate the costs and benefits of the harmful action, a utilitarian moral judgment is more likely. Empirical experiments confirm that emotional and cognitive manipulations alter the patterns of utilitarian and deontological judgment and therefore the way people respond to moral dilemmas. Participants suffering from damage to emotional brain regions make fewer deontological decisions (Ciaramelli et al. 2007; Koenigs et al. 2007; Mendez, Anderson, and Shapira 2005). Cognitive load manipulation (Conway and Gawronski 2013; Greene et al. 2008) and introducing time pressure (Suter and Hertwig 2011) selectively interfere with utilitarian decision but not with nonutilitarian moral judgment. Furthermore, a greater working memory capacity is linked to more utilitarian decisions (Moore, Clark, and Kane 2008).
Besides hypothetical triage decisions, we confront the respondents with 10 moral dilemmas adapted from the psychological literature (Conway et al. 2018; Conway and Gawronski 2013) and employ the psychometric technique of process dissociation (Jacoby 1991; Kelley and Jacoby 2000; Payne and Bishara 2009; Yonelinas 2002) to measure respondents’ inclinations toward utilitarianism and deontology (see A4 in the Appendix in the online version of the article). Greene’s (2013) dual-process model on moral judgment suggests interaction effects between respondents’ moral inclinations and patients’ attributes that are salient from an utilitarian or deontological point of view. More specifically, we put the following pair of hypotheses to the test:
Hypothesis 1a: Utilitarian attributes have a stronger effect on triage decisions for respondents with a higher inclination toward utilitarianism than for respondents with a lower inclination toward utilitarianism.
Hypothesis 1b: Deontological attributes have a stronger effect on triage decisions for respondents with a higher inclination toward deontological principles than for respondents with a lower inclination toward deontological principles.
Our testing of these two hypotheses focuses on those attributes that are nonambiguously and strongly salient from either a utilitarian or a deontological perspective. We do so because it is theoretically perfectly reasonable that a pure utilitarian only takes the two most important utilitarian attributes (i.e., short-term survival chance and long-term life expectancy) into consideration and simply ignores all other attributes. Note also that our study is much more informative with respect to Hypothesis 1a than to Hypothesis 1b because in view of the ethical discussion among experts, it can be expected that the two most important utilitarian attributes have much more impact on triage decisions than the ventilation status of patients (see Emanuel et al. 2020).
In addition, we put the central tenet of Greene’s (2013) dual-process model of moral judgment to the test. According to Greene et al. (2001), utilitarian judgment is more likely to follow from a reflective Type 2 process. In our study, we measure the tendency of our respondents to engage in cognitive reflection via the Cognitive Reflection Test (see Frederick 2005; Kahneman and Frederick 2002). We hypothesize an interaction effect between this tendency toward reflection and attributes that are salient from a utilitarian perspective:
Hypothesis 2: Utilitarian attributes have a stronger effect on triage decisions for respondents with a higher tendency toward cognitive reflection than for respondents with a lower tendency toward cognitive reflection.
Again, in testing this hypothesis, we focus on the most important utilitarian attributes for the same reason already explained. Note also that we do not hypothesize that more reflective respondents put less weight on deontological attributes than more intuitive respondents in making triage decisions. Greene’s (2013) dual-process model of moral reasoning does not rule out that deontological considerations can play a role or even dominate a moral judgment that comes about in a Type 2 process; otherwise, the huge and sophisticated philosophical literature on deontological ethics would constitute an empirical anomaly of the model (Greene 2007). However, Greene’s (2013) dual-process model does claim that moral judgment can be driven by intuition or by reflection and that the cost-benefit analysis required for utilitarian judgment is a hallmark of reflective Type 2 processes.
Data and Method
Study Sample
Our study was an experimental online survey implemented via respondi, a German online access panel provider where people can voluntarily register to participate in opinion polls. 2 Invitations to participate were sent to 13,591 persons randomly selected from the access panel. In all, 3,465 subjects responded to the invitation link, providing an overall response rate of 25.5%. The entire questionnaire was completed by 2,646 study subjects (for a more detailed description of the sample, see A2 in the Appendix in the online version of the article). The interviews were conducted in German. Data collection was conducted in February 2021 using SoSci Survey (https://www.soscisurvey.de).
Triage Vignette and Conjoint Design
Three different choice experiments were implemented. In the baseline experiment, 881 respondents participated; in the mask experiment, we had 880 respondents; and in the vaccination experiment, there were 885 respondents. Each respondent was confronted with 10 hypothetical triage decisions where the respondent had to choose which of two patients should receive ventilation (paired conjoint design with forced choice; for exemplary choice sets and further details on all measures used, see A3 in the Appendix in the online version of the article). By experimental design, all variables that refer to attributes of patients are uniformly distributed and statistically independent. Post-hoc checks confirmed both properties. Table 1 provides an overview of all attributes and attribute levels. In some decisions, missing values occurred (baseline experiment = 46, mask experiment = 33, vaccination experiment = 30). Note that we did not use listwise deletion (i.e., our analysis is based on all decisions in which no missing values are observed). 3
Respondents’ Characteristics
In line with our theoretical arguments, we made use of only three variables describing characteristics of our respondents. These were the respondents’ inclinations toward utilitarianism (U) and deontology (D) and the respondents’ tendency to engage in reflective Type 2 processing.
By design, U varies between –1.0 and 1.0 (see A4 in the Appendix in the online version of the article). Because we used five pairs of moral dilemmas to measure moral inclinations, U took on only multiples of .2. Empirically, over all three studies, U took values between –.6 and 1.0 and was approximately normally distributed (M = .438, SD = .278, 11 missings). In testing our hypotheses, we used the indicator “high U,” which took a value of 1 if U was at least .8 (M = .180), and the indicator “low U,” which took a value 1 if U was not greater than .2 (M = .302). The cutoff points .8 and .2 were chosen such that these two groups roughly refer to the 25% most extreme respondents in our sample, respectively.
By construction, D varied between 0 and 1. Both extreme values were actually observed in our studies (0 = 21.92%, 1 = 14.99%). In the interior of the unit interval, D was approximately normally distributed (M = .480, SD = .328, 105 missings). 4 Analogously to U, the indicators “high D” (M = .235) and “low D” (M = .266) were derived from D using the cutoff points .72 and .3, respectively.
The Cognitive Reflection Test (CRT) measured a respondent’s tendency to engage in Type 2 processing (Frederick 2005; Kahneman 2011).
5
The instrument consists of three questions that are easy to answer once the respondent actually thinks about them. However, each question suggests an intuitive answer, which is wrong (see A4 in the Appendix in the online version of the aticle). The CRT score simply counted the number of correct answers and varied between 0 and 3 (
Results
Causal Effects of Attributes
Figures 1 through 3 comprise estimates of the causal effects of patients’ attributes on the probability of getting ventilation as observed in our three experimental studies (see also A5 in the Appendix in the online version of the article). To be more specific, the depicted numbers are nonparametric estimates of average marginal component effects (AMCEs; Hainmueller et al. 2014). To help the reader with interpretation, consider the approximately .1 effect of patients with children in the baseline and the mask experiments. This indicates that patients who are in charge of children on average have a 10% higher probability of getting ventilation than patients who have no responsibility for children. The depicted 95% confidence intervals are based on robust standard errors, which take the clustering of choices within respondents into account.
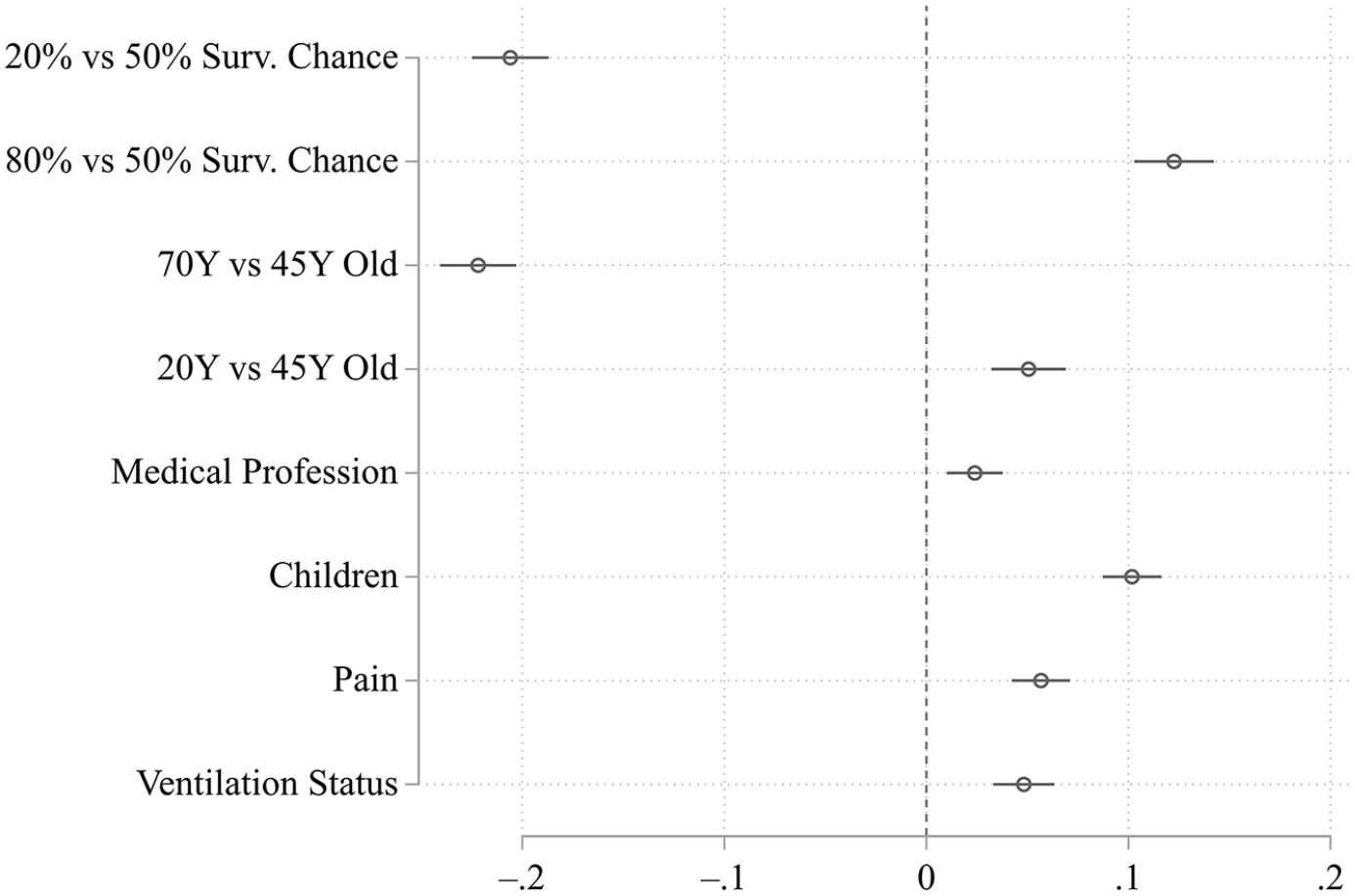
Causal Effects of Patients’ Attributes on the Probability of Getting Ventilation (Baseline Experiment).
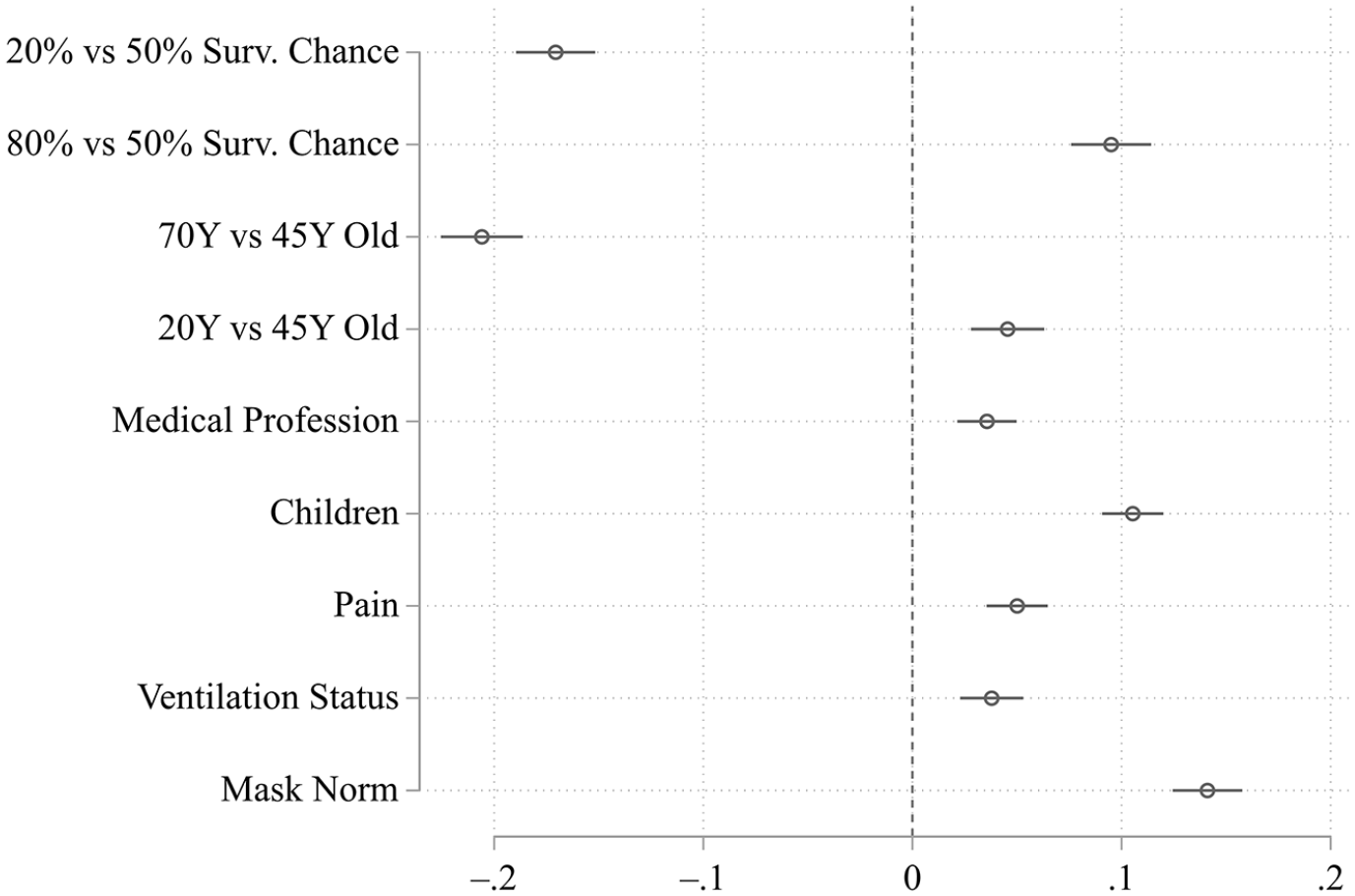
Causal Effects of Patients’ Attributes on the Probability of Getting Ventilation (Mask Experiment).
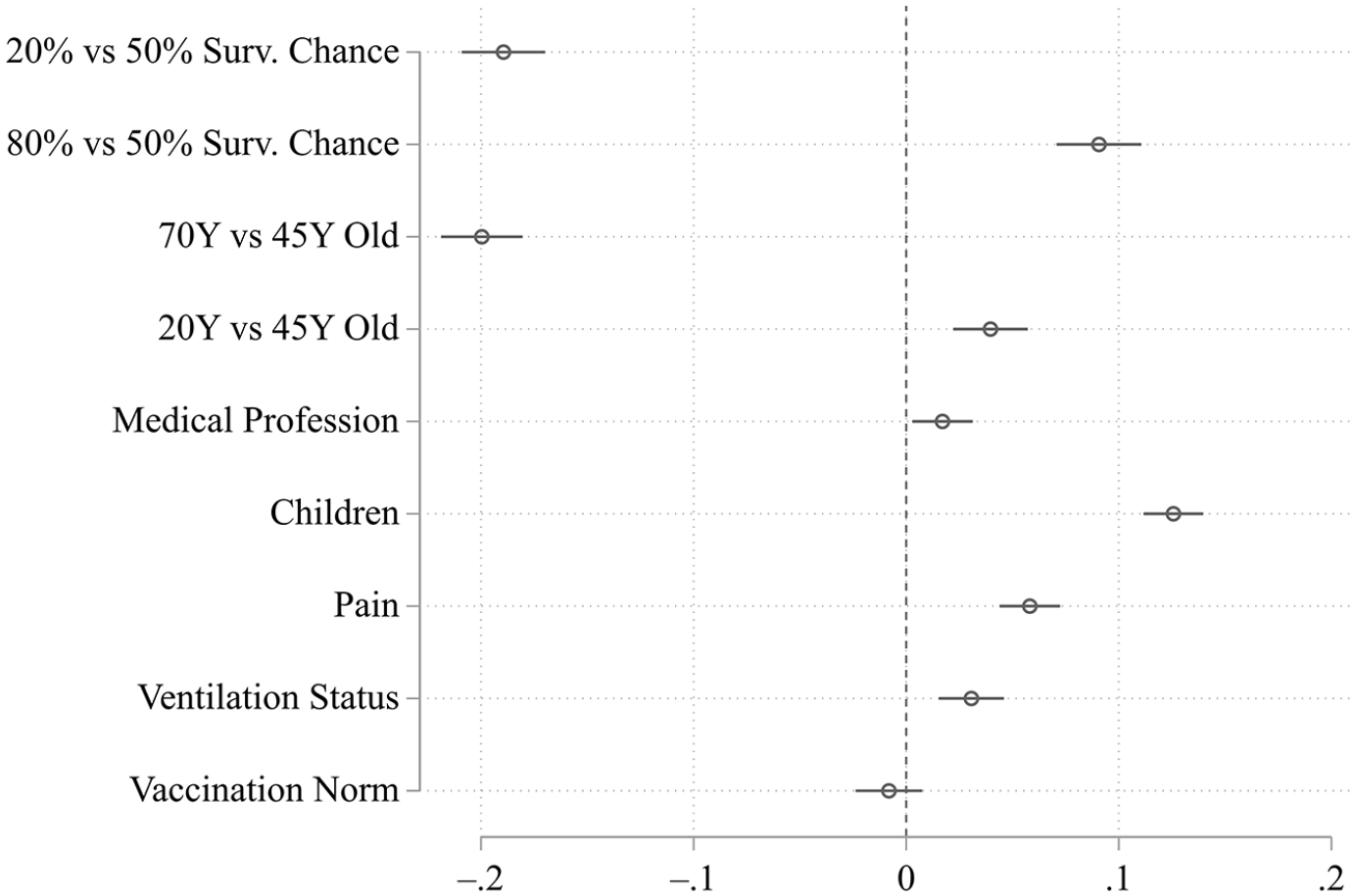
Causal Effects of Patients’ Attributes on the Probability of Getting Ventilation (Vaccination Experiment).
The first thing to note in looking at Figures 1 through 3 is that estimates are surprisingly robust across all three experiments. The inclusion of an additional attribute in the mask and the vaccination experiments does not affect the estimates of the causal effects of the attributes in the baseline treatment. Against this background, we can summarize our findings without conditioning our exposition on the underlying experiment.
We find strong causal effects for most of the attributes that we classified as salient from a utilitarian point of view. Both short-term chances of survival and long-term life expectancy of the patient (measured by age) show strong effects. Patients that have an 80% chance of survival if ventilated on average have a 28.0% to 32.9% (range of differences across the three experiments) higher probability of getting ventilation than patients with a 20% survival chance. 70-year-old patients have a 24.0% to 27.3% lower probability of getting ventilation than 20-year-old patients. To a considerably lesser degree, it also matters whether patients are responsible for children (10.2% to 12.5%). Although significantly different from zero, the effect of having a medical profession is in comparison quite small and perhaps negligible (1.7% to 3.6%).
In the theory section, we classified only one attribute of patients, ventilation status, as purely salient from a deontological point of view. Empirically, it matters only slightly whether the patient is already receiving ventilation (3.1% to 4.8%).
With respect to the remaining attributes, which are hard to classify as either salient from a utilitarian or a deontological point of view, a nuanced picture emerges. Across the three experiments, patients articulating the experience of pain have a 5.0% to 5.8% higher probability of getting ventilation than patients who do not articulate pain. Interestingly, the two attributes that refer to patients’ adherence to social norms in the pandemic differ considerably in their causal effects. Although it makes a sizeable difference for our respondents whether the patients obey the norm of wearing face masks (14.1%), they consider obedience to the norm of getting vaccinated totally irrelevant. We discuss this finding in the final section.
Moral Inclinations and Cognitive Reflection
In this subsection, we explore the bivariate relationships between moral inclinations and the tendency toward Type 2 processing. To simplify our exposition, we pool our data across all three experiments. To be clear, the correlational analyses in this subsection are located on the level of respondents, not on the level of decisions.
The left panel of Figure 4 depicts a scatter plot between U and D and the predicted values of D on the basis of a bivariate regression. Apparently, respondents with a stronger inclination toward utilitarianism are somewhat less inclined by deontological principles. Although the negative correlation is rather weak by conventional standards, it is statistically significant (correlation = –.165, p < .000). This finding is kind of surprising against the background of the studies by Conway and Gawronski (2013) and Conway et al. (2018), who typically find smaller and statistically insignificant correlations between U and D. Still, our findings back the fundamental idea that utilitarianism and deontological principles should not be thought of as opposing poles on a continuum.
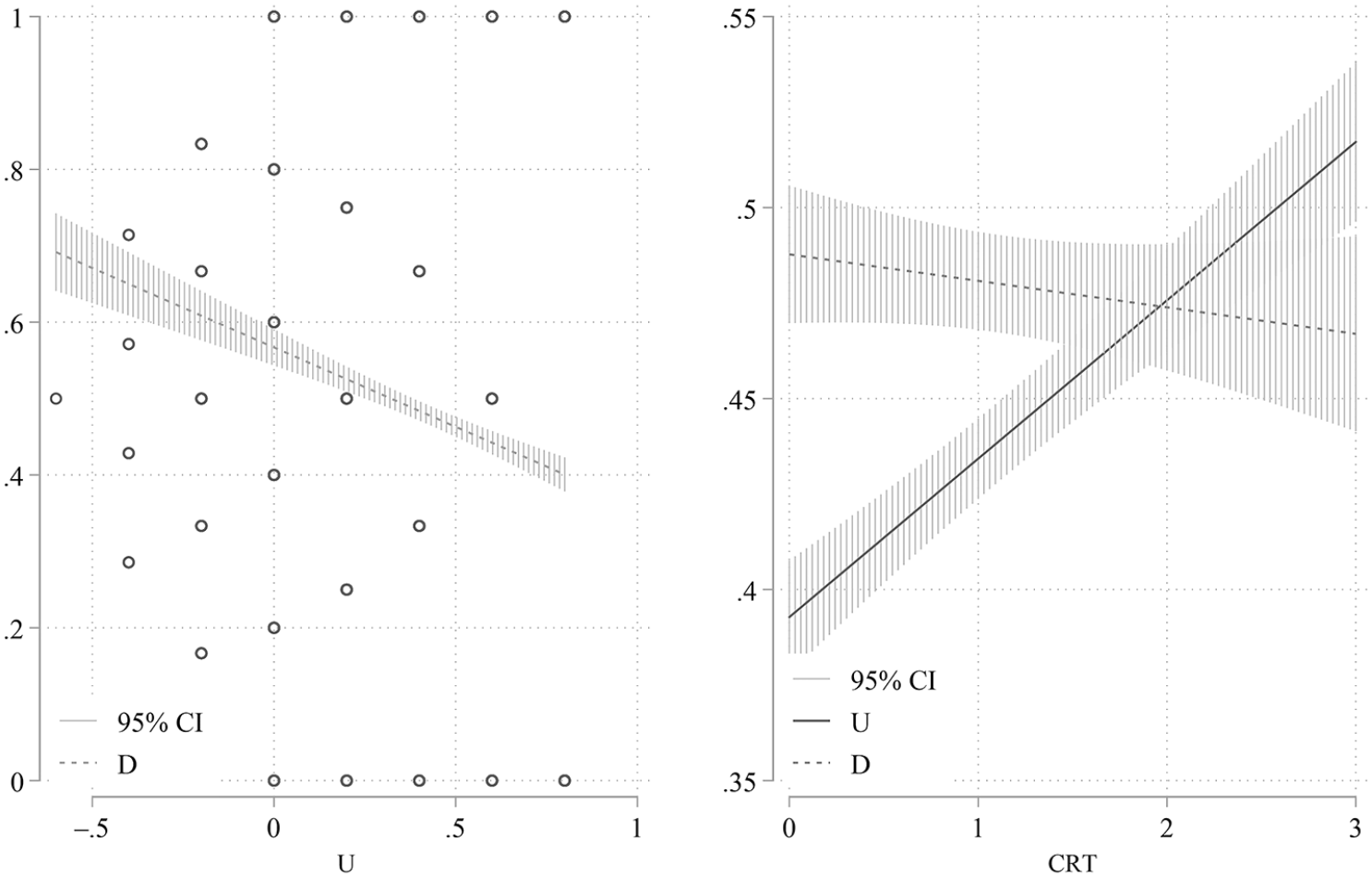
Bivariate Regressions between Respondents’ Moral Inclinations, U and D (Left Graph Showing Predicted Values of D), and between Cognitive Reflection Tendencies (CRT) and U or D (Right Graph Showing Predicted Values of U or D) (Pooled across All Experiments).
The right panel of Figure 4 shows how the respondents’ tendency toward reflection as measured by the CRT score correlates with each of the two moral inclinations under consideration (bivariate regressions of U and D on CRT, respectively). We find that more reflective respondents tend a bit more toward utilitarianism (correlation = .164, p < .000), whereas the CRT score and D do not correlate at all (correlation = –.021, p < .242). This finding is in line with Greene’s (2013) dual-process model of moral judgment according to which utilitarianism is more appealing for more reflective actors. The result also replicates findings by Conway and Gawronski (2013) on correlations between U and D and an alternative measure for the tendency toward cognitive reflection (i.e., Need for Cognition scale).
Testing the Hypotheses
Now, we turn to the examination of our two hypotheses. Recall, the first hypothesis posits an interaction effect between respondents’ underlying ethical orientations and the corresponding attributes of patients. The second hypothesis claims a different type of interaction effect according to which respondents who tend more toward reflection are more sensitive to utilitarian attributes than respondents who tend more toward intuition.
Before presenting our hypotheses tests, two preliminary remarks are in order. First, the previous analyses demonstrate that our estimates of causal effects are very robust across the three experimental studies. This justifies pooling the data when testing the hypotheses, which simplifies our exposition considerably. Second, we restrict our attention to those attributes that we identified in the theory section as nonambiguously and most strongly salient from either a utilitarian or a deontological point of view. As indicated, in the ethical debate among experts, short-term survival chance and long-term life expectancy (measured by age in our experiments) are regarded as the most important attributes from a utilitarian perspective. Notably, our previously discussed findings indicate that our respondents consider these two utilitarian attributes as most relevant as well. Because our study contains only a single attribute, which is purely salient from a deontological point of view, we have no alternative to using ventilation status for a test of Hypothesis 1b, although its empirical effect on triage decisions is rather small.
Figure 5 presents our main findings regarding Hypotheses 1a and 2. This figure displays causal effects of attributes estimated on the basis of the pooled data set but estimated separately for subgroups of respondents using indicator variables that identify respondents as either having strong or weak inclinations toward utilitarianism and having either high or low CRT scores, respectively.
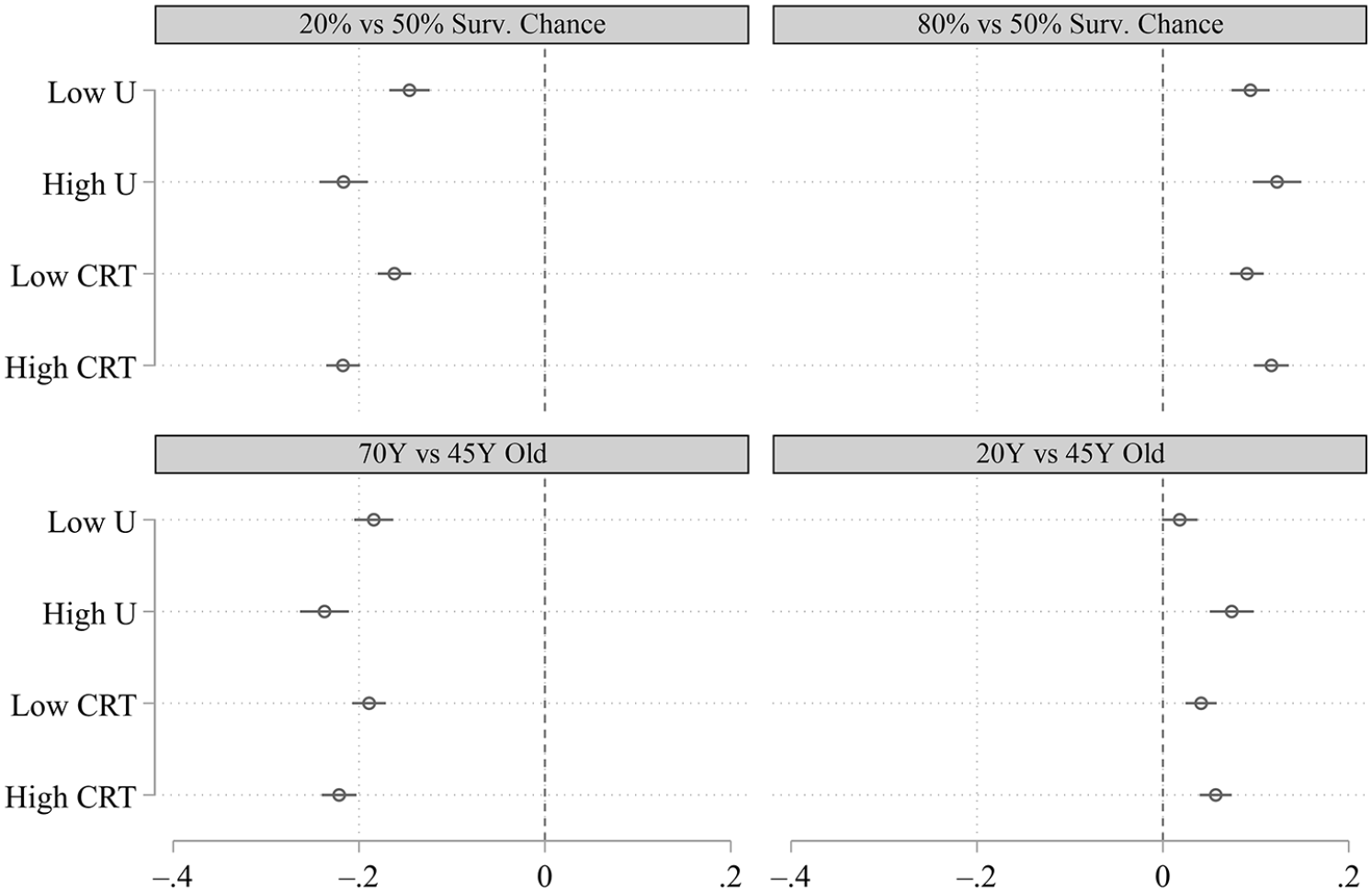
Subgroup Specific (Low U Versus High U; Low CRT Versus High CRT) Causal Effects of the Utilitarian Attributes Survival Chance and Age on the Probability of Getting Ventilation (Pooled across All Experiments).
The results displayed in Figure 5 support Hypotheses 1a and 2. First, we observe that respondents with a greater inclination toward utilitarianism do indeed place greater weight on the utilitarian attributes than respondents with a smaller inclination toward utilitarianism. Although the differences in effect sizes are rather low across subgroups (low U vs. high U), three of them are significant at the 5% level, and one is significant at the 10% level (20% vs. 50% survival chance: χ2 = 16.98, p < .00; 80% vs. 50% survival chance: χ2 = 2.86, p < .091; 70 years old vs. 45 years old: χ2 = 9.55, p < .002; 20 years old vs. 45 years old: χ2 = 13.09, p < .003). 6
Second, regarding the interaction between respondents’ tendency toward cognitive reflection and utilitarian attributes, our results show that more reflective respondents do place greater weight on the short-term chances of survival and the long-term life expectancy of patients than respondents that tend toward intuitive judgment. With the exception of 20 years old versus 45 years old, all observed differences in effect strengths are significant across subgroups (low CRT vs. high CRT) at the 5% level (20% vs. 50% survival chance: χ2 = 18.05, p < .00; 80% vs. 50% survival chance: χ2 = 3.99, p < .046; 70 years old vs. 45 years old: χ2 = 5.93, p < .015; 20 years old vs. 45 years old: χ2 = 1.65, p < .199).
Turning to the test of Hypothesis 1b with respect to the single nonambiguously deontological attribute, we find that the inclination toward deontological principles among respondents matters a little bit with respect to the weight that the respondents place on the ventilation status of patients. That is, among respondents with a high inclination toward deontological principles, the estimated causal effect of ventilation status equals 4.6%, whereas among respondents with a low inclination toward deontological principles, the causal effect amounts to 2.9%. This small difference in effect sizes across subgroups (high D vs. low D) is not statistically significant (χ2 = 1.71, p < .191).
Taking all of the findings in this subsection into account, we draw the conclusion that Hypotheses 1a and 2 get validated by our data, whereas Hypothesis 1b is rejected. As expected, both the inclination toward utilitarianism (Hypothesis 1a) and the tendency toward cognitive reflection (Hypthesis 2) amplify the causal effects of attributes that are most salient from a utilitarian perspective in triage decisions. Although we do find that respondents who are more inclined by deontological principles place a little more weight on the single nonambiguously deontological attribute than respondents who are less inclined by deontological principles, the observed difference in causal effects lacks statistical significance (Hypothesis 1b). In interpreting the latter finding, it has to be kept in mind that Hypothesis 1b met considerably harsher conditions than its counterpart, Hypothesis 1a, because the single nonambiguously deontological attribute is among those attributes with the lowest overall effect on triage decisions observed in our study, whereas the utilitarian attributes are the strongest predictors. 7
Section A5 in the Appendix in the online version of the article provides all estimates of causal effects of the attributes included in the baseline experiment for all subgroups under consideration, based on the pooled data from all three experiments. Although not all differences between subgroups reach statistical significance, in descriptive terms, all but two differences are in line with our hypotheses and Greene’s (2013) underlying dual-process model of moral judgment. 8
Discussion
In this article, we present results from choice experiments on triage decisions in the context of a pandemic crisis. Respondents are confronted with a hypothetical triage scenario in which they have to choose who out of two patients gets ventilation. Patients are characterized by a set of attributes such as short-term survival chance, long-term life expectancy, and their current ventilation status. These attributes are selected based on a review of the ongoing ethical discussion among experts in regard to the COVID-19 pandemic (De Castro-Hamoy and De Castro 2020; Emanuel et al. 2020) and can be classified according to their salience from a utilitarian or a deontological point of view.
By and large, we find that the hypothetical triage decisions of our nonexpert respondents agree with the official triage guidelines developed by experts on prioritizing utilitarian attributes. That is, the two most important utilitarian attributes (i.e., short-term survival chance and long-term life expectancy [measured by age]) have the greatest influence on hypothetical triage decisions among all attributes under consideration. By contrast, the only purely deontological attribute, which refers to the patient’s ventilation status, carries only little weight among our respondents. Interestingly, our respondents also attach some importance to attributes that should be irrelevant from the experts’ point of view. In particular, we observe that our respondents assign ventilation to patients who do not adhere to the norm of wearing face masks with a probability that is on average 14.1% lower than the probability of patients who adhere to this norm. Although this effect of patients’ compliance with newly emerged norms in the triage situation is sociologically interesting, it does not per se undermine the overall impression that our respondents are rather oriented toward utilitarianism than deontology in making triage decisions given that sanctioning behavior can be explained against the background of both orientations. Note that these results should not necessarily be interpreted as suggesting that our respondents are generally more inclined by utilitarianism than deontology. Triage decisions are extreme choice situations, in which high stakes are at line, and not representative for the everyday conduct of our nonexpert respondents. Presumably, the unfamiliarity with these triage decisions contributed toward a reflective and calculating approach among our subjects that favors a utilitarian style of decision-making.
We find support for both hypotheses and hence for Greene’s (2013) underlying dual-process model of moral judgment. As predicted, respondents who are more strongly inclined toward utilitarianism show a significantly stronger reaction to variations in the two most important utilitarian attributes (i.e., short-term survival chance and long-term life expectancy). Although respondents who are more strongly inclined toward deontology do not show a significantly stronger reaction to variations of the single, nonambiguously deontological attribute, this finding needs to be put in perspective in evaluating Greene’s (2013) dual-process model because this attribute has a comparatively low overall effect on triage decisions that limits the potential to find significant differences between subgroups. Finally, we also find that more reflective respondents are consistently more sensitive to utilitarian attributes than respondents who tend toward intuitive decision-making.
Our article contributes to the sociological discourse on the dual-process perspective by strengthening two arguments according to which the established sociological dual-process model (Vaisey 2009) can be interpreted as neglecting important advances in the psychological literature (Brett and Miles 2021; Leschziner and Brett 2019; Luft 2020). First, Vaisey’s (2009) model draws heavily from Haidt’s (2001) theory of moral judgment, according to which the great bulk of moral judgment comes about in a Type 1 process on the basis of automatically activated moral emotions. In Haidt’s (2001) social intuitionist model, reflective Type 2 moral reasoning does only occasionally cause moral judgments and primarily serves to rationalize emotionally grounded moral judgments post hoc. Vaisey (2009) adopts this idea and argues that nondeclarative forms of cultural orientations, which are automatically processed, exert a greater impact on behavior than declarative cultural orientations, which are subject to reflective Type 2 processing (see also Miles 2015). In contrast to Haidt (2001), Greene (2007, 2013) argues that moral judgment can be the outcome of both moral intuitions and moral reasoning (i.e., the outcome of intuitive Type 1 and reflective Type 2 processes; see Luft 2020). Our results are well in line with Greene’s (2013) model in demonstrating that the moral judgments of nonexperts are influenced by both intuitive deontological and reflective utilitarian orientations. This finding strengthens calls for attention to dual-process models that allow one to theorize on the influence of cultural orientations via both Type 1 and Type 2 processes (Leschziner and Brett 2019; Luft 2020).
The second aspect in which our study contributes toward the ongoing discourse on the dual-process perspective among sociologists lies in demonstrating empirically that individual differences in thinking dispositions and cognitive styles are indeed key in empirical applications. Recent advances in the psychological dual-process literature do not stop at positing a duality of types of cognitive processes but examine the interplay of Type 1 and Type 2 processes in shaping overt behavior. The crucial question is under which conditions behavior comes about via either a Type 1 or a Type 2 process. In this regard, the dominant position is called default interventionism (Evans and Stanovich 2013). Accordingly, Type 1 processes generate intuitive responses that have to be endorsed by Type 2 processes before a behavioral output is generated. The level of engagement in Type 2 processing depends on a number of factors, which can be grouped in motivational factors and cognitive resources (Evans 2018). Thinking dispositions and cognitive styles as measured by the Cognitive Reflection Test (Frederick 2005; Kahneman and Frederick 2002), the Need for Cognition scale (Cacioppo and Petty 1982), or the Rational-Experential Inventory (Brett and Miles 2021; Epstein et al. 1996) serve as particularly important metacognitive, dispositional factors influencing the occurrence of Type 1 or Type 2 processes. Our finding that more reflective respondents have a greater tendency toward utilitarian judgment than intuitive respondents supports this idea and strengthens calls for a greater attendance among sociological proponents of the dual-process perspective to dispositional factors regarding the occurrence of Type 1 and Type 2 processes in applications. This is important given that the dominant version of sociological dual-process theory (Vaisey 2009) has been criticized to neglect the complex interplay of Type 1 and Type 2 processes in generating overt behavior by assuming that certain types of behavioral tasks and choice situations are tied to either Type 1 or Type 2 processes (Brett and Miles 2021; Leschziner and Brett 2019), thereby making it difficult to explain the emergence of creative forms of behaviors (Leschziner and Brett 2019) and being blind to the fact that thinking dispositions, and hence the prevalence of Type 1 and Type 2 processes, are socially patterned (Brett and Miles 2021).
A finding we want to highlight and discuss is the fact that the norm of vaccination has absolutely no impact on triage decisions in our study. Taken on face value, this is a strong finding suggesting that our nonexpert respondents are strictly against the idea of hinging triage decisions on the vaccination status of patients, which has been part of the public debate on the COVID-19 crisis in Germany (Vehlewald 2020). For example, behavioral economist Armin Falk has argued in favor of vaccination status as a criterion for triage decisions (Pennekamp 2021). The results of our study clearly point in a different direction. Because our nonexpert respondents agree with the international consensus among experts that prioritizing patients in triage situations should not be based on their past (prosocial) behavior (Gelinsky 2020:10), the policy implication can be derived that this should continue to be the case. However, why do the respondents react so differently to a violation of the norm of wearing face masks and the norm of getting vaccinated? A possible explanation for this finding is that in the instructions of our vaccination experiment, the respondents were told that they should imagine a situation in which vaccination is accessible for everyone and provides protection for both the person who is vaccinated and his or her contacts (see A3 in the Appendix in the online version of the article). At the time the study was conducted (February 2021), this scenario was very much hypothetical against the background of the COVID-19 situation in Germany. In particular, during this time, vaccines were in fact very rare in Germany, and many people wishing to be vaccinated had actually no opportunity to do so. It is entirely in the realm of possibility that our finding regarding the zero effect of the vaccination norm on triage decisions is due to a conflation of the real-life situation and the hypothetical scenario by our respondents; if vaccines are rare, there can be no moral obligation to get vaccinated. This argument can also explain why the respondents reacted so differently to a violation of the norm of wearing face masks and the norm of getting vaccinated. It would be very instructive to simply repeat the vaccination experiment now or in the near future when vaccines are or will actually be widely and easily available to bring some clarity to this ambiguous finding of the current study.
Naturally, there are other interesting directions for future research. For instance, in the present study, we focus on triage decisions regarding the ventilation of patients. However, recently there have been reports in the media according to which triage is currently practiced in the domain of psychological therapy, in particular with respect to children and adolescents (Bogner 2021). Future research is invited to adapt our experimental design to these new scenarios and conduct similar studies to learn about the moral judgment in this context. More generally, we feel that combining conjoint analysis, with its merits from a causal–analytical point of view, and the dual-process perspective in studying moral judgment is a stimulating research agenda that can be fruitfully applied to many other domains of social life.
Supplemental Material
sj-docx-1-hsb-10.1177_00221465221080958 – Supplemental material for Triage in Times of COVID-19: A Moral Dilemma
Supplemental material, sj-docx-1-hsb-10.1177_00221465221080958 for Triage in Times of COVID-19: A Moral Dilemma by Andreas Tutić, Ivar Krumpal and Friederike Haiser in Journal of Health and Social Behavior
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge funding support from the Dr. Hans Riegel-Stiftung through the grant “Ad hoc-Sonderförderung von wirtschafts- und sozialwissenschaftlicher Forschung zu Themen der Covid-19-Pandemie.” Any opinions, findings, and conclusions or recommendations expressed in this paper are those of the authors and do not necessarily reflect the views of the funder.
Supplemental Material
The Appendix is available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.