
Abstract
The criminalisation of drug use and stigma create barriers to healthcare and harm reduction, limiting access due to fear of legal consequences and mistrust of health services. Queensland’s Drug Diversion Program (DDP) aims to address these issues by redirecting people into support services. This study explored the lived-living experiences of people who use drugs, assessing their perceptions of the DDP through semi-structured interviews with 30 participants (Mean age = 28, SD = 4.6; 25 men, 5 women). Key themes included: societal and familial challenges before program entry, positive reception of diversion, mixed experiences with health services, and post-program outcomes emphasising accessibility and personalisation. Findings highlight that stigma, criminalisation, and service gaps shape how participants access care. While the DDP builds trust and offers critical support, limitations in awareness and cultural responsiveness remain. Enhancing program flexibility and visibility, alongside broader reform, is key to improving outcomes.
Introduction
Drug use imposes significant economic burdens on criminal justice and public health systems (Mazerolle et al., 2020). Criminalisation, punitive drug laws, and prohibitionist approaches dominate many regions (Levine, 2003; Taylor et al., 2016; Wood & Gruenewald, 2006), creating a context where systemic barriers intersect. In many countries, drug use remains criminalised, with severe legal penalties for possession and use, even for personal consumption (Greer et al., 2022; Maher & Dixon, 2017; Piatkowski, Gibbs, & Dunn, 2024; Stevens et al., 2022). However, it is important to note that traditional law enforcement approaches, like prohibition, have shown limited effectiveness (Taylor et al., 2016) in reducing drug-related harms and may even worsen social and health outcomes (Wood & Gruenewald, 2006). For example, across Southeast Asia (Johnson & Fernquest, 2018; Raffle, 2021) and Europe (Sarang et al., 2010), punitive responses—such as mandatory detention, forced rehabilitation, and even capital punishment for drug-related offenses—create climates of fear and mistrust, making it difficult for people who use drugs to access support services. Similarly, in the United States (Provine, 2011) and Canada (Khenti, 2014), the war on drugs has disproportionately targeted marginalised communities, particularly communities of colour, through punitive drug policies that have enabled systemic racial profiling, discriminatory sentencing practices, and widespread incarceration (Daniels et al., 2021; Rosino & Hughey, 2018). These legal and structural mechanisms, including mandatory minimums and the criminalisation of minor drug offences, have deepened existing inequities and intensified surveillance and social control over racialised populations (Godkhindi et al., 2022). This is further compounded by societal stigma (Gehring et al., 2022; Haritavorn, 2014; Selfridge et al., 2020), which fuels discrimination in healthcare, employment, and housing, further marginalising people who use drugs and dissuading them from accessing available services. Stigma creates profound mistrust in health systems, with individuals fearing mistreatment or being reported to authorities (Cox et al., 2024; Muncan et al., 2020; Paquette et al., 2018). This dynamic reinforces cycles of harm by isolating people who use drugs and denying them opportunities for care and recovery. This has led to increased support for alternatives, such as police-based diversion programs that direct individuals away from the criminal justice system to social services (Bernard et al., 2020; Hayhurst et al., 2019; Hughes et al., 2019; Lindquist-Grantz et al., 2021).
Police-based diversion programs emerged in the 1990s as alternatives to incarceration for drug-related offenses, emphasising treatment and harm reduction over criminalisation (Harrison & Scarpitti, 2002). Diversion can occur at various points in the criminal justice process, with the Sequential Intercept Model outlining five key stages (Munetz & Griffin, 2006), from law enforcement encounters to community corrections. Diversion measures at the initial point of contact—during interactions between police and people who use drugs—have been adopted in an increasing number of jurisdictions (Stevens et al., 2022). Police-led diversion measures, such as Portugal’s Commission for the Dissuasion of Drug Addiction (Hughes & Stevens, 2010) and the U.S. Law Enforcement Assisted Diversion program (Clifasefi et al., 2017), have been implemented to address drug use while providing social services.
In Australia, however, people who use drugs face multiple, interlocking barriers that go well beyond legal sanctions. Only around 20% of Australians with a diagnosed substance use disorder access specialist treatment each year (Kingston et al., 2017), leaving a vast unmet need. Wait-times for outpatient alcohol and other drug services regularly are lengthy in metropolitan areas and are often unavailable in rural and remote regions (Calabria et al., 2021), where Indigenous communities may reside hundreds of kilometres from the nearest clinic (Allan, 2010). Transport costs, inflexible clinic hours, and the requirement for multiple in-person visits further exacerbate drop-out rates (Krakouer et al., 2022). Within the mainstream healthcare system, stigma is consistently reported by people who use drugs (Piatkowski, De Andrade et al., 2025), which translates into delayed referrals, withheld pain management, and punitive discharge practices. On the social services front, rigid eligibility criteria for housing support, mandatory ‘dry’ accommodation requirements, and intrusive child protection screenings deter many from seeking help, particularly women and parents (Heath et al., 2022). These systemic obstacles create a landscape in which criminal justice diversion may be the only practical access point for health and social support for people who use drugs. In this vein, we acknowledge that positive outcomes have been demonstrated alongside the implementation of drug diversion programs in various Australian jurisdictions (Hughes et al., 2019, particularly in reducing socio-structural barriers to employment and housing (Weatherburn et al., 2020). These programs have been associated with improved health outcomes and increased engagement with treatment services (Blais et al., 2022; Hayhurst et al., 2019). By diverting individuals from the criminal justice system into rehabilitation and support services, these programs help mitigate the long-term consequences of criminal records, which often hinder access to employment and stable housing.
In 2024, the Queensland Parliament enacted the Drug Diversion Program (DDP) through amendments to the Police Powers and Responsibilities Act 2000 (s. 378B), representing the state’s first statutory framework to formally redirect people found in possession of illicit substances to health, education, and social support services rather than the courts (Queensland Health, 2024). Before these reforms, discretionary police cautions or local diversion schemes varied widely across regions, often lacking consistency and clear referral pathways (Hughes & Ritter, 2008). In this paper, we use the term ‘diversion’ to refer to structured legal pathways that redirect individuals away from the criminal justice system and into health or social services after contact with police. This contrasts with ‘deflection’, commonly used in U.S. contexts, which typically involves redirection before any formal police processing or charges occur (Lindquist-Grantz et al., 2021). Eligibility is determined at the point of police contact—either on arrest or when a police officer reasonably suspects personal-use possession, and officers themselves issue a Police Diversion Notice in lieu of a court summons (Queensland Police, 2024). Individuals are eligible if they have no pending indictable charges, no prior convictions for violence or trafficking, and possess amounts deemed for personal use. This Notice functions as an official legal instrument requiring the individual to attend a DDP assessment within 28 days; failing to do so reactivates standard prosecution under section 791.
The DDP is structured as a single, mandatory 60–90 minute, face-to-face session conducted by a registered AOD clinician at designated Queensland Health clinics or co-located community health centres. There is no inpatient component; all services are outpatient and voluntary beyond the attendance requirement. The session comprises: (i) a brief health, social, and substance-use needs screening, (ii) a structured brief intervention utilising motivational interviewing techniques and education specific to the substance(s) involved. Following this, each participant receives an individualised referral plan, which may include outpatient alcohol and other drug treatment programs (e.g., counselling, group education) and mental health services (e.g., psychology referrals). All referrals are voluntary. There is no formal aftercare program mandated by the DDP statute, but the intention is that participants are connected to longer-term support via referral pathways. The DDP does not involve ongoing communication between Queensland Health clinicians and police or courts beyond the initial Notice and completion notification. On successful completion of the assessment session, demonstrated by attendance and participation, participants incur no court appearance, no formal charges, and no public criminal record (Queensland Police, 2024). Police maintain an internal diversion record but do not share ongoing reports with the courts (Queensland Police, 2024). Should a participant decline, fail to attend, or disengage from the single session, their matter is returned to standard criminal proceedings (see Figure 1). Roadmap for drug diversion program.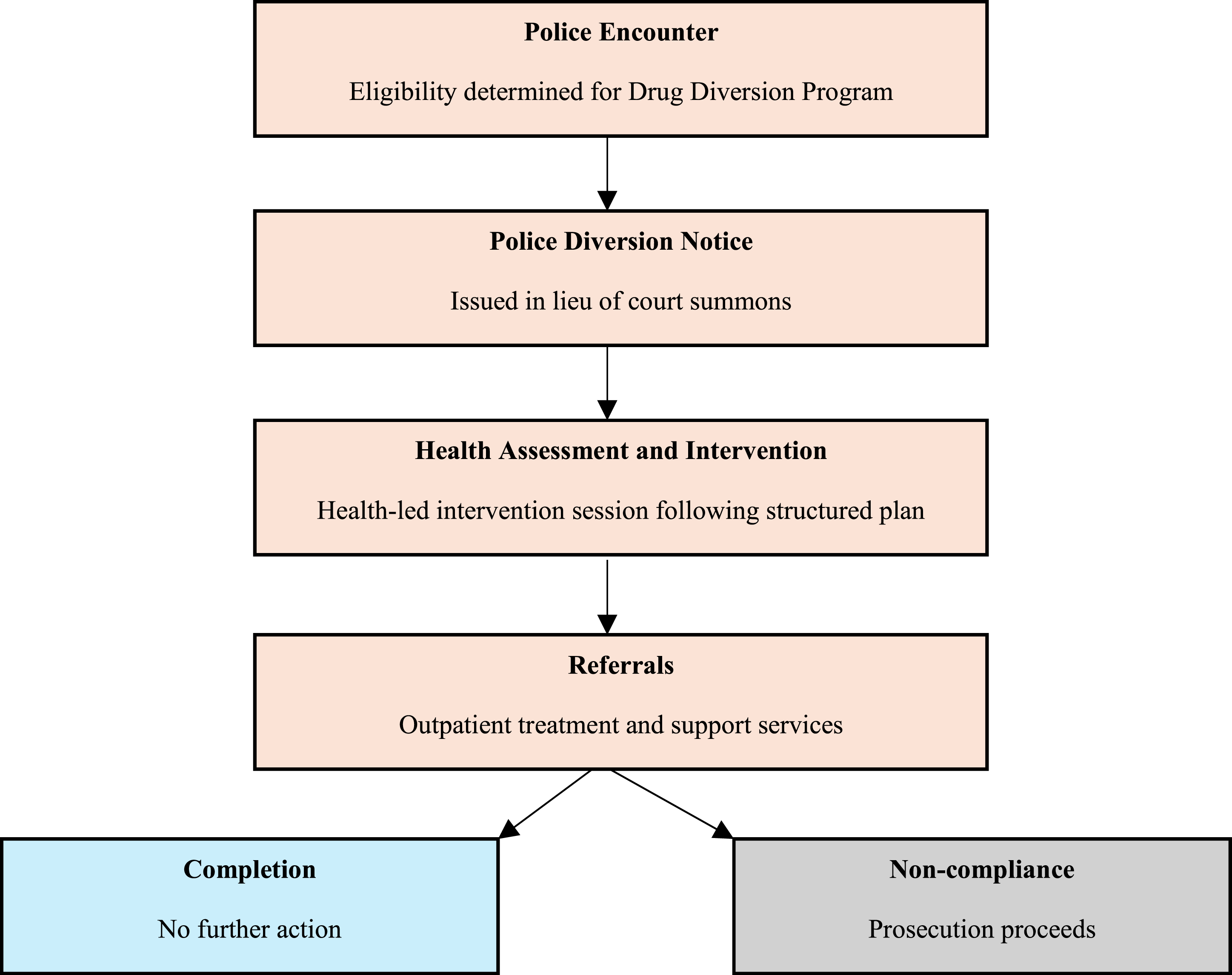
The DDP adopts a generalist harm minimisation framework, in line with Australian drug policy (Commonwealth Department of Health, 2017). The DDP’s harm minimisation content is limited to education and individualised risk conversations. These may cover mental health self-management or guidance on reducing use frequency or intensity. The limited scope reflects both the single-session design and the program’s integration within a clinical setting. Nonetheless, this approach aligns with evidence that brief interventions and early referral can reduce high-risk use patterns over time (Hayhurst et al., 2019). Despite its promise, the DDP faces significant structural challenges. For instance, service deserts in remote and regional Queensland mean many participants must travel over 100 km for assessment, incurring costs that deter uptake (Calabria et al., 2021; Clough et al., 2018). Limited culturally tailored resources constrain engagement among Aboriginal and Torres Strait Islander peoples (Krakouer et al., 2022; Lee et al., 2023) and healthcare stigma remains a barrier (Sutherland et al., 2024). To bridge policy and lived-experience, our study aimed to explore community experiences of the DDP by people who use drugs in Queensland.
A Peer-Led Approach
Throughout this paper, we refer to “lived-living experience” (LLE) as a deliberate term recognising not only past experiences of drug use but also the ongoing, dynamic nature of engagement with substance use, treatment, and social systems. This framing reflects contemporary approaches in peer-led research and service design, where ongoing use and recovery are not treated as binary categories (see Piatkowski, Seear, & Kill, 2024). Community engagement has become a cornerstone of developing equitable and inclusive harm reduction practices, healthcare policies, and research globally (Chang et al., 2019, 2021; Piatkowski, Kill, et al., 2025; Piatkowski, Seear, & Kill, 2024). Central to this approach is a commitment to participatory methods that empower individuals to influence decisions, policies, and organisational practices directly affecting their lives. For people who use drugs, engagement moves beyond consultation; it signifies a transformation toward community-driven leadership, where solutions are designed by and for those most impacted. This shift is especially evident in peer-led initiatives, which embody principles of equity, empowerment, and collaboration, centring the voices of people who use drugs to challenge systemic inequities and foster meaningful, lasting change.
At its core, being peer-led is more than including people with LLE in harm reduction efforts—it means leadership driven by those directly affected, informed by real-world expertise and community knowledge (Brown, Perry, et al., 2019; Madden & Wodak, 2014). Rooted in harm reduction and ‘drug user’ movements, peer engagement amplifies the voices of those with LLE in policymaking, service delivery, and research. It transforms harm reduction from a service delivery model into a dynamic movement grounded in trust, relatability, and practical expertise. Peers bring unique insights into drug-use environments and social networks, ensuring that programs and interventions remain relevant, acceptable, and effective within local contexts (Carl et al., 2023). This embeddedness enables peers to reduce stigma, foster open communication, and build trust (Chang et al., 2021; Elkhalifa et al., 2020) —critical components for addressing systemic barriers often encountered by current structures.
Peers have been instrumental in driving innovations such as steroid checking, hepatitis C prevention initiatives, overdose prevention strategies, and broader substance use treatment frameworks (Chen et al., 2023; Piatkowski, Coomber, et al., 2025; Silano et al., 2022). Their roles have evolved to include educators, harm reduction service providers, group facilitators, researchers, and advisory committee members (Brown, Crawford, et al., 2019; Brown et al., 2018; Piatkowski & Kill, 2024). Beyond their technical contributions, peers influence social norms within drug-using networks, foster health-promoting behaviours, and facilitate access to critical health services (Latkin et al., 2013; valentine et al., 2020). Collectively, this research demonstrates that peer-led interventions often result in increased engagement with health services, reduced stigma, and improved outcomes at both individual and community levels.
Building on this growing recognition of the value of peer engagement, our research investigates the LLE of people who use drugs in Queensland, focusing on their perceptions of the recently implemented DDP. By capturing narratives of their interactions with the program, we aimed to uncover insights into the community’s attitudes toward this policy change and its real-world implications. To achieve this, our research adopted a peer-centred, co-productive approach. We engaged in iterative, two-way conversations that positioned peers as co-researchers. Peer researchers shaped every stage of the research process—from designing the methodology to interpreting and disseminating findings. This approach ensured that the knowledge generated was not only informed by peers but also co-produced in continuous dialogue with the community, fostering a dynamic and evolving understanding of their experiences (Piatkowski, Kill, et al., 2025). The peer researchers [redacted], one of whom had been involved in previous iterations of DDP, played a key role in co-designing the methodology, collecting and analysing data, and contributing to the interpretation and dissemination of findings.
Methods
Sampling and Recruitment
This exploratory qualitative study focused on the LLE of people who use drugs who participated in Queensland’s new Drug Diversion Program (DDP), introduced in May 2024. Participants were recruited through the Queensland Injectors Voice for Advocacy and Action (QuIVAA) professional network. Eligible participants were over the age of 18, had used illicit drugs, and had been formally engaged in the Queensland DDP since its implementation. A total of 30 participants were recruited. All had participated in the program, typically following a police or court referral, with varying levels of engagement in education or treatment components depending on individual circumstances. Of the thirty participants aged between 20–38 years old (M = 28, SD = 4.6), 25 identified as men and 5 as women. All participants had engaged with the DDP. Participants received a US$40 AUD gift card in recognition of their time and expertise. This project received approval from (Redacted) University’s Human Research Ethics Committee (Approval Number: [redacted]).
Data Collection
Two interviewers (redacted) conducted the interviews. Demographic information was collected to gain an understanding of the participants but also maintain their confidentially and keep interview times at a reasonable length. The interview guide, developed by the research team and informed by existing literature and LLE, followed a semi-structured format. Semi-structured interviews were conducted to explore participants’ perceptions of Queensland’s new DDP, focusing on their experiences, challenges, and the program’s effectiveness. The interviews were recorded via videoconferencing to ensure accessibility and accommodate participants’ needs. These were approximately 25 minutes in length on average (SD = 7 minutes, range = 15–40 minutes). To deepen understanding, the interviews incorporated elements of journey mapping, capturing participants’ experiences at key stages of the program. This approach highlighted emotional responses, critical touchpoints, and the broader social, structural, and institutional factors shaping their engagement with the DDP. The interviews included questions designed to uncover participants’ understanding and experiences with the program. For instance: Can you share your understanding or experience with Queensland’s drug diversion program? Regarding the program, was the process you would have to go through clear to you? How do you perceive the effectiveness of the drug diversion program in addressing drug-related issues? Were you offered rehab or other types of counselling during the process? Were you able to access these? From your perspective, do you believe police discretion was used in your case? Did you experience any stigma or discrimination? What improvements or changes would you suggest for the drug diversion program to better meet the needs of people who use drugs? This combination of narrative inquiry and experiential mapping provided rich, layered insights into participants’ interactions with the DDP.
Data Analysis
Transcripts were analysed using NVivo (v12, QSR). For this study, data analysis employed a modified experience mapping approach (Kalbach, 2020) to explore participants’ perceptions of Queensland’s new DDP. Experience journey mapping, adapted from business service design and developmental frameworks, was used to visualise the sequential and relational aspects of participants’ interactions with the program (Joseph et al., 2020; Ly et al., 2021; Westbrook et al., 2007). This approach allowed for an in-depth understanding of their LLE, structured across various stages of engagement with the DDP.
The framework was applied to structure and contextualise participants’ accounts of their engagement with the program. This method involved mapping participant experiences across key stages: 1. Pre-program engagement (e.g., initial contact with the program and expectations), 2. Program entry (e.g., reception, orientation, and first impressions), 3. Program involvement (e.g., participation in activities, support received, and personal reflections), and 4. Post-program outcomes (e.g., perceived benefits, challenges, and takeaways).
These stages were analysed to identify recurring patterns and the socio-structural factors shaping participant experiences of the diversion process. This study did not seek to evaluate behavioural outcomes or future offending. Rather, the framework emphasised the dynamic interplay between individual actions and broader system interactions, with a focus on how participants encountered and navigated the program, and how these experiences informed their understanding of harm reduction and service access. Please see Figure 2 for a visual representation of the experiential map. Experiential Journey Map.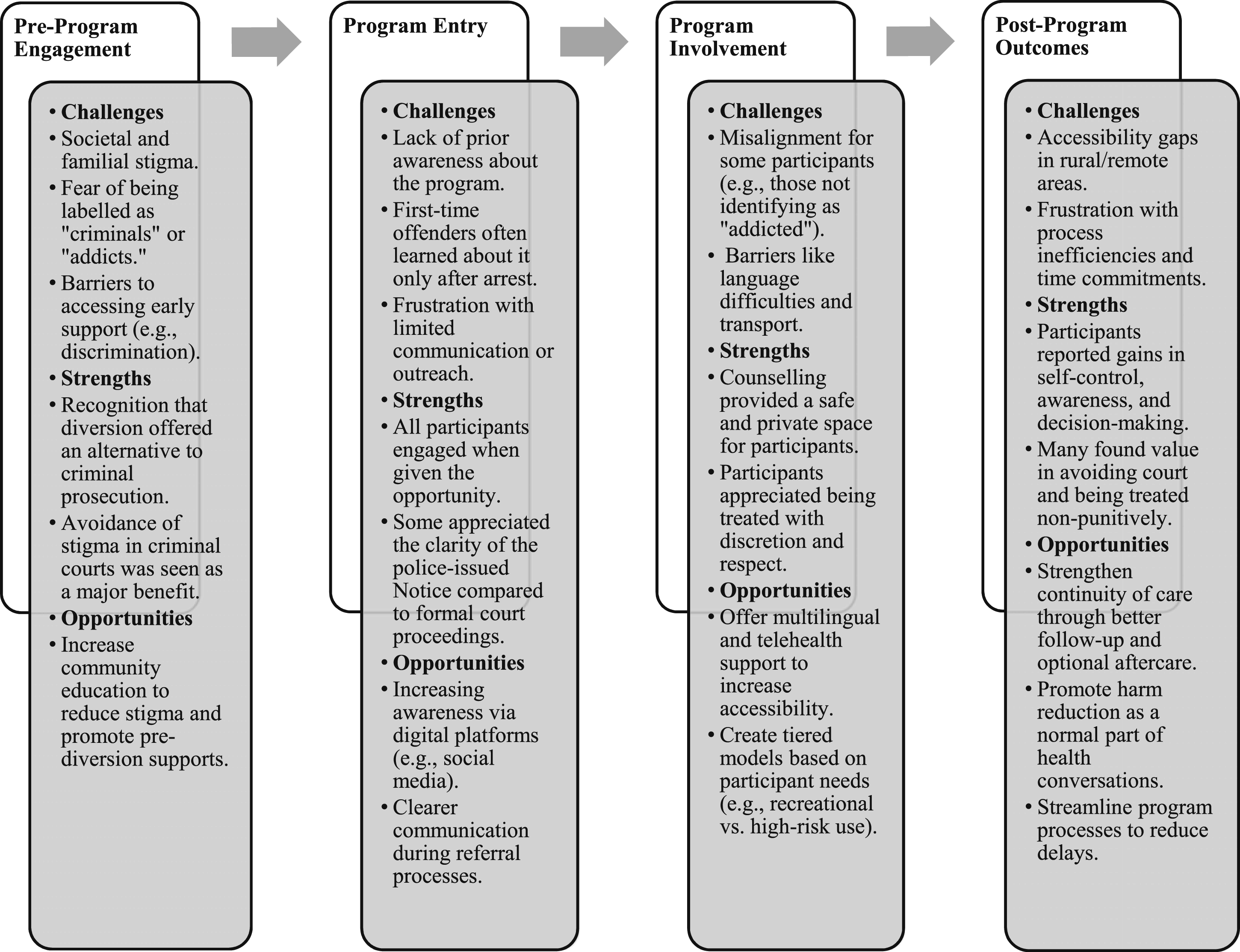
Results
Pre-program Engagement: Systemic Issues and Stigma
To understand participants’ feedback on the Drug Diversion Program DDP, it is important to first outline the circumstances that led to their involvement. All participants were referred to the DDP following a police encounter in which they were found in possession of a small quantity of an illicit substance for personal use. Rather than proceeding through the criminal courts, eligible individuals were issued a Police Diversion Notice that mandated their attendance at a single-session intervention. For many, it was their first formal interaction with health services for substance use, and it occurred in the context of criminal legal intervention.
The experiences shared by participants reveal the pervasive stigma and systemic challenges faced by people who use drugs. Stigmatisation not only affects how people perceive themselves but also influences how they are treated by society and within their communities. This stigma often manifests as discrimination from peers, law enforcement, and even family members, creating barriers to recovery and support.
Many participants recognised the stigma attached to being labelled a criminal, which can deter individuals from seeking help or entering treatment programs. At the same time, some participants attempted to distinguish their drug use from other forms of criminality. This ‘decoupling’ from this ‘criminal element’, where illicit drug use was perceived as different from other criminal offences people could be charged with. Jason (24, man): I'm not a criminal, and I've not stolen before, so it's easier to go to this than to appear in a criminal court.
Mitchell’s comment highlighted how the perception of drug users as criminals was entrenched in societal attitudes, complicating efforts for rehabilitation. This perspective could create a barrier to understanding the underlying reasons for drug use, which is crucial for effective intervention. He also pointed to how this criminal framing leads to broader misunderstandings about drug use itself and the complexity of people’s lives. Mitchell (32, man): I think illicit drug users tend to be described as criminals, and regardless of where and when we’re caught. And I think that has always had more reasons [to] come with a lot of misunderstanding.
Many participants emphasised the stigma of being labelled, which can create a sense where people feel less-than. This negative labelling was a significant systemic issue that could hinder individuals’ motivation to seek help. Aaron’s reflection also highlights how these labels persist even during recovery, shaping how people are treated and how they view themselves. Aaron (28, man): Most times you get seen as an addict (sic). And you just think it’s as an individual who's beyond recovery, you know and sometimes judgment during recovery. So, there’s been a lot of negative labels […] It makes a massive difference, and those labels sit with you.
Several participants also highlighted the role of familial expectations in exacerbating feelings of shame and stigma. While stigma was not always experienced among peers, especially where drug use was normalised within social circles, family contexts often presented a more difficult terrain. Albert described feeling a sense of stigma rooted in the fear of disappointing his family, even in the absence of explicit discrimination. Interviewer: Did you experience any stigma and or discrimination? Albert (30, man): When we say stigma, I'll say not really to friends. Cause most of my circle then were also into drugs. But to my family. I would say yes, I got a bit of that stigma, and though not discrimination, but the stigma because you know a family expects much from you. And you know, when your family does not know you do drugs, it will be very disappointing and embarrassing to them.
These participants also highlighted the benefit of the DDP in avoiding stigma with families and in their communities by not going through the criminal courts. Rowan (30, man): I think it [drug diversion program] has helped more, in avoiding the stigma […] there have been a lot of situations where people who often see us as offenders, you know, for drug possessions, and most times, first time offenders get treated differently, get treated badly in communities and societies.
Rowan’s quote reflects the protective function of DPP, by keeping people out of court and away from formal criminal records, the program reduces community and familial stigma. Programs aimed at drug diversion must address these systemic issues to create an environment that fosters understanding, support, and effective treatment, which this program presented some evidence of having done. David (27, man): They did use discretion. In the area of the officers cause you’re doing your job right? I will give you credit to them. Alright because, they did a job […] they did their job perfectly and I would say they did it with utmost discretion. They handled the matter in such, in such discretion that like without saying OK it's OK it's fine [to use drugs] alright.
The program discussed in these interviews seeks to mitigate the stigma associated with drug use by providing a supportive environment focused on providing information and options rather than punishment. By emphasising health services, counselling, and education, the program aims to offer individuals the tools necessary to make informed decisions around their drug use. Moreover, fostering a community that recognised and addresses the systemic issues surrounding drug use can help shift perceptions and reduce stigma, ultimately leading to better outcomes for participants. This holistic approach not only supports individual recovery but also contributes to broader societal change in how people who use drugs are viewed and treated.
Program Entry: Awareness and Engagement with the Drug Diversion Program
Before their referral, most participants had no awareness of how the DDP operated. Despite this initial unfamiliarity, all participants engaged with the program once it was offered to them. Entry typically occurred after a police encounter related to personal possession of an illicit substance, where officers issued a formal Diversion Notice in lieu of court proceedings. This legal mechanism required attendance at a single-session intervention with a health professional. Many participants had no prior understanding of the DDP until they were directly involved in it. Interviewer: Did you have an understanding of the changes in laws before they occurred? Albert (30, man): Not at all. Interviewer: So you found out once the drug diversion program was sort of offered to you? Albert (30, man): Yeah
This revealed a gap in awareness about available alternatives to criminal prosecution for people who use drugs. However, we note many participants found diversion to be a salient and viable option for them moving forward. Albert (30, man): I was caught with drugs with my friends like I told you on our way back from the club [..] just that once. Well, I've been taking drugs, but I've never been caught […] So and I think through [the] Drug Diversion program I came to self-realisation of, you know, I just had to collect my past life and had to make a new decision for myself.
There were many personal narratives of ‘first-time offenders’ who, despite prior drug use, only learned about the DDP after being apprehended. It underscored the notion that drug-related offenses regularly go unnoticed until legal intervention, pointing to an opportunity for earlier engagement with harm reduction initiatives rather than post-offense involvement.
Many participants frequently expressed frustration with the lack of easily accessible information regarding drug diversion programs. This highlights the need for a more robust dissemination strategy, particularly utilising social media and digital platforms to reach a wider audience. Increasing accessibility and visibility of such programs could encourage participation and improve outcomes. Morris (28, man): I think there should be [better] access to the information, on social media platforms, and in emails. Because most people they wish they have information about the drug diversion program easily but, sometimes they lack access to such information. Maybe information could provided on social media or emails. I think it will go [a] long way.
The referral process was seen as a critical point of engagement, where people are assessed based on their drug use history and criminal record. This structured process could effectively divert individuals from the criminal justice system into therapeutic programs, provided the eligibility criteria are clear and consistently applied. Jesse (25, man): I've been using cocaine for a period of time and stopping it… It felt like I like this […] It was like a struggle for me. I think the first step I had to go with was I was assessed by the police officer. And then they checked my drug history and my criminal history. And then they deemed me [fit] to participate. That's when I received a referral. When I was referred to the programme, they told me the basics I needed to know. What it entails. What I would stand to benefit from the programme and what I if I fail to comply with the programme, what would await me. The paths that I would have to face. So, with that knowledge. I consented.
Overall, the reception of the DDP was positive. A majority of participants expressed an understanding of the clear benefits offered by the program, including an alternative to punitive measures. The structured environment, coupled with the emphasis on personal development and privacy, made diversion programs an attractive alternative for many individuals. Similarly, another participant expressed relief at the opportunity to avoid a harsh penal system while receiving treatment marked a crucial point of intervention. Edward (24, man): 100% better. Extremely better. There’s really no one who would rather go through the courts... nobody likes going there.
This collectively highlighted how diversion programs present a viable route for participants to access care and avoid the punitive nature of jail time, with its long-term social consequences. Overall, the reception of the diversion programs was positive. Several participants expressed appreciation for the privacy, support, and rehabilitation opportunities they offered. Virginia (26, woman): The effectiveness of the programme, I'll say it's effectiveness is quite good, I mean. Look at me after getting the services, I can actually abstain for four weeks without taking drugs. I see that as effective because it's something I could not […] I could not go without doing. After getting the services from the program have actually […] I can say I have self-control in regard to drugs.
There was a clear consensus amongst participants that these programs provided a better alternative to the criminal justice system, allowing people to have an honest relationship with their substance use in an environment which respected their human rights.
Program Involvement: Wrap-Around Supports
All participants attended the required session with a clinician, as mandated by the DDP. During this session, they received brief education and counselling tailored to their substance use, as well as optional referrals to additional supports, such as drug and alcohol counselling, mental health services, or peer-led programs.
Several participants highlighted both the positive aspects and limitations of their experience with some of the health supports offered to people who were diverted from punitive measures, for example counselling. Martha suggested that when counselling was tailored to her specific patterns of use and personal circumstances, it was more meaningful and potentially more impactful. She emphasised the value of one-on-one sessions that went beyond surface-level engagement to focus on underlying issues, coping strategies, and the broader context of her drug use. Interviewer: Were you offered other types of counselling during the process? Martha (32, woman): We were offered counselling. I mean that kind of aligned with tackling some of the issues […] Like one on one sessions that focus on specifics of usage issues an personal challenges, coping and strategies.
Participants, such as Jason, suggested that counselling provided them with a safe space to express emotions that they had previously struggled to articulate. Jason (24 man): It really, helped because it helped me to open up to people, I was finally able to express my emotions. It allows you to open up to someone while you were there.
Similarly, Virginia emphasised the privacy and confidentiality of the diversion experience, comparing it favourably to the more public and stressful experience of going to court. She appreciated the therapeutic space where her story remained private, unlike in the courtroom where her personal history became public knowledge. Virginia (26, woman): Everything I told the counsellor was just between me and her. I would say kind of better than going to court.
Further, many participants recounted the approach of the services provided as being generally supportive, emphasising the structured nature of the diversion program.
Some participants emphasised the importance of feeling safe in the counselling space. They appreciated that this process circumvented the otherwise hostile and stigmatising environment and were not judged or made to feel like a ‘criminal’, allowing them to be open about their drug use without fear of legal consequences and, subsequently address the factors involved in problematic use. The initial fear of being arrested or exposed highlights the stigma and fear often associated with seeking help, but participants ultimately found comfort in the counselling environment. Dennis (28, man): This connection that you have someone that you can explain all of what you're going through, and you feel you're safe. So, you no one's blackmailing you or no, no one is rubbing it at your face that you're a bad person, or that you do something illegal, and you the law enforcement might be against you. So, the space was a lot more free, for me to disclose some [things] that I've done related to drugs, and I was feeling safe.
Some participants did describe some challenges encountered, for example, due to language and transportation barriers. The participant’s strong accent created communication difficulties with the healthcare provider. Scott described how his accent created communication difficulties with a healthcare provider, which left him feeling misunderstood and unsupported. This highlights the need for culturally responsive service delivery that takes into account linguistic diversity and communication styles, particularly in programs designed to support people from a range of backgrounds. Without such considerations, participants may feel excluded or alienated, reducing the effectiveness of interventions (see Lee et al., 2023). Scott (25, man): But the only difficult [part] was communication barriers, because I'm black. And I kind of have this kind of strong accent. So, the health provider, it [was] kind of hard for him to understand me. So that was there was a challenge that I really faced because of my language barrier.
There was also a potential misalignment between the support offered and peoples’ needs, as they did not identify as someone struggling with drug addiction. David (27, man): I was offered the counselling where they said that was also part of the program. But I'm not kind of addicted to weed, I'm not even into drugs. Greyson (23, man): I felt like I wasted some people time, as I only smoke weed and will smoke weed after and it does not impact on my or other’s life.
This indicates that the program may benefit from a more tailored, needs-based approach to counselling, focusing on the individual’s specific circumstances rather than applying a standard intervention to all participants. For example, a harm reduction approach, equipping people with information regarding safer use could be considered.
Post-program Outcomes: Improvements and Supports
After completing the program, many participants reflected positively on certain aspects of the experience, particularly when they felt respected and not judged. Several noted shifts in their understanding of substance use or a renewed willingness to seek help. However, participants also identified gaps and areas for improvement. For example, some participants emphasised that accessibility remains a significant issue. There is a lack of awareness and service availability in remote areas, which could deter willing participants from accessing the program. Martha (32, woman): I have a lot of improvements like I wanna talk about... The program was good, but boy, it's we should ensure that, services and resources could be readily available in all areas and also particularly in the remote.
Furthermore, a number of participants highlighted the need for a more personalised approach that considers individual circumstances, including diverse cultural backgrounds and personal health challenges. Martha (32, woman): I'd also say that you know, I believe that different people like myself, we have needs, we have different people with different needs. This program could benefit from a more personalised plan where they're taking into account maybe the unique circumstances of each person, including the diverse cultural backgrounds.
They also advocated for increased accessibility through language support and telehealth services to reduce barriers for diverse and vulnerable populations. Aaron (28, man): And we also have the language support. And I do know that I do know that people providing mostly English resources, you know, like interpreters, you know full known English speakers as well, you know. And that will. That will make the program more accessible, you know, in a more diverse community.
Many participants articulated the importance of education and awareness to ensure that people, especially first-time offenders, are informed about the DDP and the support it offers. Aaron (28, man): Yeah, you know, I think people understand more about something, when as when they’ve been introduced to it a little bit more and deeply. So yeah, so they have more wider understanding. And they're more aware about on this writing and more aware about the program. And they’re just aware about what the program holds, but also way about the improvements and the importance of this program. The engagement in this program, the results in this program. So I think just knowing a lot about that and pushing this out into the communities would be more helpful.
Several participants also placed an emphasis on producing more harm reduction focused elements. Rather than relying solely on abstinence-based or punitive frameworks, they advocated for services that acknowledge continued use and offer practical, non-judgmental support. Douglas, for example, highlighted the importance of embedding harm reduction into these programs, not just for those with more complex needs, but also for individuals facing minor charges or continuing to use drugs. Douglas (35, man): I'd love to add something to that [...] that you have certain programs, you know, that focuses more on harm reduction […] You know to have harm reduction services for, you know, individuals who continue to use drugs, and for low level offenders as well.
There were also participants, such as David, who expressed frustration with the length of the process and its interference with their personal responsibilities. David (27, man): It wasted a lot of my time because what I wanted to be doing at that particular period I had to, I had to postpone it. ‘Cause I was detained for quite a long time.
His comments reflect how, despite the non-punitive intentions of the diversion program, the logistics and procedural delays still had disruptive effects on participants’ lives. This highlights the need for the diversion process to be more efficient, minimising unnecessary delays and respecting participants’ time. David (27, man): I thought I was going to stay there for like a 15–30 minutes. And then I wasn't given proper explanation of the facts and the intensity of it was as if they could be more open and transparent and stuff like that. OK, that would be great.
Streamlining procedures, such as simplifying referral processes, reducing wait times, and improving communication, could reduce the program’s perceived burden and improve uptake and outcomes for people.
Discussion
Our analysis indicates that the DDP provides more direct and supportive relief to people who use drugs by offering a confidential space to address drug consumption and reduce criminalisation. Participants consistently emphasised that the DDP diverted them away from criminal charges in practical and meaningful ways, avoiding court processes and the long-term consequences of a criminal record. In this sense, the Program was largely successful in achieving its core aim: offering an alternative to prosecution that facilitates engagement with health and support services. The DDP demonstrates its capacity to foster trust, build capacity in under-resourced health services, and empower communities to mitigate some of the adverse impacts of stigma and punitive policies.
The participants frequently acknowledged the DDP’s ability to reframe their identity away from the ‘criminalised archetype’ of addict (Fomiatti et al., 2022; Fraser et al., 2017). For many, this decoupling from criminalisation allowed for reduced social stigma within their families and communities, enabling a more positive self-concept. The counselling services offered through the DDP were identified as a critical point of support for many participants. The therapeutic environment provided a safe space for individuals to reflect on their substance use without fear of judgment or legal repercussions. This aligns with broader evidence suggesting that non-stigmatising, confidential care is key to fostering engagement and long-term positive outcomes for people who use drugs (Francia et al., 2023). However, it is important to note that some participants questioned the assumption that intervention was necessary, particularly if they did not view their drug use as problematic. This highlights a potential tension between public health aims and individual perceptions, and reinforces the need for more flexible, person-centred approaches.
Participants also offered suggestions to improve the Program’s reach and relevance. Some described challenges around access, particularly in rural and regional areas. Others noted a mismatch between the DDP’s standardised content and their LLE. These findings suggest several opportunities for refinement: expanding telehealth delivery, improving interpreter access, and adapting content to reflect the specific needs of different cultural and social groups. For participants who did not see themselves as needing treatment, a shift away from mandatory ‘intervention’ language toward collaborative health conversations may enhance engagement. Incorporating harm reduction strategies such as safer use information and attention to social determinants of health could improve both relevance and acceptability. Challenges such as language barriers and accessibility limitations were noted, particularly for participants from diverse cultural backgrounds or rural areas (see Lee et al., 2023).
Our analysis also reveals that the DDP is not designed to serve as a comprehensive substitute for systemic reform but rather as a targeted intervention aimed at partially mitigating the harmful effects of current punitive frameworks (Piatkowski & Kill, 2024; Piatkowski, Kill, et al., 2025). While the DDP offers a valuable diversion from criminal charges, its impact is necessarily limited, benefiting a proportion of individuals per instance of criminalisation. This limitation highlights that the DDP functions as a reactive measure to address the immediate consequences of a system that continues to stigmatise and marginalise people who use drugs, rather than transforming the underlying structural conditions that impede access to care. Moreover, our results indicate that the DDP cannot, on its own, overcome the broader institutional challenges, including inadequate healthcare provision and persistent negative perceptions among medical professionals (Cox et al., 2024; Rehman et al., 2024), that perpetuate harm. Instead, these findings highlight the need for a dual strategy that pairs targeted harm reduction with broader policy reform. Future research could usefully explore how programs like the DDP interface with wider systemic barriers, such as housing insecurity, service fragmentation, and ongoing criminalisation—that affect participant outcomes post-diversion. Longitudinal studies tracking recidivism, service uptake, and health outcomes following DDP participation would also be valuable.
Our community’s narratives serve as a reminder of how pervasive stigma, compounded by systems of criminalisation and under-resourced health services, limits access to care and entrenches cycles of marginalisation (Selfridge et al., 2020). Stigma manifests itself across multiple dimensions. It shapes self-perceptions, influences interpersonal relationships, and reinforces societal attitudes (Fomiatti et al., 2022) and, thus, poses significant barriers to seeking help (Treloar et al., 2013). These barriers are often amplified by criminalisation and prohibitionist drug policies, which perpetuate fear, discrimination, and punitive legal consequences for people who use drugs. Nevertheless, the community narratives have illustrated one step toward mitigating stigma by diverting people from punitive systems into environments centred on empathy, care, and harm reduction. However, the entrenched stigma participants described underscores a need for systemic cultural shifts that go beyond the program itself. We think it pertinent to remind our audience that the narratives emphasise the need for both structural and systemic reforms, including the decriminalisation of drug use and investment in harm reduction services, to address the drivers of stigma and criminalisation. Without such changes, the ability of any programs to deliver meaningful, sustained harm reduction will remain constrained by broader socio-political barriers. Broader public education initiatives, as well as institutional training for law enforcement and healthcare providers, may help challenge harmful stereotypes surrounding drug use and those affected.
Limitations
While this research offers valuable insights, there are limitations to consider. One key limitation is the lack of detailed contextual information about participants’ broader life circumstances, such as the strength of their social support networks, housing stability, or prior contact with treatment services, prior to entry into the DDP. These contextual factors likely shape how participants experience diversion and whether they are able to benefit from the program. For example, those with stronger family or community supports may have been better positioned to follow through with referrals or implement behavioural changes. Another limitation relates to the DDP’s eligibility criteria and the diverse needs of its participants. For instance, some people in the current study who were diverted for cannabis possession, and who did not identify their use as problematic, reported frustration or disengagement with the service. This raises important questions about the appropriateness of a single-session, clinical model for people whose needs may not be health-related or who do not experience harms from their substance use. The program may therefore be better suited to individuals with greater or more complex health and social needs, whereas low-level recreational users might benefit more from alternate forms of diversion, such as education-only models, peer-led brief interventions, or civil de-penalisation pathways (see Stevens et al., 2022).
These issues also reflect broader concerns about the degree to which the intervention is tailored to the diverse realities of people who use drugs. While some participants found the session helpful and validating, others felt it was generic and failed to address their specific circumstances. This misalignment between service design and client need may limit the long-term efficacy of drug diversion programs, especially if it discourages future help-seeking. A key consideration when interpreting these findings is that, while the DDP aims to divert people away from prosecution, some participants may ultimately face legal consequences due to non-compliance with program requirements. This highlights that diversion programs operate within a broader punitive legal framework, where not all individuals successfully avoid prosecution. Understanding the experiences and outcomes of those who do not complete diversion is important for assessing the program’s overall effectiveness and equity. Future research should prioritise more inclusive and intersectional data collection to better understand the diverse needs of this community and enhance the applicability of harm reduction approaches. It should also explore stratified outcomes based on pre-existing life circumstances, patterns of drug use, and readiness for support to determine who benefits most from this kind of intervention, and whether alternate models are needed for priority populations.
Conclusions
This study highlights how peoples’ perceptions of the drug diversion program, particularly regarding privacy, support, and reduced criminalisation, can be transformative in fostering greater engagement with care-oriented services. Participants’ appreciation of the program challenges prevailing punitive approaches and underscores the importance of diversionary models that prioritise respect and confidentiality. These narratives suggest that such programs may serve as a critical starting point for reducing stigma and rebuilding trust between people who use drugs and the systems designed to support them. While this study reflects client perspectives, the findings point to the potential for diversion programs to catalyse shifts in broader societal and systemic responses, moving away from punishment toward compassionate, harm reduction-focused care. Achieving this vision requires sustained investment and collaboration among policymakers, healthcare providers, and community organisations to co-design inclusive and adaptive programs that address both individual and structural drivers of harm.
Footnotes
Acknowledgements
We are immensely grateful to the participants of the study for sharing their experiences with us. Thank you to the Peers who continually offer and provide a safe space for our community.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Emma Kill is the CEO of Queensland Injectors Voice for Advocacy and Action [QuIVAA], and Dr. Piatkowski is a Director on the Board the organisation. QuIVAA is a non-government owned and not-for-profit ‘Drug-User Organisation’.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Queensland Injectors Voice for Advocacy and Action [QuIVAA] who provided funding for participant reimbursement.
Ethical Statement
Data Availability Statement
Data available from corresponding author on reasonable request.