
Abstract
While there is relatively high patronage of traditional healers in South Africa, their approaches toward mental illness remain shrouded in mystery. The research therefore explored the beliefs and practices of traditional healers at Dube Village, Soweto, South Africa regarding the reasons for and treatment of mental illness and was guided by an Afrocentric theoretical perspective. Qualitative interviews with 14 traditional healers revealed that mental illness could be identified by throwing the bones, observations, and history-taking. They attributed mental illness to spiritual, socio-cultural, psychosocial, and physical factors. Methods used to treat mental illness included removing evil spirits through washing, steaming, induced vomiting, and administering herbal remedies. Findings suggest that while there are many similarities with biomedicine, traditional healing differs in terms of its links with spirituality and the efforts of healers to answer the question why things happen from a collectivist perspective.
Keywords
Standard textbooks of abnormal psychology refer to the conceptualization of mental illness as clinically significant psychological behavior associated with disability or distress (e.g., Hooley et al., 2020). Mental disorders do not only reflect individual psychopathology within the person, but may also be related to broader political and socio-economic processes (Kaiser & Jo Weaver, 2019). According to Madzhie et al. (2014), factors in the South African context that contribute to mental health issues include diseases such as HIV/AIDS, poverty, unemployment, drug and alcohol abuse, political violence, and the weakening of the traditional value and kinship system. More recently, researchers such as Gone and Kirmayer (2020) have found that many indigenous peoples, including black South Africans, who have experienced the devastating impact of European colonization in the form of transgenerational trauma, continue to suffer from high rates of mental health problems. In terms of impact, mental illness causes severe distress for affected persons and their families, makes it difficult for people to hold down jobs, raise a family or relate to others socially, and incurs high costs in healthcare (Jacob & Coetzee, 2018; Madzhie et al., 2014). With regard to prevalence, it is estimated that approximately 450 million people globally suffer from some type of mental disorder, while a South African epidemiological study identified a mental disorder prevalence rate of 16.5% of the adult population (Williams et al., 2007). Research suggests that 3% of the population suffer from severe mental illness and that 90% of these persons do not receive treatment (Williams et al., 2007).
Essentially there are three healthcare systems in South Africa, namely, the western-based public healthcare system which accounts for approximately 40 million people in the country or 84% of the population who do not have medical insurance; the western-based private healthcare system for 16% of the population who have medical aid; and the traditional healthcare sector. Approximately 80% of the South African population utilize the services of traditional healers, either alone or together with modern biomedical healthcare professionals through the process of medical pluralism (Mendu & Ross, 2019). However, this figure is based on a guesstimate rather than empirical evidence as people are often reluctant to reveal that they have approached traditional healers and the latter usually do not keep written records.
In the South African context, a traditional healer is someone who possesses the gifts of receiving spiritual guidance from the ancestral world (Truter, 2007). A diviner (Sangoma) is a traditional healer who has been called to the profession by an ancestor-sent illness believed to be untreatable by modern or traditional medicine (Truter, 2007). A herbalist (Lugedla, inyanga) is a traditional healer who is said to choose his or her profession, although they may also inherit the skills from their families (Truter, 2007). They use their knowledge and understanding of plants, roots, herbs, and animal products to treat different conditions.
Prior to 1994, traditional healers did not practice openly in South Africa as their practice was prohibited (Mendu & Ross, 2019). However, the use of indigenous healers has since been formally recognized with the promulgation of the Traditional Health Practitioners Act no. 22 of 2007. This legislation represented an important step in acknowledging a medical system that has been an integral part of South African cultural life for centuries (Mendu & Ross, 2019).
Simonds and Christopher (2013) argue that statistics from African countries suggest that in many regions in Africa, 25%–40% of all people seeking medical care related to mental health, tend to approach traditional healers as their first port of call. According to Mufamodi and Sodi (2010), traditional healers are held in high esteem in Southern African societies and play the roles of doctor, psychologist, and priest. Among the reasons for preferring traditional healers is because of dissatisfaction with western health care; personal autonomy in choosing traditional medicine; philosophic congruence with their cultural and spiritual beliefs and practices; and cost-effectiveness (Mpinga et al., 2013).
Mkize (2003, p. 4), a South African psychiatrist maintains that “The African view of mental ill health currently encompasses a wide spectrum – from ancestors, folk belief in witchcraft, to modern medical science.” Healing is based on restoring good relationships between the person, other individuals, and the ancestors in the spirit world, in both the past and the present. He explains that within traditional South African cultures mental illness is incorporated within the social way of life. Consequently, in African medicine, care of persons with mental illness has for decades been relegated to traditional and religious healers who treat mental illness as part of general medical care. Whereas western medicine is concerned with finding out how the person became mentally ill so as to control the symptoms, for African medicine “the question is not how but why things happen” (Mkize, 2003, p. 4). Hence the traditional healer seeks to help patients and their families to understand what the symptoms mean. However, a counter argument against Mkize’s viewpoint, is that biomedical practice is also interested in “why” the help-seeker experiences symptoms. The difference is that traditional healing seeks to understand the “why” questions within a more collectivist framework, including using answers to such questions as focal points for treatment and support regimens.
However, very little is known about the approaches of traditional healers to mental health as their methods remain shrouded in secrecy (Kpobi et al., 2019). Given the limited knowledge of the methods adopted by traditional healers in relation to mental illness, and the high patronage of traditional healing systems, it is important to understand their beliefs and practices in diagnosing and treating mental illness (Kpobi et al., 2019). This paucity of research often contributes to misunderstanding between traditional healers and western healthcare professionals in treating mental illness, which is exacerbated by the fact that they do not usually work together. Hence it is important to understand traditional healers’ views in dealing with mental illness. Furthermore, given the adverse long-term health outcomes of delayed treatment among people with mental illnesses, there is a need to better understand areas for possible cooperation between traditional healers and biomedical healthcare practitioners in the care of such patients (Audet et al., 2017).
For these reasons, the objectives of the study were to ascertain South African traditional healers’: (1) explanations about the meaning of mental illness or why people suffer from mental illness; (2) how they decide whether a person is suffering from mental illness; (3) the methods they employ to treat and (if necessary) prevent mental illness; (4) challenges they experience in dealing with persons with mental illness and their families; and (5) their views regarding collaboration with biomedical healthcare practitioners in the treatment of mental illness. These research objectives were designed to provide an explanatory model of traditional healers’ understandings of mental illness based on psychiatrist and anthropologist Kleinman’s (1995) questions concerning the why, what, and how of illness.
Bubenzer and Litgen (2019, p. 26) state: “Western-centric mental health definitions and solutions still dominate, overshadowing under-researched local traditions, cultures and rituals and preventing the emergence of a more African-centric understanding of mental health.” Hence, the study appeared to fit well with the current discourse on indigenization and Africanisation of healthcare.
Afrocentric Perspectives
The lens guiding the research was the Afrocentric perspective. This perspective considers topics with the viewpoint of African people as participants and agents in influencing their experiences and as participants in any study about them. It seeks to re-locate the African person as a subject and active agent in human history in order to dispel the notion of them occupying a position on the margins of society and an object of Western domination (Asante, 2003) thereby challenging the Eurocentric perspective (Chukwuokolo, 2010). Moreover, African experience must guide and inform all inquiry. Proponents of this framework do not necessarily suggest that Afrocentric views be considered better than others, but rather that African ways of knowing are equally important and should not be dismissed. The experience of enslavement and racism led to the dislocation, self-alienation, disorientation and lack of agency of Afro-Americans, and created the conditions for the genesis of Afrocentric theory (Chawane, 2016). In South Africa, the racism and discrimination experienced by black persons under colonialism and apartheid provided the impetus for Afrocentrism. There are five basic assumptions underpinning Afrocentrism, namely: (1) People, animals, and inanimate objects are all interconnected; (2) A person’s identity is conceptualized as part of a collective, which encompasses a collective responsibility for what happens to others; (3) Mind, body, and spirit cannot be separated and the spiritual component of humans is as important as the physical part; (4) The affective approach to knowledge is considered as valid as the objective empirical approach (Mathebane & Sekudu, 2018); and (5) the Afrocentric perspective emphasizes the importance of location in time and space of the phenomenon being studied (Asante, 2003).
Chipfakacha (1994) believes that all cultures have disease theories that explain the causes of illness. Therefore, in order to comprehend the notion of mental illness one needs to understand the assumptions that influence the cultural value perceptions of people, particularly with regard to concepts of cause and effect. The Afrocentric perspective was regarded as a suitable theoretical framework for the present study, as the aim of the research was to ascertain the perceptions of traditional healers of mental illness, specifically in relation to the meaning of the illness and how it can be treated.
Method
Research Design
The study adopted an interpretivist design (Bhattacherjee, n.d) located within a qualitative approach.
Population and Sample
The target population of this study was both male and female traditional healers who live and practise at Dube village in Soweto, Johannesburg. Purposive and snowball sampling were used to recruit the participants. In terms of purposive sampling, participant selection criteria for recruiting the 14 traditional healers were that they needed to be aged 18 years and older, had been practising their calling for at least 5 years and had experience in treating persons with mental illness. The traditional healers needed to be able to speak at least one of the following languages: isiZulu, isiXhosa, or Sesotho because the first author who undertook the data collection is a black African and could speak these languages. In line with the Afrocentric perspective, Mizock et al. (2011) maintain that researchers of color are more able to bridge the cultural gap with black African participants because of their shared understanding of African realities. The first author conducted the study for degree purposes, while the second author was her research supervisor.
Some healers were recruited from Kwezi in Dube Village where they were known to practise. Others were recruited via snowball sampling whereby participants were asked to assist in identifying and approaching other potential participants. The researcher also attended a ceremony hosted by an elderly traditional healer who lived in close proximity to her home. At the ceremony the host healer acted as gatekeeper and allowed her to approach healers who were present. As a member of the African culture, the researcher was aware of the importance of African greetings as affirmation of a shared spirituality and interconnectedness (Nobles et al., 2016) and therefore greeted the healers respectfully and invited them to participate in her study. She endeavored to further enhance their trust by explaining the purpose and procedures of the study and their rights as research participants. In terms of positionality, the researcher was a young female and endeavored to show courtesy and deference toward the healers who were all older than her and occupied positions of esteem in the community. As several of the healers were Gobelas or teachers of initiates, they understood their obligations as teachers and were open to assisting the student with her research.
Research Instrument
An interview schedule was used as the research instrument for the study. The researcher utilized a combination of closed-ended questions to enquire about biographical details of the traditional healers; and open-ended questions to elicit their views regarding the meaning and causes of mental illness (e.g., Why do you think people suffer from mental illness?); how they identify mental illness (e.g., What signs or symptoms make you think that a person may be suffering from some type of mental illness?) and how they treat mental illness (e.g., What kinds of methods do you use to treat mental illness?); their approaches to prevention, the challenges they experience in dealing persons with mental illness and their families; and their views on collaboration with biomedical healthcare practitioners.
Data Collection
Prior to data collection, a pre-test of the interview schedule was conducted which included an interview with two traditional healers who were not included in the final administration. The pre-test showed that the interview schedule was understandable. Data were collected via individual interviews with participants. Interviews were held in the places where the traditional healers carried out their consultations and each interview lasted from 1 to 2 hours. With the permission of the participants, the interviews were audio-taped and were subsequently transcribed. In addition, since the researcher was conducting face-to-face interviews with the participants she also engaged in observation of the attire of the traditional healers and their use of artifacts such as healers’ whisks and pouches. Interviews continued until 14 traditional healers had been interviewed, at which point it appeared that saturation of codes and themes had been reached.
Consistent with the emphasis in Afrocentric theory on location in time and space (Asante, 2003; Davis et al., 2010), the time period and setting of the study are described. The interviews were conducted immediately prior to the onset of the COVID-19 pandemic and were carried out next to the Kwezi train station in Dube Village where the healers tended to live and be available to consult with community members. Dube Village is part of Dube township in Soweto. The Nguni name “Dube” means zebra. The township was established in 1954 as part of Apartheid planning of separate residential areas for black persons, and is named after John Langalibalele Dube, a popular African leader. While the majority of houses in Dube township are small “matchbox houses” (three-roomed dwellings built by the Apartheid government), the better houses are located in Dube Village. Dube residents comprise all of South Africa’s ethnic groups (Bester, n.d).
The interviews were carried out inside the traditional healers’ place of work, where they do consultations. The healing houses (indumbas) were decorated with animal skins and resembled pharmacies with their wide array of bottles and containers for storing various herbs and animal products. When the researcher approached the first participant, she wore jeans and was told to cover herself with a scarf. She therefore realized that she was expected to wear a skirt or a dress to indicate respect for the traditional healers.
Data Analysis
Data were analyzed using thematic analysis. Braun and Clarke’s (2006) six steps in thematic analysis were followed, namely, familiarization and immersion, producing preliminary codes, identifying themes in the data, re-assessing the themes, creating overall themes, and constructing the report.
Rigor
Efforts were made to increase trustworthiness of the data collection and analysis through consideration of issues of dependability, credibility, transferability, and confirmability. To ensure dependability of the research study the first author conducted all the interviews using a similar set of questions. The research ensured credibility through a detailed description of the research methodology and theoretical frameworks that underpinned the study. Credibility was further enhanced through triangulation of data methods, namely interviews and observations. Transferability was enhanced through thick descriptions of the setting and participants’ responses. Confirmability was assured through correspondence checking whereby the first author checked to see whether her identification of themes corresponded with those of the second author.
Ethical Considerations
Ethical principles that were adhered to in conducting the study included obtaining clearance from the Humanities Human Research Ethics Committee of the University of the Witwatersrand; informed consent; confidentiality; anonymity; voluntary participation; providing feedback to participants; non-deception and non-maleficence.
Participants
The sample was made up of 14 participants who were Black African traditional healers aged 18 years or older. Their ages ranged from 18 to 65 with the five persons aged between 18 and 29 years, five between 30 and 40 years, three between 41 and 50 years, and one in the age group 51 to 65 years. The majority of the traditional healers (n = 10) were male. The sample of healers comprised more herbalists (n = 8) than diviners (n = 5) with one faith healer. The distribution of ethnicity showed that 11 were isiZulu speaking participants, 2 were SeSotho, and 1 was isiXhosa.
During the interviews all the diviners were wearing their traditional healing attire with red and white beads on their heads, arm bangles, and strips of goatskin across their chests. They were also wearing the gallbladder of a goat that was woven into the hair at the back of the head. This gallbladder originates from the goat that was slaughtered to celebrate the healer’s graduation, and it is used to communicate with the ancestors. The most important colors in the attire of healers are white, black, and red. White is associated with light, day, positivity, purity, and health. Black is associated with night, dark, danger, and ill-health. Red is a twilight color between day and night, and is associated with blood and transformation. Red beads represent the healing spirit and are usually worn by initiates who are undergoing transformation, while white beads indicate that one is a graduated traditional healer. They all had cow-tail whisks (lishoba) which signified their dignified status. These objects and amulets serve to augment, protect, and strengthen the healers to withstand the forces around them (Thornton, 2017). While the diviners and the faith healer were dressed in full regalia, the herbalists were simply wearing their casual clothes and arm bangles. All the healers had cell phones which illustrated the influence of modern technology on tradition (Thornton, 2017).
Results
Findings are presented in terms of the five objectives guiding the study.
How the Healers Defined Mental Illness
As indicated by Asante (2003), the Afrocentric perspective focuses on the perspective of African individuals with a view to understanding their principles, encounters, and suppositions. In line with this perspective, participants were asked about their beliefs relating to the meaning and causes of mental illness. Analysis of the participants’ responses revealed that they defined mental illness as alterations in thinking patterns and behavior whereby a person’s contact with reality is disrupted, as reflected in the following verbatim response.
“Mental illness is madness. They do things which normal people don’t do like taking their clothes off in front of people.” [P14 – female diviner]
Explaining the causes or why people experience mental illness
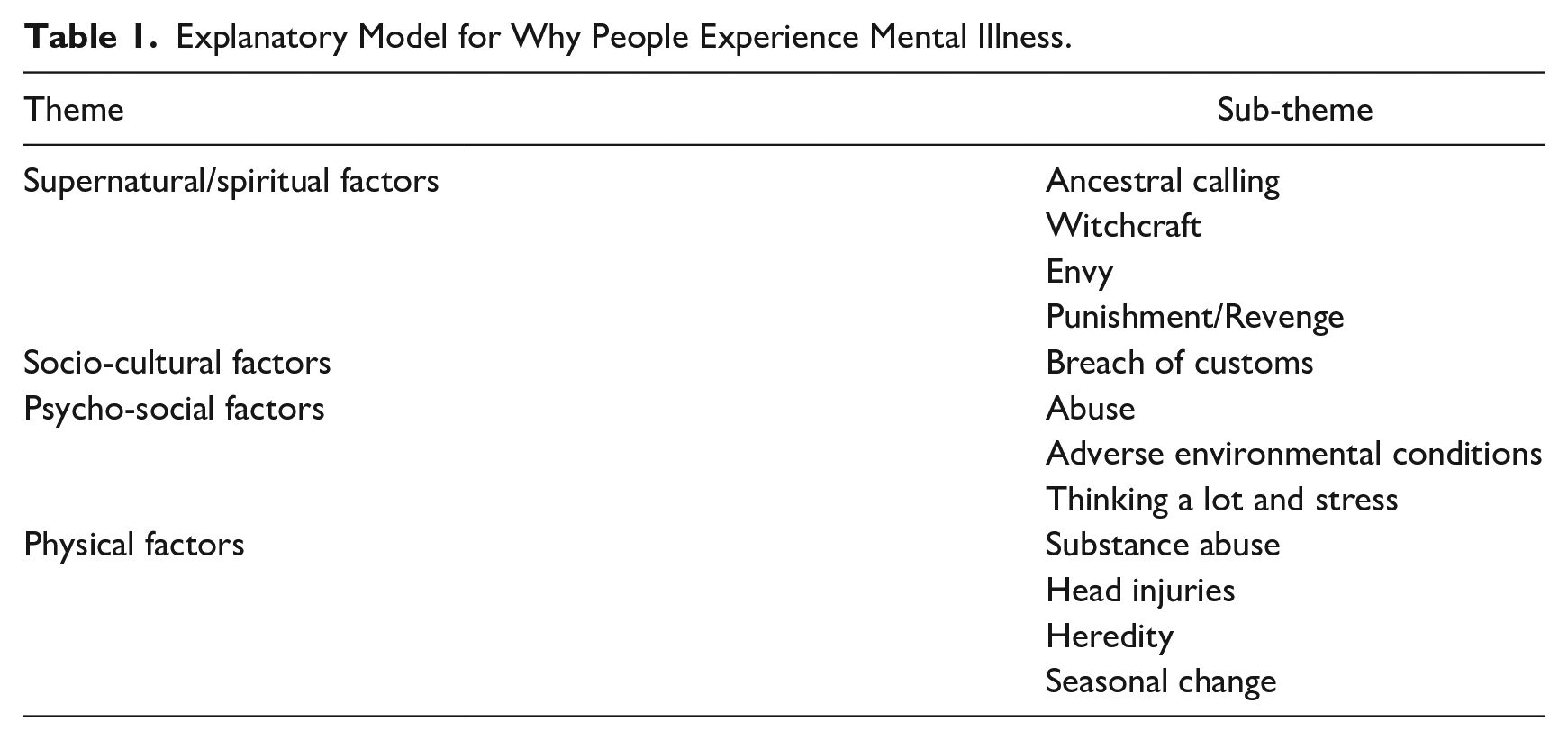
When participants were asked about the causes of mental illness, four themes emerged, namely: spiritual, socio-cultural, psychosocial, as well as physical, with each domain encompassing various sub-themes. A summary of the themes and sub-themes in respect of reasons for mental illness are set out in Table 1.
Explanatory Model for Why People Experience Mental Illness.
Spiritual factors
Participants explained that some mental illness can be a sign of being called by the ancestors to become a traditional healer. This calling may be accompanied by seeing people who have passed away, as well as snakes, trees, rivers, cows, and goats during dreams, as encapsulated in the response: “Some people experience a calling to become traditional healers. Ignoring or refusing the calling can make them become mentally ill.” [P1– female herbalist]
The causes of mental illness were perceived to be closely related to people exercising supernatural powers such as witchcraft and sorcery which can cause misfortunes and illness to be inflicted on others. Alternately, these illnesses could be the result of acts committed by the patient or his/her family. Participants described how jealousy, for example at the success of the victim, can lead relatives, neighbors, or friends to use witchcraft to inflict illness, disease or bad luck on the person. “People in your community can sometimes get jealous of the success because they cannot compete with you then they make you mad.” [P9 – male faith healer]
Socio-cultural factors
African communities are governed by certain codes of moral ethics and neglect or breach of customs was identified as a socio-cultural factor contributing to mental illness. According to the findings from this study, if a person ignores or does not uphold his or her cultural customs, their mental health can be adversely affected. “If someone in the family dies there must be a period of mourning. If you do not abide by the mourning rituals then the ancestors can make you sick – either mentally or physically. Also, having sex on the bed of a person who has recently died is taboo.” [P3 – male herbalist]
Psycho-social factors
Findings revealed that the experience of emotional or physical abuse can cause mental illness. The following quote reflects this theme: “Children, who are regularly beaten, raped as well as those whose parents may have died when they were young children can develop mental illness and that is why people should not always shout and hit children. A child that is always shouted at can develop mental illness.” [P4 – female diviner]
Social stressors such as poverty, unemployment, and family tensions were believed to lead to the development of mental illness. “Long-term poverty has harmful effects which can cause mental illness.” [P2 – male herbalist]
Participants believed that thinking a lot can cause disruptions in one’s thought patterns and behavior. It can interfere with brain functions, resulting in symptoms of mental illness like talking allowed to oneself. According to the participants, suicide was not uncommon for people with untreated mental conditions. “In some cases, the stress of discovering that one has HIV or AIDS, may come as such a shock that the person becomes mentally disturbed. They may even try to kill themselves.” [P3 – male herbalist]
Physical factors
Physical causes of mental illness mentioned by the healers included substance abuse (particularly marijuana and alcohol), head injuries, and other medical conditions. According to participants, mental illness frequently occurs among persons who are dependent on drugs and/or alcohol which can cause chemical dysfunction in the brain. “I think with my own understanding it is caused by these things now people smoke like marijuana, drugs. But before the drugs it was marijuana and they will explain in the family not to use it because traditionally no one in the family should be smoking weed. If you do you can go crazy.” [P4 – female diviner]
Findings indicated that people who sustain head injuries from motor vehicle accidents, assaults, or falls, may undergo changes in brain functions. The following quote illustrate this sub-theme: “Head injuries from car accidents often causes people to suffer mental illness.” [P1 – female herbalist]
A common belief among participants was that some people with a family history of mental illness have a genetic predisposition to developing mental illness.
“If one is from family with a history of mental illness, one has a greater likelihood of getting it as well.” [P3 – male herbalist]
Participants expressed the view that the changing of seasons can cause mental illness in some people because their bodies are unable to handle or cope with a season, particularly summer.
“To some people changing of the season causes mental illness especially summer is a dangerous season to some people, because their body cannot cope with it.” [P5 – male diviner]
Analysis of the spiritual, socio-cultural, psychological, and biological factors in the etiology of mental illness shows the holistic approach adopted by the traditional healers in the study. Such an approach is in line with the Afrocentric perspective.
How traditional healers decide whether a person is suffering from mental illness
The themes that emerged in respect of the manner in which traditional healers diagnose mental illness are summarized in Table 2.
How traditional healers determine whether a person is mentally ill.
The study revealed that those participants who were diviners used their bone throwing skills to consult with their ancestors to determine the reasons for of the sickness. After several throws they scrutinize the lie of the bones and then spell out a clear message about the illness of the person. This theme was reflected in the following verbatim response: “I use bones to ask the ancestor to guide me and give me answers about illness; they help me to see if I can be able to help a patient.” [P3 – male herbalist]
Both diviner and herbalist participants observed the behavior of the mentally ill person to determine whether the person was suffering from a form of mental illness. Participants maintained that mentally ill persons usually display anti-social behaviors like inexplicable screaming, crying and laughing, self-mutilation, wandering around aimlessly, refusing to wash, wearing the same dirty clothes, collecting refuse, sleeping and hiding in the bushes, saying things that do not make sense, and showing confusion, which they identified as manifestations of mental illness. “They are not themselves anymore. Some they become violent and they don’t want anything to do with getting help. . . those who were bewitched, they fight.” [P9 – male faith healer]
In addition, the participants reported that they usually tried to gather as much information as possible on current symptoms from the family and the ill person when making a diagnosis. They would then try to gain a comprehensive understanding of the individual’s psychological context in order to understand what might be causing the current symptoms. “I don’t ask the patient; however, I ask people who came with a patient. They usually don’t bring themselves. I know that it is them who know about the patient illness, family roots, if they can be able to fix some of family problems as the bones translated. Then after you come back to me, I will start to use traditional medicine to treat a patient.” [P4 – female diviner]
Treatment of Mental Illness
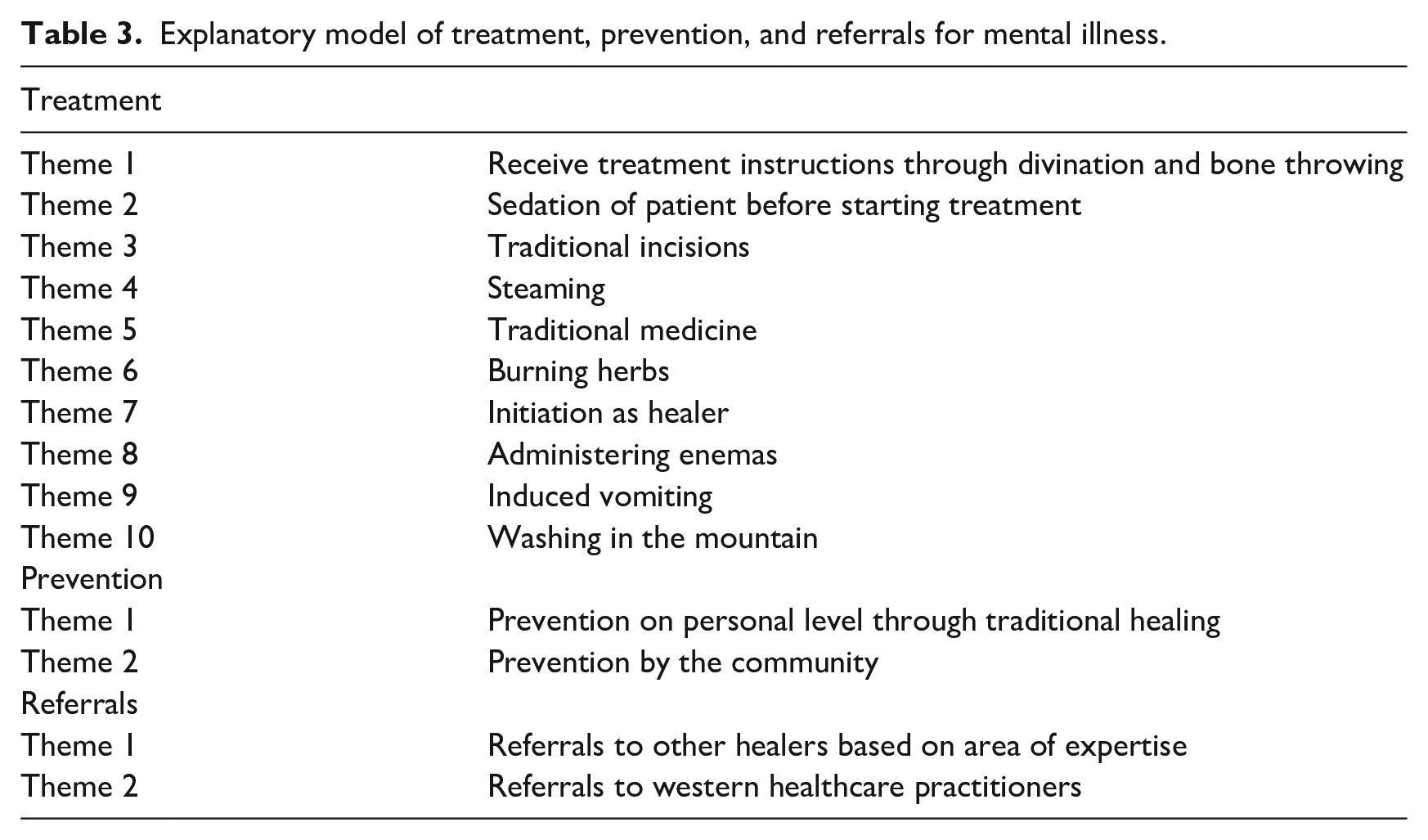
Table 3 summarizes the themes that emerged with respect to the treatment and prevention of mental illness and the referrals of persons concerned.
Explanatory model of treatment, prevention, and referrals for mental illness.
The study findings suggested that the core function of traditional healing centers on ancestor reverence. Divination through bone throwing enabled them to obtain instructions from the ancestors on treatment approaches. “Ancestors show me what sort of treatment I should follow.” [P9 – male faith healer]
As some patients are violent and aggressive, six healers reported that they utilized traditional medicine to calm and sedate patients before starting therapy. “I use traditional medicine I put it into his/her nose. I put it with water, then the mind will come before I can start doing anything.” [P7 – male herbalist]
In some cases, an incision is made in the patient’s skin to allow the illness causing substance to be dispelled from the body, as reflected in the following quote: “The bad blood must come out of the person, to allow the body to heal. That is why I sometimes incise them.” [P4 – female diviner]
Steaming was perceived as a way of cleansing the body and ridding it of evil substances. “It depends on the level of the illness. If it is moderate I use mixtures of medicinal herbs. I boil them, then the steam will be inhaled, and the body is washed. It’s a way of cleansing the person and dispelling evil forces.” [P6 – male herbalist]
All the participants reported using muti (traditional medicines) which were usually derived from a variety of medicinal herbs, bulbs and roots from plants, and animal derivatives.
“Once the person has been given the different treatment methods, he or she is given medicine.” [P5 – male diviner]
Burning of herbs was found to be efficacious in the treatment of illness. This practice was used to instill an atmosphere of peace and harmony, and for purifying, cleansing, and protecting people’s physical and spiritual bodies and expelling evil substances. It was also believed to stimulate the brain and help it to function optimally. “In some instances, the patient is asked to breathe in the smoke from herbs that have been burnt. It’s a type of ritual to make the patient stronger and remove evil spirits.” [P5 – male diviner]
According to the traditional healers, those persons presenting with symptoms of mental illness which was the result of a calling to become a traditional healer would only recover once they had accepted the calling and undergone the relevant training. “If the person does not heed the calling it will cause further illness until the person accepts their fate and goes for training.” [P6 – male herbalist]
The healers stated that sometimes an enema needed to be given to patients to cleanse the body and remove evil intrusions, as indicated in the following response: “An enema is used to flush out evil spirits. I do myself because they can’t do it.” [P7 – male herbalist]
In some instances, medicine is used to induce vomiting, through which the evil intrusions are cleansed or washed away. “In cases of food poisoning, I give the patient a mixture of herbs to make them vomit and rid themselves of evil substances.” [P7 – male herbalist]
The traditional healers explained that some conditions can be cured through the performance of certain rituals like bathing the ill person in the mountain, particularly parts of a mountain that are regarded as sacred. “I use herbs which is mixed with water to bath the mentally ill person, but it depends on the illness. If it’s severe then I usually bath them. It’s like a cleansing ceremony.” [P9 – male faith healer].
Preventing Mental Illness
The participants were of the opinion that it is possible to prevent the mental illness especially in those who are bewitched, if people can stop being jealous, refrain from stealing or killing each other and if people can care for one another. They also maintained that mental illness can be prevented if people can stop abusing substances, and talk to one other if there is something bothering them. Hence the notion of prevention was revealed by participants in two themes namely, the personal level through traditional healing and through the community.
The following quote illustrates prevention of mental illness through traditional healing: “It depends on the person’s luck because I usually have a vision or a message before it happens. Then I will tell that person those who take me seriously. I help them by telling them what to do to prevent because my ancestors will tell me everything.” [P9 – male faith healer]
The following response illustrates prevention of mental illness by the community: “People should stop abusing children, men they stop abusing their wives.” [P13 – male herbalist]
Referrals
All the healers reported that they refer patients to relevant persons who can address their specific needs. Referral to other traditional healers may be made on the basis of areas of expertise. “As healers we specialised in different areas. When I feel that I cannot help the patient I send them to the healer who has the expertise to deal with the problem. Some of us are only specialising on herbs and some throw bones so we cannot do it, our practice differs.” [P8 – male herbalist]
According to the participants in the study, every illness requires a different treatment. Some illnesses are only treatable by traditional healers while others can only be treated by western biomedical doctors. “I refer them to hospital when I want them to go and get energy because in hospital they can give them drip, I mean water. They rehydrate them and they will return with more energy. I will then begin treatment.” [P3 – male herbalist].
Challenges in dealing with persons with mental illness and their families
Themes in respect of problems in dealing with persons with mental illness and their families are summarized in Table 4.
Challenges for traditional healers in dealing with persons with mental illness and their families.
According to the traditional healers who were interviewed, treating a person with mental illness is a very challenging job as a healer and they cannot do that alone. The two themes that emerged were problems handling a person with mental illness, and problems emanating from the family of the ill person.
Challenges in dealing with a person with mental illness
According to the participants who were interviewed, a person with mental illness often presents with violent and destructive behavior which is difficult to control. “If I am treating a mentally ill person, I invite people to come and help me to tie him or her up because they can beat you like nobody’s business and you cannot do anything alone because they usually have much power. Hence they are being entered by evil spirit.” [P9 – male faith healer]
Another challenge is refusal to accept treatment and medication. “They don’t take medicine by themselves. You have to force them and I make sure that I don’t leave medicine where they can see because they dispose it and it is difficult and expensive to get other herbs.” [P10 – male herbalist]
Problems with the families of persons with mentally illness
Analysis of participants’ responses revealed three themes. The first theme was problems with payment. “Payment problems. You help the person, when the person is feeling better, they don’t pay the full payment that you agreed on.” [P10 – male herbalist]
Some families brought the patient to the healer and then abandoned him or her. “Lack of support from the family. They leave the person with you and they don’t come back to check.” [P5 – male diviner]
One of the very important responsibilities of family members and society is support, which was reported to be a challenge to traditional healers. “Conflict in the family when they are blaming or pointing fingers to other family members.” [P1 – female herbalist]
Collaboration with biomedical healthcare practitioners
Nine participants expressed the opinion that working together with western practitioners would be a good idea because the latter have a lot to offer that traditional healers do not have and that can help in providing for the well-being of people, which is a priority for them. For example, one person commented: “I think that would help because we need hospitals to sedate them because their behaviour is uncontrollable and they also help by giving them energy and water through drip.” [P3 – male herbalist]
However, five participants disagreed with the idea of working together. This viewpoint was supported by the following verbatim quote: “It will never work out. Because what I’m using, for example my traditional medicine they will kill it with their chemicals and turn them weak and cause it to unable to work as strong as it should be.” [P11 – male diviner]
Discussion
Results are discussed in relation to the objectives of the study.
Defining Mental illness
A surprising finding was that the traditional healers’ ways of conceptualizing mental illness were similar to the World Health Organization’s (WHO, 2017) definition of mental illness as alterations in thought patterns and behavior that have the effect of individuals losing contact with reality. The findings from the present study were also consistent with findings of earlier studies, for example, research by Mufamodi and Sodi (2010), Ngobi (2015), Sorsdahl et al. (2010), and Teuton et al. (2007). These researchers found that traditional healers used psychotic illness as an example of mental illness. Similarly, in the present study the traditional healers tended to equate mental illness with populist notions of “mad” or “insane” people.
Why people experience mental illness
When participants were asked to explain the causes or why people experienced mental illness, four themes emerged, namely: supernatural/spiritual (ancestral calling and witchcraft), socio-cultural (breach of customs), psycho-social (abuse, adverse environmental conditions, thinking a lot, and stress), as well as physical (substance abuse, head injuries, heredity, and seasonal change).
Consistent with the spiritual viewpoint that ancestral calling can cause mental illness, Schweitzer (1997) maintained that ukuthwasa or ancestral calling is associated with illness and spiritual and emotional breakdown. Therefore, refusing to accede to the calling by the ancestors can lead to mental illness or even death. The implication of this finding is that from the perspective of traditional medicine, ukuthwasa cannot be treated if the affected person does not submit to the arduous process of becoming a healer. Such a condition is also not treatable by biomedicine. In line with the findings that witchcraft was believed to cause mental illness, Thabede (2005) emphasizes the need to acknowledge that beliefs in witchcraft are part of the African worldview.
The socio-cultural finding regarding breach of customs causing mental illness is supported by Ngobi (2015) who argues that following the neglect of cultural practices, the individual has to own this guilt and follow through with certain rituals in order to be absolved from wrong doing. Crawford and Lipsedge (2004) posit that ancestors play the role of protecting the living from illness and harm. Therefore, if the individual neglects to fulfill certain rituals the ancestors may withdraw their protection which may result in adverse outcomes. In a similar vein, Kirmayer (2006) indicates how cultural psychiatry and medical anthropology involve “showing the ways in which a medical symptom, diagnosis or practice reflects social, cultural and moral concerns” (p. 127). These findings highlight the value attached to cultural beliefs and rituals as emphasized in the Afrocentric perspective, and how failure to adhere to cultural rituals adversely affects the person and results in psychological distress.
In terms of psycho-social factors and in line with the theme on abuse, Abramsky et al. (2011) maintain that mental health consequences of intimate partner violence can be very severe to the extent that they may cause posttraumatic stress disorder (PTSD), depression, panic and anxiety attacks, and eating disorders. In accordance with the social causation hypothesis, adverse environmental conditions such as poverty exacerbate the likelihood of mental illness through heightened exposure to financial stress, family tensions, social exclusion, food insecurity, violence, trauma, and increased obstetric risks (Flisher et al., 2007). Stress also exerts an impact on the onset and course of psychiatric disorders (Lee & Ham, 2013). It is of interest that the finding of “thinking too much” was also noted by Kaiser et al. (2015) in their review of idioms of distress in 138 studies from a wide range of countries across the globe. Thinking too much is defined as “a preoccupation with a negative situation in such a way as to subsume one’s being with negative mood and affect” (Hatala & Waldram, 2016, p. 65) and is one of the nine cultural concepts of distress in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5, American Psychiatric Association, 2013, pp. 834–835). These findings highlight the links between traditional healing and biomedicine.
In relation to physical factors, and consistent with the belief that mental illness is common among persons who are dependent on drugs and/or alcohol, Koob (2006) asserts that heavy alcohol consumption directly affects neurotransmitters in the brain and hormonal systems known to be associated with the development of mental health conditions such as mood and anxiety disorders. Patients with traumatic brain injury usually exhibit at least one or more of the following symptoms: memory loss for events before or after the onset of the injury; disorientation or loss of consciousness, posttraumatic brain-related physical symptoms, and cognitive shortfalls (Kolb & Whishaw, 2008) and psychiatric symptoms such as depression, anxiety disorders, mood disorders, and schizophrenia (Rogers & Read, 2007). In line with the belief that some people have a genetic predisposition to developing mental illness, Hyman (2000) argues that mental illness is known to run in families. Thompson et al. (2018) provide support for the belief that seasonal change can cause mental illness, based on the fact that higher ambient temperatures and heat waves have been found to be associated with increased suicide risks and increased risks of mental health-related admissions and emergency department visits. These findings again emphasized the similarity between beliefs held by traditional healers and those subscribed to by western healthcare practitioners.
While the spiritual and socio-cultural factors perceived to cause mental illness, such as witchcraft and the calling sickness highlight the influence of African cultural ideas and practices, the findings in relation to psycho-social and physical factors such as adverse social conditions, drug abuse, head injuries, and heredity suggest the possible influence of ideas from biomedicine on the traditional healers who were interviewed. In this regard, Asante (2003) insists that Afrocentrists are not afraid to draw from other cultures. In a similar vein, Thornton (2017) states that traditional healers glean from other healing practices in their environment, including the biomedical. Waldram (2000) maintains that the use of biomedical language by traditional healers is not surprising in a postcolonial era of globalization, but cautions that the use of these terms does not necessarily equate to comparable biomedical understanding. Moreover, the “use of supposed English language equivalents often leads to the erroneous belief that traditional medicine is inherently similar to, and therefore testable by biomedicine” (Good, 1994, cited in Waldram, 2000, p. 808). The search for biomedical parallels in traditional healing can also lull us into a false sense of our ability to assess the efficacy of traditional medicine (Waldram, 2000). Nevertheless, these “windows of compatibility” between these two medical systems can provide focal points for discussion and collaboration (Hatala et al., 2015) and have important implications for mental healthcare in settings such as South Africa.
Diagnosis
Although participants did not use the term “diagnose,” it emerged that the one male faith healer (Participant 9) used prayer and candles to help him to understand the patient’s illness, while diviners used their bone throwing skills and consultation with the ancestors to determine the cause of the sickness and the way in which it should be treated. The traditional healers who were interviewed also used observations of physical symptoms presented by the patient as a way of determining the problem, especially the herbalists who are unable to predict or throw bones as are the diviners. In a similar vein, Sodi et al. (2011) noted that Tsonga herbalists in South Africa used observation. Herbalists mentioned that they interviewed the patient and his/her relatives prior to reaching a conclusion on the specific nature of the illness. These results suggested a holistic approach emblematic of the Afro-centric perspective and which combined supernatural methods with practical methods employed by biomedical professionals such as observations and history-taking.
In biomedicine, diagnosis primarily involves determining the nature and cause of a disease or illness and its categorization within a body of known conditions through bodily and behavioral clues (Hatala & Waldram, 2017). Biomedical practitioners consider the narrative or ordering or events related to an illness episode with an overarching plot structure. Emplotment is the term used by Hatala and Waldram (2017) to denote the way in which this succession of events is configured into a broader story. While South African traditional healers in the present study considered bodily and behavioral clues, like the Q’eqchi Maya healers in Belize in South America (Hatala & Waldram, 2016), they also drew on additional cosmological or spiritual forces to plot the illness narrative, which is consistent with the Afrocentric perspective. Similarly, Sow (1980) conceptualized African reality as made up of three interrelated worlds consisting of the immediate perceptible world (the microcosmos); the intermediate world of spirits and beneficial or malevolent forces (the mesocosmos); and the world beyond the senses, the realm of ancestors and spiritual beings (the macrocosmos). This conceptualization resonates with the idea put forward by Nobles et al. (2016) of a community of living beings (mesocosmos), the yet-to-be born and the living-dead (macrocosmos). Being disconnected from one’s spiritual world is believed to cause spirit-related illnesses. From these findings one can conclude that while there are significant differences, particularly in relation to spiritual aspects, there are also many similarities between South African traditional healing and biomedicine in terms of pathways to arriving at a diagnosis.
Treatment, Prevention, and Referral
Treatment approaches took the form of cleansing the patient and flushing out evil spirits through inhalation of steam or smoke from burnt herbs, administering enemas, inducing vomiting, making traditional incisions, performing rituals, and prescribing various traditional medicine. Other measures included sedation, referral, and initiation as a healer. It is of interest that traditional healers and western practitioners tend to use sedation to reduce irritability or agitation of the patient. de Villiers and Ledwaba (2003) explain that traditional healers also use incisions or what they refer to as vaccinations, to remove poisonous substances from the patient’s body through the use of razor blades to make small cuts on the body surface of a person onto which a powerful medicine is rubbed. However, they caution that some of these methods may have negative implications. For example, some persons can be harmed from the application of ointments on fresh scarifications, and some persons can also develop liver and kidney damage due to some herbal toxins. According to Sorsdahl et al. (2010), another approach to treating mental illness involves burning herbs and placing them next to the person with mental illness so that he/she will inhale the fumes. It is a form of treatment that is believed to stimulate the brain and make the patient return to his/her normal state of mind. The use of herbs is in line with Afrocentric assumption of the interconnectedness of people and plants in the environment. In some cases, an enema needed to be administered to cleanse the patient’s body and remove evil intrusions. Some medicine is used to induce vomiting through which the evil intrusions are washed away. However, the risks involved in such cleansing practices is that they may reduce the effectiveness of some biomedical treatments by, for example, purging antiretrovirals from the bloodstream of persons living with HIV. The finding regarding washing the person in the mountain was consistent with those documented by Sodi et al. (2011) who found that traditional healers often utilize herbal baths and steam inhalants as a method of banishing the evil spirits that caused the illness.
The notion of prevention occurred on two levels, namely, the personal level through traditional healing and through the community. Reducing the use of substances was articulated by participants as the way of preventing mental illness and this recommendation is supported by WHO (2004). Healthy, appropriate, and caring relationships with others was expressed by the participants as another way to prevent mental illness. In this regard, Arango et al. (2018) maintain that positive relationships with other people can make individuals feels secure and valued members of their community. This viewpoint would seem to be in line with the African value of Ubuntu (community solidarity). It is also in line with the Afrocentric approach that privileges a model of healing where the individual is not isolated but is critically linked to a larger social and cultural collective and “goes beyond the individualistic and pathology driven paradigm of Western psychology” (Nobles et al., 2016, p. 54).
All the healers explained that when they are unable to assist patients, they refer them to people who have the necessary expertise or when they seek help from western doctors. Sorsdahl et al. (2013) found that traditional healers who held more favorable attitudes toward Western healthcare practitioners and believed that their practices were useful in some way because they provided treatments such as a drip to dehydrated patients, were more likely to refer their patients. This finding holds important implications for possible collaboration between traditional healers and biomedical practitioners.
Challenges
Challenges confronting traditional healers included problems emanating from the family and problems dealing with the person with mental illness. They reported that some families do not support the ill person, abandon the patients, and fail to pay for the treatment. Another challenge is religion as some families do not believe in traditional healing so they will oppose the treatment. Participants reported aggressive, violent and destructive behavior on the part of patients, and refusal to accept treatment. Consistent with this finding, Pompili et al. (2017) claim that aggressive behavior has been noted in certain serious mental illnesses, which can lead to violence and harm perpetrated against other persons. These findings suggested that the traditional healers had experienced similar challenges to western practitioners in the treatment of mental illness.
Views on Collaboration With Western Health Practitioners
A surprising finding was that the majority (9) of the participants who were interviewed favored working together with western practitioners because western practitioners can offer services that traditional healers do not have and that can help in enhancing wellbeing of people which is a priority for both groups of practitioners. This finding was in line with the Afrocentric idea that the reconstruction of post-colonial African cultures needs to involve a synthesis of both African and European contributions to humanity (Verharen, 2000). Moreover, given the preference of many South Africans for traditional medicine, its integration with western biomedicine could potentially contribute to realizing the right to equity in mental health care through its availability, accessibility, cultural acceptability, and relative quality (Mpinga et al., 2013). Nevertheless, the call for integrative healthcare needs to be more nuanced than simply calling for collaboration. Kpobi and Swartz (2018, p. 5) maintain that we need to “know more about who, and from which groups, would wish to work together for mental health, and for which reasons.” Questions of place, power and legitimacy are important components of any discussion on collaboration. However, five participants disagreed with the idea of working together, due to lack of understanding between these two healing modes and the fear of being used and of having their medicinal knowledge appropriated. Consistent with these findings, Mendu and Ross (2019) found that the traditional healers in their study were reluctant to engage in collaborative relationships with biomedical professionals for fear of being denigrated and having their medicinal knowledge stolen. According to Sodi and Bojuwoye (2011), the challenges to integrated healthcare are related to epistemology, practice, attitudes, and research. They argue that these constraints can be overcome through education, training, and collaborative research.
Limitations and Conclusions
While generalization is usually not an issue in qualitative research, it needs to be acknowledged that the use of a small, non-probability sample does not allow the findings to be generalized to the broader population of traditional healers in South Africa who offer services to persons with mental illness and their families. A second limitation is that while the study would seem to have lifted some of the secrecy surrounding traditional healers’ management of mental illness, participants may still have been reluctant to divulge some aspects of their knowledge and practices. A third limitation is that only single interviews were conducted with each of the healers.
However, despite these limitations, important conclusions can be drawn. The study revealed that African traditional healing is inextricably intertwined with spirituality. In contrast, Western healthcare practitioners conceptualize mental illness from a biopsychosocial model that pays minimal attention to spirituality. It would seem that African traditional healers play a significant role in managing mental illness by considering the context and by providing an explanation for the illness or answering the “why question” from a collectivist perspective. In this regard, the words of Kwende et al. (1997, p. 87) are particularly apposite: “. . .in many cases Africans are interested in the why of things. They want to know why this happened to me specifically, why it happened at this particular time, in this particular place.” The South African traditional healers who participated in this study would seem to have made an important contribution by providing an explanatory model of mental illness and its treatment from an Afrocentric perspective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.