
Abstract
The Cultural Formulation Interview (CFI) is a semi-structured interview in the DSM-5 comprised of three parts: a core-16-item questionnaire, an informant version for relatives or relevant others, and 12 supplementary modules placing culture and context at the center of patient assessment and treatment to clarify diagnosis and treatment and ensure patients feel understood. The paper aims to synthesize the current quantitative evidence on CFI’s favorability (i.e., whether it is feasible, acceptable, and valuable) for patients, clinicians, and relatives. A mixed-methods synthesis methodology was used to assess the impact of the favorability of the CFI for patients, clinicians and relatives, and clinicians’ cultural competence. The synthesis included 10 studies on the clinician’s competency, attitudes, training, and diagnosis, three studies on the views of the patients and clinicians about the CFI, and five studies with 34 estimates (n = 581) on the favorability of the CFI for patients, clinicians and relatives. Clinicians reported that the CFI increased their cultural knowledge across research, training, and practice settings. Patients reported that the CFI prioritized their perspective and increased rapport-building. A quantitative estimate from the five studies on the acceptability, utility, and feasibility of CFI from patients, relatives, and clinicians was favorable, suggesting that patients, relatives, and clinicians were satisfied with using the CFI. A protocol for standardizing CFI training and practice to inform future research using mixed-methods designs that include randomized control trials (RCTs) to examine the effect of the CFI on the clinician’s cultural competence, working alliance, and patient’s level of functioning was recommended.
Keywords
Mass migration to escape conflict and for greater economic opportunity has made many societies more culturally diverse, which has led to a greater awareness of the role of culture and context in mental health care. Cultural awareness has been increasingly recognized as critical to improving therapist cultural competence, building a therapeutic alliance, patient engagement and adherence, and improving patient outcomes in mental health care. The introduction of the Outline for Cultural Formulation (OCF) in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994) attempted to place the individual’s culture and context at the center of mental health assessment and encouraged the routine application of cultural assessments in clinical practice (Lewis-Fernandez et al., 2016). The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) Cultural Issues Subgroup, made up of cultural psychiatrists and medical anthropologists, converted the OCF into the Cultural Formulation Interview (CFI) by reviewing the available literature and designing and performing an international field trial testing the initial 14 questions CFI, which informed the final 16-item CFI version in the DSM-5 (Aggarwal et al., 2013). The Cultural Formulation Interview (CFI) is a semi-structured interview in the DSM-5 (APA, 2013). It comprises three parts: a core-16-item questionnaire, an informant version for caregivers, and 12 supplementary modules (Lewis-Fernandez et al., 2016). The CFI’s goal is to increase clinicians’ cultural competence by clarifying diagnosis and treatment and helping to build a stronger therapeutic alliance (e.g., Aggarwal, Jimenez-Solomon, et al., 2016; Garcini, 2017) by
transmit[ting] a more sophisticated understanding of an individual’s experience of culture as a dynamic, constantly changing distillation of multiple engagements with all communities to which he or she belongs, whether based on gender, spirituality, age, language, race/ethnicity, occupation, geographical location, leisure activities, national origin, or any other element of a person’s background and collective life. (Aggarwal, Jimenez-Solomon, et al., 2016, p. xxx)
Creating a more sophisticated understanding of a patient’s experience and cultural background is one key aspect of building a solid working alliance. The CFI provides a semi-structured interview that demonstrates a more culturally nuanced understanding so the patient feels respected, understood and less threatened. The clinician’s cultural competence and the patient’s perception of being respected and understood are closely related. The traditional definition of a clinician’s cultural competence may not fully capture the “dynamic and constantly changing distillation of multiple engagements of the patient,” as the traditional definition fails to include the clinician’s assumptions about gender, sexuality, spirituality and other culture-based attitudes and beliefs. In this article, we use a dynamic definition that combines the traditional definition of cultural competence with the clinician’s ability to make the patient feel culturally safe (Curtis et al., 2019). This expanded definition increases the likelihood of the clinician transmitting a complete understanding of the effect of the patient’s culture on their experience through (a) the acquisition of knowledge about the characteristics, cultural beliefs, and practices of culturally diverse groups; (b) acquisition and use of the skills and attitudes of empathy and compassion in interviewing and communicating with culturally diverse patients; and (c) the ongoing process of reflection on biases, attitudes, assumptions, stereotypes, prejudices, and structures and characteristics of the way care is provided that may affect the quality of care. Therapeutic alliance refers to the bond between clinician and patient and the agreement on the goals and tasks of the intervention. Clinician effects have a significant positive impact on the working alliance and patient outcomes (Del Re et al., 2021). A culturally safe clinician does not allow their own assumptions to get in the way of establishing a therapeutic alliance.
Consistent with the goals of the OCF and then the CFI, in 2006, the American Psychological Association Presidential Task Force shifted the emphasis from evidence-based treatments to evidence-based practice (Duncan, 2014). Evidence-based clinical practice is “the integration of the best available research, with clinical expertise in the context of patient characteristics and preferences” (American Psychological Association Presidential Task Force on Evidence-Based Practice, 2006, p. 273). Confirming the effectiveness of the CFI is crucial in developing evidence-based practice for culturally diverse patients.
A literature review of the CFI found good qualitative evidence for the CFI but limited quantitative research. A comprehensive narrative review of 25 studies using the pilot and final versions of the CFI concluded that patients and clinicians found that using the CFI enhanced clinical rapport (Aggarwal, Jarvis, et al., 2020). Almost half (n = 12) used qualitative methods only, including thematic analyses of debriefing interviews, case studies, case series, and focus groups. Eight of the 25 studies employed mixed methods (e.g., Aggarwal et al., 2015, 2019) and another five used quantitative methods, including three cross-sectional surveys. It did show that the use of the CFI significantly affects clinical practice, medical communication, research, and clinician training, in particular, in the revision of diagnoses, and also in better patient-clinician communication, consideration of family perspectives, improved service delivery, and cooperation within therapy (Aggarwal, Jarvis, et al., 2020). For example, the Interdisciplinary Case Discussion Seminars (ICDS) in CFI training supported the emergence of the multiplicity of perspectives that shifted clinicians’ diagnoses and formulations (Rousseau et al., 2020), and in a case study on an American Indian woman, the CFI provided a cultural context that resulted in a shift in diagnosis and the proposal of new categories of trauma bereavement (Langa & Gone, 2020). The qualitative analysis of the CFI led to the revision of the OCF to emphasize the importance of models for explaining mental illness, the role of social relationships, and the patient’s social, cultural, political, and economic contexts in reaching a cultural formulation (Paralikar et al., 2020).
The narrative review concluded that a meta-analysis was not yet possible because of the lack of randomized control trials (RCTs) comparing the use of the CFI with standard assessment and the heterogeneity of methodology and outcomes used by the studies performed to date (Aggarwal, Jarvis, et al., 2020). However, researchers continue to attempt to measure cultural competency, and its effect on clinician and patient outcomes, and several quantitative studies have been conducted since 2009, using, for example, the self-report CFI Debriefing Instrument for Clinicians and Patients (e.g., Skammeritz et al., 2020; Wallin et al., 2020). Acknowledging the limits of self-report and the need for process-orientated measurement in the CFI literature, the Shifting Cultural Lens Model (i.e., key in-session therapist behaviors, such as accessing the client’s view, expressing mental health professional views and negotiation of a shared view) has also been developed and assessed (López et al., 2020). To date, there has been no systematic review of the quantitative data on the favorability of the CFI, defined as the feasibility, acceptability, and utility of CFI for clinicians, patients, and relatives, and the impact of CFI on clinicians’ cultural competence. Despite these gaps, there is continued interest in the CFI, with Frontiers in Psychiatry (DeMarinis et al., 2023) featuring a special research topic on the CFI that included seven articles on the DSM-5 CFI, including a study protocol.
This study aimed to conduct a quantitative systematic review using a mixed-methods synthesis methodology whereby the quantitative data are extracted from quantitative and mixed-methods studies and integrated in a single review (Petticrew et al., 2013) to examine the CFI’s favorability based on the CFI’s impact on feasibility, acceptability, and utility for clinicians, patients, and relatives, and the clinicians’ cultural competence.
Method
Study Registration
This quantitative systematic review using mixed-methods synthesis, including meta-analysis and narrative summary methodology, was conducted and reported using the statement guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA; Moher et al., 2015) and Cochrane Collaboration (Higgins et al., 2011; Higgins & Green, 2005). The study was not registered in PROSPERO as it had been closed in 2020.
Search Strategy
A search of peer-reviewed journals on all studies of the CFI was conducted up to June 11, 2020. The electronic databases PubMed, PsycINFO, and Web of Science were searched, using the key search term “cultural formulation interview.” The lead author (R.K.) completed a comprehensive search of keywords in clinical trials involving humans to identify empirical studies that reported using the CFI (see Table 1).
Inclusion Table.
Eligibility Criteria
Eligibility criteria were defined a priori and are outlined in Table 1. The CFI has a 16-core question interview in the following four domains: (a) cultural definition of the problem, (b) cultural perceptions of the cause, context and support, (c) cultural factors affecting self-coping and past help-seeking, and (d) cultural factors affecting current help-seeking.
Studies with an intervention that was not primarily CFI were excluded. Examples of excluded interventions included an outline of a Brief Cultural Interview (Groen et al., 2017). In addition, qualitative studies on CFI were excluded to avoid duplication of previous systematic reviews (Aggarwal, Jarvis, et al., 2020).
Identification of Relevant Studies
The lead author (R.K.) and post-doc researcher (L.A.) screened the titles and abstracts of all the identified records of the searches of the electronic databases. Full texts of records identified as meeting eligibility criteria were retained. The same two authors coded records using a five-star rating for “yes,” a one-star rating for “maybe” and a zero-star rating for “no.” Records coded as “maybe” were discussed through meetings until consensus was achieved.
Data Extraction
The identified studies were extracted by the lead author (R.K.) and post-doc researcher (L.A.) using a data extraction form, which included the collection of the following data: author/s, year of publication, study design conditions (i.e., characteristics of intervention and comparator control where relevant), treatment duration, primary and secondary treatment outcomes for identified time points, sample size, age, percentage female, country of origin, ethnocultural background, language translation, and dropout rates.
Risk of Bias Assessment
The risk of bias was assessed by the lead author (R.K.) for all eligible studies using The Cochrane Collaboration Tool for assessing bias (Higgins et al., 2011) (see Figures 2 and 3). Also, the quality of evidence was evaluated for each eligible study using the risk of bias 29-item questionnaire for observational studies (Norris et al., 2012; Viswanathan & Berkman, 2011). A sum score of 29 risk items was created to assess the quality of evidence of eligible studies (see Tables 3 and 4). Screening the studies for cumulative bias highlights the emerging gaps in the available evidence (White et al., 2020).
Data Synthesis
For the quantitative systematic review using meta-analysis methodology, quantitative CFI estimates were collated with separate scores recorded for the subsets of items about acceptability, feasibility and clinical utility. An item-total estimate was also recorded. Studies that did not evaluate CFI outcomes through acceptability, feasibility and utility scoring were not included in meta-estimations but were reviewed and reported in the results as a separate category of evidence. For the narrative summary, the quantitative results were described for the individual studies.
Combinability of Effect Sizes
All CFI scores were transformed into a scaled outcome measure. In this step, the minimum and maximum range of all CFI Likert-type scales were converted from 0%, representing the minimal range of the Likert-type score range, to 100%, representing the maximal score on any CFI score. This step aimed to promote the combinability of effects across the studies (López-López et al., 2018), where slight but significant inconsistencies existed in how CFI Likert-type item range and scoring were used (e.g., the scoring and range of minimum and maximum). These transformed and original CFI scores can be reviewed in Tables 2 to 4.
Summary of the 18 Quantitative Studies (Including Mixed Methods).
Note. CCAT = Cultural Competence Assessment Tool; CFI = Cultural Formulation Interview; CFI-DIC = CFI Debriefing Instrument for Clinicians; CFI-DIP = CFI Debriefing Instrument for Patients; CFI-DIR = CFI Debriefing Instrument for Relatives; F = Females.
Table 2 Summary of 18 quantitative studies (Aggarwal et al., 2019; Aggarwal et al., 2015; Aggarwal et al., 2014; Aggarwal et al., 2018; Aggarwal, Lam, et al., 2016; Aggarwal, Lam, et al., 2020; Deshpande et al., 2020; Diaz et al., 2016; Garcini, 2017; Goyal et al., 2020; Hinton et al., 2015; Leon et al., 2011; Lewis-Fernandez et al., 2017; Mills et al., 2017; Padilla et al., 2016; Paralikar et al., 2015; Patil et al., 2013; Ramirez Stege & Yarris, 2017; Rohlof et al., 2017).
Favorability of CFI Based on Acceptability, Feasibility and Clinical Utility.
Note. CI = Confidence Interval; Collated Scores = a score of favorability from 0 to 100, with higher scores meaning higher favorability of the CFI; Theme SR—themes elicited in previous systematic review conducted by Aggarwal et al. (2020); Y = the number of criteria met using the 29-item risk of bias questionnaire for observational studies, the higher the Y score the lower risk of bias.
Quantitative Studies on the CFI Assessing Cultural Competency and Patient’s Working Alliance.
Note. CI = Confidence Interval; Collated Scores = a score of favorability from 0 to 100, with higher scores meaning higher favorability of the CFI; Theme SR—themes elicited in previous systematic review conducted by Aggarwal et al. (2020); Y = the number of criteria met using the 29-item risk of bias questionnaire for observational studies, the higher the Y score the lower risk of bias.
Definitions of Outcomes and Variables That Convey the Diversity of CFI Trends
The investigation of CFI employed variables that convey both the differing types of CFI outcomes, the context of CFI application, and variables that test the methodological robustness of modeling the CFI estimates. Subgroup variables were created to contrast CFI levels in the study’s research context (1) and the targeted sample (2). The research context variable created noted either a research, training, or practice context, and the targeted sample variable noted the individuals sampled as patients, clinicians, or family relatives of patients. Additional variables were also created to facilitate a series of sensitivity analyses, testing the robustness of the CFI meta-estimates. For these analyses, a variable of study bias was operationalized with the cumulative study quality score. A sample size variable was operationalized by the number of individuals within the respective analyses.
Meta-analytic Strategy
Studies that included CFI scores were categorized and analyzed as both total meta-estimates and within subgroups of interest. Multi-level models were used to estimate the CFI as feasibility, acceptability, clinical utility, and total scores. These models employed a random intercept to account for the multiplicity of CFI scores within each study and a random-effects component to account for the heterogeneity between studies. Studies that included informative but noncomparable outcomes of the CFI (e.g., revision of organizational policies following a CFI intervention) were presented in detail in Table 4 but were overlooked for the analysis of meta-effects.
In a subsequent step, the multi-level CFI model was repeated with the addition of the study sample size and study quality score, added as moderating covariates. These models were considered sensitivity models (see Supplemental Table 1), aiming to test the robustness of the meta-estimates for signs of undesirable methodological variance. An additional publication bias test was also conducted for each meta-estimate. Specifically, an Egger test and a Trim and fill procedure were included to examine file draw effects. All analyses and sensitivity analyses were conducted with “Metafor,” a specialized multi-level meta-analysis software package (Viechtbauer, 2010) within the R software environment (R Core Team, 2013).
Results
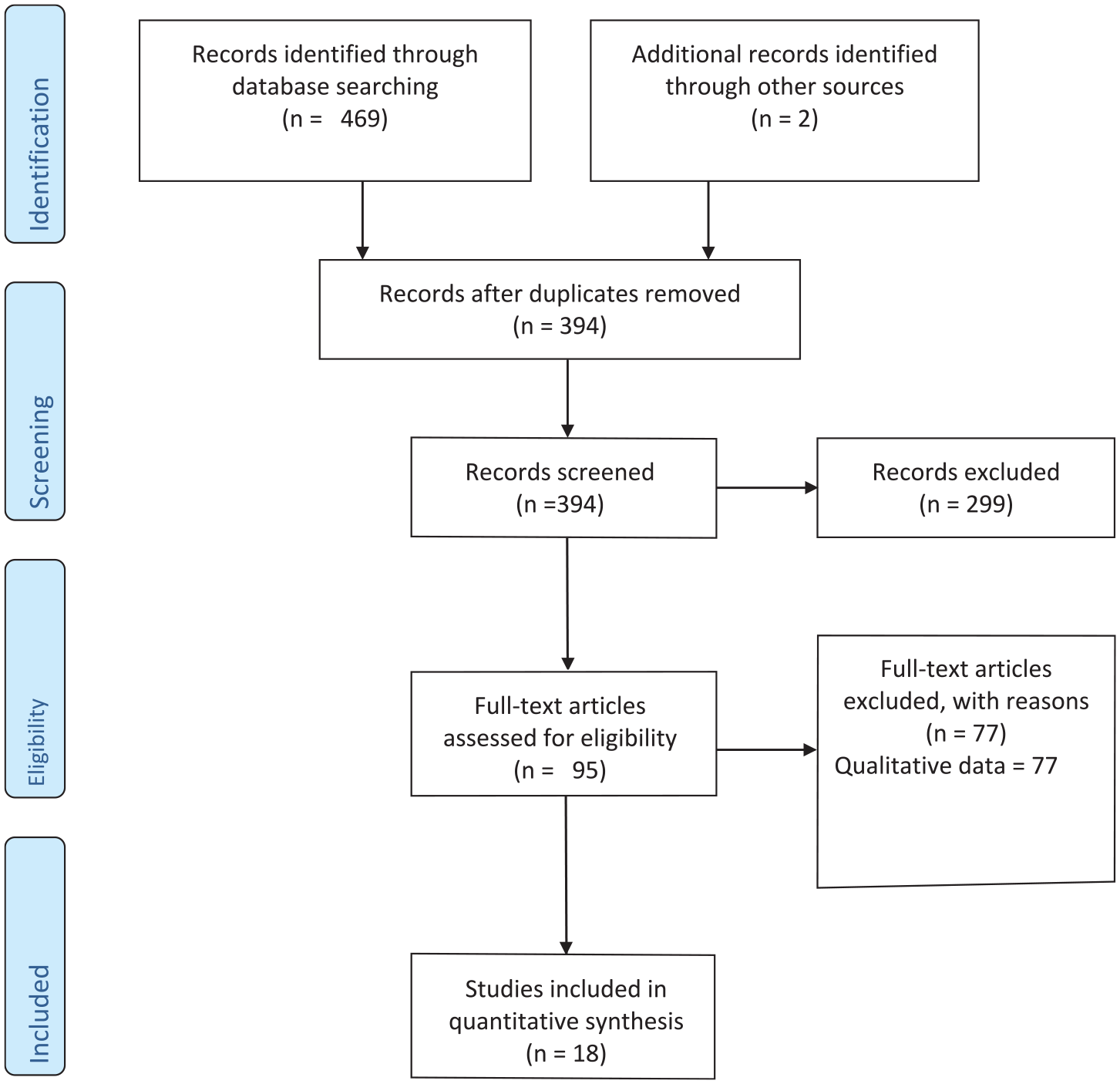
Our search of the databases generated 471 articles that included the CFI terms. Two additional articles were obtained from a published review after we had completed our literature search (Aggarwal et al., 2014; Aggarwal, Jarvis, et al., 2020). After duplicate removal and assessing titles and abstracts, 95 full-text articles were reviewed for eligibility. The quality of articles was assessed using the Quality Ratings Scheme for studies and other evidence (OCEBM Levels of Evidence Working Group, 2011). Six articles received a rating of 2 (i.e., well-designed controlled trial without randomization or prospective comparative cohort trial), six articles received a rating of 3 (i.e., case-control studies or retrospective cohort study), 15 articles received a rating of 4 (i.e., case series with or without intervention; cross-sectional study), 68 articles received a rating of 5 (i.e., opinion of respected authorities or case reports). Of the 95 full-text articles reviewed, 18 were eligible based on the eligibility criteria above (see Figure 1).
CFI Review and Selection of Articles.
Details of the 18 Eligible Quantitative Studies
Ethnocultural Background of the 18 Quantitative Studies
Clinicians’ and patients’ ethnocultural backgrounds included Indian (states of birth—Andhra Pradesh, Assam, Bihar, Gujarat, Haryana, Himachal Pradesh, Madhya Pradesh, Maharashtra, National Capital/Territory of Delhi, Punjab, Rajasthan, Tamil Nadu, Uttar Pradesh, Uttarakhand), Canadian (multicultural), Kenyan (Tribes—Arab, Kalenjin, Kamba, Kikuyu, Kisii, Luhya, Luo, Somali, Taita), Dutch, Peruvian, American (Latino, White, Black, Asian, Native American), and Mexican. Patients were also from ethnic minority populations in the Netherlands from Surinam, Morocco, Turkey, Sierra Leone, Afghanistan, Azerbaijan, Bosnia, Burundi, Guinea, Ingushetia, Iraq, and Rwanda.
Cultural and Contextual Approaches of the 18 Quantitative Studies
None of the 18 studies used interpreters or cultural brokers to stop CFI drift, that is, the introduction of cultural information not from the CFI. Two-thirds (12/18) of the studies matched the languages of clinicians to patients and translated the CFI, forms, and outcome measures. Specifically, of the 12 studies that used translations, all used forward independent translations, 16% of the 18 studies (2/12) had bilingual committees to review translations, 8% (1/12) conducted backward translations, and 8% (1/12) conducted independent piloted translations and made revisions. The CFI was translated into five languages: Dutch, Hindi, Marathi, Mexican, and Spanish. Of the six that did not conduct translations, five were because the training of clinicians was in English, and one was for the development of the CFI Fidelity instrument on a U.S. sample not requiring translation.
Outcome Measures
Twenty-eight percent (5/18) of the eligible studies used a standardized questionnaire called the Debriefing Instrument for Patients (DIP; Lewis-Fernandez et al., 2017), for Clinicians (DIC; Lewis-Fernandez et al., 2017), and for Relatives (DIR; Lewis-Fernandez et al., 2017), which assessed the acceptability, feasibility and clinical utility of CFI for patients, clinicians or relatives, respectively. Attrition rates were mainly very low for CFI, ranging from 3% to 10%. However, one study reported a high rate of 50% (Diaz et al., 2016). An additional two studies to the five studies were identified, noting a standardized measure of the Cultural Competence Assessment Tool (Mills et al., 2017) and Evidence-Based Practice Attitude Scale (Aggarwal, Lam, et al., 2020) to assess clinician’s cultural competence and attitudes toward adopting the CFI protocol respectively. The remaining 11 studies used nonstandardized outcome measures. The 13 studies that did not use the Debriefing Instrument are noted in the results in Table 4 and were omitted from the meta-analysis’ models of the utility, feasibility, and acceptability of CFI.
Mixed-Methods Studies
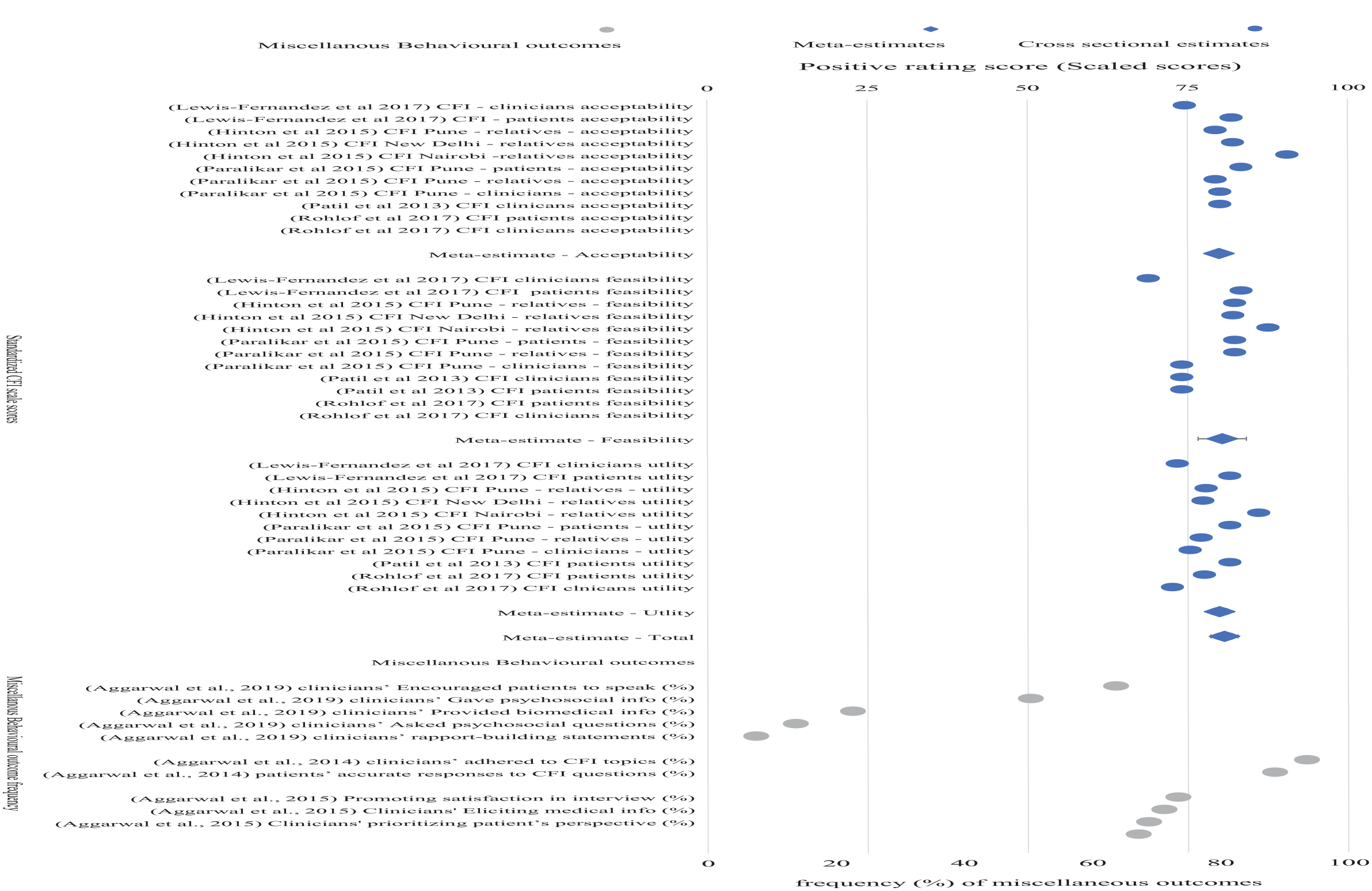
Eight of the 18 studies used mixed methods. The four mixed-methods studies that have been included in the scoping quantitative review using meta-analysis methodology (Hinton et al., 2015; Lewis-Fernandez et al., 2017; Paralikar et al., 2015; Rohlof et al., 2017) are the studies where meta-estimates of CFI-feasibility, CFI-acceptability and CFI-utility could be calculated. The studies by Aggarwal and colleagues (2014, 2015, 2019) that have been added to Table 2 were not included in the calculation of the meta-estimates as they are measuring different outcomes such as patient–clinician medical communication and statements of patients and clinicians during CFI sessions and meta-estimates of CFI-feasibility, CFI-acceptability and CFI utility could not be calculated. These three mixed-methods studies were not included in the meta-estimate calculation but have been included in Figure 4 as miscellaneous behavioral outcomes indicating the percentage of time.
Methodology of Mixed Methods
Of the eight mixed-methods studies, 50% (4/8) used content analysis, 37.5% (3/8) thematic analysis, and one used the Roter interaction analysis system (RIAS), a standardized method for examining medical interviews based on ethnographic studies of small-group communication.
Training Studies
Six of the 18 studies were for the training of clinicians. One study was conducted for training psychiatric residents (Mills et al., 2017), one for the training of clinicians in adult service and regional forensic units (Aggarwal, Lam, et al., 2020), one for the type of training preferences for CFI (Aggarwal, Lam, et al., 2016), one study used a 1-hour training online module (Aggarwal et al., 2018), one study used four by 90-minute sessions as part of a curriculum (Diaz et al., 2016), and one study used an objective standardized clinical examination (Padilla et al., 2016).
Risk of Bias of Included Studies
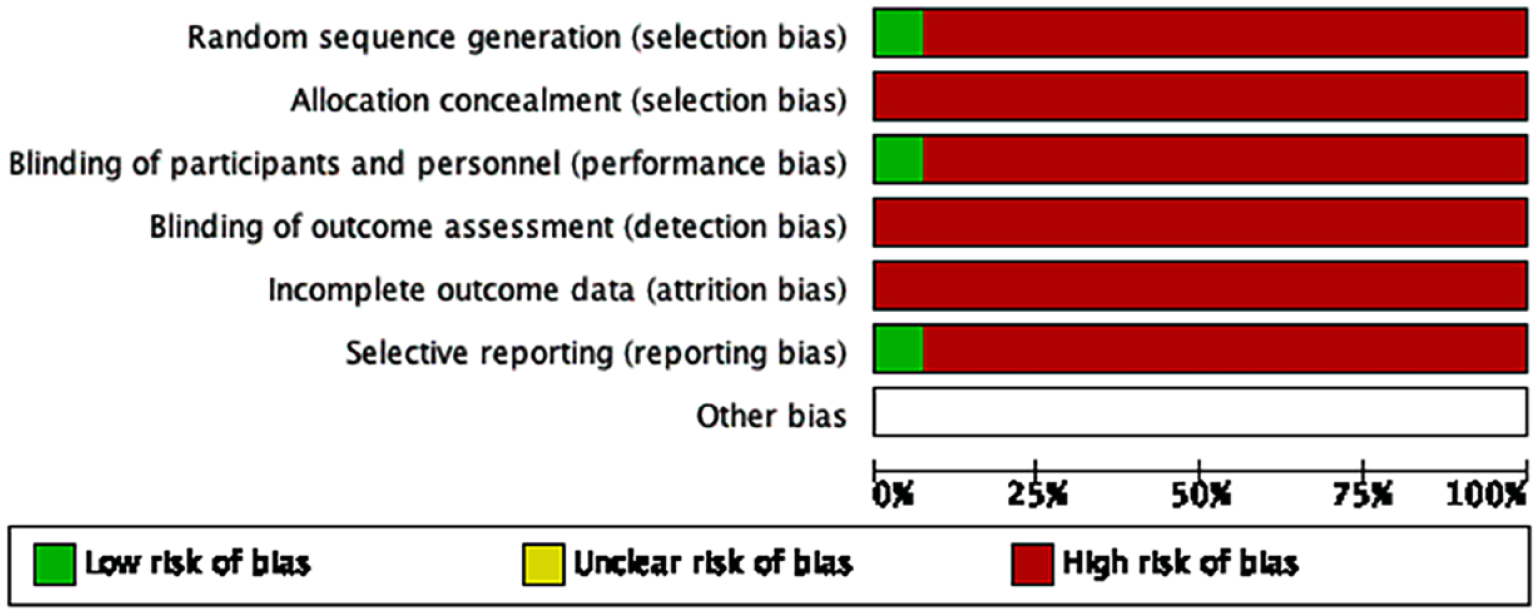
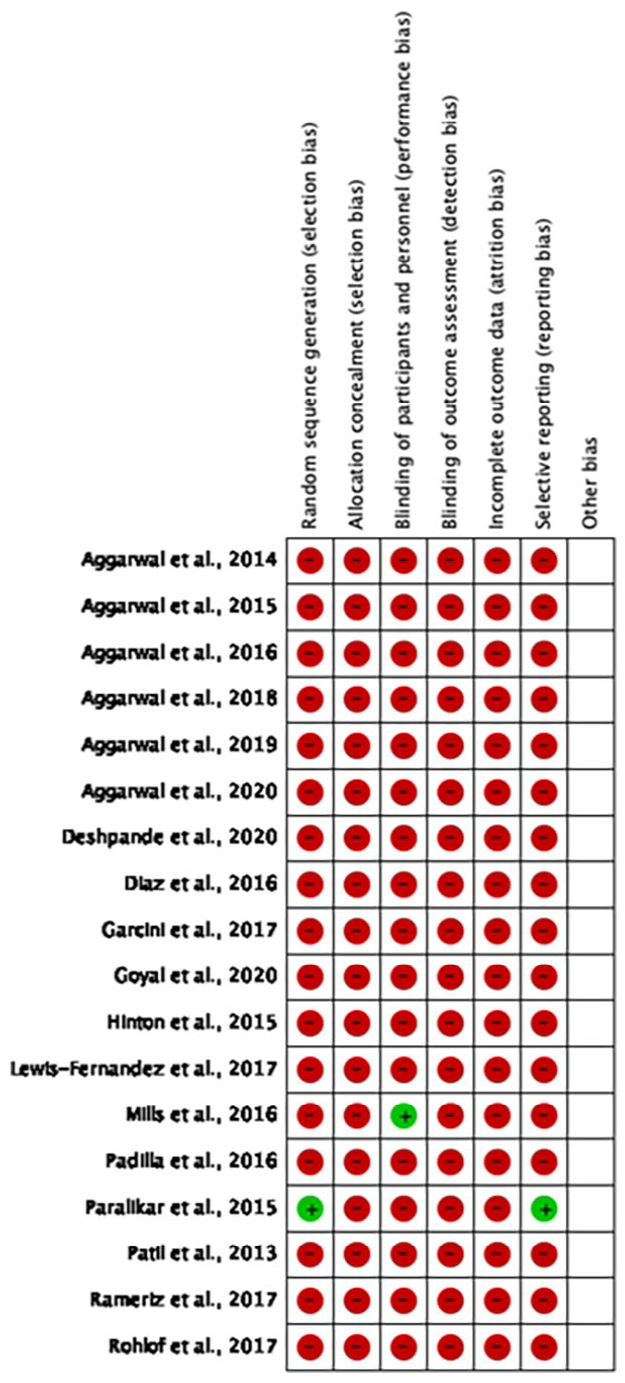
The risk of bias for the 18 included studies with the lead author’s judgments and percentages are summarized in Figures 2 and 3, respectively. Overall, the risk of bias was high across most parameters, except for reporting and attrition biases. All studies are at high risk of selection bias, with about 93% and 100% providing inadequate information regarding the random sequence and allocation concealment, respectively. Blinding of clinicians is not possible, and blinding of patients is very difficult in these types of studies. One study (5.5%) reported blinding of patients, which is important when data are collected via self-report measures. Thus, 94.5% of studies are at high risk of performance bias, and 94.5% of the studies had a high risk of reporting bias with data not fully presented or difficult to analyze. Other sources of biases, such as post hoc statistical analysis, were not reported and were unclear. Figures 2 and 3 demonstrate a clear gap (White et al., 2020) in the volume, type and quality of the evidence available in evaluating the impact of the CFI on patient and clinician outcomes.
Risk of Bias Graph—Review Author’s Judgments About Each Risk of Bias Item Presented as Percentages Across all Included Studies.
Risk of Bias Summary—Review Author’s Judgments About Each Risk of Bias Item for Each Included Study (+ = Low Risk of Bias;—= High Risk of Bias; ? = Unclear Risk of Bias).
Details of the Five Eligible Quantitative Studies With Homogeneous Meta-Estimates
Five of the 18 eligible quantitative studies examining CFI’s acceptability, feasibility and clinical utility were used to calculate meta-estimates of acceptability, feasibility and clinical utility and are reported in Table 3. These five studies are numbered 2, 3, 5, 14, and 15 and bolded in Table 3. All five studies, 75 + 318 (393), 12 + 29 + 30 (71), 36 + 12 + 8 (56), 8 + 12 (20), 30 + 11 (41) = Total 581; n = 581, were published in English, and meta-estimates were calculated based on the homogeneity of the design and outcome measures. However, details of the other 13 quantitative studies are reported in Table 2, and no meta-estimates were calculated due to the heterogeneity of design and outcome measures. These five studies were performed in six countries (i.e., Canada, India, Kenya, Netherlands, Peru, and the USA). Demographic and delivery characteristics were reported for the five studies with meta-estimates only.
For the CFI, of the five studies with meta-estimates, clinicians (17.5%), patients (68.3%), and relatives (14.2%) were evaluated. The total sample size across the five studies is 581. One of the included studies in the current review had a large sample size (i.e., 393 participants), and the other four had small to medium sample sizes (i.e., 20, 41, 56, and 71). The mean age of all the participants in these five studies was 38, of which 49.4% were female.
Delivery Characteristics
For CFI, two of the five CFI protocols (40%) were delivered in a combined individual and group format, one in-group and two as individual. All five studies were comparative cohort studies. Four of the five studies (80%) used didactic training of CFI, which health professionals delivered. In one (20%) of the studies, the clinicians were instructed only to ask the standardized questions of CFI protocol.
Effects of Intervention
Thirty-four estimates from five studies were used to calculate a meta-statistic estimate for each of the Acceptability, Feasibility, and Clinical Utility of the CFI outcomes. Estimates from the individual studies and the meta-estimation across studies are presented in Table 3 and as a forest plot in Figure 4.
Forest Plot for Acceptability, Feasibility and Clinical Utility of CFI.
Multi-level model estimates of CFI scores demonstrated high rates of Acceptability (80% [79 to 81]), Feasibility (80% [77 to 84]), and Clinical Utility as subscores (78% [76 to 81]), and total score (81% [78 to 83]).
The estimation of the CFI meta-estimate did not change as a result of the variance in the quality of study score (Q = .65, p =.648), the sample size of the studies (β = −0.20, p = .14), nor was the meta-estimate impacted by a Trim and fill estimate (β = −0.16, p = .09) that added 10 mirrored estimates to the sample (see Supplemental Table 1).
The estimation of CFI total scores differed significantly across the surveyed subgroup of clinicians, patients and relatives (Q = 100.36, p < .001), with clinicians showing attenuated but overall positive scores (76 [73 to 78]). CFI total score estimates from research or clinical practice contexts did not differ (Q = 0.67, p =.185).
Additional test statistics, heterogeneity statistics, and subgroup means are reported in Supplemental Table 1.
Discussion
This article conducted a quantitative systematic review using a mixed-methods synthesis methodology whereby the quantitative data were extracted from quantitative and mixed-methods studies (Petticrew et al., 2013), and the quantitative evidence on the impact of the CFI on patients and clinicians was synthesized. The review of the evidence found quantitative support for the effect of the CFI in five comparative cohort studies with comparable reported outcomes on the feasibility, acceptability, and clinical utility of the CFI on patient and clinician satisfaction. Furthermore, the review found 10 studies with categorically different outcomes (including four with repeated measures design) that evaluated the effect of CFI on improving clinicians’ cultural competence. We found the recommended minimum of five studies for inclusion in systematic reviews and meta-analyses (Yaffe et al., 2012) exceeded the Cochrane minimum standard of two studies for meta-analyses (Ryan, 2016). The current review of the quantitative evidence of the CFI on clinician and patient outcomes highlights the significant gaps in the evidence for the CFI because of the limited number of comparable studies (n = 5), as well as the high heterogeneity and high risk of bias in the studies that could not be included in the meta-analysis (n = 18). Moreover, no quantitative data are available on the impact of CFI on the therapeutic alliance, patient symptoms and functioning. This review of the available literature demonstrates the need for more quantitative research to examine the efficacy and effectiveness of the CFI on outcome.
The CFI was an acceptable, feasible, and clinically useful assessment tool. Patients rated the CFI most favorably, followed by relatives of patients and then clinicians. The scores in all groups were positive, suggesting the CFI is acceptable, clinically useful and feasible. However, there was no quantitative data on the direct (i.e., therapeutic alliance) or indirect effect (i.e., symptom reduction and improved functioning) of the CFI on patient outcomes, limiting the recommendation for the broader use of the CFI in clinical practice. Future research is needed to evaluate the direct impact of the CFI on the therapeutic alliance, which is one of the consistent predictors of outcome and accounts for 36% to 50% of the variance in improved treatment outcomes in therapy (Duncan, 2014), and evaluate the use of the CFI on the outcomes of patient functioning and psychological symptoms.
The available data on the impact of the CFI on clinicians’ cultural competence are favorable, but the lack of a standardized protocol makes it impossible to provide a reliable estimate of the effect. The current review found evidence that clinician training in CFI improves cultural competence, but the heterogeneity of outcome measures prevented the calculation of a meta-estimate.
The study’s main limitations are the small number of studies included in the meta-analysis (n = 5) and the absence of any RCTs. Another limitation is the potential bias of one dominant study in the scoping quantitative review using meta-analysis methodology (Lewis-Fernandez et al., 2017), with 68% (393/581) of the total participants. However, a sensitivity analysis of sample size found that the sample size of the selected studies was not a moderator of the meta-estimate calculated. A further limitation is that the meta-estimates were based on converted Likert-type scales, which measure favorability rather than from effect sizes of RCTs measuring the efficacy of CFI, meaning any interpretation of CFI’s efficacy must be reported cautiously. At best, the CFI is seen as favorable by patients, clinicians, and relatives and shows the potential of being a helpful assessment tool when engaging with culturally and linguistically diverse cohorts.
The high risk of bias and heterogeneity of the 18 quantitative studies highlights the methodological gaps in the current CFI literature. The results of the CFI, which are based purely on the self-report of patients, relatives, and clinicians, are in Phase I of clinical trials, that is, feasibility trials that use a single group design with no comparator control group (Australian Clinical Trials, 2023). As yet, no Phase II RCTs have examined the impact of CFI on both patient and clinician outcomes. This gap could be because most CFI trials were conducted in hospital settings, where it might not be easy to establish the controlled conditions required for an RCT. Also, RCT designs require resources and time that may exceed the scope and budgets of many services. Recently, a pragmatic RCT was conducted in Sweden to assess the impact of CFI on routine psychiatric diagnoses that found use of the CFI may facilitate the identification of symptoms of specific psychiatric disorders (e.g., depression among migrants who are nonnative Swedish speakers; Wallin et al., 2022). Future research will need to move beyond Phase I trials to adequately controlled trials of the effect of the use of the CFI on therapeutic outcomes. One promising study protocol is a multicentre RCT to assess the effect of the CFI on therapeutic working alliance and the potential role of perceived empathy among migrant outpatients of mental health centers in the Netherlands (Brand et al., 2024).
Despite the preliminary nature of the evidence, the CFI provides an approach that places culture at the center of the assessment and treatment of all health conditions, not just mental health conditions. During the COVID-19 crisis, and in line with the Shifting Cultural Lens model (López et al., 2020), the CFI was used to develop clinical practice guidelines that explored the patient’s and clinician’s explanatory models of COVID-19 and cultural preferences, negotiating a shared view or building a collaborative cultural formulation that promotes the patient’s sense of cultural safety and the clinician’s expertise (Kayrouz et al., 2021). This cultural/contextual approach of the CFI provides a framework for clinicians to respond to this diversity of beliefs about COVID-19 in a culturally safe manner while maintaining ethical obligations of providing the best available information and evidence about COVID-19 and vaccinations (Kayrouz et al., 2021).
Road Map Forward
The American Psychological Association Presidential Task Force on Evidence-Based Practice (2006) provides a road map that recommends “the integration of the best available research, with clinical expertise in the context of patient characteristics and preferences” (p. 273). The CFI provides clinicians with a comprehensive assessment tool that considers the context of patient characteristics and preferences and has preliminary and emerging evidence. However, the DSM-5 Cross-Cultural Issues Subgroup (DCCIS) recommendation that the CFI be used with all patients in routine care (Aggarwal, Jimenez-Solomon, et al., 2016) needs to be considered with caution as the current evidence for the CFI is favorable and preliminary, but more trials evaluating the efficacy of CFI in large RCTs and then in routine care are required. Consistent with a recent scoping review (Jones-Lavallée et al., 2023), it is recommended that patients complete standardized outcome measures for therapeutic alliance, psychological symptoms and functionality at initial assessment and pre-treatment only to assess the impact of the CFI on patient outcomes before treatment commences. Furthermore, this scoping review highlighted other gaps: (a) most of the research lacks replication across different research teams, with the same data from the same research team interpreted in a variety of ways; (b) generalizability across different settings is limited; (c) the need to include interpreters and translate the CFI into more languages; and (d) research evaluating the effectiveness of cultural training (Jones-Lavallée et al., 2023).
One critical recommendation for the CFI is a need for a standardized methodology in the training and practice of the CFI. This current quantitative review highlighted several disparate evidence-based CFI training and practice studies requiring synthesis. In terms of the training of the CFI, it is recommended that the evidence-based 1-hour online training module be considered as the didactic component (Aggarwal et al., 2018). Following the experiential and direct observation component, the evidence suggests behavioral simulations or role-plays as the preferred training mode for clinicians (Aggarwal, Lam, et al., 2016). The CFI in training needs to be presented in a linear format to clinicians for familiarization with the CFI questions, and then, clinicians need to be encouraged to use the CFI with more flexibility through interdisciplinary case discussions to avoid cultural formulations essentializing culture and ensure patients’ sense of cultural safety (Rousseau et al., 2020). In terms of evaluating the effectiveness of the training on clinicians’ cultural competency, the content of the CFI and the process of application of the CFI to the patient’s presentation need to be measured (López et al., 2020). The content-orientated outcome measure could use the CFI Fidelity instrument, providing the clinician with a CFI fidelity score (Aggarwal et al., 2014). The process-orientated outcome measure could use the key in-session behaviors from the Shifting Cultural Lens Model during the behavioral simulations or role-plays as measured by expert observers to assess the clinician’s cultural competency in training (López et al., 2020). A similar protocol could assess a clinician’s cultural competency in routine care, excluding the didactic component, with the behavioral simulation being the therapeutic consultation with the patient in routine care.
Conclusion
The CFI holds some promise and is viewed as favorable by patients, their relatives and clinicians, as well as improving clinicians’ cultural knowledge. More research using standardized protocols in research, training, and practice is needed to examine the effect of the routine use of the CFI on outcomes for both patients and clinicians.
Supplemental Material
sj-pdf-1-jcc-10.1177_00220221241269994 – Supplemental material for A Quantitative Systematic Review to Evaluate the Favorability of the DSM-5 Cultural Formulation Interview (CFI) on the Acceptability, Feasibility, and Clinical Utility for Clinicians, Patients, and Relatives
Supplemental material, sj-pdf-1-jcc-10.1177_00220221241269994 for A Quantitative Systematic Review to Evaluate the Favorability of the DSM-5 Cultural Formulation Interview (CFI) on the Acceptability, Feasibility, and Clinical Utility for Clinicians, Patients, and Relatives by Rony Kayrouz, Eyal Karin, Lauren Staples, Olav Nielssen, Shane Cross, Blake F. Dear and Nickolai Titov in Journal of Cross-Cultural Psychology
Footnotes
Acknowledgements
The research and evaluation team of the MindSpot Clinic is gratefully acknowledged.
Author Contributions
R.K. conceived and designed the study, conducted literature review, interpreted the data, and drafted the manuscript. E.K. conducted analyses and drafted the analysis sections of the manuscript. N.T., B.D., E.K., L.S., O.N., and S.C. reviewed the design, analysis, interpretation of data, and the manuscript. All authors have contributed to, read, and approved the manuscript.
Data Availability
Access to data will be provided for the purpose of verifying the findings presented in the current study. Access will be provided to researchers, subject to a formal written request, the generation of a methodologically sound research protocol, the establishment of appropriate data governance, and the approval of an independent and recognized Human Research Ethics Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.