
Abstract
Contingency management is an effective behavioral intervention for treating substance use disorders that provides patients with incentives for objective verification of completed targeted recovery behaviors including abstinence from substances, attending treatment, and medication adherence. Accredited/licensed opioid treatment programs provide effective, medications for opioid use disorder. This study evaluated the prevalence of frequent contingency management use among a national sample of opioid treatment programs in the U.S. (N = 672). A binary logistic regression model examined factors associated with providing contingency management, including state-level fatal overdoses, number of pharmacotherapies, outpatient treatment, facility ownership, and residential treatment. Most evaluated facilities provided contingency management (n = 440; 65.5%). Facilities that prescribed more pharmacotherapies, were located in states with high drug overdose death rates, and for-profit (compared to nonprofit) providers were more likely to offer contingency management. Because contingency management effectively treats substance use disorders, contingency management should be offered more broadly across opioid treatment programs.
Keywords
Introduction
The unprecedented number of drug overdoses occurring yearly in the U.S. underlines the public health impact of high-risk substance use (Centers for Disease Control and Prevention [CDC], 2022) and substance use disorders (SUDs; Substance Abuse and Mental Health Services Administration [SAMHSA], 2022). From 1999 to 2020, more than 930,000 individuals have died from a fatal overdose in the U.S. (Hedegaard et al., 2021; National Institute on Drug Abuse [NIDA], 2023). Today, the primary driver of these overdoses is opioids, which were involved in nearly 75% of fatal overdoses in 2020 (Hedegaard et al., 2021; NIDA, 2023). Effectively treating opioid use disorders (OUDs) is thus necessary to save lives and improve the well-being of individuals nationwide (Stringfellow et al., 2022; Wakeman et al., 2020). Encouragingly, findings indicate that combining evidenced-based medications and behavioral interventions to treat OUDs may provide more treatment benefits than either intervention alone (Bolívar et al., 2021; Griffith et al., 2000). However, it is also worth noting that among individuals with lower complexity OUD, evidenced-based medications alone, absent behavioral interventions, have provided effective treatment (Fiellin et al., 2006).
Opioid treatment programs (OTPs) exemplify the benefits of combining evidenced-based medications and behavioral intervention treatment elements. Namely, OTPs are treatment facilities that, in addition to providing counseling and behavioral therapy, are accredited or licensed to provide medications for opioid use disorder (MOUD), such as methadone, buprenorphine, or naltrexone (SAMHSA, 2023). A prominent behavioral intervention often used to treat SUDs is contingency management (Brown & DeFulio, 2020): an evidence-based intervention with an extensive body of research evidence supporting its effectiveness across a variety of populations and therapeutic outcomes (Benishek et al., 2014; Brown & DeFulio, 2020; Davis et al., 2016; Dutra et al., 2008; Getty et al., 2019; Griffith et al., 2000; Higgins et al., 2011; Lussier et al., 2006; Prendergast et al., 2006). Contingency management views drug use as biologically normal operant behavior that is maintained by the reinforcing consequences of drug self-administration (Bigelow & Silverman, 1999; Schuster & Thompson, 1969). From this perspective, the feature that makes SUDs so difficult to treat is that drug self-administration provides potent, drug-specific consequences shortly (nearly immediately) after administration, and these consequences can be produced reliably via self-administration as frequently as an individual desires. Contingency management works by providing a competing reinforcer (e.g., an incentive of monetary value) for behavior that is incompatible with substance use (e.g., providing drug-negative urine samples) or for behavior that may support recovery (e.g., OUD medication adherence). Over the years, researchers have found that contingency management procedures that provide high-quality consequences (e.g., high-magnitude incentives; Dallery et al., 2001) shortly after evidence of drug abstinence tend to have the greatest therapeutic effect when treating SUDs (Lussier et al., 2006; Silverman et al., 2023).
At the most basic level, contingency management procedures incentivize behavior that is incompatible with drug use; however, they can also be embedded within other procedures aimed to produce therapeutic outcomes for individuals at high risk of health-related harms. For example, contingency management has been leveraged to increase adherence to HIV medication regimens (Silverman, Holtyn, Rodewald et al., 2019) and engagement with weight-loss (John et al., 2011) and cardiac rehabilitation (Gaalema et al., 2019) programs. Contingency management procedures have also been embedded in employment-based reinforcement procedures to promote job readiness skills (Koffarnus et al., 2013) and work in university-based (Silverman et al., 2001) and community-based (Holtyn et al., 2020) jobs. In a recent randomized controlled trial, Holtyn et al. (2020) arranged a version of contingency management (called abstinence contingent wage supplements) to encourage abstinence from opiates and cocaine and promote employment among unemployed adults with OUDs and lower socioeconomic status. Findings showed that beyond helping participants maintain their abstinence from the targeted drugs and gain employment, the intervention also helped participants improve their socioeconomic status. Whether applied in isolation or in combination with other therapeutic interventions, contingency management procedures have a demonstrable potential to benefit populations who need additional support in their recovery from SUDs (Silverman, Holtyn, & Toegel, 2019).
Considering the effectiveness of contingency management interventions in assisting people achieve treatment-related goals, it is recommended as an adjunctive intervention in OTPs (Bolívar et al., 2021; Griffith et al., 2000; Scott et al., 2021). Additionally, contingency management is particularly effective in treating stimulant use disorders (Bentzley et al., 2021; Brown & DeFulio, 2020). Given that stimulants and opioids are often co-used (Choi et al., 2022; Gladden et al., 2019; Palamar et al., 2020; Rawson et al., 2023; Strickland et al., 2021; Ware et al., 2021) and co-involved in overdose fatalities (Hedegaard et al., 2021; NIDA, 2023; Palis et al., 2022), contingency management interventions may be particularly useful within programs already treating populations with OUDs.
Because of the potential utility of contingency management in programs that treat populations with OUD, the present study examined a national sample of U.S. OTPs that treat persons with OUD and co-occurring SUDs to identify whether they frequently use contingency management as part of their provided services. We examined facility-level characteristics—namely, the fatal drug overdose death rate of the facility’s state, ownership (facility profit status), outpatient treatment availability, and residential treatment availability—as factors potentially associated with an OTP’s likelihood of providing contingency management. We further examined state-level data to identify the number of OTPs in each state and calculate state-level proportions of OTPs that frequently use contingency management.
Methods
Datasets
Data from two publicly available sources were used for these analyses: 2020 Drug Overdose Death Rates from the Centers for Disease Control and Prevention (CDC, 2023), and the National Survey of Substance Abuse Treatment Services, 2020 (N-SSATS) from the Substance Abuse and Mental Health Services Administration (SAMHSA, 2021). The 2020 Drug Overdose Death Rates lists state-level counts, age-adjusted rates, and rate ranges of drug overdoses in the U.S. in 2020; these drug overdose rates are per 100,000 and are compiled using death data for a 12-month period (CDC, 2023). N-SSATS 2020 is an annual census of SUD treatment providers in the U.S. that describes the characteristics, locations, and services offered by these providers in 2020 (SAMHSA, 2021). SUD treatment providers completed the N-SSATS survey by mail, phone, or online to describe their organization (e.g., its profit status) and services provided (e.g., pharmacotherapies and behavioral interventions to treat SUD; SAMHSA, 2021).
Sample Selection
The sample of facilities was identified using N-SSATS 2020 (SAMHSA, 2021) with the following selection criteria: (a) the facility offers SUD treatment (some facilities may only provide screening or referral services); (b) the facility operates an OTP; (c) the facility does not only treat persons with OUD (allowing for the possibility for individuals with co-occurring SUDs to receive treatment); (d) the facility is based in the U.S. (excluding territories); and (e) the facility has an answer (Yes/No) to the outcome, the contingency management measure. After applying the sample selection criteria, 672 OTPs were included in the analyses.
Measures
Measures used in this study included: (a) contingency management, (b) contingency management or community reinforcement plus vouchers, (c) drug overdose death rate range, (d) geographic location, (e) number of pharmacotherapies, (f) outpatient treatment, (g) ownership, and (h) residential treatment. The drug overdose death rate measure was captured from the 2020 Drug Overdose Death Rates data (CDC, 2023); remaining measures were captured from N-SSATS 2020 (SAMHSA, 2021). Independent variables were selected to examine the context of state-level overdose data, treatment levels of care, and facility profit status as potential factors associated with the provision of contingency management. The following subsections further describe each variable.
Contingency Management
This item was captured from the “CONMGMT” variable in N-SSATS 2020. This variable had binary (Yes/No) responses to “Facility frequently uses contingency management” (SAMHSA, 2021). This variable was used as an outcome in our binary logistic regression model.
Contingency Management or Community Reinforcement Plus Vouchers
This item was captured from the “CONMMGMT” and “CRVOUCHER” variables in N-SSATS 2020. The CONMGMT variable is described in the previous subsection. In N-SSATS 2020, the “CRVOUCHER” variable has binary (Yes/No) responses to “Facility frequently uses community reinforcement plus vouchers” (SAMHSA, 2021). Our a priori coding plan was to create a four-level variable: (1) No contingency management or community reinforcement plus vouchers; (2) Contingency management only; (3) Community reinforcement plus vouchers; and (4) Contingency management or community reinforcement plus vouchers. However, only n = 8 facilities only offered community reinforcement plus vouchers without contingency management, meaning that using this planned four-level variable as an outcome in a multinomial logistic regression model would be suboptimal. Therefore, for the purpose of our analyses, we created a two-level (i.e., 1 = Yes; 2 = No) variable that indicated if the facility frequently offered contingency management or community reinforcement plus vouchers. This variable was used as an outcome in a binary logistic regression model.
Drug Overdose Death Rate Range: State Level
This item was captured from the 2020 Drug Overdose Death Rates data to identify age-adjusted drug overdose mortality rates. The age adjusted range categories in the dataset are “6.9 to 11.0,” “11.1 to 13.5,” “13.6 to 16.0,” “16.1 to 18.5,” “18.6 to 21.0,” and “21.0 to 82.0” (CDC, 2023). This coding only included one state (South Dakota) in the 6.9 to 11.0 rate range and only one state (Nebraska) in the 11.1 to 13.5 rate range. To account for two separate categories only having n = 1 at the state level, this variable was recoded from six categories to the following three categories: (a) 10.3 to 24.51 (n = 21 states), (b) 24.52 to 38.72 (n = 18 states), and (c) 38.74 to 81.4 (n = 11 states and the District of Columbia). This variable was used as an independent variable in two binary logistic regression models with 10.3–24.51 as the reference group.
Geographic Location
Using the “STATE” variable in N-SSATS 2020, facilities were identified as being in one of the four U.S. Census regions (SAMHSA, 2021): Northeast, Midwest, South, and West. The geographic location of the facilities was described by visually plotting them on state-level figures containing all 50 U.S. states and the District of Columbia. The region variable was used to describe the sample. Neither the region nor the state variable were used in the logistic regression models because of the potential for collinearity with the Drug Overdose Death Rate Range variable.
Number of Pharmacotherapies
This item was captured from the “PHARMACOTHERAPIES” variable in N-SSATS 2020. This continuous variable had a possible value range of 0–16 as a response to “Number of pharmacotherapies offered by this facility” (SAMHSA, 2021). This variable was used as an independent variable in the two binary logistic regression models.
Outpatient Treatment
This item was captured from the “CTYPE1” variable in N-SSATS 2020. This variable contains Yes/No responses to “Facility offers any outpatient substance abuse service” (SAMHSA, 2021). This variable was used as an independent variable in two binary logistic regression models, with No as the reference group.
Ownership
The item was captured from the “OWNERSHP” variable in N-SSATS 2020. This variable records the “Organization that operates the facility” and has six responses: (a) private for-profit organization, (b) private non-profit organization, (c) state government, (d) local, county, or community government, (e) tribal government, and (f) federal government (SAMHSA, 2021). For the purposes of this study, response options were recoded to 1 = for-profit, 2 = government, and 3 = non-profit. This variable was used as an independent variable in two binary logistic regression models, with non-profit as the reference group.
Residential Treatment
This item was captured from the “CTYPE7” variable in N-SSATS 2020. This variable has Yes/No responses to “Facility offers non-hospital residential treatment services” (SAMHSA, 2021). This variable was used as an independent variable in two binary logistic regression models, with No as the reference group.
Analyses
IBM SPSS Version 28.0 was used to conduct all statistical analyses (IBM Corp, 2021). Descriptive statistics were used to identify characteristics of the sample of OTPs in this study. Two multivariate binary logistic regression models were conducted, with model 1 examining the outcome of contingency management and model 2 examining the outcome of contingency management or community reinforcement plus vouchers. State-level data regarding the number of OTPs and the percentage of OTPs offering contingency management were plotted using R (R Core Team, 2022) with the rgdal (Bivand et al., 2023) and rgeos (Bivand & Rundel, 2023) packages.
Results
Description of Opioid Treatment Programs
Opioid Treatment Program (OTP) Facility Characteristics.
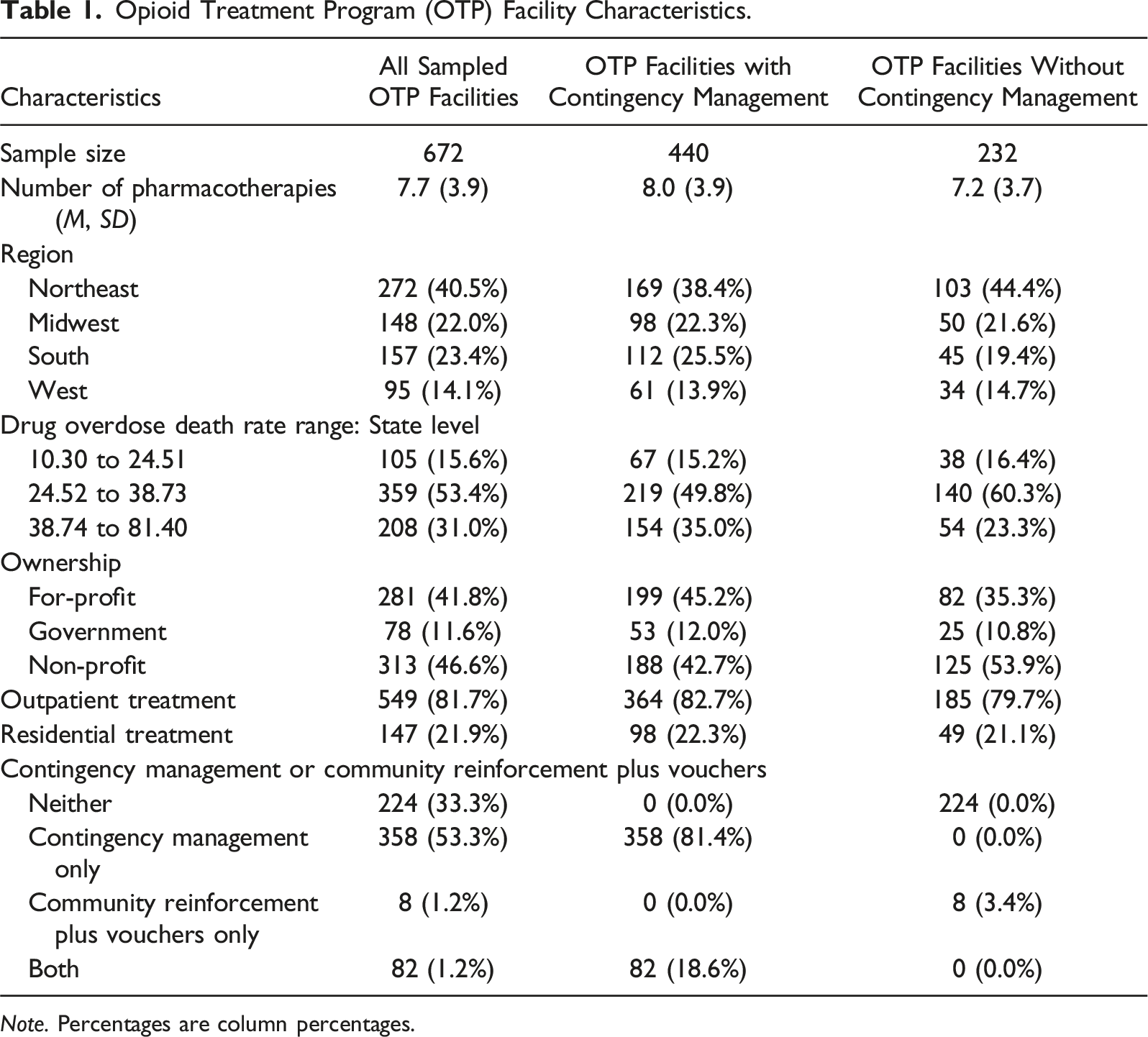
Note. Percentages are column percentages.
OTPs, State-Level Data
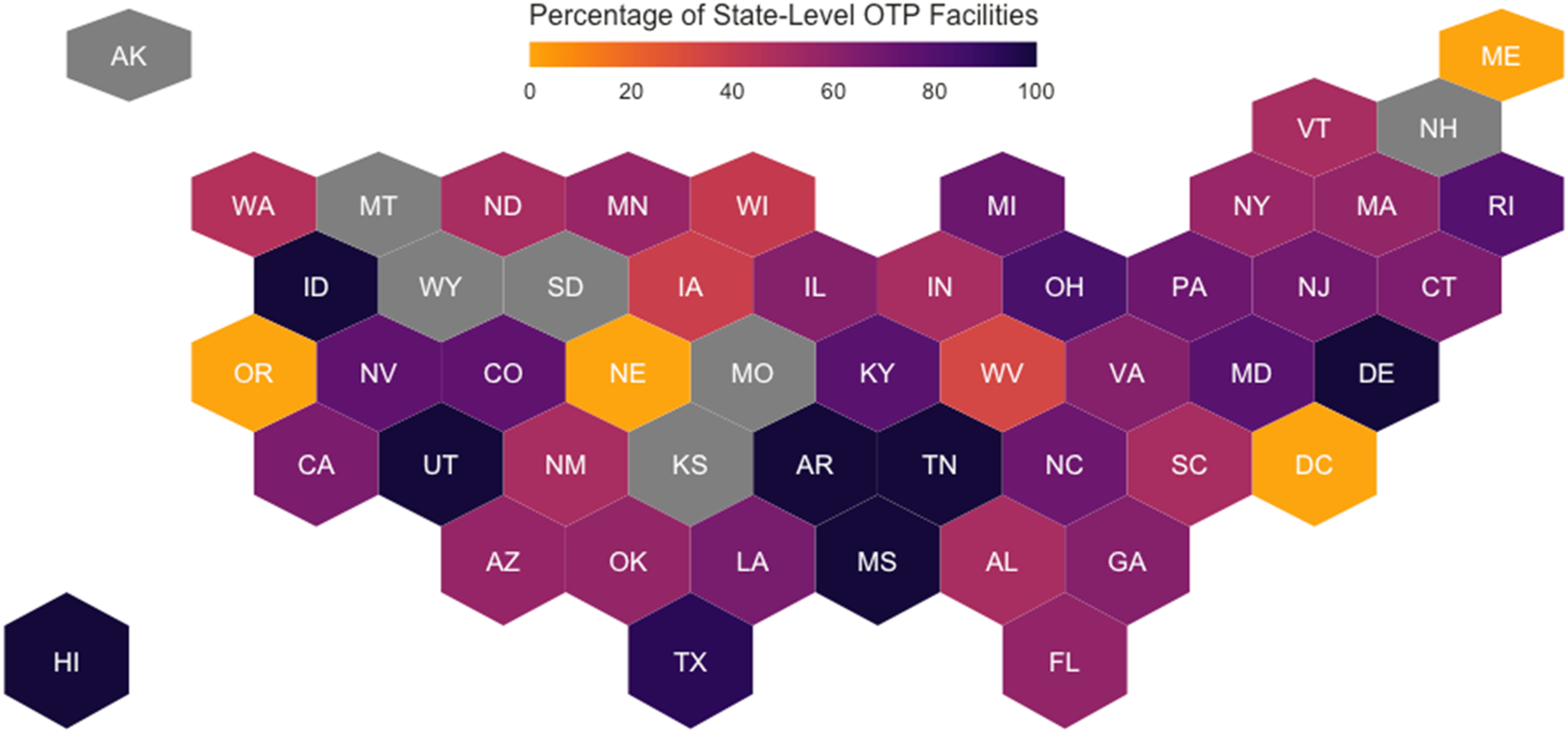
States with the most OTPs were New York (n = 87; 12.9%), Pennsylvania (n = 58; 8.6%), Massachusetts (n = 49; 7.3%), Illinois (n = 48; 7.1%), and Ohio (n = 46; 6.8%). States with no OTPs that met the study inclusion criteria were Alaska, Kansas, Missouri, Montana, New Hampshire, South Dakota, and Wyoming. All OTPs (100.0%) in the following states frequently used contingency management: Arkansas, Delaware, Hawaii, Idaho, Mississippi, Tennessee, and Utah. States (and DC) with no OTPs (0.0%) that frequently used contingency management included DC, Maine, Nebraska, and Oregon.
Figure 1 plots state-level counts of OTPs that met our sample selection criteria in each state, and Figure 2 plots state-level proportions of OTPs with contingency management. Number of opioid treatment programs in each state. Note. Gray indicates no opioid treatment programs that met our sample selection criteria. Percentage of opioid treatment programs that frequently use contingency management in each state. Note. Gray indicates no opioid treatment programs that met our sample selection criteria.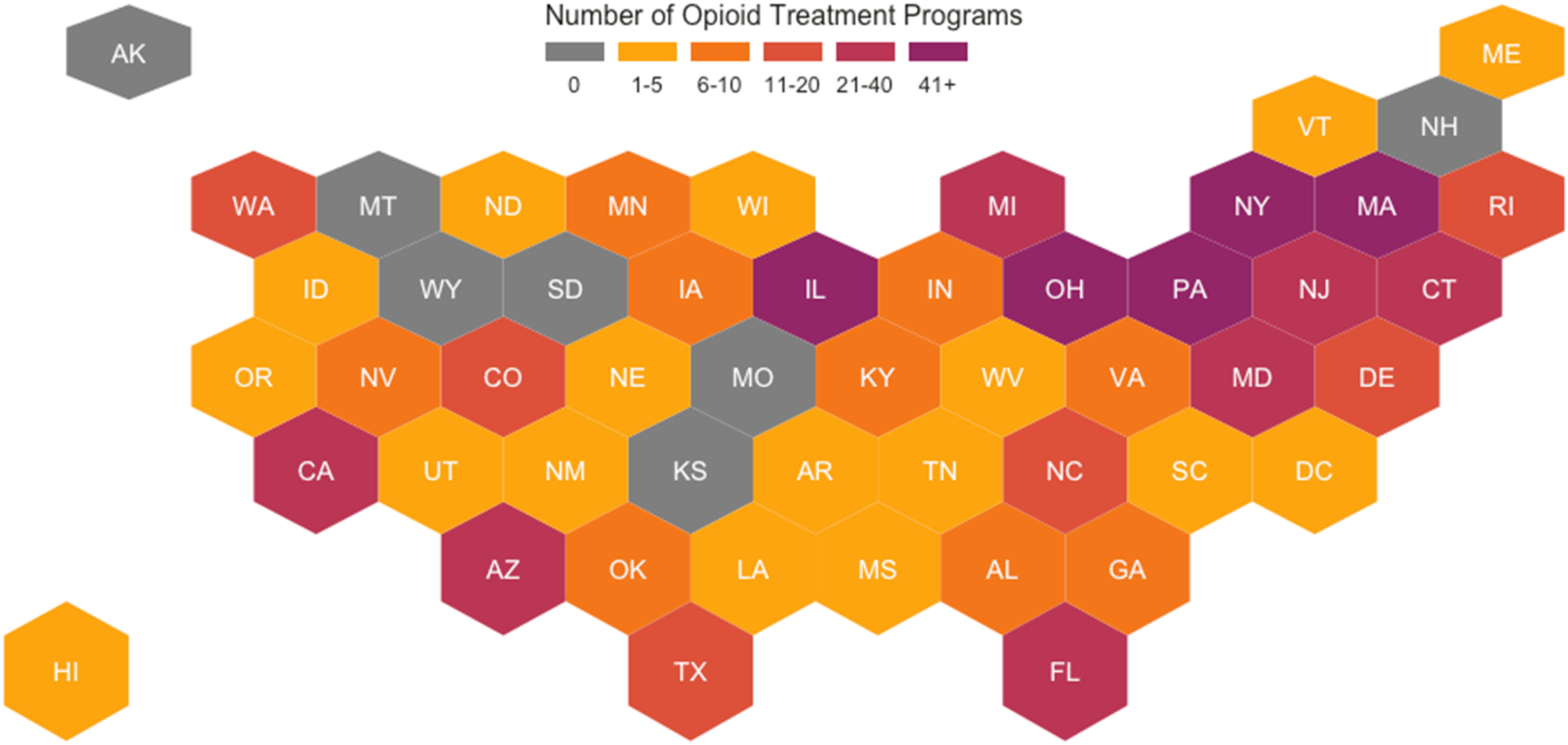
Availability of Contingency Management in OTPs
Binary Logistic Regression Model Examining Opioid Treatment Programs Using Contingency Management.
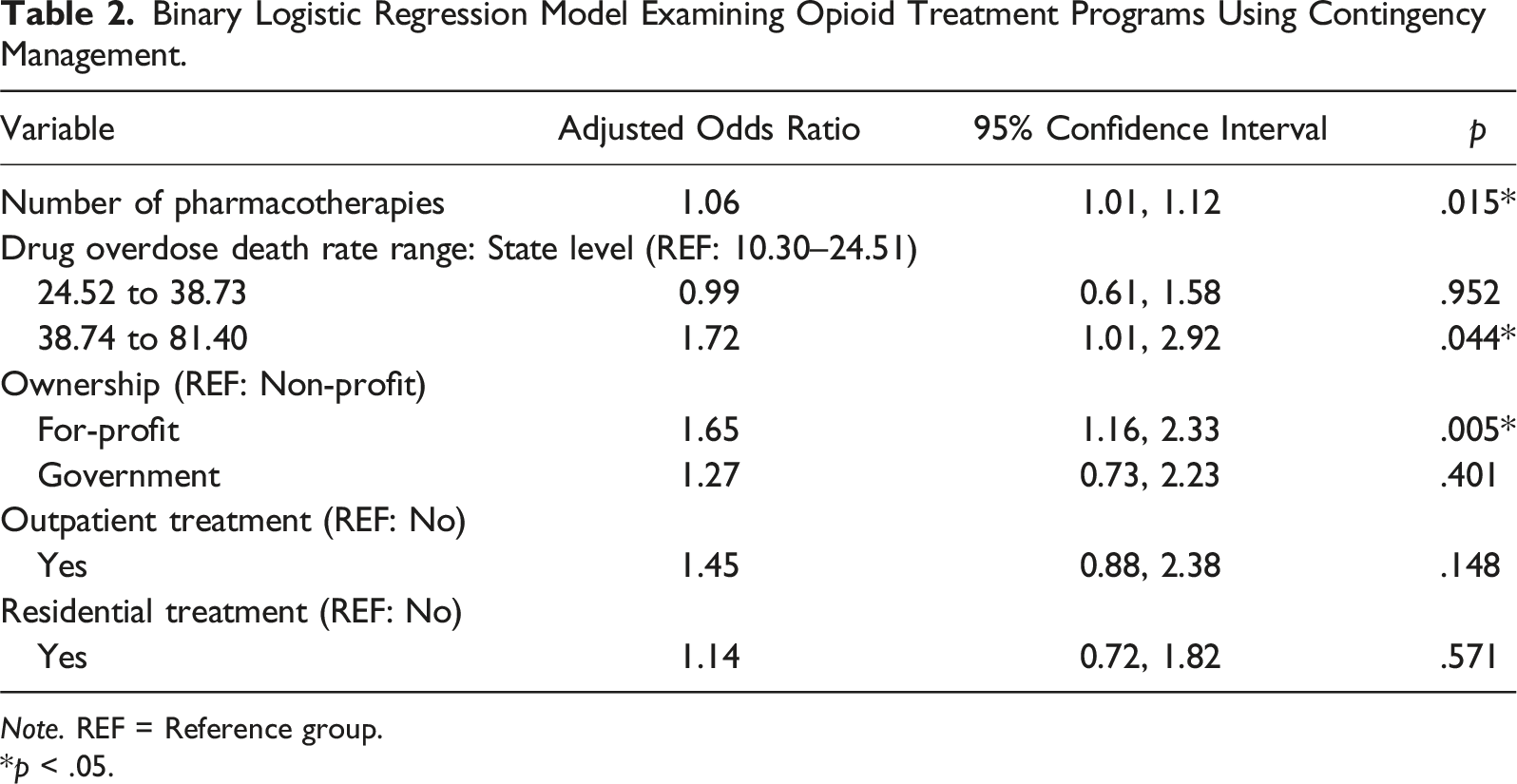
Note. REF = Reference group.
*p < .05.
Availability of Contingency Management or Community Reinforcement Plus Vouchers in OTPs
Multivariate Binary Logistic Regression Model Examining Opioid Treatment Programs Using Contingency Management or Community Reinforcement Vouchers.
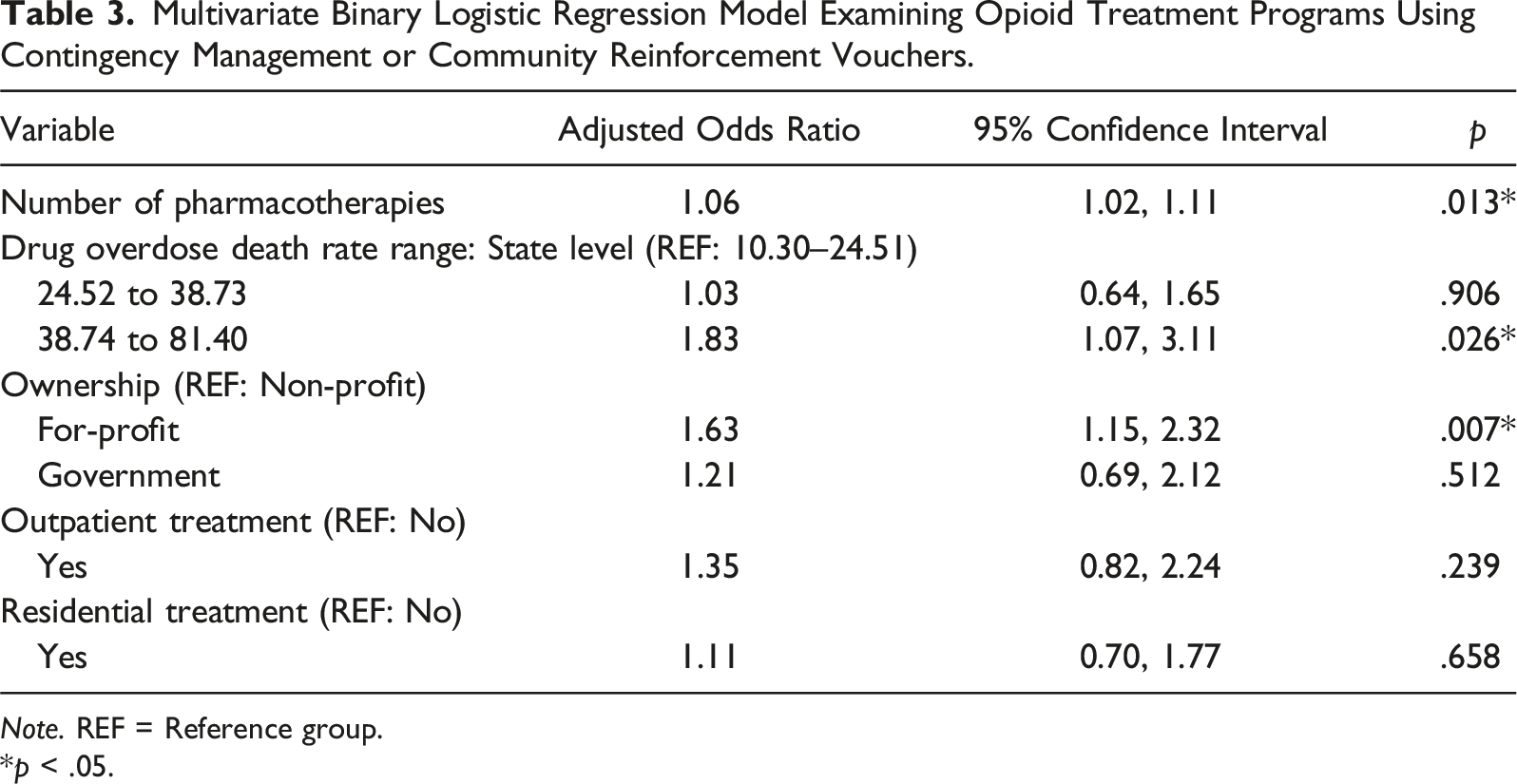
Note. REF = Reference group.
*p < .05.
Discussion
With approximately 2.7 million people with an OUD in the U.S. (Substance Abuse and Mental Health Services Administration, 2022), it is imperative to implement comprehensive behavioral and pharmacological interventions that effectively reduce the risk of harmful outcomes such as overdoses among this sizeable population. Given the substantial evidence that contingency management is effective in treating SUDs, we examined a national sample of 672 OTPs in the U.S. that provide treatment for more than opioid use disorder only, focusing on state-level drug overdose death rates, facility ownership status, outpatient treatment availability, and residential treatment availability as factors associated with the likelihood of OTPs frequently using contingency management. We further identified state-level proportions of OTPs in our study sample that provide contingency management.
Findings from this study identified that 66% of OTPs in our sample frequently use contingency management. Further, results from our multivariable analyses found that OTPs were more likely to frequently use contingency management when they (1) offered more pharmacotherapies, (2) were located in states with the highest drug overdose rates (relative to states with the lowest drug overdose rates), and (3) were for-profit (relative to non-profit).
The positive association between the number of pharmacotherapies within an OTP and the availability of contingency management in that OTP could indicate that these settings have a robust availability to treat other SUDs beyond OUD. Although no gold-standard medications exist for stimulant use disorders (Brandt et al., 2021), the other pharmacotherapies offered in these OTPs may include medications such as acamprosate or disulfiram for an alcohol use disorder (Zindel & Kranzler, 2014). Therefore, these facilities may be more equipped to treat SUDs beyond OUD, indicating their greater capacity to provide contingency management treatments for stimulant use disorder and other SUDs.
Our finding that OTPs that provide treatment for more than only opioid use disorder in states with the highest fatal overdose rates are more likely to use contingency management indicates that these OTPs may have a greater incentive to provide this behavioral intervention to reduce the risk of a fatal overdose. Indeed, the risk of a fatal overdose among OTPs’ treatment population is especially concerning, considering the risk of overdose and other harmful outcomes if an individual returns to previous patterns of use after discontinuing MOUD (Burns et al., 2022). Considering the high national rates of fatal opioid overdoses, combining evidenced-based medications and behavioral interventions (e.g., contingency management) to treat OUD may provide more treatment benefits than either intervention alone (Bolívar et al., 2021). Considering that contingency management service availability was both associated with being located in states with the highest drug overdose rates and facilities being for-profit may highlight greater availability of resources allocated to reduce drug overdoses. This factor is critical as one of the most prominent barriers to contingency management availability is resources for incentives (Rawson et al., 2023).
This study identified a concerning lack of contingency management services in OTPs nationwide, with just 66% of OTPs reporting frequently using contingency management. Considering that most OTPs offer outpatient services, contingency management is an ideal intervention to provide between treatment visits. Some reasons why OTPs may not provide contingency management may include concerns related to anti-kickback regulations, unclear billing codes, lack of training and expertise, insufficient funding for the intervention, and insufficient clinical hours (DeFulio, 2023; Petry, 2010; Proctor, 2022; Volkow, 2022). However, bringing information to providers, conducting provider trainings, and/or implementing regularly scheduled facilitation of contingency management services by an outside vendor may assuage these concerns and assist OTP leaders/administrators with implementing and providing contingency management within their settings (Becker et al., 2019; Hartzler et al., 2014; Petry, 2010; Scott et al., 2021). Expanding the use of contingency management in OTPs nationwide may require initiatives focused on bringing evidence-based knowledge about contingency management’s tenets and effectiveness to treatment facilities around the U.S. For instance, funded consultants with expertise in contingency management could make good headway in facilitating OTPs’ adoption of and increased competence in using contingency management procedures, leading to improvements in treatment and reductions in unnecessary deaths from opioid overdose.
Limitations
Although this study provides up-to-date data regarding the use of contingency management in OTPs across the U.S., these findings should be interpreted in light of some limitations. One limitation is that this study examines SUD treatment facilities that include an OTP; therefore, a different component within the same treatment facility may use contingency management even if the OTP does not. As such, a facility could respond in the affirmative to operating an OTP and respond in the affirmative to frequently using contingency management, yet contingency management may never be used in the OTP but in another location or program of the treatment facility instead. However, this study points to the co-location of contingency management in facilities that operate OTPs and the potential of providers to use contingency management in the OTP. Facilities with Government ownership were only 11.6% of this sample, which could be underpowered in the multivariable analyses. This study also did not examine differences between states that applied for an 1115 Medicaid waiver, which may increase contingency management availability as it could be funded by Medicaid. Another limitation is that our outcome variable was specifically coded for OTPs that reported frequently using contingency management, meaning that we may have excluded facilities that reported occasional or even moderate use of contingency management. Another limitation is selecting facilities that do not only treat persons with OUD. While this allowed us to examine OTPs that may treat individuals with more than only OUD diagnoses, results from our study may not be generalizable to facilities that only treat OUD. However, as a post hoc exploratory examination, we identified the percentage of facilities frequently using contingency management after applying our same sample selection criteria but selecting facilities that
Implications for Future Research
OTPs are facilities that are accredited/certified to use MOUD in the treatment of OUDs. Contingency management is a behavioral intervention which, as indicated by a substantial body of evidence, is effective in treating SUDs (Brown & DeFulio, 2020). It is therefore critical to incorporate contingency management services into OTPs to assist clients with meeting their treatment goals and to provide another tool to curb fatal and non-fatal overdoses among those clients (Bolívar et al., 2021; Griffith et al., 2000). This study found that approximately 66% of OTPs in the U.S. frequently provide contingency management, reflecting the clear and urgent need to implement this behavioral intervention more broadly in these facilities. Future studies should examine the needs of OTPs seeking to incorporate contingency management into their treatment repertoire and identify salient barriers and facilitators of adopting contingency management in these settings. Both implementation and intervention scientists should take steps to identify what outreach or implementation efforts would most effectively expand this contingency management to all available OTPs. Moreover, given the present study’s exclusive focus on OTPs operating in 2020, future studies should examine historic trends in the proportion of OTPs offering contingency management to identify potential factors (e.g., policy changes) that led to the increase, decrease, and/or redistribution of such facilities across the U.S. over time, and track emerging trends moving forward.
Footnotes
Acknowledgments
Dr. Jordan Wingate, thank you for your thoughtful edits.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.