
Abstract
Treating culturally diverse patients (CDPs) presents considerable challenges for psychotherapists, including language barriers, differing beliefs, and insecurities. Improving their transcultural competence requires training, but empirical evidence is lacking. This 6-week randomized controlled trial evaluated the impact of standardized internet-based training on psychotherapists’ transcultural competence (i.e., awareness, engagement, and handling challenges). Demographic data were collected before training. Transcultural competence was measured at pre-training, post-training, and 3-month follow-up. Training satisfaction was assessed at post-training and follow-up visits. In the guided training group (GTG; n = 83), psychotherapists received hands-on training with practical exercises, weekly knowledge assessments, and online feedback. The second condition comprised a non-guided control group (CG; n = 90) that received only text-based training. Primary analyses on both intent-to-treat (n = 173) and completer analyses (n = 95) indicated significant improvements in transcultural awareness and engagement after 6 weeks of training for both groups. Significant within-group improvements were noted, as evidenced by large Cohen’s d effect sizes for both groups. No between-group differences were observed. Qualitative assessments revealed that GTG participants evaluated the training’s concept and content significantly more positively than CG participants and felt significantly less insecure about treating CDPs. Such training could pave the way for the long-term development of innovative, culturally sensitive mental health care services that more effectively meet the needs of CDPs.
Given the ongoing political conflicts worldwide resulting in increased rates of forced displacement, the issue of cultural diversity in psychotherapy has rapidly increased in importance (United Nations High Commissioner for Refugees, 2020). Throughout the migration process, people experience high levels of stress and are specifically vulnerable to developing mental health conditions, including posttraumatic stress disorder, depression, and anxiety (Acarturk et al., 2016; Borho et al., 2020). In his review of barriers to mental health services for displaced individuals, Satinsky et al. (2019) emphasized the role of therapist training.
While training for psychotherapists can positively affect the mental health of refugees (Mattar et al., 2023), transcultural therapy settings continue to present therapists with several challenges, including divergent values and concepts of illness and disease models, language barriers, misdiagnosis, and prejudices (Potter et al., 2023). Treating culturally diverse patients (CDPs) can cause practitioners to feel frustrated and helpless (Costa & Dewaele, 2018), which may make them reluctant to offer treatment (Mösko et al., 2012). Patients in these settings often display lower treatment adherence and higher dropout rates than regular patients (for a review, see de Haan et al., 2018). Other challenges include the need for interpreters, cultural variations in emotional expression, concerns about cultural misunderstandings, missing information about mental health services, and passive care attitudes (Asfaw et al., 2020; Costa & Dewaele, 2018; Mösko et al., 2013). However, there is a lack of focused training for psychotherapists treating patients of diverse backgrounds (Costa & Dewaele, 2018; Naz et al., 2019).
Scope of Previous Training
Transcultural competence training is vital to refugee treatment (Mattar et al., 2023; Naz et al., 2019) and is helpful for therapists (Costa & Dewaele, 2018). The ethical principles of psychologists mandate a culturally competent behavior (American Psychological Association [APA], 2017); furthermore, it has been affirmed as a foundation for treatment (Asfaw et al., 2020).
Despite the abundance of training approaches (Mattar et al., 2023), training that fosters mental health care for ethnically diverse patients is limited to specific disorders or treatment modalities (for meta-analyses, see Rathod et al., 2018). Most training approaches are designed for nursing staff (Oliynyk & Pedorenko, 2019) and undergraduate students in social work (Gruner et al., 2020) rather than psychotherapists. Some trainings address therapy for specific ethnic groups (e.g., Acarturk et al., 2016); others focus on the transcultural treatment of specific disorders (e.g., Kip et al., 2020) or specifically adapted training procedures (e.g., imaginary rescripting, Lechner-Meichsner et al., 2022; narrative exposure therapy, Hijazi et al., 2014), often limited to English-speaking therapists (Benuto et al., 2018; Bhui et al., 2007).
While transcultural competence can be operationalized in various ways, it usually involves the development of awareness, knowledge, and skills that enable practitioners to effectively work across cultures (Sue et al., 1992). This includes (a) awareness—the ability to recognize one’s own cultural biases and assumptions; (b) knowledge—the understanding of different cultural values, beliefs, and behaviors; and (c) skills—the ability to adapt one’s behavior and communication.
von Lersner et al. (2019) provide clear learning objectives, emphasizing self-reflection and acquiring culturally sensitive skills for positive therapeutic outcomes. von Lersner and Kizilhan (2017) introduce key theoretical concepts for culturally sensitive psychotherapy, covering Hofstede’s (2001) cultural dimensions, Kirmayer at al. (2011) psychological phases of migration and relevant diagnostic tools (Cultural Formulation Interview; APA, 2013).
Few training approaches improve therapists’ transcultural competence (Chu et al., 2022). Notably, von Lersner et al. (2019) reported psychotherapists’ cultural knowledge and awareness improved after training. Significant effects on culturally specific therapeutic skills have been reported after a 3-month follow-up period (Kulik & Roberson, 2008; von Lersner et al., 2019). Both transcultural awareness and skills are associated with patient adherence, satisfaction, and improved treatment outcomes (Owiti et al., 2014). Costa and Dewaele (2018) reported that training increased awareness of the psychotherapist’s and patient’s own perspectives and reduced unconscious fears and biases, concluding that training can facilitate professional interactions with CDPs.
Research on transcultural competence training to enhance transcultural competence for psychotherapists is sparse (for a review, see Satinsky et al., 2019), although there are defined quality criteria for such programs (Benuto et al., 2018; Mösko et al., 2012). Existing trainings have rarely been evaluated with a randomized controlled trial (RCT) design with follow-up assessment (for reviews, see Benuto et al., 2018; Venkataramu et al., 2021), present vague descriptions of study and curricular content (for reviews, see Benuto et al., 2018; Bhui et al., 2007), and lack evidence of their effectiveness (Benuto et al., 2018; Venkataramu et al., 2021).
Purpose
Our RCT evaluated an internet-based training program to improve psychotherapists’ transcultural competence. Its theoretical concept was based on the three-factor model by Sue et al. (1992). The training was operationalized as a learning process integrating a set of skills, behaviors, attitudes, and ongoing practices (Sue et al., 1992). Transcultural competence comprises the following three components: transcultural engagement, awareness, and handling challenges (Atzor et al., 2022).
According to Vega (2005), brief training sessions without professional guidance rarely improve transcultural competence. Contrastingly, ongoing support fosters learning, offering a safe environment for reflection and personal growth (Zhao et al., 2022). Valenstein-Mah et al. (2020) found that incorporating online consultation significantly enhances the acceptability of training. In addition, internet-based training with practical and engaging components can significantly elevate cultural awareness (e.g., Kaihlanen et al., 2019).
We included two conditions to evaluate the impact and satisfaction of practical guided training (guided training group, GTG; i.e., including individual online support and hands-on interactive tasks) versus non-guided text-based training (control group, CG). We hypothesized that participants in the GTG would report higher transcultural awareness, higher levels of engagement, and a better ability to respond to challenges than the CG at post-training and follow-up measurements. The significance of participant satisfaction in training extends to its potential impact on patient care and training effectiveness. Higher satisfaction levels among participants are linked to improved learning outcomes and increased motivation to apply learned competence in practice (Shao et al., 2018). We thus investigated whether participants in the GTG would report higher satisfaction with the training and its modules at post-training than the CG.
Methods
Study Design and Procedure
The study was approved by the ethics committee of the department of psychology at our university and registered with clinicaltrials.gov (no. NCT03038347). The primary outcome measure was the OnTracc questionnaire, which has been validated (Atzor et al., 2022). Data were collected across Germany as part of a project conducted at the University of Marburg, in collaboration with the Humboldt University in Berlin, from September 2020 to January 2021.
Participants were recruited through both social media (Facebook, Twitter, and Instagram) and national educational institution mailing lists. Registered clinical psychologists working in private practices within the county of Hesse in Germany were invited via their publicly accessible email to participate. The primary eligibility criterion was that participants were psychotherapists or psychiatrists (licensed or in postgraduate training) for adults or children and adolescents. Another prerequisite was that participants were interested in expanding their transcultural therapy competence and had sufficient time and motivation to work on the training modules (about 1 hour per week for 6 weeks).
After signing informed consent, participants were randomly assigned via computer-generated random numbers (www.randomization.com) to either the GTG or CG. The simple randomization method was used (Suresh, 2011), and a random allocation sequence with equal randomization (allocation ratio 1:1) was generated. Randomization was conducted by a researcher not involved in this study. Participants logged into the platform and started completing the initial questionnaire. Upon completing the first module, they unlocked access to the subsequent module, and this process continued on a weekly basis until all six modules were available on the platform. Following the training, participants received the post-training and follow-up questionnaires via email, and reminders were sent to ensure timely completion, if needed. After completing the follow-up assessments, full participation was rewarded with a certificate of attendance. Licensed therapists received accreditation from the Hessen Chamber of Psychotherapists in Germany.
Training Content
The training modules were exclusively created for this study, newly developed by an expert team of practicing psychotherapists and researchers in the field of transcultural psychotherapy from the Universities of Marburg and Berlin. While this specific online training has not been evaluated in other studies prior to this research project, the conceptual framework was mainly based on von Lersner and Kizilhan (2017) and the established Guidelines for Transcultural Competence Training of Psychotherapists (von Lersner et al., 2016). Contrary to von Lersner et al.’s (2019) training, which occurred in person over 2 consecutive days and again for 1 day after 3 weeks, our content was fully implemented online through personal login via a website, providing flexibility and accessibility from any location. The internet-based training comprised six E-learning modules and encompassed additional important topics beyond the approach of von Lersner et al. (2019), including an introduction to transcultural models within the diversity concept, critical reflection on transcultural interactions with a focus on prejudices and discrimination, post-migratory acculturation processes and their influences on psychotherapeutic settings, and culturally sensitive measurements in diagnostics (Supplemental Appendix Table A). The training centers on CDPs, encompassing individuals from diverse cultural backgrounds, including immigrants and refugees, who often face similar mental health challenges (Sangalang et al., 2019). We emphasized the specific challenges that refugees may encounter to better address their unique needs and experiences.
The first module was designed to establish participants’ personal learning goals and encourage reflection. In each subsequent module, the new learning content was presented first before a short scientific introduction to the module’s topic was given. Descriptions of different fictional patients accompanied participants in all modules. The modules concluded with a summary of the key messages, followed by an outlook for the next module. Participants had the option to provide ratings for each module based on its helpfulness and comprehensibility.
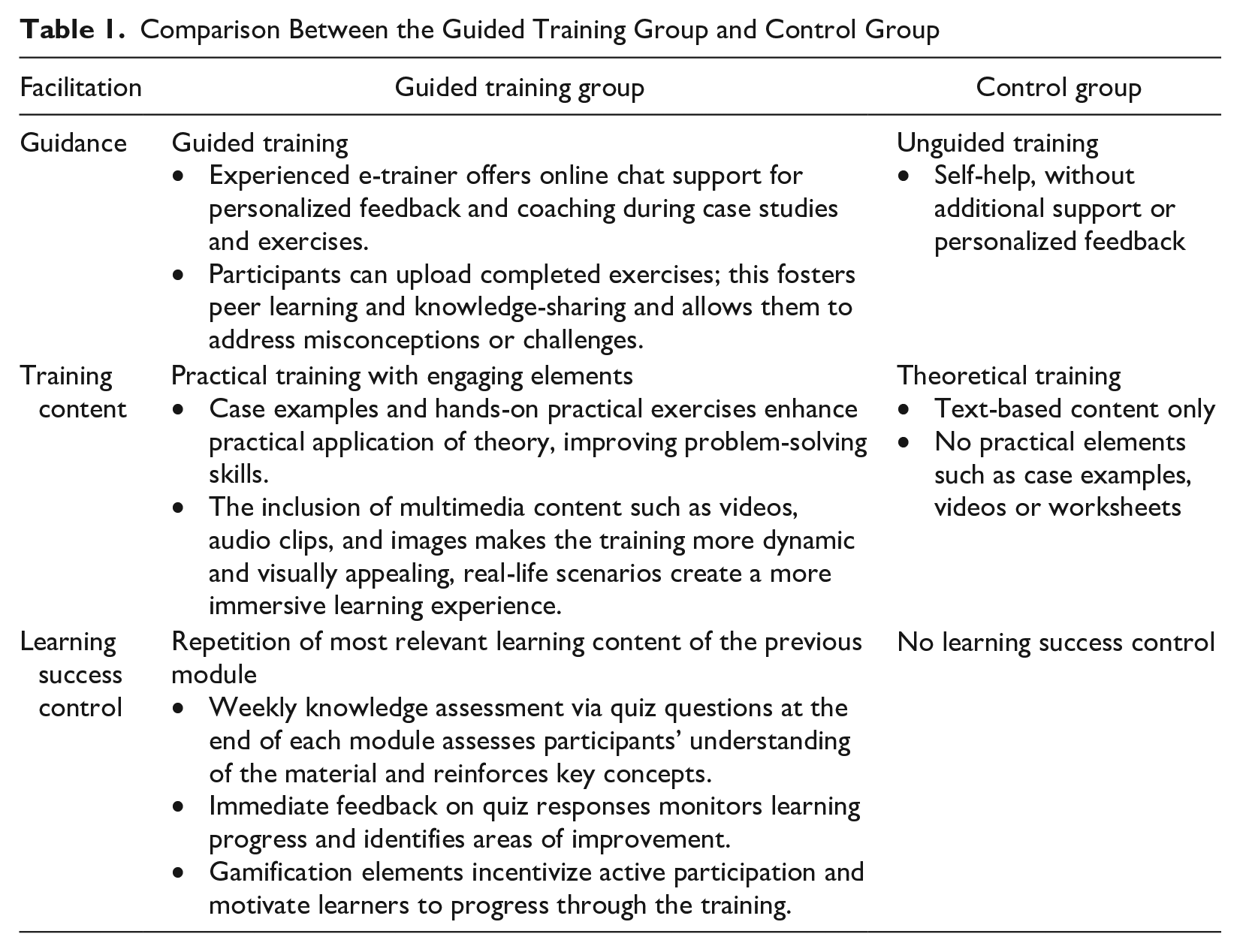
Module structure and content were identical for both groups. Participants assigned to GTG additionally received hands-on exercises with the aim of deepening the theoretical contents. These exercises varied and included information texts, case examples, videos (which include informational material, testimonials, or exercises), self-reflection exercises with self-awareness components (e.g., self-reflection on one’s own cultural integration), additional worksheets, and open or multiple-choice quiz exercises. The interactive and engaging elements of the practical training included weekly knowledge assessments to reflect on the learned content at the end of each module. The GTG further received optional feedback and guidance via online chat from a transcultural e-trainer, instructed in transcultural therapy. The CG received pure text-based training without further practical training or guidance; their modules were not editable (Table 1).
Comparison Between the Guided Training Group and Control Group
Assessment Instruments
Data were acquired before (pre), immediately after (post), and 3 months after (follow-up) the training. General sociodemographic data (age, sex) were assessed in Section (1). Section (2) assessed their psychotherapeutic education and expertise. Section (3) surveyed their work experience with CDPs. Finally, previous training experience in transcultural therapy and their needs and expectations for this training were surveyed.
Primary Outcome Measure: Transcultural Competence (OnTracc)
Transcultural competence was measured with the OnTracc questionnaire (Atzor et al., 2022) since no other adequate instrument for the context of psychotherapy was available in German. The inventory was developed with a specific focus on assessing transcultural competence in the context of psychotherapy in Germany, particularly when working with patients who have had migration experiences. It comprises 38 self-report items on awareness (e.g., “I integrate my patients’ culturally shaped explanation model into therapy”), engagement (e.g., “I am actively involved in the process of reducing barriers for refugees and people with a migration background in accessing psychotherapy”), and challenges (e.g., “I succeed in building good therapeutic relationships with my patients despite cultural differences”) in transcultural therapy. The reliability of the original subscales ranged between ω = .66–.76 (based on McDonald’s omega). Reliability in this study for pre-training, post-training, and follow-up training was acceptable at ω ≥ .73 (Watkins, 2017). Test–retest reliability was good with Pearson’s r-values ≥.87.
Secondary Outcome Measure: Training Satisfaction at Post and Follow-Up
Secondary outcome measures included training satisfaction questionnaires related to content and scope, as well as optional module ratings for participant evaluation. Participants’ perceptions of module comprehensibility and helpfulness were measured weekly after module completion with two items rated on a five-point Likert-type scale from (1) not at all comprehensible/helpful content to (5) very comprehensible/helpful content. Furthermore, an open question to freely comment on the module as well as a rating of overall satisfaction with the module (ranging from 1 [I liked the module less] to 5 [I liked the module very much]) were included. To assess knowledge acquisition, the GTG responded to five quiz questions pertaining to the respective module’s content.
Overall training satisfaction was assessed directly after finishing training (post-training). Based on 16 items, three factors (implementation of the content, trained competence, and scope) were mapped. They included the structure, scope, and technical implementation of the course of training, ease of use, and comprehension. The study operationalized whether the training helped address uncertainties in the treatment of CDPs.
The transfer of acquired transcultural competence in everyday therapeutic work was measured 3 months after training (3-month follow-up). Participants were asked whether they had been able to apply the contents and whether they felt that their willingness to treat CDPs had changed, respectively, in the long term. Qualitative feedback was measured through open-ended questions at post-training and follow-up. Participants reflected on experiences and suggestions about the training content, structure, and overall training process. Data were systematically and iteratively analyzed using codes to categorize and label themes, identifying key statements and recurring patterns. Summarized in tables, the findings were validated by comparing them with quantitative results.
Statistical Methods
Internet-based training for transcultural competencies in the psychotherapeutic context has not yet been systematically evaluated. However, existing training in the broader field of transcultural encounters shows small to medium effects. Accordingly, we based our power calculations on a medium effect (f = 0.25, α = .05, power 95%; Benuto et al., 2018). Using G*Power (Faul et al., 2007), a 2 × 3 multivariate repeated-measures analysis of variance (MANOVA) yielded a total sample size of N = 74. For primary analysis, the OnTracc factors (awareness, engagement, challenges) were included as dependent variables in a 2 (group: CG vs. GTG) × 3 (time: pre-training, post-training, follow-up) MANOVA to test for differential changes over time. According to the Greenhouse-Geisser criterion epsilon >.75, the Huynh-Feldt correction was used. The partial eta squared was converted into the most widely used effect size d according to Cohen (1992).
As Andrade (2022) recommended, analyses were conducted for both the sample of completers (per protocol) and for an intent-to-treat (ITT) sample (Armijo-Olivo et al., 2009). ITT analyses present data from all randomized participants, regardless of whether they dropped out completely or participated irregularly. ITT analyses were conducted using hierarchical linear modeling, testing full factorial models, including effects of group, time, and the interaction between the two factors. Completer analyses included only those participants who completed this study per protocol. For dropout analysis, Little’s Missing Completely At Random (MCAR) test (Li, 2013) was employed to test the assumption that data occured completely at random. Internal consistency of the measures used in this study was determined using McDonald’s omega (Hayes & Coutts, 2020). Group comparisons of baseline data, secondary outcomes, and confounding variables were conducted using independent t-tests or Mann–Whitney U and χ2 tests, depending on the data level. All statistical analyses were conducted using IBM SPSS statistics (Version 21) and the RStudio Team (2020).
Results
Sample Attrition
Of the 186 potential participants who registered, 13 did not start the training and were excluded before randomization. Accordingly, 173 participants completed the survey at pre-training and were randomized to the GTG or CG. Some participants completed only pre-training, but no further measurement was obtained (never returned: n = 56; GTG: n = 33; CG: n = 23), making them ineligible for completer analysis. Other participants completed pre-training, then dropped out of the survey at post-training, but returned to the training at follow-up (returned at follow-up [t3]: n = 12; GTG: n = 4; CG: n = 8). At post-training, 105 provided complete datasets (GTG: n = 46; CG: n = 59). At follow-up, 95 fully completed the questionnaires (GTG: n = 41; CG: n = 54); 10 participants, 5 in each group, completed the post-training but were lost to follow-up. Finally, 95 were included in the completer analysis and 173 in the ITT analysis (Figure 1).
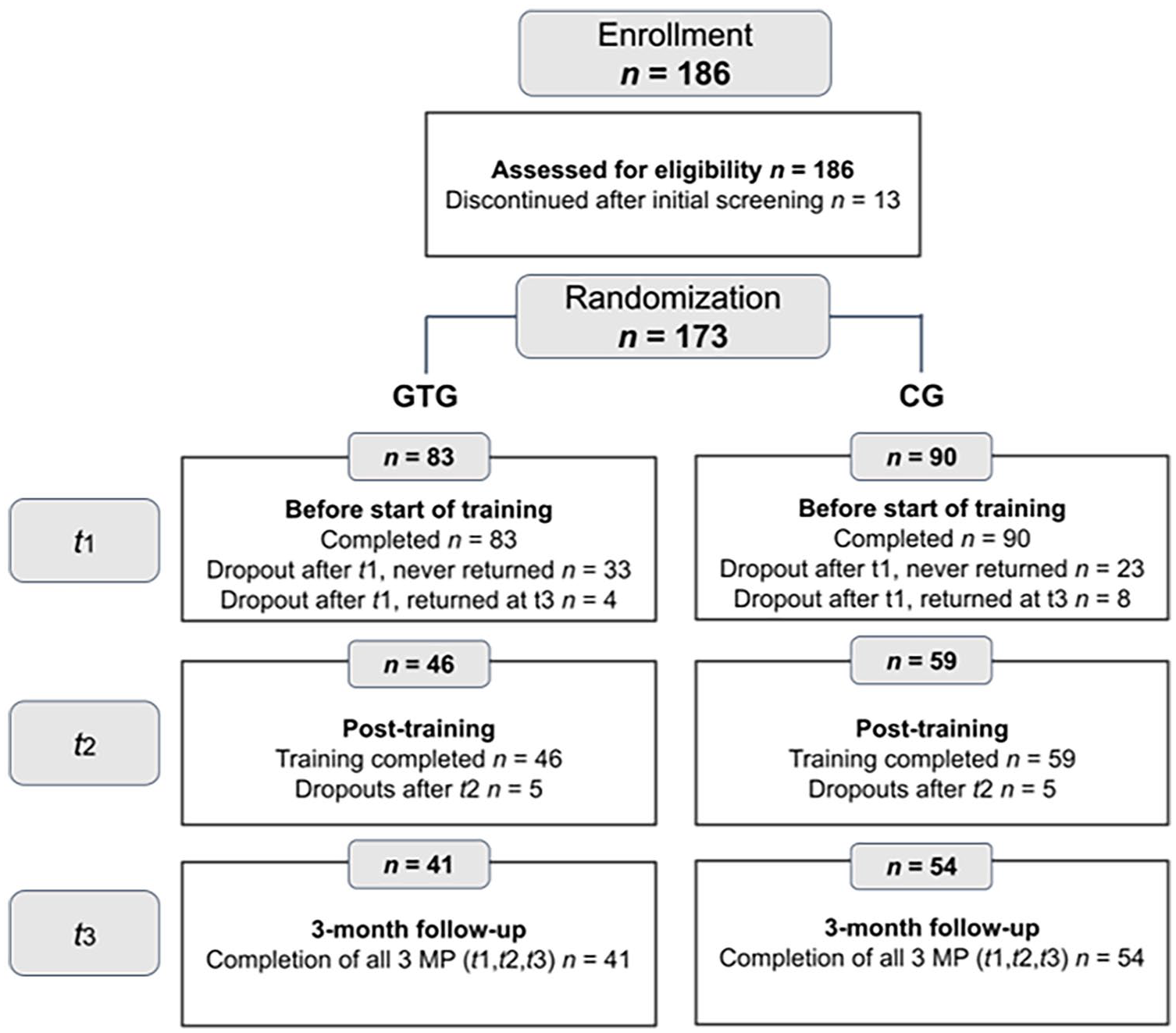
Flow Diagram of Participants.
Comparisons of the dependent variables and demographic and clinical characteristics between completers and dropouts at pre-training and post-training were calculated using analyses of variance and χ2 tests. Participants who dropped out did not differ from those who remained in this study in the variables analyzed (ps > .05). Dropouts at post-training and follow-up had read significantly fewer modules than completers in both groups, t(88.40) = 11.32; p < .001. The qualitative analysis of the comment section on the platform revealed that participants cited various reasons for dropout, with a predominant theme being limited time availability owing to personal circumstances. These circumstances included sickness and disruptions caused by the COVID-19 pandemic, with other prioritized commitments. The non-significant MCAR test, χ2(15, n = 173) = 12.85, p = .61, showed that all dropouts were missing completely at random; that is, their missingness did not depend on either of the observed or missing values.
Sociodemographic Data
Table 2 shows the demographic characteristics of GTG and CG at baseline. The total completer sample consisted of 95 mental health professionals (81.1% women; aged 21–75 years [M = 39.05, SD = 13.88]). Participants’ occupational psychotherapeutic experience ranged from 0 to 45 years (M = 9.69; SD = 11.06). More than half were licensed (52.6%; mostly adult psychotherapists). The most common field of practice was cognitive behavioral therapy (75.8%); most worked in outpatient clinical settings. Furthermore, 10.5% had immigrated to Germany. Participants spoke more than two languages fluently (36.4%), and 52.6% had lived abroad for more than 6 months. Some volunteered with refugees (28.3%). Most had already worked with CDPs (84.2%), although only 6.3% conducted specific cultural supervision. Around a third (36.8%) had already participated in further training on the broader topic of “culture in psychotherapy.” When asked about their motivation for attending training, 87.9% said it was for continuing personal education, and 72.8% thought participation was necessary for their education. Others saw it as an important contribution to research (41.6%). Only 5.8% and 7.5% said it was relevant for their own research or a pastime, respectively. To investigate the potential causes of attrition, we compared the baseline attributes of the ITT samples between those who remained at follow-up. The completer and ITT sample did not differ significantly for any variables.
Sociodemographic Characteristics of Completer and ITT Sample at Baseline.
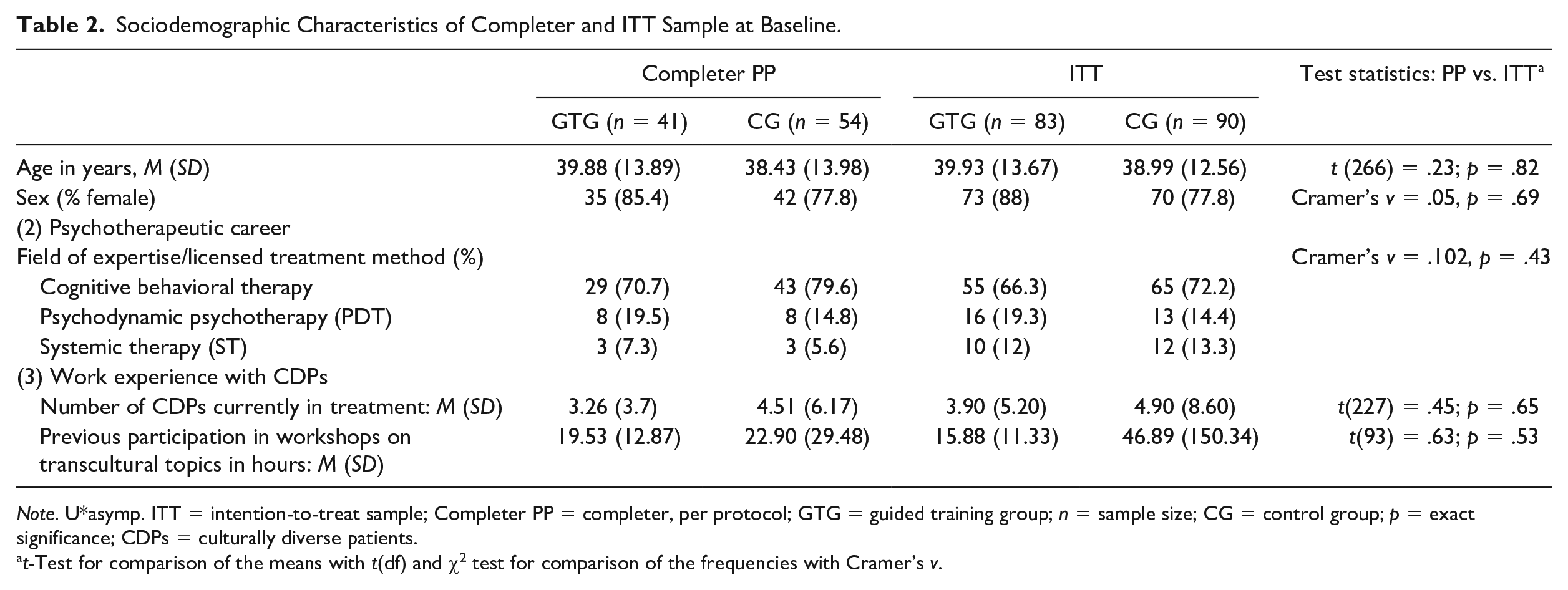
Note. U*asymp. ITT = intention-to-treat sample; Completer PP = completer, per protocol; GTG = guided training group; n = sample size; CG = control group; p = exact significance; CDPs = culturally diverse patients.
t-Test for comparison of the means with t(df) and χ2 test for comparison of the frequencies with Cramer’s v.
Main Analysis: Transcultural Competence
Group Comparison of Transcultural Competence: ITT Analysis Findings
To approach H1, we used a hierarchical linear regression analysis of the ITT sample to test improvements in transcultural competence from pre-training, post-training, and 3-month follow-up and differences between the two groups (Table 3). Awareness and engagement improved significantly from pre-training and follow-up (awareness: b = −0.33, p < .001; engagement: b = −0.26, p < .05), but did not differ between groups for the ITT sample (awareness: b = 0.12, p = .26; engagement: b = −0.02, p = .85). Neither a main effect of time nor a cross-level interaction effect of group and time was found in transcultural challenges (ps > .05; Table 4). Overall, both groups improved in awareness and engagement after the training period. However, no group differences were found. For challenges, neither an improvement in handling challenges after the training nor a group effect was confirmed.
Means and Standard Deviations of the ITT.
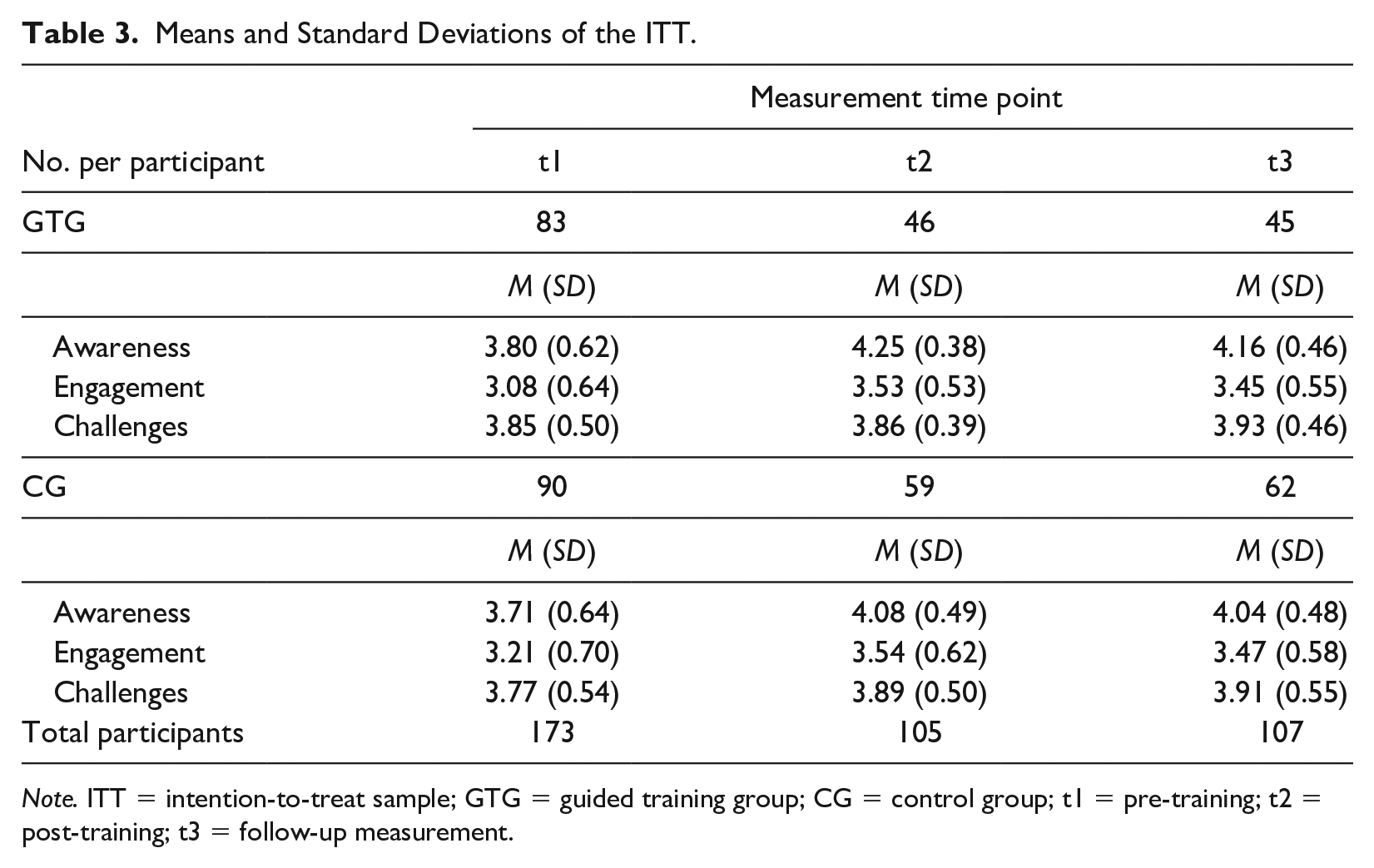
Note. ITT = intention-to-treat sample; GTG = guided training group; CG = control group; t1 = pre-training; t2 = post-training; t3 = follow-up measurement.
Hierarchical Linear Model Analyses (Estimation of Fixed Effects).
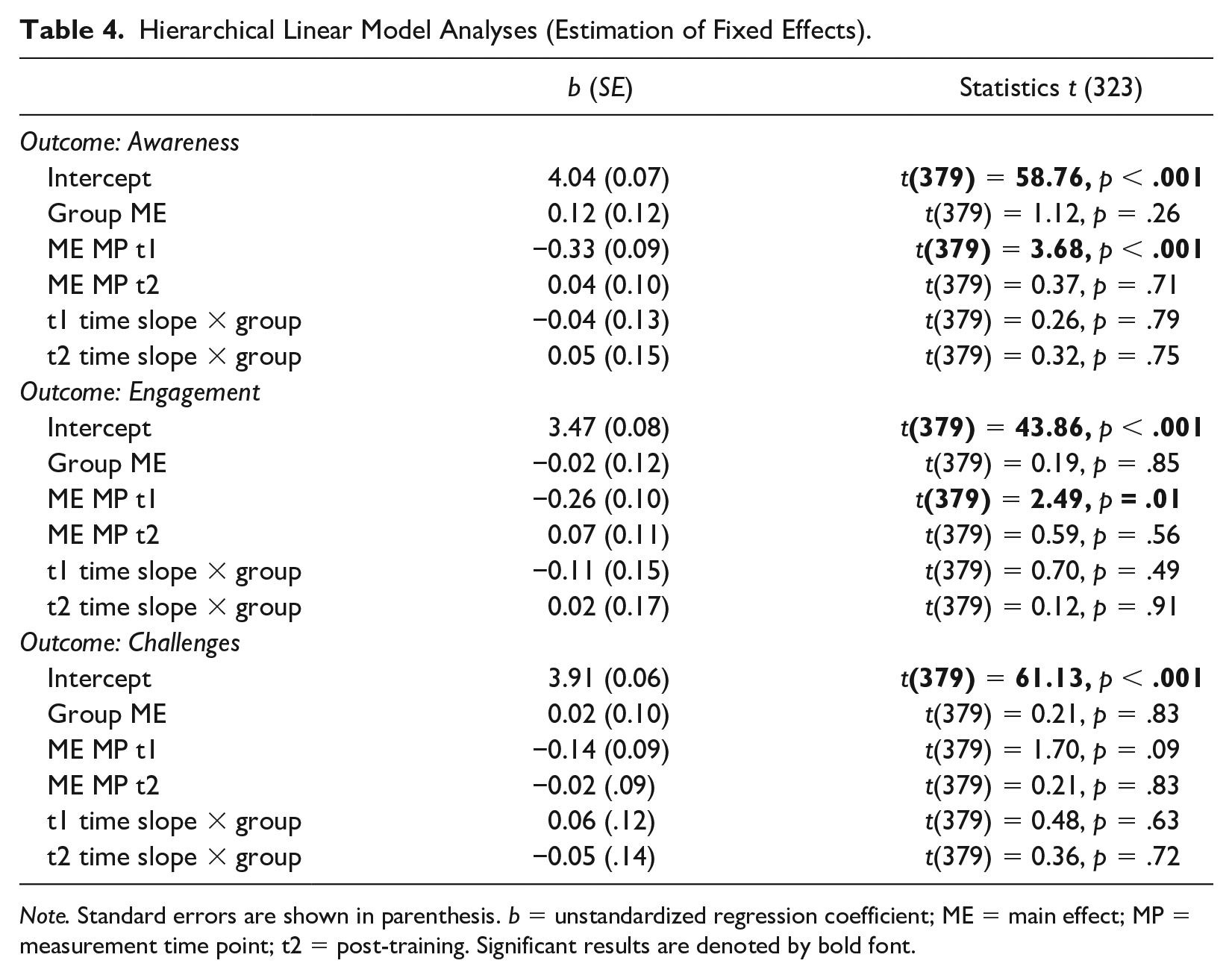
Note. Standard errors are shown in parenthesis. b = unstandardized regression coefficient; ME = main effect; MP = measurement time point; t2 = post-training. Significant results are denoted by bold font.
Group Comparison of Transcultural Competence: Per Protocol Analysis Findings
For the completer sample, the repeated-measures MANOVA (time: before, after, 3-month follow-up) also showed (just like the ITT) that the groups did not differ in any of the variables over time (ps > .05). Other than the ITT analysis, the MANOVA showed significant main effects in awareness and engagement from pre-training to post-training, awareness t1 vs. t2: F(1,93) = 61.694, p < .01, ηp2 = .399; engagement t1 vs. t2: F(1,93) = 47.786, p < .01, ηp2 = .339. As with the ITT sample, there was a significant multivariate effect of time for awareness and engagement from pre-training to follow-up, awareness t1 vs. t3: F(1,93) = 42.829, p < .01, ηp2 = .315; engagement t1 vs. t3: F(1,93) = 36.654, p < .01, ηp2 = .283. The ITT and completer analyses did not differ in the transcultural challenges factor, in which we found no significant time or time × group effects in both analyses. In summary, training effects did not differ between the GTG and CG in the ITT and the completer sample; thus, H1 was rejected.
Secondary Outcomes: Training Satisfaction
Weekly Module Ratings and Knowledge Assessment
Modules were evaluated as comprehensible (M = 4.46; SD = .63) and helpful (M = 3.93; SD = .92) in both groups. Overall module satisfaction was M = 3.99; SD = .88 (all participants for all modules: N = 464, ratings increase from 1 to 5). The groups did not differ significantly in their weekly module ratings, with the exception of Module 4, which the GTG (M = 4.48; SD = .73) found significantly more helpful than the CG (M = 3.95; SD = .93), partly confirming H2, t(64) = 2.35; p = .02.
Training Satisfaction at Post-Training (t2) and Follow-Up (t3)
Training satisfaction at post-training (t2) in both groups was measured with three factors (implementation of content, trained competence, and scope). Participants in both groups commented that the training had a clear structure. The groups differed significantly in the assessment of the scope of the training, which was perceived as significantly more manageable in the 6-week time frame by the CG, M = 3.66; SD = .85; scope scale: t(99) = 2.34; p = .02, compared to the GTG (M = 3.27; SD = .83). The GTG found the training significantly more useful to train individual competence, noting that it reduced insecurities and further increased openness in dealing with CDPs and confidence in treating them as patients; trained competence scale—GTG: M = 3.99; SD = .74; CG: M = 3.51; SD = .99; t(99) = 2.76; p < .01. They also indicated that the training provided a good overview and structure to stimulate further interest in the topic more than the CG, confirming H3; implementation of content scale—GTG: M = 4.27; SD = .59; CG: M = 3.52; SD = .89; t(96.16) = 5.07; p < .001.
The qualitative examination of open follow-up questions further corroborates the quantitative results. In the CG, some participants mentioned that the theoretical aspects covered in the training were insightful and expanded their understanding of transcultural psychotherapy. However, they expressed a desire for practical examples—they found the learning content too abstract. In the GTG, 37 participants actively engaged in the online chat feature during the training. They reported that the opportunity to receive guidance from a professional e-trainer clarified their doubts and deepened their understanding of the content. Participants in the GTG expressed enthusiasm for the engaging case studies and practical exercises, stating that they helped them understand and apply transcultural concepts in real-life scenarios. While the GTG appreciated the engaging training elements, they also highlighted that the time frame, especially owing to COVID-19 interruptions, was too short.
Discussion
The present RCT evaluated the effects of internet-based training on transcultural competence. Although transcultural awareness and engagement were significantly improved at post-training and follow-up, contrary to the hypotheses, no group differences were detected in ITT nor completer analyses. Handling transcultural challenges did not improve significantly over the course of the training in either group.
Our results on awareness and engagement coincide with previous findings, which also demonstrated a positive effect of training on cultural awareness (e.g., Costa & Dewaele, 2018; von Lersner et al., 2019). Improving awareness and engagement is key, as these are core competencies in CDP treatment (Benuto et al., 2018; Heim & Kohrt, 2019). Owiti et al. (2014) reported a correlation between transcultural competence, improved therapist engagement, and ultimately higher patient satisfaction. Transcultural competence training can mitigate mental health inequalities by raising awareness of treatment and engagement.
The lack of reduction in transcultural challenges after training in either group may be attributed to participants’ development of cultural humility. Cultural humility involves therapists adopting a humble and respectful attitude toward the cultural backgrounds of their patients (Hook et al., 2013), recognizing and acknowledging the limitations of their own knowledge, and understanding diverse cultures (Zhu et al., 2021). The various topics addressed in the training may have increased participants’ awareness of the challenges they encountered in their work with patients without immediately changing their actual handling in practice. Consequently, they may realize that gaining complete mastery of every cultural nuance is impossible. This realization can lead to a sense of humility toward learning from their patients in a collaborative process. Cultural humility may manifest as an acceptance of the challenges that arise when working with CDPs (Chu et al., 2022). Rather than attempting to eliminate these challenges, practitioners may view them as opportunities for growth and learning. However, their actual handling may only become apparent when behavioral measures are collected over a longer period; that is, when practitioners encounter challenges in practice and can then apply transcultural competence (Carballeira Carrera et al., 2020).
Since both groups had comparable levels of transcultural competence prior to the training, a balanced comparison was possible. Interestingly, all participants demonstrated an increase in transcultural awareness and engagement following the training, regardless of whether they participated in the guided training with exercises, knowledge tests, and feedback or educational text-based training without additional practical exercises. This suggests that all participants perceived some level of benefit from the training, regardless of their group affiliation. The self-report nature of the questionnaires may have contributed to participants’ belief in their training benefits and improved awareness and engagement, potentially explaining the absence of between-group differences in OnTracc scores. Compared to other competence training, guided training tends to be more effective (Seewer et al., 2022). Since participants were already experienced in transcultural treatment (e.g., workshop experience, culturally specific supervision, and some even had CDPs in treatment), the CG may not have needed guidance to enhance their competence and were motivated enough to work through the text-based training on their own.
Training satisfaction differed significantly between the groups. Secondary findings indicated that the GTG, which offered a more interactive approach, received more positive evaluations in both quantitative and qualitative data than the CG. As hypothesized, the GTG rated the training’s concept and content as more interesting. They also rated the integration of tools (e.g., videos and case examples) and the overall technical implementation better than the CG. In line with this research, interactive training can be more engaging and enjoyable for learners than theoretical training because it involves active participation and hands-on learning experiences (Fidan, 2023). In addition, active guidance may help participants strengthen their newly acquired knowledge in dealing with uncertainties in transcultural therapy (Guzder & Rousseau, 2013). Interestingly, at post-training and follow-up, the GTG reported a higher feeling of competence in dealing with CDPs and reduced feelings of insecurity compared with the CG. One potential explanation is that the interactive training approach offered participants greater opportunities for hands-on practice and experiential learning, enabling them to directly confront real-world challenges and develop self-assurance in their capabilities. The personalized nature of the GTG’s training facilitated feedback and coaching from experienced practitioners, assisting participants in identifying and addressing specific areas for improvement, reducing their insecurities.
Strengths and Limitations
In view of the lack of previous studies in this field (for a review, see Bhui et al., 2007), our pilot RCT provides important information. The sample, which represented psychiatrists and psychotherapists from diverse competence fields, was comparably large and, unlike many other studies, was randomly assigned and blinded to minimize bias (e.g., Venkataramu et al., 2021). We opted for a superiority design that employed theoretical, non-guided training as the active control condition. The 3-month follow-up gives the first insight into the practitioners’ actual application of the knowledge gained in their practical work with CDPs. The utilization of behavioral outcomes warrants increased frequency in empirical research on cultural training because they may provide objective measures of the effectiveness of the training (von Lersner et al., 2019). Follow-up measures can help establish the practical relevance of cultural training sustained over time, identify areas in participants’ transcultural competence that were not addressed in the initial training, and provide directions for further training (Benuto et al., 2018).
The training’s clear framework for improving sustained transcultural awareness and effective engagement (von Lersner & Kizilhan, 2017) aligns with the updated guidelines for multicultural competence (Ratts et al., 2016). The contemporary understanding emphasizes the interactive and dynamic nature of developing transcultural competence, which is a critical aspect of our training (e.g., by incorporating elements such as professional development, self-reflection, and critical analysis within the training modules).
The training content and design were developed from scratch with a team of researchers and practitioners in the field, and a dedicated website with a project logo was created for its implementation. By adopting an online approach, we established a cost-effective means of providing remote training in clinical education, as advocated by Vega (2005). In addition, our training provided regular feedback to participants regarding their learning process, which Vega (2005) recommended for successful training. The modules and case examples are carefully designed to challenge therapists’ assumptions, beliefs, and biases, fostering a deeper understanding of cultural humility as described by Hook et al. (2013) and Zhu et al. (2021). By emphasizing these principles in the context of psychotherapist training, our program contributes valuable insights to the development of cultural humility in therapeutic practice. Transcultural competence was assessed using the OnTracc questionnaire, which includes items that inherently capture humility in engagement and awareness. These scales encourage practitioners to approach their patients with a humble and open mind-set.
By combining quantitative data (e.g., questionnaire scores) with qualitative data (e.g., open-ended responses), we comprehensively explored participants’ experiences and perceptions of the training’s impact. No existing studies have reported participants’ satisfaction with training, which serves as a useful supplemental resource to evaluate and further refine training (Bhui et al., 2007).
Despite these strengths, this study had some limitations. The effects of the training were mainly operationalized with the construct of transcultural competence. However, there is still no formal consensus on how to define, implement, and distinguish this broad construct from general competencies (for reviews, see Stubbe, 2020; Vega, 2005; Venkataramu et al., 2021). Accordingly, this study is limited to the use of tools and benchmark measures to establish training evaluation standards in the early stages of development (Benuto et al., 2018). Hence, continued dialogue and reflection on how best to promote cultural understanding in increasingly diverse clinical practice are necessary.
The strict time frame made it challenging for participants to work through all modules and complete the interactive tasks, leading some participants to drop out at short notice. Thus, they did not complete all modules by the time of the post-assessment. The decreased participation in the GTG compared to the CG could be attributed to the increased time involvement required in the GTG for engaging in interactive elements, participating in online feedback sessions, and completing practical exercises. This might have caused some participants to find it challenging to navigate their other responsibilities. As with many internet-based intervention studies (Mak et al., 2018), the dropout rate (32.37% during training/5.78% after 3 months) was rather high in this study, which does raise concerns about the feasibility of this training approach in real-world settings. While the interactive nature of the GTG can offer significant benefits by enhancing training satisfaction and learning outcomes, it might also place greater demands on participants’ time and resources.
It might be helpful to consider ways to optimize the training’s feasibility without compromising its interactive and practical elements. To discover the possible reasons for dropout at the content level, we followed the recommendation of Kulik and Roberson (2008) and evaluated individual training modules to suggest changes for future applications of the training (e.g., modifying lower-rated modules [M1, M2] or content-challenging knowledge assessment [M6], offering the flexibility to choose learning modules or exercises based on participants’ individual interests and needs, or omitting content for time-strapped clinical settings). In the qualitative analysis, most participants found the content to be new and helpful. However, some CG participants mentioned prior familiarity with certain content. Interestingly, similar results were found in the GTG’s quiz results, particularly regarding M3 (prejudices and discrimination), which was perceived as comparatively less helpful, indicating a need for adaptation that moves beyond well-known theory concepts (e.g., promoting peer interaction in establishing online forums for psychotherapists to exchange experiences, insights, and challenges regarding stereotypes and discrimination; and including interviews with patients who have experienced its impact in therapy). To enhance participants’ training adherence, we could offer flexible scheduling options, provide support for time management, and set achievable goals at the outset. Creating a sense of community and fostering social interactions in discussion forums to share resources can keep participants motivated and maintain engagement throughout the training and beyond.
Given our reliance on self-reported measures, the results could be inaccurate and biased. The internal consistency of the self-administered OnTracc scales was acceptable. However, the training effect might solely be a retest effect of the OnTracc. We addressed these limitations through a mixed-methods evaluation with weekly knowledge assessments and module and training satisfaction ratings at post-training and follow-up, allowing for secondary analysis to shed light on quantitative data (Supplemental Appendix Table B).
Practical Implications for Further Research, Practice, and Implementation
The challenge of evaluating the impact of transcultural competence training based on self-reports is indicative of the need for innovative methods for evaluating cultural competence learning models (Gozu et al., 2007). Perceived barriers might manifest at a behavioral level (von Lersner et al., 2019), and the question of the transfer of transcultural competence between online training and actual therapeutic practice remains open. Rather than relying strictly on self-reports, observations of the psychotherapists’ actual behavior (e.g., via video recordings of therapy sessions) may provide more meaningful and objective data, distinct from performance measures (Bhui et al., 2007; von Lersner et al., 2019). As von Lersner et al. (2019) suggested, seeking evaluation in direct interactions with patients and measuring patient outcomes could provide valuable insights into the real-world impact of the training. The study results emphasize integrating practical and interactive elements into training. Participants’ qualitative feedback guides future iterations, tailoring an impactful and enriching learning experience for participants. We hope to contribute to the repository of best practices and the development of (remote) training approaches that are easy and convenient to complete to strengthen scientifically based transcultural training in mental health care. The compact scientific training content could be translated into other languages or adapted and evaluated for other (health) professions. Transcultural competence should be implemented as an integral element of advanced clinical training among mental health care staff (Mattar et al., 2023) to support culturally sensitive psychotherapy that improves mental health care for CDPs.
Conclusion
This study evaluated internet-based training to improve transcultural competence for psychotherapists in Germany. Both guided practical training and non-guided training enabled practitioners to become more culturally aware, reflect on their biases toward different belief systems, and engage with CDPs. The integration of practical and interactive elements effectively met participants’ needs and expectations, elevating the training experience. Future studies should continue to evaluate the training in RCT studies, including extended follow-ups with a focus on behavioral measures.
Supplemental Material
sj-docx-1-jcc-10.1177_00220221231221095 – Supplemental material for Effectiveness of Internet-Based Training on Psychotherapists’ Transcultural Competence: A Randomized Controlled Trial
Supplemental material, sj-docx-1-jcc-10.1177_00220221231221095 for Effectiveness of Internet-Based Training on Psychotherapists’ Transcultural Competence: A Randomized Controlled Trial by Marie-Christin Atzor, Gerhard Andersson, Ulrike von Lersner and Cornelia Weise in Journal of Cross-Cultural Psychology
Footnotes
Acknowledgements
The authors thank the participating psychotherapists for their motivation and perseverance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is partly funded by a grant from the Outpatient Clinic for Psychotherapy, Marburg, Germany.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.