
Abstract
The present study compared two types of emotion beliefs–emotion malleability (can control beliefs) and emotion control (should control beliefs)–in low-income Chinese American (CA; N = 222) and Mexican American (MA; N = 91) immigrant parents and examined their relations with depressive symptoms. 313 CA and MA immigrant parents (Mage = 40.09 years, 183 mothers 130 fathers) completed validated measures assessing can control beliefs, should control beliefs, depressive symptoms, and socio-demographic variables. No significant differences were detected between CA and MA parents in can control and should control beliefs. Several socio-demographic variables predicted can control and should control beliefs. Can control beliefs were associated with lower depressive (β = −.28, p < .001), while should control beliefs were associated with higher depressive symptoms (β = 1.99, p < .01) in both CA and MA parents. Cultural group did not moderate these relations. CA and MA parents endorsed comparable levels of emotion beliefs and the relations between emotion beliefs and depressive symptoms were consistent across groups. These findings suggest that interventions targeting emotion beliefs among low-income immigrant parents should focus on enhancing can control beliefs while addressing potentially maladaptive should control beliefs.
Introduction
Low-income U.S. immigrant families face a combination of stressors including financial hardships, acculturative stress, discrimination, and barriers to resources (Cassells & Evans, 2017; Guruge & Butt, 2015). Additionally, compared to middle- and high-income immigrant families who are more likely to migrate to the U.S. as a unit, low-income immigrant families often face the necessity of migrating serially (i.e., one family member at a time), a process that is linked to unique economic and emotional strains (Cassells & Evans, 2017). For many families, these strains are further compounded by transnational obligations, such as sending remittances or supporting relatives abroad, which can add financial and emotional burden (Cassells & Evans, 2017).
The Family Stress Model posits that financial hardship strains parents' mental health, which in turn hinders supportive parenting practices and contributes to poorer parent and child outcomes (Conger et al., 2010; McLoyd et al., 2014). Consistent with this theory, research has demonstrated that parental depression mediated the relation between economic hardship and child adjustment (Cassells & Evans, 2017). Given the mediating role of depression in the association between poverty and child outcomes, identifying factors that might buffer against depressive symptoms in low-income U.S. immigrant parents is critical for both parent and child.
Emotion beliefs refer to people’s evaluations about what emotions they can or should experience, alter, or regulate (De Castella et al., 2013). Emotion beliefs have been linked to clinically relevant outcomes including anxiety, depression, and social adjustment in predominantly white adult and college-aged samples (De Castella et al., 2013; Ford et al., 2018; Johnston et al., 2023; Zhu et al., 2021). However, little research has investigated the link between emotion beliefs and psychological adjustment in immigrant populations, despite emerging evidence that culture shapes what and how individuals choose to experience, express, or regulate emotions (Mesquita & Albert, 2007; Tsai et al., 2006). Much of the existing research on culture and emotion has focused on comparisons between Western and East Asian cultures and often collapses diverse ethnic groups into broad categories such as “collectivistic,” “Latino,” or “Asian” (Alegría et al., 2017). This approach overlooks the nuanced cultural values and beliefs immigrants bring from their countries of origin, as well as individual factors like years in the U.S. and acculturation. These limitations necessitate a more targeted examination of the relations between emotion beliefs and psychological adjustment in immigrant populations.
The present study addresses these gaps by examining the concurrent link between emotion beliefs and depressive symptoms in low-income Chinese American and Mexican American immigrant parents. As two of the largest and fastest growing immigrant populations in the United States, Chinese Americans account for 24% of the Asian American population and Mexican Americans account for approximately 60 % of the Latino American population (U.S. Census Bureau, 2019). Although Chinese and Mexican cultures are both considered collectivistic cultures compared to European American culture, there is considerable heterogeneity across the two cultures (Ruby et al., 2012; Senft et al., 2021; Soto et al., 2005) suggesting these groups may differ in their emotion-related beliefs and associated outcomes.
Emotion Beliefs and Links to Psychological Adjustment
Emotion Beliefs
The present study focuses on two forms of emotion beliefs–emotion malleability beliefs and emotion control values. Emotion malleability beliefs (hereafter can control beliefs) are beliefs about whether emotions can be changed or controlled (Tamir et al., 2007) while emotion control values, in the present context, refer to beliefs about whether emotions should be controlled (Mauss, Butler, Roberts, et al., 2010). Although emotion control values (hereafter should control beliefs) are sometimes conceptualized as distinct from emotion beliefs (Kisley et al., 2024), Kisley and colleagues (2024) offer a precise definition of emotion beliefs as “statements about emotion that an individual endorses as true, or likely to be true,” providing a useful benchmark for classifying such constructs. By this definition, values construed as normative statements such as “emotions should be controlled” qualify as emotion beliefs. Thus, appreciating emotion control or preferring it as an ideal affective state (Tsai, 2007) is conceptually distinct from believing that emotions should (or should not) be controlled. Because should control beliefs are particularly susceptible to the influences of cultural norms and values (Mauss & Butler, 2010; Mauss, Butler, Roberts, et al., 2010), they are essential to examine in the context of immigrant families.
Emotion Beliefs and Psychological Adjustment
In predominantly White samples, can control beliefs have been associated with individuals’ better adjustment (Hong & Kangas, 2022). Similarly, in Chinese-heritage samples, higher can control beliefs have been associated with higher positive affect and life satisfaction and reduced negative affect, whereas lower can control beliefs have been associated with greater anxiety and depressive symptoms (Zhang et al., 2023; Zhu et al., 2021). Relations between can control beliefs and psychological adjustment are far less studied in Mexican-origin individuals, although malleable mindsets have been associated with increased psychological wellbeing in Mexican college students (Ortiz Alvarado et al., 2019). Empirical studies on links between should control beliefs and psychological adjustment are limited. However, there is some evidence that greater should control beliefs are associated with reduced anger experience in Asian Americans, but not in White Americans (Mauss, Butler, Roberts, et al., 2010).
Prior studies suggest that the relation between emotion beliefs and psychological adjustment is mediated by emotion regulation. For example, cognitive reappraisal has been shown to mediate the relation between can control beliefs and symptoms of anxiety and depression (Somerville et al., 2023) and expressive suppression has similarly mediated this relation, with lower can control beliefs linked to increased anxiety and depressive symptoms through heightened expressive suppression (Deplancke et al., 2022). These findings align with theoretical work suggesting that emotion beliefs can shape individuals’ decisions about whether (or not) to regulate specific emotions, perceived ability to regulate emotions, strategy use, and the relative success of efforts (Ford & Gross, 2019; Tamir & Mauss, 2011).
However, growing evidence indicates that emotion beliefs may also influence psychological adjustment beyond regulatory behaviors (Kisley et al., 2024). Kneeland, Dovidio, et al. (2016) propose two additional possible mechanisms underlying the links between lower can control beliefs and higher depressive symptoms (Joormann & Gotlib, 2010; Leahy, 2002). First, individuals who hold low can control beliefs may experience greater fear of negative emotional experiences as a result of believing that emotions cannot be changed in the moment. Second, individuals with depression are theorized to perceive lower controllability in both external and internal events (Alloy et al., 1988), which may translate to their beliefs about emotion controllability.
Notably, stronger beliefs that one should control emotions do not necessarily coincide with stronger beliefs that one can control them. For example, Goodman et al. (2021) found that individuals with social anxiety disorder (SAD) reported lower can control beliefs and higher should control beliefs than healthy controls. This finding suggests that people with SAD hold conflicting emotion beliefs that might result in a “no-win” situation.
Cultural Considerations in the Links between Emotion Beliefs and Psychological Adjustment
Although little research has directly examined culture’s role in can control beliefs (Ford & Gross, 2019), growing evidence highlights meaningful cultural variability in how emotion beliefs relate to regulation strategies and their adjustment functions. Although the present study focused specifically on emotion beliefs, prior research on cultural variability in how these beliefs relate to regulation strategies provides important context for interpreting their links to psychological adjustment. For instance, can control beliefs are generally linked to better adjustment across both White and Chinese-origin samples (Hong & Kangas, 2022; Zhang et al., 2023; Zhu et al., 2021). However, while can control beliefs are associated with greater use of cognitive reappraisal and lower expressive suppression in predominately White samples (Hong & Kangas, 2022), can control beliefs are associated with both cognitive reappraisal and expressive suppression among Chinese Americans (Zhu et al., 2021). Furthermore, while should control beliefs are linked to greater expressive suppression and poorer adjustment in predominantly White samples (Mauss & Butler, 2010; Mauss, Butler, Roberts, et al., 2010; Zerwas et al., 2023), they have been associated with reduced anger experience in Asian Americans (Mauss, Butler, Roberts, et al., 2010). Notably, expressive suppression has been linked to reduced negative affect in Chinese and Asian American individuals (Butler et al., 2007; Soto et al., 2011), likely because suppression and emotion control are viewed as strategies to preserve interpersonal harmony–a key cultural value (Senft et al., 2021). Evidence from Mexican-origin individuals further illustrates this nuance. One study found that suppression of negative emotions predicted lower anhedonia, whereas suppression of positive emotions predicted higher anhedonia (Young et al., 2022). These findings align with simpatía–a Mexican cultural script which encourages the control of negative emotions and the open and vibrant expression of positive emotions (Acevedo et al., 2020; Senft et al., 2021; Triandis et al., 1984).
Given these cultural variations, it is important to examine how immigrants’ experiences of acculturation may further influence their emotional patterns and psychological adjustment. As immigrants encounter and adapt to new cultural environments, they experience cultural and psychological changes collectively referred to as acculturation (Berry, 2005, 2019). Low-income Chinese and Mexican immigrants experience similar levels of acculturation (Uchikoshi, 2022). However, empirical research on emotional acculturation–increased fit with the emotional norms of one’s new culture (Jasini et al., 2018)–in immigrants suggests that the emotional patterns associated with one’s new culture do not necessarily replace those from their heritage culture. Instead, they may come to co-exist within the individual and different contexts may activate different emotional patterns (De Leersnyder, 2017; De Leersnyder et al., 2020; Perunovic et al., 2007). Previous research has also demonstrated that immigrants’ emotional acculturation is contingent on feelings of social acceptance during interactions with majority group members (Jasini et al., 2018). Low-income immigrants may face an elevated risk of social exclusion by majority group members in the U.S. and consequently barriers to emotional acculturation, regardless of their perceived cultural orientation.
Relations of Sociodemographic Factors to Emotion Beliefs and Depressive Symptoms
Nomaguchi and Milkie (2017) emphasized the importance of a sociological approach to examining parents’ mental health, considering the role of structural and cultural factors such as socioeconomic status, ethnic culture, and nationality. Low-income Chinese and Mexican immigrants share common migration-related stressors, including economic instability and language barriers. Furthermore, both Chinese American and Mexican American immigrants encounter racism and racial and ethnic discrimination (Chavez, 2013; Hwang & Goto, 2008; Lee & Waters, 2021; Romero, 2015). However, these groups differ in key socio-demographic factors that shape their parenting experiences. For example, on average, Chinese immigrants tend to have higher educational attainment whereas Mexican immigrants face greater economic hardship and higher rates of serial migration, contributing to different stressors related to financial stability and family support (Buttiler et al., 2023; Rusch & Reyes, 2013).
We considered several socio-demographic variables that have been theorized to relate to emotion beliefs and depressive symptoms as potential predictors of emotion beliefs and as covariates when testing the relations between emotion beliefs and depressive symptoms. Given the relations between culture and emotion beliefs reported in the literature, we examined acculturation (American orientation and heritage orientation) and years living in the United States. Higher education has been linked to stronger can-control beliefs (Sasaki et al., 2023), whereas lower socioeconomic status and female gender are associated with increased risk for depressive symptoms (Ettman et al., 2023; Salk et al., 2017). Notably, single parents often face unique stressors that exacerbate financial burden and depression risk (Kim et al., 2018). Given these associations, socioeconomic status, gender, and marital status were included as covariates in the models examining links between emotion beliefs and depressive symptoms.
The Present Study
The present study examined can control and should control emotion beliefs and depressive symptoms in a sample of Chinese American (CA) and Mexican American (MA) immigrant parents living at or below the poverty line. The study had two aims. Our first aim (Aim 1a) was to compare parents’ emotion beliefs between cultural groups. Because no prior theory or research suggests the two groups differ on can control beliefs, we did not predict any cultural group differences. For should control beliefs, research indicates that Chinese culture encourages should control beliefs (regardless of valence) while Mexican culture encourages control of negative emotions specifically. However, the high undesirability of negative emotional expression may counterbalance the high desirability of positive emotional expression in Mexican Americans, potentially resulting in similar should control beliefs between Mexican and Chinese Americans. Given these two possibilities, we tested cultural group differences in should control beliefs as an exploratory aim. Moreover, we examined sociocultural predictors of emotion beliefs (Aim 1b). Based on prior research examining relations between gender and education and emotion beliefs (Sasaki et al., 2023; Mauss, Butler, Roberts, et al., 2010; Timmers et al., 1998), we predicted that male gender would be associated with should control beliefs and higher socioeconomic status would be associated with can control beliefs in both groups. Based on the nuanced findings regarding emotional acculturation (Jasini et al., 2018)—where emotional patterns from heritage and host cultures may coexist and are influenced by social acceptance—we tested relations between American and heritage cultural orientations and emotion beliefs as an exploratory hypothesis. Aim 2 was to examine the association between emotion beliefs and depressive symptoms in CA and MA immigrant parents and test cultural group as a moderator in these relations. Based on prior research supporting a positive relation between can control beliefs and wellbeing (Ortiz Alvarado et al., 2019; Zhang et al., 2023; Zhu et al., 2021), we predicted that can control beliefs would be negatively associated with depressive symptoms (Aim 2a). Research on relations between should control beliefs and adjustment is limited; however, existing evidence suggested positive relations between should control beliefs and expressive suppression. Due to mixed findings in prior research on links between expressive suppression and adjustment (Hu et al., 2014; Soto et al., 2011; Su et al., 2015), we predicted that should control beliefs would be unrelated with depressive symptoms (Aim 2b). As an exploratory aim, we will test whether culture group moderated the relations between emotion beliefs and depressive symptoms (Aim 2c).
Method
Participants
Participants consisted of 313 parents (58% female) from low-income Chinese American (CA; N = 222) and Mexican American (MA; N = 91) families who participated in Wave 1 assessment of an ongoing longitudinal study on language and socioemotional development of dual language learners in Head Start preschool programs in Northern California (masked for blind review). Enrollment in Head Start indicates that all families are living at or below the poverty line. Participation criteria included that both parents identified themselves as Chinese American or Mexican American, their home language was either Chinese (Cantonese or Mandarin) or Spanish, and the children could speak two-word phrases in their heritage language by age three with no developmental disorders. Participating parents were on average 40 (SD = 7.41) years of age and had been living in the United States for 14.17 (SD = 18.56) years at the time of data collection. Eighty-four percent were foreign-born (first-generation immigrants). Eighty-eight percent were married or living with a partner. Full sample characteristics are detailed in Table 1. Univariate comparisons were conducted using independent sample t-tests. On average, Mexican American parents lived in the United States longer than Chinese American parents, t(60.65) = −2.22, p = .031, and Chinese American parents were older t(173.93) = 2.01, p = .046 and had more years of education than Mexican American parents, t(173.99) = 3.18, p = .002. The mean annual per capita income (total estimated income divided by household size) for parents was 9,427 USD. On average, per capita income was higher among Chinese American parents than Mexican American parents, t(208.63) = 2.97, p = .003 though perceived economic hardship was lower in Mexican American parents than in Chinese American parents, t(213.24) = 2.03, p = .044.
Descriptive Statistics for Full Sample and by Cultural Group.
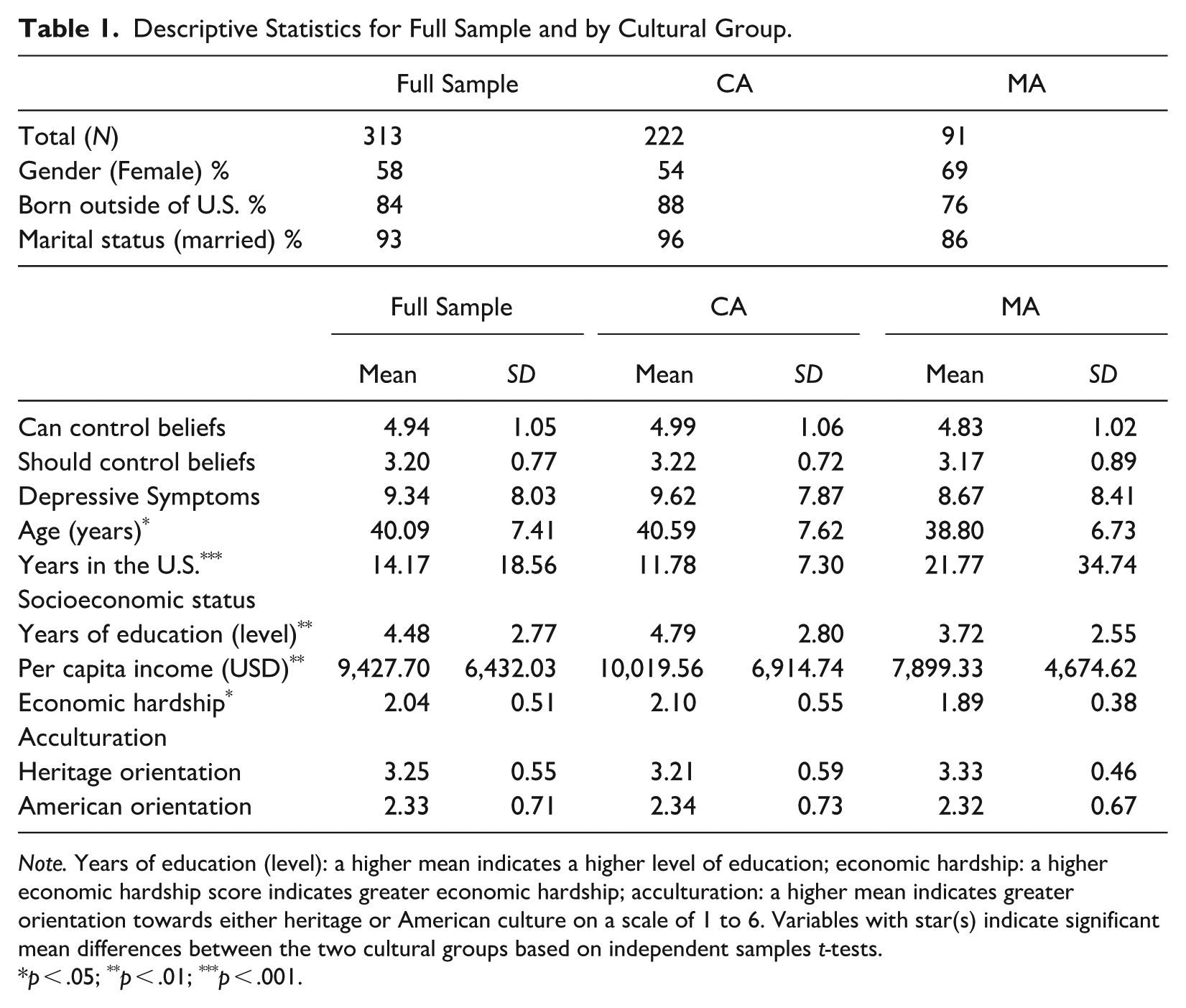
Note. Years of education (level): a higher mean indicates a higher level of education; economic hardship: a higher economic hardship score indicates greater economic hardship; acculturation: a higher mean indicates greater orientation towards either heritage or American culture on a scale of 1 to 6. Variables with star(s) indicate significant mean differences between the two cultural groups based on independent samples t-tests.
p < .05; **p < .01; ***p < .001.
Procedure
The study was approved by the institutional review board at the authors’ institutions. Written informed consent was obtained in the parents’ preferred language prior to data collection. While data was collected as part of a larger longitudinal study, only the data applicable to this study will be discussed. A team of trained bilingual research assistants visited the families’ homes to collect data through a combination of one-on-one interviews and written self-report measures. Parents completed surveys in their preferred language (10% English and 90% heritage language) and received 75 USD upon completion for their participation.
Measures
Demographics
Parents were administered the adapted version of the Family and Demographics and Migration History Questionnaire (Roosa et al., 2008; see also S. H. Chen et al., 2014) by a bilingual interviewer. Items included age, generation status, years living in the US, marital status, employment status, family income in the past year, and total number of adults and children living in the household. Years of education was assessed through the following categories: 0 = No formal schooling 1 = Less than high school, 2 = Some high school, 3 = High school graduate, 4 = High school GED, 5 = Technical school/Vocational school/ Certification, 6 = Some college, 7 = Associate's degree, 8 = Bachelor's degree, 9 = Master's degree, 10 = Doctorate (JD, MD, PhD).
Emotion Beliefs
Can control beliefs were measured using the Implicit Theories of Emotion Scale (Tamir et al., 2007). The scale consists of four items–two of which refer to the malleable nature of emotions (i.e., “everyone can learn to control their emotions,” “if they want to, people can change the emotions that they have”) and two of which refer to the fixed nature of emotions (i.e., “no matter how hard they try, people can’t really change the emotions that they have,” “the truth is, people have very little control over their emotions”). Parents indicated their agreement with each statement on a scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Following Tamir et al. (2007), we reverse-scored the two fixed items and then averaged across all items to form one score, with higher scores indicating greater can control beliefs. Should control beliefs were assessed using the Emotion Control Values Scale (Mauss, Butler, Roberts, et al., 2010). The scale consists of six items to capture general beliefs about emotional control (e.g., “People should not express their emotions openly,” or “It is better for people to let out pent up emotions”). Both the Implicit Theories of Emotion Scale and the Emotion Control Values Scale have been validated in diverse samples (Kornilova & Zhou, 2021; Mauss, Butler, Roberts, et al., 2010). McDonald’s omega (McDonald, 1999) was calculated to measure scale reliability. This method is more accurate than Cronbach’s alpha coefficient, which misestimates scale reliability except in the rare situation where the measurement model contains no error covariances and the items are tau-equivalent (Hayes & Coutts, 2020; McNeish, 2018). Omega reliabilities for the can control belief items were .66 overall, .78 for Chinese Americans and .53 for Mexican Americans. Omega reliabilities for the should control belief items were .79 overall, .81 for Chinese Americans, and .78 for Mexican Americans.
Depressive Symptoms
Depressive symptoms were measured using the Center for Epidemiological Study - Depression scale (CESD; Radloff, 1977). The CES-D is a self-report measure of depressive symptoms that has been widely used in research and clinical settings. It consists of 20 items that assess the presence and severity of depressive symptoms experienced over the past week, with response options ranging from 0 (rarely or none of the time) to 3 (most or all the time). The items cover a range of domains, including mood, somatic symptoms, and interpersonal relationships.
Total scores on the CES-D range from 0 to 60, with higher scores indicating greater severity of depressive symptoms. A score of 16 or above is typically used as a cut-off for identifying individuals at risk for clinical depression, although this threshold may vary depending on the specific population being studied. The CES-D has been shown to have good internal consistency and has been validated in community samples, clinical populations, and diverse racial and ethnic groups including Chinese Americans (Kim et al., 2021; Li & Hicks, 2010) and Mexican Americans (Radloff, 1977). The CES-D scale showed good internal consistency in our sample. The Omega reliabilities were .93 for Chinese Americans and .92 Mexican Americans.
Acculturation
Parents self-reported on American and heritage cultural orientations using the Cultural and Social Acculturation Scale (CSAS; X. Chen & Lee, 1996). The CSAS assesses for engagement in both heritage and host cultures across domains, including: language proficiency (8 items), media use (10 items), and interpersonal relationships (6 items). Because the subscales were highly intercorrelated, composite scores for American Cultural Orientation and Heritage Cultural Orientation (12 items each) were created by standardizing subscale scores and averaging them. Higher American cultural orientation scores indicate greater adoption of aspects of American culture, whereas higher heritage cultural orientation scores indicate stronger retention of values and traditions from parents’ culture of origin. These scores are not mutually exclusive. The CSAS has been validated in previous studies with Chinese American and Mexican American immigrant families with socioeconomically diverse backgrounds (S. H. Chen et al., 2014; S. H. Chen & Zhou, 2019). The Omega reliabilities for American and heritage cultural orientations were .92 and .85 in Chinese Americans and .90 and .77 in Mexican Americans.
Economic Hardship
Economic hardship was assessed with a measure adapted by Barrera et al. (2001) for African American, European American, and Mexican American populations. A composite economic hardship score was created by calculating z-scores for each of the following four scales and averaging them: inability to make ends meet (2 items), not enough money for necessities (7 items), economic adjustments/cutbacks (9 items), and financial strain (2 items). The Omega reliabilities were .92 for Chinese Americans and .89 Mexican Americans.
Data Analysis Plan
First, as preliminary analyses, descriptive statistics and in-dependent sample t-tests were conducted examine cultural group differences in sociodemographic variables, emotion beliefs, and depressive symptoms. Pearson correlations were computed to examine the relations between sociodemographic variables and emotion beliefs and depressive symptoms within each culture group. Descriptive statistics and correlations were computed using R Statistical Software (v 4.2.0; R Core Team, 2022).
Next, to test Aim 1a (cultural group differences in emotion beliefs) and Aim 1b (socio-demographic predictors of emotion beliefs), we conducted two multiple regression analyses to predict can control beliefs and should control beliefs from culture group (MA vs. CA) and sociodemographic predictors (socioeconomic status, gender, and years living in the U.S.). To reduce the number of predictors in the model, we created a socioeconomic status composite by combining years of education, per capita income, and financial hardship, following a common data reduction strategy in immigrant samples (e.g., S. H. Chen et al., 2014). This composite was created by calculating the mean of the standardized scores for each of the variables.
To test Aim 2a and Aim 2b (relations of emotion beliefs to depressive symptoms), we computed two multiple regressions predicting depressive symptoms simultaneously from emotion beliefs and sociodemographic variables. Can control beliefs and should control beliefs were tested in different regression models because we were interested in examining their differential relations to depressive symptoms. To test Aim 2c (moderation by culture group), we computed the interaction terms of emotion beliefs × culture group and included it as a predictor in the regression models. The regression models were tested in Mplus 8.6 (Muthén & Muthén, 2017) using the full information maximum likelihood (FIML) to handle missing data. Given that parents were clustered within families, the models were estimated using the TYPE = COMPLEX feature in Mplus, which accounts for the nonindependence of observations when computing standard errors (Muthén & Muthén, 2017).
Missing Data
Only parents who completed the CES-D for depressive symptoms, the Implicit Theories of Emotion Scale, and the Emotion Control Values Scale (at least 70% each) were included in the present study. Out of the 316 parents, 313 met these criteria. In regression analyses, missing data were handled using the FIML estimation in Mplus 8.6.
Results
Descriptive Statistics and Correlates Between Theorized Covariates and Study Variables
Descriptive statistics of demographic and study variables are displayed in Table 1. All study variables were within acceptable values of skewness and kurtosis (Kline, 2015), except for parents’ years living in the U.S., which was positively skewed and had high kurtosis, indicating that most parents have lived in the U.S. for fewer years and there was limited range of variability in the sample. Years in the U.S. was log-transformed and its skewness and kurtosis were within acceptable values after transformation. The log-transformed variable was used in all subsequent analyses to examine the study aims. Zero-order correlations were computed to examine the pairwise relations among sociodemographic variables, emotion beliefs, and depressive symptoms for each cultural group (Table 2). Two demographic variables were significantly correlated with both emotion beliefs and depressive symptoms in CA parents. Heritage orientation was positively associated with can control beliefs (r = 0.32), negatively associated with should control beliefs (r = −.21), and negatively associated with depressive symptoms (r = −.31). American orientation was positively associated with can control beliefs (r = .27) and negatively associated with depressive symptoms (r = −.27). No demographic variables were significantly correlated with both emotion beliefs and depressive symptoms in MA parents. Following the suggestion of Steiner et al. (2010), and to preserve parsimony, we included variables from our list of theorized covariates as actual covariates in subsequent analyses if they were significantly correlated with both the predictor and the outcome. Based on the correlation results, American cultural orientation and Heritage cultural orientation were included as covariates in analyses for Aim 2 (relations between emotion beliefs and depressive symptoms)
Zero-order Correlations for Study Variables.
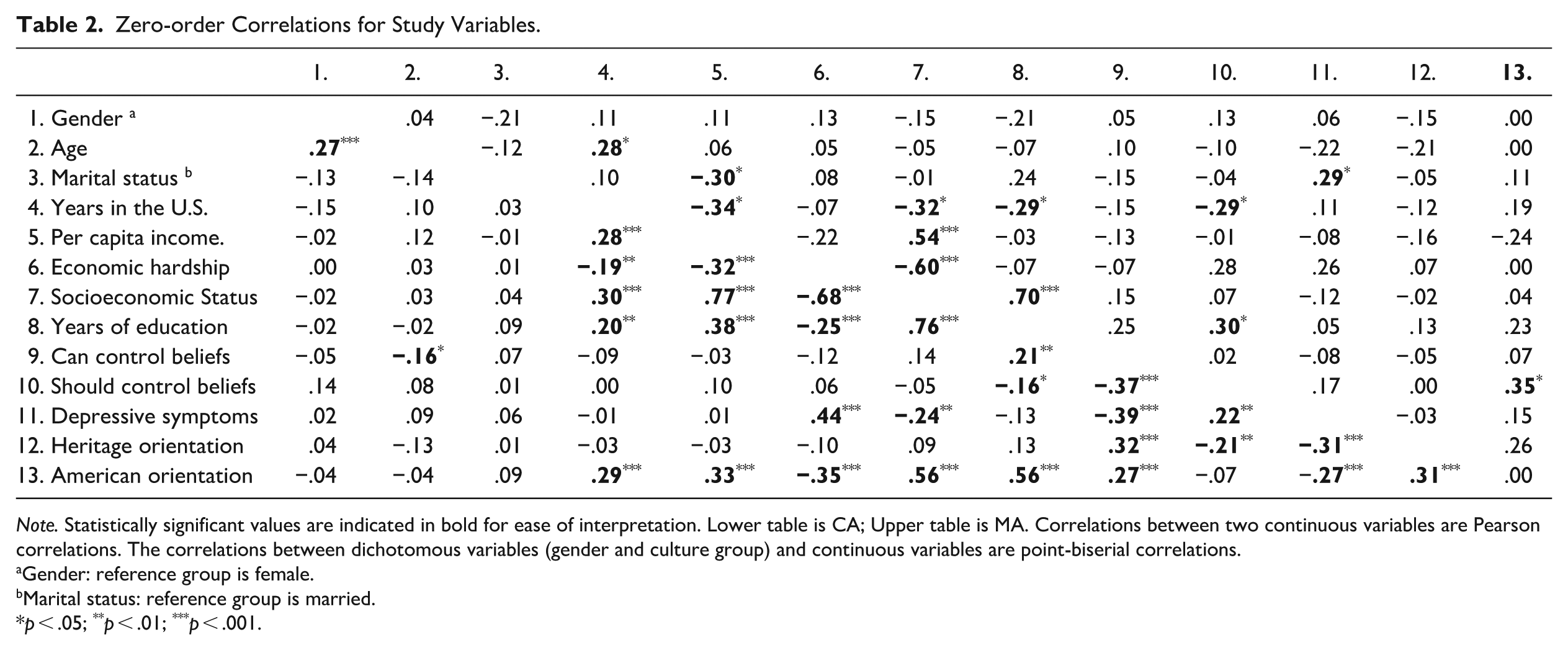
Note. Statistically significant values are indicated in bold for ease of interpretation. Lower table is CA; Upper table is MA. Correlations between two continuous variables are Pearson correlations. The correlations between dichotomous variables (gender and culture group) and continuous variables are point-biserial correlations.
Gender: reference group is female.
Marital status: reference group is married.
p < .05; **p < .01; ***p < .001.
Cultural Group Differences in Emotion Beliefs and Sociocultural Predictors of Emotion Beliefs (Aims 1a and 1b)
Results from the two regression models predicting emotion beliefs from culture group and socio-demographic variables are shown in Table 3. In both models, culture group was unrelated to emotion beliefs controlling for sociodemographic variables. However, socio-demographic variables were significantly associated with emotion beliefs. Specifically, years living in the U.S. were negatively associated with can control beliefs (β = −.27, p < .05), and both heritage and American cultural orientations were positively associated can control beliefs (βs = 42 and .36, ps < .05). In contrast, gender was significantly associated with should control beliefs, such that compared to females, males endorsed higher should control beliefs (β = .19, p < .05). Moreover, heritage cultural orientation was negatively associated with should control beliefs (β = −.36, p < .05).
Multiple Regressions Predicting Emotion Beliefs from Culture Group and Other Socio-demographic Variables.
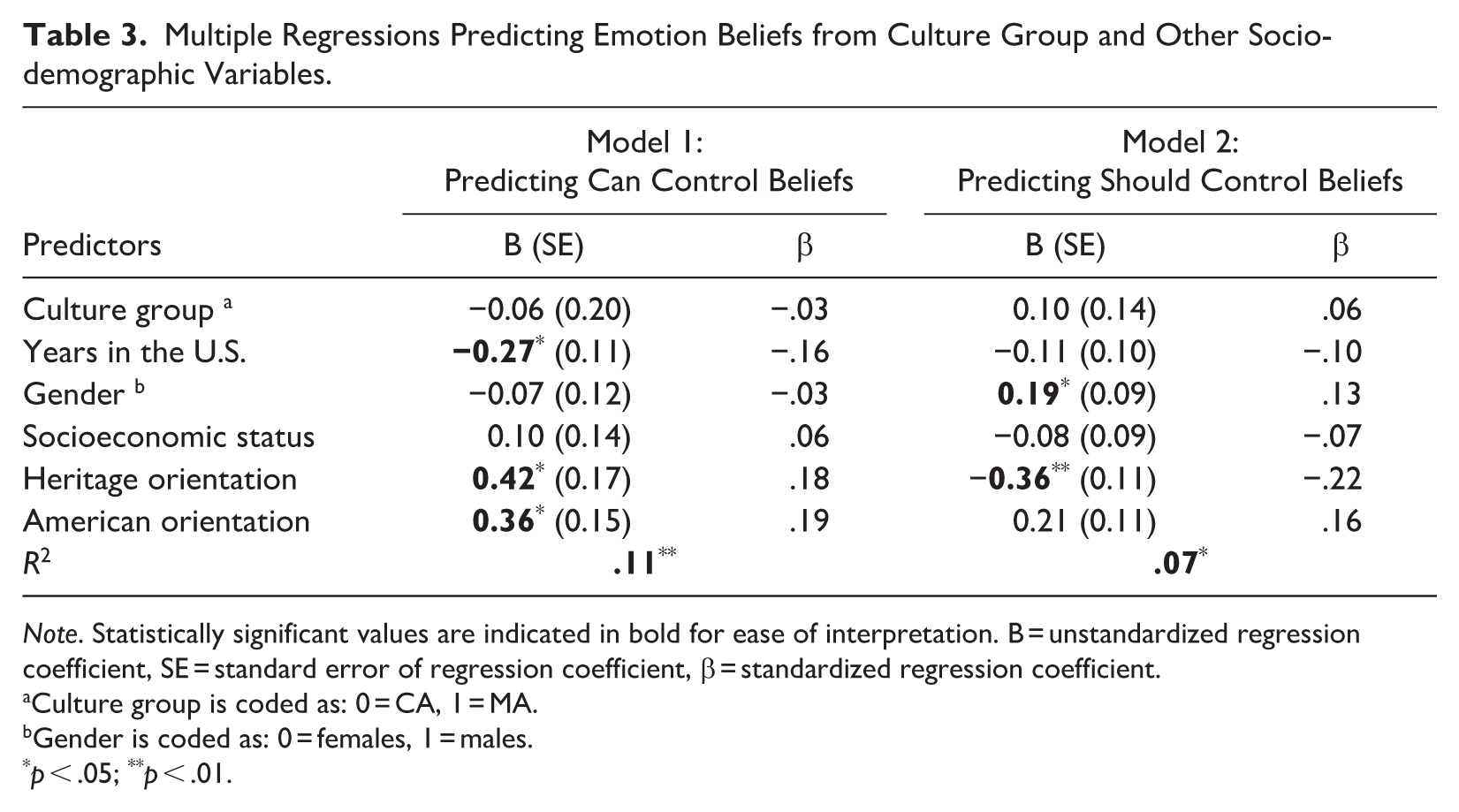
Note. Statistically significant values are indicated in bold for ease of interpretation. B = unstandardized regression coefficient, SE = standard error of regression coefficient, β = standardized regression coefficient.
Culture group is coded as: 0 = CA, 1 = MA.
Gender is coded as: 0 = females, 1 = males.
p < .05; **p < .01.
Relations Between Emotion Beliefs and Depressive Symptoms, and Moderation by Culture (Aims 2a, 2b, and 2c)
Results from the two regression models predicting depressive symptoms from emotion beliefs, culture group, and culture group x emotion beliefs interaction are presented in Table 4. As expected, can control beliefs were significantly and negatively associated with depressive symptoms (β = −.28, p < .001). In contrast, should control beliefs was significantly and positively associated with depressive symptoms (β = −1.99, p < .01). Moreover, both heritage and American cultural orientations were negatively associated with should control beliefs (βs = −1.62 and −2.63, ps < .05). The interaction term of culture × emotion beliefs was not significant in either model, indicating no evidence of moderation by culture group.
Multiple Regressions Predicting Depressive Symptoms from Emotion Beliefs, Culture Group, and Its Interaction.
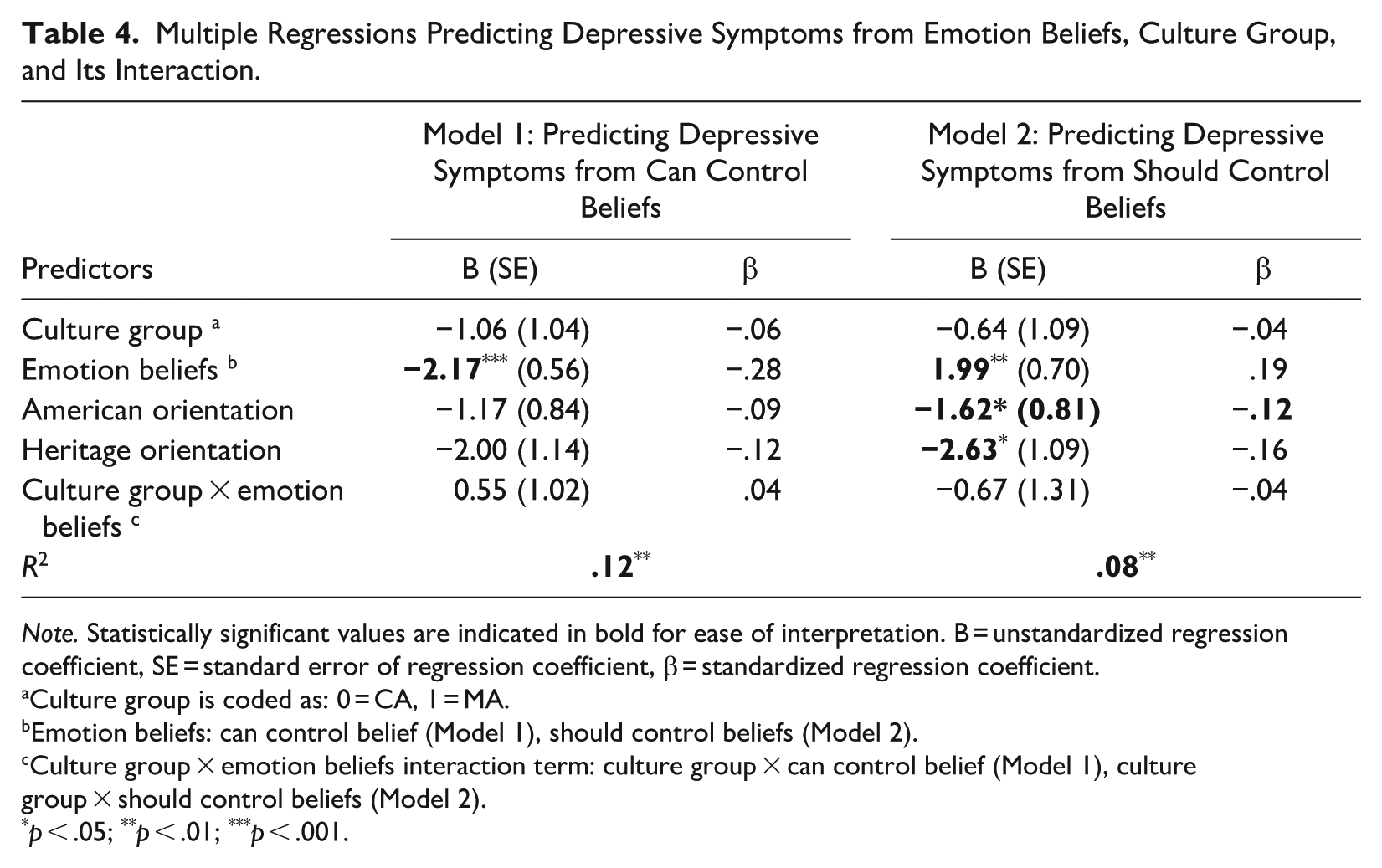
Note. Statistically significant values are indicated in bold for ease of interpretation. B = unstandardized regression coefficient, SE = standard error of regression coefficient, β = standardized regression coefficient.
Culture group is coded as: 0 = CA, 1 = MA.
Emotion beliefs: can control belief (Model 1), should control beliefs (Model 2).
Culture group × emotion beliefs interaction term: culture group × can control belief (Model 1), culture group × should control beliefs (Model 2).
p < .05; **p < .01; ***p < .001.
Discussion
The present study examined cultural group differences and sociodemographic predictors of can control and should control beliefs among low-income CA and MA immigrant parents. We further tested whether these beliefs were linked to depressive symptoms and whether such associations varied by culture group.
Consistent with our first hypothesis, we did not detect significant cultural group differences in can control beliefs between CA and MA parents. Similarly, significant group differences were not detected in should control beliefs. These results suggest that CA and MA parents endorsed comparable levels of beliefs about people’s ability to control their emotions and the extent to which they should control them. However, the relatively small sample size of Mexican Americans (n = 93) and low reliability of the can control beliefs measure in this group limits the generalizability of these findings.
Furthermore, we examined potential socio-demographic predictors of emotion beliefs. Controlling for other socio-demographic variables, we found that years living in the U.S. were negatively associated with can control beliefs and both heritage orientation and American orientation were positively associated with can control beliefs, though the association was slightly stronger for heritage orientation. As expected, gender was positively associated with should control beliefs such that males endorsed higher should control beliefs than females and heritage orientation was negatively associated with should control beliefs. At first glance, the observed associations between years living in the U.S., cultural orientation, and emotion beliefs may appear counterintuitive, given that collectivistic cultures are often linked to stronger emotion control values compared to individualistic cultures. However, research on emotional acculturation shows that heritage and host culture emotional patterns can coexist, with different contexts activating different responses (De Leersnyder, 2017; De Leersnyder et al., 2020; Jasini et al., 2018; Perunovic et al., 2007). Importantly, successful emotional acculturation depends on feelings of social acceptance (Jasini et al., 2018). Individuals in our sample possess multiple minoritized identities (e.g., low-income, ethnic minority, immigrant status); thus, they may face an elevated risk of social exclusion by majority group members in the U.S. and consequently barriers to emotional acculturation, regardless of their cultural orientation. Our findings provide support for the idea that cultural orientation alone does not necessarily predict emotional patterns. Finally, our finding that males reported higher should control beliefs than females is consistent with prior research showing gender differences in should control beliefs and may also reflect culturally rooted gender roles in both Chinese and Mexican families, where fathers are often expected to serve as breadwinners, stricter authority figures, and to control emotions (Novianti et al., 2023).
For our second aim, we sought to understand the relations between emotion beliefs and depressive symptoms. Consistent with our hypothesis (Aim 2a), greater can control beliefs were significantly associated with lower depressive symptoms. Contrary to our hypothesis (Aim 2b), greater should control beliefs were significantly associated with higher depressive symptoms. One possible explanation for this finding is that although expressive suppression can sometimes be adaptive in collectivistic contexts (e.g., maintaining group harmony), the rigidity of believing that one should control emotions may undermine emotional flexibility and, in turn, increase vulnerability to depressive symptoms. These associations between emotion beliefs and depressive symptoms did not differ by cultural group, as the interaction terms were nonsignificant (Aim 2c). Taken together, these findings suggest that among both CA and MA parents, believing one can control emotions may serve as a protective factor against depressive symptoms, whereas believing one should control emotions may represent a vulnerability factor for greater depressive symptoms.
Limitations and Future Directions
The present study broadens our understanding of two core emotion beliefs–can control and should control beliefs in a unique sample–low income Chinese American and Mexican American immigrant parents matched on socioeconomic status.
While the present study illuminates valuable insights regarding the complex interplay between culture, emotion beliefs, and depressive symptoms, findings should be interpreted in light of the following limitations. Firstly, all measures were self-reported, introducing inherent subjectivity. In particular, cultural norms, stigma, and social desirability biases may shape how depressive symptoms are reported on instruments such as the CES-D. For example, individuals may underreport symptoms due to concerns about stigma or instead express depression in terms of somatic complaints and culturally specific idioms of distress, which may not be fully captured by the CES-D. Although the CES-D has been validated in diverse populations, differential reporting could partially influence the observed associations. Second, our assessment of emotion beliefs did not differentiate between parents’ can control and should control beliefs about emotions in general versus beliefs about their own emotions, which may differ in some individuals and have clinical implications. For example, De Castella et al. (2014) found that individuals with low personal can control beliefs relative to general can control beliefs were more likely to be diagnosed with social anxiety disorder. Recent empirical work by Shulkin et al. (2025) provides further compelling evidence for the importance of distinguishing between general and personal emotion beliefs. They found that while general and personal emotion beliefs may represent different dimensions of the same underlying construct rather than completely distinct factors, personal beliefs consistently emerged as stronger predictors of affective distress compared to general beliefs across multiple studies. Future research should therefore distinguish between personal and general emotion beliefs and examine them in relation to one another. Thirdly, our study was cross-sectional so causality cannot be inferred from these results. Prior research has shown that emotion beliefs prospectively predict psychological functioning (e.g., Ford et al., 2018; Tamir et al., 2007) and experimental work has further demonstrated that these beliefs can be modified and lead to changes in emotional experience, regulation, and physiological reactivity (e.g., Karnaze & Levine, 2020; Kneeland, Nolen-Hoeksema, et al., 2016; Predatu et al., 2020). Building on this literature, future studies should continue to consider ways in which can control and should control beliefs can be experimentally manipulated to explore their link with depressive symptoms. Fourthly, our measurement of should control beliefs did not include valence, which is an important consideration given that the Mexican value of simpatía emphasizes expression of positive emotion and suppression of negative emotion. Future studies should consider incorporating valence in their measures of should control beliefs. Doing so may reveal more nuanced cultural differences in the association between should control beliefs and depressive symptoms. Due to the relatively small sample size of Mexican Americans and the low reliability of the can control beliefs measure in this group, the generalizability of findings is limited, and testing measurement invariance was not feasible. Future research with a larger sample of Mexican American immigrant parents is needed to examine measurement properties, ensure valid cross-group comparisons, and enable more robust analyses such as mediation testing. Additionally, including a clinical sample could yield more insights into the relations between emotion beliefs and depressive symptoms.
It is timely to expand our knowledge of emotion beliefs in culturally diverse populations. Future research should investigate which specific emotion regulation strategies (if any) are associated with can control beliefs and should control beliefs in Chinese American and Mexican Americans immigrant parents, as well as which emotion regulation strategies effectively mediate the relations between emotion beliefs and depressive symptoms. Doing so will help us better understand the mechanisms through which emotion beliefs are connected to depressive symptoms in these populations and opportunities for prevention and intervention. Relatedly, future research should examine potential mechanisms through which cultural values (e.g., interpersonal harmony and simpatía) may shape emotion beliefs or their links to depressive symptoms. Furthermore, our findings provide support for the idea that cultural orientation alone is not sufficient for predicting emotional patterns. Future research should continue to examine the nuanced process of emotional acculturation in low-income Chinese American and Mexican American immigrants–particularly the potential role of various contexts in activating different emotion beliefs at the individual level and the role of social acceptance in emotional acculturation.
Lastly, our findings offer insights for mental health professionals working with immigrant families. Because emotion beliefs are theorized to underlie multiple stages of the emotion regulation process and form the foundation of treatments such as Cognitive Behavioral Therapy (Beck,1979), assessing clients’ emotion beliefs, cultural values, and cultural orientation early in treatment may enhance case formulation and intervention planning. Findings of our study suggested that low-income CA and MA immigrant parents with low can control beliefs may benefit from interventions targeting these beliefs before introducing regulatory strategies that depend on them. Given the heterogeneity of immigrant families, clinicians should avoid overgeneralizing the adaptive functions of emotion beliefs and instead adopt a culturally responsive, collaborative assessment approach which considers factors such as socioeconomic status, generational status, years in one’s country of residence, acculturation and multiculturalism. These factors may influence which emotion beliefs individuals adopt, as well as the relations between those beliefs and depressive symptoms.
Footnotes
Acknowledgements
We are grateful to all the parents, children, teachers, and school staff who have participated in or assisted with the study. We also wish to thank the graduate and undergraduate students at University of California Berkeley and University of California Davis who have assisted in participant recruitment, data collection, and coding.
Author Contributions
Conceptualization: E. Roach, Q. Zhou, I. Mauss; Methodology: E. Roach, Q. Zhou, I. Mauss; Formal Analysis: E. Roach; Investigation: Q. Zhou, Y. Uchikoshi; Writing–Original Draft Preparation: E. Roach; Writing–Review & Editing: Q. Zhou, I. Mauss, Y. Uchikoshi; Funding Acquisition: Q. Zhou, Y. Uchikoshi, E. Roach; Supervision: Q. Zhou; Validation: Q. Zhou
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [R01HD091154], the Sheldon Zedeck Program for Culture, Behavior and Management Study, and a Ford Foundation Predoctoral Fellowship administered by the National Academies of Sciences, Engineering, and Medicine.
Ethical Considerations
The study was approved by the Committee for Protection of Human Subjects at University of California Berkeley
Consent to Participate
Informed consent was obtained in the parents’ preferred language prior to data collection.
Consent for Publication
Not applicable.