
Abstract
Dental caries in permanent teeth affects over 2 billion individuals globally. Despite declining rates among children, its cumulative impact throughout adulthood remains a challenge. The World Health Organization advocates integrating community water fluoridation (CWF) into health strategies, recognising its role in caries prevention. Recent reviews highlight the need for research examining long-term associations between CWF exposure and dental caries. The island of Ireland provides a natural comparison, as the Republic of Ireland (ROI) has fluoridated public water supplies since 1964, while Northern Ireland (NI) has not implemented CWF. This study examines associations between CWF exposure and dental caries experience in adults with near-lifetime exposure to CWF and assesses whether associations differ across tooth surfaces. Epidemiological, demographic, and sociological data collected from adults in a previous survey were analysed. Caries experience was assessed using the decayed, missing, and filled teeth (D3CMFT) and tooth surface (D3CMFS) indices. The primary analysis estimated associations between region (as a proxy for long-term CWF exposure) and caries experience. Negative binomial regression models, appropriate for overdispersed count data, estimated incidence rate ratios for explanatory variables, including CWF exposure, in relation to dental caries experience. Adults in the ROI exhibited significantly lower caries experience than those in NI. In adjusted analyses, individuals in the ROI had 10.6% and 15.6% lower D3CMFT and D3CMFS scores, respectively. The largest difference was observed on approximal surfaces (18.6%), followed by smooth (14.9%) and occlusal surfaces (11.9%). These findings support an association between long-term CWF exposure and reduced dental caries experience in adulthood. The results provide additional life-course evidence using clinical measures of disease and contribute to the ongoing evaluation of population-level fluoride policies. Alongside contemporary research, these findings may inform public health decision-making regarding CWF and its role in improving oral health outcomes in adult populations.
Introduction
Dental caries remains one of the most prevalent noncommunicable diseases worldwide, with caries in permanent teeth affecting over 2 billion people (Murray et al 2020). Community water fluoridation (CWF), the controlled addition of fluoride to public water supplies, is widely recognised as an effective population-level preventive measure (World Health Organization [WHO] 2024), yet important gaps remain in understanding its long-term associations with caries in adulthood.
Recent systematic reviews (Iheozor-Ejiofor et al 2015, 2024) highlight limitations in the evidence base for CWF, including reliance on studies conducted prior to widespread fluoride toothpaste use (Goldman et al 2008) and limited evidence of effects in adults (Iheozor-Ejiofor et al 2024). Methodological challenges in evaluating CWF exposure in adults are well recognised (Rugg-Gunn et al 2016; Do et al 2017; Moore et al 2024), and the island of Ireland provides a unique population setting for examining long-term exposure.
The Republic of Ireland (ROI) introduced CWF in 1964 (McDonnell et al 2012) and currently reaches approximately 71% of the population (Cronin et al 2021). In contrast, Northern Ireland (NI), part of the United Kingdom, does not fluoridate its water supply (Peakin 2021; British Association for the Study of Community Dentistry 2023), creating a long-standing population contrast in exposure.
Previous oral health surveys conducted in both jurisdictions indicate similar oral health status in the early 1960s (Department of Health 1961; Sheane 1963), prior to the introduction of CWF in the ROI, supporting their comparability for policy evaluation. Subsequent surveys reported improvements in both jurisdictions following the introduction of fluoride toothpaste, but consistently greater reductions in dental caries in the ROI (Todd and Dodd 1985; O’Mullane et al 1986; Todd and Lader 1991; O’Mullane and Whelton 1992; Evans et al 1999; O’Mullane et al 1999; Whelton et al 2006a, 2007). However, variation in study design and outcome measures limits the reliability of direct cross-jurisdictional comparisons.
Caries distribution varies across tooth surfaces, and CWF exposure may differ in its relationship with disease at these sites. Surface-level analyses provide a more sensitive description of long-term disease patterns and may better reflect differences associated with lifetime exposure than aggregate decayed, missing, and filled teeth (DMFT) measures (Chestnutt et al 1996; Batchelor and Sheiham 2004; Hopcraft and Morgan 2006; Stangvaltaite-Mouhat et al 2021).
Few studies have examined adults with near-lifetime exposure using detailed clinical measures. This study examines associations between near-lifetime CWF exposure and dental caries experience in adults, and whether these associations differ across tooth surfaces. It provides a rare opportunity to evaluate adults exposed to fluoridated and non-fluoridated water over much of the life course using clinically assessed outcomes.
The natural policy contrast between the ROI and NI provides a population comparison for examining long-term exposure within broadly comparable social and behavioural contexts, while surface-level analyses extend previous work by characterising how cumulative fluoridation exposure relates to disease patterns across different tooth sites.
Methods
This study used data from a previously unpublished survey of oral health, demographic, and sociological characteristics among adult cohorts from a fluoridated region of the ROI and a non-fluoridated region of NI. Sample size was determined using nQuery Advisor, based on estimates from the Irish National Adult Oral Health Survey (NAOHS) (Whelton et al 2007). A stratified convenience sample of 485 adults (ROI: n = 245; NI: n = 240), aged 34 to 45 years and born between 1961 and 1973, was recruited from similar workplaces in Cork, ROI (fluoridated), and Belfast, NI (non-fluoridated). This WHO index age group captures near-lifetime CWF exposure and accumulated caries experience.
Eligibility required lifetime residence within one jurisdiction on the island of Ireland. Residential histories were linked to CWF status to determine cumulative exposure among ROI participants and confirm non-exposure among NI participants. Halo effects may have affected both populations. However, formal quantitative adjustment for halo exposure was not possible with the available data. Details of the inclusion and exclusion criteria are provided in Appendix Table 1.
Data collection occurred between April 2006 and October 2008. CWF was introduced in Cork in May 1965 (O’Hickey 1972), indicating exposure from early childhood among ROI participants. By contrast, the study cohort in Belfast had no exposure to CWF (Peakin 2021).
Ethical approval for the initial study funded by the Health Research Board (HRB), Ireland (PR060/2001), was granted by the Clinical Research Ethics Committee of the Cork Teaching Hospitals (CREC) in 2003 (Protocol No. OHSRC00703) and the Office of Research Ethics Committees Northern Ireland (ORECNI) in 2006 (Ref: 06/NIR01/31). Approval was renewed by the CREC in 2023 (Ref: ECM3(FFFF), October 24, 2023). The ORECNI confirmed that no further ethical approval was required for this secondary data analysis.
Dental Caries Information
Dental examinations included visual inspection using a mouth mirror, dental light, and a Community Periodontal Index (CPI) ‘C’ probe. Caries was recorded for each tooth surface, with both visual (non-cavitated) and cavitated lesions assessed at the dentinal level of involvement. Reasons for tooth absence were also charted. Coding criteria are available in Appendix Table 2.
Demographic and Sociological Variables
Participants were recruited from clerical and non-clerical staff within public-sector employment. Data were collected on factors known to influence dental caries experience, including age, gender, occupation type, and education level, as well as oral health knowledge and behaviours. Variables included in the analysis are detailed in Table 1. The questionnaire is provided in Appendix Table 3, with binary coding described in Appendix Table 4.
Explanatory Variables Considered in the Analysis.
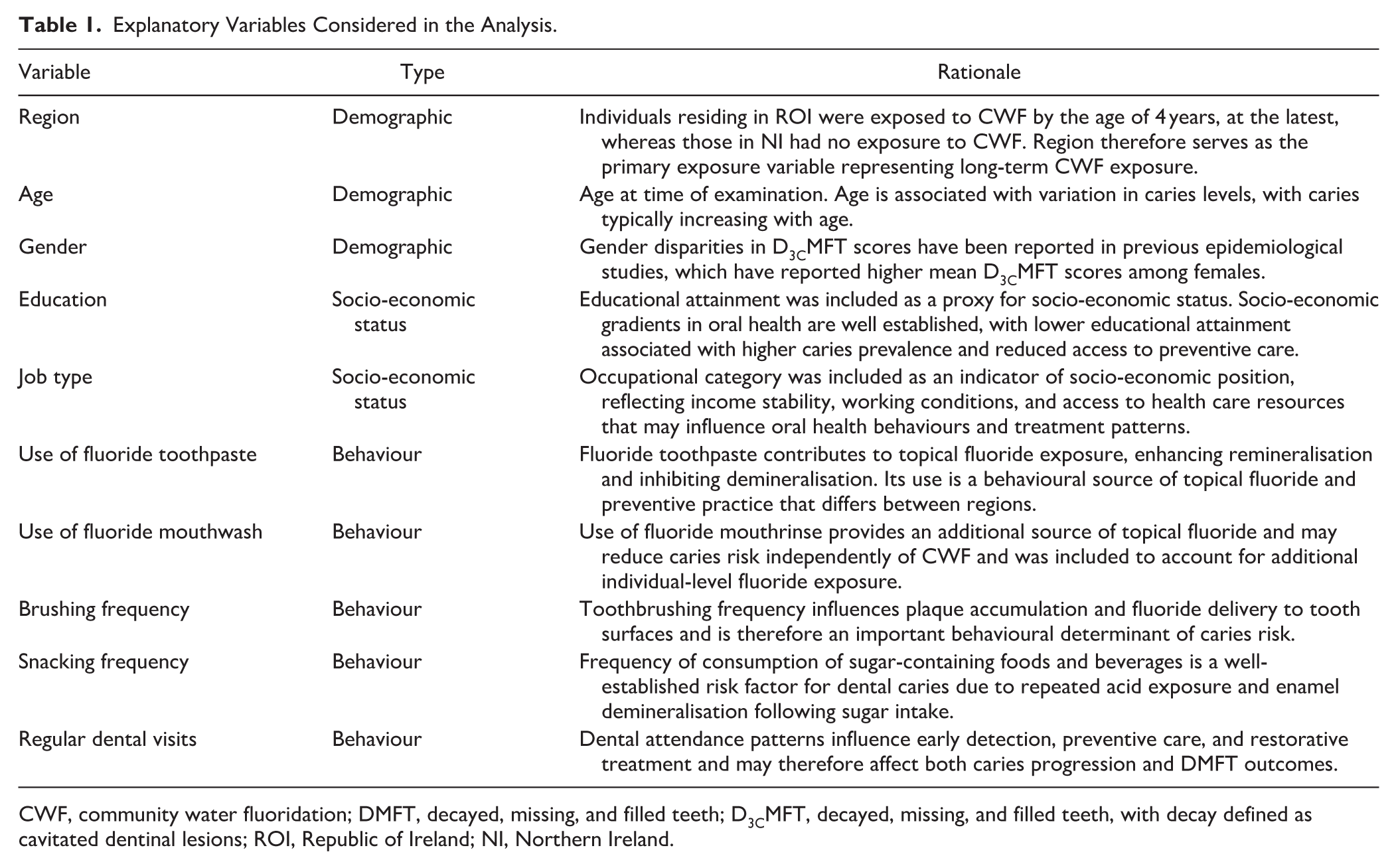
CWF, community water fluoridation; DMFT, decayed, missing, and filled teeth; D3CMFT, decayed, missing, and filled teeth, with decay defined as cavitated dentinal lesions; ROI, Republic of Ireland; NI, Northern Ireland.
Data Analysis
Caries experience was measured using decayed, missing, and filled teeth (D3CMFT) and surfaces (D3CMFS), with decay defined as cavitated dentinal lesions (D3C) only. Third molars were excluded from the analysis (Hopcraft and Morgan 2006; Stangvaltaite-Mouhat et al 2021). Given the bilateral symmetry of caries distribution, corresponding left and right tooth surfaces were combined for analysis. To assess whether associations between CWF and caries varied by site, surfaces were grouped as all surfaces, occlusal, smooth (buccal and lingual), and approximal (mesial and distal) surfaces.
The analysis was designed to estimate associations rather than causal effects. Covariate selection was specified a priori based on relevant literature and a directed acyclic graph (DAG) describing relationships between CWF exposure, socio-demographic characteristics, oral health behaviours, and caries outcomes. Socio-demographic variables (age, gender, education, and occupational class) were treated as baseline confounders of the region–caries association. Behavioural variables (toothbrushing frequency, sugar intake, fluoride toothpaste use, and mouthrinse use) were included in primary models to capture regional differences in preventive practices and individual fluoride exposure. Dental visits were excluded, as the DAG indicated this variable acts as a collider, potentially influenced by both regional context and underlying caries risk, and adjustment could introduce collider bias (Appendix Fig. 1).
Primary negative binomial models adjusted for socio-demographic and behavioural covariates. Sensitivity analyses using propensity score–stratified models, restricted to the socio-demographic confounder set, assessed whether the regional association was robust to adjustment for baseline confounding alone. Behavioural variables were conceptualised as potential mediators or proximal determinants of caries and included to estimate the region–caries association conditional on preventive practices, while propensity score models adjusted only for baseline socio-demographic confounders.
Model diagnostics evaluated the adequacy of the negative binomial specification and overall model fit, including Pearson-based dispersion, variance inflation factors (VIF), and simulation-based residual diagnostics.
Results
Descriptive Statistics
Individuals with missing data were excluded from the analysis. The final sample comprised 474 individuals (ROI: n = 239; NI: n = 235). Participants in the ROI had been exposed to CWF from age 4 at the latest, 37.2% had lifelong exposure to CWF, and 69.5% had exposure for more than half of their lives. Formal comparisons by exposure duration were not undertaken. Participants in the ROI were aged 34.2 to 44.8 years (mean 39.6 years), while NI participants with no CWF exposure were aged 34.9 to 44.9 years (mean age 39.7 years).
The cohort was predominantly female (ROI: 61%; NI: 63%) and included a high proportion of participants with third-level education (ROI: 62%; NI: 54%). Job types were similar across regions, with approximately half in clerical roles (ROI: 48%; NI: 49%). Routine dental attendance differed, with 60% of adults in the ROI reporting regular dental checkups compared with 82% in NI, but this was not associated with caries outcomes in univariate analyses. Demographic and sociological characteristics by region are presented in Appendix Table 5.
Caries outcomes revealed a mean D3CMFT of 10.54 in the ROI and 11.98 in NI, with no significant regional differences in the proportional contribution of decayed, missing, and filled components. Similar patterns were observed for mean D3CMFS scores (ROI: 26.85; NI: 32.75), with higher values in the maxillary arch (ROI: 14.72; NI: 18.26) than in the mandibular arch (ROI: 12.14; NI: 14.10). Molars exhibited the highest caries levels (ROI: 17.91; NI: 20.29), followed by premolars (ROI: 5.98; NI: 8.71).
At the tooth level, first molars showed the highest decay experience (D3CMFS) (ROI: 11.87; NI: 12.71), followed by second molars (ROI: 6.04; NI: 7.58). Canines had the lowest caries levels (ROI: 0.40; NI: 0.60), followed by the lateral (ROI: 1.09; NI: 1.37) and central (ROI: 1.48; NI: 1.78) incisors, respectively. Full details are provided in Appendix Tables 6 to 10.
Caries distribution across surface types was similar in both cohorts. Occlusal surfaces were most affected, accounting for 33% of the total D3CMFS score and representing 38% of the D3CMFS score for molars and premolars in the ROI. Similarly, in NI, these figures were 32% and 36%, respectively. Distal (ROI: 18.4%; NI: 19.6%), mesial (ROI: 18.3%; NI: 19.0%), and lingual (ROI: 15.6%; NI: 15.9%) surfaces followed, with buccal surfaces showing the lowest susceptibility, contributing approximately 14% to the total D3CMFS score in both regions. An overview of caries distribution by tooth and surface type is presented in Appendix Figures 2 to 5.
Results of the Regression Analyses
Tables 2 and 3 present selected outputs from the regression models. Coefficients were exponentiated and reported as incidence rate ratios (IRRs). The “Adjustment” column indicates the percentage change in the expected rate of caries relative to the reference case for categorical variables and per 1-unit increase for continuous variables.
Binomial Regressions—DMFS.
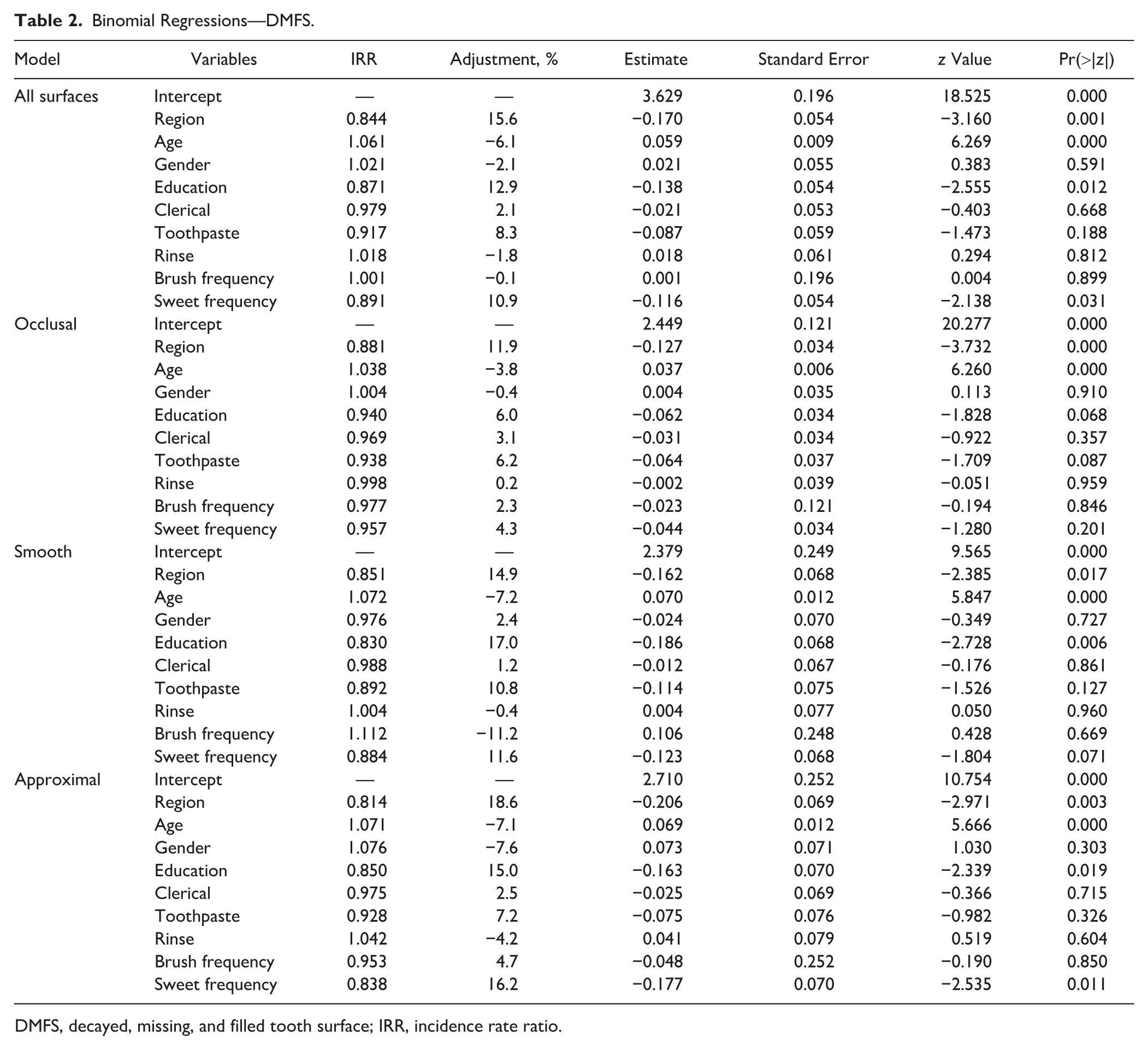
DMFS, decayed, missing, and filled tooth surface; IRR, incidence rate ratio.
Binomial Regression—DMFT.
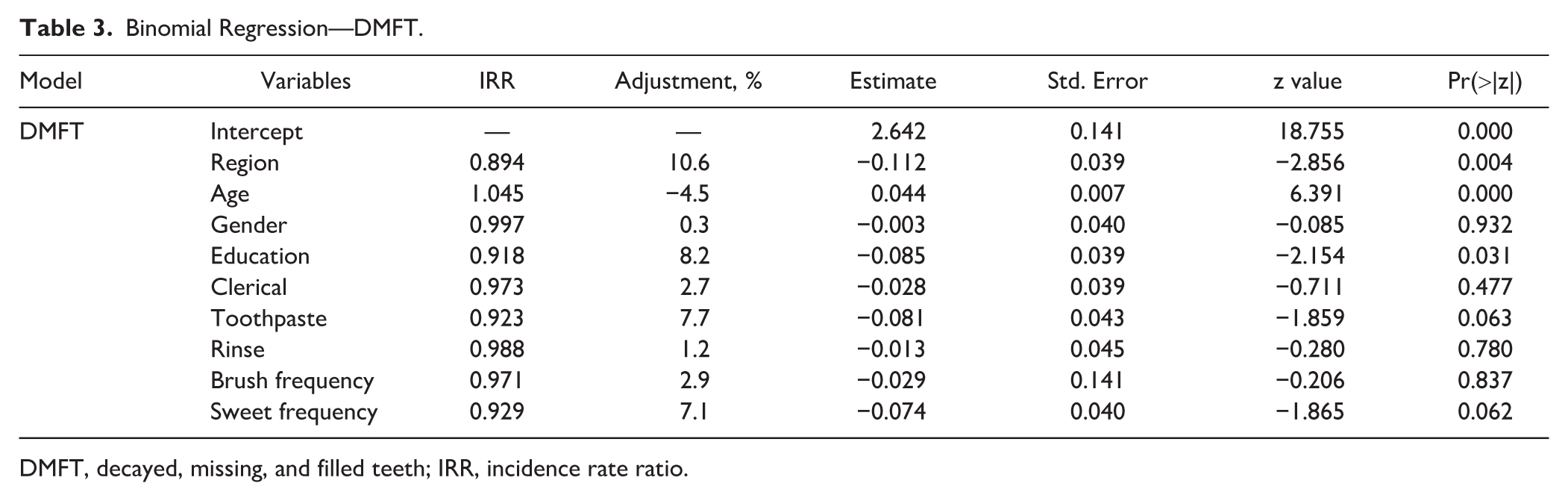
DMFT, decayed, missing, and filled teeth; IRR, incidence rate ratio.
In each model, the reference individual was defined using the baseline categories in the regression specification: residing in NI (Region = 0; non-fluoridated), age at the sample mean (grand mean-centered), male (Gender = 0), non-third-level education (Education = 0), non-clerical occupation (Clerical = 0), not always using fluoride toothpaste (Tooth paste = 0), not using fluoride mouth rinse (Rinse = 0), brushing less than daily (Brush frequency = 0), consuming sugar-containing foods or beverages at least once daily (Sweet frequency = 0), and reporting reactive dental attendance (Reason = 0). Percentage differences reported below are derived from adjusted IRRs.
The analysis showed that region of residence and age were consistently associated with all caries outcomes. After adjustment, adults in the ROI with near-lifetime exposure to CWF had 15.6% fewer carious surfaces compared with those in NI, with the largest reductions observed on approximal surfaces (18.6%), followed by smooth (14.9%) and occlusal (11.9%) surfaces.
Each additional year of age above the sample mean was associated with a 6.1% increase in caries, with greater increases on smooth (7.2%) and approximal (7.1%) than occlusal (3.8%) surfaces.
Educational attainment and frequency of sugar consumption showed less consistent associations. Tertiary education was associated with 12.9% lower caries levels overall, with significant reductions for smooth (17.0%) and approximal (15.0%) surfaces, while the association for occlusal surfaces was smaller and non-significant (6.0%, P = 0.068). Consuming sugar-containing foods or beverages less than once daily was also associated with lower caries (10.9%), with a significant reduction on approximal surfaces (16.2%), whereas associations for smooth (11.6%, P = 0.071) and occlusal (4.3%, P = 0.201) surfaces were not significant.
For D3CMFT, individuals with near-lifetime CWF exposure had approximately 10.6% fewer carious teeth than those with no exposure. Each additional year of age was associated with a 4.5% increase in caries experience. Tertiary education was associated with an 8.2% lower caries level, while less frequent consumption of sugar-containing foods and beverages showed a non-significant inverse association (7.1%, P = 0.062).
Model diagnostics indicated an adequate fit of the negative binomial models. Pearson dispersion ratios were close to unity across all models (range: 0.954–1.013), with no evidence of residual overdispersion (Table 4). Multicollinearity was low (maximum variance inflation factors <1.30 in all models), and residual diagnostics (DHARMa) did not indicate violations of model assumptions.
Regression Diagnostics—DMFS and DMFT.
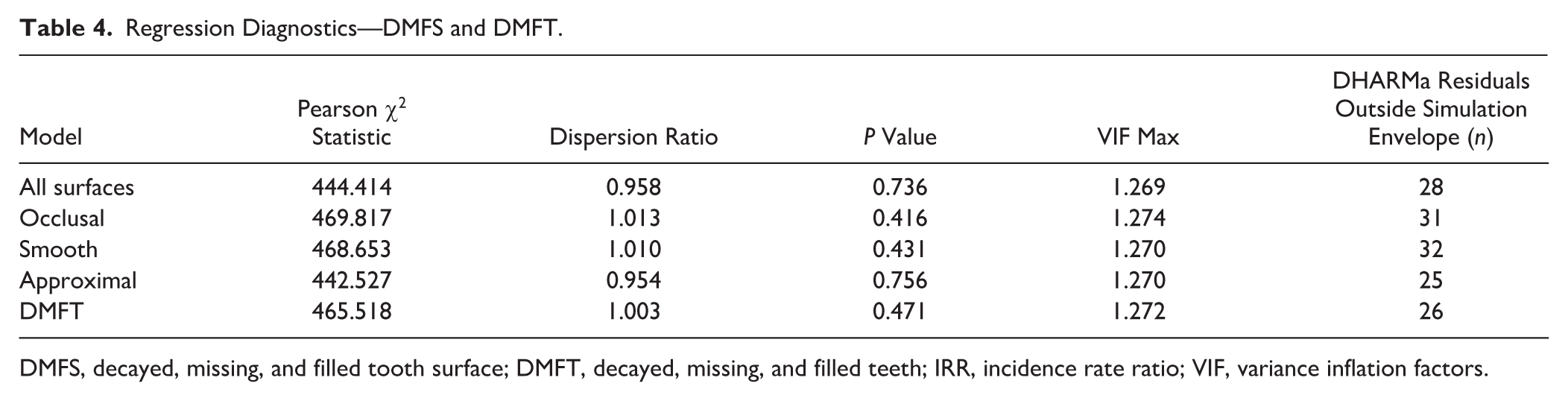
DMFS, decayed, missing, and filled tooth surface; DMFT, decayed, missing, and filled teeth; IRR, incidence rate ratio; VIF, variance inflation factors.
Univariate negative binomial models indicated that residence in the ROI was associated with lower caries outcomes compared with NI across all outcome measures (Appendix Table 11). Unadjusted estimates indicated reductions of approximately 12% to 22% in caries experience, depending on the outcome and surface grouping.
Sensitivity analyses using propensity score–stratified negative binomial models were conducted to assess the robustness of the primary multivariable findings (Appendix Table 12). Estimated regional IRRs were highly consistent with the primary models, with minimal attenuation of effect sizes and overlapping confidence intervals across outcomes. The consistency between the full multivariable and confounder-only propensity score models suggests that socio-demographic differences alone do not account for the observed regional association.
Discussion
Few datasets provide clinically assessed outcomes among adults with near-lifetime exposure to fluoridated or non-fluoridated water. This analysis therefore offers a rare opportunity to examine long-term associations between CWF and dental caries in comparable neighbouring populations. As a population-level intervention, CWF is most appropriately assessed through community comparisons. This policy contrast approximates a natural experiment, although causal inference remains limited and residual confounding cannot be excluded.
Adults aged 34 to 45 years in the ROI, with near-lifetime exposure to CWF, exhibited lower dental caries experience than their counterparts in non-fluoridated NI, with D3CMFT and D3CMFS levels approximately 10.6% and 15.6% lower, respectively. These findings align with previous research linking lifetime CWF exposure to lower caries levels, even in the presence of multiple fluoride sources (Hopcraft and Morgan 2005; Whelton et al 2007; Slade et al 2013; Crocombe et al 2014; Peres et al 2016). Potential halo effects may have attenuated regional differences, suggesting the observed association is likely conservative.
A recent retrospective cohort study using NHS dental claims data in England reported a modest (~2%) reduction in DMFT associated with CWF exposure in adults (Moore et al 2024). Differences in effect size likely reflect variation in exposure assessment, outcome measures, and study context. Administrative datasets capture treated disease, whereas the present study used clinical indicators of cumulative caries experience. These approaches provide complementary evidence and should be interpreted within their methodological contexts.
Across tooth surfaces, the strongest associations between CWF and caries were observed on approximal surfaces (18.6%), followed by smooth (14.9%) and occlusal (11.9%) surfaces. This pattern is consistent with previous research on surface susceptibility and preventive exposure, with stronger fluoride associations typically reported for approximal and smooth than for occlusal surfaces (Chestnutt et al 1996; Batchelor and Sheiham 2004; Hopcraft and Morgan 2006; Stangvaltaite-Mouhat et al 2021; Moores et al 2022).
Age was also associated with caries experience, with each additional year above the mean age corresponding to a 4.5% and 6.1% increase in D3CMFT and D3CMFS, respectively. This relationship has been reported previously (Hopcraft and Morgan 2006; Krustrup and Petersen 2007; Whelton et al 2007; Sheiham and Sabbah 2010; Slade et al 2013). However, the relatively narrow age range of the sample limits generalisation, and future studies, including broader age groups, could assess whether this association is linear across adulthood.
Educational attainment, used as a proxy for socio-economic status, was the socio-economic factor most strongly associated with caries outcomes. D3CMFT and D3CMFS were lower among individuals with third-level education, by 8.2% and 12.9%, respectively. This social gradient is consistent with previous research linking lower educational attainment to higher DMFT (Hopcraft and Morgan 2005; Aldossary et al 2015) and DMFS (Hopcraft and Morgan 2006; Krustrup and Petersen 2007) scores.
Individuals reporting infrequent sugar consumption had 7.1% and 10.9% lower D3CMFT and D3CMFS scores, respectively, than those who consumed sugar more frequently. Although the association with D3CMFT was weak, the pattern is consistent with extensive evidence linking sugar consumption to caries in both child (Whelton et al 2006b; Sheiham and James 2014; Ha et al 2021) and adult populations (Whelton et al 2007; Oscarson et al 2017).
Gender was not significantly associated with any grouped surface outcomes or with D3CMFT. This aligns with findings from previous research (Hopcraft and Morgan 2006; Whelton et al 2007; Demirci et al 2010). However, some studies report higher levels of caries among women (Krustrup and Petersen 2007; Slade et al 2013), highlighting the need for further investigation.
The survey design addressed key challenges in assessing CWF exposure and caries outcomes in adults. Caries experience reflects behavioural, social, and environmental influences, including fluoride exposure (Do et al 2017; Moore et al 2024). The neighbouring populations recruited for the ROI/NI survey shared broadly similar demographic and socio-cultural characteristics but differed in lifetime CWF exposure.
Previous studies have highlighted the challenges of reconstructing accurate residential histories in adults, particularly over long recall periods (Do et al 2017; Spencer et al 2017; Moore et al 2024). In the ROI/NI survey, residential histories were mapped and linked to water supplies to support exposure classification. To reduce misclassification, the analysis was restricted to individuals who had resided exclusively within either ROI or NI throughout their lives.
The age of the data is an important limitation. Although collected between 2006 and 2008, the dataset had not previously been analysed to examine near-lifetime CWF exposure in relation to adult caries. Renewed policy interest in CWF prompted this analysis to address evidence gaps regarding long-term CWF exposure and adult caries outcomes. This is timely given recent national data from England showing a reversal of earlier improvements in adult oral health, with a marked increase in caries prevalence between 2009 and 2023 (Office for Health Improvement and Disparities 2025), alongside renewed CWF policy discussions in the United States. Although oral health in high-income countries has changed over the past two decades, and absolute caries levels may not be generalisable to current populations, this dataset enables comparison of adults with and without near-lifetime CWF exposure. Tightly defined exposure groups with detailed clinical, residential, and behavioural data are uncommon in adult populations (Slade et al 2013; Rugg-Gunn et al 2016; Do et al 2017; Spencer et al 2017; Moore et al 2024).
The study population was not representative of the general populations in either ROI or NI, as participants were recruited from comparable workplace settings. Caution is therefore required when generalising the findings beyond this demographic. A further limitation relates to the ceiling effect of the DMFT index, particularly its missing component (Do et al 2017; Moore et al 2021). As this is a cross-sectional analysis, the findings should be interpreted as associations rather than causal effects. Nevertheless, the comparison provides additional evidence consistent with lower observed caries levels among individuals exposed to CWF. These findings provide clinically detailed, life-course evidence on long-term CWF exposure, complementing contemporary administrative and cohort studies and helping to contextualize long-term oral health patterns across adulthood.
Conclusion
This analysis indicates that adults aged 34 to 45 years in the ROI, with near-lifetime exposure to CWF, had lower dental caries experience than their counterparts in non-fluoridated NI, despite exposure to multiple fluoride sources. Exposure was consistently associated with caries outcomes across the variables assessed.
These findings align with existing evidence reporting associations between long-term fluoridation and lower caries levels in adults and provide complementary life-course evidence to inform ongoing public health policy evaluation of CWF and efforts to improve oral health outcomes.
Author Contributions
J. Cronin, contributed to conception and design, data analysis and interpretation, drafted and critically revised the manuscript; S. Moore, contributed to design, data analysis and interpretation, critically revised the manuscript; N. Woods, contributed to conception, data analysis and interpretation, critically revised the manuscript; H. Whelton, M. Harding, contributed to conception, data acquisition and interpretation, critically revised the manuscript. All authors gave their final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345261442955 – Supplemental material for Long-Term Associations between Water Fluoridation and Adult Dental Caries
Supplemental material, sj-docx-1-jdr-10.1177_00220345261442955 for Long-Term Associations between Water Fluoridation and Adult Dental Caries by J. Cronin, S. Moore, N. Woods, H. Whelton and M. Harding in Journal of Dental Research
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study used data from the HRB-funded survey “Oral Health of Employed Adults and Its Impact on Quality of Life in the Republic of Ireland and Northern Ireland” (2006–2008). No additional funding was received for this manuscript.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.