
Abstract
Syrian refugees underutilize mental health services in Western receiving countries, which is partly attributable to negative attitudes toward seeking professional psychological help (APPH) and denial of the need for psychological help (DNPH). Interventions tailored to culture-specific characteristics of Syrian refugees are needed. We tested an intervention that disseminated information about the benefits of psychotherapy via ostensible interview vignettes to 205 German residents and 187 Syrian refugees residing in Germany. We used a 2 (group: residents vs. refugees) × 2 (source of information: ingroup vs. outgroup member) × 2 (therapy content: skill training vs. emotion regulation) × 2 (gender: women vs. men) between-participants design with the dependent variables APPH and DNPH. We measured adherence to masculine norms, support by religious faith, and distress disclosure as additional predictors. Refugees reported more negative APPH and higher DNPH than residents. Source of information and therapy content had no detectable effect. Men reported more negative APPH and higher DNPH than women. Adherence to masculine norms emerged as the strongest predictor of APPH. Masculine norms and support by religious faith partly explained differences between refugees and residents in APPH and DNPH. Exploratory post hoc analyses with nonintervention samples of 182 Syrian refugees and 202 residents from a similar study indicated that Syrian refugees who received an intervention (vs. no intervention) reported more positive APPH. No such difference was found for residents. Disseminating information about psychotherapy could positively impact APPH/DNPH in refugees but needs to be tailored to their sociocultural context. We outline recommendations for further research.
Keywords
Since the outbreak of the Syrian civil war, more than 6 million Syrians have been forced to flee their home country, with more than 1 million Syrians having arrived in Germany since 2015 (United Nations High Commissioner for Refugees [UNHCR], 2020). Syrians currently constitute the largest group of asylum seekers in Germany (Renner et al., 2020). Experiences of war and persecution, migration perils, and resettlement stressors make them vulnerable to a range of mental disorders (Henkelmann et al., 2020). However, refugees underutilize mental health services in Western receiving countries (Satinsky et al., 2019). Administrative barriers and legal issues contribute to this discrepancy (Satinsky et al., 2019). Among Syrian refugees in Germany who are in need of mental health care, only 5% actually receive such support within an average waiting period of 6 months (see Bundesweite Arbeitsgemeinschaft der psychosozialen Zentren für Flüchtlinge und Folteropfer [German Network of Rehabilitation Centers for Refugees and Survivors of Torture], 2016). In addition, in the first 15 months after arrival in Germany, cost coverage of therapy is uncertain because of restrictions in immigration and asylum laws. Although the mental health needs of refugees and culturally sensitive therapy approaches are widely known (de Graaff et al., 2020, 2022), a lack of interpreters, limited therapy places, and bureaucracy pose severe barriers to mental health treatment of refugees in Germany (Böttche et al., 2016; Golchert et al., 2019).
Beyond these practical barriers, cultural and psychological factors such as (fear of) stigma and negative attitudes toward seeking professional psychological help contribute to the lack of service use (Byrow et al., 2020). Attitudes toward seeking professional psychological help (APPH) and the denial of the need for psychological help (DNPH) are important predictors of actual help-seeking behavior (Byrow et al., 2020; Schlechter, Wagner, et al., 2023). APPH and DNPH restrict the acknowledgment of psychological problems and may thus hinder treatment-seeking among refugees (Hassan et al., 2015). Targeting these factors in refugees should therefore be a public health priority.
Providing specific information about psychotherapy is crucial for promoting positive APPH and reducing DNPH (Gulliver et al., 2012). Interventions that disseminate knowledge about the benefits of psychological help-seeking seem to be one promising outreach to target refugee populations (Nickerson et al., 2020). Ideally, such interventions should have a wide outreach while simultaneously reducing demands on the receiving end. Before implementing any interventions, effects of their components need to be tested empirically for which creating interview vignettes is pertinent (Hughes & Huby, 2012). Here, we present ostensible interview vignettes to pinpoint whether the factors source of information and therapy content promote APPH and reduce DNPH in Syrian refugees in Germany.
Source of Information
Qualitative research suggests that Syrian refugees in Germany have poor information about mental health services and concludes that adequate information about therapy needs to be provided (Renner et al., 2020). The source of information of such intervention efforts seems critical because it is likely to affect susceptibility to, and trust in, disseminated information about psychotherapy. Refugees often express a lack of trust and concerns about confidentiality in mental health services and providers of relevant information (Byrow et al., 2020). Therefore, providing information about mental health services needs to be tailored to refugees’ sociocultural background (Nickerson et al., 2020). However, both practitioners and patients in Europe typically lack sufficient experience with and knowledge about culture-specific views of mental health in Syria (Böttche et al., 2016). Accordingly, Syrian refugees may have insufficient trust in sources of mental health information (provided by either practitioners or patients) who belong to the majority groups of receiving societies.
Issues afflicting Syrian refugees’ susceptibility and trust in mental health information could be remedied when they receive such information from other refugees who possess relevant experience and are sufficiently trustworthy. We examined whether providing information about the benefits of mental health services is more effective when it is conveyed by other refugees (vs. someone with the typical background of a receiving Western society). Specifically, the perceived legitimacy of information about these services may increase when fellow refugees report symptom relief from seeking psychological help. This aligns with the findings that information provided by ingroup members is more likely to initiate behavioral and attitude changes (Reynolds et al., 2015). Other refugees may be particularly appropriate sources because they often share the experiences of forced migration, migration perils (Echterhoff et al., 2020), and similar cultural and religious values.
Therapy Content
Patients’ expectations of mental health treatment, including therapeutic content, may critically influence APPH. Refugees often report symptoms related to anxiety, depression, sleep problems, somatization, and traumatic stress (Borho et al., 2021; Henkelmann et al., 2020; Lies et al., 2021). Especially two forms of mental health treatment appear effective for such symptoms, namely (1) trauma-focused therapy to deal with emotional consequences of traumatic events (Bisson et al., 2007) and (2) skill training that provides practical coping strategies for stressful situations or sleep problems (Van Heemstra et al., 2019).
Syrian refugees show lower levels of distress disclosure than residential populations, which partly explains their more negative APPH (Schlechter, Kamp, et al., 2021). They tend to express psychological symptoms in indirect ways using specific idioms and do not want to be exposed as weak or vulnerable persons (Hassan et al., 2015). Therefore, Syrian refugees could fear a lack of cultural sensitivity within Western therapeutic settings (Hassan et al., 2015; Robards et al., 2018). Moreover, refugees hold the view that personal problems need to be discussed within the family and not with mental health professionals (Hassan et al., 2015). In general, members of refugee communities may also express concerns that disclosing distressing emotions could be a reason for deportation or other asylum decisions (Raymond-Flesch et al., 2014). Although speaking about emotional experiences is important during therapy, for example, in the context of posttraumatic stress disorder (Bisson et al., 2007), Syrian refugees may express more negative APPH when they expect that they have to talk about their emotions during a therapeutic session. As a countermeasure, refugees could learn that there are other benefits of therapy beyond the disclosure of emotions.
Somatic symptoms are central in understanding refugees’ mental health (Schlechter, Wilkinson, et al., 2021), and refugees may be interested in learning specific skills in therapy to cope effectively with these symptoms (e.g., positive activities, relaxation exercises, or sleep training). They may prefer to learn how to cope with their symptoms without talking about potentially underlying reasons or feelings associated with their conditions, especially if they fear that therapy elicits trauma-associated memories (Reebs et al., 2017). Learning these skills may be perceived as faster and less intense than other therapy forms and can be delivered in group sessions (Van Heemstra et al., 2019), thus posing fewer demands on refugees. Although in many cases emotionally intense therapies like trauma-focused cognitive behavior therapy are more effective than other therapy forms (Bisson et al., 2007), focusing on skills may thus be a better starting point to motivate refugees to reach out for help. Indeed, recent transdiagnostic intervention approaches tailored to refugees’ needs aim to enhance self-efficacy without directly addressing the content of traumatic events (Van Heemstra et al., 2019). In addition, the World Health Organization developed Problem Management Plus, a brief transdiagnostic intervention targeting symptoms of depression, anxiety, and distress that was effective among Syrian refugees (de Graaff et al., 2020, 2022).
Gender and Psychological Help-Seeking
When disseminating such interventions, it is important to consider that in Germany, the context of the present study, the majority of asylum seekers are male (BAMF, 2020). According to culture-specific norms, men may believe that sharing distressing feelings is a sign of weakness and that doing so results in the loss of face or reputation (Addis & Mahalik, 2003; Leong & Zachar, 1999). This often leads to more negative APPH in men than in women (Mackenzie et al., 2006). As a result, men (vs. women) reach out less frequently for psychological help (for a meta-analysis, see Nam et al., 2010). In many Middle Eastern cultures, suffering is commonly conceptualized as an inherent part of human experience (Hassan et al., 2015). According to the corresponding cultural norm, individuals, especially men, are expected to have the strength to cope with adversity and suffering (Hassan et al., 2015). It is, therefore, important to examine the effects of gender in the context of interventions aiming at increasing psychological help-seeking attitudes in Syrian refugees.
Further Relevant Constructs
As outlined above, the key goal of the present research is to investigate how the source and content of information about mental health services and psychotherapy affect Syrian refugees’ APPH and DNPH. However, it is also important to consider other potential predictors of these outcomes. Beyond gender, one critical variable is refugees’ willingness to disclose distressing emotions, which has been found to partially mediate differences in APPH between refugees and residents (Schlechter, Kamp, et al., 2021). Moreover, sharing distressing information is an act of admitting psychological problems and could thus be inherently related to DNPH. Furthermore, support by religious faith can play a critical role in coping with mental health problems in refugees (El-Khani et al., 2017). In previous studies, refugees reported religious faith to provide a positive perspective because they believed that their future relied on God/Allah (El-Khani et al., 2017; Reed et al., 2012). Syrian refugees may thus report more negative APPH when they have more religious faith because they see no necessity to turn to Western mental health practitioners. Adding to our considerations concerning gender, conformity with masculine norms is another key variable. Men often adhere to norms of masculinity that they must be strong, in control, and able to handle problems by themselves—seeking help and admitting mental health problems is seen as a sign of weakness (Vogel & Heath, 2016). Agreement with masculine norms is an important antecedent of help-seeking attitudes (Wong et al., 2017). It is thus relevant to assess the degree of conformity to masculine norms in relation to APPH/DNPH.
The Present Study
We designed vignettes including information about psychological help, with the aim of improving APPH and reducing DNPH in Syrian refugees. The vignettes were presented to Syrian refugees residing in Germany and to German residents, constituting the quasiexperimental factor “group” (German residents vs. Syrian refugees in Germany). We varied the source of information (ingroup vs. outgroup) and therapy content (skill vs. emotion regulation training) experimentally and included gender (women vs. men) as a factor in our analyses.
We expected an interaction effect of source of information and group in that both groups report more positive APPH when an ingroup member presents the information compared with an outgroup member. We expected this effect, however, to be more pronounced in Syrian refugees because of an assumed positive baseline level of attitudes toward help-seeking in residents (Schlechter, Kamp, et al., 2021). Because this previous study found that Syrian refugees report lower levels of distress disclosure than residents, we predicted that Syrian refugees react hesitantly when they learn about working on emotions as an inherent part of therapy. Syrian refugees were thus expected to report more positive APPH when practical skill training was described compared with emotion regulation training.
Overall, we expected Syrian refugees to report more negative APPH and higher DNPH than German residents (Schlechter, Kamp, et al., 2021). Men were expected to report more negative APPH and higher DNPH than women (Nam et al., 2010). We predicted that Syrian refugees would report less distress disclosure and more support by religious faith and agreement to masculine norms than residents. We expected associations of these variables with APPH/DNPH and, therefore, tested the indirect effects of these variables in accounting for group differences.
Methods
Participants and Design
We used a 2 (group: German residents vs. Syrian refugees residing in Germany) × 2 (source of information: ingroup member vs. outgroup member) × 2 (therapy content: skill training vs. emotion regulation) × 2 (gender: women vs. men) between-participants design. Dependent variables were APPH and DNPH. While group memberships (refugees vs. residents/women vs. men) were quasiexperimental factors, participants were randomly assigned to one of the experimental conditions resulting from combinations of the other two factors, source of information and therapy content. Previous studies that tested the effects of improving stigma-related knowledge in vulnerable populations reported small-to-moderate effects (Clement et al., 2015; Nickerson et al., 2020). Given the potential outreach of our intervention strategy, we considered an effect size of f = .25 meaningful.
A power analysis indicated that 45 participants are needed per group to detect such an effect (α = .05; power, 1−β = .80). To account for nonusable data, we aimed to include around 50 participants for each experimental condition in both the refugee and resident groups. Initially, N = 410 individuals participated; 205 were German residents, and 205 were Arabic-speaking refugees residing in Germany. Because 11 refugees were not from Syria, their data were excluded from further analyses. Data from seven further refugees were excluded after an attention check (see below), resulting in n = 187 Syrian refugees (total N = 392).
Participants had to be at least 18 years old, had to speak German or Modern Standard Arabic, and had to be nonpsychologists. To implement our study, we used the program unipark questback (https://www.unipark.com). This software assigned participants randomly to one of the four experimental conditions. We disseminated the link to our online survey via social media (e.g., Facebook groups like “Syrians in Germany” with approximately 70,000 members) and email (using lists that were acquired through contacts with social workers and volunteers) to refugees and residents. Monetary compensation for participation was 5 Euros. Arabic native speakers of a German translation office working according to certified norms (DIN EN ISO 17100) translated all materials into Modern Standard Arabic. The received material was carefully double-checked by an Arabic native speaker, which led to slight adjustments of the wording. The study was approved by the ethics committee of the psychology department of the University of Münster (2018-44-JKn). Demographic data are shown in Table 1. More residents were women, whereas more refugees were men, χ2 (1, N = 392) = 116.27, p < .001. Most refugees arrived in Germany 3 years before data collection.
Demographic Characteristics of the Sample, N = 392.
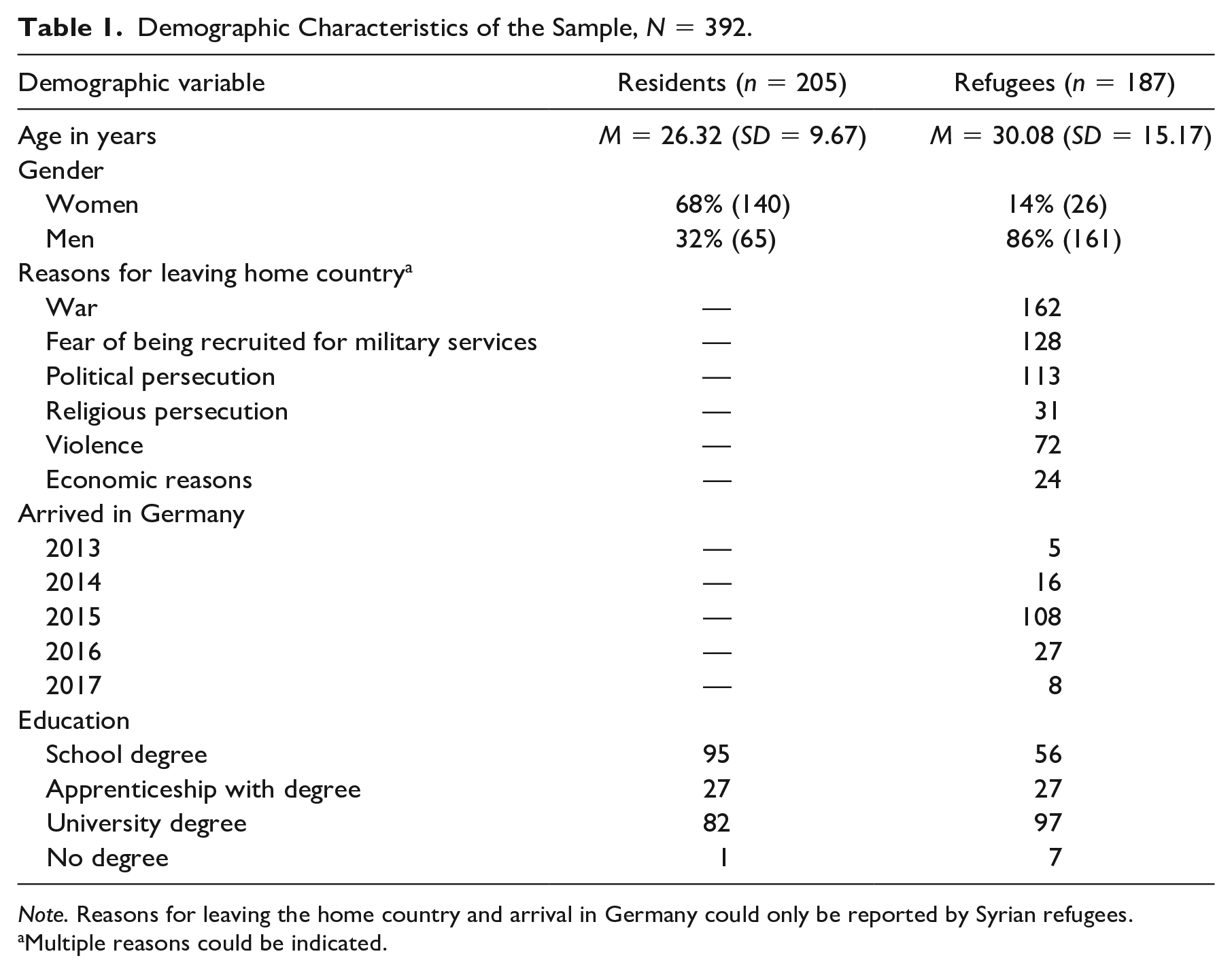
Note. Reasons for leaving the home country and arrival in Germany could only be reported by Syrian refugees.
Multiple reasons could be indicated.
Materials
First, participants were informed about the purpose of the study, the anonymity of participation, and the possibility of ending their participation at any time without any negative consequences. Participants provided informed consent by agreeing to these terms of participation. To assess the levels of depressive and anxiety symptoms, we then asked participants to complete the Patient Health Questionnaire-4 (Gräfe et al., 2004). An Arabic version was used for Syrian participants, and a German version was used for residents of Germany. Next, they read the interview vignettes and responded to the attention check. The other questionnaires were presented in the order in which they are presented in the following sections.
Interview Vignettes
Participants read interview vignettes developed by the authors of the study. In all vignettes, a person was presented who benefited from seeking professional psychological help after encountering mental health problems. Four different versions of the interview vignettes covered the combinations of the two independent variables: (1) source of information (ingroup vs. outgroup) and (2) therapy content (skill training vs. emotion regulation training). To make ingroup or outgroup membership salient, the name of the person was either Mohammed or Michael, representing a common Syrian or German name, respectively. This way, Mohammed represents an ingroup member for Syrian refugees and an outgroup member for residents, whereas Michael represents an outgroup member for Syrian refugees and an ingroup member for residents. Mohammed was forced to leave his country and had to flee to Germany. During his flight, he encountered potentially traumatic events. We did not specify the traumatic events because experiences can differ widely, but most refugees can relate to the experience of forced migration having experienced stressful and potentially traumatic events during their flight (Echterhoff et al., 2020). Michael, on the other hand, left his hometown and moved into a new city. Recently, he also experienced potentially traumatic events. In all vignettes, the described person visited a general practitioner because of somatic complaints (e.g., headache, stomach pain), matching the fact that many Syrian refugees in Germany report somatic symptoms that are medically unexplained (Borho et al., 2021). When no organic causes for the complaints could be identified, the general practitioner referred them to a psychotherapist for a mental health examination. After initial hesitation, the described person visited a psychotherapist. Now, he reflects on the benefits of going into psychotherapy in an interview format with a local newspaper. In all vignettes, the person reports symptom relief as a result of therapy and describes how he learned long-term strategies for coping with mental health problems.
The vignettes also differed as a function of the second independent variable therapy content. In the emotion regulation version, the person learned emotion regulation strategies and to identify, understand, disclose, and cope with distressing emotions. In the skill training version, the person describes specific skills and exercises that he learned during therapy (e.g., establishing positive activities in his life, the usage of relaxation exercises). In all vignettes, the interviewed person reports positive effects of the therapy on their life and reflects on how this process helped them to overcome stigma toward mental health problems. Vignettes were held constant in terms of wording and length. All materials can be found in the Supplemental Material and the open science framework (OSF) project in German, Arabic, and English (https://osf.io/g38j6/?view_only=13d3e45482d34b99bc304fc8782644b9). Note that only the German and Arabic versions were presented. The English version is based on our own translation and meant for readers not fluent in the two languages used in the study.
Attention Check
To ensure attentive reading, we asked three single-choice questions about the content of the interview: (1) “What did Mohammed (Michael) learn during the therapy?”, (2) “What is one specific example of a technique that Mohammed (Michael) learned during the therapy?”, and (3) “Why did Mohammed (Michael) initially go to a general practitioner?”. The response options are included in the Supplemental Material. As mentioned above, the data from seven refugees were excluded from analyses because of wrong responses to this attention check.
Psychometric Considerations
Scales that have been developed in Western contexts do not necessarily capture the same underlying constructs in non-Western refugee populations (Milfont & Fischer, 2010). Therefore, multigroup measurement invariance (MI) across residents and refugees was tested for the proposed factor solutions of the scales we have used. To this end, we tested increasingly constrained models in a confirmatory factor analysis framework. Given the ordinal data, we used the weighted least squares mean and variance-adjusted estimator for all models (Asparouhov & Muthén, 2010). First, the factor structure was constrained to be invariant across groups (configural MI). Second, factor loadings were constrained to be equal across groups to discern whether items relate in the same way to the underlying construct (metric MI). Finally, item thresholds were constrained to be equal over time to establish scalar MI. For unbiased mean comparisons, scalar MI should be established (Milfont & Fischer, 2010). The following criteria were used to evaluate model fit: The comparative fit index (CFI) and the Tucker–Lewis Index (TLI) should both be larger than .95 or .90, for a good or acceptable model fit, respectively. For the root mean square error of approximation (RMSEA) and standardized root mean square residuals (SRMR), values lower than .05 indicate good fit, values of .05 to .08 indicate moderate fit, and values of .08 to .10 indicate acceptable fit (Hu & Bentler, 1999). Next, we evaluated changes in CFI and RMSEA indices to establish MI: ΔCFI ≥ .015 and ΔRMSEA ≥ .010 to indicate deterioration in model fit (Milfont & Fischer, 2010). When full MI was not supported, we tested a partial MI model by relaxing constraints on certain parameters (Milfont & Fischer, 2010). Table 2 shows the results of the MI analyses.
Test of Measurement Invariance of All Tested Scales.
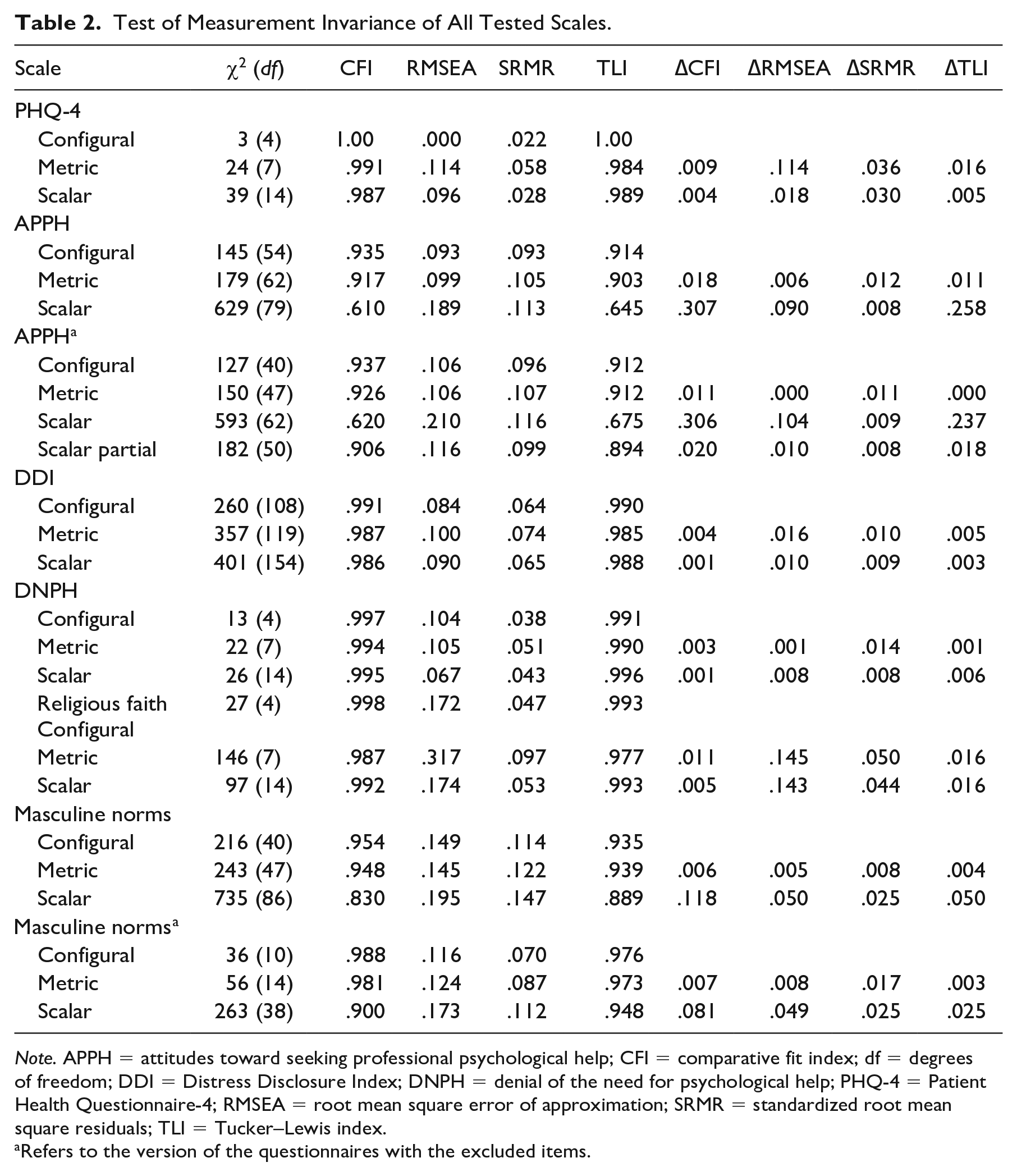
Note. APPH = attitudes toward seeking professional psychological help; CFI = comparative fit index; df = degrees of freedom; DDI = Distress Disclosure Index; DNPH = denial of the need for psychological help; PHQ-4 = Patient Health Questionnaire-4; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residuals; TLI = Tucker–Lewis index.
Refers to the version of the questionnaires with the excluded items.
Mental Health Symptoms
The Patient Health Questionnaire-4 (PHQ-4) comprises four items on a four-point scale from 0 (not at all) to 3 (nearly every day). It asks about symptom endorsement in the last 2 weeks, enabling a brief measurement of core symptoms of depression and anxiety (Gräfe et al., 2004). An Arabic version of the PHQ-4 has been validated in a representative sample of Syrian refugees in Germany (Kliem et al., 2016; α = .76–.83). In our analyses, a one-factor solution of the PHQ-4 was confirmed. All factor loadings in both groups were good (all > .60). Despite deterioration in model fit, according to all fit indices, the model fit for the model with measurement constraints on scalar MI was good to acceptable. This is in line with a representative study establishing MI of this measure between German residents and refugees (Tibubos & Kröger, 2020).
Attitudes Toward Seeking Professional Psychological Help
The Attitudes Toward Seeking Professional Psychological Help-Scale (ATSPPH-S; Ang et al., 2007; Fischer & Farina, 1995) comprises nine items ranging from 1 (disagree) to 4 (agree) and has been tested across different cultures (Ang et al., 2007, α = .70–.73). In our analysis, the model fit for configural MI was good, indicating that the factor solution is equally represented across groups. While metric MI was partially supported by the fit indices, model fit deteriorated substantially according to all fit indices when scalar MI was tested. A closer examination of the psychometric properties indicated that Item 4 displayed low factor loadings in both groups (≤.11). Hence, we excluded this item and tested MI again. The scalar MI model was problematic again, but when relaxing parameter constraints on the thresholds of Items 2, 7, 8, and 9, the model fit for partial scalar MI was acceptable. However, the model fit deteriorated compared with the metric MI model. This implies that the mean-level comparisons between the groups need to be interpreted carefully. An example item is “If I believed I was having a mental breakdown, my first inclination would be to get professional attention.”
Denial of the Need for Psychological Help
DNPH was assessed with a subscale of the Questionnaire on Psychotherapy Motivation (Fragebogen zur Psychotherapiemotivation—FPTM-23; Schulz et al., 2003) consisting of 23 items with six subscales ranging from 1 (strongly disagree) to 4 (strongly agree). The subscale DNPH consists of four items. The FPTM-23 is well validated for the German population (Schulz et al., 2003; α = .71). The model fit in our own analyses was good, all λs were >.40, and scalar MI could be established. An example item reads, “Most people with mental problems actually lack only willpower.”
Distress Disclosure
The Distress Disclosure Index (DDI; Kahn & Hessling, 2001) measures the tendency to disclose unpleasant feelings. The DDI comprises 12 items on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). Construct and criterion validity of the DDI have been established in several studies in different languages (for a review, see Kahn et al., 2012; α = .89–.95). In our own psychometric analysis, model fit and parameter estimates were acceptable to good, all λs were >.40, and scalar MI could be established (see Table 2). An example item is “I try to find people to talk with about my problems.”
Support by Religious Faith
The support by religious faith scale is a subscale of the Stress and Coping Inventory (Satow, 2012; α = .89). It consists of four items assessing how much support individuals find in religious faith when they are stressed, on a four-point scale from 1 (do not agree) to 4 (fully agree). Reliability and validity of this scale have been confirmed in further studies (Wurzer, 2016). The CFI, TLI, and SRMR indicated good model fit for the model testing scalar MI while the RMSEA did not. All factor loadings were good, all >.60 (Table 2). An example item reads, “When I am stressed, I find support in faith.”
Masculine Role Norms
We assessed masculine role norms with the Male Role Norms Inventory–Short Form (MRNI-SF; Levant et al., 2013; α = .89). Response options ranged from 1 (I do not agree) to 7 (fully agree). Construct validity of this scale was previously confirmed (Levant et al., 2013). Model fit for a one-factor solution was good in both groups, and metric MI could be established, yet scalar MI could not be established. We identified items that were problematic concerning factor loadings and item thresholds between groups. We thus excluded Items 1, 2, 7, and 9 from the model. While model fit for scalar MI was acceptable according to the CFI and TLI, it deteriorated compared with the model for metric MI. This suggests that mean comparisons between refugees and residents may be biased to a certain extent. An example item is “Men should not be too quick to tell others that they are important to them.”
Data-Analytical Strategy
Analyses were performed in R (R Core Team, 2021). The analysis code can also be found in the OSF project. First, we compared mean-level differences between refugees and residents and between women and men with regression models. Second, the effects of the intervention were examined with two 2 (group: German residents vs. Syrian refugees residing in Germany) × 2 (source of information: ingroup member vs. outgroup member) × 2 (therapy content: skill training vs. emotion regulation) × 2 (gender: women vs. men) between-participants analyses of variance (ANOVA) with the dependent variables APPH and DNPH. For post hoc comparisons, we used the Bonferroni-Holm correction. Third, we tested a pathway model with the variables outlined in the introduction (see Figure 1) using the lavaan package in R (Rosseel, 2012). The dependent variables were again APPH and DNPH. Group (German residents vs. Syrian refugees) and gender (women vs. men) were the independent variables, and distress disclosure, support by religious faith, and masculine norms were tested as potential mediators. For the indirect effects in this model, nonparametric confidence intervals (CIs) were generated with 10,000 bootstrap resamples (Hayes, 2015). We set α = .05, except for post hoc comparisons.
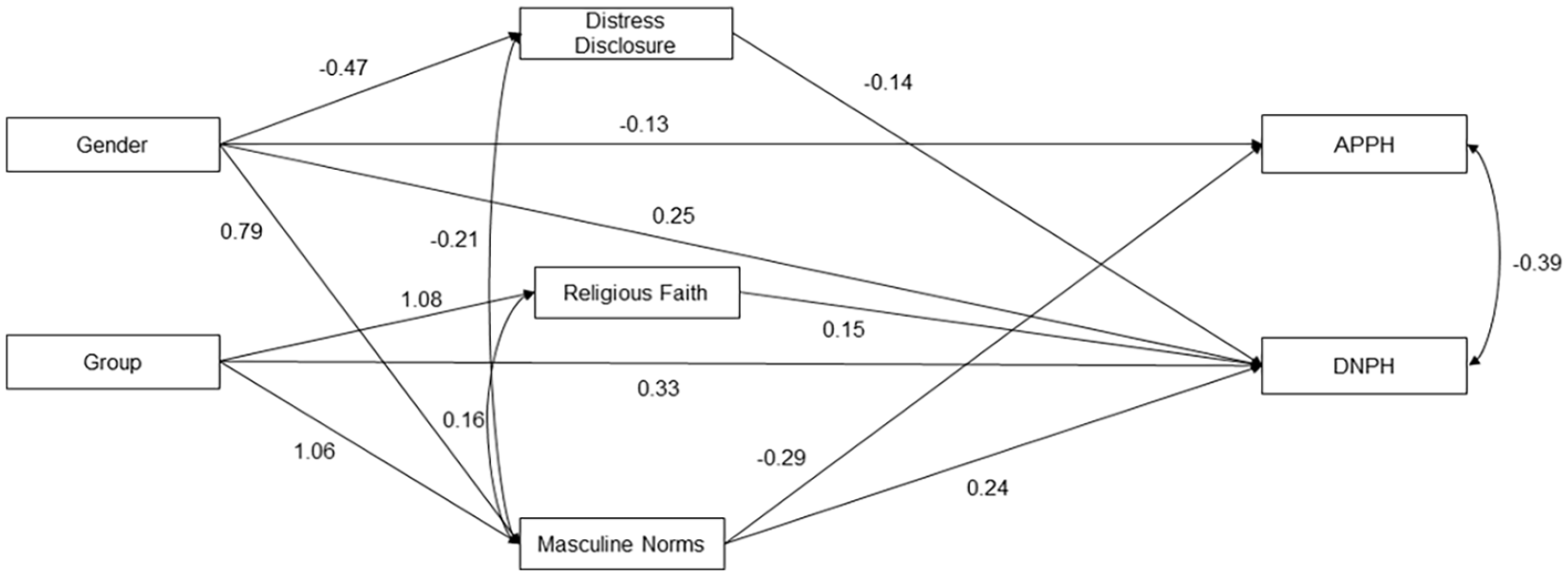
Pathway Model With All Variables
Results
Group Differences
Refugees reported more mental health problems, less positive APPH, more DNPH, more support by religious faith, and more agreement to masculine norms than residents (Table 3). Men reported less positive APPH, more DNPH, lower levels of DDI, and more agreement with masculine norms than women (Table 3).
Mean Scores With Standard Deviations in Parentheses and Simple Regression Models With Group (German Residents = 0; Syrian Refugees = 1) and Gender (Women = 0; Men = 1) as Predictors (Adjusting for Gender).
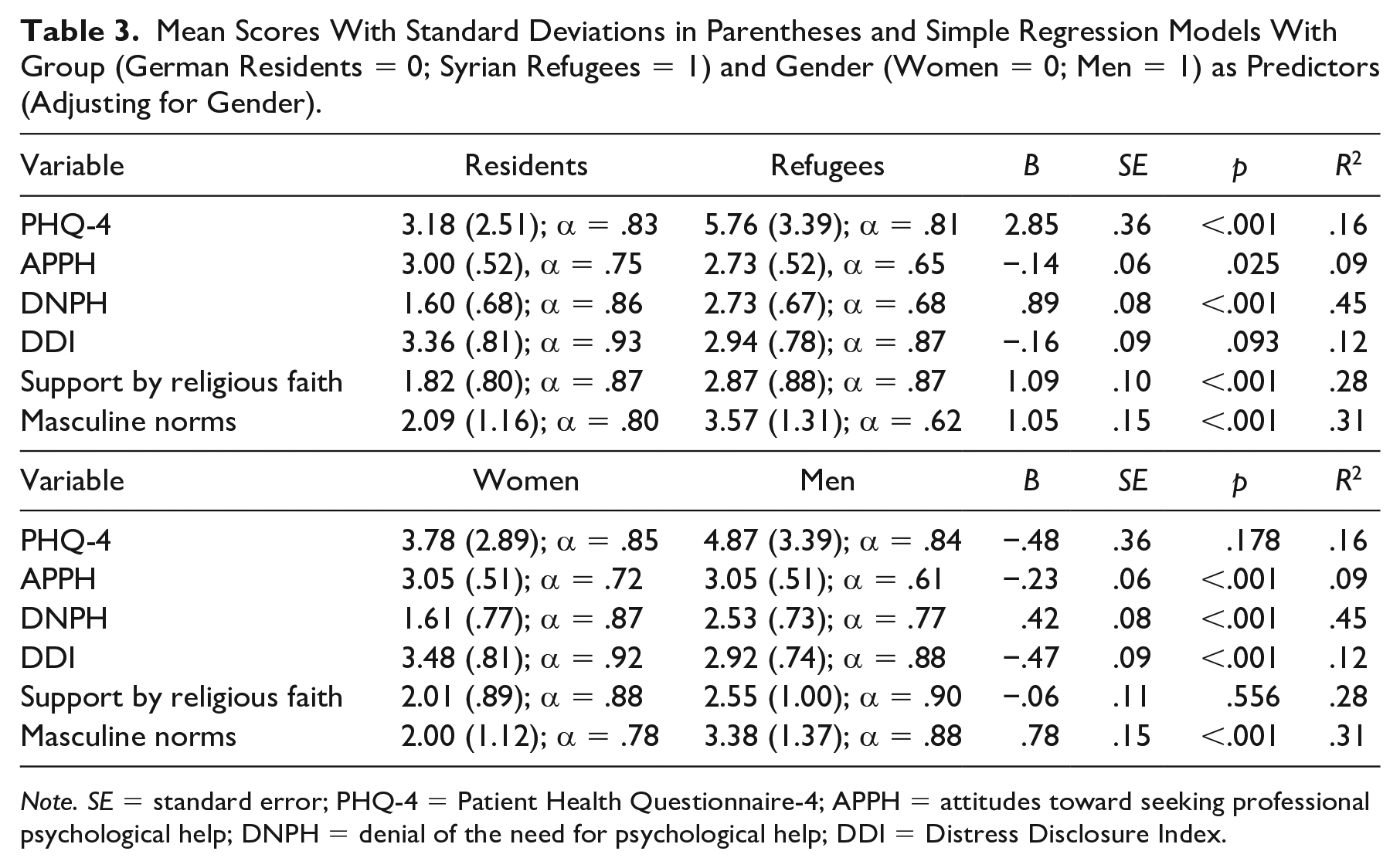
Note. SE = standard error; PHQ-4 = Patient Health Questionnaire-4; APPH = attitudes toward seeking professional psychological help; DNPH = denial of the need for psychological help; DDI = Distress Disclosure Index.
Effects of Group, Gender, Source of Information, and Therapy Content
Means and SDs for both dependent variables separated for the experimental conditions are shown in Table 4 separately for refugees and residents and for women and men. The ANOVA yielded a significant effect of group on APPH, F(1, 376) = 26.36, p < .001,
Means and Standard Deviations (in Parentheses) for the Dependent Variables Separated for Groups and Gender and the Independent Variables Source of Information (Ingroup vs. Outgroup) and Therapy Content (Skill Training vs. Emotion Regulation Training) .
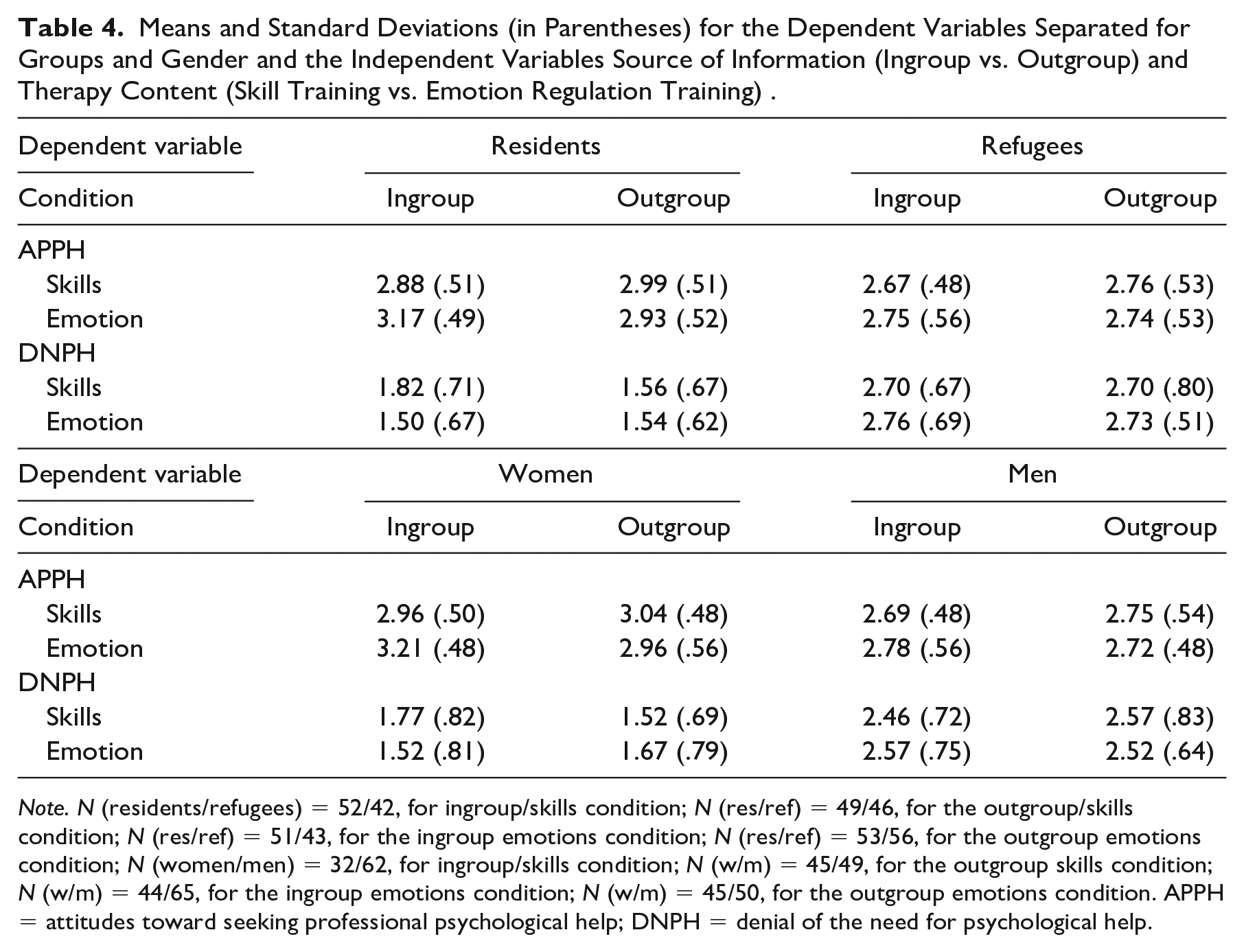
Note. N (residents/refugees) = 52/42, for ingroup/skills condition; N (res/ref) = 49/46, for the outgroup/skills condition; N (res/ref) = 51/43, for the ingroup emotions condition; N (res/ref) = 53/56, for the outgroup emotions condition; N (women/men) = 32/62, for ingroup/skills condition; N (w/m) = 45/49, for the outgroup skills condition; N (w/m) = 44/65, for the ingroup emotions condition; N (w/m) = 45/50, for the outgroup emotions condition. APPH = attitudes toward seeking professional psychological help; DNPH = denial of the need for psychological help.
Furthermore, the ANOVA revealed a strong effect of group on DNPH, F(1, 376) = 295.95, p < .001,
Pathway Model
There were no differences between residents and refugees in APPH once we controlled for distress disclosure, religious faith, and masculine norms (Figure 1 & Table 5). Women reported more positive APPH than men. Masculine norms predicted APPH, but distress disclosure and religious faith did not. The indirect effect of group and masculine norms on APPH was significant (indirect effect = −.11, 95% CI = [−.17, −.06], p < .001), and so was the indirect effect of gender and masculine norms on APPH (indirect effect = −.08, 95% CI = [−.13, −.04], p < .001). The effect of group on DNPH remained significant with refugees reporting more DNPH than residents. Men reported more DNPH than women (Table 5). Distress disclosure (negatively), religious faith (positively), and masculine norms (positively) predicted DNPH. The indirect effects of group via religious faith (indirect effect = .14, 95% CI = [.06, .23], p < .001) and masculine norms (indirect effect = .16, 95% CI = [.09, .23], p < .001) on DNPH were significant. The indirect effects of gender via distress disclosure (indirect effect = .07, 95% CI = [.02, .12], p = .003) and masculine norms (indirect effect = .16, 95% CI = .12 [.06, .18], p < .001) on DNPH were significant. APPH were positively related to DNPH. Masculine norms were negatively associated with distress disclosure and positively with religious faith.
Coefficients of the Main Pathway Model (Figure 1) Along With Correlation and Partial Correlation Coefficients (German Residents = 0; Syrian Refugees = 1; Women = 0; Men = 1).
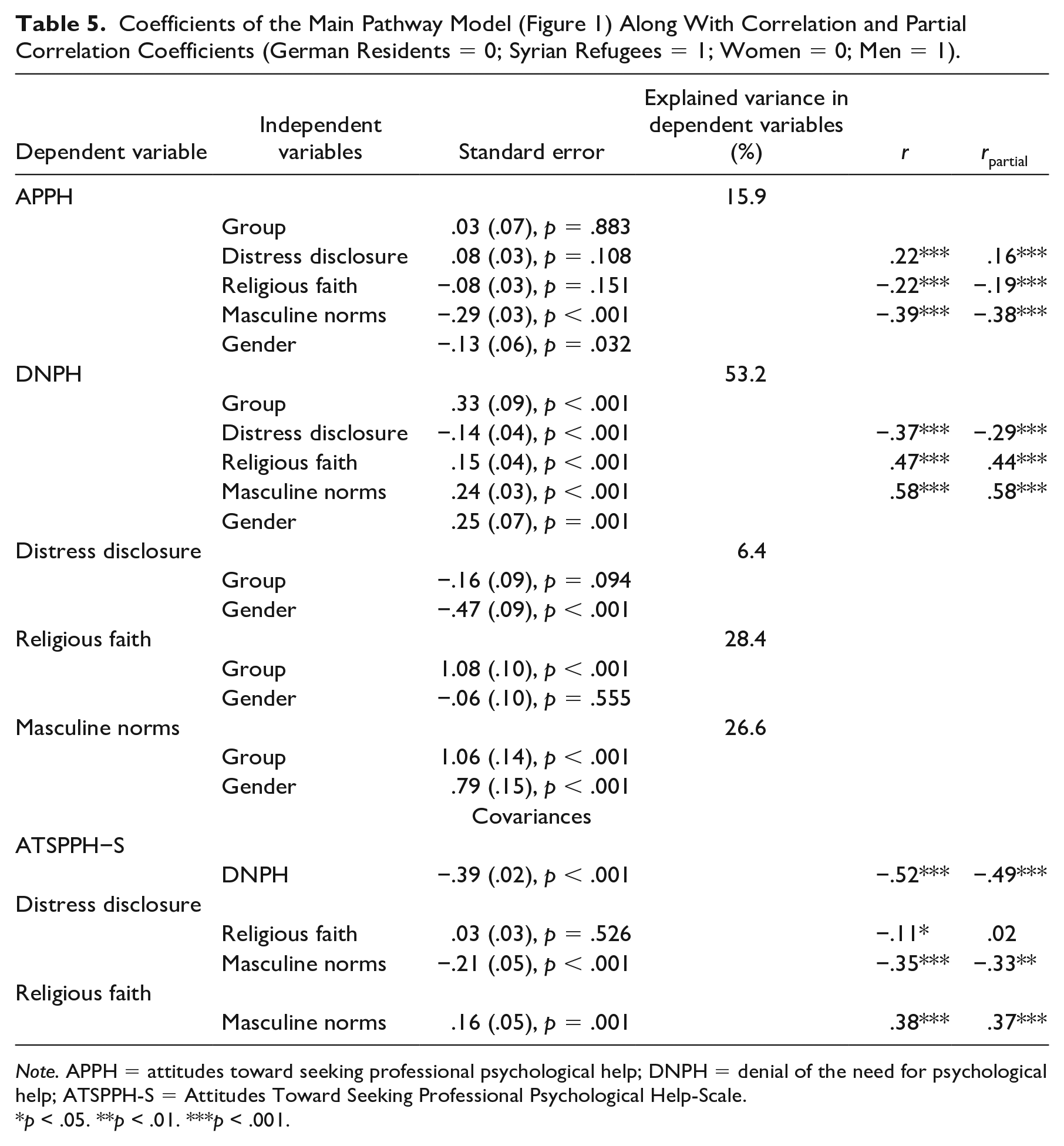
Note. APPH = attitudes toward seeking professional psychological help; DNPH = denial of the need for psychological help; ATSPPH-S = Attitudes Toward Seeking Professional Psychological Help-Scale.
p ˂ .05. **p ˂ .01. ***p ˂ .001.
Exploratory Comparison With a Previous Study
The present study lacked a control group without any intervention. Thus, it was not possible to determine whether the provision of information alone had an effect on APPH. To remedy this issue, we compared the findings from the present study to an existing data set, in which the ATSPPH-S was also assessed as a dependent variable (for details, see Schlechter, Kamp, et al., 2021). Importantly, no information about therapy was given in this prior study that cross-sectionally compared APPH between Syrian refugees and residents and tested the influence of distress disclosure (Schlechter, Kamp, et al., 2021). The comparison of these groups may thus function as a proxy of information versus no information about therapy (see “Discussion” for limitations). In the former study, Syrian refugees were recruited online via social media platforms and contacts to local refugee support centers. In brief, 202 German residents and 182 Syrian refugees participated. Of the German participants (Mage = 28.13 years, SD = 7.35 years), 154 participants were women, and 48 were men. Of the Syrian refugees (Mage = 25.56 years, SD = 9.19 years), 36 participants were women, and 146 were men. Recruitment methods, sample size, and demographic characteristics including the unbalanced gender distribution of this previous study were very similar to those of the present study. Therefore, we ran a 2 (group: German residents vs. Syrian refugees residing in Germany) × 2 (study: present vs. former) × 2 (gender: women vs. men) ANOVA on APPH. We note that this was an exploratory post hoc analysis, which we decided to conduct after data were collected.
The ANOVA revealed an effect of group, F(1, 768) = 47.09, p < .001,
Discussion
Consistent with previous work, Syrian refugees reported more mental health problems than residents and expressed more negative APPH and stronger DNPH (Schlechter, Kamp, et al., 2021). This highlights the need to target these barriers in refugees. To this end, we examined the effects of providing information about psychological help-seeking to Syrian refugees in Germany by designing interview vignettes of individuals benefiting from psychotherapy.
Source of Information and Therapy Content
Neither source of information nor therapy content had an effect on APPH or DNPH. We initially assumed that Syrian refugees’ APPH or DNPH would improve as a result of learning about reports from other refugees, due to greater trust and perceived socio-cultural commonalities (Hassan et al., 2015). Potentially, the experience of traumatic events, which were also described in the outgroup vignettes, was the salient factor that Syrian refugees were relating to, over and above other intergroup differences. Conversely, solely mentioning forced migration and traumatic events may have been too generic to evoke an ingroup affiliation. In addition, presenting vignettes may not suffice to increase trust and ingroup thinking compared with face-to-face conversations or videos, in which facial expressions and nonverbal behavior can be observed and contribute to the content of the discourse. These factors may have prevented us from detecting an effect of information source.
The factor therapy content did not reveal any effects either. It could be that the focus on specific aspects of the therapy content was not substantial enough. While reading the vignettes, participants may have focused on the overall concept of therapy and mental health symptoms so that the specifics of the content were not decisive. Potentially, it was rather relevant for the participants to reflect on the overall benefits of seeking psychological help. On a positive note, learning about sharing distressing emotions during therapy did not result in substantially lower mean levels. This is a relevant result in light of low levels of distress disclosure among Syrian refugees (Schlechter, Kamp, et al., 2021) and also in light of the efficacy of trauma-focused therapy (Bisson et al., 2007).
Effects of Gender
Men (vs. women) reported more negative APPH and greater DNPH in line with a previous meta-analysis (Nam et al., 2010). This may be attributable to social norms that are common in the culture of Syrian refugees (Hassan et al., 2015) and also reflected in the reports obtained in our study. Men may perceive reaching out for help as a sign of weakness that may result in the loss of face (Addis & Mahalik, 2003). However, we note that gender was unequally distributed, with more men in the refugee sample but more women in the resident sample, which limits the reliability of the analysis. Nonetheless, the gender effects found in the present study are relevant given that most asylum seekers in Germany are male (BAMF, 2020). Future intervention studies should address help-seeking attitudes especially among men who may feel they are expected to be sufficiently strong to handle their mental distress alone (Mackenzie et al., 2006).
Comparison With Previous Study
It is possible that sharing information alone influenced APPH (Gulliver et al., 2012). To shed light on this possibility, we analyzed cross-sectional data from participants whose characteristics were similar to those of the present study (Schlechter, Kamp, et al., 2021). Syrian refugees without any intervention reported more negative APPH than Syrian refugees that received an intervention in our study. German residents, however, did not differ from each other in this between-study comparison. This may indicate that our intervention influenced APPH in Syrian refugees. The vignettes may have provided an opportunity to reflect on the possibility of using mental health services. German residents, in contrast, may have been aware of the provided information as reflected in high mean levels across both studies. We note that the comparison of these groups can merely serve as a proxy of information about therapy versus no information about therapy.
Although recruitment methods, sample sizes, and demographic characteristics were comparable in both studies, there are still important limitations to this between-study comparison. We cannot pinpoint whether some individuals participated in both studies. Moreover, there was a period of a few months between the two data collection sessions; there may have been mean-level changes in the refugee population due to time-varying differences depending on the migration stage (Wu et al., 2021). Critically, we decided to conduct the analyses post hoc after data were already collected, reflecting limitations of our design. Given that practical interventions derived from our study are easy to administer with a broad outreach, the present effect size is nonetheless of practical relevance. Notably, the magnitude equals the effect size of a study that investigated a larger online-intervention program to reduce mental health stigma in Arabic-speaking refugees in Australia compared with a wait list control group (Nickerson et al., 2020). Future studies should examine APPH interventions longitudinally to discern whether they translate into actual help-seeking behavior.
Distress Disclosure, Support by Religious Faith, and Masculine Norms
Masculine norms emerged as the strongest predictor of APPH, and higher mean levels in Syrian refugees explained the group differences of a more negative APPH in refugees as well as gender differences between men and women, in accordance with previous work in nonrefugee populations (Heath et al., 2017; Vogel & Heath, 2016). Importantly, distress disclosure and religious faith were not significant in predicting attitudes when tested simultaneously with masculine norms.
Being a refugee (vs. resident), being a man (vs. woman), and all three measured predictors (distress disclosure, support by religious faith, and masculine norms) were associated with DNPH and displayed significant indirect effects, underscoring their relevance. Distress disclosure is a logical predictor of DNPH because admitting mental health problems is by definition an act of distress disclosure. In a therapeutic setting, it is crucial to disclose distressing information to enhance diagnosis, treatment processes, and therapy success (Vogel et al., 2006). However, coping with psychological distress does not necessarily involve sharing of emotional vulnerability in other cultures. Refugees may consider religious or other culturally specific rituals as appropriate ways of healing (Dein & Illaiee, 2013), as reflected in the association between higher levels of support by religious faith and more DNPH in Syrian refugees. Syrian refugees may find relief in their trust in God/Allah, without seeing the necessity of sharing their mental health problems (El-Khani et al., 2017). Masculine norms predicted DNPH and were more pronounced in Syrian refugees. Although more men were in the Syrian refugee group, this effect was present despite including gender as a factor so that it cannot be attributed exclusively to the unbalanced gender distribution. Among Syrian refugees, opening up on mental health problems may be seen as a sign of weakness because they may believe that men have to handle their problems by themselves (Vogel & Heath, 2016). Masculine norms and distress disclosure were negatively correlated. Internalizing masculine norms may cause lower levels of distress disclosure, which needs to be shown empirically. If demonstrated, interventions could be more successful when they address masculine norms instead of distress disclosure. This could also be a reason why our manipulation of therapy content was not successful. Although we provided information about someone who learned to disclose distress, we did not address masculine norms. Masculine norms could have prevented participants from stronger changes in APPH when presented with information about distress disclosure. Further studies could describe men as role models that maintained their masculinity despite seeking help.
Implications
Our study was designed from a Western perspective of psychotherapy and is prone to ethnocentric bias. Future interventions could expand these descriptions and emphasize more culturally adapted specifics to create a better fit between Western psychotherapy and the need of non-Western refugees. Syrian refugees have specific idioms that represent psychological distress (Hassan et al., 2015). Describing their successful treatment may improve APPH. It needs to be considered that Syrians come from diverse ethnic and religious backgrounds. Among the 21 million citizens are Syrian Arabs, Kurds, and Assyrians among others (Regional Office for the Eastern Mediterranean, n.d.). The largest ethnic group is represented by Syrian Arabs, and the largest religious group is Sunnis. These context factors are important for an adequate delivery of mental health treatment. In a similar vein, intervention factors need to be tailored to the specific resettlement stage (e.g., crisis intervention after arrival vs. long-term therapy) because the postmigration period is not a fixed time (Wu et al., 2021). At the time of the data collection, most Syrian refugees in the current sample had been in Germany for around 3 years, and it needs to be investigated whether their attitudes change as a function of time. In addition, many Syrian refugees in the current study hold university degrees and were well educated. It is important to tailor interventions to the educational background of individuals. Furthermore, it is critical to consider additional variables such as stigma, mental health literacy, degree of acculturation, trust in the receiving countries’ health care systems, treatment-seeking intentions, self-efficacy, and behavioral antecedents to understand APPH and DNPH (Gulliver et al., 2012; Schlechter et al., 2023).
Limitations
We recruited a sample of Syrian refugees currently residing in a Western receiving country. Although a representative sample would be desirable, demographics of the refugee group, especially age and gender, reflect those described by official sources of refugees in Germany (Juran & Broer, 2017). While we included gender as a factor in all analyses, studies with more balanced samples are needed to reduce the extent of gender bias in the study conclusions. The interviewed person in the vignettes was always male. Given the findings regarding masculine norms, gender effects need to be investigated more systematically to inform future intervention research. While our overall sample size was reasonably large, the sample sizes for each cell were relatively small, which may have contributed to a lack of statistical power. Moreover, the study lacked a control question to gauge the extent to which participants related to the person in the vignettes, which would have increased confidence in our intended manipulations. In addition, we did not include a manipulation check that specifically tested whether trust was elicited by the source. Indirect effects must be interpreted with caution because cross-sectional data cannot establish causality. Materials were translated into Modern Standard Arabic for Syrian refugees. For most scales, we could establish scalar MI. However, for the ATSPPH-S and MRNI-SF, scalar MI was not fully established. Hence, mean-level comparisons between refugees and residents may be biased and need to be interpreted carefully (Milfont & Fischer, 2010). Also, the internal consistencies of APPH, DNPH, and masculine norms were relatively low in the refugee group.
Conclusions
Promoting APPH in current refugee populations may be achievable by disseminating information about psychotherapy. Research underpinned by our findings could elucidate more culturally tailored factors that could improve APPH in refugees. Further research is crucial for intervention studies, practitioners, and refugees suffering from mental health problems.
Footnotes
Data Availability
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by SAFIR Muenster.
Supplemental Material
Supplemental material for this article is available online.