
Abstract
The idea that socioeconomic differences are a “fundamental cause” of health and well-being is the basis for large volumes of research. However, one of the challenges in this area is that of linking socioeconomic positions to etiological mechanisms in theoretically informative ways. The situation is doubly challenging because the expression and meaning of socioeconomic positions and the mechanisms they activate change over time. Focusing on depression and applying mediation analysis to data from a large multinational sample from European countries, we find strong support for a three-stage model where occupational differences are largely mediated by exposure to precarious work, which itself is mediated by social marginality. The model is largely robust across welfare state regimes. Ultimately, the research extends fundamental cause perspectives by highlighting connections between “old” and “new” dimensions of socioeconomic status and the social and social psychological sequelae that connect them to psychological well-being.
Fundamental cause theory (FCT) emphasizes the primacy of socioeconomic differences in the etiology of health and well-being (Link and Phelan 1995; Pampel, Krueger, and Denney 2010). Its key insight concerns the totalizing character of socioeconomic status: Socioeconomic status affects health in all times and places because people draw on their income, education, and employment in myriad ways to avoid disease and extend longevity. This is apparent in the ubiquity of socioeconomic inequalities in health across all societies that reflect differing exposures to health risks and differences in strategies to neutralize risks when experienced. Although FCT posits that this generic pattern is universally observed for preventable or treatable conditions, the specificities of socioeconomic status, health risks, risk management strategies, and common morbidities vary by time and place. The key challenge of FCT, then, is to add specificity to this generalized account within and between societies.
With a focus on occupational position and psychological well-being, this article extends FCT perspectives in four ways. First, it articulates multifaceted precarious work 1 as a proximal risk factor of lower socioeconomic status. Precarity in work is one of the major transformations of twenty-first-century labor relations and is increasingly viewed as a combination of characteristic of employment, conditions of work, and adequacy of compensation and benefits (Julià et al. 2017; Lewchuk et al. 2003; Tompa et al. 2007; Vives et al. 2010). Surprisingly little work has empirically examined connections between occupational position and precarious work, and differential exposure to precarity may be an important link between socioeconomic status and inequalities in health and well-being.
A second contribution is to expand conceptualization of the social dynamics that link precarious work to mental health and by extension, help explain socioeconomic gradients in psychological well-being. Although prior studies have proposed a number of mechanisms linking precarious work to health (for a general discussion, see Benach et al. 2014), we focus on a unique vector-heightened social marginality (external to the workplace). Importantly, the latter is implicated in inequalities in health and well-being (Berkman et al. 2000) yet largely unexplored as a mechanism linking socioeconomic status, precarity in work, and psychological well-being.
Third, we situate such processes within broad political and economic contexts that are argued to both moderate exposure to precarity in work and provide a range of extramarket supports. Although early work in this area focused on the welfare state framework of Esping-Andersen (1990; e.g., Kim et al. 2012), ideas around “varieties of capitalism” (Hall and Soskice 2001) and employment regimes and their relation to quality of work (Gallie 2009a, 2009b) are also important considerations. In developing these ideas, we provide a deeper understanding of the political economic backdrop to precarious work and its consequences and hence sharpen understanding of its implications for psychological well-being.
Finally, we test this model using a structural equation framework and data from a large multinational sample of European countries that is one of the largest labor markets in the world. Collectively, the research provides a unique theory-expanding test of the fundamental cause perspective by linking the micro, meso, and macro dimensions of socioeconomic status with precarious work and its consequences.
Background
Occupational Position, Precarity, and Mental Health
Considerable attention has been paid to associations between socioeconomic status and mental health, with important research in sociology (Kessler and Neighbors 1986; Link, Lennon, and Dohrenwend 1993), epidemiology (Marmot et al. 1991; Muntaner et al. 1998; Smith et al. 1998), economics (Case and Deaton 2020; Cutler, Deaton, and Lleras-Muney 2006), and psychology (Argyle 1994; Karasek et al. 1988; Lachman and Weaver 1998). Special attention has focused on occupational position as an omnibus indicator of socioeconomic status because variable locations within market economies, specifically position within the occupational division of labor, is the fundamental generator of social inequalities (Rose and Harrison 2007). FCT echoes this basic idea by emphasizing differential access to power and resources that reflect different positions in occupational orders as a core basis of health inequalities (Link and Phelan 1995).
Although occupations are “social addresses” that locate people in social structures, they do not a priori provide mechanistic accounts of why differences in positions affect the probability of poor health (Muntaner et al. 2004). Indeed, identification of the factors that link occupational positions to health is the key theoretical challenge and often something missing or assumed. We argue that precarity in work is a proximal risk factor of occupational position, literally the expression of socioeconomic status in the form of conditions of work and its consequences, that both influences psychological well-being directly and has important social externalities that collectively account for occupational variation in mental health.
Precarity in Work as a Proximal Consequence of Occupational Position
Early research on precarious work emphasized precarity in employment—employment without formal contracts or conditions and typically of undefined and often short(er) duration—and showed that precarious employment in general was associated with poorer psychological well-being but also that there is considerable heterogeneity in effects depending on operationalization, sample, and model/methodology (see review in Benach et al. 2014). Recent decades have seen conceptualization broaden to incorporate a number of dimensions, including employment, conditions of work, compensation, benefits, protections, and issues of power and representation (see e.g., Julià et al. 2017; Lewchuk et al. 2003; Tompa et al. 2007; Vives et al. 2010). Such work echoes both conceptual work stressing the multifaceted nature of precarious work (see e.g., Standing’s [2011] emphasis on multifaceted “insecurity”) and empirical work showing that nontraditional employment relations open the door for widespread restructuring of employment activities and experiences (see e.g., Kalleberg, Reskin, and Hudson’s [2000] emphasis on the link between limited duration contracts and “bad jobs”). We too adopt a multidimensional conceptualization and focus on five aspects of precarity—non-indefinite contracts, low job control, low organizational influence, employment gaps, and financial vulnerability. Still, we recognize that there are competing conceptualizations (e.g., Schneider and Harknett’s [2019] focus on scheduling precarity), and our approach is simply one among many complementary alternatives (see discussions of conceptual issues in Arnold and Bongiovi 2013; Kalleberg and Vallas 2018; Vives et al. 2010).
Although both its conceptualization and relationship to health are reasonably well developed, how precarious work relates to traditional occupational structures that determine socioeconomic status is less so. Most conceptualizations of occupational differentiation involve attention to authority and control in the workplace (e.g., owners, managers, supervisors, and supervised employees) coupled with the types of activities typically engaged in (e.g., professional service work vs. manual labor). It is the combinations of these categories that typically determine occupational position (Muntaner et al. 2010). For example, the European Socioeconomic Classification (ESeC) emphasizes four basic employment positions: employers, the self-employed, employees, and those involuntarily outside of paid labor (see discussion in Rose and Harrison 2007). Whereas the former two groups are differentiated in terms of scale (e.g., large vs. small employers), employees are differentiated in terms of contract type and the type of work done. Contract type is a response to problems in ensuring that employees perform as required. Monitoring problems occur when the amount and quality of work cannot be monitored directly (e.g., profession or higher managerial work vs. manufacturing). Asset specificity problems involve issues in dealing with high skills or specialized knowledge that is either uniquely valuable and not easily substitutable within the firm or quite marketable outside the firm. Work situations with low monitoring problems and low asset specificity are typically characterized by a “labor contract” where compensation is based on piece or time. By contrast, work situations with high monitoring problems and high asset specificity typically employ a “service relationship” that is more long term, where compensation and benefits are greater and more stable, and where employment is embedded within a clear(er) system of promotion and opportunity.
The ESeC classification, like most others, does not a priori capture the multiple aspects of precarious work, but it does anticipate variation in the risk of precarity associated with occupational position. In general, precarity should increase in a relatively linear way as one moves down the occupational ladder given decreasing occupational skill, increasing task-specific work unanchored from skills, and fewer monitoring problems. 2 Under such conditions, workforce can be adjusted to changing supply and demand, tasks can be shifted to reflect immediate organizational needs, workers can be substituted or replaced with relative ease, and compensation can be organized around micro-units of tasks completed or time spent. All are hallmarks of precarious work. Empirically, however, there have been few attempts to study the relationship between occupational position and precarity in work and hence leave open the question of whether the latter may “explain” socioeconomic differences in psychological well-being.
Social Marginality as a Mechanism
If the first etiological link between occupational position and psychological well-being involves precarity in work conditions, then the second link involves social externalities beyond the workplace. To start, Standing (2011:70) argues that “the precariat” are subject to wide-ranging stigma and may have fewer social ties and relationships due to their lack of a firm occupational identity and clear, nonephemeral position with firms. For us, such arguments suggest externalities for social integration, specifically heightened risks of social marginality as a consequence of precarious work. We see at least three aspects of social marginality that have relevance for psychological well-being: (perceived) social failure, (low) social capital, and (poor) social integration. All three factors index social marginality insofar as they indicate how people are separated socially and psychologically from conventional society, social institutions, and social activity and are themselves important in the etiology of psychological well-being (Berkman et al. 2000).
Starting with perceived social failure, Standing (2011:44–45) describes precarious work as involving both job and skill reproduction “insecurities” that limit one’s ability to “retain a niche in employment” and reduce “barriers to skill dilution and opportunities for upward mobility in terms of status and income.” Such work also involves inadequate “opportunities to gain skills . . . as well as opportunities to make use of competencies.” Such a view echoes classic research on the social psychology of work that finds that those whose work involves simpler tasks, those who experience greater supervision, and those whose work is more routinized have a lower sense of agency and diminished feelings of control over occupational activities (Kohn 1989). Importantly, such feelings extend beyond the workplace and result in lower self-confidence and increased levels of fatalism and anxiety in general (Kohn and Schooler 1982). Because almost all concepts of agency index one’s ability to successfully manage social interactions and relationships, experiences of precarious work should result in heightened perceptions of social failure, which themselves should have consequences for psychological well-being.
A second dimension of social marginality is low social capital. Social capital emphasizes social ties between actors, which are infused with obligations and expectations (Coleman 1988). Consistent with this, precarious work may undermine ties to others not just within the workplace but also in the broader community by virtue of negative social attributions that accompany unemployment and the stigmatization of the unemployed (Standing 2011:70). Inadequate wages, which are characteristic of precarious work, may also lead to problems in the management of everyday life and likely undermine the desire for higher order needs of belonging, esteem, and self-actualization. This will foster negative social psychological orientations toward others, diminish trust, and undermine perceptions of others as resources (Macmillan and Shanahan 2021). Extending the argument to psychological well-being, low social capital may limit the flow of prohealth information or undermine social control over deviant health-related behaviors, impede access to services and amenities that are resources for the maintenance of good health, and impair affective support that fosters self-esteem and mutual respect (Kawachi and Berkman 2000). An important element here is trust and the ways in which trust fosters both reciprocity and exchange and the perception of reciprocity and exchange, which makes people feel better about themselves and their communities.
A third dimension of social marginality is limited social integration. The key, some say defining feature of precarious work is its ephemeral nature, which reduces opportunities for meaningful workplace participation (Standing 2011). Competition is also institutionalized as “real” workers struggle to maintain their position in the firm while those in precarious work compete to gain entry to nonprecarious employment. Ephemerality in employment is coupled with heightened socioeconomic vulnerabilities, which likely reduce the frequency of interactions with other employees outside of work (Standing 2011). Cyclical unemployment and financial vulnerability should also undermine the willingness and the ability to form ties due to perceived stigma and lower capacity for social interactions beyond the workplace, thereby contributing to the general marginalization of precarious workers (Handler and Hasenfeld 2006).
Figure 1 is a graphic version of the overall conceptual model. The model begins with sociodemographic and socioeconomic background, which includes age, gender, nativity, and marital status. These variables are complemented with measures of socioeconomic status in one’s family of origin indexed by family social class and parents’ educational attainment and the respondent’s educational attainment, labor market position (e.g., being employed or looking for work), and low income. Although causal order is ambiguous in some cases, we treat these factors as exogenous to contemporary occupational position. This then shapes exposure to precarious work, with the general expectation that exposure to precarity in work increases as one moves down the occupational ladder. Heightened precarity, in turn, increases social marginality, including perceptions of social failure, social capital, and social integration, all of which have direct effects on psychological well-being. Importantly, we allow the background variables to influence mental health directly but view social marginality and precarious work measures as largely accounting for occupational differences in mental health.
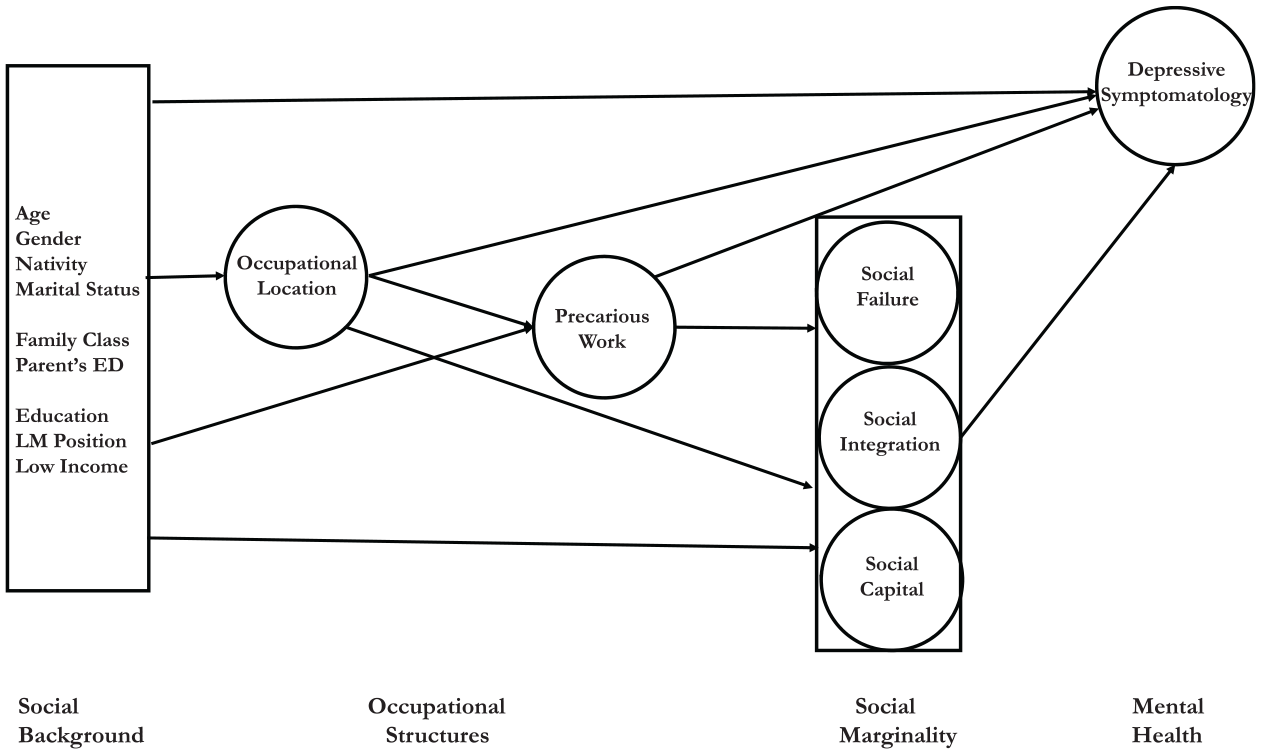
Conceptual Model.
Welfare state contingencies
Although a fundamental cause perspective offers a totalizing perspective on the relationship between socioeconomic status and health, prior work on the European context suggests macro-level contingencies. Of primary importance is the intersection of production regimes, employment regimes, and welfare state context that should shape both exposure to precarious work and the extent of extramarket supports that could buffer otherwise negative consequences (see discussions in Bambra and Eikemo 2009; Esping-Andersen 1990; Gallie 2009a; Hall and Soskice 2001). Based on prior work, we adopt a five-fold classification that differentiates Scandinavian, Continental, Anglo-Saxon, Mediterranean, and Eastern European contexts.
In general, we expect that the psychological implications of precarious work would be weakest in Scandinavian countries. Here, labor protections are comparatively high, including those limiting exposure to fixed term contracts (Barbieri and Cutuli 2016). Early skill formation and consequent skill specificity are also more prevalent. This increases costs and risks of casually hiring and firing employees, devolves responsibility for tasks to workers, raises costs for (micro)management, and ultimately increases consensus-based approaches to decision-making that necessitate the involvement of workers (Gallie 2009a). Unemployment, particularly chronic unemployment, is comparatively low given stronger commitment to universal employment (Bambra 2011), more resources devoted to training and labor market placement of the unemployed (Gallie 2009a), and stronger scaffolding for moving people from fixed term contracts to more stable employment (Barbieri and Cutuli 2016). Finally, the Scandinavian regime has particularly strong extramarket supports for both workers and those outside paid employment (Esping-Andersen 1990), and thus financial vulnerability associated with precarious work should be low. Given this, we expect that both the occupational structure of precarious work and the direct and indirect effects on psychological well-being to be comparatively weak in the Scandinavian context.
At the other end of the spectrum is the Eastern European context. First, the absence of early capitalists or financial intermediation created a unique form of privatization that produced remarkable employment precarity. Job loss is common, and its impact on health is profound (Stuckler, King, and McKee 2009). Second, the retention of authoritarian and repressive institutions hampered the development of a coordinated market economy and resulted in low levels of labor protection and reduced freedom for smaller businesses. As a consequence, control over work and ability to influence the direction of activities is remarkably low (Lane 2007). Third, economic structuration was fragmentary and often ephemeral (Knell and Srholec 2007). Given this, Eastern European countries were particularly susceptible to external influences, particularly when they were easy to implement and fit with a low level of economic coordination and a weakened state apparatus. Flexibility in employment relations and other features of precarious work are archetype examples. Finally, financial vulnerability is high given limited social welfare, particularly income supports (Fenger 2007), that is coupled with comparably low wages and low purchasing power (Rainnie, Smith, and Swain 2002). In sum, exposure to precarious work should be most pronounced in the Eastern European context.
The situation in Anglo-Saxon, Continental, and Mediterranean regimes is less clear.
With respect to skill formation, formal systems are extensive in Continental countries but virtually nonexistent in Mediterranean ones. Moreover, there is little early skill formation in Anglo-Saxon countries, but it increases with advancing career (Gallie 2009a). Given this, non-indefinite or fixed term contracts should be most prevalent in Mediterranean countries, followed by Anglo-Saxon and Continental countries. Likewise, early skill formation should foster greater task discretion among workers in Continental countries (Gallie 2009a, 2009b), but both task discretion and organizational influence may be higher in Anglo-Saxon countries given increases in occupational skills with advancing tenure (Gallie 2009a) and the stronger unionization (Visser 2006:Table 3). In contrast, weak skill formation systems and minimal vocational training in Mediterranean countries should undermine both job control and organizational influence. Decommodification and support for universal employment is also variable across the three contexts. Although unemployment rates in general are relatively low, Anglo-Saxon regimes have minimal reentry programming for those out of work, and this exacerbates risks of chronic unemployment. In contrast, there are stronger institutional supports for returning people to paid employment in the Continental context. Cultural proclivities in the Mediterranean context view the family as a functional alternative to state-sponsored welfare, with the consequence of a fairly high tolerance for unemployment, particularly among women (Saint-Arnaud and Bernard 2003).
Finally, extramarket supports and social welfare in general are also variable. In Anglo-Saxon contexts, social welfare provision is marginal, means-tested, and stigmatized, and this should increase financial vulnerability due to both low wages and minimal extramarket supports. In contrast, continental countries are quite generous with respect to social benefits, and this should mitigate financial vulnerability associated with precarious work. In Mediterranean countries, there is a preference for social spending on old age pensions that concomitantly fosters financial vulnerability among those unemployed (Sapir 2006). In the aggregate, there are not particularly strong grounds for rank-ordering Anglo-Saxon, Continental, and Mediterranean regimes with respect to risks of precarious work except to hypothesize that exposure to precarious work should be higher in Mediterranean countries, although the distinctions may not be large.
Data and Methods
The data came from the 2012 cycle of the European Social Survey (ESS), chosen due to the unique availability of key measures. Given our interest in paid employment, the sample was restricted to those between the ages of 18 and 75 in private residences and who were either working or actively looking for work at the time of data collection. The final sample consisted of just over 18,000 respondents from 23 European countries representative of the five welfare state regimes described earlier. 3 Detailed information about the ESS can be found at https://www.europeansocialsurvey.org.
Measures
Depressive symptomatology was measured with the eight-item Center for Epidemiologic Studies Depression Scale (CES-D). This was a summative index based on responses to questions asking how often one “felt depressed,” “felt everything they did was an effort,” had “restless sleep,” “was happy” (reverse-coded), “felt lonely,” “enjoyed life” (reverse-coded), “felt sad,” and “could not get going.” Responses ranged from none or almost none of the time to all or almost all of the time. The final score was standardized to range from 0 to 100, with higher values indicating poorer psychological well-being.
Occupational position was based on Rose and Harrison’s (2007) revised ESeC. The EseC differentiated (a) large employers, higher-grade professionals, and administrative/managerial occupations (e.g., lawyers, scientists, higher educational professionals, engineers); small employers and self-employed occupations (b) excluding or (c) including agriculture; (d) lower-grade professionals, administrative and managerial occupations, and higher-grade technician and supervisory occupations (e.g., school teachers, social workers, nurses, pilots, journalists); (e) intermediate occupations (e.g., clerical occupations, administrative assistants); (f) lower-grade supervisory and technician occupations (e.g., telephone line installers, precision instrument makers, electronic fitters); (g) lower-grade services, sales, and clerical occupations (e.g., shop workers, care workers); (h) lower-grade technical occupations (e.g., toolmakers, fitters, plumbers, and bus or train drivers); and (i) routine occupations (e.g., cleaners, laborers, drivers, assemblers, machine operators, porters, messengers). Collectively, the categories captured a broad variation in the nature of work, hierarchies in labor markets, and social positions of varying prestige and social standing.
As noted earlier, precarious work incorporated five dimensions. Consistent with early interest in precarity in employment, non-indefinite work differentiated those with a contract of indefinite duration from those with a contract of limited duration or no formal contract. Low job control indexed respondents who fall within the bottom fifth of the distribution on the item concerning the degree to which respondents can “decide how your own daily work is/was organized” (ranging from 0 = I have/had no influence to 10 = I have/had complete control). Similarly, low organizational influence was measured based on whether respondents can/could “influence policy decisions about the activities of the organization” (ranging from 0 = I have/had no influence to 10 = I have/had complete control). Employment gaps was based on whether respondents reported “ever being unemployed and seeking work for a period of more than three months.” Finally, financial vulnerability was measured with a question asking respondents whether they find it “difficult” or “very difficult” to live on their income.
Consistent with prior work arguing for a multidimensional conceptualization, we used item response theory (IRT) scaling to create a cumulative index of precarious work. With IRT, individual items have unique “difficulties” that define their relationship to the cumulative measure (de Ayala 2013). In our case, the greatest difficulties were seen for contract status (1.40), low job control (1.32), and low organizational influence (1.42), which indicated that higher precarious work values necessitated high probabilities of these three work traits. Although weaker, there was also significant differentiation for employment gaps (.67) and financial vulnerability (1.18). Still, the statistical significance of each individual item (p < .001) and the tight clustering of scores on a latent variable with a minimum of -4 and a maximum of 4 attests to the integrity of the measurement model (i.e., the range of IRT scores is only 0.75; [from .67 to 1.42]). The empirical realization of the latent variable was standardized to range from 0 to 100, with 0 indicating no exposure to any aspect of precarity and 100 indicating exposure to all five dimensions. 4
Because the second phase of our research examines welfare state variation in exposure to precarious work and its consequences, it is useful to briefly examine the distribution of precarity across items and contexts. This is shown in Figure 2. Consistent with expectations, all forms of precarity, including the cumulative index, were lowest in Scandinavian countries. At the same time, precarity was greatest in Eastern European countries for four of the five components and the cumulative index. As anticipated, differentiation was less clear for the other three contexts except to say that the countries of the Mediterranean context had greater average precarity on three of five components and the cumulative index. In sum, differences in exposure to precarious work were most pronounced when Scandinavian countries were compared with Eastern European ones.
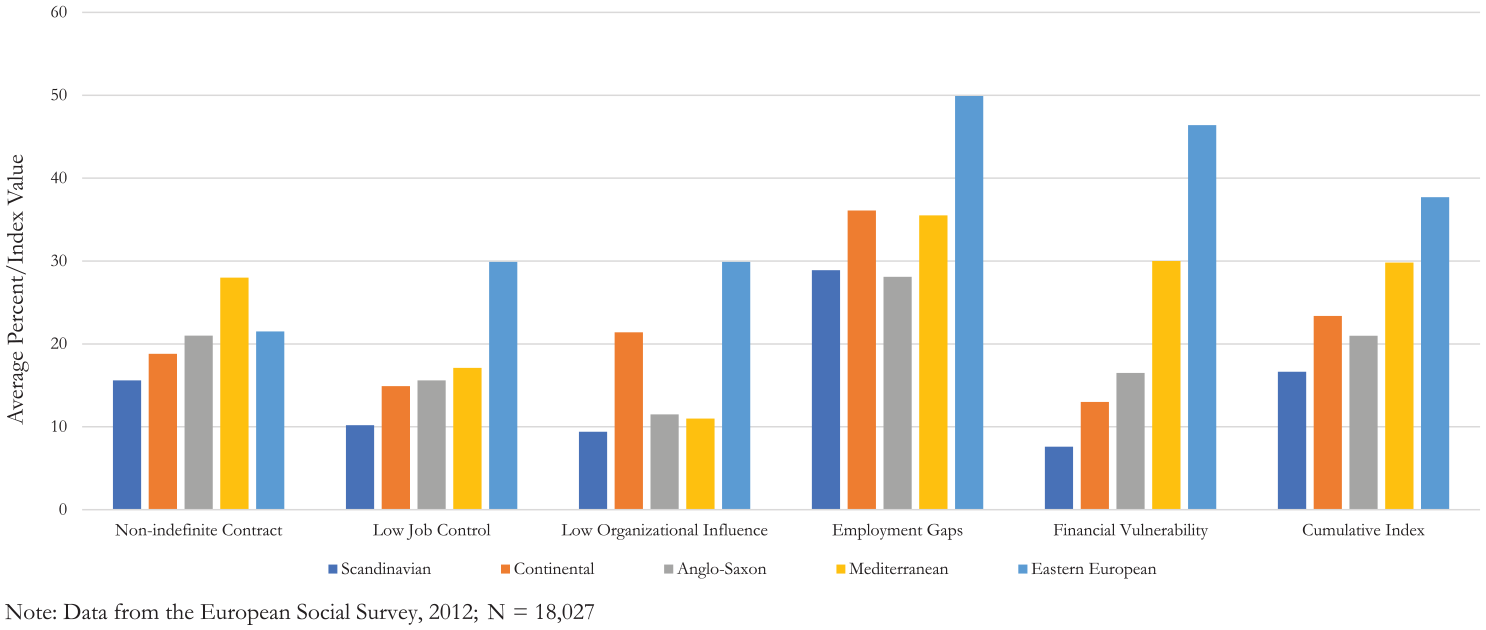
Dimensions of Precarious Work by Welfare State Regime.
Social marginality included perceived social failure, social integration, and social capital. The former was a summative index comprised of responses to three questions: “At times, [Respondent] feels like a failure”; “[Respondent] feels accomplishment about things done” (reversed); and “When things go wrong in life, it takes a long time to get back to normal.” Social integration was measured with three items, including the number of people the respondent could talk to about intimate or personal matters (from 0 to ≥10); how often the respondent met socially with friends, relatives, or colleagues (from never to every day); and the respondent’s perception of how often they took part in social activities compared to others of the same age (from much less than most to much more than most). Because these three items were on different scales, we created a normalized factor score to capture variance. Finally, social capital was a summative index comprised of whether the respondent thought “people in the community help one another” and feels “that people treat you with respect.” All three measures were standardized with range of 0 to 100.
Age, sex, nativity, marital status, family class background (at age 15), parental educational attainment, respondent’s educational attainment, and low household income (i.e., approximately the bottom decile) were included as control variables. Descriptive statistics are shown in Table 1.
Descriptive Statistics, European Social Survey–2012 (N =18,027).
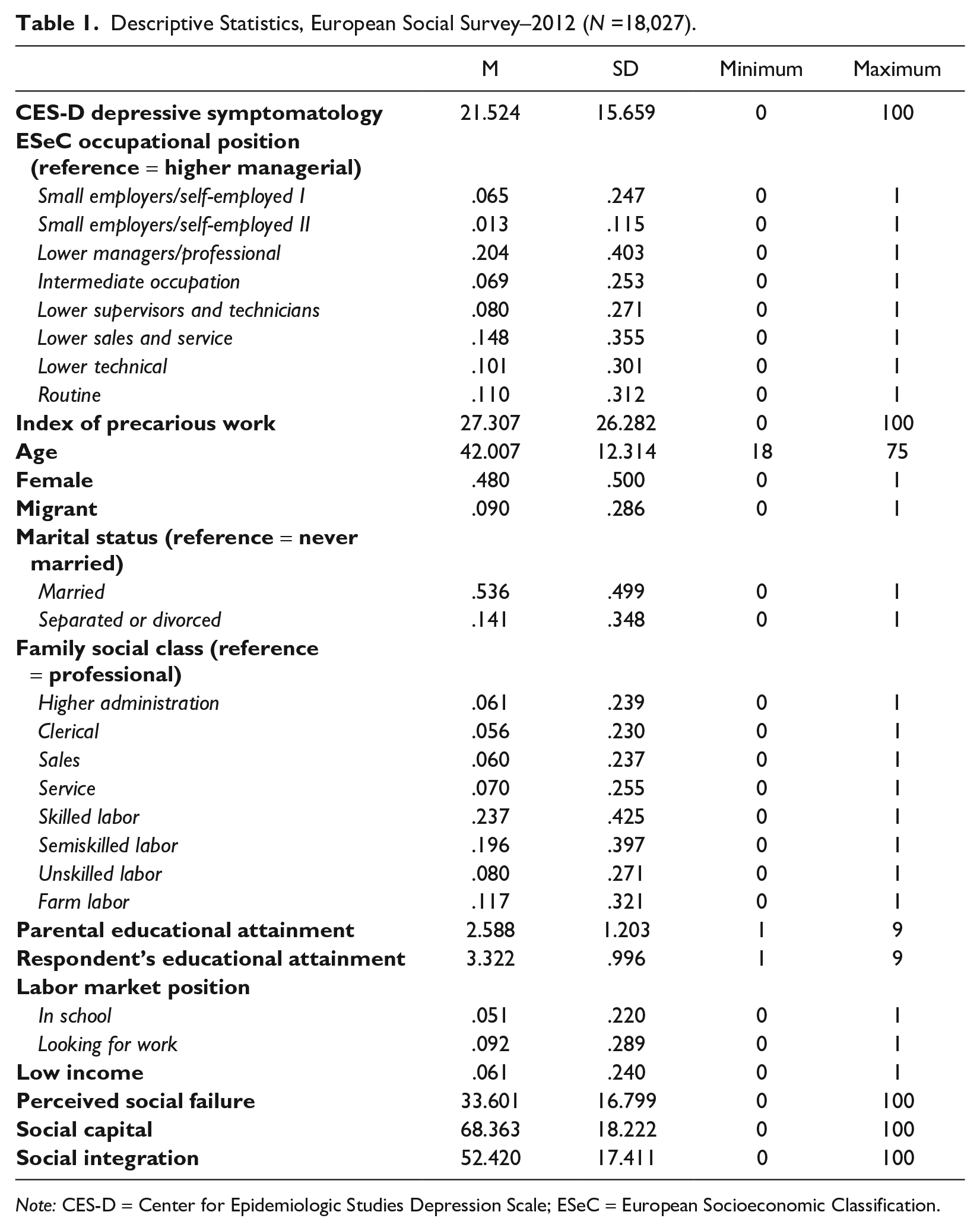
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ESeC = European Socioeconomic Classification.
Methods
The logic of statistical mediation analysis yielded six expectations (Baron and Kenny 1986). First, we expected statistically significant differences in depressive symptoms based on occupational position (i.e., the “total effect,” which was the total effect conditional on the background factors but before statistically accounting for exposure to precarious work or social marginality). Second, we expected occupational position to predict exposure to precarious work because this is the first link in the causal chain. Third, we expected a statistically significant total effect of exposure to precarious work on depressive symptoms. Fourth, we expected statistically significant effects of precarious work on all three indicators of social marginality. Fifth, we expected significant indirect effects of precarious work through the social marginality indicators. Finally, we expected strong, statistically significant “direct” effects of the proximal mechanisms—social marginality—coupled with significantly reduced effects of precarious work and occupational position on depressive symptomatology. Extent of mediation was assessed by comparing the total effects with the direct effects. Although the models included country fixed effects and a rigorous set of controls, causal inference requires the assumption of no unmeasured confounders at each “link” in the causal chain, and we recognize this as a limitation of our research.
We employed a structural equation modeling (SEM) approach in Stata 17 to estimate total, direct, and indirect effects that capture the mediation process and to take advantage of many of the recommendations of critics of the Baron and Kenny approach (e.g., VanderWeele 2016). Specifically, we used an asymptotic distribution free approach (ADF), also known as a generalized method of moments, that is appropriate when data deviate from assumptions of multivariate normality. The models estimated were substantively saturated models with all exogenous variables predicting all endogenous variables. The only restricted paths were those between the three social marginality indicators, and inspection of modification indices indicate that none would improve model fit. Given this, traditional goodness-of-fit statistics were uninformative and showed only that the model was a significant improvement over the baseline. We assessed robustness with a range of estimators, including maximum likelihood, quasi-maximum likelihood, and maximum likelihood with missing values. We also estimated standard errors using a bootstrap approach with 500 replications. Although all results were consistent, we report the ADF estimates with bootstrap standard errors in the accompanying tables. 5
Results
Occupations and Precarious Work: Mediational Models of Depressive Symptomatology
The analyses begin by examining the socioeconomics of depressive symptomatology with regression coefficients shown in Table 2. Models 1 through 6 show effects of each indicator of socioeconomic status without controls for other indicators. In each case, lower status is associated with higher symptomatology, with the largest effects seen for respondents from an unskilled labor background with respect to family social class (b = 3.932, p < .001, Model 1), respondents who were actively looking for work (b = 5.171, p < .001, Model 4), having a low household income (b = 7.574, p < .001, Model 5), and having an occupational position characterized by routine work (b = 4.985, p < .001, Model 6). Model 7 includes all six measures of socioeconomic status simultaneously. Here, the effects of socioeconomic status in one’s family of origin are largely eliminated, as is the effect of educational attainment. The remaining effects are large and robust and include contemporaneous unemployment (b = 3.580, p < .001), low household income (b = 5.789, p < .001), and a large occupational gradient with statistically significant effects for five of eight positions (bmax = 3.666, p < .001). In sum, the results show both the overall significance of differences in socioeconomic status and the substantive importance of occupational position.
Regression Coefficients: Depressive Symptomatology Regressed on Indicators of Socioeconomic Status with Select Controls, European Social Survey–2012 (N = 18,027).
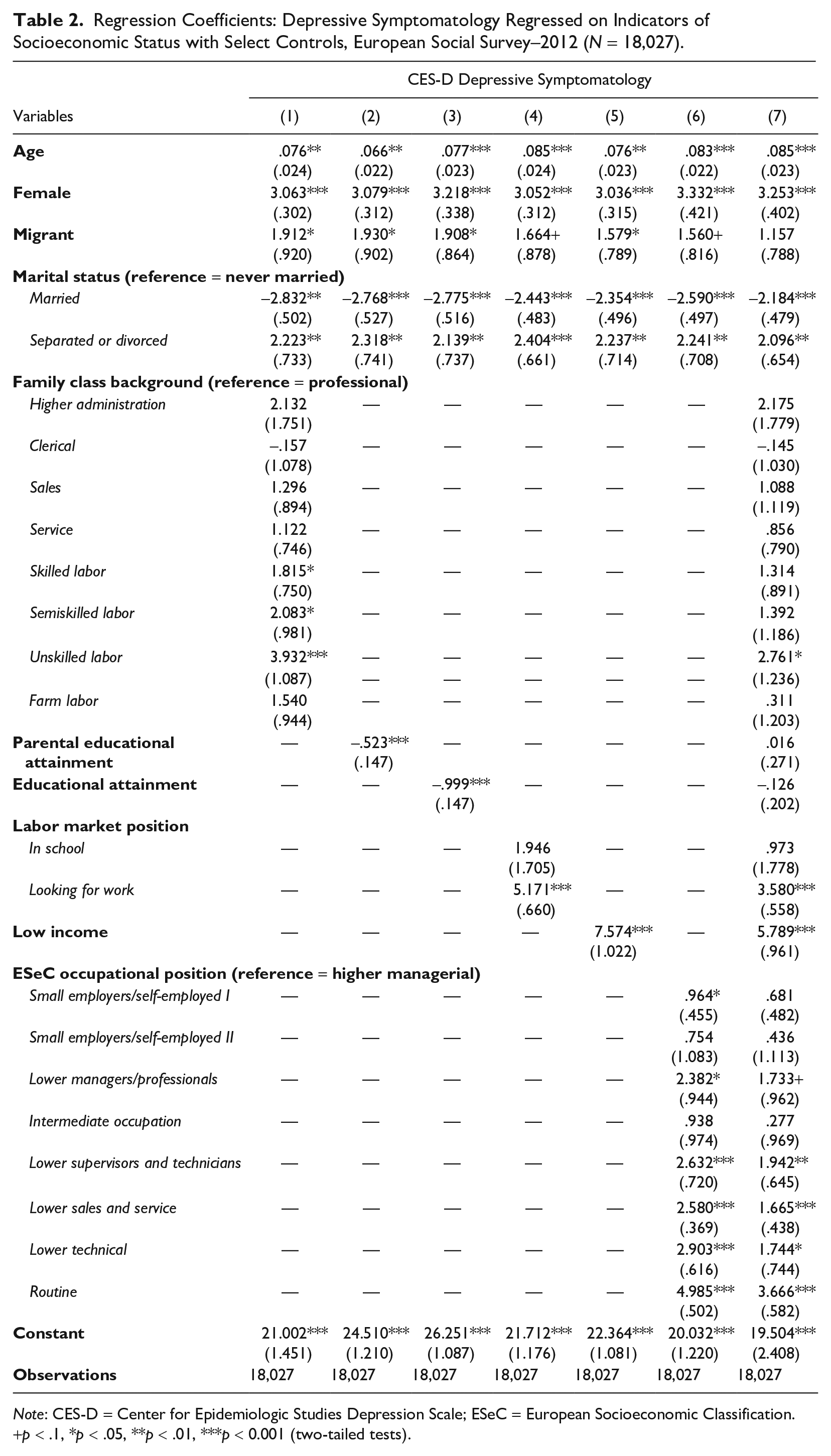
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ESeC = European Socioeconomic Classification.
p < .1, *p < .05, **p < .01, ***p < 0.001 (two-tailed tests).
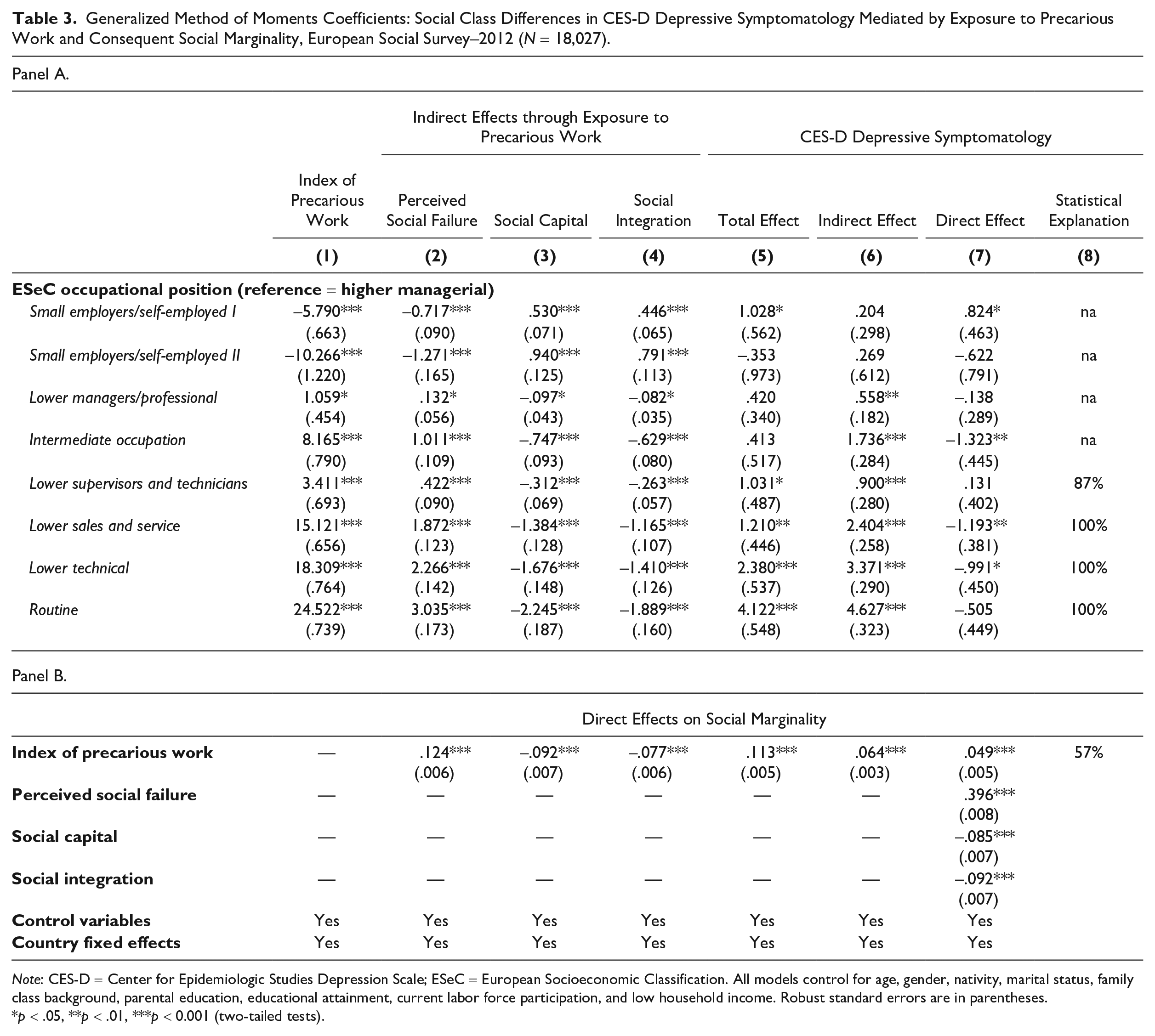
To save space, the tables showing the mediational processes include coefficients only for occupational position, precarious work, and the measures of social marginality predicting depressive symptomatology. The full models include country fixed effects, age, gender, marital status, family class background, parents’ educational attainment, respondent’s educational attainment, labor force position, and low income. Coefficients for the full sample analyses are shown in Table 3.
Generalized Method of Moments Coefficients: Social Class Differences in CES-D Depressive Symptomatology Mediated by Exposure to Precarious Work and Consequent Social Marginality, European Social Survey–2012 (N = 18,027).
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ESeC = European Socioeconomic Classification. All models control for age, gender, nativity, marital status, family class background, parental education, educational attainment, current labor force participation, and low household income. Robust standard errors are in parentheses.
p < .05, **p < .01, ***p < 0.001 (two-tailed tests).
The necessary conditions for statistical mediation include associations between occupational position and precarious work and between occupational position and depressive symptomatology. In the former case (see Panel A, Column 1), exposure to precarious work is lowest for small employers or those self-employed in agricultural work (b = −10.266, p < .001) and highest for those in routine work (b = 24.522, p < .001). This indicates an occupational gradient of almost 35 points on the index of precarious work. In the latter case (see Panel A, Column 5), depressive symptomatology is lowest for those in small employer/self-employed in agriculture position (b = −.353, ns) and highest for those in routine work positions (b = 4.122, p < .001). There is also significantly higher symptomatology for those in lower supervisorial and technical positions, those in lower sales and service positions, and those in lower technical positions. The unmediated effect of precarious work on depressive symptomatology is also large (b = .113, p < .001) and indicates that the shift from no precarity to high precarity increases depressive symptomatology by 40% of a standard deviation of the outcome (see Panel B, Column 5). Precarious work is also a strong determinant of the three social marginality indicators, with effects of .124 (p < .001), −.092 (p < .001), and −.077 (p < .001) for perceived social failure, social capital, and social integration, respectively (see Panel B, Columns 2–4).
Precarious work is also consequential for linking occupational position to social marginality, as demonstrated by the strong and fairly linear gradients for indirect effects on of occupational position on social failure, social capital, and social integration (see Panel A, Columns 2–4). In addition to this, the direct effects of the social marginality indicators are large: .396 (p < .001) for social failure, −.085 (p < .001) for social capital, and −.092 (p < .001) for social integration (see Panel B, Column 7), and there is a large indirect effect of precarious work through social marginality (b = .064, p < .001), which accounts for 57% of the conditional direct effect of precarious work (see Panel, B, Column 6). As a final issue, the model largely accounts for the occupational gradient in depressive symptomatology, including 87% of the effect of being in a lower supervisor and technician position and 100% of the differences associated with the lower sales and service, lower technical, and routine work classes (see Panel A, Column 8). In sum, all facets of the proposed model are consistent with the proposed mechanism of precarious work and social marginality accounting for occupational differences in depressive symptomatology.
Precarious Work and CES-D Depressive Symptomatology across Welfare State Regimes
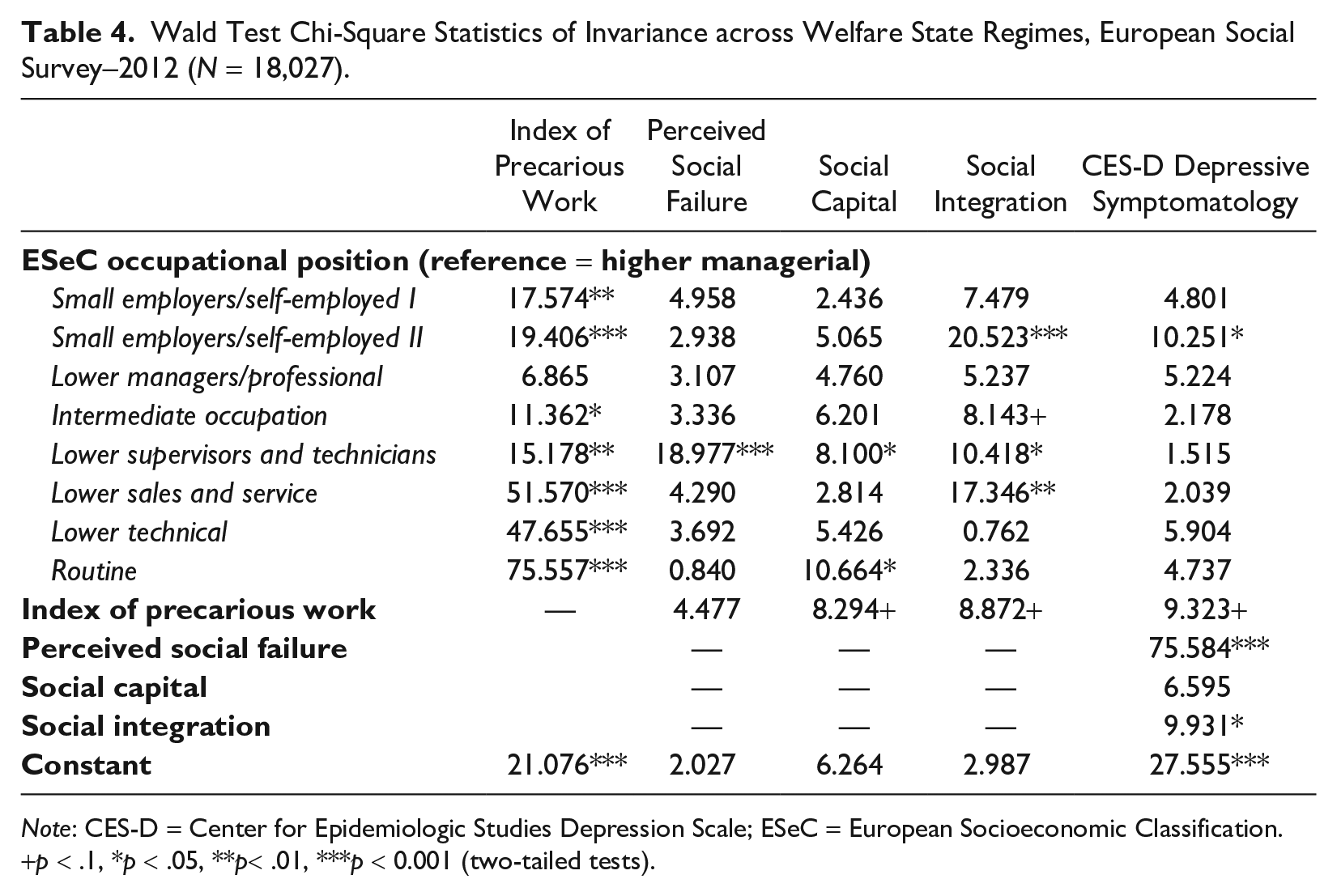
The second aspect of the research assesses variation in effects and explanation across welfare state regimes. With an SEM approach, a Wald test provides a chi-square statistic for welfare state variation in the magnitude of each of the core parameters in the model. The relevant values are shown in Table 4. There are three notable results. First, there is clear evidence that welfare state regimes moderate exposure to precarious work. One dimension of this is the significant value for the constant, indicating significant variation in the index average. Another dimension is statistically significant differences for seven of the eight occupational positions. Second, welfare state variation in the effects of precarious work on both depressive symptomatology and the social marginality indicators, while statistically significant (p < 0.1), are substantively marginal and indicate small differences across welfare state regimes. Third and equally important, two of the three social marginality indicators have variable effects on depressive symptomatology. With respect to occupational position, only the effect of being a small employer or the self-employed in agricultural work on depressive symptomatology varies across welfare state regimes. In the aggregate, there seems strong enough grounds to examine variation across welfare states, and we do so in Table 5 with a specific comparison of the strongest welfare state context—Scandinavian countries—and the strongest market-oriented context—Eastern European countries. 6
Wald Test Chi-Square Statistics of Invariance across Welfare State Regimes, European Social Survey–2012 (N = 18,027).
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ESeC = European Socioeconomic Classification.
p < .1, *p < .05, **p< .01, ***p < 0.001 (two-tailed tests).
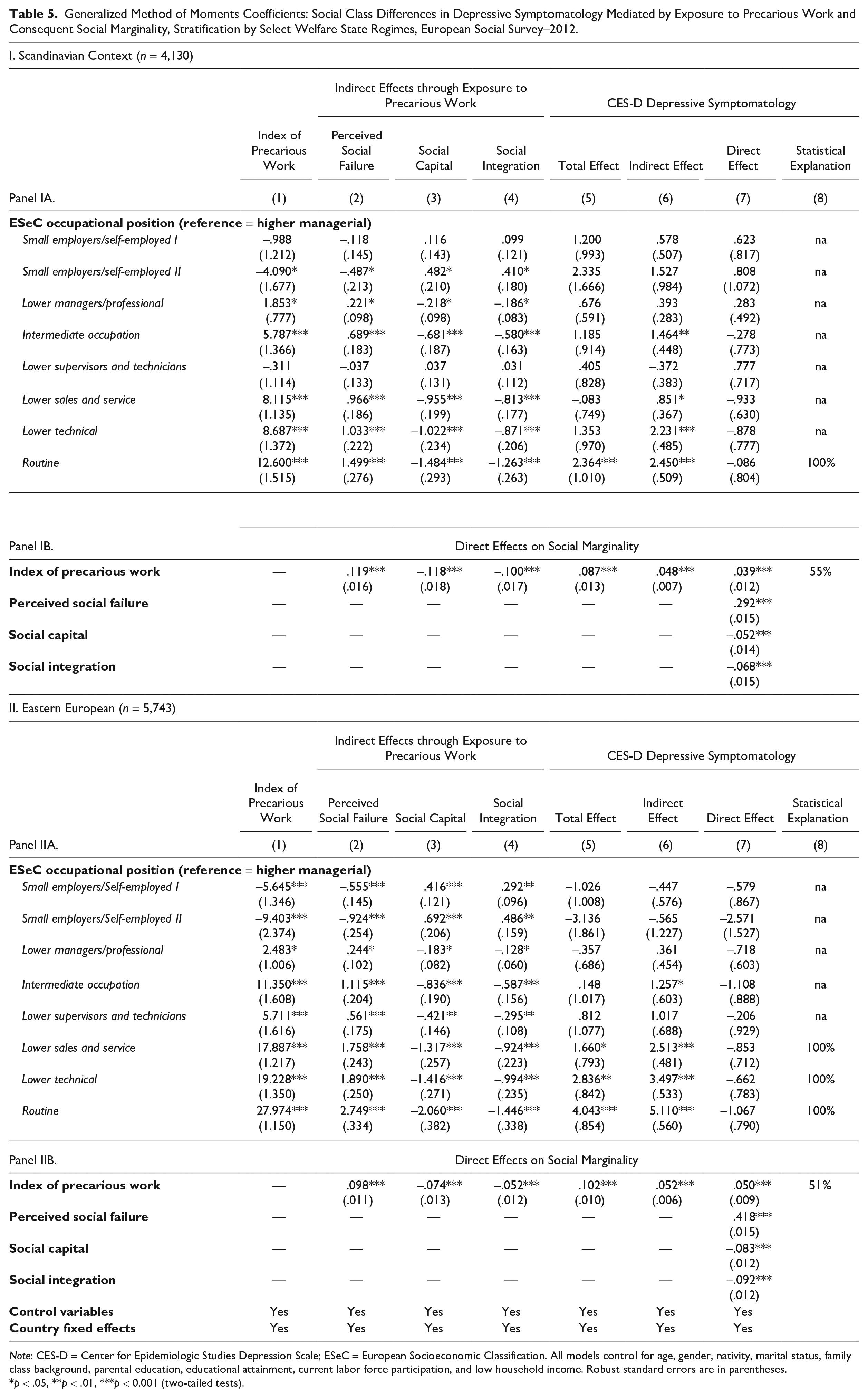
Generalized Method of Moments Coefficients: Social Class Differences in Depressive Symptomatology Mediated by Exposure to Precarious Work and Consequent Social Marginality, Stratification by Select Welfare State Regimes, European Social Survey–2012.
Note: CES-D = Center for Epidemiologic Studies Depression Scale; ESeC = European Socioeconomic Classification. All models control for age, gender, nativity, marital status, family class background, parental education, educational attainment, current labor force participation, and low household income. Robust standard errors are in parentheses.
p < .05, **p < .01, ***p < 0.001 (two-tailed tests).
To start, we see reasonable support for the argument that the model should be least salient in the Scandinavian context. Occupational differences in exposure to precarious work (see Panel IA, Model 1) are relatively weak but still show a gradient with coefficients ranging from −4.090 (p < .01) for small employers and the self-employed in agricultural work to 12.600 (p < .001) for those in routine work. The overall gradient of 16.690 is substantially smaller than a gradient of almost 35 for the full set of countries. Mitigated exposure to precarious work is coupled with minimal differences in depressive symptomatology by occupational position prior to accounting for exposure to precarious work (see Panel IA, Column 5). The core of the conceptual model is, however, still relevant. Exposure to precarious work has a significant total effect on depressive symptomatology (b = .087, p < .001; see Panel IB, Column 5), a positive effect on perceived social failure (b = .119, p < .001), and negative effects on social capital (b = −.118, p < .001) and social integration (b = −.100, p < .001; see Panel IB, Columns 2–4). All three indicators of social marginality also have significant direct effects on depressive symptomatology (bs = .292, −.052, and −.068, p < .001, for perceived social failure, social capital, and social integration, respectively; see Panel IB, Column 7) and collectively explain 55% of the overall effect of precarious work (see Panel IB, Column 8). The corresponding indirect effect is large and significant (see Panel IB, Column 6). Ultimately, we find that the nexus of precarious work and social marginality are important determinants of depressive symptomatology in the Scandinavian context but cannot explain differences by occupational position due to only minimal initial associations.
Panel II shows the coefficients for the Eastern European context—the most market-oriented regime with the weakest social safety net. Here, there are large differences by occupational position in both risk of precarious work and depressive symptomatology, with coefficients generally larger in magnitude than those seen in the Scandinavian context (see Panel IIA, Columns 1 and 5). Comparison of the cumulative gradients show that the occupational gradient for precarious work in the Eastern European context (27.974 – −9.403 = 37.377) is 2.2 times larger than that in the Scandinavian context (16.690). Likewise, the occupational gradient for depressive symptomatology is almost 3 times larger in the Eastern European context than the Scandinavian context: (4.043 – −3.156) / (2.364 – −.083) = 2.933. Precarious work also has direct effects on perceived social failure (b = .098, p < .001), social capital (b = −.074, p < .001), and social integration (b = −.052, p < .001; see Panel IIB, Columns 2–and 4). The “total” effect of precarious work on depressive symptomatology is also statistically significant (b = .102, p < .001; see Panel IIB, Column 5), as are the effects of the three social marginality measures (perceived social failure: b = .418, p < .001; social capital: b= −.083, p < .001; and social integration: b = −.092, p < .001; see Panel IIB, Column 7). Finally, social marginality explains 51% of the effect of precarious work on depressive symptomatology (see Panel IIB, Column 8), and the nexus of precarious work and social marginality explains all of the differences associated with being in lower sales and service work, lower technical work, and routine work (see Panel IIA, Column 8). Statistical explanation is moot in the other occupational positions given that there were no differences in the total effects (see Panel IIA, Column 5). As a general summary, occupational gradients are larger in the Eastern European context for all six outcomes, whereas the effects of precarious work on social marginality and depressive symptomatology and the effects of two of three social marginality indicators on depressive symptomatology are substantively similar across contexts. 7
Discussion
Precarious work provides a novel etiological pathway linking occupational position to variation in psychological well-being. Recent decades have seen a rapid expansion of precarity in work such that it is increasingly a defining characteristic of employment in the globalized economy (Kalleberg 2009). Whereas early research emphasized precarity in employment and the growth of non-indefinite contracts, recent research shows how nontraditional employment is associated with a host of other precarities, including precarity in control, influence, stability of employment, and the ability to earn a living wage (Kalleberg et al. 2000; Standing 2011; Tompa et al. 2007; Vives et al. 2010). In addition, important work has speculated on the social and social psychological consequences of precarious work, specifically those related to social marginality (Standing 2011). Ultimately, such research suggests a novel but previously untested vector of influence on health inequalities. Focusing on depressive symptomatology, our empirical work examines such connections—occupational position, exposure to precarious work, and social marginality—and shows them to be a unique and powerful path through which socioeconomic status influences health. Furthermore, consideration of political economic context shows that the chain of influence is largely robust across welfare state regimes but still mitigated by a stronger welfare state and interventionist context.
Identifying the occupational structure of depressive symptomatology and its relationship to precarity in work provides insight into the dynamics of fundamental cause perspectives on mental health. As an operationalization of occupational position, the ESeC classification is powerful in its ability to differentiate between employers and workers and in the broad conditions under which work is typically done. With this approach, a primary distinction is between small employers and the self-employed on the one hand and those that work for others on the other. In general, we find strong occupational gradients with respect to all facets of our model, notably exposure to precarious work and depressive symptomatology, and the indirect effects via social marginality. Collectively, this adds to our understanding of the dynamics underlying fundamental cause approaches to psychological well-being. Importantly, however, small employers and the self-employed occupy a unique position in that they are both less exposed to precarious work and have lower overall depressive symptomatology. In other words, they are doubly insulated. Small employers and the self-employed are, however, the smallest occupational groups and comprise only about 7% of the workforce. For other occupational positions, there is clear evidence that both the risk of precarious work and depressive symptomatology increase as one moves down the occupational ladder.
The model we propose has two novel elements that extend thinking on socioeconomic inequalities in mental health and by extension, fundamental cause explanations of psychological well-being. First, we highlight precarity in work as a primary consequence of low occupational standing that connects it to poor mental health. Although precarious work has been on the epidemiological radar for over a decade, there have been few attempts to situate it in relation to traditional measures of socioeconomic status. We fill this gap by showing a structural relationship between low occupational status and increased risk of precarity that has direct implications for mental health. In doing so, we add depth to fundamental cause arguments by advancing a “new socioeconomics” of psychological well-being whereby occupational structures shape health disparities in contemporary society because (a) they increase exposure to precarious work and (b) precarious work amplifies inequalities in mental health associated with occupational position. Here, simple algebra reveals that the combination of being in routine work and having high precarity increases depressive symptomatology by a full standard deviation compared to those in the higher managerial class with low precarity. The situation is similar for the bottom four occupational positions. Because these groups comprise almost half of the total occupational structure, the expansion of precarious work among those in lower occupational positions is a uniquely potent vector of health inequalities.
The second contribution of this work is to identify the distal mechanisms that link occupational position, precarious work, and psychological well-being. Prior work has focused largely on workplace experiences, including authority, social support, and exposure to hazards (e.g., Borrell et al. 2004; Muntaner et al. 1998; Stansfeld, Head, and Marmot 1997). By contrast, we build off of Standing’s (2011:56) articulation of the “four As—anger, anomie, anxiety, and alienation” derivative of precarious work and argue for the relevance of social marginality outside the workplace as a mechanism that links precarious work and by extension, occupational position to psychological well-being. We operationalize the latter as perceived social failure, diminished social capital, and weakened social integration and find strong support for the idea that these are distal consequences of occupational position by virtue of heightened risk of precarious work and that they statistically “explain” over half of the association between precarious work and depressive symptomatology and virtually all of the occupational gradient in mental health. Given highly variable extents of statistical explanation (e.g., Borrell et al. 2004; Hämmig, Gutzwiller, and Kawachi 2014; Kaikkonen et al. 2009) and even evidence of contradictory effects of workplace conditions (e.g., Rahkonen et al. 2006) in prior work, social marginality appears to be a uniquely powerful and robust mechanism that identifies the specific dynamics of FCT arguments in theoretically cogent ways.
At the same time, such findings suggest a need for flexibility in how we think about “power” and “resources” as a function of socioeconomic status. One aspect of this is the nature of work associated with different positions or strata and how the notion of precarity—in employment, in conditions of work, and in compensation and benefits—provides a useful theoretical frame for capturing occupational differentiation. Yet another aspect of this is the social and social psychological consequences of work that extend far beyond the workplace. Such things are resources in that they index perceptions of power and resources—realized or in the offing—that directly connect socioeconomic status to health broadly conceived. Because such issues have not received the same degree of attention as the immediate conditions of work, the challenge moving forward is to identify the broader universe of factors of relevance and empirically examine their influence.
A third contribution is a consideration of the larger political economic context surrounding occupational position, precarious work, and psychological distress. Systematic assessment of variation in effects across welfare state contexts suggests some important nuance to FCT. Countries vary in their social policy frameworks, with important differences in structures that foster skill development and specialization, willingness to intervene in market processes, and the provision of extramarket supports, financial and other. These ultimately alter the overall relationship between occupational position, exposure to precarious work, implications for social marginality, and their joint implications for psychological well-being. Although we considered five welfare state contexts, moderation is best seen by comparing the two ends of the spectrum—Scandinavian and Eastern European countries. Comparing the former with the latter, exposure to precarious work is significantly lower, and the occupational gradient is comparatively smaller. Occupational differences in depressive symptomatology are also smaller and confined to those in routine work. Drilling down to the explanatory aspects of our model, however, shows few significant differences across contexts, indicating that the nexus of precarious work and social marginality is a robust predictor of depressive symptomatology even if traditional socioeconomic status differences are muted.
There are a number of limitations of our work. Most importantly, the use of observational data limits our ability to make causal claims. We offset this with a rich, theoretically informed statistical model and country fixed effects that absorb a range of contextual influences, but causal inference still requires exogeneity assumptions. Our measurement of precarious work is also limited by the fact that different conceptualizations have suggested a number of aspects of work that could not be included (e.g., limited collective representation, perceptions of mobility prospects, scheduling precarity). There may also be other mechanisms at work, including immediate workplace hazards, social stress at work, and work-family conflict, to name a few. Another limitation is that differentiation by welfare state context highlights variation but does not pinpoint the mechanisms at work. Welfare state context is also only one of several conceptualizations of political economic differentiation (e.g., the varieties of capitalism approach; Van Winkle and Fasang 2017). There are many ways in which we can think about grouping countries into theoretical cogent collectives, and our approach, although grounded in a small number of strong theoretical frames, should be evaluated against other approaches. Thus, future research should consider other political economic frameworks and mechanisms of influence. Importantly, research on precarity in work, how it fits into broader questions of socioeconomic differentials in health, and the mechanisms that link it to health is really in its infancy, and future research will no doubt shed valuable light on the dynamics at work.
Research on the socioeconomic basis of health and well-being has been enormously important for epidemiological investigations over the last century and lies at the core of FCT accounts of health inequalities. However, conceptual and operational variation in defining socioeconomic status and its meaning greatly complicates empirical work and often undermines the accumulation of coherent evidence for both science and public policy. In this article, we bring together “old” and “new” aspects of socioeconomic status—occupational position and exposure to precarious work, respectively—and situate them in relation to an epidemiologically relevant but empirically unexplored proximal determinant of health—social marginality. This expands existing explanations by identifying a novel set of processes that explain why position in occupational structure is a fundamental cause of health and well-being. Given that there is no evidence that the expansion of precarious work is slowing, the processes we describe should become increasingly prevalent and will ultimately reshape the how and why of occupational inequalities in health for years to come.