
Abstract
An increase in the flow of drugs into the UK via international postal systems poses challenges for law enforcement. ‘Controlled delivery’ can be used to disrupt supply networks and secure intelligence for prosecution; however, critics argue that law enforcement should instead focus on reducing drug-related harm. In Scotland, national drugs strategy adopts a public health approach but it is unclear whether this extends to policing practice. Therefore, this paper examines whether controlled delivery of drug parcels aligns with a public health policing approach. We find evidence of alignment in terms of potential harm to individual users, particularly in relation to legal highs, but not in terms of drug-related harms within the communities to which parcels were destined. We argue that further investigation is required in order to assess the extent to which political intent and policing practice in Scotland align around the principles of harm reduction and public health.
Introduction
Widespread access to the internet and the development of new encryption technologies have significantly facilitated the expansion of illegal drug markets from physical to online spaces (Mounteney et al., 2016). These technologies have changed the dynamics of buying drugs, by connecting customers to a much wider global supply network and enabling the direct delivery of drugs via postal systems (Martin, 2014; National Crime Agency, 2018). While reducing some of the risks to buyers associated with traditional physical markets, including detection and exposure to violence (Bakken, Moeller, and Sandberg, 2018), purchasing drugs online has also increased the potential for greater drug-related harm to both individuals and communities (MacCoun and Reuter, 2001; Matthews et al., 2021). While it is impossible to quantify the scale of global online drugs markets, the NCA (2018) has expressed concern that the increasing volume of illicit drug consignments transiting the UK border via fast parcels and post is likely to continue rising in line with online consumer demand. Moreover, the Covid-19 pandemic has substantially increased the online drugs trade (NCA, 2021).
Parcels entering the UK through the international postal system are subject to checks by Border Force officers who try to intercept and seize those containing illicit items, including drugs. Seizing drugs parcels removes potentially harmful substances from the supply chain; however, it also offers the opportunity to disrupt drug networks and apprehend distributers (Martin, 2014). This can be done using ‘controlled delivery’ whereby a law enforcement officer posing as a postal worker attempts to deliver the parcel to the purchaser (usually with the drugs removed) under controlled conditions and using surveillance (Cutting, 1983). The UNODC (2018) definition of controlled delivery makes it clear that its purpose is purely law enforcement, such as tracing the transit routes of illicit goods and securing evidence to pursue arrest and potential prosecution. However, little is known about the use of this law enforcement tactic, such as the basis on which parcels are selected for delivery or the intended outcome.
Understanding more about such law enforcement tactics is important in the UK context given that drug-related harm, crime and violence, and wider societal impacts are estimated to cost around £20 billion annually (Black, 2020). Drug-related deaths are a particular problem, especially in Scotland which has the highest rate in Europe (National Records of Scotland, 2021). Critics claim that the war on drugs has been lost and that law enforcement policies do not reduce supply chains (Holland, 2020), but are counterproductive and potentially damaging (Maher and Dixon, 1999; Kerr et al., 2005; Paoli et al., 2013). Instead, it is now widely agreed that drug control regimes should focus on harm minimization, such as reducing drug-related health risks and other socially damaging impacts (Bull et al., 2016). This is in keeping with a growing realisation that many complex societal problems straddle the domains of law enforcement and public health (van Dijk & Crofts, 2017) and, therefore, require a ‘public health approach’ to policing (Christmas and Srivastava, 2019).
Drugs flowing through postal systems clearly represent a degree of harm to potential users, depending on the amount and type of drugs contained in each individual parcel. However, they also pose a threat to the communities to which such parcels are destined, which often suffer from deprivation and health-related vulnerabilities (Saberi Zafarghandi et al., 2022). Caulkins and Reuter (2009: 9) note that “law enforcement is uniquely empowered to address market-related harms”; therefore, it is of interest to know whether the use of controlled delivery aligns with a harm reduction approach.
In Scotland, the language of harm reduction has been central to drug strategy for many years (Scottish Government, 2008, 2021); however, responsibility for drug policy is reserved to the UK Government and sits within a law enforcement portfolio (UK Government, 2021). According to the Scottish Affairs Select Committee (2019), lack of domestic power over drugs policy has constrained efforts to implement public health measures in Scotland; and critics note that policing strategies towards the control of drugs remain rooted in punitive enforcement rhetoric (McLean, Holligan and McPhee, 2018). However, there is very little research on operational policing practice in relation to drugs in Scotland and nothing on whether it aligns with a harm reduction approach. Therefore, using a novel administrative dataset, this paper examines the use of controlled delivery by law enforcement officers in Scotland to determine whether it shows evidence of a public health approach that has the potential to reduce drug-related harm.
Illegal Drugs and Law Enforcement
Purchasing illegal drugs from online markets has grown in popularity, not least because it allows users to interact anonymously without leaving traces of their illegal activities (Martin, 2014; Moyle et al., 2019). The delivery process relies largely on postal distribution networks (Aldridge & Décary-Hétu, 2014; Christin, 2013; Décary-Hétu et al., 2016), which is convenient to purchasers and reduces some of the risks associated with purchasing drugs face-to-face (Bakken et al., 2018). The risk of interception by border control agencies, and the potential threat of arrest or other law enforcement action, does not seem to deter buyers. Indeed, online forums often provide information about the dangers associated with the delivery of illegal drugs (Martin, 2014), and advice about packaging techniques and how to use postal services without raising suspicion (Aldridge & Askew, 2017). The determination of customers and the resourcefulness of vendors in avoiding detection pose a significant challenge for law enforcement, especially when using mainstream forms of transportation, such as postal and courier services (EMCCDAE, 2019). As Martin (2014) notes, one of the biggest barriers to identifying illegal drug consignments is the sheer volume of legitimate post in circulation, which makes it unfeasible to scrutinise all incoming foreign mail.
The scale of the problem is unknown, although the National Crime Agency has reported an ongoing rise in the volume of drug shipments entering the UK via fast parcels and post (NCA, 2018), and a shocking 245% increase in the seizure of drug parcels during the pandemic (NCA, 2021). The ever-increasing number of drug parcels seized by law enforcement agencies poses a challenge in terms of deciding how to deal with them. Any illegal drugs are ultimately destroyed; however, seized parcels can provide valuable information about drug producers, distributors and consumers, including the origin of consignments, concealment methods, and even components linked to specific manufacturers, batches, or retailers (Martin, 2014). In some cases, therefore, a decision is taken to undertake a ‘controlled delivery’ (Matthews et al., 2020).
A controlled delivery is a ‘technique for allowing suspicious shipments or cargo to leave, pass through or enter a jurisdiction with the knowledge and supervision of authorities’ (UNODC, 2018). In the case of drugs, it involves the real-time delivery of the parcel to the addressee by a law enforcement officer, dressed as a postal worker, under controlled conditions and using surveillance (Cutting 1983). Controlled deliveries do not always result in high quality evidence or an arrest, as purchasers may be attuned to the possibility of apprehension and employ strategies to minimise their risks (Aldridge & Askew, 2017). As a result, they must be carefully justified in terms of financial and human resources, especially if they relate to small consignments (Martin, 2014). Importantly, the defined purpose of controlled delivery is purely law enforcement (UNODC, 2018); however, little is known about its use, such as the basis on which parcels are selected for delivery or the intended outcome.
Harm Reduction and Public Health Policing
While policing responses to drug control have traditionally focused on targeted enforcement, this can be counterproductive and potentially damaging to both drug users and wider society (Maher and Dixon, 1999; Kerr et al., 2005; Paoli et al., 2013), while doing little to disrupt supply chains (Holland 2020). In recent years, the principle of ‘harm minimization’ has come to dominate global drugs policy, although it is a controversial concept that lacks universal agreement on practical implementation (Bull et al., 2016). Nevertheless, it is widely accepted that the success of drug control regimes should be measured through reductions in the health-related harms and wider societal impacts associated with drugs markets (Black, 2020).
Calls to move towards approaches that incorporate elements of public protection and harm reduction (Saloner et al., 2018) are supported by evidence that these can have greater benefits, such as reducing drug-related violence (Kammersgaard, 2019) and facilitating access to treatment services rather than arrest (Clifasefi et al., 2017). However, there are considerable challenges at an operational level (Caulkins & Reuter, 2009), and not all harm reduction efforts are successful (Rhodes et al., 2006). Nevertheless, adopting harm reduction strategies hold the potential to improve outcomes for both individuals (e.g. drug users) and communities (Kerr et al., 2005), as well as increasing trust in the police and improving community safety (Fordham & Stevens, 2013).
The notion of harm reduction aligns closely with the concept of ‘public health approaches’ to policing, which recognise that many complex societal problems straddle the domains of law enforcement and public health (Punch & James, 2017; van Dijk & Crofts, 2017). Such an approach requires a good understanding of the needs of the population to enable effective targeting of resources (Christmas and Srivastava, 2019). In the context of illegal drugs, it has been proposed that drug-related harms should be identified, evaluated and prioritised according to the level of severity and breadth of impact on society (Paoli et al., 2013; Greenfield & Paoli, 2013). Caulkins and Reuter (2009: 10) observe that “much drug-related harm is suffered by people other than drug users and much drug-related harm is caused by drug markets and/or drug-related crime and violence, as opposed to drug use directly”. Therefore, a public health policing approach to controlled delivery should reflect both the potential harm posed to individual users (i.e. by identifying parcels that contain the largest quantity and the most dangerous drug type), and the potential for wider societal harm (i.e. by assessing the level of vulnerability within the community to which parcels were destined). Given the cost and complexity of such law enforcement operations, understanding when and where controlled delivery is used and how closely it is aligned with harm reduction approach should be a policy priority, especially in contexts where concern about drug-related harm is heightened, which is certainly the case in Scotland.
The Drug Problem in Scotland
According to a recent House of Commons Scottish Affairs Select Committee (2019), “Scotland is in the midst of a drugs crisis”. Since 1996, there has been a four-fold increase in the number of both drug-related acute hospital admissions (Information Service Division, 2019a) and drug-related deaths (Scottish Government 2021a), with a particularly sharp increase from 2013 onwards. Prevalence data shows that drug use amongst the general population followed a similar level and trend to that for England and Wales until around 2014/15, but the percentage of adults using drugs rose more steeply in Scotland thereafter (UK Government, 2021a). Moreover, patterns of consumption amongst drug users in Scotland show higher than average use of Cocaine (Scottish Drugs Forum, 2018), Opioids and Benzodiazepines (UK Government, 2021a), and more frequent poly-drug use (Crew 2000, 2019). Scotland’s drug-related death rate reached a record high in 2020, and is more than 3.5 times that for the UK and higher than all other EU countries (National Records of Scotland, 2021). The scale of the problem has prompted the establishment of a Drug Deaths Taskforce with a “national mission to reduce what is currently a national disgrace” (Scottish Government, 2021b).
The reasons for Scotland’s drug problem are complex and multi-faceted, although evidence suggests they are not that different to other parts of the UK, just more severe (Scottish Affairs Select Committee, 2019). Experts point to longstanding problems associated with poverty, deprivation and inequality as underlying causes (Liddell, 2019), and concerns that these have been exacerbated by budget cuts to vital drug services (McPhee, 2021). Drug dependence is higher in the most deprived communities (Information Service Division, 2019a), where residents are 18 times more likely to die from drugs than those in the least deprived communities (National Records of Scotland, 2021). However, recent research shows a proliferation of drug distribution across the country (Densley et al., 2018), with easy access to drugs expanding well beyond areas of intense deprivation (Crew 2000, 2019), including into previously protected remote and rural communities (Matthews et al., 2021). The growth of online markets has contributed to this proliferation, making drugs more easily accessible to both individual users and serious and organised crime gangs (Densley et al., 2018) and increasing the volume, variety and purity of illegal drugs entering Scotland (Crew 2000, 2019).
What to do about the drugs problem in Scotland poses a challenge for both politicians and policing. Under the 1999 devolution settlement, responsibility for drugs policy is reserved to the UK Government and sits within the portfolio of the Minister of State for Crime, Policing and the Fire Service, which means it relies heavily on the language of enforcement (UK Government, 2021b). In Scotland, however, drugs have been situated within a public health context since the publication of the 2008 National Drugs Strategy (Scottish Government, 2008). While efforts to implement a range of public health measures have been constrained (Scottish Affairs Select Committee, 2019), Scotland’s First Minister remains committed to dealing with the problem of drugs “from a public health perspective and not a criminal justice perspective” (Scottish Government, 2021b). Yet, critics argue that this sits incongruously alongside Scottish policing policy, especially in terms of dealing with serious and organised drug crime, which remains situated in a ‘one size fits all’ punitive law enforcement narrative (McLean et al., 2018). This contradiction in Scottish policy perspectives raises important questions about whether, and in what way, operational policing practice reflects a public health approach which could contribute to reducing drug-related harm. As there has been no previous research on this topic, this paper offers valuable insights into one specific area of drug-related policing and its alignment with public health outcomes.
Aims, Hypotheses and Objectives
Using a bespoke administrative dataset on illegal drug parcels seized en route to Scotland, the aim of this paper is to examine patterns of controlled delivery to determine whether there is any evidence of alignment with a public health approach. There is no pre-existing definition of a public health approach within the context of controlled delivery and we did not have access to information about law enforcement decision making in respect of individual parcels. However, we hypothesise that patterns of delivery that aligned with increased potential for drug-related harm, and not just illegality, would provide evidence of a public health approach. At the level of individual users, we hypothesise that parcels containing substances that were known to be most harmful to health and those containing the largest quantities of drugs would most likely result in controlled delivery; whereas, at a community level, we hypothesise that controlled delivery would be most likely for parcels destined to areas already demonstrating greater susceptibility to drug-related harms. The research had three specific objectives:
(1) To identify whether controlled delivery was more likely in cases where parcels posed a greater risk of drug-related harm based on drug type and quantity, which would be supportive of public health policing at the level of individual users. (2) To identify whether controlled delivery was more likely in cases where parcels were destined for vulnerable locations characterised by deprivation and drug-related harm (including drug-related death rates, hospital admissions and crime), which would be supportive of public health policing at a community level. (3) To explore the extent and nature of variation in the use of controlled delivery across Scotland once both parcel and area characteristics were taken into account, to determine whether spatial differences in the use of controlled delivery may have been due to other factors.
Research Design
The study involved multi-level modelling of a unique administrative dataset shared by the NCA with the Scottish Centre for Administrative Data Research for research purposes. This anonymised dataset contained details of 1,374 illegal drugs parcels seized by the UKBF en route to Scotland between April 2011 and January 2016, including: destination of the parcel, size and type of commodity, date of seizure, and whether or not the parcel was subject to a controlled delivery. Destination addresses were aggregated to datazone1, which provides an approximate location at a small area level suitable for examining relatively low-level clustered patterns of drug purchase and for linking to community-based data from other sources (as discussed below). Some parcels may have contained more than one substance; however, the NCA dataset only included information about the primary drug type. For more details about the dataset, see Matthews et al. (2020).
Variable Description
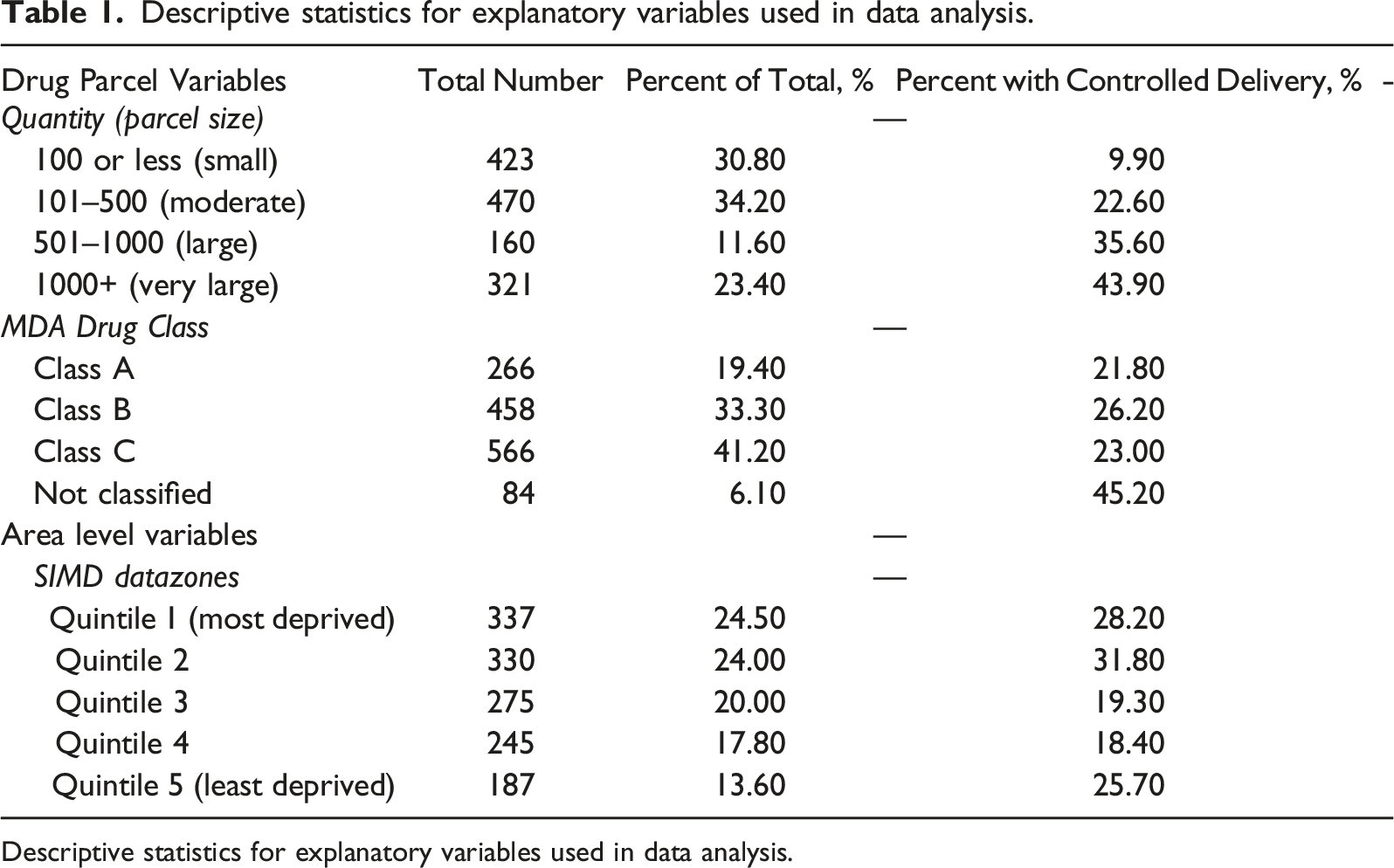
Descriptive statistics for explanatory variables used in data analysis.
Descriptive statistics for explanatory variables used in data analysis.
Correlation between drug-harm indicators and controlled delivery and intercepted parcels rate.
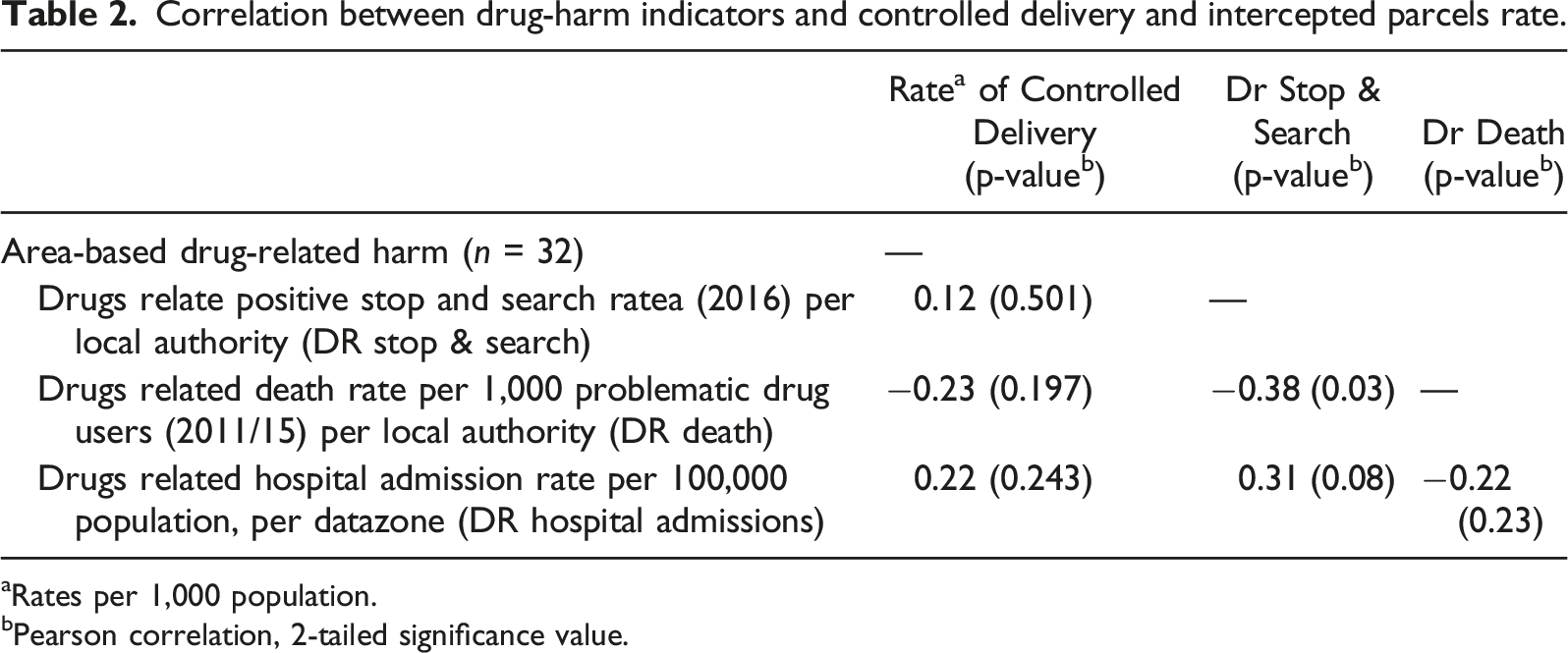
aRates per 1,000 population.
bPearson correlation, 2-tailed significance value.
Drug Parcel Variables
From a public health policing perspective, we hypothesised that controlled delivery should reflect both the seriousness of the substance (in terms of both illegality and potential for harm) and the quantity contained within the parcel. The variables measuring drug type and quantity are discussed below.
Drug Seriousness
Parcels were classified into categories under the Misuse of Drugs Act 1971, which takes account of relative harm and sentencing level. As shown in Table 1, two fifths of parcels contained Class C drugs (e.g. Benzodiazepines, steroids and GBL), a third contained Class B drugs (e.g. Cannabinoids, some Amphetamines, Ketamine, and some Opioids), and a fifth contained Class A drugs (e.g. Cocaine, Ecstasy/MDMA, Heroin and LSD). We hypothesised that controlled delivery would be more likely for the most serious drugs based on MDA classification as they were likely to be most harmful; however, Table 1 shows little difference in the likelihood of controlled delivery based on drug classification alone.
A category was also created for substances ‘not classified’ under the MDA. This predominantly included New Psychoactive Substances (NPS): synthetic drugs that mimic the effect of illegal substances such as Cocaine, Cannabis and Ecstasy. Originally known as ‘legal highs’ because they could be purchased legitimately (Birdwell et al., 2011), concern about the harmfulness of NPS (Stephenson and Richardson, 2014) prompted the UK Government to ban them under the Psychoactive Substances Act 2016. As substances in this category were legal at the time our data were collected, controlled delivery for purely law enforcement purposes was unlikely; however, we hypothesised that likelihood of controlled delivery would be increased under a public health policing approach. As shown in Table 1, unclassified substances represented only 6% of all parcels, but they were around twice as likely to result in a controlled delivery compared to the drug parcels classified under the MDA.
Drug Quantity
Drugs come in different units of measurement (e.g. grams, ampoules, tablets, etc.), which makes it difficult to compare them. Using the EMCDDA (2011) approach for classifying bulk transactions of drugs based on weights and number of units, we defined four broad categories (from small to very large) based on the volume of drugs contained in each parcel. Table 1 shows that two thirds of all parcels contained a small (31%) or moderate (34%) amount of drugs. Large parcels were the least common, while almost a quarter of all parcels were defined as very large. Under a public health policing approach, we anticipated that larger parcels were more likely to be subject to controlled delivery. As shown in Table 1, only 9.9% of small parcels resulted in this action compared with 43.9% of very large parcels.
Area-Based Variables
Four spatial variables were included in the analysis to examine whether controlled delivery was aligned with a number of area-based drug-related factors within the communities to which parcels were addressed. These variables are described, and discussed in relation to public health policing, below.
Area-Based Deprivation
The Scottish Index of Multiple Deprivation 2 (SIMD) was used as a measure of community vulnerability, due to the strong link between deprivation and drug-related harm (Information Service Division, 2019a). From a public health policing perspective, we hypothesised that controlled delivery would be higher for drug parcels addressed to the most deprived communities. Table 1 shows that this was not the case at a simple descriptive level. Indeed, the proportion of drug parcels resulting in a controlled delivery within the least deprived areas (quintile 5) was almost the same as that in the most deprived areas (quintile 1).
Drug-Related Stop and Search
Using open-source data from Police Scotland, we included the rate of positive drug-related stop searches per 1,000 population for each of Scotland’s 32 LAAs as a measure of drug-related crime. From a public health perspective, we hypothesised that parcels were more likely to result in a controlled delivery if they were destined to LAAs where police officers were recording a higher level of drug-related activity and, therefore, harm. Table 2 shows a weak, and non-significant, correlation of 0.12 between the positive drug search rate and the rate of controlled delivery by LAA, which provides no evidence at a descriptive level that policing activity was skewed towards LAAs with greater levels of drug-related crime.
Drug-Related Deaths
Using open-source data from Public Health Scotland, the rate of drug-related deaths between 2011 and 2015 per 1,000 problem drug users within Scotland’s 32 LAAs was used to measure problematic drug use. From a public health perspective, we hypothesised that controlled delivery would be higher in areas with a higher than average drug-related death rate; however, Table 2 shows a negative correlation (−0.23) between the rate of controlled delivery and the drug-related death rate at LAA level. Although weak and non-significant, these findings suggest that controlled deliveries were slightly skewed towards LAAs with a lower drug-related death rate.
Drug-Related Hospital Admissions
Also using open-source data from Public Health Scotland, drug-related hospital admissions (DRHA) were used as a proxy measure for serious drug misuse within Scotland’s 32 LAAs. The rate is based on the European Age-Sex Standardised Rate and reflects the number of DRHA per 100,000 population (Information Service Division, 2019b). From a public health perspective, we hypothesised that the proportion of drug parcels resulting in a controlled delivery would be greater in LAAs with higher rates of DRHA. Table 2 shows a weak but positive correlation of 0.22 between DRHA rates and the rate of controlled delivery. Although non-significant, it does provide some evidence that controlled delivery may have been aligned with a public health approach.
Using LAAs as our unit of analysis has reduced our likelihood of finding significant correlations (as there are only 32 in Scotland); nevertheless, our descriptive analysis is useful as it indicates that the rate of controlled delivery may be positively associated with DRHA, but negatively associated with drug-related deaths, while it is unlikely to be related to drug-related crime. These correlations provide inconclusive evidence that use of controlled delivery was aligned with a public health policing approach; however, modelling these factors simultaneously provides greater clarity.
Modelling Approach
Using multilevel models for binary responses (Gelman, 2013; Kruschke, 2014), we further assessed the association between controlled delivery and our drug-related harm indicators at both individual and community level. Multilevel models account for the clustered structure of the data; in this case, parcels nested within LAAs. The probability of controlled delivery was modelled as a function of level 1 variables, denoted by the physical characteristics of the parcels (type and quantity), and a set of level-2 variables representing the area-based measures of drug-related harm and deprivation relating to their destination.
The model can be defined by the following equation:
In equation (1),
One of the advantages of multilevel models in this research is that they allow us to explore the influence of contextual characteristics, which could indicate harms to individual and/or communities, on the probability of controlled delivery. In addition, these models account for the bias introduced by the clustering of parcels (Tranmer and Steel 2016), allowing us to explore the effect of higher level grouping structures (LAAs) on the likelihood of a controlled delivery.
The locus of both seized parcels and controlled deliveries was highly clustered in some areas and very sparse in others (Matthews et al. 2021). The sparsity of the data made it challenging to implement traditional statistical methods, as low sample size can affect statistical power, which can yield non-significant or potentially biased results (Gelman, 2013; Kruschke, 2014). Under these situations, Bayesian methods have the advantage of producing more reliable estimation, even in the presence of small sample sizes (Browne & Draper, 2006; Snijders & Bosker, 2011). Therefore, we used weakly informative priors based on the t-distribution with small degrees of freedom which is appropriate for logistic models, and Bayesian predictive checks to evaluate the adequacy of the fit of the model to the data (Gelman, 2013). This gives an indication of the plausibility of the model estimated for the purposes for what it would be used. The “leave-one-out cross validation” method (Gabry et al., 2019; Vehtari et al., 2017) was used to assess the adequacy of the models. All the models were fitted in R Studio, using the Rstanarm package (Goodrich et al. 2018).
Results
The results from the best fitting model are presented in Figure 1. The estimates for each independent variable are presented as a dot representing the mean (or point) estimate of the association between it and the likelihood of a controlled delivery, with a line representing the 95% credible interval. Level 1 represents drug type and quantity (individual harms), level 2 represents the area-based variables (community harms). Posterior estimates of the associations between independent variables and the likelihood of adopted controlled deliveries.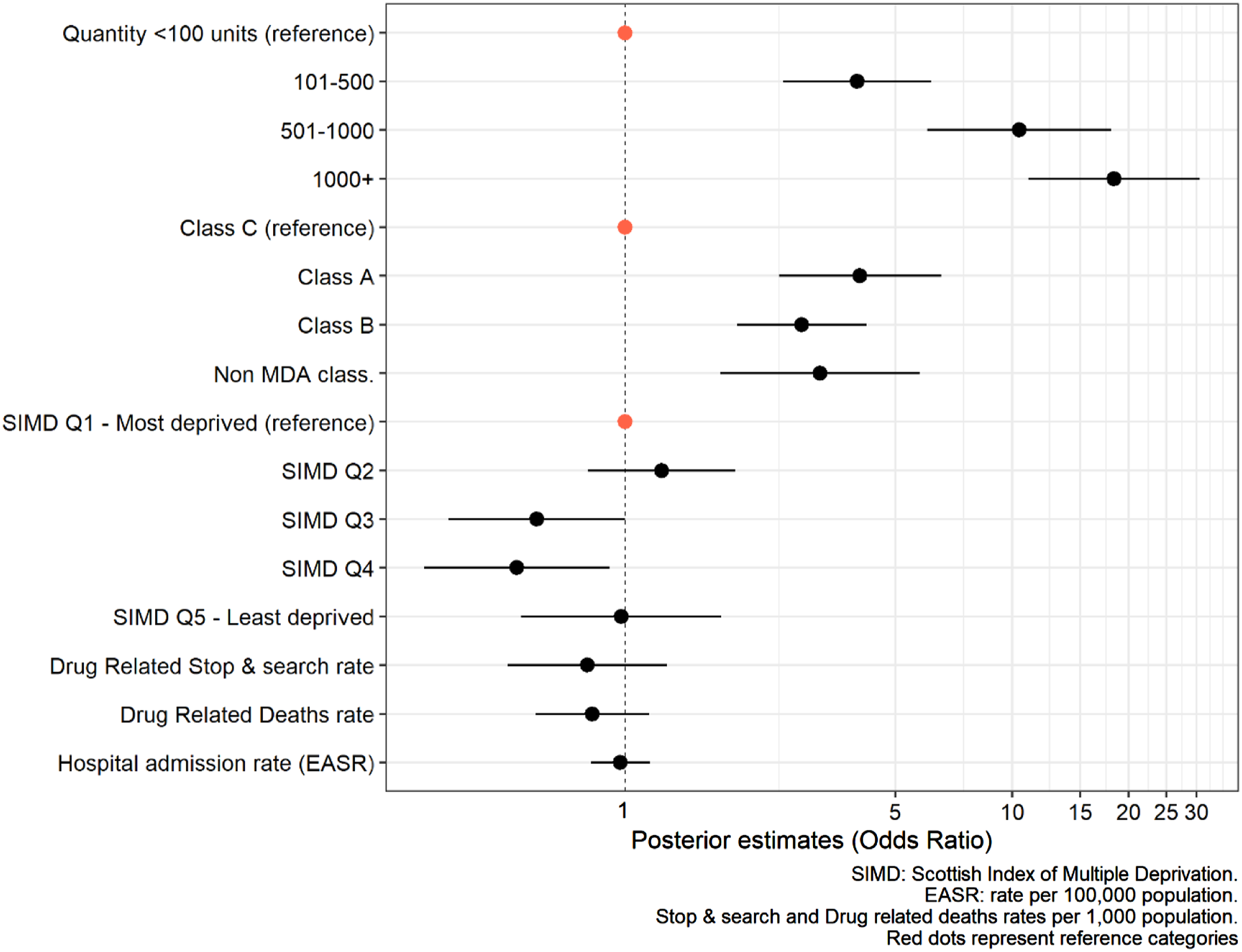
Assessing Individual Level Harms
Our first objective was to identify whether controlled delivery was more likely in cases where parcels posed a greater risk of drug-related harm at an individual level based on drug type and quantity. Figure 1 shows that quantity had the strongest association with controlled delivery, such that the larger the parcel the more likely it was to result in law enforcement action. A controlled delivery for a moderate parcel (between 101-500 units) had almost four times the odds (OR=3.9) of resulting in a controlled delivery than a parcel smaller than 100 units. For large parcels (between 500-1000 units) the odds of controlled delivery more than doubled (OR=10.4); and then almost doubled again (OR=18.0) for very large parcels (above 1,000 units). Previous research shows that parcels containing larger quantities of illegal drugs (especially over 500 units/gr) are most likely associated with redistribution and wholesale rather than personal use (Pantoja et al., 2022). Therefore, increased likelihood of controlled delivery may have been driven by law enforcement concerns about criminality (e.g. the purchaser’s status as a dealer, involvement in serious and organised crime, or potential for violence). However, controlled delivery of larger quantities of drugs also fits with a public health approach, since these would pose a greater level of health-related harms to the individual purchaser and other users to whom the drugs were intended for distribution.
Figure 1 also shows that drug classification was associated with controlled deliveries. The results shown in Table 1 suggested that (with the exception of non-MDA classified substances) there was little difference in the likelihood of controlled delivery based on drug type. However, when controlling for the other factors, Figure 1 reveals that the odds of a Class A parcel resulting in a controlled delivery was 4 times the odds for a Class C parcel (OR=4.04), whereas the equivalent odds for a parcel containing Class B drugs was nearly 3 times (OR=2.8). Again, controlled delivery of the most serious drug types under the MDA fits with a law enforcement approach targeting those who may be involved in criminality. However, from a public health policing perspective, parcels containing Class A and B drugs could represent a greater immediate degree of risk to individual users than Class C drugs in terms of their potential for health-related harm.
Interestingly, however, parcels containing substances that were not classified under the MDA also had 3 times greater odds (OR=3.2) of being adopted for a controlled delivery than Class C parcels. From a purely law enforcement perspective, these substances (which mainly comprised NPS) were not illegal and so it is difficult to explain how controlled delivery could be justified on these grounds alone. Rather, the increased probability of controlled delivery compared to Class C drugs suggests that law enforcement officers prioritised these parcels for other reasons. Under our hypotheses, it is plausible that use of controlled delivery for non-classified substances was driven primarily by concerns about the health-related effects of the substances contained in these parcels, especial NPS which showed a distinct increase in sales from 2010 onwards, until they were banned in 2016 (Peacock et al., 2019).
Figure 2 illustrates the interaction between quantity and drug type. It shows that likelihood of controlled delivery increased according to quantity for all drug types; however, it increased at a far lower rate for Class C drug parcels than for those containing Class A and B drugs, and non-classified parcels. In other words, the amount of drugs seized was a greater driver of controlled delivery than substance type, which suggests that law enforcement was targeting distribution and wholesale activities more than the strength and harmful potential of the substance itself. Nevertheless, the fact that unclassified parcels were just as likely as Class A and B drugs to be subject to controlled delivery does indicate a clear public health dimension to the policing approach at this time. Predicted probability of controlled delivery by drugs MDA classification and size of the consignment.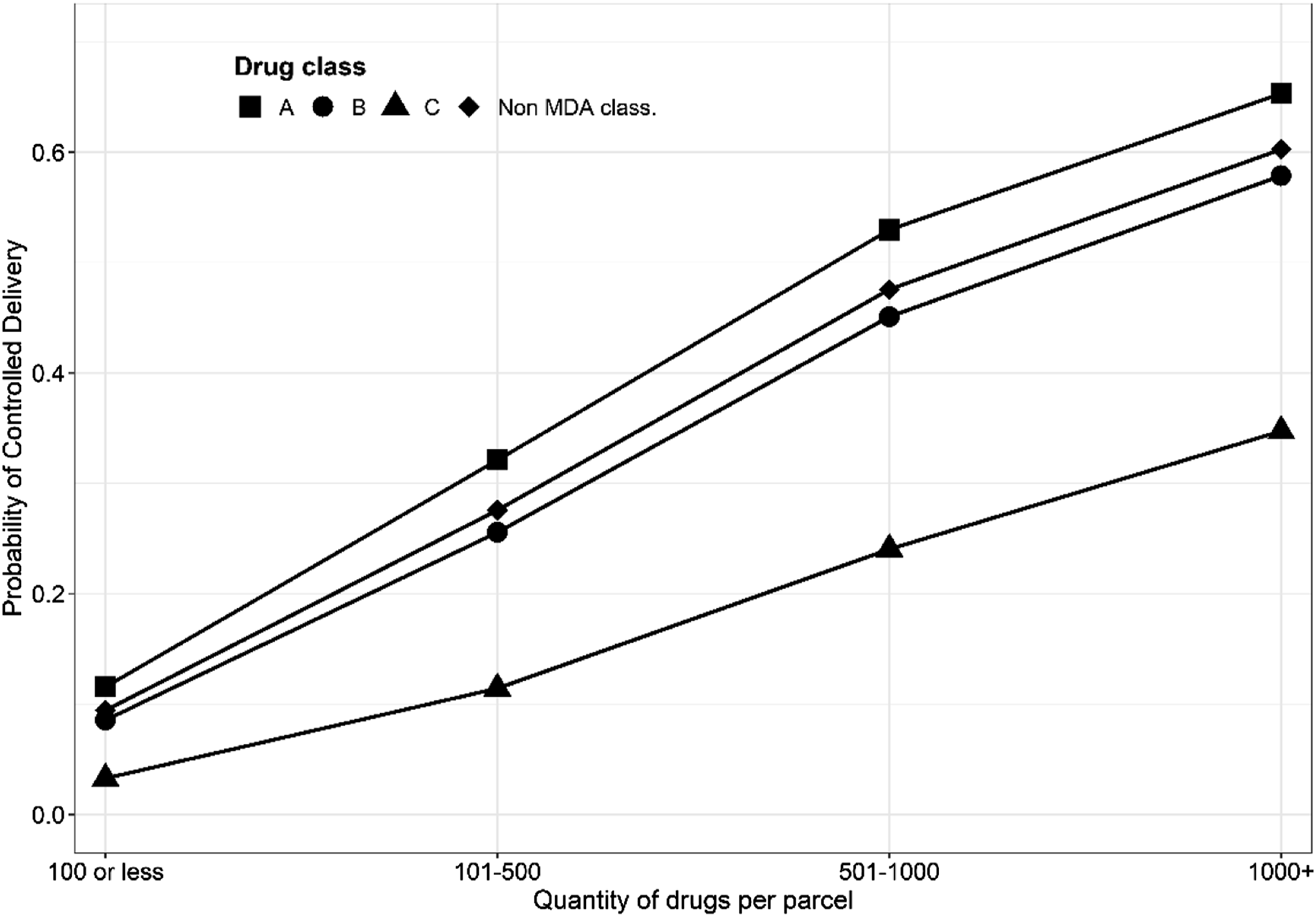
Assessing Community Level Factors
Our second objective was to identify whether controlled delivery was more likely when parcels were destined for vulnerable locations, characterised by area deprivation and drug-related harm. Figure 1 indicates that the probability of controlled delivery varied by SIMD quintile in a way that broadly fits with a public health approach. For examples, parcels destined to datazones in the third and fourth quintile (which were less deprived) were significantly less likely to be subject to a controlled delivery than those destined for addresses in the most deprived quintile. However, there was no difference in the odds of a controlled delivery for parcels addressed to areas in the most and least deprived quintile. This refutes our hypothesis that controlled delivery would be higher in more deprived areas of Scotland, even after taking account of drug type and quantity, as drug dependence (Information Service Division, 2019a) and death (National Records of Scotland, 2021) are known to be so much greater in these communities.
Beyond the findings about SIMD, we found no evidence of association between the area-based variables included in the model and likelihood of controlled delivery. The model suggested that controlled delivery was slightly less likely to occur in LAAs where the police recorded higher rates of positive drug searches and in LAAs with a higher drug-related death rate, although these findings were not significant. There was no measurable difference at all by hospital admission rate, despite the fact that this looked plausible in the descriptive analysis. This suggests that law enforcement activities aimed at dealing with illegal drug parcels did not align with concerns about underlying drug-related harms that pre-existed within communities, as might be captured in these contextual variables. Consequently, the absence of a statistical relationship could reflect a missed opportunity for law enforcement to support wider public health concerns.
Assessing Spatial Variation
Our final objective was to explore the extent and nature of variation in controlled delivery across Scotland after both parcel and area-based characteristics had been taken into account. The ‘excess likelihood’ (or random effect) of a controlled delivery by LAA, which represents the unique contribution of each LAA to the odds of a parcel resulting in a controlled delivery, is illustrated in Figure 3. Darker shades indicate authorities with a higher probability of controlled deliveries. We can see considerable variation across Scotland; however, the map shows that law enforcement activity did tend to concentrate in certain LAAs. First, we find an excess likelihood of controlled delivery in some large, urban LAAs (specifically Stirling and Edinburgh) but not in others (such as the cities of Glasgow, Dundee and Aberdeen). Second, there was excess likelihood of controlled delivery within some LAAs with very small population sizes: namely, Clackmannanshire, Midlothian and East Lothian (to the right of the map) and Dumfries and Galloway (to the bottom left of the map), but not others (such as the Highlands and Islands). Interestingly, there was very little excess likelihood of controlled delivery in most LAAs in the West of Scotland, despite the fact that drug use and drug-related crime are higher in these parts of Scotland (Information Service Division, 2019a; Scottish Government, 2019). adjusted estimates of controlled delivery by Local Authority.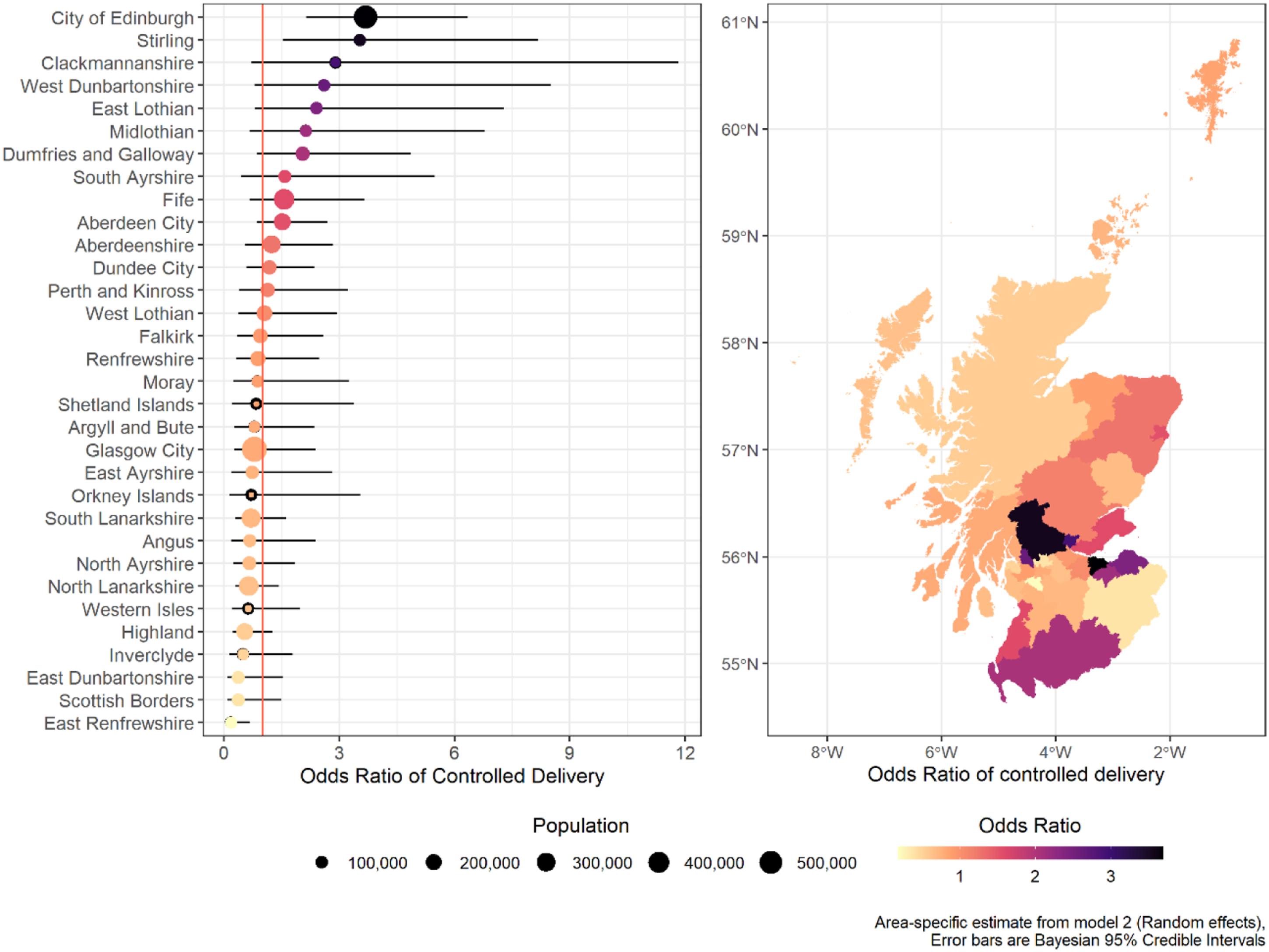
While there is not space to discuss in detail the geographical patterning in Figure 3, the variation in excess likelihood of controlled delivery indicates the existence of explanatory factors at LAA level that were unaccounted for in our models. These factors could well be related to specific policing intelligence about certain groups or individuals, trends in wider drug dealing activity, or simply due to resource issues or staffing levels. It should be noted that, in April 2013, Scotland’s eight police forces were merged into one single Police Service for Scotland. Therefore, the data on controlled deliveries were collected during a period of considerable turmoil and restructuring in policing terms. Nevertheless, the majority of the parcels were seized in the period following police reform (Matthews et al., 2020), so less variation across the country may have been expected. It is also important to acknowledge that analysis at LAA level may not pick up important distinctions in local policing practice, which is a limitation of our work that is discussed later.
Another factor that could have influenced use of controlled delivery was spatial variation in the level of demand; therefore, we examined the relationship between the odds of a controlled delivery and the rate of parcels seized per capita for each LAA. Figure 4 plots the number of parcels seized per 10,000 residents within each LAA on the x-axis against the excess likelihood of a controlled delivery on the y-axis. The dots represent each of Scotland’s 32 LAAs. Four quadrants have been created using a dashed horizontal line to represent the baseline odds ratio of 1 (i.e. equal likelihood of a positive or negative controlled delivery), and a dashed vertical line to represent the national average rate of parcels seized (2.3 per 10,000 people). Association between rate packages delivery by council area and odds of controlled delivery.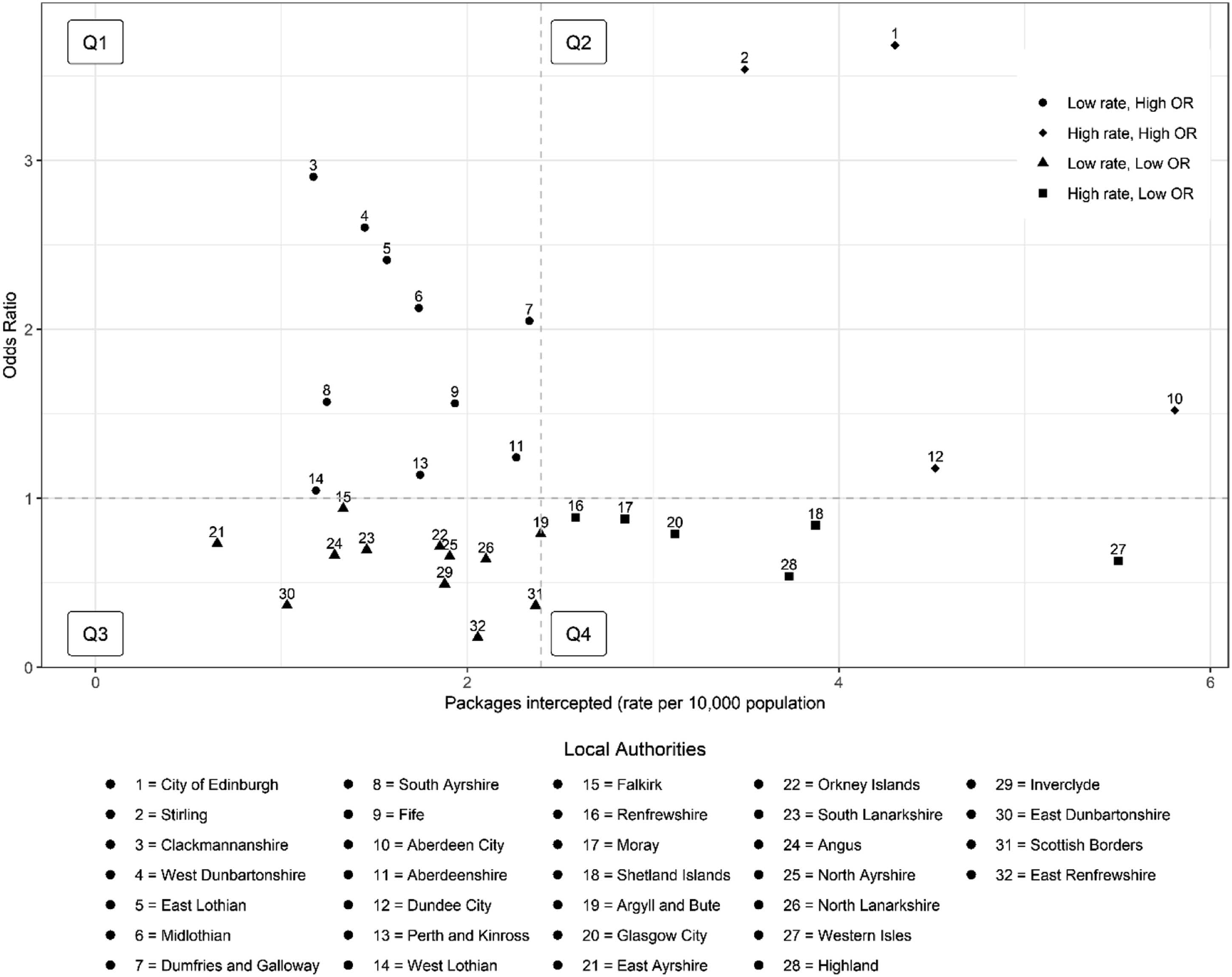
After accounting for both parcel and area-based characteristics, Figure 4 shows no clear relationship between rate of parcels seized and odds of a controlled delivery. There were 22 LAAs with a parcel delivery rate equal to or below the national average (Quadrants one and 3), while 10 LAAs had a higher than average delivery rate (Quadrants two and 4). Amongst this group of 10, four large urban LAAs stand out: parcels en route to Edinburgh and Stirling had an excess likelihood of a controlled delivery while those destined for Aberdeen and Dundee had odds of controlled delivery that were much closer to the average (Quadrant 2). Parcels destined for the remaining six LAAs had a lower than average likelihood of resulting in controlled delivery, despite there being a higher rate of delivery to these areas. This included a mix of LAAs with larger urban populations in the West of Scotland, such as Glasgow and Renfrewshire, and some extremely remote and rural authorities in the Highlands and Scottish Islands (Quadrant 4).
The six LAAs in Quadrant four are of particular interest because they could suggest that a higher threshold was being used by law enforcement before deciding to conduct a controlled delivery in these areas, despite a higher than average rate of parcel interception. Since this is not accounted for by differences in the size and type of the commodity or area-based variables known to be related to problematic drug use, these findings suggest that there were other factors at play in determining the use of controlled delivery. One possible explanation is that ‘clusters’ of smaller drug parcels were being addressed to certain areas within a LAA that – individually - go unnoticed by law enforcement, but – collectively – pose a high risk of harm. Another explanation could be that some online drug purchasers buy smaller quantities of drugs but on a more frequent basis as a strategy to avoid detection (Densley et al., 2018), which could have a cumulative effect of increasing the risk of both individual and community level harm. Unfortunately, we do not have sufficiently fine-grained data to explore these hypotheses; however, understanding these intricate geographical patterns in the data could shed important light on drug purchasing behaviours that have a high risk in terms of individual and community level harm but a low risk of attracting law enforcement attention.
Discussion
This paper set out to examine whether there was any evidence that use of controlled delivery, used by law enforcement agencies to deal with illegal drug parcels intercepted in the international postal system, aligned with a public health policing approach. The significant rise in drugs entering the UK after being purchased via online markets are a significant cause of concern (NCA, 2018, 2021), especially in countries such as Scotland that have a serious problem with drug-related hospital admissions and deaths (Scottish Government 2021). Scotland’s drugs strategy is firmly premised on a public health model that aims to reduce drug-related harm (Scottish Government 2008, 2021); although, critics argue that policing approaches to drug control remain rooted in a punitive enforcement rhetoric (McLean et al., 2018). In the absence of any research on the use of controlled delivery, we hypothesised that patterns of delivery that aligned with increased potential for drug-related harm, and not just illegality, would provide evidence of a public health approach. Using a unique administrative dataset from the National Crime Agency, we examined potential drug-related harms at both an individual level (based on drug type and quantity) and a community level (using various measures of are-based harm). In doing so, we offer unique insights into an under-investigated area of law enforcement activity and demonstrate mixed evidence that Scottish policing activity was aligned with the public health narrative contained in the national drugs strategy.
At an individual level, we hypothesised that a public health policing approach would reflect greater likelihood of controlled delivery for parcels containing the most harmful substances and the largest quantities. Generally speaking, this is exactly what we found. Likelihood of controlled delivery increased as the quantity of substances increased, and Class A and B drugs were more likely to result in a controlled delivery than Class C drugs; however, this was also true for non-classified parcels, mostly containing NPS or legal highs. In fact, the probability of controlled delivery was around the same for non-classified parcels as Class A and B drugs, regardless of parcel size. Our findings on classified drug type and quantity align with both law enforcement and public health narratives. Targeting the individuals responsible for purchasing larger consignments of drugs, especially those of a more serious nature, implies that officers prioritised parcels that were intended for onward supply (potentially linked to serious and organised crime). This aligns with a criminal justice approach aimed at gathering intelligence and pursuing prosecution, but also a public health approach aimed at minimizing potential harm to vulnerable individuals. However, the pattern of controlled delivery for non-classified substances aligns more closely with a public health approach, as it is likely that this was due to public concern about the health-related impacts of what were legal substances during our period of study. In Scotland, in particular, benzodiazepine NPS (e.g. Etizolam) was linked to a significant rise in drug-related harm mortality at this time (UK Government 2022; Peacock et al., 2019).
At a community level, we hypothesised that controlled delivery would be more likely for parcels destined to areas already demonstrating greater susceptibility to drug-related harms. However, we found no evidence of this in our analysis. There was some variation according to level of area deprivation; however, controlled delivery was just as likely to be used for parcels en route to Scotland’s most affluent communities as to the poorest. It is possible that this reflected law enforcement suspicions about the underlying motivation of drug purchasers; for example, Pantoja et al. (2022) found that parcels intended for wholesale dealing did not differ greatly by area deprivation. Nevertheless, public health approaches to policing are likely to have the greatest impact within poor, disadvantaged and marginalised communities (van Dijk & Crofts 2017); and so, it is surprising that we did not find use of controlled delivery to be greater in intervening in the drug supply chains within neighbourhoods of greatest deprivation in Scotland.
Importantly, our modelling found no association between the likelihood of controlled delivery and three spatial indicators of drug-related harm. The rate of positive police searches on suspicion of possession of drugs provides a proxy measure of drug-related crime and, as such, we hypothesised that this would be positively associated with likelihood of controlled delivery; however, this was not the case. The rate of drug-related hospital admissions and deaths are measures of serious drug-related harm; however, neither was significantly associated with the probability of controlled delivery. These findings provide no evidence that this type of drug-related law enforcement activity was aligned with a public health approach at a community level.
After taking account of the characteristics of the parcel and indicators of deprivation and harm, we found that there was still considerable variation in the likelihood of controlled delivery across Scotland. Of course, we may have missed important information that determined decision-making (e.g. intelligence about drug purchasers, other drug-related policing activity, or availability of appropriate policing resources). Nevertheless, the variation in spatial patterning is of interest from a criminal justice and a public health point of view. We found excess likelihood of controlled delivery in several Scottish cities, but not those that are known to have significantly higher rates of drug-related crime, harm and deaths (including Glasgow, Dundee and Aberdeen). In addition, use of controlled delivery was notably lowest in the west of Scotland, despite drug use and drug-related crime being highest on that side of the country (Scottish Government, 2019). These spatial patterns are definitely out of kilter with what might reasonably be assumed under a public health approach.
Even though the rate of seized parcels did not help explain spatial variation in law enforcement practice, it did highlight areas with much lower than average use of controlled delivery. This included a mixture of LAAs with large urban populations in the West of Scotland, such as Glasgow and Renfrewshire, and some extremely remote and rural LAAs in the North of Scotland, including the Highlands, and the Shetland and Western Isles. Previous analysis of NCA data (Matthews et al., 2021) found evidence of spatial clustering of seized drug parcels at datazone level – especially within remote and rural locations of Scotland. This could be suggestive of strategic purchasing activity, where larger numbers of smaller parcels are purchased in an attempt to evade law enforcement detection or prosecution (see Densley et al., 2018). Again, this raises important questions, both from a criminal justice point of view, in terms of whether there are certain localities where online drug purchasing is more prevalent and problematic; and from a public health point of view, in terms of high risk drug consignments entering rural and remote communities where fewer specialist drug services exist.
It is important to note that we do not argue that controlled delivery is, or should be recognised as, a method of public health policing. Rather, we have considered controlled delivery as an example of drug-related law enforcement intervention with the purpose of examining whether there was evidence of alignment with a public health policing approach. We cannot make any judgement or inference about the effectiveness of controlled delivery in disrupting drug markets, as we do not have appropriate data. Likewise, our findings cannot determine whether any hypothetical alignment with a public health policing approach was intended to, or actually did, result in harm minimization. Nevertheless, we believe our approach addresses an important issue within the study of drug-related policing and offers a novel avenue of research for those interested in pursuing it further. From a policy perspective, we would argue that further investigation is required in order to assess the extent to which political intent and policing practice in Scotland align around the principles of harm reduction and public health.
Limitations of This Paper
Our dataset and analysis have some limitations which mean our findings need to be interpreted with caution. First, the time period covered by the data (2011–2016) pre-dates the current drug-related deaths crisis in Scotland. Access to more recent data may have enabled us to identify a stronger link between drug-related deaths with use of controlled delivery. Nevertheless, the period analysed encompassed a rapid increase in drug-related deaths and hospital admissions (from 2013), a substantial rise in online drug purchasing within the UK (from 2014), and was covered by the Scottish Government’s national drugs strategy (from 2008). Second, the data only included drugs delivered to Scotland from overseas through postal services, which means that we cannot make any inferences about drugs trafficked by other means, including internal supply routes and County Lines. However, the focus of the paper was on use of controlled delivery, rather than the policing of wider drug-related activity, so our findings are relevant in that specific context.
Third, our analysis was constrained by the sparsity of the data (in relation to seized drug parcels) and lack of small-area data for indicators of drug-related harm (which meant we had to rely on analysis at LAA level). This is referred to as the Modifiable Areal Unit Problem (MAUP) (Manley, 2019), and means that we could not properly account for the concentration of both drug deliveries and drug-related harms within communities. In addition, we included only three drug-related harm indicators in our study. Information about a wider range of harm indicators, such as those suggested by Paoli et al. (2013) and Caulkins and Reuter (2009) would have improved the robustness, validity and utility of our research. Future research should consider potential solutions to these problems.
We must caution against over-interpretation of our findings as the true extent of drug-related harms within communities are unlikely to have been reflected in our model. Nevertheless, our approach does illustrate the potential benefit of using administrative data – alongside other data sources - to provide law enforcement organisations with greater insights to support a public health policing approach to reducing drug-related harm.
Conclusion
This paper has taken an innovative approach to analysing law enforcement data from the NCA to determine whether the use of controlled delivery for seized drug parcels is in line with a public health policing approach to reducing drug-related harm. Overall, we found mixed evidence that controlled delivery was in line with a public health policing approach. To the extent that law enforcement activity was driven by concern about drug-related harms, this appeared to be specific to the risks posed by individual packages, rather than influenced by concerns about the drug-related vulnerability within the wider community. This study demonstrates the potential value from both a law enforcement and public health perspective of considering a broad spectrum of contextual evidence, not just about the risks posed by individual drug parcels but the wider community-level risks, when taking decisions about policing intervention. With the ever increasing rise in online drug purchasing through social media sites and cryptomarkets, the findings presented here illuminate the potential for better data sharing and collaborative working amongst those who share a common purpose and responsibility for tackling the problem of drug-related harms within communities. We propose that there are opportunities for law enforcement agencies to learn from this analysis in terms of considering a wider set of criteria when making decisions about controlled delivery. This is of particular relevance to practitioners and policy makers working in Scotland where the problem of drug misuse and drug-related deaths is so acute.
Footnotes
Acknowledgments
We thank Dr Stuart Weatherley from the National Crime Agency for providing the study data and for helpful discussions about the analysis. We thank the eDRIS team at Public Health Scotland, and particularly Suhail Iqbal and Julian Augley, for facilitating data access via the National Safe Haven.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council (ES/S007407/1).