
Abstract
Although there is some literature analysing the factors impacting upon migrant and resettled African communities in Australia, there is limited evidence reporting on African-Australian people’s experiences of what promotes or obstructs good health. This article examines the promoters and barriers to good health identified by an African-Australian community in South-Eastern Melbourne as a key element to co-designing a sports-based youth development program, the Junior Black Rhinos Basketball Program. Data from 10 interviews with 14 African-Australian community members was thematically analysed. The participants identified personal, interpersonal, and structural promoters and barriers to experiencing good mental and physical health. Barriers to good health were reported as (a) resettlement, (b) generational differences in understanding mental health, and (c) racism and discrimination. Promoters of good health were reported as (a) sport and other group-based activities, (b) spending time outdoors, (c) employment and education, and (d) community connection. In designing the program, participants proposed the program could counteract these barriers through the inclusion of (a) mental health education; (b) life skills development; and (c) promoting safety, inclusion, and African community values. It is important to design health interventions with the community the program aims to serve that may result in the valorisation of community knowledge, values, and experience and decentre western assumptions about what constitutes good health.
Keywords
Introduction
This article draws on qualitative interviews with members of the African-Australian community in South-Eastern Melbourne, Australia, that focus on the social and structural factors that shape experiences of health and well-being within their community. These interviews were part of a broader co-design process for developing an expanded version of the Black Rhinos Basketball Program, a crime prevention and social inclusion sports program for young men involved in the justice system. The ‘Junior’ Black Rhinos project is the result of a collaboration between Afri-Aus Care, a community-based organisation supporting the health and well-being of people and families who have resettled in Australia from African countries, and researchers at RMIT University.
Co-design is an iterative process that brings together the expertise of multiple stakeholders with experiences of a problem, to create innovative solutions (Sanders & Stappers, 2012). In the co-design phase reported here, we sought to understand what community members identified as the social and structural barriers that undermined individual and community experiences of health, including those factors that are central to good health and well-being. Building on an analysis of the factors that shaped their experience of health, participants then articulated what the program should look like, feel like, and include, to best support the health and well-being of younger participants aged 8 to 14.
The purpose of this article is to report on these objectives and by doing so, contribute to the paucity of literature examining African-Australian well-being, and explore factors that contribute to a culturally responsive and community-based health intervention for African-Australian communities.
Review of Relevant Factors Promoting and Restricting Good Health and Well-being
Barriers to Good Health
For many African people resettling in Australia, particularly because of forced migration, experiences of belonging are a key determinant of health (Silove et al., 2017). Some young people and their families who were displaced from their home countries face significant and enduring barriers to physical and mental health before arriving in Australia, including the loss of community supports, friends, family, inadequate resources, trauma, and interrupted psychosocial development, education, and belonging (Silove et al., 2017). A large body of Australian research illustrates how upon migration, institutional and everyday experiences of racism and othering continue to disrupt belonging for African-Australian people (Ikafa et al., 2022; Majavu, 2018; Mude & Mwanri, 2020; Shepherd et al., 2022; Udah & Singh, 2019; Uptin, 2021). Racism contributes to perceptions of non-acceptance within Australian society, a major factor that shapes the mental health of young African-Australian people (Uptin, 2021). The experience of Othering is reinforced by the construct of Australia as a ‘White space’ (Uptin, 2021), with Udah and Singh (2019, pp. 852–853) highlighting how participants in their research ‘found themselves categorized and positioned within the racialized discourses of blackness as deficit’. Young African-Australian people report feeling compelled to ‘integrate’ into the dominant (White) Australian society and culture, yet constant overt and subtle reminders of their ‘visible difference’ lead some to conclude that ‘they can never belong here’ (Uptin, 2021, p. 89).
Racism and discrimination, in education, employment, and the media are recognised in the experience of belonging for African-Australian people and communities (Abur & Mphande, 2020; Correa-Velez et al., 2010, 2017; Edgeworth, 2015; Miller et al., 2022). Young African-Australian people in primary and secondary schools experience racism from their peers, school staff, and the broader school communities (Abur & Mphande, 2020; Edgeworth, 2015; Miller et al., 2022). For young people resettling in a new country, these experiences can significantly impact academic performance and engagement (Correa-Velez et al., 2010, 2017). For example, Miller et al. (2022) found that teaching staff expected students to assimilate within the school environment, while Edgeworth (2015) highlight how Sudanese students in urban and regional schools were treated as outsiders and subject to discrimination by their student peers. Ziersch et al. (2023) and Young (2020) found that these experiences of discrimination and racism were also felt by adult African-Australian people in securing employment and within the workforce.
Negative media discourses around young African-Australian men reproduce experiences of racism and non-belonging (Majavu, 2018; Shepherd et al., 2022; Uptin, 2021; Young, 2020). Political and media narratives have conceptualised young African-Australians as a homogenous group who share problematic characteristics (Majavu, 2020; Uptin, 2021; Young, 2020). Such stereotyping criminalises young African-Australian people, resulting in over-policing, surveillance, and suspicion of this population (Hopkins, 2020; Majavu, 2020; Uptin, 2021).
Impacts of Resettlement
Resettlement is associated with belonging experiences that are impacted by loss of connection to places, family and social ties, and disruption to cultural connections which were significant in peoples’ home countries (Mude & Mwanri, 2020; Nunn et al., 2022). For many young people, the resettlement process can impact self-perception and social identity, leading to a feeling of being torn between two places and cultures (Mude & Mwanri, 2020). These cultural challenges also manifest in relation to family structure and broader community connection in societies such as Australia, which are seen as more individualised in nature (Abur & Mphande, 2020). Young people may demonstrate greater adaptability to the new culture compared with adult family members, while simultaneously experiencing increased responsibilities to support older family members to understand and adapt to the new social and cultural environments (Correa-Velez et al., 2010). Greater levels of independence are subsequently sought by young people, creating a clash with the expectations and cultural values of family members (Correa-Velez et al., 2010; Mooren et al., 2020). Further challenges are created by support programs geared towards the needs of children and young people, which are designed and implemented without seeking input from parents (Abur & Mphande, 2020, p. 416; Halliday et al., 2014). These experiences can undermine parents’ sense of responsibility and respect towards them within the family (Abur & Mphande, 2020; Halliday et al., 2014; Mooren et al., 2020).
This research contextualises how people resettling in Australia, from African countries and cultures, are impacted by structural inequalities that shape economic inclusion and access to health care and housing (Fozdar, 2023; Mude & Mwanri, 2020; Ziersch et al., 2023). For instance, access to healthcare in Australia is impacted by language barriers, and often through limited cultural competency and understanding by organisations and staff delivering healthcare services (Fauk et al., 2022; Fozdar, 2023; McCann et al., 2016). Access to mental healthcare is further shaped by limited knowledge and understanding of mental health within African-Australian communities (Abur & Mphande, 2020; Fauk et al., 2022). Difficulties accessing healthcare compound barriers that undermine help seeking behaviour, such as a fear of stigma associated with mental health within African-Australian communities, and the cost of healthcare (Abur & Mphande, 2020; McCann et al., 2016). In addition, the perception of healthcare providers and programs as exploitative of African-Australian communities are reinforced by a lack of partnership with community (Shepherd et al., 2022). As Fauk et al., (2022) suggest, accessibility of healthcare for African-Australian families can be supported through greater incorporation of African cultural and religious values in service provision.
Promoters of Good Health
Several articles highlight the value of social capital and social connection as social determinants of health, which facilitate belonging (Abur, 2016; Baak et al., 2020; Fozdar, 2023; Ikafa et al., 2022; Mwanri et al., 2023). Increased access to social resources is evident in the inclusion of African-Australian people in employment, which can contribute to a stronger sense of identity, improved income and access to resources, and a sense of contributing to society (Ziersch et al., 2023). For young African-Australian people, social capital and self-identity can be facilitated through sport, which can provide an entry point to other services and supports (Abur, 2016; Mude & Mwanri, 2020; Nunn et al., 2022). Social connection in sport is greatest in familiar environments, such as schools and within ethnic organisations (Baak et al., 2020). These environments can promote feelings of safety and security, which are not always evident in mainstream sporting organisations (Abur, 2016).
Increased safety and security are connected to the key values of African families living in Australia, which centre around community connection and ties, and the significance of connecting families with community networks (Gatwiri & Anderson, 2021; Halliday et al., 2014; Ikafa et al., 2022; Mude & Mwanri, 2020). Having access to others for support and being connected to community is a contributing factor to better experiences of health (Babatunde-Sowole et al., 2020). As Mude and Mwanri (2020) suggest, finding others and acceptance within the community is central to the conditions for a felt sense of safety, connection, and well-being.
According to research with African-Australian communities, help seeking is also strengthened by connection to community support systems and feeling able to be open with others (Halliday et al., 2014; McCann et al., 2016). However, the conceptualisation and delivery of organisational support is also critical. Fundamentally, researchers suggest that programs focusing on health and well-being would better support young people’s outcomes if they were developed through family and community-based approaches and reflected their larger socio-ecological and geographical environment, instead of focusing on one section of the community and their needs (Correa-Velez et al., 2017; Frounfelker et al., 2020; Halliday et al., 2014; Mooren et al., 2020). In addition, help seeking and access to healthcare, as well as the effectiveness of services, are facilitated by programs that are culturally responsive and culturally sensitive (Halliday et al., 2014; McCann et al., 2016; Mude & Mwanri, 2020; Renzaho et al., 2011). The benefits of offering culturally responsive services are further supported by employment of culturally diverse staff, in places such as schools (Baak et al., 2020; Miller et al., 2022). In addition, greater health literacy through education and attempting to counteract stigma associated with mental ill health, is central to supporting good health (McCann et al., 2016).
Finally, the literature speaks to the importance of listening to communities and providing opportunities for African-Australian people to share their stories, as part of a strengths-based approach to valuing and recognising the experiences and knowledge, values, and needs of the community (Babatunde-Sowole et al., 2020; Fozdar, 2023; Gatwiri & Anderson, 2021; Uptin, 2021).
Current Study
Research with African-Australian people examines the negative health impacts of forced migration, racism, and discrimination (Shepherd et al., 2022; Udah & Singh, 2019; Uptin, 2021), resettlement experiences within contexts such as schools and education, workplaces and employment, housing, and engagement with government and community services (Shephard et al., 2022; Silove et al., 2017; Uptin, 2021), and the value of social and cultural connection and belonging to promote good physical and mental health (Gatwiri & Anderson, 2021; Uptin, 2021; Ziersch et al., 2023). However, few studies centre on the lived experiences of Melbourne-based African-Australian communities regarding the determinants of health, nor what components of a community program might promote good physical and mental health.
In this context, we sought to answer two research questions: (a) What does health and well-being mean to African-Australian community members in South-Eastern Melbourne? and (b) How might a new basketball program that promotes good health and well-being be effective for African-Australian young people, their families, and their community? Our objective for understanding these concepts was twofold: firstly, to embed the community perspectives, experiences, and aspirations into the program design. Secondly, to determine those factors underpinning a culturally responsive and fit-for-purpose program that would address community identified barriers to good health and well-being.
Method
Background
The Black Rhinos Basketball Program is a crime prevention sports program, established in 2016 and hosted by Afri-Aus Care. The program focuses on primary intervention for young males aged 18 to 30 involved in the justice system by providing a site for positive social interaction, physical exercise, teamwork, and inclusion. The program also offers psychosocial support including counselling, referral, intake, and assessment to culturally appropriate services, and legal advice and education. Reflecting the predominantly African-Australian population participating in the program and accessing Afri-Aus Care services, the African philosophy Ubuntu underpins the program. Ubuntu relates to humanness and relationality, described by Winschiers-Theophilus et al. (2012, p. 91) as ‘a person is a person through other people’ and through the values of trustworthiness, generosity, reciprocity, and participation. Ubuntu is reflected in the program by supporting at-risk participants to connect with culturally responsive services, promoting their involvement in the broader community, and through pro-social skills and leadership development.
The current study relates to the co-design of the Junior Black Rhinos Basketball Program for a younger age-group, delivered in two schools and one community-based setting in South-Eastern Melbourne. The Junior Rhinos focuses on enhancing health and well-being outcomes for 8- to 14-year-olds through building resilience, social and community connection, positive social skills and enhancing young people’s education through mentoring, in-class support, tutoring, and strengthening the connections between families and the school environment. The Junior Rhinos program therefore aims to mediate potential negative impacts associated with resettlement, discrimination, and exclusion (Abur & Mphande, 2020; Shepherd et al., 2022) from a younger age.
Research Design
Community-based co-design (CBCD) was chosen to design the program because it utilises the iterative, creative, and collaborative processes of co-design (Sanders & Stappers, 2012), as well as the values and norms of the community, who are viewed as active contributors and partners in the research (Till et al., 2022). Embedding the Ubuntu philosophy into the research design ensured the dominance of African-Australian cultural values and norms and provided a framework to allow the collective experiences and knowledge of community members to inform how the sports program might benefit a younger age-group. The first three phases for co-design (define, discover, and define) recommended by global design and innovation company IDEO.org (2015) informed the research design. The methods employed throughout each phase are reported elsewhere (Goff et al., 2024). The themes reported in this article are drawn from qualitative interviews conducted during the ‘discover’ phase, which facilitated a deep exploration of community values, views, and experiences and their relationship to the participants’ desired outcomes for the program.
Participants
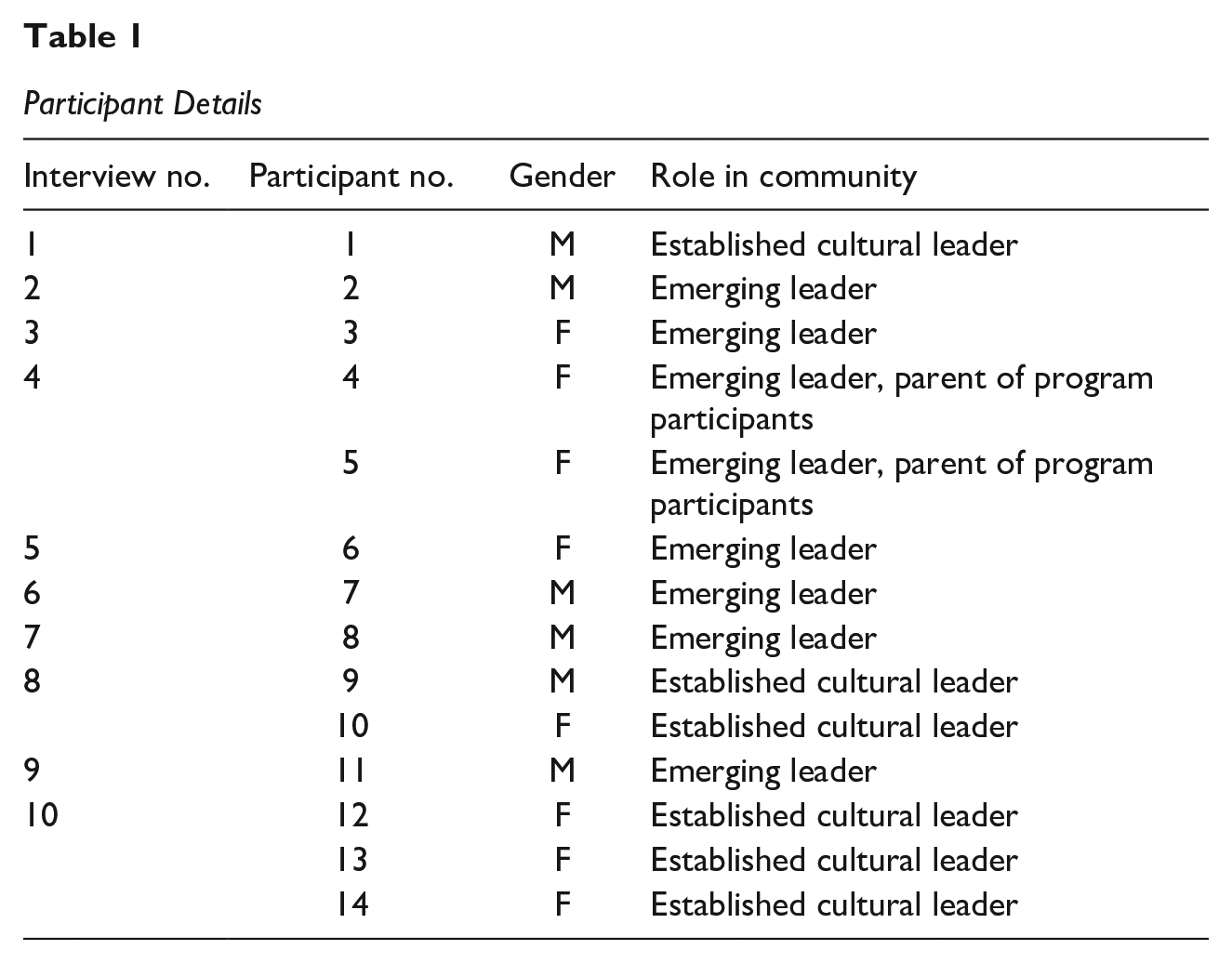
Seventeen participants were involved in the wider co-design project and 14 elected to participate in interviews that explored African-Australian community member’s practice of Ubuntu, experiences of community, health and well-being, and the desired impact of the new program. Participants were purposively sampled by the project manager, with the inclusion criteria encompassing: >18 years old, currently involved in the existing Black Rhinos program or Afri-Aus Care and identified by the project manager as demonstrating emerging or established community leadership, including older community members with cultural knowledge and authority. Including a diversity of perspectives in the design process was essential to develop the program ideas and values, and the practical considerations of what the program should aim to achieve for young participants and their community networks. There were eight female and six male participants, aged between 60 and 21. Eight were older than 35 and 6 were in their 20s and early 30s. All participants were of African descent, migrating from east African countries including Somalia, Ethiopia, South Sudan, and Zimbabwe, as well as the West African country of Senegal. All participants were broadly familiar with Ubuntu in relation to their native language or specific cultural practices. All participants provided their verbal and written informed consent to take part in the research, including audio-recording of their interviews (Table 1).
Participant Details
Interviews
Authors 1, 2, and 6 conducted semi-structured interviews between October and December of 2022 and lasting between 60 and 90 min. Ten interviews were conducted, as participants were given the choice for individual or small group interviews to enhance their comfort and control. Seven of these were individual interviews and three were group interviews with either two or three participants. The researchers gave participants the option of using a card sort, a common co-design method where the researcher prompts participants to share a narrative response related to a word or image on a card (Mannay, 2013). Prompts were based on the question ‘What does health and well-being mean to you?’ Participants were asked to prioritise and discuss selected cards that represented their understanding and experience of health (Supplemental Material 1). These words were derived from existing health-focused literature with African communities or culture (Abur & Mphande, 2020; Mabasa, 2020) and previously agreed to by participants (Goff et al., 2024).
To identify those social and structural factors that promote health and well-being for young participants in the new program, another card sort was utilised, with words drawn from impact measures identified by Cunningham et al. (2020) within sports-based youth development programs. These cards (Supplemental Material 2) were previously co-developed with participants (Goff et al., 2024). Prompts related to the question ‘How might the new program promote good health and well-being for young people and their families?’
Two of the 14 participants opted to forego the card sort and provide narrative responses to the questions, where they shared their understanding of health, what being healthy means to them, and what supports or restricts good health. Prior discussions with participants (Goff et al., 2024) highlighted that having an alternate option was important to their sense of control over the interview process. Because a card sort prompts narrative responses, there were no noticeable differences in the interview content.
Researcher Positionality
The authors are comprised of a mix of university researchers and a member of Afri-Aus Care who share varied cultural identities, research interests, and expertise. The authorship team (except author 5) are Social Work academics who were invited to partner on this project by Afri-Aus Care leadership based on their long-standing social work field education collaboration. This relationship was vital for enabling ongoing trust and dialogue between the organisation, community participants, and the authors. The university researchers share practices in participatory and community-centred methodologies in phenomena including community health, organisational partnerships, lived experience research, social inclusion, sport, and young people from priority populations. Authors 1, 2, 3, 4, and 7 are White, and our practice of cultural humility (Goff et al., 2024) promoted reflexivity, with project meetings, participant engagement and research design being led by team members with cultural expertise and cultural authority. In this context, authors 5 and 6 held this cultural expertise through their African-Australian identities and connection to the community context. Author 5 is the Afri-Aus Care project manager and attended researcher meetings to ensure cultural and organisational suitability.
Connected to the authors’ cultural identities and ethical, organisational, and disciplinary commitment to challenge structural oppression, we believe in the importance of decentring western ways by highlighting the lived experiences and future aspirations of the African-Australian community who engaged in this research. Therefore, all authors engaged in discussions about how to practice Ubuntu principles including cultural humility, curiosity, collaboration, respect, partnership, and reciprocity throughout the project (Goff et al., 2024). Critically reflecting on these values, choices, and actions helped to examine our influence over the research (Braun et al., 2019; Levitt et al., 2018) and make transparent our cultural standpoints. For example, the researchers were guided by CBCD (Till et al., 2022), reflexive thematic analysis (Braun et al., 2019), and Ubuntu principles practiced by the Afri-Aus Care community by engaging in discussions with each other throughout all stages of the research. This included challenging biases and assumptions so to accurately capture and represent the views and experiences of participants. Authors 1 and 2 prepared this manuscript, and all other authors provided feedback and contributed to the drafting process. Authors 5 and 6 were instrumental in providing feedback and clarification to the broader research team during the research related to cultural experiences of resettlement, age, gender, and race.
Analysis
The researchers utilised reflexive thematic analysis (Braun & Clarke, 2012; Braun et al., 2019) to interpret and generate patterns in the qualitative data and to foreground participants’ views and experiences. Prior to analysis, all interviews were transcribed by authors 1, 2, and 6. At this stage, participants were offered the opportunity to review their transcript to confirm the credibility of the information, however none elected to do so. Identifying features were then removed to maintain anonymity and confidentiality. In phase 1, the transcripts were divided between university researchers, with at least two researchers reading each transcript to familiarise themselves with the data. Then, the researchers met to discuss the transcripts, and their assumptions related to their values, identities, or subject expertise (Braun et al., 2019). In phase 2, the team assessed their allocated transcripts through deductive reasoning (Braun & Clarke, 2012). In a shared online document, similar terms and quotes were grouped together according to sensitising concepts relevant to the overall project aims (integration of Ubuntu, promoting health and well-being, developing community, and identifying program priorities). During phase 3, the university researchers and program manager met several times to review and label codes and identify deeper meanings in the data in relation to the cultural expertise provided by authors 5 and 6. During this process, the authors approached the data from a social constructivist viewpoint, identifying latent meanings as indicative of participants relationship to their social and cultural worlds. In phase 4, authors 1 and 2 met to revise the initial themes and determine themes for the data. In phase 5, the themes were shared, further refined, and endorsed by the participants to represent their experiences and worldviews more closely, and to inform subsequent program development and implementation. During phase 6, authors 1 and 2 selected participant quotes that reflected the themes to put into the manuscript, which was then reviewed and endorsed by the broader team.
Results
This section reports data that relates to three key themes (a) structural factors that contribute to negative experiences of health and well-being and non-belonging; (b) those factors that support experiences of good health; and (c) program priorities, activities, and goals to promote good health. Within these three themes, 10 sub-themes are reported. It is important to acknowledge that most participants described good health as relational and experienced through their involvement in physical and community related activities. Many participants did not differentiate between physical and mental health but saw these as complementary and mutually reinforcing.
Barriers to Good Mental and Physical Health
Participants identified individual and social barriers to experiencing health. These barriers included (a) resettlement, (b) generational differences in understanding mental health, and (c) racism and discrimination.
Resettlement, Culture Shock, and Intercultural Tensions
Prior to resettlement in Australia, migrant participants identified cultural practices that contributed to good health experiences, yet some experiences of migration and resettlement presented unique challenges and consequently impacted upon social and cultural connection, employment, physical health, and practice of culture. Participant 5 described their experience of culture shock: One of the biggest [challenges] was culture shock. Where I came from, we had someone to talk to. . . I was not educated that mostly you’re going to see white people. The social worker, wherever I looked, it was all white. It’s not that I don’t like white, but it was a little bit scary because almost for 11 years I had been seeing the same kind of people.
The cultural load associated with resettlement was also highlighted by Participant 3, who discussed the differences between collective and individualised cultures. They stated: On a simple level, any family has their own culture and that doesn’t always align with what is happening elsewhere. But there is also the family’s culture and then there is your heritage and how that influences your family’s culture. As a young child, you’re trying to navigate that.
However, for some older participants who maintained more traditional cultural practices within their families and homes, there was concern that western culture would interrupt their African identities and practices, which Participant 9 describes as making it ‘difficult to engage young people in an African way’.
The tensions associated with resettlement and navigating Australian norms and practices may lead to isolation, loneliness, and impact young people’s education. For example, Participant 11 reported language as a barrier to their education and ability to develop peer connection: I came here knowing literally no English at all and trying to navigate through that. I went to school, had teachers talking to you and other people talking to you and you couldn’t really understand. Because of that lack of communication, I felt like I wasn’t really being heard, and people couldn’t understand what I was trying to say. Because of that I ended up being reserved and stepped back and didn’t really talk as much and I didn’t involve myself in many things.
Therefore, navigating the tensions associated with learning new social and cultural norms, language and values may challenge social connection and belonging.
Generational Differences in Understanding Mental Ill Health
There were marked generational differences between those over 35 who were more likely to have experienced migration as an adult, and those under 35 who reported faster acculturation to the Australian context. Understanding mental health and willingness to access service support was most identified as a generational barrier to feeling healthy and well. These factors were also reported to impact upon interpersonal relationships within a family setting. Older participants with lived experience of resettlement noted that understanding the complexities of a Western health system was challenging. Participant 11 observed that for many older people who fled conflict, ‘I don’t think they view mental health as a big thing’ in comparison to previous conflict-related trauma. They noted ‘that lack of understanding is a grey area’.
Younger participants (<35) reported that such generational differences produced a disconnect with some older members of their families, whereas older community participants seemed to interpret behaviours indicating mental ill health (e.g. social withdrawal) as contributing factors to these relationship issues. This tension is again captured by Participant 11, who highlighted differences in knowledge systems and contemporary understandings of mental health: What I’ve noticed in a lot of the African communities is understanding mental health and just how they view it and what’s done about it. I guess that lack of knowledge of how to handle situations has been a big issue and may need to be looked at.
All participants agreed that mental health education was needed and a potential reason for lack of understanding between young people and their elders. Therefore, incorporating mental health literacy into the program may decrease family conflict and support participants’ mental health.
Racism and Discrimination
Almost all participants, regardless of age or place of birth, reported encounters of prejudice, judgement, discrimination, or racism. Three described instances of racism at school or work, and two reported incidents on public transport and on the street. These experiences were psychologically distressing and highlight the impacts of racism on mental health. For example, Participant 6 noted, ‘How are we making the world a better place if we can’t share two seats on a train together?’ Others said: There have been times when I have encountered racism and discrimination based on a personal prejudice from other people. For example, my colleagues. And it has been difficult. . . So, it’s not a personal thing. It’s just, unfortunately, there are some people in the world who do judge you and do have these underlying biases and act on them consciously. (P8) It happened to me so many times that I walk behind somebody, and they have their kids, and their kids are running around and doing things. But once they turn around and see there is a black man there, they freak out. They just run and grab the kid’s hand. (P1)
The media was reported by some participants to perpetuate negative constructs of young African people or refugees. Participant 3 expressed frustration that African people were portrayed as a homogenous group and synonymous to experiences of hardship and ‘needing help’: It becomes glamourized and it’s like ‘Oh, you made it against all adversity’. But not everyone has been through adversity. . .. We are multifaceted as a group of people because we have the same pride in being African. . . But when someone says, ‘all Africans’, it’s like no, ‘we are all different’. It’s about holding competing truths. Yes, we function as a community and together, but we are different. . . this is who we are.
These ‘competing truths’ were felt in other ways, including the racial discrimination that informs unconscious bias. Participant 8 perceived this bias as contributing to ‘automatically thinking that the kids aren’t doing the right thing if they are walking around. Calling them intimidating if they are in a large group of kids. You see large groups of White people walking around all the time’. Overall, these varied experiences of racism and discrimination led to perceived experiences of social exclusion and stigma.
Promoters of Mental and Physical Health
Alongside factors obstructing good health, sport and other group-based activities, nature, work, and education, and community connection were identified as promoters of mental and physical health and are presented as sub-themes below.
Sports and Other Group-Based Activities
Participants described a range of individual, interpersonal, and community promoters of good mental and physical health that were unique to their experiences and histories of resettlement. Engaging in team sports, such as soccer or basketball, was suggested to increase happiness amidst periods of poor health. Participants also felt that sport was pivotal to enhance resilience, reduce stress, consistency, connection, and belonging with other members of the team and the wider community. For example, Participant 2 said ‘It was good in terms of keeping me connected to people. African people and a strong community and kept me fit. If I wasn’t playing basketball. . .I wasn’t taking care of my physical health either’.
Other interpersonal activities were also reported to promote mental health. For example, cooking with others and sharing meals. Mental well-being was described by Participant 1: When you are lonely. . . activities will help out a lot. Like sport, or Ubuntu, the cooking programs and stuff like that. Those things help a lot. Even those African mothers when they are together cooking you see. . . that they are very happy.
Other participants reported group activities as a site of safety, community involvement, and confidence building.
Nature as a Facilitator of Health and Community Values
Participants suggested their physical and mental health was supported by spending time outside and connecting with others in nature. Gardening, growing food and ‘having my hands in the soil’ (P13) nourished their physical and spiritual health and promoted self-care. Participant 14 reiterated that spending time outdoors with others facilitated social connection and provided opportunities to share practical or emotional concerns that may be causing stress: When we go outside, if it is sunny. . . to get warm, we drink tea there, we talk, we watch the garden, it makes us happy. Also, it is part of our wellbeing. If someone has a problem, and you sit down there watching, nice, green things. It will clear out your mind.
The outdoors represented a site for participants to practice the reciprocity and mutual care evident within African cultural values and the Ubuntu philosophy.
Well-being Through Work and Education
There were varying experiences of education and employment within the participant group, particularly within different age groups. For some older participants <35 whose resettlement in Australia occurred after migration, finding work was aspirational and perceived as an activity that would reduce the financial stressors. Participant 10 highlighted the link between financial and physical well-being. For those older participants, whose acculturation to the Australian context differed, there were differing reports of employment as a mediator of empowerment, self-worth, and well-being. Participant 14 reports: A lot of the ladies now are working. They are showing wellbeing now because, before they were not working, they feel depressed. . . They got employed and they are getting payment, they are happy, this is the change in the community. . .If I got a job, I will feel powerful because I have job and money. But if not, I will feel low. And if your power is gone, then you are not healthy. All health and power is coming from the mind. When the mind is busy with good things you have power. When the mind is busy with bad things your power is down.
Among younger participants who were more likely to have grown up in Australia, similar feelings were associated with schooling and education experiences, particularly if they were positive. Participant 2 described a willingness to learn and engage in education to escape ‘messed up’ or challenging experiences that impacted their mental health.
Community Connection to Support Responses to Negative or Challenging Experiences
Community connection facilitated participants’ capacity to respond to negative or challenging experiences. For example, sharing problems with others was considered a way to share their burdens and embody Ubuntu. Participant 9, a community elder stated: Culturally if you have a problem. . . I call upon others to share my burden and they give the solutions. . . The more you share the more you give trust. . . and the more you get better and more you get energised and the more you get mental health. They share the burden from you, so because of the ‘we [are because] I am’, my problem is our problem.
Participant 7 described other mental health benefits resulting from social connection: If we are not socially connected, we tend to isolate ourselves, which then causes the problems that we then face. Mental health, depression, anxiety. If we are constantly with community, then we are able to think about others and not think about ourselves.
Most participants suggested that community and family connection enhanced positive mental well-being through creating a ‘sense of belonging’, ‘acceptance’, ‘talking with other people’ about their past, ‘laughing and joking’, and reminiscing about memories from their past. Together, these experiences suggest empowerment and ability to envision the future. These statements signify Ubuntu by highlighting a relationship between community and individual health.
Program Priorities, Activities, and Goals
This section examines the practical steps and goals that participants proposed should be embedded within the new program and could mediate the barriers to good mental and physical health. These include (a) mental health education, (b) life skills development, and (c) promoting safety, inclusion, and African community values.
Mental Health Education
Participants proposed that the new program should focus on mental and physical health but should infuse contemporary understandings with holistic and cultural values and practices grounded within the Ubuntu philosophy. For example, culturally informed cooking classes alongside the training component may enable children to learn from community elders about traditional food and learn to nourish their bodies for optimum sporting performance. Participant 1 preferred ‘for an African person to talk to an African person about mental health’ and others suggested that interventions would ideally build upon existing community activities. However, participants also reported a lack of African mental health experts.
Combining a fun and engaging educational program alongside the basketball was suggested to provide consistent health information and help to address those intergenerational differences in understanding and managing mental health. Age appropriateness of information was also identified by parent participants as a contributing factor to addressing these differences, ensuring that information was relevant regardless of life experience, age, or context. Participant 2 suggested that relevant information could provide insight about how untreated mental ill health could impact on family members, and Participant 3 highlighted the need for child-friendly information and activities such as being able to identify and respond to different emotions. Most participants agreed that more information could improve health literacy overall, with potential positive impacts beyond mental health but in other domains including reducing drug and alcohol consumption and criminal behaviour and improving family relationships and community engagement. Similarly, another priority was mediation, information, or referrals to existing and well-regarded mental health services specific to the person’s circumstances. Both older and younger participants reported that a more holistic approach may support children and their families beyond the program delivery.
Life Skills Development
Life skills development was desired as a core program component across the participant cohort. Ideas proposed by participants include fun and engaging activities centred around ‘life lessons’ and learning opportunities for children on topics such as confidence building, leadership, financial skills, English language development, emotional coping mechanisms, athletic capability, life responsibilities, positive behaviours, and developing self and community care strategies. Such activities would reportedly support children with the ‘struggles’ they experienced across different emotional, physical, behavioural, and social aspects of their lives and were reflected in the Ubuntu philosophy. For those who identified this component, life skills development was considered an important first step towards problem-solving and may equip children with the knowledge and capacities to live well in the future. For example, Participant 7 discussed their interest in the economy, and developing economic literacy early may assist young people to secure employment, contribute to the economy and ‘even just helping create. . . solving problems in people’s lives’.
Program mentors were identified by participants as a vital role in helping young people develop life skills, where coaches and mentors would reinforce positive behaviour and teach children appropriate ways of engaging with their peers. As Participant 9 said, ‘to learn that at a young age is very important’.
Promoting a Cohesive, Safe, and Inclusive Community
All participants indicated that the new program should incorporate activities that promoted safety, inclusion, and existing community cohesion, which related to their existing positive experiences of community connection as a precursor to good health and were reported to counteract the racism and discrimination often encountered in other settings. Across the participant group, a sense of cultural and emotional safety, belonging and physical security were identified as foundational to thriving children and families. Furthermore, embedding these principles into the program might contribute to rebuilding trust with other social groups where discrimination was reported.
For some participants, incorporating anti-racism training within the host primary school might help to create a safer and more inclusive environment for students. Engaging in sub-conscious bias and active bystander training was thought to develop a greater awareness of discriminatory behaviours and would also encompass ‘teachable moments’ for children. Participant 2 commented that if teachers demonstrated increased awareness and accountability of their biases and actions, they might offer important role modelling for students to understand how stigma, bias, and racism ‘affects other people’s behaviour’.
Other inclusion activities responded to the desire for family involvement at the basketball games. Some suggestions included simultaneous social games for children and their parents; information sharing and peer support that would let ‘people know that support and help is there any time’ (P11); and explicit strategies that would cater to different genders, religions, and cultures playing together (e.g. a modest uniform for Muslim girls).
Discussion
Understanding community members’ views and aspirations for the Junior Rhinos Basketball Program produced new findings that address a literature gap on those factors that promote and restrict African-Australian peoples’ health and well-being. The findings also highlight potential factors which may contribute to the development of a culturally responsive and fit-for-purpose program, and which inform the design and implementation of the Junior Rhinos program for school-aged children.
This study examines how African-Australian communities living in South-Eastern Melbourne experience structural barriers and promoters of health and well-being. Furthermore, the findings of this research suggest that community involvement in program design may valorise community values, practices, and knowledge. The study builds on recent studies that demonstrate the importance of social connection and social capital as mediators of belonging, perceived accessibility of services and increased health (Abur & Mphande, 2020; Fozdar, 2023; Mwanri et al., 2023). Additionally, this article contributes to a growing body of evidence detailing how African-Australian peoples’ experiences of racism and social exclusion has direct implications for health outcomes and experiences of health (Ikafa et al., 2022; Majavu, 2018; Mude & Mwanri, 2020; Shepherd et al., 2022; Udah & Singh, 2019; Uptin, 2021).
Participants identified social and structural barriers to good health by highlighting negative experiences in social settings, which they describe as having implications for an individual’s belonging and social connection. In addition, participants spoke of the consequences that these experiences of non-belonging had upon economic stability and educational attainment. These factors reflect broad themes identified within existing literature, in contexts such as human services organisations and schools, as well as social and public spaces (Ikafa et al., 2022; Shepherd et al., 2022; Uptin, 2021). By prioritising activities promoting connection and belonging into the new program, we suggest that experiences of racism, discrimination, and the interpersonal and intercultural factors of resettlement might be mediated.
Although these barriers may not be unique to the participants in this study, the specific experiences articulated by participants might reflect the challenges felt by African-Australian communities particular to the context of study. Furthermore, this work is critical in then informing the design of the Junior Rhinos Basketball Program that aims to support health and well-being of young African-Australian people within this location. We propose that participants’ desire for safety and inclusion strengthens existing arguments that sports programs such as the Black Rhinos Basketball Program may have greater chance of enhancing individual health outcomes when they are co-designed to incorporate culturally sensitive interventions (McCann et al., 2016; Mude & Mwanri, 2020) specific to the values and needs of its beneficiaries and in the community that they live.
An interesting and novel finding with significant and community-wide implications for the program relates to generational differences in the conceptualisation and experience of mental health among participants. Although migration may present barriers to mental health in some cases, manifesting through the interruption of social connection and family ties (Nunn et al., 2022), family conflict (Correa-Velez et al., 2010), and increasing individualisation (Abur & Mphande, 2020), we posit that participants’ desire for culturally informed mental health education and life skills development as core components of the program highlights a shared desire to better understand and practice good health – individually and as a community. These program priorities illustrate the mutuality, moral responsibility, and interconnectedness evident within the Ubuntu philosophy (Winschiers-Theophilus et al., 2012) and further reinforces our suggestion that community – and cultural – promoters of health must first be identified and then incorporated into the design of a health program prior to its implementation.
Although the involvement in community sports and other outdoor group activities, education and employment is evident within existing literature (Baak et al., 2020; Ikafa et al., 2022; Ziersch et al., 2023), participants’ articulation of the potential benefits of these activities adds to this body of research and are relevant to the co-design of the Junior Rhinos program. For example, the participants’ feeling that the new program should increase these mediators of health as a potential way to counteract systemic barriers, namely racism and discrimination, as well as western-centric information and language or health discourse. Participant’s suggestion to incorporate both western and cultural health interventions may enhance social connection and social capital (Baak et al., 2020). However, we note that existing evidence suggests that systemic racism is more likely to be challenged by decentring the dominant western, White service interventions delivered to migrant and resettled communities (Udah & Singh, 2019; Uptin, 2021), which address and measure health through a white lens. As such, based on study findings we suggest that designing and developing health programs such as the Junior Rhinos Basketball Program could provide a powerful opportunity to centre African-Australian experiences, needs, and aspirations for their individual and community health.
Implications and Recommendations for Policy and Practice
Related to these findings, we identify two recommendations for practice a policymaking and program design levels. Firstly, because of the tendency in westernised countries for health interventions to focus on individualised treatments (Miller et al., 2022), it is likely that African-Australian people (among other migrant and resettled groups) may continue to face obstacles to good health unless there are explicit efforts to engage with the communities they are designed to serve prior to implementation. A crucial step may be for policymakers and program designers to undertake a coordinated and multi-level approach to designing health interventions that are grounded in community values, and for practitioners to consider the role of Ubuntu and community support more effectively within African-Australian community and better integrate these cultural factors into their planning. Secondly, researchers, practitioners, and program designers could demonstrate curiosity, flexibility, and preparedness to work in more culturally responsive ways to valorise community knowledge and decentre assumptions about what promotes or obstructs health. Similarly, practising reflexivity and cultural humility may also enhance trust, partnership, and collaboration, principles explicit to co-designing culturally responsive programs (Goff et al, 2024).
Limitations and Future Directions
There are some study limitations. Although we purposefully sought wider community understandings of what obstructs or promotes good health, the conditions of the university ethics approval meant that young people aged 8 to 14 who would participate in the new program were not interviewed or involved in the co-design process. The absence of young people’s views means that the program is designed through an adult lens. However, young adults (18–21) with current or very recent experience of the existing program did participate, increasing the relevancy of the program priorities. Secondly, recruitment was based on geographical location and involvement in the partnering agency, limiting the program priorities, activities, and goals to this context. Both limitations present opportunities for future research to understand the factors that shape health and well-being in a younger cohort and in other Australian and international settings.
Conclusion
When considering what promotes or restricts health and well-being for African-Australian people in Melbourne, participants reported various structural, interpersonal, and personal factors that impact upon their experience of good health. Such findings suggest that when designing programs aimed to support the health and well-being of migrant communities, incorporating localised community experience, knowledge, values, needs, and desires may be an important first step to embed health promoting interventions and to decentre western views and constructions of health that perpetuate racialised health outcomes. Ideally, when programs are designed with communities and based on their lived experience and a shared vision of a healthy and well life, it presents a transformative opportunity for young people, their communities, and the well-being of society at large.
Supplemental Material
sj-docx-1-prv-10.1177_26320770251351953 – Supplemental material for Promoters and Barriers to Good Health Within the African-Australian Community in South-Eastern Melbourne
Supplemental material, sj-docx-1-prv-10.1177_26320770251351953 for Promoters and Barriers to Good Health Within the African-Australian Community in South-Eastern Melbourne by Rachel Goff, Patrick O’Keeffe, Rob Cunningham, Ronnie Egan, Abraham Kuol, Bawa Kuyini and Robyn Martin in Journal of Prevention and Health Promotion
Supplemental Material
sj-docx-2-prv-10.1177_26320770251351953 – Supplemental material for Promoters and Barriers to Good Health Within the African-Australian Community in South-Eastern Melbourne
Supplemental material, sj-docx-2-prv-10.1177_26320770251351953 for Promoters and Barriers to Good Health Within the African-Australian Community in South-Eastern Melbourne by Rachel Goff, Patrick O’Keeffe, Rob Cunningham, Ronnie Egan, Abraham Kuol, Bawa Kuyini and Robyn Martin in Journal of Prevention and Health Promotion
Footnotes
Acknowledgements
The authors acknowledge the guidance of Selba-Gonzalez Luka, CEO and Founder of Afri-Aus Care, the Afri-Aus Care community for their partnership, and the support of VicHealth in funding this project.
Ethical Consideration
Ethical approval for this project was given by RMIT University Human Research Ethics Committee (Reference Number 25696).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Victorian Health Promotion Foundation (VicHealth) [Grant OPP-25155].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.