
Abstract
Based on social support theory and exercise promotion health theory, we verified the mediating role of exercise self-efficacy and health-related quality of life in the relationship between social support and the relapse tendency of Chinese people who struggle with drug addiction. Samples who had received traditional Chinese health-promoting exercise interventions over 3 months were recruited from two drug rehabilitation centres in Zhejiang Province (n = 415). The participants completed the Social Support Rating Scale, Exercise Self-Efficacy Scale, Health Survey Short Form Questionnaire Chinese version, and Relapse Tendency Scale. Correlation analysis showed significant positive correlations between social support, exercise self-efficacy, and quality of life. In contrast, social support, exercise self-efficacy, and quality of life were negatively correlated with relapse tendency. In addition, intermediary effect analysis showed that social support has a direct negative predictive effect on relapse tendency in two ways: as an independent intermediary of exercise self-efficacy and as a chain intermediary of exercise self-efficacy and quality of life. Good exercise habits and adherence, as well as early establishment of social support, are beneficial not only for reducing craving and relapse behaviour but also for enhancing the quality of life of people who struggle with drug addiction, thereby facilitating the recovery efficacy for maintenance.
Introduction
Drug addiction is a chronic relapsing disorder characterized by persistent drug-seeking and drug-taking behaviours (O’Brien & Thomas McLellan, 1996). Drug abuse has a severe impact on the health of patients and harms them and their families. It also poses a significant threat to social governance and public safety. Different kinds of drugs can inflict long-term health damage and thus reduce the lifespan of users. For example, cocaine causes severe cardiopulmonary toxicity over time, and chronic users of methamphetamine show not only dramatic changes in mood and behaviour but also psychotic symptoms (Glei & Preston, 2020). Deaths related to psychostimulants, such as methamphetamine and the combined use of the opioid fentanyl, have surged dramatically (Newman et al., 2021).
The World Drug Report 2021 showed that approximately 275 million people worldwide used drugs in 2020, and approximately 5.5% of the population aged 15–64 years had used drugs at least once in the past year, of which 13% (approximately 36.3 million people) suffered from drug abuse disorders. Between 2010 and 2019, the number of people abusing drugs increased by 22%, in part because of global population growth. Based on demographic projections, globally, the number of people who use drugs will increase by 11% by 2030. The report also stated that the COVID-19 epidemic has led to a more flexible service delivery model, innovative and adaptable drug prevention and treatment services, and the introduction or expansion of telemedicine services in many countries (UNODC, 2021). According to the National Drug Control Commission of China, in 2019, there were approximately 2.4 million registered people using drugs in China. Synthetic drugs have replaced opioids as the most commonly used drug in China in recent years, and the availability of novel psychoactive substances (NPS) has risen rapidly (Theunissen et al., 2022; Zhong et al., 2019). More than half are individuals who have relapsed and failed detoxification (National Narcotics Control Commission of China, 2019). Effective treatment strategies, including approved drug therapies, are needed but do not currently exist. The U.S. National Institute on Drug Abuse (NIDA) recommended that drug rehabilitation treatment outcome studies measure other domains, particularly cravings, psychosocial function, self-efficacy, quality of life (QoL), and social support (Tiffany et al., 2012). To reduce stigma and negative bias when talking about addiction, we use “people who struggle with drug addiction/patient” instead of “addict/drug abuser”.
Relapse after detoxification is a complex problem in global drug control and detoxification strategies. Relapse behaviour is the progression of substance use that interrupts the initiation or maintenance of abstinence (Hendershot et al., 2011). Research shows that the relapse rate in Western countries with advanced detoxification conditions and methods is more than 60% within six months (Njoroge, 2017), while relapse rates in developing countries are generally above 90% (Ramsewak et al., 2020; L. Zhang et al., 2019). Relapse tendency refers to the possibility and willingness of recurrent behaviour, an essential prerequisite for individuals to produce a specific behaviour (Krueger et al., 2000). The higher the recurrence tendency, the higher the possibility of relapse behaviour (Zeng & Wei, 2021). Preventing relapse is the key to detoxification for people with addictive behaviours (Maisto & Connors, 2006).
Studies have shown that the increased relapse frequency is related to the decreased perception of social support from family and friends and decreased total social support. Active social support (such as family relationships, communities, related institutions, and essential others) is vital in helping those struggling with drug problems eliminate or slow addictive behaviour. In 2018, China’s Ministry of Justice established a unified basic model of judicial administrative drug rehabilitation to help patients rebuild their social support system and promote exercise intervention as a replacement therapy for them. Relevant studies have shown that exercise has an impact on the stages of the drug addiction cycle (initiation, maintenance, relapse) (Morais et al., 2018). Moderate intensity aerobic exercise is effective in improving abstinence and reducing the relapse rate among patients (T. Zhang et al., 2021). Supervised short-term exercise intervention has achieved good results in physical and mental recovery, but how to translate these interventions into long-term, sustainable exercise remains uncertain. Individuals with high, generalized self-efficacy are more likely to benefit from exercise intervention rehabilitation programs than those with low self-efficacy in patients. According to the above-described background, the research question of this study was whether social support, exercise self-efficacy, and health status perceived by patients were associated with relapse tendency. To find answers to the research question, a cross-sectional survey was conducted.
Social support includes potentially useful information or resources that may positively impact health and well-being (BENSCHOP et al., 2009). Social psychologists have proven that support measures for the general population are not enough for specific groups, and specific support methods are necessary for people with mental illness and with substance use problems (Md Hatah et al., 2015). In this article, social support is referred to as services provided by others and perceived by the recipient as helpful, emotional, and tangible assistance (Ban et al., 2021). Therefore, given many previous studies on the relationship between social support and relapse tendency, we assume that social support can strongly predict relapse tendency.
Self-efficacy refers to the ability of individuals to initially decide to make behavioural changes and successfully adhere to specific healthy behaviours, such as abiding by a sports training program (Bandura, 1997). Exercise training is a high-benefit low-risk intervention for most patients. In recent years, there has been an increase in studies on physical activity and the risk of relapse (Motaghinejad et al., 2015; K. Wang et al., 2019; T. Zhang et al., 2020). Exercise can also enable individuals with drug addiction to achieve better fitness results and improve their psychological states, such as positive changes in personality and psychological characteristics, including emotional improvement, self-confidence, and willpower. Exercise can change individuals’ attitudes towards life and drugs, enhance their willpower and desire to detoxify or develop drug resistance, and prevent relapse (Victor et al., 2016; T. Zhang et al., 2021). We hypothesize that exercise self-efficacy is an intermediary between social support and relapse tendency.
The health and quality of life of those who struggle with drug use are receiving more attention in China (G. Zhang et al., 2018). HRQoL is an essential aspect of human health, embedded in one’s physical health, mental state, social relations, personal beliefs, and relationship with environmental characteristics (Lu et al., 2014). The size, tightness, intensity, and type of social support network will directly affect the social support received by the individual, which may directly or indirectly affect their health status (Bi et al., 2022; Morey et al., 2021). The quality of life and mental health of those with drug dependencies are often lower than those of people without substance use disorders (Zivari-Rahman et al., n.d.). However, the impact of HRQoL on the utilization of health services of those with substance use disorders in China has not been reported.
Lack of support from family or friends is widely recognized as a risk factor for drug addiction and reduces QoL (Guimarães et al., 2013). As a risk factor for relapse, lack of social support may have a dual impact. Due to the increase in psychological distress and social exclusion, recession and unemployment increase the possibility of drug abuse or relapse (FEASTER et al., 2010; Nagelhout et al., 2017). Drug rehabilitation should focus on simple abstinence and strive to restore patients' QoL and physical and mental health (Giménez-Meseguer et al., 2020). Having a high degree of social support can improve QoL, eliminate drug dependence, and reduce relapse. Therefore, given many previous studies on the relationship between social support and QoL, we assume that social support will positively impact QoL, and QoL may play an intermediary role in the effect of social support on relapse tendency.
People with higher self-efficacy are more confident in performing tasks, which helps to reduce the pressure on caregivers and improve their health (Kershaw et al., 2015). There is a negative correlation between self-efficacy, self-esteem, and many aspects of individual mental health (Dule, 2021; Kroll et al., 2007). Exercise can improve self-esteem and cognitive function, reduce social withdrawal, and improve QoL (Mikkelsen et al., 2017). Therefore, more attention needs to be paid to their daily self-management habits and quality of life to improve their exercise compliance. However, there is no research on the relationship between exercise self-efficacy and relapse tendency. We hypothesize that exercise self-efficacy and HRQoL play a chain intermediary role between social support and relapse tendency.
In conclusion, this study aims to explore the influence of social support on relapse tendency, test the independent intermediary role and chain intermediary role of exercise self-efficacy and HRQoL, and provide valuable suggestions for promoting the overall rehabilitation of those struggling with drug addiction.
Methods
Participants and Procedures
A cross-sectional survey study was conducted in two drug rehabilitation centres in Hangzhou city, China, in April 2020. This study adopted a random cluster sampling method. All participants volunteered to participate in the offline test. The test emphasized anonymity, confidentiality, and the use of data only for scientific research. Each test was approximately 30 minutes long. The inclusion criteria were as follows: (1) aged 18 years or above, (2) illegal drug-dependent use (assessed by the Chinese version of the Addiction Severity Index) and (3) medium-intensity traditional Chinese health-promoting exercise interventions lasting at least three months. The exclusion criteria consisted of (1) cognitive impairment and ability to complete the questionnaire independently, (2) serious diseases that prevent participation in physical activities, and (3) undergoing psychotropic drug treatment. A total of 430 questionnaires were distributed; 15 incomplete questionnaires were excluded from the analysis, leaving 415 valid questionnaires (96.5%). The participants included 300 men (72.3%) and 115 women (27.7%). Their ages ranged from 20 to 62 years (M = 38.5, SD = 8.13). Of the participants, 233 (56.1%) were addicted to methamphetamine, 170 (41.0%) to heroin, and 12 (2.9%) abused marijuana or other drugs. In terms of history of relapse, 94 of the participants (22.7%) were first-time drug users, 208 (50.1%) relapsed 1-3 times, and 113 (27.2%) relapsed more than 3 times. A variance analysis found no significant differences in gender and marital status. The research protocol was approved by the Institutional Ethical Review Board of Zhejiang Police Vocational College. Informed consent was obtained from each participant.
Instruments
Social Support Rating Scale
Xiao (1994) developed the SSRS, which has 10 items and three dimensions: subjective support (four items), objective support (three items), and support utilization (three items). While subjective support reflects the perceived interpersonal network that an individual can count on, objective support signifies the degree of actual support an individual received in the past. Support utilization refers to the pattern of behaviour that an individual utilizes when seeking social support. The response options of the eight items ranged from 1 to 4. One item among them has five subquestions; each question was scored from 1 to 4. Two items were scored 0–9 based on the support resources. Social support scores ≤ 44 are classified as a low support level, while those > 44 are classified as a high support level. The Cronbach alpha coefficient was .769 in the present sample. Each item was scored using a four-point Likert scale. Item scores of the SSRS were computed by summation, generating a total support score ranging from 12 to 66, a subjective support score ranging from 8 to 32, an objective support score ranging from 1 to 22, and a support-seeking behaviour score ranging from 3 to 12.
Exercise Self-Efficacy Scale
We used the recently verified Chinese version of the ESES (Y. Liu et al., 2016). The ESES is an instrument used to evaluate confidence in being physically active (Bay et al., 2018). The scale consists of 10 items, and each item is scored on a four-point Likert scale ranging from 1 to 4 (1 = not at all true, 2 = rarely true, 3 = moderately true, 4 = always true). The best possible ESES score is 40 points. The ESES is a validated instrument with high internal consistency and scale integrity (Kroll et al., 2007). The Cronbach alpha coefficient was .879 in the present sample.
Health Survey Short Form Questionnaire (SF-36) Chinese version
This is a self-rating scale with good reliability and validity widely used in the HRQoL measurement of the general population, diseased populations, and others (Ware et al., 1993; Xie et al., 2009). The scale included physical (PCS, Physical Component Summary) and mental domains (MCS, Mental Component Summary). The PCS score was obtained from four dimensions: physical functioning (PF), physical roles (RP), bodily pain (BP), and general health (GH). The MCS score was obtained from four dimensions: vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). The total score in each of the eight domains can be converted into a 0–100 scale, with higher scores indicating better HRQoL. The Cronbach alpha coefficient was acceptable for the PCS (.885) in the current study and the MCS (.784).
Relapse Tendency Scale
The RTS was compiled by Geng Wenxiu (W. Zhu & Geng, 2002). This scale consists of 18 items, including self-assessment of confidence in detoxification, current drug influence, objective environment, degree of physical and mental damage, and support system, with a score of six levels (0 being “almost impossible” and 5 being “very easy”). The higher the total score, the higher the relapse tendency (Xia et al., 2022). In this study, there was excellent internal consistency in this questionnaire (Cronbach’s α = 0.856).
Analysis Strategy
In this study, SPSS 25.0 and AMOS 21.0 were used for descriptive analysis, correlation analysis, and regression analysis. The significance level of all of the variables was determined as α = 0.05. The PROCESS program developed by Hayes examined the mediation model, and the percentage bootstrap method of deviation correction was used to test the significance of the mediating effect. In this study, gender and age were used as control variables, and 95% unbiased correction confidence intervals were constructed by SPSS plug-in PROCESS 3.4 according to the bootstrap method (5000 samples were extracted). Model 4 in PROCESS 3.4 was selected to examine the separate mediating effect of exercise self-efficacy and QoL. Model 6 was then selected to test the chain mediating effect between these factors.
Results
Bivariate Correlations Between Variables of Interest
Correlations, Means, and Standard Deviation of Variables in the Study (N = 415).
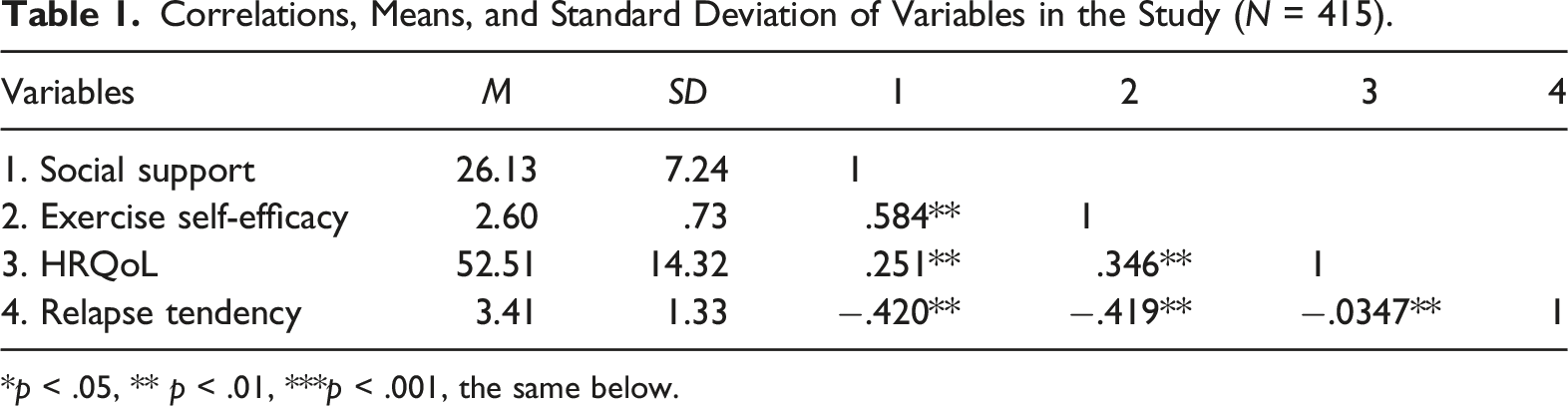
p < .05, ** p < .01, ***p < .001, the same below.
Test for Mediating Effect
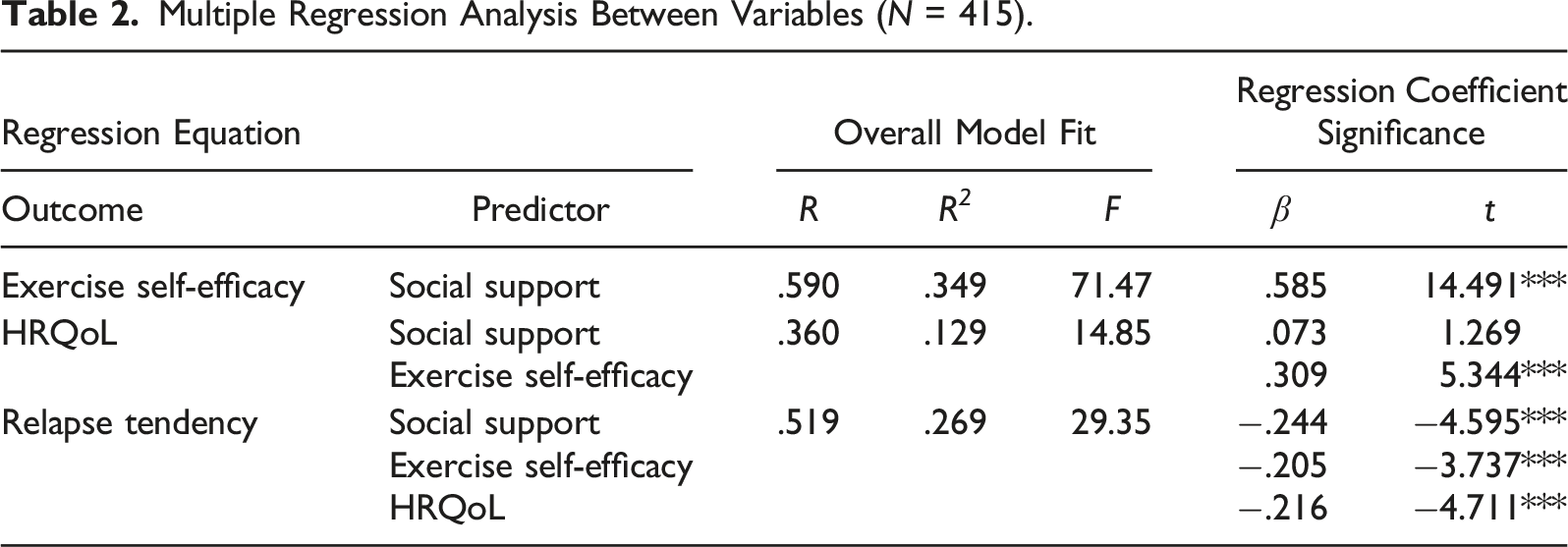
Multiple Regression Analysis Between Variables (N = 415).
Indirect Effect of Social Support on Relapse Tendency via Exercise Self-Efficacy and HRQoL (N = 415).
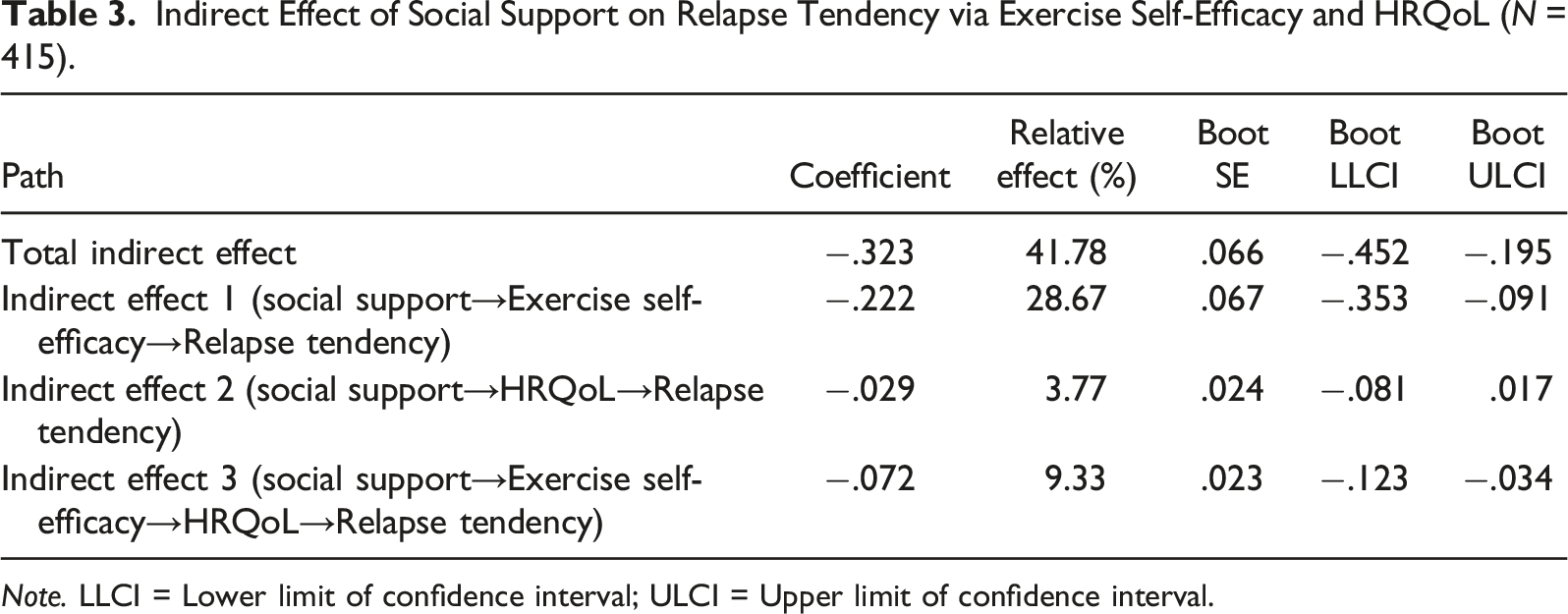
Note. LLCI = Lower limit of confidence interval; ULCI = Upper limit of confidence interval.
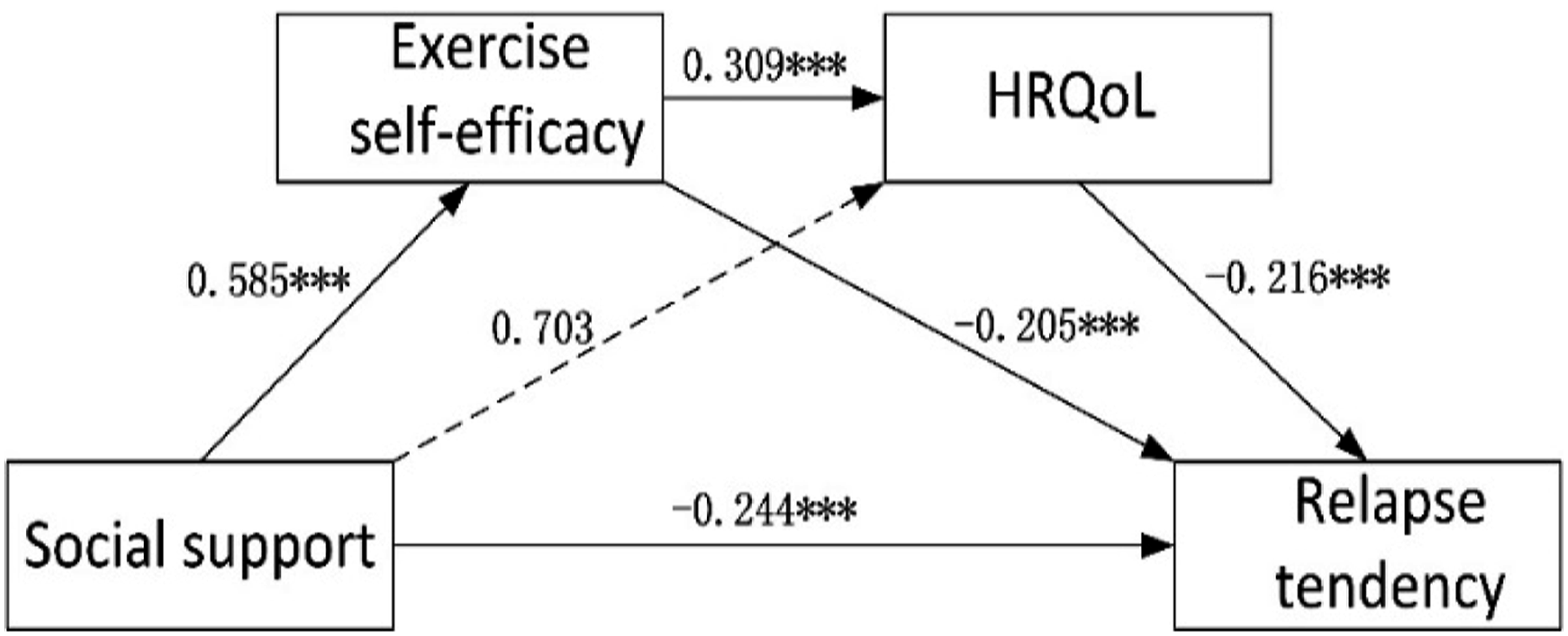
Path analysis for the social support-exercise self-efficacy-HRQoL-relapse tendency model. Values are shown as standardized coefficients.
Discussion
This study’s results showed a significant positive correlation between social support and exercise self-efficacy and a nonsignificant positive correlation between social support and HRQoL. We also found a significant negative correlation between social support and relapse tendency. The results showed that social support played a positive role in promoting the exercise efficacy of those struggling with drug addiction. At the same time, social support also positively promoted physical and mental health and reduced relapse tendency.
Many studies have confirmed that there is a significant relationship between social support and relapse tendency or a significant negative correlation, which is consistent with the results of this study (Caravaca-Sánchez & García-Jarillo, 2020; Massah et al., 2016; Rodríguez-Sáez et al., 2021). Some studies have used different social support scales and come to the same conclusion, such as a significant negative correlation between family support and relapse tendency (Li Liu et al., 2022; Xia et al., 2022; Zeng & Tan, 2021). In addition, this study found that exercise self-efficacy and QoL were significantly negatively correlated with relapse tendency, indicating that exercise self-efficacy acquired with social support (such as training guidance and obtaining positive comments) and QoL (physical and mental health) play an essential role in promoting health and reducing the tendency of relapse among those with substance use disorders.
This study and previous studies show that QoL improvements contribute to reducing drug abuse (Manning et al., 2019). According to the self-medication hypothesis (Khantzian, 1997), relapse may occur as a coping mechanism for managing mental distress, pain, or complex/severe psychosocial issues. Individuals are more likely to reduce their drug use only after finding alternate solutions that improve their QoL. Those who abuse drugs that have poor physical and/or mental health (a substantial proportion of the population) and, more generally, those with poor QoL, often must find ways to reduce relapse. A study found that it was efficient to use exercise to improve the QoL and social interaction among patients dependent on methamphetamine (D. Zhu et al., 2016). Exercise is one of the adjustable strategies to promote a healthy lifestyle and can reduce the incidence of drug abuse. Traditional sports and exercise routines have shown promise as interventions for drug addiction, with suggestions that exercise may attenuate craving states and reduce relapse through interactions with the neurotransmitters active in neural reward pathways, including dopamine and glutamate. Medium-to-high intensity and long-term exercise can encourage the brain to secrete endorphins, resulting in a sense of comfort and pleasure (Kilani et al., 2020). Based on our findings, we believe that the beneficial effects of exercise interventions on QoL should be further explored.
Further results showed that the influence of social support on relapse tendency occurs through the independent intermediary role of exercise self-efficacy and the chain intermediary effect of sports self-efficacy and QoL. However, QoL does not play an independent intermediary role. Most clinical studies have found that social support can significantly positively predict QoL (S. M. Davis et al., 2019; Grills-Taquechel et al., 2011; Jessani et al., 2021; Z. Wang et al., 2022); however, we have not reached a consistent conclusion among those struggling with substance abuse issues. Social support is not always positive and can actually be quite stressful or work against being free from drugs (e.g., domestic violence, negative family relations, peer pressure). In the field of criminology, some scholars believe that social support may not always have a beneficial effect on those struggling with drugs (Deng et al., 2020). Generally, positive social support can have a buffering effect on stress responses, resulting in reduced effects of drugs of abuse. QoL includes two dimensions, physical and mental functioning. Both are harmed by drug addiction because of the negative physical (e.g., bodily pain and physical weakness) and mental (e.g., depression, anxiety, and disruption of family relations) consequences of addiction (Eshagh Afkari et al., 2013).
Social support is a reliable predictor of physical health, but social support and physical health were not associated with adverse mental health outcomes (E. B. Davis et al., 2021). We found that three aspects of social support are of great significance to the QoL of those struggling with drugs. In addition to employment and community integration support, dignity and caring support are critical to those with substance use disorders. In general, the self-esteem of these individuals is significantly lower than that of the general population (Gossop, 1976). A qualitative study shows that taking drugs can give users a feeling of guilt or self-hatred, damaging their self-esteem and self-image (Butler et al., 2010). This difference may also be related to gender. Gender affects psychological functioning, so females struggling with drug use, being more sensitive than males, are more vulnerable to psychological damage. This provides a new conceptual framework for future research to measure the social support needed by this specific group and complements the existing theory of social support. Meanwhile, it also provides some references and guidance for improved interventions.
In this study, exercise self-efficacy plays an intermediary role in the influence of social support on relapse tendency, which showed that the effect of exercise intervention is the same as that of social support, which can effectively reduce the relapse tendency of those struggling with substance use disorders. Motaghinejad et al. and Strickland et al. also believed that physical activity could reduce relapse tendency and the relapse rate both for animal models and humans (Motaghinejad et al., 2015; Strickland et al., 2016). Exercise has also been indicated as a therapy for drug addiction, either in isolated exercise-based interventions or in combination with other addiction treatment strategies (Chen et al., 2022). For example, Schwinn et al. investigated the self-efficacy of women with substance use disorders and found that women with low self-efficacy are more likely to relapse (Schwinn et al., 2016). We speculate that exercise self-efficacy is related to emotions, and those with substance use disorders willing to adhere to rehabilitation exercises have improved emotions, forming a virtuous circle and reducing relapse. Kresina et al. found that different treatments, especially methadone, must be accompanied by behavioural therapy to reduce recurrence (F. Kresina, 2012). We suggest psychological counselling, exercise training, and other behavioural therapy instead of relying solely on drug treatment. To ensure that everyone is able to exercise, the patient’s fitness, pain level, and access to exercise need to be measured first, as unsafe neighbourhoods, high rates of gym membership or limited space or money for exercise will reduce exercise adherence and efficacy. We recommend moderate intensity traditional Chinese health-promoting exercises, such as Baduanjin, Tai Chi, and Wuqinxi (Jia et al., 2022).
This study also discussed the chain mediation between exercise self-efficacy and HRQoL. Long-term drug abuse leads to poor physical functioning, which is also the main factor affecting the psychological function of those with drug addiction (Liu Liu et al., 2018). The level of exercise self-efficacy has a reliable correlation with persisting exercise and has a negative correlation with psychological disturbance and physical discomfort (Hötting et al., 2012). Zhu et al. used drug addiction/dependence (QOL-DA) to assess QoL, and the results showed that it was very effective to use exercise to improve QoL and social interaction among those with drug addictions (D. Zhu et al., 2016).
There are some limitations to this study. First, this study used cross-sectional data, and future studies may adopt a longitudinal design approach to detect the causal relationships between variables. Second, our participants were from mainland China, and the results may not apply to other countries and regions. Third, this study found that exercise self-efficacy partially mediates social support and relapse tendency. Whether other factors, such as specific physical activities, drug abuse history, and improved QoL (including environmental and social domains), moderate or mediate the associations between social support and relapse tendency warrants future research.
The present study shows that social support plays a positive role in promoting exercise self-efficacy and the physical and mental health of those with substance use problems and reduces the tendency of relapse. In particular, exercise self-efficacy acts as an independent mediator of the relationship between social support and relapse tendency, and there is a chain intermediary between exercise self-efficacy and HRQoL. Rehabilitation treatment of those struggling with drug addiction ultimately aspires to improve their QoL by reducing or ceasing their drug use. However, the association between these treatment outcomes should be researched further. Treatment interventions emphasizing appropriate activity and exercise levels, social support, and managing health perceptions may reduce cravings and relapse in those struggling with drug use.
Footnotes
Declaration of Conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 2022 Soft Science Research Program of Zhejiang Province, 2022C35056.
Ethical Approval
The studies were reviewed and approved by the ethics committee of Zhejiang Police Vocational College. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Data Availability
The original contributions presented in the study are included in the article/Supplementary Materials, and further inquiries can be directed to the corresponding author.