
Abstract
There is limited evidence to support optimal patient-centered management for compromised first permanent molars (cFPM) in children. Based on an online discrete choice experiment (DCE), this study elicits UK adult general population preferences and calculates willingness to pay (WTP) for pathways to manage cFPM. The DCE was designed with information from semistructured interviews and literature reviews, as well as focus groups with an expert panel of dentists, citizens, and policy makers. A statistically optimal D-efficient design generated 18 choice tasks, split across 2 blocks. Each respondent answered one block of 9 tasks to reduce survey fatigue. Choice tasks varied across 5 attributes: type of treatment, provider of care, who makes the management decision, number of future visits avoided, and cost. An opt-out was included (no treatment). Conditional logit models (fixed effects) were used for data analysis, and marginal WTP for each attribute level was calculated. An overall 430 respondents completed the DCE. Respondents valued children receiving care as compared with not. Restoring a cFPM was valued equally to spontaneous or orthodontic gap closure. In contrast, having a partial gap, prosthetic replacement with a bridge, or a full unit gap was valued less than restoration or full gap closure. General dentists were preferred to dentists with enhanced skills, but there was no evidence of a preference for general dentists over specialists in pediatric dentistry. Respondents preferred to be wholly or partly involved in the decision-making process as opposed to the dentist making the decision alone. Respondents preferred less costly treatments and the avoidance of future dental work. Dental care service providers must consider service user preferences for health and nonhealth outcomes in any service redesign. Furthermore, the results provide marginal WTP estimates that can be used to value dental care services.
Keywords
Introduction
Optimal management of compromised first permanent molars (cFPMs) in children is complex and can be categorized, at a high level, into restoration or extraction; however, insufficient evidence exists to suggest superior effectiveness of either option (Taylor et al. 2019; Lygidakis et al. 2022). In children, the most prevalent carious tooth is the first permanent molar, with the most recent national UK child dental health survey reporting this to be 25% by age 15 (Pitts et al. 2015). cFPMs significantly affect children, as pain, eating difficulties, sleep loss, disruption of daily activities, and time off school are reported (Taylor et al. 2018). Children, carers, and the public have preferences, each accruing costs to the family, health service, and broader society. Clinical and policy changes need to incorporate preferences of service users or those contributing indirectly—for example, through taxation in addition to effectiveness and costs (NICE 2022).
Valuing health care is critical to determine how best to allocate resources within a fixed health care budget. Discrete choice experiments (DCEs) are a widely accepted preference elicitation method used to value health (de Bekker-Grob et al. 2012), although their use in dentistry remains limited (Barber et al. 2018). Alternatively, contingent valuation methods could be used to elicit preferences and/or establish a willingness to pay (WTP; Ryan et al. 2008). Contingent valuation methods are useful when clinical or nonclinical outcomes are known, but they are not suited to situations where aspects of the process or outcomes of care vary or are being simultaneously determined. Contingent valuation methods are arguably less desirable in establishing WTP due to an increased incidence of protest zero bids or implausibly high valuations (Ryan et al. 2008). DCEs are underpinned by the theories of demand (Lancaster 1966) and random utility (McFadden 1974). These state that any goods or services can be described by a set of characteristics and that the utility (value) of any health care good or service is equal to the sum of the values attached to its underlying characteristics (attributes; Lancsar and Louviere 2008). DCEs value the characteristics of goods or services and comprise several sequential scenarios (choice tasks), with respondents making choices between 2 or more alternatives, each of which is described in terms of the same attributes. What differs between the alternatives is the levels that these attributes might take. Combining respondents’ answers across multiple choice tasks permits the relative importance of the levels of each attribute to be estimated. Including a cost attribute (Lancsar and Louviere 2008) enables marginal WTP (mWTP) values to be estimated for changes in each attribute level.
Currently, there is no DCE that explores population preferences and mWTP for cFPM. The aim of this study was to elicit UK general population preferences and WTP for pathways to manage cFPM.
Methods
The study was conducted in accordance with best practice guidance (Reed-Johnson et al. 2013; Hauber et al. 2016). Reporting conformed to accepted recommendations (Bridges et al. 2011). Favorable ethical opinion was obtained from the North of Scotland Research Ethics Service (20/NS/0124; 22/10/2020).
Attribute and Level Selection
Attributes and levels (Table 1) were identified by the following: initial analyses of 5 semistructured interviews with the public, focused literature searches (Appendix Method), expert panel opinion (comprising academics, clinicians, patients, and policy makers), and research team discussions. Expert panel opinion validated attributes and agreed levels (Appendix Table 1).
Final List of Attributes and Levels Included in the Discrete Choice Experiment.

A nonspecialist dentist who has a specialist interest in providing pediatric dentistry.
Experimental Design
There were 486 combinations (6 × 34) of attributes and levels, leading to 117,855 unique choice tasks. An effects-coded D-optimal experimental design was created with Ngene (ChoiceMetrics 2012), reducing the number of choice tasks to 18. Prior coefficient values were not readily available and assumed to be zero. The 18 choice tasks were blocked into 2, to minimize participant burden, with respondents being randomized to answer only 1 block of 9 choice tasks. Attribute and level balance checks confirmed that each attribute level appeared with the same frequency in choice tasks across each block. Each choice task consisted of 2 dental care packages and a “no treatment” alternative. To assess the rationality of responses, an additional 2 choice tasks were added to each block (a consistency test and a dominance test). Following best-practice recommendations, responses to validity tasks were not included in the final analyses. However, respondents who failed these were not excluded from the estimation sample. Pass rates for the tests are reported for comparison with other studies.
Questionnaire Layout
Specific details on the questionnaire layout, including the full online questionnaire and nested methodological experiment, are available in Appendix Methods 1 and 2 and Appendix Figure 1.
Data Collection: Sample and Setting
Based on the sample size calculation
The DCE was a self-administered online survey, disseminated to a nationally representative sample of the UK adult population by an established online panel hosted by National Centre for Social Research (NATCEN). NATCEN was asked to obtain 430 respondents. Respondents were invited by NATCEN during a 6-wk period between October and November 2021 and were reimbursed for their participation. Intermittent checking was carried out to ensure that the required 430 completed responses were obtained. Targeted efforts were made to increase responses of underrepresented characteristics identified during the intermittent checking. The number of respondents invited to complete the survey was likely >430. Obtaining an exact number is not feasible, as the panel size can fluctuate on a daily basis and NATCEN does not record how many panel members viewed the opportunity to take part in this survey. The final sample exceeded the minimum 112 needed to permit interaction analyses (Appendix Method 3, Appendix Tables 2–4). Timers (minimum 30 s/page) were included to ensure that respondents spent sufficient time reading each page. Data collection was conducted by NATCEN using Qualtrics software (version 2021).
Data Analysis
A conditional logistic regression analysis (fixed effects) in Stata 17 (StataCorp 2021) estimated preferences (utility) for different processes and outcomes of care (service attributes and levels) in the population. In DCE analysis models, the observable component of utility within a random utility framework is determined by a linear additive function of the utility derived from opting into care (the model’s alternative-specific constant term) and the utility gained from the attribute levels, with each coefficient representing the impact of that attribute level on preferences. An error term is added to capture variation in preferences not explained by the model. Data were dummy coded, with each coefficient representing the impact of that attribute level as compared with the reference level on preferences (Bech and Gyrd-Hansen 2005).
Model coefficients were estimated on the logit scale to allow calculation of marginal rates of substitution between each attribute level and cost (also the mWTP). Specifically, the mWTP for each attribute level was derived by dividing the coefficient of 1 attribute level by the negative coefficient of the cost attribute, mWTPk = −βk/βcost (Mott et al. 2020).
Results
In total, 430 respondents completed the survey. Internal validity was good, with 75.6% (n = 325) and 91.4% (n = 393) passing the consistency and dominance tests, respectively. There was no evidence of serial nontrading (i.e., always choosing option A or B). Of the 4730 choice tasks completed by the entire sample (11 × 430), the opt-out choice of no treatment was chosen in 1.64% (n = 78) of tasks.
Demographics, oral health characteristics, and anxiety levels are shown in Table 2 and Appendix Tables 5 and 6. The sample was fairly representative of the UK population, as age, gender, ethnicity, household composition, and main economic activity were similar to the most recently available and comparable census data (Office for National Statistics 2021b). The same was found for the total average monthly income per household (Office for National Statistics 2021a). Unfortunately, no robust data source exists to confirm political party identification.
Respondent Characteristics (N = 430).
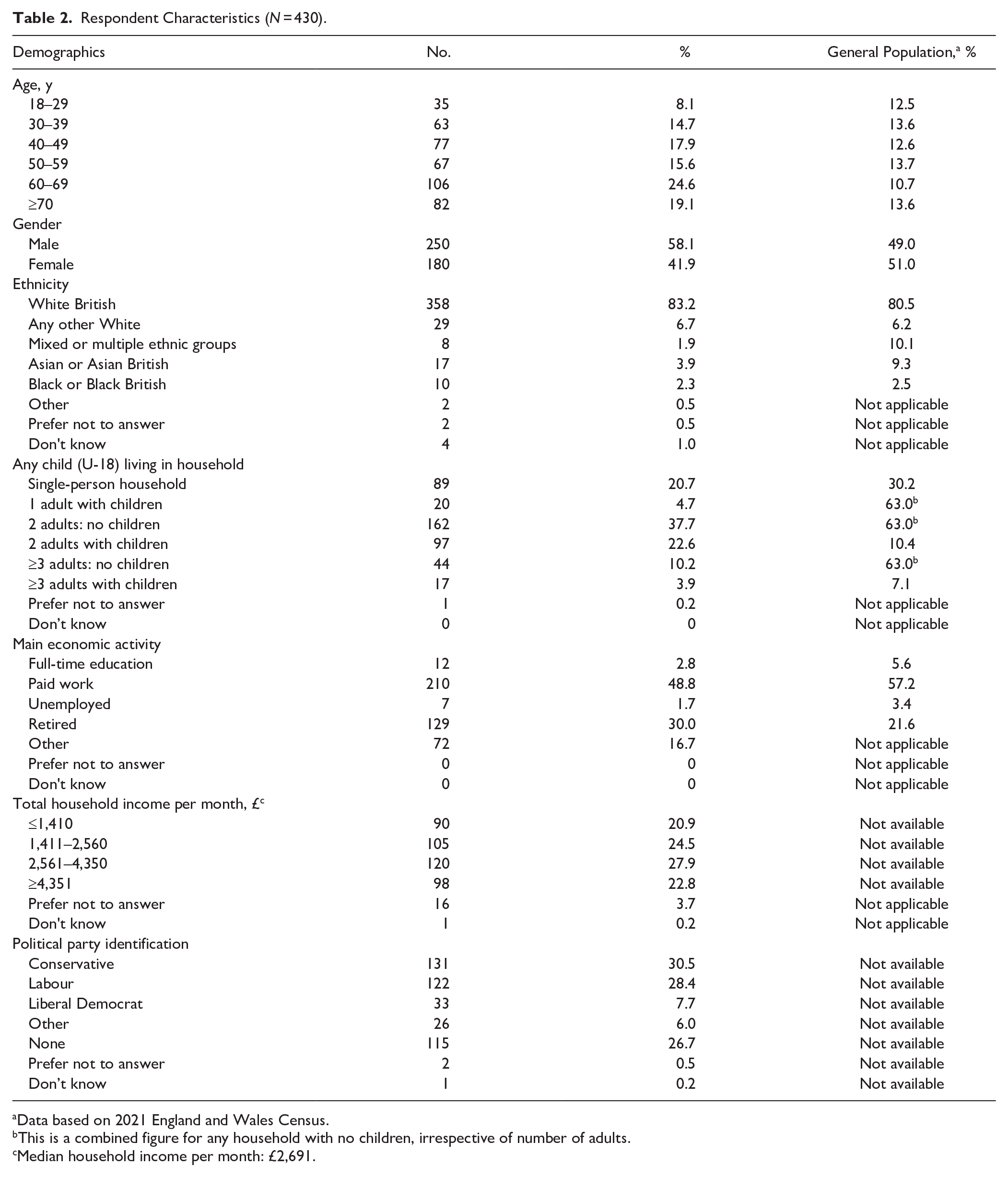
Data based on 2021 England and Wales Census.
This is a combined figure for any household with no children, irrespective of number of adults.
Median household income per month: £2,691.
The results are shown in Table 3. The negative and positive coefficient signs indicate preference of lower and higher levels of an attribute, respectively. The size of the coefficient in isolation provides little meaningful information, as coefficients are designed to be interpreted relative to one another. The alternative-specific constant has a positive coefficient, indicating that the general population prefers to manage cFPM, as compared with not, with a WTP of £5,068 (95% CI, £4,545.92–£5,591.56; P < 0.001). The negative cost coefficient (−0.000843) suggests that if all other attributes are held constant, the public prefers packages of care that cost less, which also demonstrates theoretical validity. An example of how a hypothetical package of care would be valued is shown in Appendix Method 5.
Regression Analysis Including Mean WTP in Great British Pound Sterling.
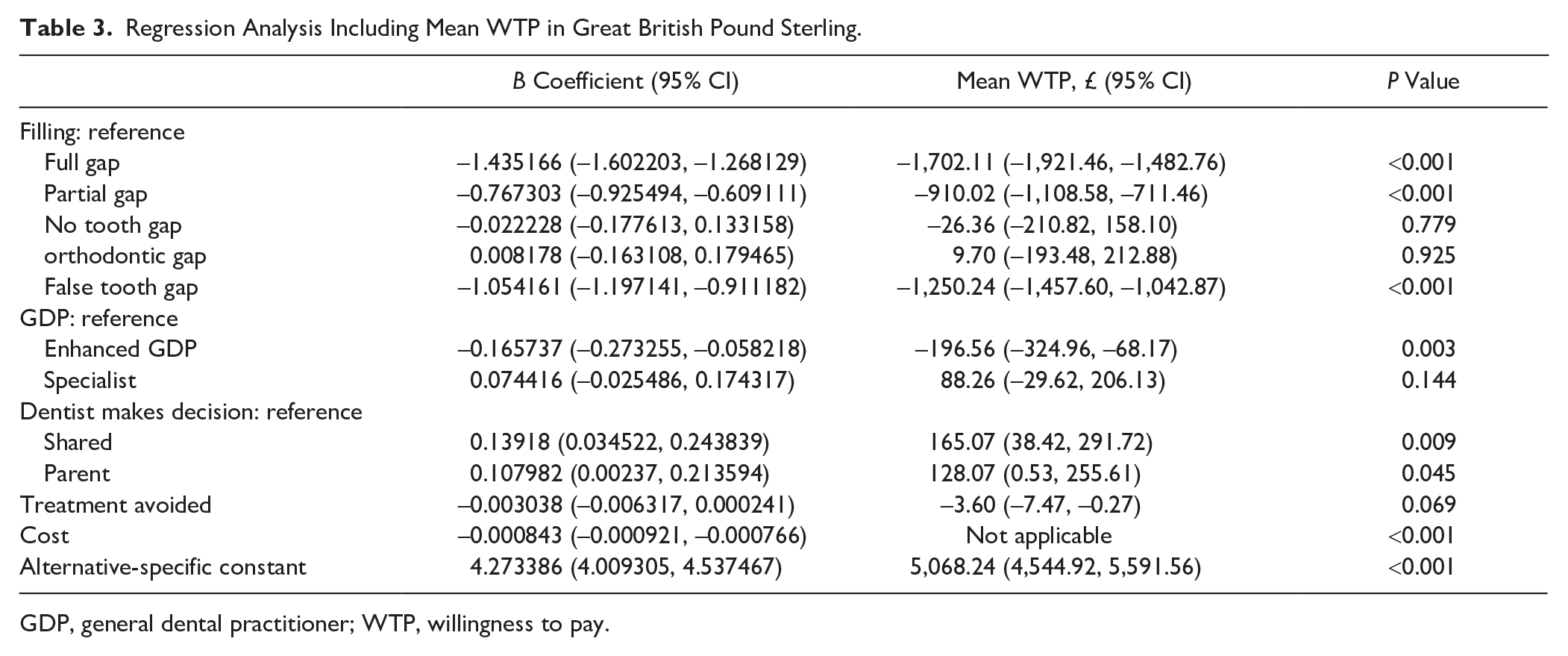
GDP, general dental practitioner; WTP, willingness to pay.
Discussion
This is the first study to use a DCE to elicit public preferences for managing cFPM in children. The public prefers to manage cFPM than not.
There was no evidence of a preference for a cFPM being either restored or extracted where the space is closed naturally by mesial migration or orthodontically. Respondents value a management strategy that results in a functioning unit with no gap. Considering the potential outcome and sequalae of these options, deciding whether restoration or extraction is the optimal option remains a challenge (Taylor et al. 2019; Lygidakis et al. 2022). In contrast, having a partial gap, prosthetic replacement, or a full unit gap is valued less in decreasing order. The functional impairment and reduced oral health–related quality of life following tooth loss could explain preferences. Alternatively, it could be the negative aesthetic consequences of having a gap. Negative oral health–related quality of life due to missing teeth does appear to be more prominent with anterior teeth and, to a much lesser extent, molar teeth (Tan et al. 2016).
Previous dental experience and dental anxiety had a mixed effect on preferences. Anxiety about having a filling, as well as experience with fillings and extractions, did not influence preferences. In contrast, being anxious about having an extraction significantly influenced the need for perfect closure, making it more desirable. It could be that extraction anxiety invokes the need for the most favorable outcome as a reward for overcoming this fear. Patients who had previous orthodontic treatment showed a higher preference for orthodontic gap closure. It could be that orthodontic treatment was perceived as socially acceptable with an assumption of consistent treatment success. In reality, complete orthodontic closure following cFPM extraction is not guaranteed.
In the UK NHS system, restoring or extracting a cFPM for a child accrues the same NHS fee with no out-of-pocket costs to the parent for either option. Although the fee accrued is the same, the cost to deliver both options and their perceived effectiveness among providers do differ (Osborne et al. 2023). There is a risk that these factors influence which treatments are offered or provided for cFPM, overriding preferences.
Patient-centered care approaches to decision making were valued by the public. It is unlikely that a parent will make health care choices without input from a health care professional. In the United Kingdom, there have been efforts to push a theoretical shift away from paternalistic models toward shared decision making, promoting discussions and joint decisions between service users and health care professionals about the care that they should receive (NICE 2021). Shared decision making for cFPM is vital, given the lack of superior clinical effectiveness of any particular option (Lygidakis et al. 2022) and the equal value placed on the main treatment options.
The extent to which health care professionals involve service users, in particular children, in decision making remains low (Driever et al. 2022). Professionals may not actively acknowledge or seek patient views, and patients may be unsure of engaging in a shared decision (Driever et al. 2022). Dental professionals need to encourage shared decision making, ensuring that all options, where appropriate, are offered. Providing information such as appropriate risks and benefits permits the young person and/or parents to decide what they want to do, allowing them to incorporate their values. A recent qualitative study with young people, parents, and adults in managing cFPM reinforces the inclusion of the views, values, and opinions of all stakeholders and certainly those of the young person (Taylor et al. 2024). Actively including young people in shared decision making could be challenging for dental professionals (Coyne et al. 2014). Bespoke training and emphasis on shared decision making with children and parents across undergraduate dental curricula would be required to develop this.
A preference for care to be provided by a general dental practitioner (GDP) or specialist in pediatric dentistry was expressed, with the public valuing them equally. The public values the relationship that it has with its GDPs, while balancing the additional value of being managed by a specialist against the trust and familiarity of GDPs. Alternatively, the extra value of a specialist may not be understood, and the public is equally happy to see either. In contrast, being managed by a dentist with enhanced skills (DES) was valued less. Prior experiences could explain this, or alternatively, DESs were not understood by respondents. DESs are suggested as important for future service provision, given that they can provide expedited access to more “specialized services” closer to home, reducing hospital referrals (NHS England 2015). Integration into the dental workforce and future policies need increased public education to mitigate any concerns or confusions that patients appear to have.
No evidence existed that the public preferred a package of care that avoided additional future treatment visits. This suggests that the emphasis is on the short-term outcome (i.e., the gap being closed or not), instead of the process saving future appointments. Alternatively, there may be a genuine disinterest in avoiding future appointments. Outcomes or events that occur in the future are known to be commonly valued less than those occurring in the present (Claxton et al. 2011). Individuals are expected to make choices by balancing risk for consequences with benefits of action (Ferrer and Klein 2015). The perceived present and future uncertainties around care and costs might explain why individuals prefer to have money and certainty now rather than later. Alternatively, respondents may have been unable to conceptualize 33 future treatment visits. Anecdotally, only a small proportion of respondents may have experienced this number of intervention visits; however, the number of reported episodes of treatment is known to be greater in older adults (Morris et al. 2011).
It was assumed that respondents with higher monthly incomes would be less concerned about the cost attribute. In this DCE, this was not the case, contradicting other WTP studies suggesting that higher income correlates with higher WTP (Tan et al. 2017). Cost might not be important to the public when considering an intervention in children. In nondental health studies, the link between household income and parental health-related behaviors (e.g., decision making) has mixed effects on child health outcomes (Cooper and Stewart 2021).
We acknowledge that DCE tasks are based on hypothetical choice questions and that children’s treatment under the NHS is not paid for directly by the parent. Respondents may not fully consider their ability to pay when making choices. As DCEs are hypothetical, participants are not duty bound by their choices, so an over- or underestimation of WTP could be obtained (Clark et al. 2014). Training materials, such as explicit reminders for respondents to consider their budget constraints (as was the case in this study), can lessen this by attempting to contextualize the hypothetical nature of DCEs (Vass et al. 2020). Cost attributes were realistic to encourage trading in both an NHS context and a private context; however, they were not so high that respondents were likely to automatically make a choice based on price alone (Clark et al. 2014). Concerns were not raised about the plausibility of salience of the cost attribute during think-aloud pilot interviews. Similarly, the nested methodological experiment identified no evidence that choices were based on price alone, as those who were given the high-cost DCE example were not any more sensitive to cost than those who given the low-cost example (P > 0.05). While explicitly testing for hypothetical bias was not feasible, the results, including pilot analyses, showed a cost attribute with a magnitude and direction of effect on the utility function that was aligned with a priori expectations. Using the results of the DCE to estimate marginal WTP provides a means to establish value in a situation where respondents had existing NHS coverage and were not directly paying for care. As such, marginal WTP values provide the means to conduct cost-benefit analyses relevant to the NHS perspective.
There were strengths and limitations to this study. The sampling framework was a strength as using NATCEN, a robust online panel, ensured sufficient representativeness of the UK population. However, it did pose some challenges. A selection bias could have been introduced as panel members were able to choose whether to complete the survey or not. Yet, NATCEN hosts a probability-based research panel (panel members are recruited at random rather than being based on a nonrandom convenience sample), which minimizes the impact of this potential bias, more so than dissemination via dental clinics or social media platforms. Offline representation was not possible due to the impact of COVID-19. Specific population groups were underrepresented, not uncommon with this approach (Hays et al. 2015). Respondents may be regular survey completers and motivated to complete surveys quickly and without due consideration to gain the reward; thus, answers may not reflect true preference (Hays et al. 2015).
Combining qualitative interviews, expert opinion, and a literature review to develop attributes and their levels was a strength. This reduced the risk of including attributes that are important to respondents who complete it. Including “decision making” in this DCE was novel, with no previous dental DCE studies using this as an attribute (Barber et al. 2018). Validity checking and piloting the DCE gave further clarity and context.
It is possible that the management attribute may not have fully explored the treatment process associated with these choices. Pain related to the condition (symptoms), procedure, or postoperative sequalae of cFPM was considered but would have been challenging to operationalize. Existing evidence would support that symptomatic teeth would almost certainly be removed (Taylor et al. 2019; Lygidakis et al. 2022), thus precluding the relevant option of restoration. Similarly, procedural pain was assumed to be equivalent across all options, as participants were informed that once anesthetized, any procedural pain associated with filling or extraction should be equal. However, this did not include the postoperative sequalae, which could be considered a limitation.
The lack of public preference and clinical effectiveness for the 2 main management options makes allocating resources for policy makers challenging. marginal WTP values could be used in a cost-benefit analysis, aiding resource allocation decisions. Finally, this is the first study to use a DCE to understand management of cFPM in children. There are few published DCEs in dentistry (Barber et al. 2018) and a paucity of those conducted with children as participants. Establishing preferences from young people in how to manage cFPM is arguably most important as they are the service users in this context. Further research is required in this field.
Conclusion
The binary options of restoring a cFPM and extraction, followed by spontaneous or orthodontic gap closure, were valued equally, placing an importance on having no gap as the outcome. Relevant stakeholders in this context need to understand the implications of this DCE to improve care and the delivery of dental services.
Author Contributions
G.D. Taylor, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; D. Boyers, contributed to design, data analysis and interpretation, critically revised the manuscript; C. Exley, N. Innes, L. Vale, C.R. Vernazza, contributed to conception and design, data interpretation, critically revised the manuscript. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jdr-10.1177_00220345241285154 – Supplemental material for Public Valuations of Managing Compromised Molars: A Discrete Choice Experiment
Supplemental material, sj-docx-1-jdr-10.1177_00220345241285154 for Public Valuations of Managing Compromised Molars: A Discrete Choice Experiment by G.D. Taylor, D. Boyers, C. Exley, N. Innes, L. Vale and C.R. Vernazza in Journal of Dental Research
Footnotes
Acknowledgements
The views expressed are those of the authors and not necessarily those of the National Institute for Health and Care Research or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: G.D. Taylor was funded by a National Institute for Health and Care Research Doctoral Research Fellowship (NIHR300251) during this research study.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.