
Abstract
Introduction
Exposure to the criminal justice system at various stages (e.g., criminal conviction, incarceration in a facility) is a less-studied but important socio-environmental factor that impacts individuals’ behavior and outcomes, including substance use (Fernandes, 2020; Massoglia & Remster, 2019). Beginning around 18 years of age, emerging adulthood is a time of profound life changes (Scott, Rosen, & Paulman, 2023; Friedman, Miyake, Altamirano et al., 2016) such as enrolling at a university and/or getting married. Yet it is also a period when higher order thinking skills are still in development (Arnett, 2000; Lebel & Beaulieu, 2011). Justice system involvement during emerging adulthood could result in an individual incurring a label of ‘criminal’ that could limit their future, including employment opportunities (Bernburg & Krohn, 2003; Kurlychek, Brame, & Bushway, 2007). These limitations may contribute to subsequent re-arrest and re-conviction (Chiricos, Barrick, Bales et al., 2007), as well as other adverse outcomes such as substance use (Lopes, Krohn, Lizotte et al., 2012). While some research has been conducted on the impact of justice system involvement on health, the health effects – including substance use trajectories – of the continuum of justice system involvement remain understudied (Fernandes, 2020). The present study addresses this gap in the literature by examining how involvement with the justice system (conviction, incarceration) during in emerging adulthood contributes to substance use trajectories through individuals’ mid-thirties.
This study tested the idea that justice system involvement (JSI) during emerging adulthood beyond arrest contributes to increased substance use during subsequent years. In prior work (Hassett-Walker et al., 2017; Hassett-Walker & Shadden, 2020; Hassett-Walker, 2022), the author found that arrest – the first point of entry into the justice system – was related to both increased and decreased use of substances. The present study replicates the author’s work (Hassett-Walker, 2022) on the impact of JSI on cigarette smoking trajectories, this time examining the effect of two types of JSI beyond arrest (conviction, incarceration) on binge drinking, marijuana smoking and hard drug use.
The present study contributes to the growing body of research on the impact of criminal legal stigma on health, including substance use (Howell, Earnshaw, Garcia et al., 2022; Martin, Taylor, Howell et al., 2020). The research is grounded in life course and labeling theories, described below. As many criminological studies operationalize having a label and incurring stigma as having been arrested or incarcerated, it is worth considering alternative types of justice system involvement (Martin et al., 2020), specifically incurring a criminal conviction.
Theoretical Background
Life Course Theory
Broadly speaking, life course theory refers to how individuals develop – psychologically, physically, socially – from birth until death (Kunkel & Settersten, 2021). The theory is rooted in the field of psychology but also draws from sociology and social gerontology. In discussing life course theory, Kunkel and Settersten (2021) note the concept of different “life phases” (p.11), including childhood, adolescence, adulthood and middle age. These phases are defined more by common experiences (e.g., health developments) and societal expectations (e.g., when people should marry, have children) rather than specific ages. How individuals change and respond to social stimuli during these different phases is a main focus of studies of the life course.
In terms of substance use, life course theory (Moffitt, 2017; Elder, 1994) suggests that there should be no single pattern of substance use. Rather, it is likely that there are numerous trajectories of behaviors such as alcohol and drug use (Zuber, Bechtiger, Bodelet et al., 2023). A trajectories approach holds that behaviors change over time, influenced by developments in an individual and their social circumstances. It makes sense to study substance use through the lens of life course theory, as a person’s relationship to substances such as alcohol and marijuana is an ongoing process that changes over time (Barban, 2013; Jacobs & Chele, 2023). Through the life course lens, how a person drinks alcohol or uses drugs in their early and mid-twenties is likely to differ from how they drink and use drugs a decade later. Hser et al. (2007, p. 519) note that criminological life course research “closely parallels drug abuse research in its conceptualization of dynamic patterns of long-term behavior as a combination of static and temporal patterns.”
Labeling Theory and Stigma
Prior scholarship holds that entanglement with the justice system – from arrest to criminal conviction, to incarceration – may increase (Spohn & Holleran, 2002), decrease (Murray & Cox, 1979; Smith & Gartin, 1989), or have little effect (Gottfredson, 1999; Huizinga & Espiritu, 1999) on substance use. The criminological labeling theory (Bernburg, 2019; Bernburg, Krohn, & Rivera, 2006) posits that individuals caught up in the justice system through arrest or more serious JSI levels incur a label (e.g.,‘felon’) that will adversely affect them in the future in areas such as the inability to secure gainful employment (Kurlychek et al., 2007; Chiricos, Barrick, Bales et al., 2007; Lopes, Krohn, Lizotte et al., 2012). Rima and colleagues (2023) recently found that arrest, conviction and incarceration all predicted health problems and suicidal ideation.
Labeled individuals may also be negatively impacted (e.g., reduced self-esteem) by the stigma that comes with having a criminal record (Moore, Wyatt, Phillips et al., 2023; Smith, Hoven, Cheslack-Postava et al., 2022). A review (Martin et al., 2020) of 25 published articles found that incarceration in particular was connected to multiple types of stigma (perceived, internalized, anticipated), resulting in psychological distress. Individuals with an incarceration history in particular have been found to have worse health outcomes (Rima et al., 2023), including but not limited to substance use disorders (Massoglia & Pridemore, 2015). A healthy body of research supports the negative impact of stigma on myriad health outcomes, including substance use (Earnshaw, 2020).
Beyond arrest – the initial point of entry into the justice system – a convicted individual will likely find themselves under the supervision of the Department of Corrections in some capacity (e.g., probation, incarceration). This would group them with other, similarly labeled individuals (Lopes et al., 2012; Phelps, 2024; Restivo & Lanier, 2015) further solidifying the label and associated stigma. The individual may internalize their label and begin to see themselves as a bad or worthless person. Substance use can be a way to cope with negative emotions (e.g., stress, anxiety) stemming from such situations (Colby, Linsky, & Straus, 1994). The labeled person may also be exposed to more individuals who use substances, thus reinforcing the behavior. For instance, Lopes et al. (2012) examined the consequences of criminal sanctioning in earlier life on later adulthood outcomes, finding that arrest in early life was related to substance use later on.
Substance Use and Stigma
Individuals with a substance use disorder often must contend with the stigma attached to alcohol and/or drug addiction (Hassett-Walker, 2023). Stigma associated with substance use communicates that the affected individual may be weak and lack the self-control to handle their problem (Zwick et al., 2020; McGinty & Barry, 2020). One review (Yang, Wong, Grivel et al., 2017) of research, both U.S.-based and international, found that negative reactions to substance use disorder were stronger than towards other types of mental health conditions. Stigma can impact the healthcare an addicted individual receives (Farrugia, Pienaar, Fraser et al., 2021; Kelly et al., 2010; Zwick et al., 2020). A review (Van Boekel, Brouwers, Van Weeghel et al., 2013) of 28 studies of health professionals’ attitudes about substance use disorder found that negative opinions about patients with the condition were common and connected to providing substandard care for those individuals. Individuals anticipating being stigmatized for their addiction may attempt to hide it, partaking in risky behaviors and socially isolating (McGinty & Barry, 2020). A person who internalizes the stigma may avoid seeking help altogether. At the broader societal level, public stigma around addiction contributes to discrimination in employment and housing, and resistance to have community-based resources (e.g., safe injection sites) established in some neighborhoods (McGinty & Barry, 2020; Barry, Sherman, & McGinty, 2018). One response to the addiction-stigma problem has been the call (Broyles, Binswanger, Jenkins et al., 2014; Robinson, 2017) to adopt person-first language (e.g., an individual with a substance use disorder, an individual with an alcohol use disorder) rather than potentially stigmatizing words like ‘alcoholic’ or ‘addict’.
Other Theoretical Explanations
Labeling and life course theories are not the only explanations for the crime-substance use relationship. Other explanations include subcultural theories (Golub et al., 2005), economic theory (Murphy & Dennhardt, 2016; Rasmussen et al., 1998), and the role that other factors play (e.g., genetic predisposition for addiction; Volkow & Muenke, 2012). It should be noted that there is not one sole type of substance-involved person. da Agra (2017) identified several different actors, including occasional and regular substance users, hard core/physically addicted individuals, and those involved in selling substances (i.e., drug dealers). Additionally, there is a wide range of substance types used, from legal substances such as alcohol, prescription medication, tobacco and even glue, to ‘lighter’ substances (e.g., marijuana), to ‘harder’ drugs (e.g., cocaine, crack, heroin). Historically, different substance types have become popular with different demographic groups (e.g., marijuana’s popularity in the 1960’s among middle class White youth with anti-establishment views; Adler et al., 2001). In short, there is no one theory that will explain all substance use for all individuals.
Literature Review
Substance Use in Adolescence and Adulthood
There is great heterogeneity of substance use trajectories over the life course (Hser et al., 2007), with individuals using a variety of substances (e.g., cocaine, heroin, marijuana, methamphetamines; Hser, Boyle, & Anglin, 1998). Myriad risk factors contribute to individuals’ substance use in both adulthood and adolescence, at the individual, family, and community level. These include but are not limited to dabbling in criminal activity, truancy and a lack of parental supervision for juveniles (Nicklas, Patrik, & Mats, 2022), and prior involvement with the criminal justice system (Hassett-Walker et al., 2017). Additional risk factors include peer substance use (Burrow-Sánchez & Ratcliff, 2022; Cambron, Rick, Rhew et al., 2020), living in a high-crime neighborhood (Cambron et al., 2020; Sampson, 1997), past histories of abuse (Ballard, Arnold, Vidrascu et al., 2024), stress (Linden-Carmichael, Van, Bray et al., 2022), impulsivity (Mauricio, Little, Chassin et al., 2009), “peer pressure, drug availability, or other risk factors in an individual’s social or family environment” (Hser et al., 2007, p.528). Adolescent drinking has been linked to adult drinking (Bonomo, Bowes, Coffey et al., 2004; Mason & Spoth, 2011) and adolescent drug use has been found to predict drug use in adulthood (Allen, Loeb, Narr et al., 2021; Haller, Handley, Chassin et al., 2010; Gustavo, Crockett, Wilkinson et al., 2011; Kandel et al., 1986).
Emerging Adulthood
Beginning around 18 years of age (Arnett, 2007) emerging adulthood is a period of increased risk for beginning substance use (Hammond, 2005; Stone, Becker, Huber et al., 2012; Wechsler, Rigotti, Gledhill-Hoyt et al., 1998). It is a period when an individual is still developing higher order reasoning (Arnett, 2000; Carroll, Willoughby, Badger et al., 2007; Ferriman, Lubinski, & Benbow, 2009; Giedd, Blumenthal, Jeffries et al., 1999; Lebel & Beaulieu, 2011). Young adults find themselves entering a time of greater freedom, less parental supervision, and possible solo living than during their teen years (Bonnie, Stratton, Kwan, 2015; Stone, Becker, Huber et al., 2012; Yi, Mayorga, Hassmiller et al., 2017). Increases (Chen & Kandel, 1995; White, Bray, Fleming et al., 2009) and fluctuations (White et al., 2009) in smoking, as well as use of other substances (e.g., marijuana and binge drinking) have been recorded during this time (Chen & Jacobson, 2012; Tucker, Ellickson, Orlando et al., 2005).
Substance Use and Criminality
The relationship between substance use and criminality, and vice versa, is complex. As Adler et al. (2001) have noted, substance abuse may not cause criminal behavior per se, but it enhances offending. Within the criminal justice system, “the life course of drug use in offender populations is complicated by repeated cycles of arrest, incarceration, community supervision, drug courts” (Hser et al., 2007, p.533). Jails, prisons, probation and parole offices are populated with both substance-using offenders, and offenders with histories of both property and violent crime who also abuse substances (Hser et al., 2007). A meta-analysis (Bennett et al., 2008) of thirty studies about the substance use-offending relationship found that odds of criminality were up to four times higher for drug users than non-drug users (highest among users of crack cocaine, lowest among recreational drug users); and that the relationship held regardless of crime type (violence, property crime).
That said, not all substance use-related behaviors are inherently criminal or problematic. For instance, while the acquisition of some (illegal) substances is inherently a crime, acquiring substances like alcohol (for those over 21 years) or prescription drugs is not against the law. Also, laws change over time in terms of what is versus is not illegal (case in point: recent years’ legislation legalizing the recreational use of marijuana). Historically, research has often found that when drug users were arrested, it was largely for property offenses (Adler et al., 2001; Kirwan, Quinn, Winter et al., 2015). This seemed to shift, however, with the rise of violence connected to newer drugs, particularly crack cocaine (Adler et al., 2001). While much criminal justice research has focused on drug and alcohol use leading to criminality and justice system involvement (Gottfredson et al., 2008; Inciardi & Pottieger, 1986; McGlothlin et al., 1978; Tiger, 2012), examining the causal order in reverse – that is, justice system involvement as a contributing factor to subsequent substance use – is a lesser investigated area in criminal justice research (Vaughn, Salas-Wright, Delisi et al., 2014). The topic of health including substance use of justice system-involved individuals (e.g., prisoners) has been explored perhaps more by public health researchers (e.g., Fernandes, 2020; Håkansson & Berglund, 2012; Lintonen, Obstbaum, Aarnio et al., 2012; Makris et al., 2012; Nall, Jurecka, Ammons et al., 2024; Zhang, Balles, Nyland et al., 2022). The present study contributes to the body of knowledge about justice system involvement contributing to subsequent substance use.
Family Factors
Major family-related transitions such as having children and/or marrying can reflect a commitment towards conventional life goals, and may contribute to reduced usage of substances (Bachman, O’Maley, Schulenberg et al., 2014; Labouvie, 1996) or at least a desire to desist from substance use (Kang & Kruttschnitt, 2022). Some criminological research (Sampson, Laub, & Wimer, 2006; Skardhamar, Savolainen, Aase et al., 2015; Salvatore, Gardner, & Kendler, 2020; Kerr, Capaldi, Owen et al., 2011) has found that marriage improves men’s behavior and life outcomes. Changes in women’s substance use have been linked to moving out of her parents’ home, marriage, pregnancy, and parenthood (McDermott, Dobson, & Owen, 2006; McDermott, Dobson, & Owen, 2007; Murphy & Arroyo, 2000).
Victimization Experience
Prior involvement with the justice system (e.g., arrest, incarceration) is related to being intentionally assaulted and injured (e.g., getting shot or stabbed; Hassett-Walker & Boyle, 2007). Prior victimization experience may be a cause of stress or other emotions that could contribute to increases in substance use (Crane, Hawes, & Weinberger, 2013; Lo et al., 2008; Nayak, Lown, Bond et al., 2012). In a study of justice system-involved Canadian youth (Gouin, Brunelle, Marcotte et al., 2023), participants that had experienced past victimization connected those experiences to their future criminal behavior and use of psychoactive substances.
Hypothesis
The current study tested the following hypothesis: Justice system involvement in emerging adulthood will be related to increased use of all substances during subsequent years.
Data, Variables, Model Building & Analysis
Data
Seventeen waves of data from the National Longitudinal Survey of Youth (NLSY97) were analyzed. A program of the U.S. Bureau of Labor Statistics, the NLSY97 is a deidentified, publicly available national probability sample of individuals 12 to 18 years old when they were first interviewed in 1997. A list of housing units for a cross-sectional sample, and an oversample of Black and Hispanic or Latino participants, were assembled via two independently selected, stratified multistage area probability samples, ensuring solid representation of different parts of the population as per income, race, region, and additional factors (National Longitudinal Surveys, nda). Respondents (n = 8,984) have been interviewed annually since 1997, and the retention rate through round 17 – the final survey wave in which questions about substance use were asked – is 78.1% (National Longitudinal Surveys, ndb). After 2011, interviews were conducted biennially (e.g., 2013, 2015, 2017).
Respondents are asked about a variety of topics including substance use, delinquency and crime participation, and involvement with the justice system including incarceration. By the final survey wave in which questions about substance use were asked, subjects ranged in age from 30 to 36 years of age. The idea was to follow respondents as far as possible into their life course as was available in the NLSY97. Mid-thirties can be thought of as early middle age. Other research (e.g., Morrell et al., 2000) holds that middle age ranges from 40 to 59 years of age.
Ethics
Approval from the author’s institutional review board (IRB) was sought prior to conducting any analyses. An exemption was approved on December 4, 2020 since the NLSY97 data are de-identified and publicly available through the Bureau of Labor Statistics (BLS) website through its “NLS Investigator” tool (National Longitudinal Surveys, ndc).
Variables
Dependent Variables – Binge Drinking, Marijuana Use, Hard Drug Use
Respondents were asked in every survey wave, from 1997 through 2011 and in 2015, about (a) the number of days they had 5+ drinks per day in the past 30 days (i.e., binge drinking); (b) the number of days they used marijuana in the last 30 days (i.e., marijuana use); and (c) the number of times they had used cocaine or hard drugs since the date of the last interview (i.e., hard drug use). (Note: Questions about alcohol drinks, marijuana use or hard drug use were not asked in the survey waves from 2012 through 2014. No questions about alcohol drinking, marijuana use or hard drug use were asked in the survey waves after 2015).
There are other substance use-related questions available through the NLSY97. These include whether the respondent had ever drank alcohol; if the respondent had drank alcohol since the date of the last interview; the number of drinks the respondent had in the past 30 days; if the respondent had ever used marijuana; if they had used marijuana since the date of the last interview; if the respondent had ever used cocaine or hard drugs; and whether they had used cocaine or hard drugs since the date of the last interview. Ultimately, the decision was made to select the variables discussed in the prior paragraph as they best operationalized the concept of problematic substance use, the focus of the study, rather than recreational use.
As subjects ranged in age from 12 to 18 in 1997 (and had a similar seven-year spread in ages in subsequent survey waves), the three substance use variables were recoded to reflect ‘Any [binge drinking/marijuana use/hard drug use] at __ years old’. The dependent variables pertained to the years after emerging adulthood JSI; that is, from 22 years old through 36 years old. Hence 15 new variables were created – one for each year, from 22 years through 36 years – which were subsequently used to create the dependent variables: binge drinking class, marijuana use class, and hard drug use class. (See also Figure 1 through 3. The dots on each trajectory line in each of the figures represent the responses to the question about substance use for that year). Binge Drinking Classes by Age, 5-Class Quadratic. BIC = −470454.77 (N = 933728) BIC = −470436.46 (N = 135856) AIC = −470343.17 ll = −470324.17 (see also Appendix A) Marijuana Use Classes by Age, 5-Class Linear. BIC = −266529.31 (N = 988752) BIC = −266515.44 (N = 136320) AIC = −266446.68 ll = −266432.68 (see also Appendix A) Hard Drug Use by Age, 5-Class Cubic. BIC = −121005.24 (N = 968528) BIC = −120981.59 (N = 135056) AIC = −120863.83 ll = −120839.83 (see also Appendix A)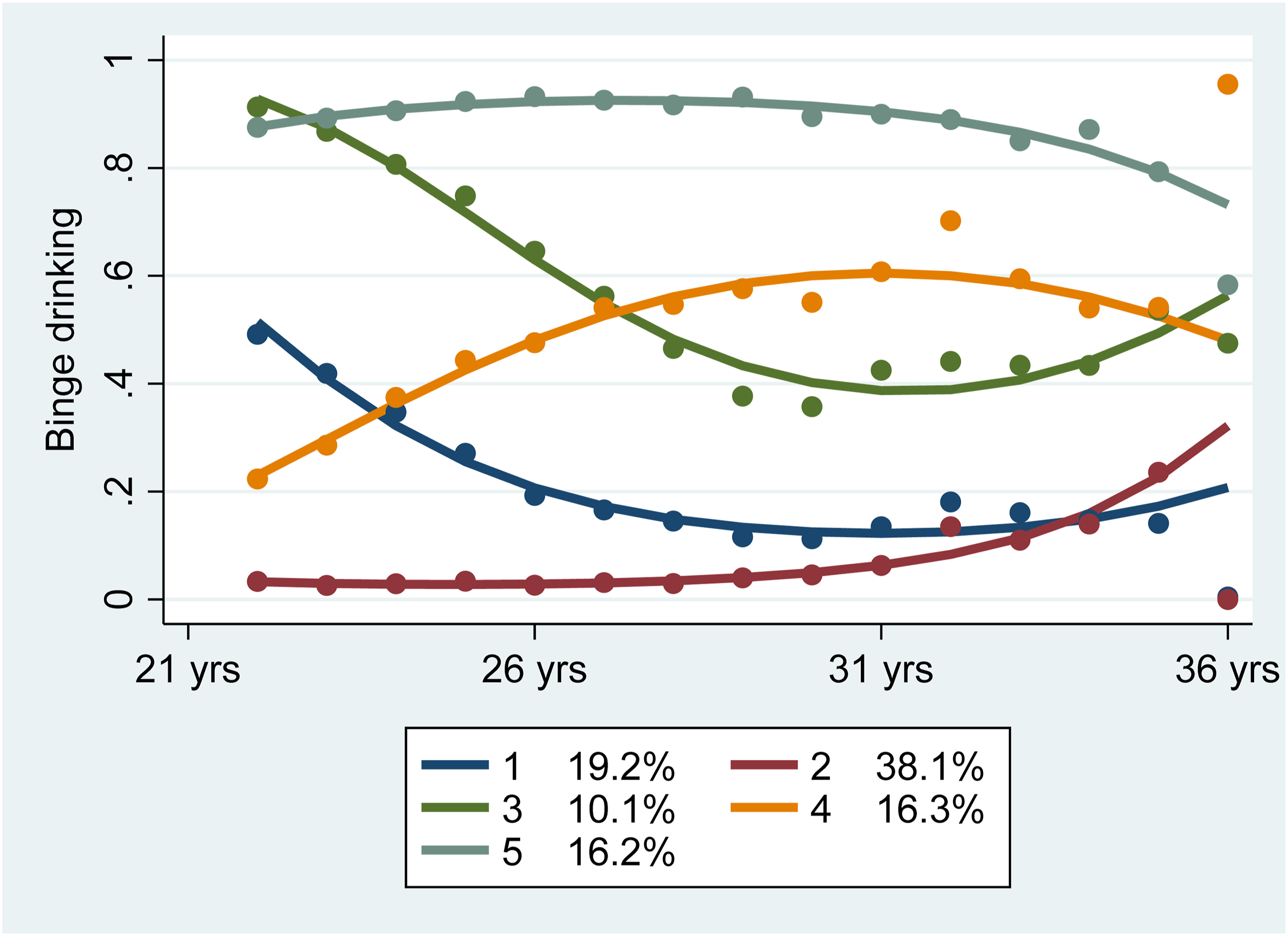
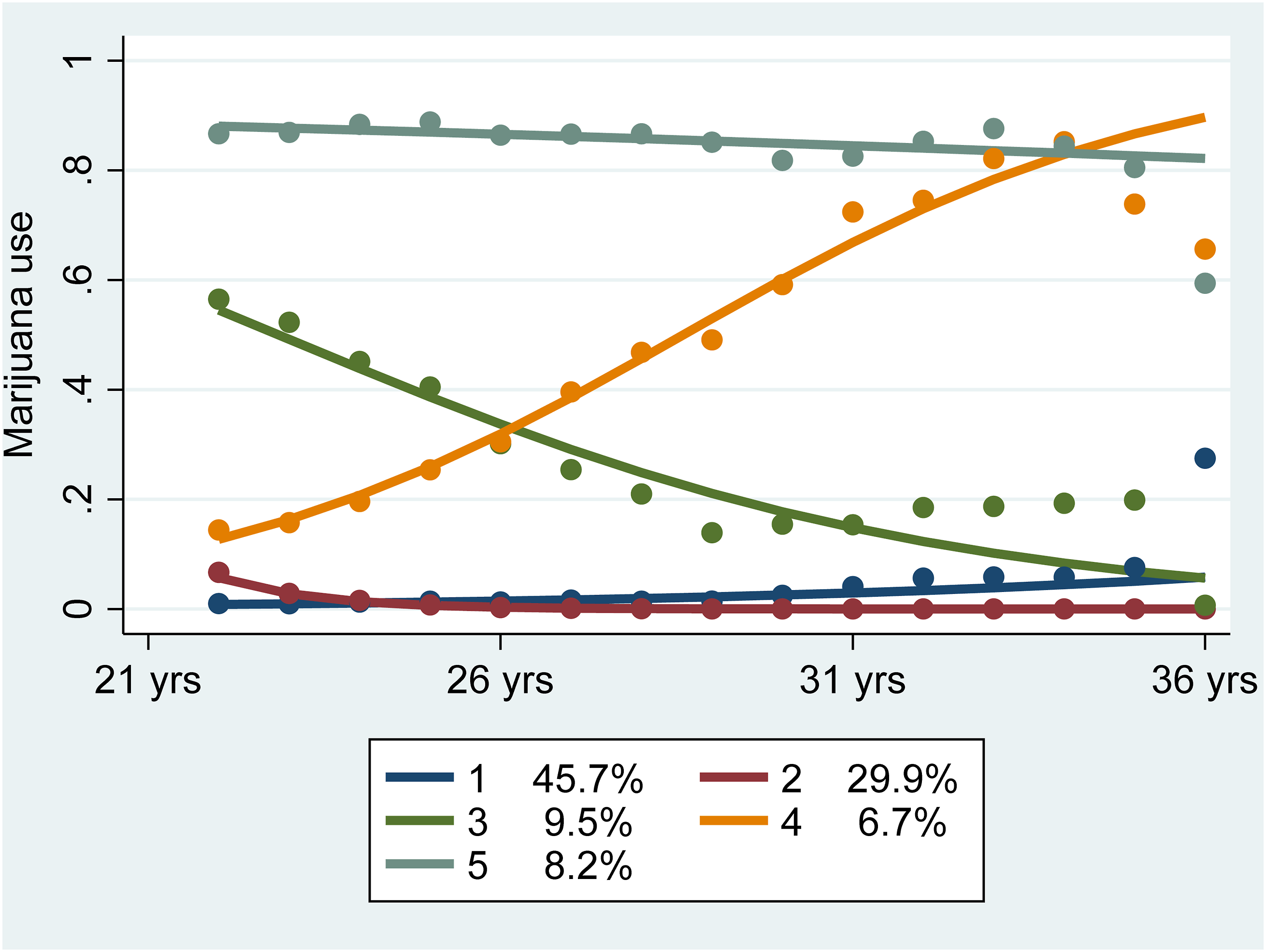
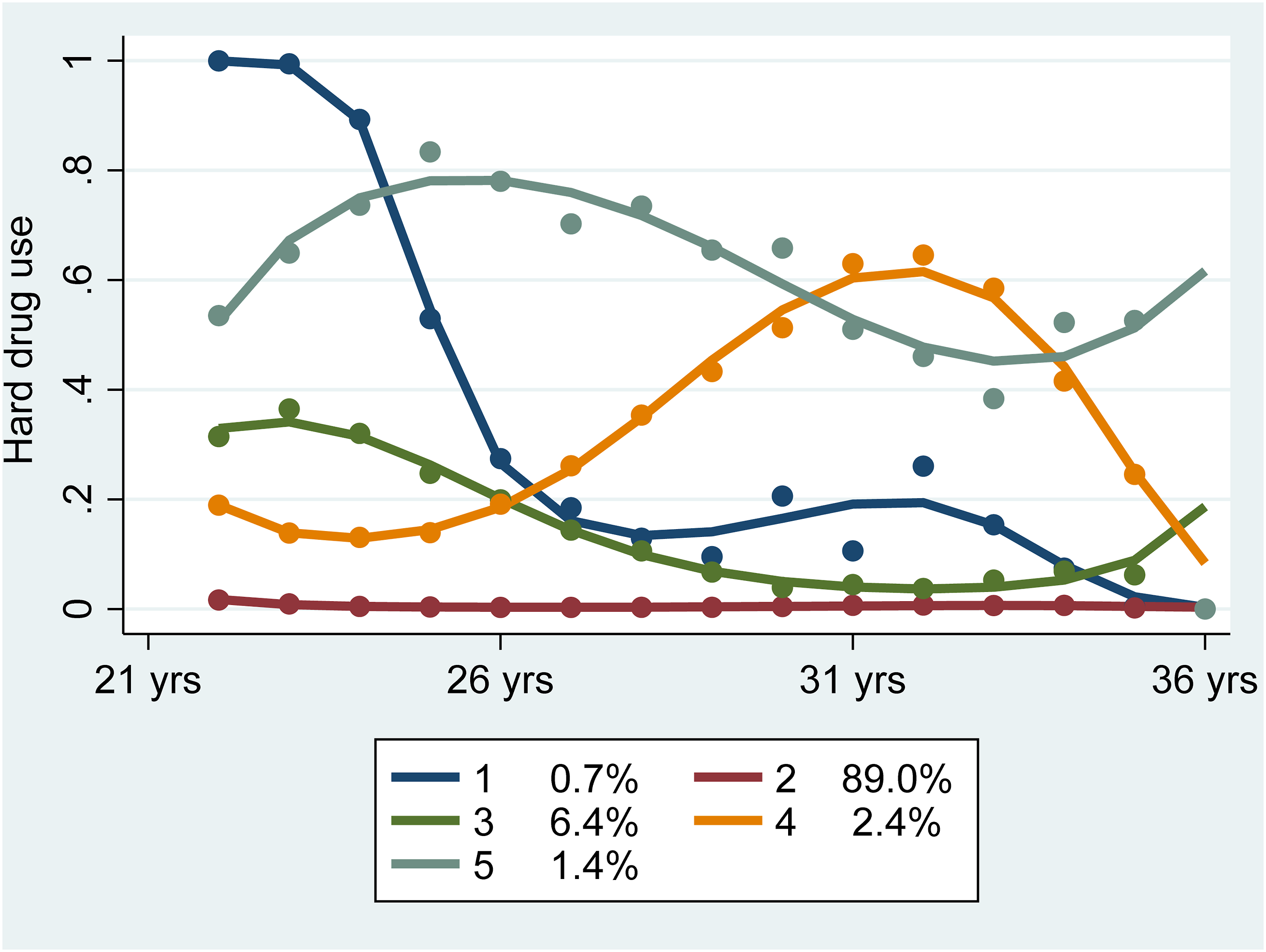
The data were then restructured to long format, and the syntax was run in Stata statistical software (see Appendix A) to determine the right number of classes. Visual representations of the binge drinking, marijuana use, and hard drug use classes (Figures 1–3) were created using the code “trajplot” in Stata.
The BIC scores for each possible configuration of each of the dependent variables were recorded and compared in Excel, for the different possibilities (e.g., 3-group linear, quadratic, cubic; 4-group linear, quadratic, cubic, etc.). The 5-group models, (quadratic/binge drinking; linear/marijuana use; cubic/hard drug use) were found to have the lowest BIC scores with all significant parameter estimates. The 5-group models are discussed below in greater detail in the model building and analyses section.
Main Independent Variable – Justice System Involvement (JSI) in Emerging Adulthood
In every survey wave, respondents were asked about whether they had been convicted or incarcerated since the date of the last interview. Since the time period of interest was emerging adulthood, defined as ages 18 to 21, the two JSI variables from survey waves 1997 to 2006 were recoded to reflect, for example, conviction at 18, conviction at 19, conviction at 20, and conviction at 21. (The same recoding was performed separately for incarceration.) 1997 through 2006 were the survey waves that contained individuals ages 18, 19, 20 and 21. Ultimately the recoded-by-age JSI variables were additionally recoded into two dichotomous independent variables: convicted_18to21 (yes/no) and incarcerated_18to21 (yes/no).
Juvenile Binge Drinking, Marijuana Use and Arrest
Relevant juvenile behaviors – binge drinking, use of marijuana, and having been arrested – were included in the analyses. Having 5+ drinks per day in the past 30 days, from ages 12 through 17 (survey waves 1997-2002), was created as a series of dichotomous variables (yes/no) using the same recoding process as described for the dependent variables. Juvenile marijuana use and juvenile arrest (from ages 12 to 17) were also included in the models, created as dichotomous variable using the same processes as just described for juvenile binge drinking.
Marital Status and Parenthood
In the NLSY97 data, a ‘collapsed marital status as of survey date’ variable is included for 1997 through 2011, and then in 2013. The options for response were: 0/never married, 1/married, 2/separated, 3/divorced and 4/widowed. During the same survey waves, respondents were also asked about the number of children (living at home and away from home) they had. These series of variables were recoded from ‘by survey year’ to ‘by respondent age’, with age 22 as the ‘start’ age (i.e., the first age after emerging adulthood). Both sets of variables were then recoded into fixed effects variables, to embody ‘marital status from 22 through 36 years old’; and ‘number of children from 22 through 36 years of age’.
Victimization Experience
A question about having been a victim of a crime in the past 5 years (yes/no) was asked in 2002 and again in 2007. Both variables were included in the models.
Demographic Covariates
Demographic variables were also included in the analyses to control for gender, racial and ethnic, and education-related differences in substance use outcomes. These were gender (1/male, 2/female), race/ethnicity (1/Black, 2/Hispanic, 3/mixed-race non-Hispanic, 4/non-Black, non-Hispanic), and degree earned by age 21 (0/none, 1/GED, 2/high school diploma, 3/associate’s degree, 4/bachelor’s degree, 5/master’s degree, 6/PhD, 7/professional degree).
Model Building and Analyses
Several analyses were performed to determine the effect of JSI and other variables on binge drinking, marijuana use and hard drug use classes. First, group-based trajectory modeling (GBTM) was conducted in Stata (StataCorp LLC., n.d.) software to determine the number of binge drinking, marijuana using, and hard drug using classes (i.e., classes = subgroups of individuals based on similar behavior). GBTM has been used by others (Evans, Simons, & Simons, 2016; Nagin & Piquero, 2010) studying behavior over the life course. As described by Nagin and colleagues (2024), GBTM can “identify the model with the smallest number of trajectory groups that still captures distinctive features of the population relevant to the study objectives” (Nagin et al., 2024, p. 303). The author used this same approach in prior work (Hassett-Walker, 2022) that focused on smoking trajectories. The Stata code used to run the GBTM to determine the different substance use classes is provided in Appendix A.
In preparing the manuscript the author conferred with colleagues well-versed in advanced statistical modeling and longitudinal analyses to double-check that GBTM followed by multinomial logistic regression was still considered the current cutting-edge statistical approach when doing trajectory-based longitudinal analyses. She was assured that it is. While this will likely change in the future as statistical methods and software progress, the author is of the opinion that at this moment in time, GBTM is the best approach to use.
As Stata does not have its own trajectory analysis function, the author used open-source code (Jones, n.d.) to install a plug-in (net install traj) to be able to run the GBTM. First, the best-fitting model (i.e., most parsimonious) was determined (Nagin, 2005) by comparing BIC scores across the different combinations of numbers of classes. BIC fit scores are commonly referred to in research that uses GBTM (Nagin, Jones, Passos et al., 2018). In addition to the BIC scores, the author considered which models did vs. did not have significant parameter estimates, which is another ingredient for selecting the best model (e.g., Saunders, 2010). (Details on the models, the BIC and AIC scores, and the Stata code used to create the models are included in Appendix A.)
Once the ideal numbers of substance use classes were determined through GBTM, next a series of multinomial logistic regressions were performed using the most parsimonious model (for binge drinking, for marijuana use, for hard drug use) as the dependent variable in each regression. This is the appropriate analytic approach for nominal dependent variables produced through GBTM (Nagin, 2005) since it allows for comparing each substance use class to the baseline ‘no use’ or ‘low use’ reference class. For each GBTM run (i.e., for binge drinking, then for marijuana use, then for hard drug use), Stata creates a new variable, traj group (or in this case, three new variables). The new variables were each renamed and used as the dependent variables – binge drinking class, marijuana use class, and hard drug use class – in the multinomial logistic regressions. Class 2 (low binge drinking, very low marijuana use, non-hard drug use) was set as the reference class for each of the regression models. It should be noted that Stata assigns the numbers to the differ classes using a computation, and the ‘low’ or ‘no’ use classes are not necessarily assigned the lowest number (e.g., 0 or 1).
The NLSY97 data were restructured to long format prior to running all the analyses. The author checked for multicollinearity and skew in the variables; neither presented a problem.
Results
Classes of Substance Use
As seen in Figures 1 through 3, there were five classes of each of the substance use types. For binge drinking, the 5-class quadratic model had the lowest BIC scores while having all significant parameter estimates (see Appendix A). For marijuana use, the 5-class linear model was the best fitting model. For hard drug use, the 5-class cubic model was the best fitting model. For binge drinking the five trajectories, or classes, of binge drinkers can be described as decreasing and low drinkers (classes 1 and 2, respective); high, fluctuating (decreasing, then increasing) binge drinkers (class 3); steady drinkers (class 4) and high, chronic drinkers (class 5). Classes 3, 4 and 5 are considered the ‘problem’ binge drinking classes (i.e., individuals whose alcohol consumption may be crossing the line from use to abuse).
The classes of marijuana users are low and very low users (classes 1 and 2, respectively); decreasing users (class 3); increasing users (class 4), and chronic users (class 5). Classes 4 and 5 are considered the ‘problem’ marijuana users. Finally, the classes of hard drug users include the non-users (class 2), the sharp decrease (class 1), and the slow decrease into low-use (class 3). Class 4 includes the fluctuating low users with a strong increase (and then decrease) in the early thirties. Both Class 4 and Class 5, the fluctuating high use class, are considered the ‘problem’ hard drug use classes.
Crosstab of Binge Drinking Classes by Justice System Involvement (JSI)
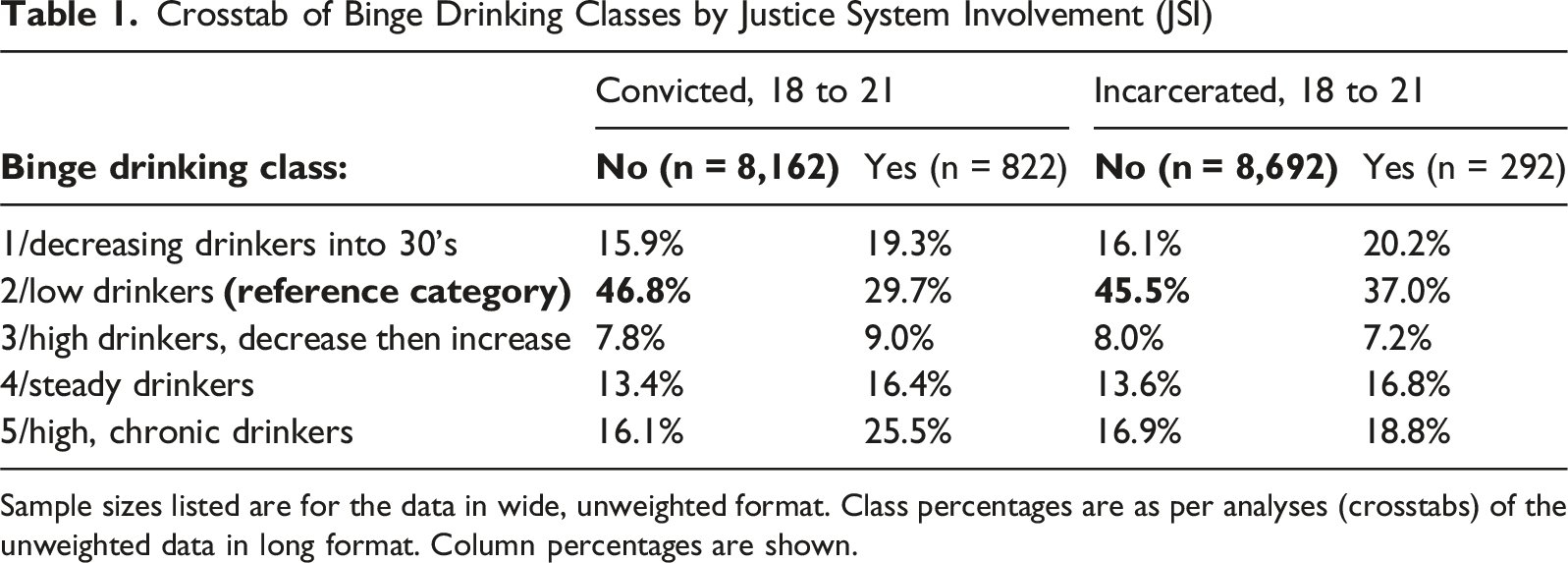
Sample sizes listed are for the data in wide, unweighted format. Class percentages are as per analyses (crosstabs) of the unweighted data in long format. Column percentages are shown.
Crosstab of Hard Drug Use Classes by Justice System Involvement (JSI)
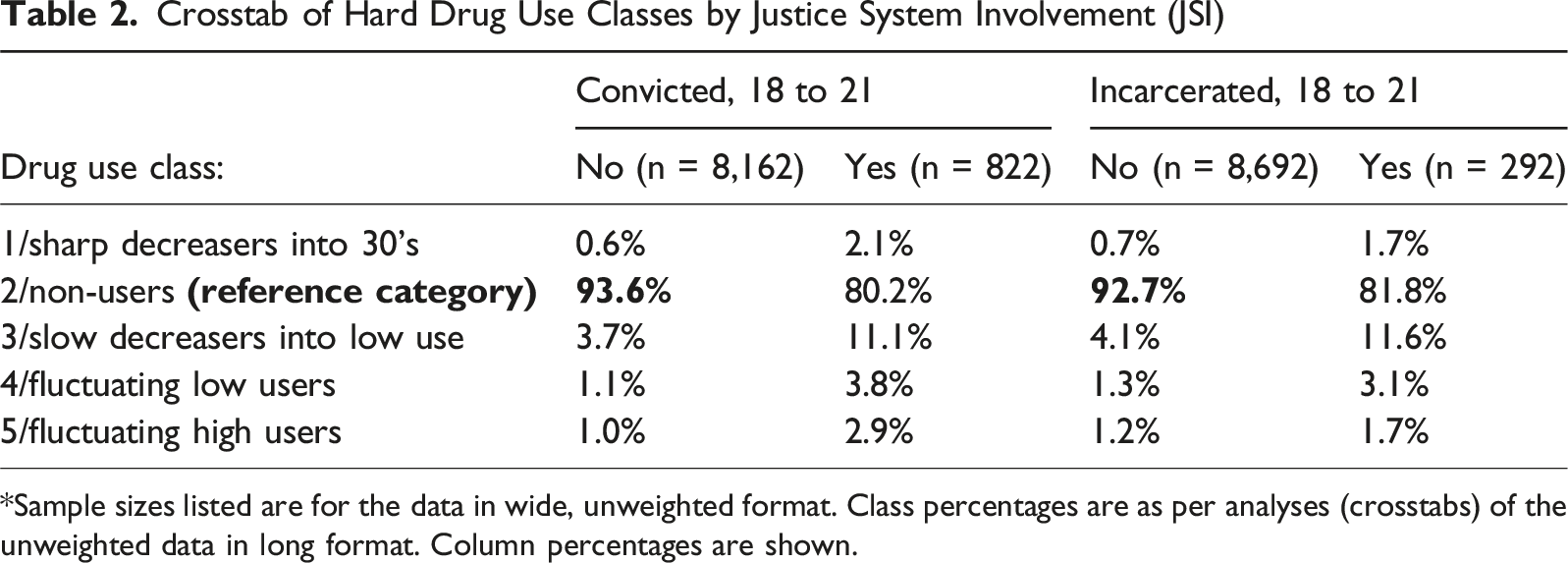
*Sample sizes listed are for the data in wide, unweighted format. Class percentages are as per analyses (crosstabs) of the unweighted data in long format. Column percentages are shown.
Crosstab of Marijuana Use Classes by Justice System Involvement (JSI)
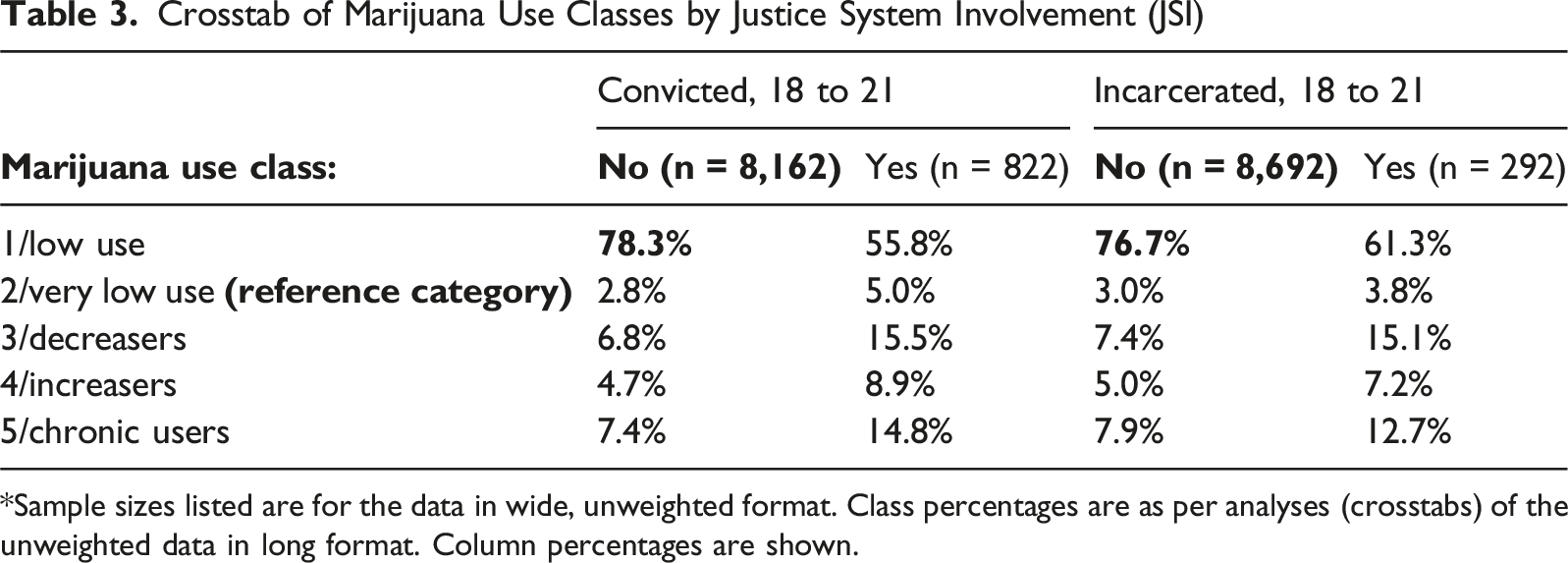
*Sample sizes listed are for the data in wide, unweighted format. Class percentages are as per analyses (crosstabs) of the unweighted data in long format. Column percentages are shown.
Hypothesis Testing: Justice System Involvement in Emerging Adulthood Will Be Related to Increased Use of all Substances During Subsequent Years
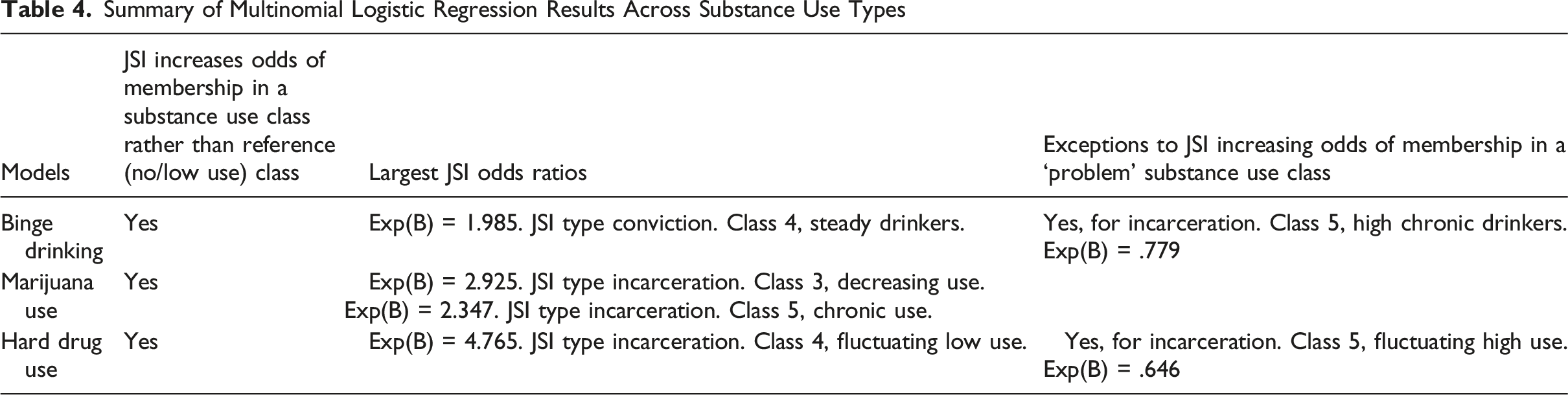
Summary of Multinomial Logistic Regression Results Across Substance Use Types
Abbreviated a Multinomial Logistic Regressions, Binge Drinking
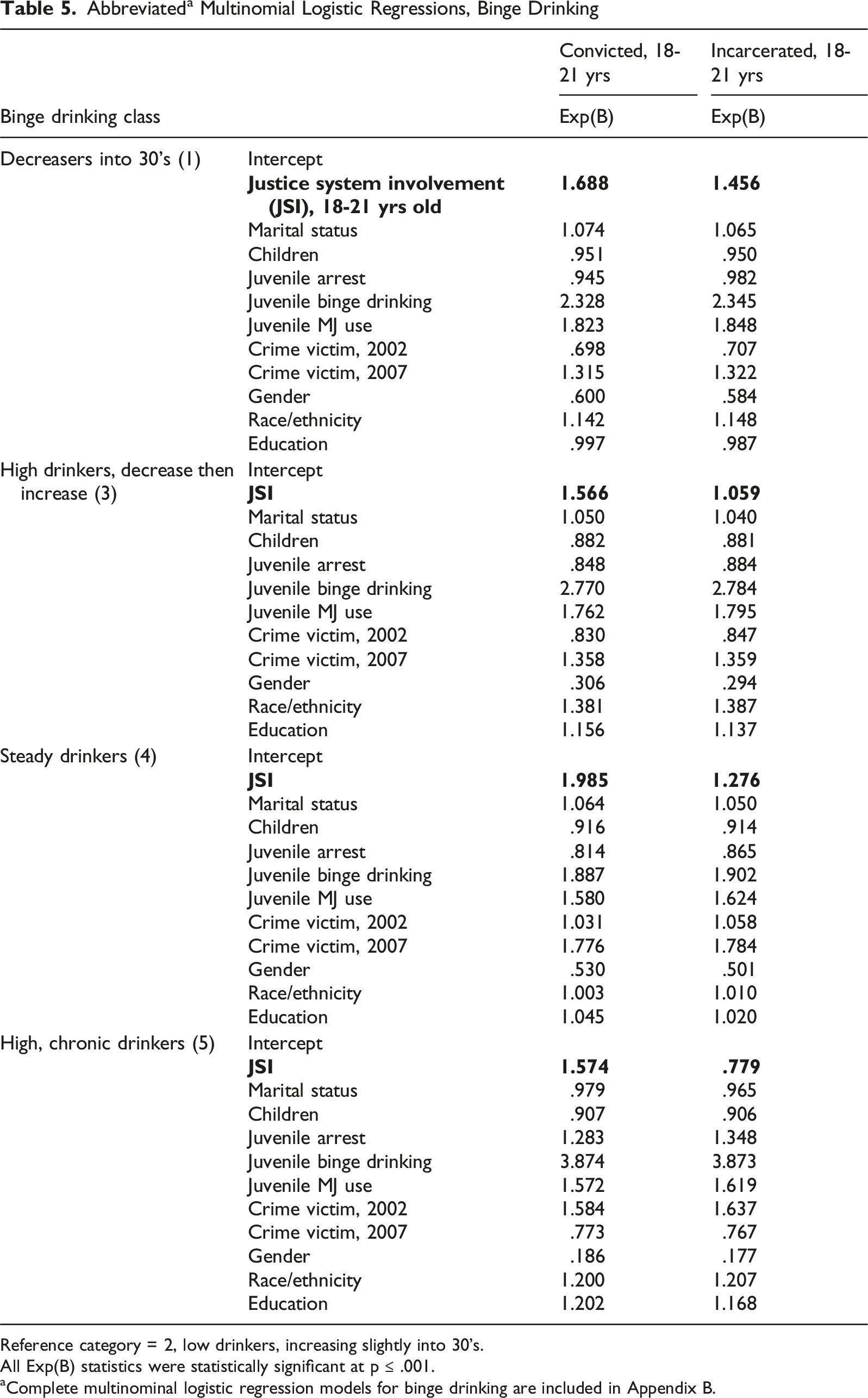
Reference category = 2, low drinkers, increasing slightly into 30’s.
All Exp(B) statistics were statistically significant at p ≤ .001.
aComplete multinominal logistic regression models for binge drinking are included in Appendix B.
Abbreviated a Multinomial Logistic Regressions, Marijuana Use
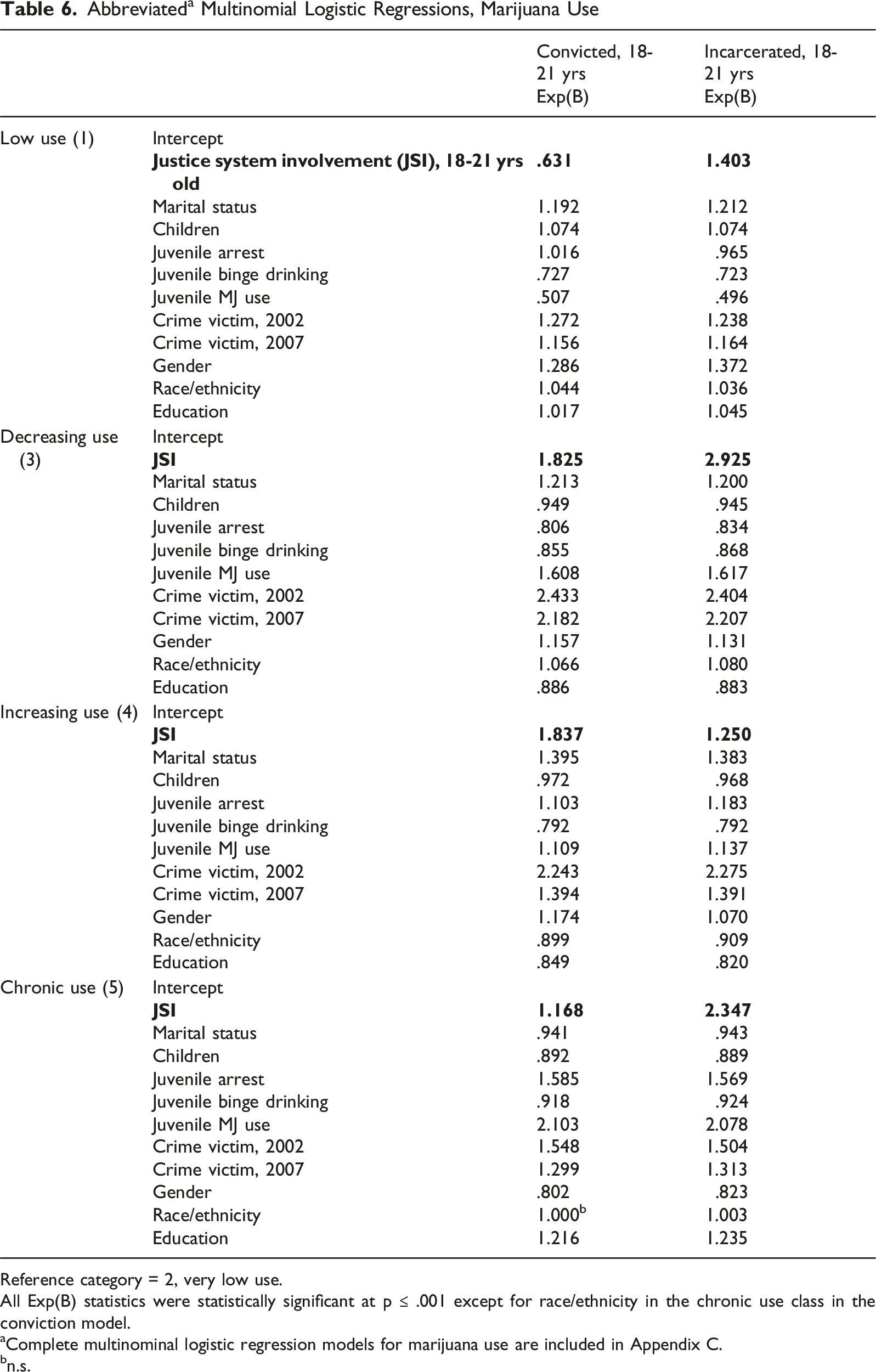
Reference category = 2, very low use.
All Exp(B) statistics were statistically significant at p ≤ .001 except for race/ethnicity in the chronic use class in the conviction model.
aComplete multinominal logistic regression models for marijuana use are included in Appendix C.
bn.s.
Abbreviated a Multinomial Logistic Regressions, Hard Drug Use
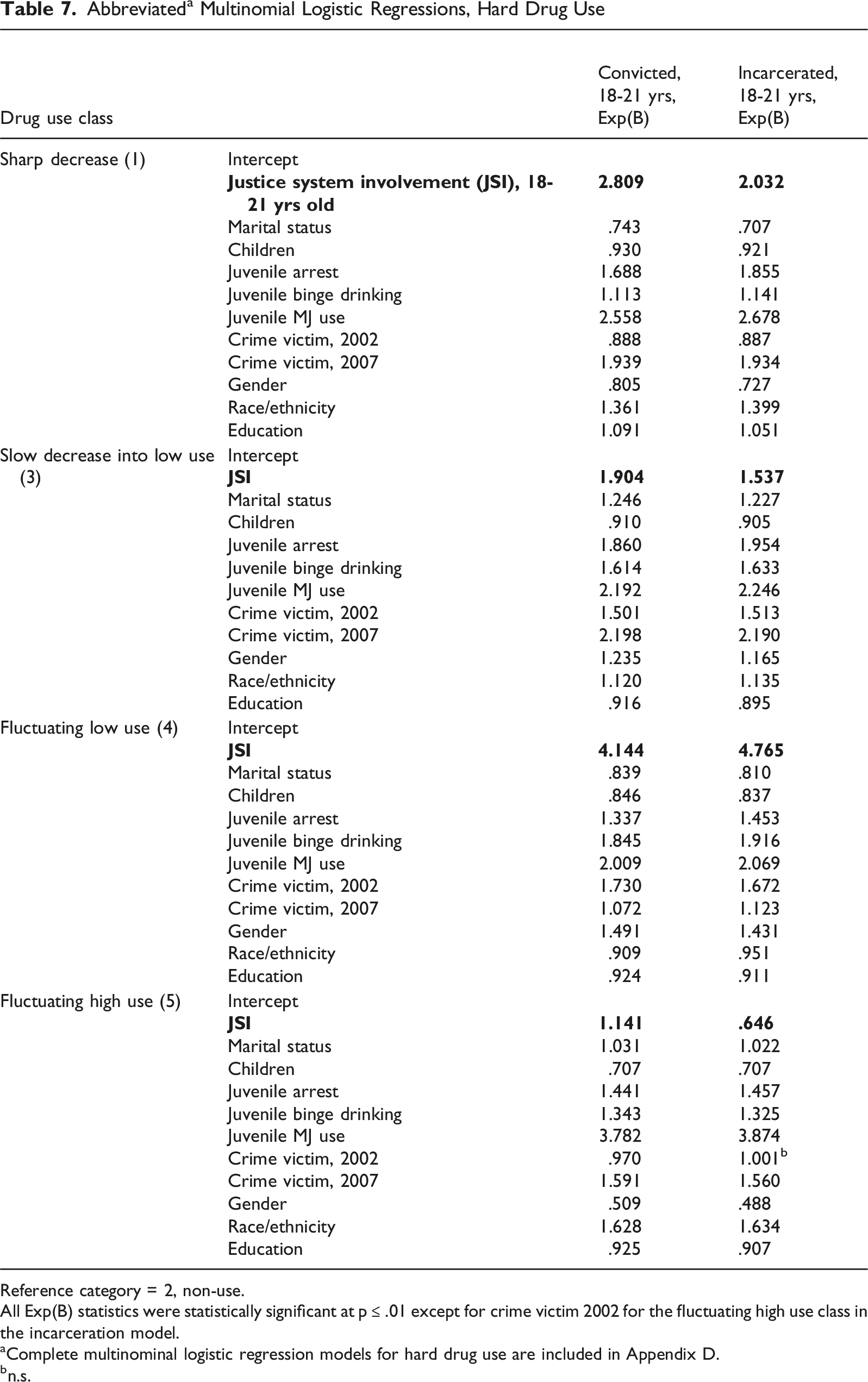
Reference category = 2, non-use.
All Exp(B) statistics were statistically significant at p ≤ .01 except for crime victim 2002 for the fluctuating high use class in the incarceration model.
aComplete multinominal logistic regression models for hard drug use are included in Appendix D.
bn.s.
In terms of JSI increasing the odds of being in one of the ‘problem’ use classes (classes 3, 4 and 5 for binge drinking; classes 4 and 5 for marijuana use; classes 4 and 5 for hard drug use), as opposed to the low- or non-use class for each substance type, the results were mixed and it depended on the substance type. This pattern is seen
As seen in Table 6, in terms of marijuana use both conviction and incarceration were related to increased odds of an individual being in the increasing user class (class 4) or the chronic user class (class 5), as opposed to the no-use or low-use reference class. The odds ratio was particularly robust for class 5, the incarceration model (Exp[B] = 2.347).
As for hard drug use (Table 7), conviction was related to increased odds of being in class 4 (fluctuating low use; Exp[B] = 4.144) and class 5 (fluctuating high use; Exp[B] = 1.141), as opposed to the low-use or no-use reference class. The odds ratio for class 4 was particularly robust. While the odds ratio for incarceration was robust for class 4 (fluctuating low use; Exp[B] = 4.765), having been incarcerated in emerging adulthood decreased the odds of an individual being in class 5 (fluctuating high use; Exp[B] = .646), as opposed to being in the reference class.
Other Findings of Interest
Juvenile Substance Use
Binge drinking as a juvenile strongly predicted the odds of being in a problem drinking class (3, 4 or 5) in both the conviction and incarceration models in Table 5. The odds ratios were particularly robust for membership in class 5 (high chronic drinkers (Exp[B] = 3.874/conviction; Exp[B] = 3.873/incarceration). Juvenile marijuana use was more strongly predictive of marijuana and hard drug using classes than was juvenile binge drinking. For marijuana use class 5 (chronic use), the odds ratios for juvenile marijuana use were 2.013 in the conviction model and 2.078 in the incarceration model (Table 6). The juvenile marijuana use odds ratios for hard drug use (Table 7) were similarly high in class 4 (fluctuating low use; Exp[B] = 2.009/conviction model and Exp[B] = 2.069/incarceration model) and class 5 (fluctuating high use; Exp[B] = 3.782/conviction model and Exp[B] = 3.874/incarceration model).
Juvenile Arrest
In terms of the impact of juvenile arrest on future substance use, in the binge drinking classes (Table 5) juvenile arrest had the greatest impact (highest odds ratios) on membership in class 5, high chronic drinking. By contrast, individuals with a juvenile arrest were more likely to be in the reference class (2) than in the steady binge drinking class (class 4) or the high drinking decrease than increase class (class 3). As for ‘problem’ marijuana use (Table 6), individuals arrested as juveniles had greater odds of being in the increasing use (class 4) and chronic use (class 5) classes than being in the reference class. Juvenile arrest produced odds ratios above 1 for membership in all hard drug use classes (Table 7), as opposed to the non-use reference class (class 2). These findings suggest that individuals arrested as juveniles were more likely to be a hard drug user (as opposed to a non-user), regardless of whether their hard drug use was decreasing (classes 1 and 3), fluctuating (class 4), or chronic (class 5). The largest odds ratios were for class 3, slow decrease into low hard drug use. In the conviction model, individuals arrested as juveniles were 86% more likely to be in class 3 than in the reference class; and in the incarceration model, individuals arrested as juveniles were 95% more likely to be in class 3 than in the non-use reference class.
Marital Status, Parenthood
As seen in Table 5, marital status slightly increased the odds of an individual being in two of the ‘problem’ binge drinking classes (3 and 4) rather than in the no-use or low-use reference class. This was not the case with class 5 (high chronic drinkers), in which marital status weakly decreased the odds of being a high chronic drinker, in both the conviction (Exp[B] = .979) and incarceration (Exp[B] = .965) models. One interpretation of these results might be that moving further through the marital status stages (e.g., from non-married to married, to separated, to divorced) is related to lower substance use. Another possibility is that aging explains the substance use-marital status relationship. In other words, as individuals age, they likely move through the different life-partner relationship stages. Additionally, as individuals grow older they also often develop new health issues, and may be more inclined to try and quit, or at least reduce, their use of substances. A similar relationship between marital status and smoking trajectories was found in earlier work (Hassett-Walker, 2022).
A similar pattern is seen in Table 6 for marijuana use. Marital status increased the odds of being in class 3 (decreasing use) and class 4 (increasing use), rather than in the reference class, for both the conviction and incarceration models. The odds ratios for marital status in class 4 are the most robust (Exp[B] = 1.395/conviction model; Exp[B] = 1.383/incarceration model). However, marital status decreased the odds of being in the chronic marijuana use class (class 5). As seen in Table 7 for hard drug use, marital status decreased the odds of being in the fluctuating low use class (class 4), but increased the odds of being in the fluctuating high use class (class 5), as opposed to being in the reference category. The largest odds ratios for marital status were for being in class 3 (slow decrease into low use), in both the conviction (Exp[B] = 1.246) and incarceration (Exp[B] = 1.227) models.
In terms of parenthood, in Tables 5–7, in both the conviction and incarceration models in each table, having children decreased the likelihood that an individual would be a binge drinker, marijuana user, or hard drug user. The most robust results are seen in Table 7, hard drug use, for membership in the fluctuating low use class (class 4; Exp[B] = .846/conviction; Exp[B] = .837/incarceration) and the fluctuating high use class (class 5; Exp[B] = .707/conviction; Exp[B] = .707, incarceration).
Victimization, Gender and Race/Ethnicity
Having been a victim of a crime in 2007, more so than in 2002, was significantly related to mostly increased odds of being in a substance use class, as opposed to the reference class, in the binge drinking, marijuana use and hard drug use models.
In all the binge drinking models (Table 5), female gender was related to greater membership in the reference class (class 2/low drinkers), across both JSI types (conviction, incarceration). (For the gender variable, males were coded as 1 and females were coded as 2.) Another way to interpret this is that males, more so than females, were more likely to be any type of drinker other than a low drinker regardless of past JSI type (conviction vs. incarceration). The results were more mixed for the marijuana use models (Table 6). Females were more likely to be in the low use (class 1) and decreasing marijuana use (class 3) classes, and in the increasing use class (class 4), than in the marijuana use reference class in both the conviction and incarceration models. Males had increased odds of being chronic marijuana users (class 5) than did females in both JSI models. In other words, men with past histories of JSI are more likely to be the most problematic types of marijuana smokers. In terms of hard drug use (Table 7), males had greater odds of being in the sharp decrease class (class 1) and the fluctuating high use class (class 5), whereas females had greater odds of being in the slow decrease into low use class (class 3) and the fluctuating low use class (class 4). One interpretation of this might be that males used hard drugs more than females, whereas females tended to fall into one of the lower use classes.
The results for race/ethnicity are less neatly interpreted given the variable’s categories (1/Black, 2/Hispanic, 3/mixed race ethnicity, 4/non-Black, non-Hispanic). The most robust results were as follows. In the binge drinking models (Table 5), the most robust odds ratios are for class 3, high drinkers decreasing then increasing. The odds ratios are nearly identical for the conviction and incarceration models (1.381 vs. 1.387) and could be interpreted as: individuals whose race/ethnicity is moving towards non-Black and non-Hispanic (i.e., White individuals) are more likely to be high drinkers than to be in the reference class. The other notable result for race/ethnicity is in the hard drug use model (Table 7). As individuals whose race/ethnicity moves towards White, they are much more likely to be in the fluctuating high use class (class 5) than in the reference class. The odds ratios are similar regardless of JSI type (conviction, incarceration).
Discussion
Grounded in life course and labeling theories, this study examined whether two forms of justice system involvement during emerging adulthood – criminal conviction and incarceration – contribute to increased substance use during subsequent years. As to the study’s hypothesis, both types of JSI generally increased the likelihood of being in a steady-use or increasing-use binge drinking, marijuana or hard drug-use class, rather than being in the non- or low-use reference class. The findings support the idea that incurring a label early in adult life can continue to negatively impact an individual’s substance use as they move into their thirties. This may be because justice system involvement during emerging adulthood results in a label (e.g.,‘criminal’, ‘felon’) and its resulting legal and social stigma, which in turn limits future opportunities such as employment or dating options. Such limitations could lead to subsequent JSI and other adverse outcomes, including but not limited to substance use. This is with the caveat that the JSI measures do not perfectly embody having a label or incurring criminal legal stigma. While it can be inferred that convicted and incarcerated individuals experience stigma that contributes to future substance use, it is also possible that lingering stress from the JSI contributed to future substance use. It is not possible to definitively determine which factor – stigma from a label, or residual stress – predicts future substance use based on the variables used.
The findings also point to the possible impact of incurring a label through having a criminal conviction, which does not necessarily mean being locked up in a correctional facility. A conviction can result in a sentence of probation rather than incarceration, for example. Having a conviction in emerging adulthood and being sentenced to probation, for instance (i.e., serving time ‘on the outside’), is as harmful, or more consistently harmful, to individuals in terms of future substance use as getting locked up. This may be due to the stigma that comes with having a criminal conviction on one’s record, and how an individual may internalize the stigma. This interpretation is with the caveat that conviction is only a proxy measure for stigma. While experiencing and internalizing stigma from a criminal conviction is inferred, it is not an absolute fact.
There may be alternative explanations for the findings, such as cumulative disadvantage or other mental health issues among individuals in the sample. It is worth considering some of the mixed findings, such as conviction but not incarceration predicting high chronic drinking. One explanation might be that incarceration by definition means a person’s JSI requires confinement in a correctional facility. Conviction, on the other hand, may mean probation and wearing an ankle monitor, but serving the sentence while remaining at home and in the community. Individuals who experienced incarceration would have had their access to alcohol limited as per jail or prison policy. If they acquired the habit of not drinking (because they hadn’t been able to during emerging adulthood, because they were locked up), they might end up staying the course in terms of low- or non-drinking. A similar pattern is seen with fluctuating hard drug use being greater among convicted rather than incarcerated individuals. That formerly incarcerated individuals were more likely to be non-users of hard drugs may reflect the different experiences of being incarcerated rather than just convicted. Jail and prison are scary places to be, and the use of hard drugs may have seemed like a ticket straight back to incarceration. Incarceration facilities may have also offered greater drug and alcohol treatment resources to individuals than probation offices (for example).
Ideas for alternative explanations aside, the findings of the study fit with existing literature (Martin et al., 2020; Rima et al., 2023) that has found that justice system involvement generally contributes to worse substance use later on in life. As most prior criminological research has operationalized incurring a label typically as arrest (and sometimes incarceration), the present study’s finding that criminal conviction is as harmful as incarceration in terms of predicting greater future substance use is a novel contribution to the knowledge base.
The ’surprise’ finding was that juvenile substance use – adolescent marijuana use in particular – predicted adult substance use as robustly, or more robustly, than conviction or incarceration. Juvenile substance use was included in the models to control for the effect of adolescent substance use on substance use in adulthood. Interestingly, juvenile marijuana consistently predicted adult binge drinking, whereas juvenile binge drinking predicted reduced marijuana use in adulthood. One possible explanation is that chronic binge drinkers in adulthood used multiple substance types in adolescence (alcohol, marijuana), but chronic adult users of marijuana always preferred marijuana beginning in their teenage years, rather than alcohol. These findings support other research (e.g., Allen et al., 2021; Mason & Spoth, 2011) that has found that juvenile substance use predicted adult substance use.
Limitations
As with all studies, there are limitations of the present work that should be acknowledged. The NLSY97 data are based on self-report and subject to response bias (e.g. social desirability, recall) (Farrington, Loeber, Stouthamer-Loeber et al., 1996; Piquero, Macintosh, & Hickman, 2002). That said, self-reported substance use has been found to have acceptable levels of reliability and validity (Huizinga & Elliott, 1986). An advantage of self-report data is that respondents' behavior is less likely to be underestimated than when using official data sources such as arrest (Chaiken & Chaiken, 1990). Additionally for the NLSY97, so as to minimize social desirability bias, reports of sensitive behaviors were obtained via audio computer-assisted self-interviewing. As with any study, it is possible that other factors not accounted for in the present analyses (e.g., justice system involvement occurring after age 21) may account for the link between JSI in emerging adulthood and later substance use.
Conviction and incarceration variables were used as proxies for labeling theory and stigma. This is a contribution to the literature on labeling theory, as prior criminological research has often used arrest to operationalize labeling. That said, no measure perfectly encapsulates all the facets of the concept it purports to operationalize. It is possible that some individuals with past JSI did not particularly feel particularly stigmatized during their subsequent years (e.g., if they had strong family resources and ended up working a family business). The NLSY97 does not include a variable that specifically asks whether the respondent felt stigmatized by their JSI experience. There are also other sources of stigma that people encounter in life, such as filing bankruptcy, being a crime victim, or becoming known as a drug addict or alcoholic. As with any study, the choice of variables inherently faces limitations.
While group-based trajectory modeling and multinomial logistic regression may be statistically sophisticated means of testing the study’s hypotheses, the results may appear unwieldly. It is challenging to craft a coherent narrative around what the many tables show, given that there are three different types of substance use, each with five classes of use, and two different types of justice system involvement to consider.
Conclusion
Despite the limitations, this study contributes to the literature on how justice system involvement impacts substance use pathways into individuals’ thirties. The approach used for this study is interdisciplinary, drawing on both criminal justice and public health scholarship. While the criminal justice and public health disciplines draw on similar methods and datasets, the framing of problems of concern (e.g., chronic substance use) to both fields differs. The public health view of substance use focuses on sickness and healing, and opposed to what is legal versus illegal and the resulting consequences. A more common approach for criminologists is to examine substance use as a causal factor for subsequent criminality. Through an epidemiological lens, it is possible to examine the causality in reverse; that is, how involvement with the justice system affects a person’s subsequent health including their substance use.
Justice system involvement in all forms is a negative health factor that contributes to increased substance use. Taking steps to ameliorate the impact of JSI on individuals’ subsequent life and health trajectories should be an area of concern for substance use counselors – and criminologists, who tend to focus more on reduced recidivism and increased employment. Substance use is an area of concern in both fields, and collaborations between substance use, public health, and criminal justice professionals would serve affected individuals well. Policy implications of the study include enhanced substance use recovery resources for individuals that come through the justice system, beginning with juveniles. These should be offered not only in jails and prisons, but also in adult and juvenile probation offices, given the strong predictive effect of juvenile substance use.
Supplemental Material
Supplemental Material - Justice System Involvement As a Risk Factor for Substance Use Into Mid-Thirties
Supplemental Material for Justice System Involvement As a Risk Factor for Substance Use Into Mid-Thirties by Connie Hassett-Walker in Journal of Drug Issues
Footnotes
Ethical Considerations
This research was conducted in accordance with the U.S. Department of Health and Human Services regulations for the protection of human subjects, 45 CFR 46 (see https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html). Approval from the Norwich University institutional review board (IRB; IRB #00005859) was sought prior to conducting any analyses. An exemption was approved on December 4, 2020 since the NLSY97 data are de-identified and publicly available through the Bureau of Labor Statistics (BLS) website (![]() ). No consent was sought from participants, as the data are deidentified and publicly available. The chair of the Norwich University IRB is Dr. Mark Stefani,
). No consent was sought from participants, as the data are deidentified and publicly available. The chair of the Norwich University IRB is Dr. Mark Stefani,
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this study was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number P20GM103449. Its contents are solely the responsibility of the author and do not necessarily represent the official views of NIGMS, NIH, or the Vermont Biomedical Research Network (VBRN) by Christopher Francklyn.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.