
Abstract
The present study investigated the associations between self-construal, acculturation, and autonomy–connectedness, as well as the relations between autonomy–connectedness and psychopathological symptoms, controlling for self-construal and acculturation. Participants were 1,209 Dutch individuals, of whom 693 (57.3%) were immigrants with a non-Western background. Results showed that an independent self-construal was positively associated with self-awareness and capacity for managing new situations, and was negatively associated with sensitivity to others (which are the three components of autonomy–connectedness). Moreover, an interdependent self-construal was negatively associated with self-awareness and capacity for managing new situations, and was positively associated with sensitivity to others. Importantly, the latter associations were similar for both Dutch natives and immigrants, and the associations between acculturation and autonomy–connectedness were small and nonsignificant. Autonomy–connectedness, after controlling for self-construal and acculturation, explained a large amount of additional variance in anxiety (12.7%) and depression (14.1), and a medium amount of additional variance in drive for thinness (3.7%) and bulimia (4.8%). Autonomy–connectedness, thus, seems to be an important construct for people with a Western background, as well as for immigrants with a non-Western background.
Autonomy–connectedness is the ability for self-governance under the condition of connectedness to others (Bekker, 1993; Bekker & van Assen, 2006). The classical conceptualization of autonomy one-sidedly emphasized independence and separation (e.g., Erikson, 1968). Healthy psychological functioning, however, requires an intricate balance of self-governance and synchronizing one’s behavior with that of others. According to Bekker (1993), connectedness to others, therefore, is a prerequisite for autonomy and should be part of its definition. The more modern concept autonomy–connectedness, thus, both entails the ability to be aware of and being able to realize one’s goals and the ability to synchronize one’s own needs to those of others.
Autonomy–connectedness is informed by attachment theory (Bowlby, 1969, 1973) and a neoanalytical object-relation theory on the development of gender identity (e.g., Chodorow, 1989). Healthy autonomy stems from secure attachment experiences. Importantly, although attachment and autonomy–connectedness are related, they are not confounded (Bekker & Croon, 2010). More specifically, whereas insecure attachment styles reflect ways of coping with insecure attachment experiences, autonomy–connectedness deficits primarily reflect the resulting deficits in the self and its steering capacity (Bekker, 1993).
According to Chodorow’s neoanalytical object-relation theory, autonomy develops differently in boys than in girls (e.g., Chodorow, 1989). The integration of her feminist neoanalytical object-relation theory with attachment theory makes autonomy–connectedness a gender-sensitive construct (Bekker, 1993). This gender sensitivity is, among other things, reflected by women consistently scoring higher than men (Bekker & van Assen, 2006; van Assen & Bekker, 2009) on one of the components that autonomy–connectedness is composed of: sensitivity to others. Sensitivity to others reflects sensitivity to the opinions, wishes, and needs of other people; empathy, as well as the capacity and need for intimacy.
The other two components of autonomy–connectedness are self-awareness and capacity for managing new situations (Bekker, 1993; Bekker & van Assen, 2006). Self-awareness is the capacity to be aware of one’s own opinions, wishes, and needs, and the capacity to express these in social interactions. The component of self-awareness is closely related to sensitivity to others. That is, not being aware of and expressing what one wants and needs may result in overreliance on the needs and wishes of others. Overly relying on the needs and wishes of others may then, in turn, hamper the development of self-awareness.
Capacity for managing new situations lies less at the core of autonomy, but follows from the importance of secure attachment in developing a healthy autonomous self. Capacity for managing new situations comprises of feeling at ease in new situations, flexibility, an inclination to explore, and not needing to depend on familiar structures. It reflects the drive to explore that follows from secure attachment (Bekker, 1993).
Taken together, autonomy–connectedness deficits are characterized by high sensitivity to others together with low self-awareness and a low capacity for managing new situations (Bekker, 1993; Bekker & van Assen, 2017). Indeed, research within Western cultures has shown that this autonomy–connectedness pattern (high sensitivity to other, low self-awareness, and low capacity for managing new situations) is associated with various types of psychopathology, such as anxiety (e.g., Bekker & Belt, 2006), depression (e.g., Burke & Haslam, 2001), and eating disorders (e.g., Kuipers, Hollander, van der Ark, & Bekker, 2017), as well as with milder types of psychological problems, such as work–home interference and work stress (Bekker, Willemse, & De Goeij, 2010). However, the association between autonomy–connectedness and mental health has not been investigated outside of Caucasian Western groups.
Self-Construal and Acculturation
Although autonomy–connectedness reflects independence and interdependence on a psychological level, self-construal reflects the view of the self in relation to the collective (Markus & Kitayama, 1991) on a cultural level. According to Markus and Kitayama, there are two distinct, independent versus interdependent, forms of self-construal. Interdependent self-construal is characterized by intense relatedness of individuals to each other, whereas individuals with independent forms of self-construal seek to maintain their separation from others. These forms of self-construal should be viewed as two related dimensions (e.g., Singelis, 1994), as cultures are never entirely individualistic or collectivistic (e.g., Allik & Realo, 2004). Indeed, similar to the fact that connectedness to others is a prerequisite for autonomy in the concept autonomy–connectedness, individualistic and collectivistic cultural values coexist and complement each other. For example, people who live in a collectivistic culture cannot be considered to lack autonomy, just as people adhering to individualistic cultural values, which stress independence, nevertheless, do value relatedness and connectedness to others (Kagitcibasi, 2005).
Integrating self-construal and autonomy–connectedness, we expect that an interdependent self-construal would be related most strongly to sensitivity to others, as belongingness and loyalty to others is central to both constructs. Independent self-construal might especially relate to self-awareness, as both constructs reflect a focus on individual needs, choices, decisions, and interests. Next to self-construal, when studying immigrants, acculturation (adaptation to the host culture and maintenance of the culture of origin) is also important to take into account.
Therefore, Bekker, Arends-Toth, and Croon (2011) investigated the associations between autonomy–connectedness, self-construal, as well as acculturation in Dutch immigrants from Turkish and Moroccan descent and Dutch natives. In the immigrant group, they hypothesized a positive association between sensitivity to others and maintenance of the culture of origin, as well as a positive relation between adaptation to the Dutch culture and self-awareness, as the immigrants moved from a more collectivistic to a more individualistic culture. In line with expectations, Bekker et al. (2011) found positive associations between an independent self-construal and self-awareness in the immigrant group, 1 and between an interdependent self-construal and sensitivity to others in both groups. An independent self-construal was furthermore associated with greater capacity for managing new situations, likely reflecting a positive acculturation process.
Not in line with expectations, Bekker et al. (2011) found that higher scores on sensitivity to others were associated not only with maintenance of the culture of origin but also with adaptation to the Dutch culture. Also not in line with expectations, immigrants were found to score lower on sensitivity to others than Dutch natives. Bekker et al. explain that this could be due to the difficulty of balancing two cultures: On one hand, immigrants may want to adapt to their new culture, but on the other hand, they may also struggle to live up to or be loyal to the values of their culture of origin and family members (e.g., Rodriguez, Myers, Bingham Mira, Flores, & Garcia-Hernandez, 2002). No significant relations between adaptation to the Dutch culture and self-awareness or capacity for managing new situations were found.
The Present Study and Hypotheses
The first aim of the present study was to replicate and expand Bekker et al.’s (2011) findings in a larger group (N = 1,209), both men and women, consisting of Dutch natives and immigrants from various backgrounds who are more representative of the Dutch (immigrant) population. As already discussed, women have been shown to consistently score higher than men on sensitivity to others (e.g., van Assen & Bekker, 2009), which is often explained by differences in the development of gender identity in childhood (e.g., Chodorow, 1989). For this reason, and also because men and women might have different roles in various cultures, we explicitly included sex as a principal predictor in our models.
Bekker et al. (2011) made important first steps in showing that autonomy–connectedness is a useful concept in a multicultural context, but they did not investigate its associations with psychopathology, shown only within Caucasian Western contexts. Our second aim, therefore, was to investigate the relation between autonomy–connectedness and psychopathological symptoms in immigrants compared with Dutch natives, controlling for self-construal and acculturation. Because self-construal likely shares a significant amount of variance with autonomy–connectedness, as does acculturation with psychopathological symptoms, we used hierarchical regression analysis to investigate how much variance was explained by autonomy–connectedness, after controlling for self-construal and acculturation.
In line with previous research, we focused on symptoms of anxiety, depression, and eating-related psychopathology. The reason the literature has paid so much research attention to anxiety, depression, eating-related psychopathology, and antisocial behavior 2 is that these problems are characterized by large sex differences, which have shown to be mediated by autonomy–connectedness sex differences (Bekker & van Assen, 2017).
Regarding our first aim, in both groups we expected the following:
With regard to acculturation of the immigrants, we hypothesized the following:
Regarding our second aim and in line with previous literature (e.g., Bekker & Belt, 2006; Burke & Haslam, 2001; Kuipers et al., 2017), we expected the following:
As the association between autonomy–connectedness with mental health for other than Caucasian Western groups is still largely unknown, we explored differences between Dutch natives and immigrants by using ethnicity as a moderator in our analyses.
Method
Participants and Procedure
Participants were 1,209 individuals of whom 693 (57.3%) had a non-Western immigrant background: Indonesia: 144 (11.9%), Morocco: 113 (9.3%), Turkey: 96 (7.9%), South Africa: 83 (6.9%), Surinam: 74 (6.1%), and Dutch Antilles: 68 (5.6%). Immigrants from Western societies (N = 115) were excluded. Indonesian immigrants were also excluded from the main analyses because this group could not be clustered with the other groups of immigrants (see “Group Differences” section of the “Results” section). This left us with a total sample of 516 Dutch natives and 549 immigrants. In the present study, immigrants were defined as people who were not born in the Netherlands, or from whom at least one parent was not a Dutch native.
Data were acquired with use of the Longitudinal Internet Studies for the Social Sciences (LISS; www.lissdata.nl) panel administered by CentERdata. The LISS panel consists of about 5,000 households in the Netherlands. Participants are invited frequently to complete surveys. The survey used in the present study was completed in three waves during a 3-month period in 2012. Responses were matched based on respondents’ unique participant number. 3 The study was carried out in compliance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
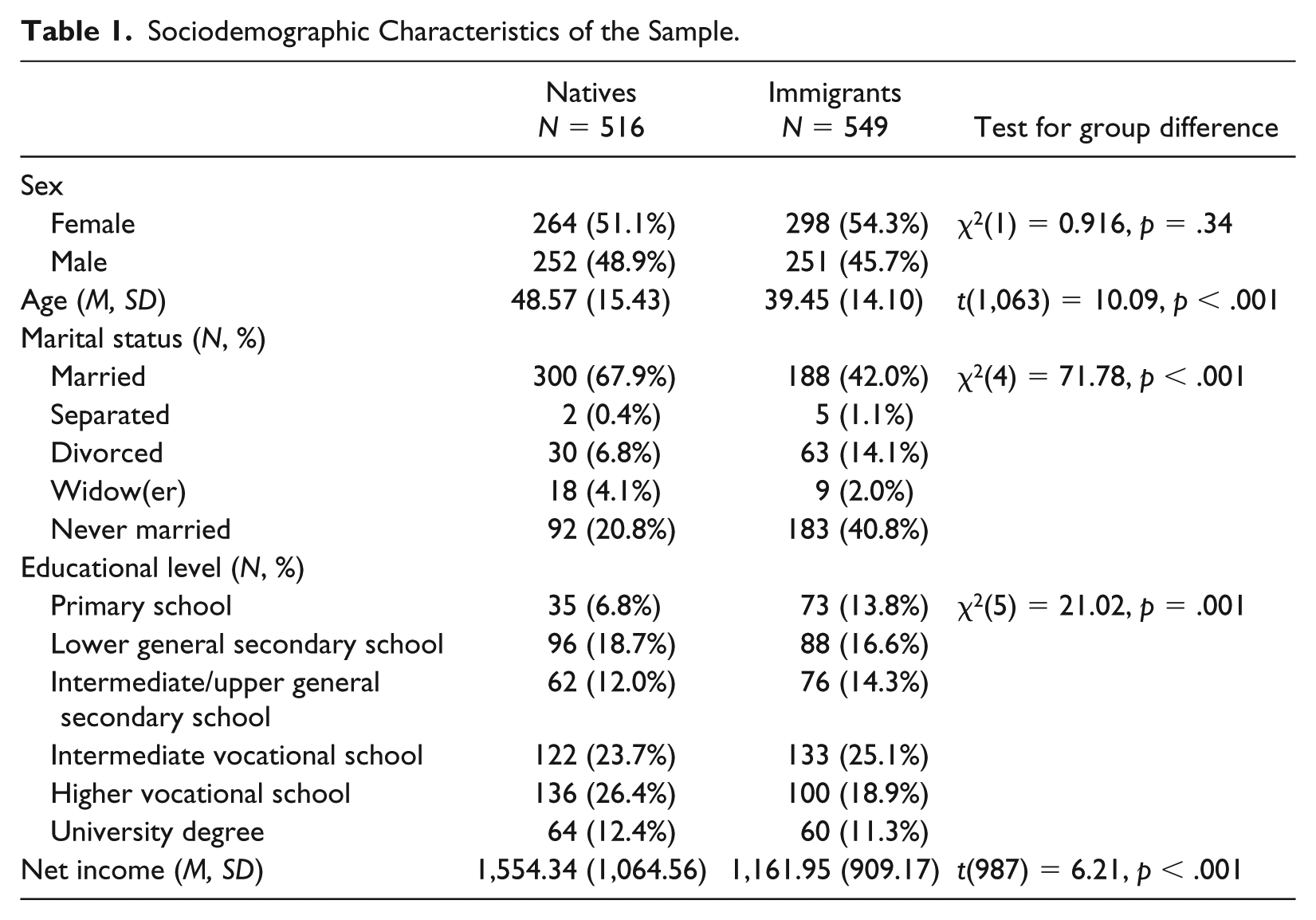
Sociodemographic characteristics (sex, age, marital status, educational level, net income) are reported in Table 1. Dutch natives and immigrant participants did not differ with respect to their sex distribution, but Dutch natives were on average 9.12 years older, and had a higher net income than the immigrant groups. The groups also differed with respect to marital status and educational level. The analyses comparing Dutch natives and immigrant participants reported below, therefore, controlled for age, net income, marital status, and educational level.
Sociodemographic Characteristics of the Sample.
To make sure the immigrant sample would understand all questionnaire items correctly, we approached two nonnative Dutch volunteers. These volunteers were two Dutch Turkish workers. If at least one of them did not understand an item, we reformulated it. Two of the authors (ER and MB) thereafter checked the items to make sure the adapted and the original versions had the same meaning. We reformulated 16 items of the Autonomy–Connectedness Scale, seven items of the Self-Construal Scale, five items of the Eating Disorder Inventory, four items of the Beck Depression Inventory, and two items of the Symptom Checklist–90 Anxiety subscale. All participants, including the Dutch natives, responded to the same simplified Dutch questionnaire items.
Measures
The Autonomy–Connectedness Scale (ACS-30; Bekker & van Assen, 2006) was used to assess autonomy–connectedness. This questionnaire consists of 30 items and has three subscales: Self-Awareness (seven items, three of which are reverse coded; e.g., “I often do not know what my opinion is”), Sensitivity to Others (17 items, eight of which are reverse coded; e.g., “I often wonder what other people think of me”), and Capacity for Managing New Situations (six items, three of which are reverse coded; e.g., “I quickly feel at ease in new situations”). All items are measured on 5-point scales, ranging from disagree to agree. The ACS-30 has been shown to have good reliability and validity (Bekker & van Assen, 2006, 2008). Although the Autonomy–Connectedness Scale has also been used in several ethnic samples (Bekker et al., 2011; Moleiro, Ratinho, & Bernardes, 2016), its usage is not as well substantiated outside of Western samples. As we included a variety of ethnic minorities in the present study, we subjected the Autonomy–Connectedness Scale to confirmatory factor analyses, presented in Supplement B in the supplementary material. Although the fit was unsatisfactory, all items loaded significantly on their hypothesized factors. Also, scale reliabilities were sufficient. In the Dutch sample, α for Self-Awareness, Sensitivity to Others, and Capacity for Managing New Situations was .76, .79, and .73, respectively, and, in the immigrant sample, .76, .75, and .70. The significant factor loadings and sufficient reliabilities justify the ACS-30’s use in the present samples.
The Self-Construal Scale (SCS; Singelis, 1994) was used to assess independent and interdependent forms of self-construal. Its 22 items are divided into two subscales: Independence (11 items, e.g., “I go my own way regardless of what other people think”) and Interdependence (11 items, e.g., “I feel well while cooperating with others”). The items are answered on 5-point scales. Reliability and validity of the scales have been reported to be acceptable, and the two distinct factors have been found in multiethnic samples (Singelis, 1994). In the present study, α for the Independence scale was .69 for the Dutch and .73 for the immigrant sample. For the Interdependence scale, α was .73 for the Dutch and .74 for the immigrant sample.
The Acculturation Questionnaire (Arends-Tóth & van de Vijver, 2007) covers two acculturation attitudes, represented in two subscales, that is, Maintenance of the Culture of Origin and Adaptation to the New Culture. Maintenance and Adaptation are assessed in various life domains, such as language, news, social contacts, cultural habits, and celebrations (e.g., “I think it is important to live according to the Turkish/Moroccan/or other culture” vs., e.g., “I think it is important to have Dutch friends”). The Acculturation Questionnaire consists of 22 items (11 for each scale) that are answered on a 5-point scale. The questionnaire was only completed by the immigrant sample in the present study and showed good reliability with Cronbach’s alphas of .93 and .77 of the Maintenance and Adaptation subscales, respectively.
Psychopathological symptoms were assessed by measures of anxiety, depression, and eating disorder symptoms. The 10-item Anxiety subscale of the Symptom Checklist–90 (SCL-90; Derogatis, 1977; Dutch translation by Arrindell & Ettema, 1986) was used to assess whether and to what extent participants reported symptoms of anxiety (e.g., “How much were you bothered by worrying too much about things”). Answer categories of the items range from 1 (not at all) to 5 (very much). The SCL-90 has been used and validated in numerous countries (e.g., Holi, Marttunen, & Aalberg, 2003), including in studies investigating psychopathological distress in collectivistically oriented cultures (e.g., Yeh, 2003). Reliability of the Anxiety subscale in the present study was good (Dutch sample: α = .91; immigrant sample: α = .94).
The Dutch translation (van der Does, 2002) of the Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996) was used to assess depressive symptoms. The scale consists of 21 items with four answering options. For example, for the “past failure” item, respondents had to choose between the four options: “I do not feel like a failure”; “I have failed more than I should have”; “As I look back, I see a lot of failures”; and “I feel I am a total failure as a person.” The BDI-II has been established as both a reliable and valid measure of depressive symptoms (e.g., Krefetz, Steer, Gulab, & Beck, 2002) and has been used in many countries (see Richter, Werner, Heerlein, Kraus, & Sauer, 1998). Reliability in the current study was high (Dutch sample: α = .90; immigrant sample: α = .94).
For eating disorder symptoms, we used three relevant subscales of the Eating Disorder Inventory–2 (EDI-2; Garner, 1991; Dutch translation by van Strien, 2002): Drive for Thinness (seven items), Body Dissatisfaction (nine items, five of which are reverse coded), and Bulimia (seven items). The Dutch version of the EDI-2 shows good reliability, concept validity, and criterion validity (van Strien & Ouwens, 2003). The EDI has been used internationally, both in individualistically oriented as well as collectivistically oriented societies (e.g., Boyadjieva & Steinhausen, 1996; Nevonen & Broberg, 2000). In the Dutch sample, α in the present study was .77, .87, and .82 for Drive for Thinness, Body Dissatisfaction, and Bulimia, respectively. In the immigrant sample, α was .76, .88, and .85, respectively.
Statistical Analyses
The first aim of the present study was to investigate the associations between autonomy–connectedness, self-construal, and acculturation, in line with Bekker et al. (2011). We conducted three separate hierarchical multiple regressions, one for each autonomy–connectedness component. After first controlling for age, marital status, educational level, and net income (Step 0), in Step 1, principal predictors ethnicity and sex were added (Dutch natives and women were coded 0, immigrants and men were coded 1). We added the two self-construal scales in Step 2, and, only in the immigrant sample, acculturation (maintenance and adaptation) in Step 3. In the final step (Step 3 for the Dutch natives and Step 4 for the immigrants), we added the interactions between ethnicity and all other variables to test whether associations were different for Dutch and immigrant participants. Using one omnibus test, we first tested whether the model including the interactions explained significantly more variance than the model without interactions (thereby controlling for Type I error). When indicated, we then examined each interaction separately by adding only this interaction to the model with main effects (i.e., the model of Step 2) to avoid multicollinearity problems caused by highly correlated interaction terms. We corrected for the amount of tests carried out using the Bonferonni correction.
The second aim of the present study was to investigate the associations between autonomy–connectedness and psychopathological symptoms, controlled for in(ter)dependent forms of self-construal and acculturation. For this purpose, we carried out hierarchical regression analyses similar to those described above with psychopathological symptoms (anxiety, depression, and eating disorder symptoms) as predicted variables. The autonomy–connectedness components were added after the self-construal and acculturation steps but before entering the interactions between ethnicity and all other variables.
We used IBM SPSS version 23 in all analyses. We used all available data in our analyses. We did carry out sensitivity analyses for the main analyses and discuss the robustness of our findings in the notes below. More specifically, in these sensitivity analyses, we checked for outliers and repeated the analyses with the outliers (based on the Mahalanobis distance with p < .001; Tabachnick & Fidell, 2007) removed.
Results
Group Differences
Before conducting our main analyses, all immigrant groups (immigrants from Indonesia, Morocco, Turkey, South Africa, Surinam, and Dutch Antilles) were compared using ANOVAs and Welch’s tests 4 with regard to autonomy–connectedness, self-construal, and psychopathological symptoms to check for homogeneity of the immigrants as a group. These tests indicated differences on most dependent variables (see Note 2). Tukey and Brown-Forsythe 5 post hoc tests were conducted after a significant ANOVA/Welch’s test to examine these group differences more closely. Although presenting all group comparisons is beyond the scope of the present article, immigrants from Indonesia differed consistently from one or more groups on every dependent variable, and, thus, compromised the homogeneity of the immigrant sample. We, therefore, decided to omit them from the main analyses reported below. 6 Correlations between all variables under study, after exclusion of the non-Western and Indonesian immigrants, are reported in Table 2.
Partial Correlations Between All Variables Under Study (Controlled for Age, Marital Status, Educational Level, and Net Income).
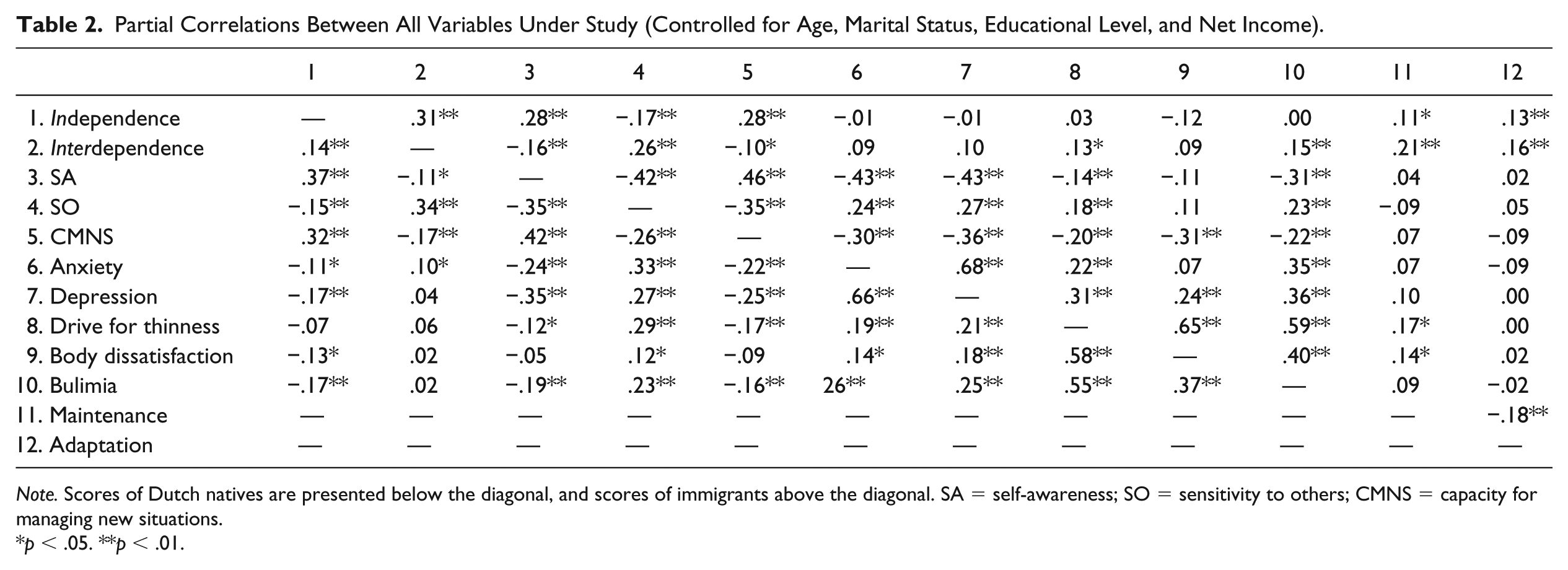
Note. Scores of Dutch natives are presented below the diagonal, and scores of immigrants above the diagonal. SA = self-awareness; SO = sensitivity to others; CMNS = capacity for managing new situations.
p < .05. **p < .01.
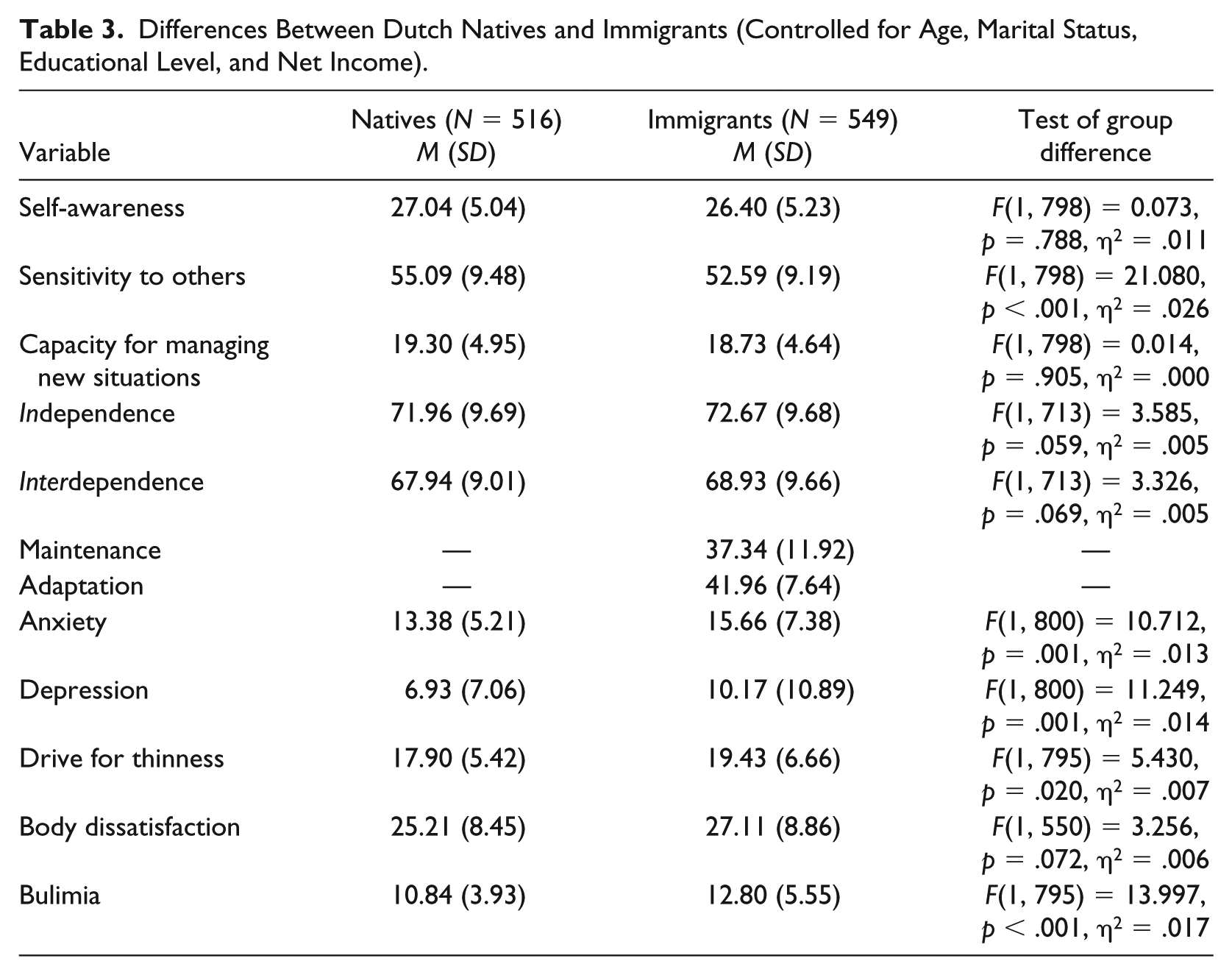
Next, ANCOVAs (controlling for age, net income, marital status, and educational level) were conducted to investigate whether the remaining immigrant groups differed from Dutch natives with respect to the three autonomy–connectedness scales, self-construal, and psychopathological symptoms (anxiety, depression, drive for thinness, body dissatisfaction, and bulimia). Results are reported in Table 3. On average, immigrants scored lower than Dutch natives on sensitivity to others, and they scored higher on psychopathology symptoms, except for body dissatisfaction. Effect sizes were small to medium, with the strongest effect on sensitivity to others (ɳ2 = .026). There were no differences in forms of self-construal and capacity for managing new situations.
Differences Between Dutch Natives and Immigrants (Controlled for Age, Marital Status, Educational Level, and Net Income).
First Aim: Associations Between Self-Construal, Acculturation and Autonomy–Connectedness 7
To investigate the associations between autonomy–connectedness, self-construal, and acculturation, we conducted three separate hierarchical multiple regression analyses; one for each autonomy–connectedness component. An overview of these analyses is presented in Table 4. No multicollinearity was present in any of the analyses, as the maximum variance inflation factor (VIF) was 1.684. Overall, self-construal accounted for the most additional variance in all autonomy–connectedness components (11.4%-15.9%), representing large effect sizes. Ethnicity and sex explained a significant amount of additional variance in sensitivity to others (11.5%) and capacity for managing new situations (2.1%), but not in self-awareness (0.4%). The final model explained 20.8% of variance in self-awareness, 28.6% in sensitivity to others, and 18.4% in capacity for managing new situations. In this final model, sex was negatively associated with capacity for managing new situations, indicating higher scores in men, whereas it was positively associated with sensitivity to others, indicating higher scores in women.
Multiple Hierarchical Regression Analyses With the Autonomy–Connectedness Subscales as Dependent Variables (Controlled for Age, Marital Status, Educational Level, and Net Income).
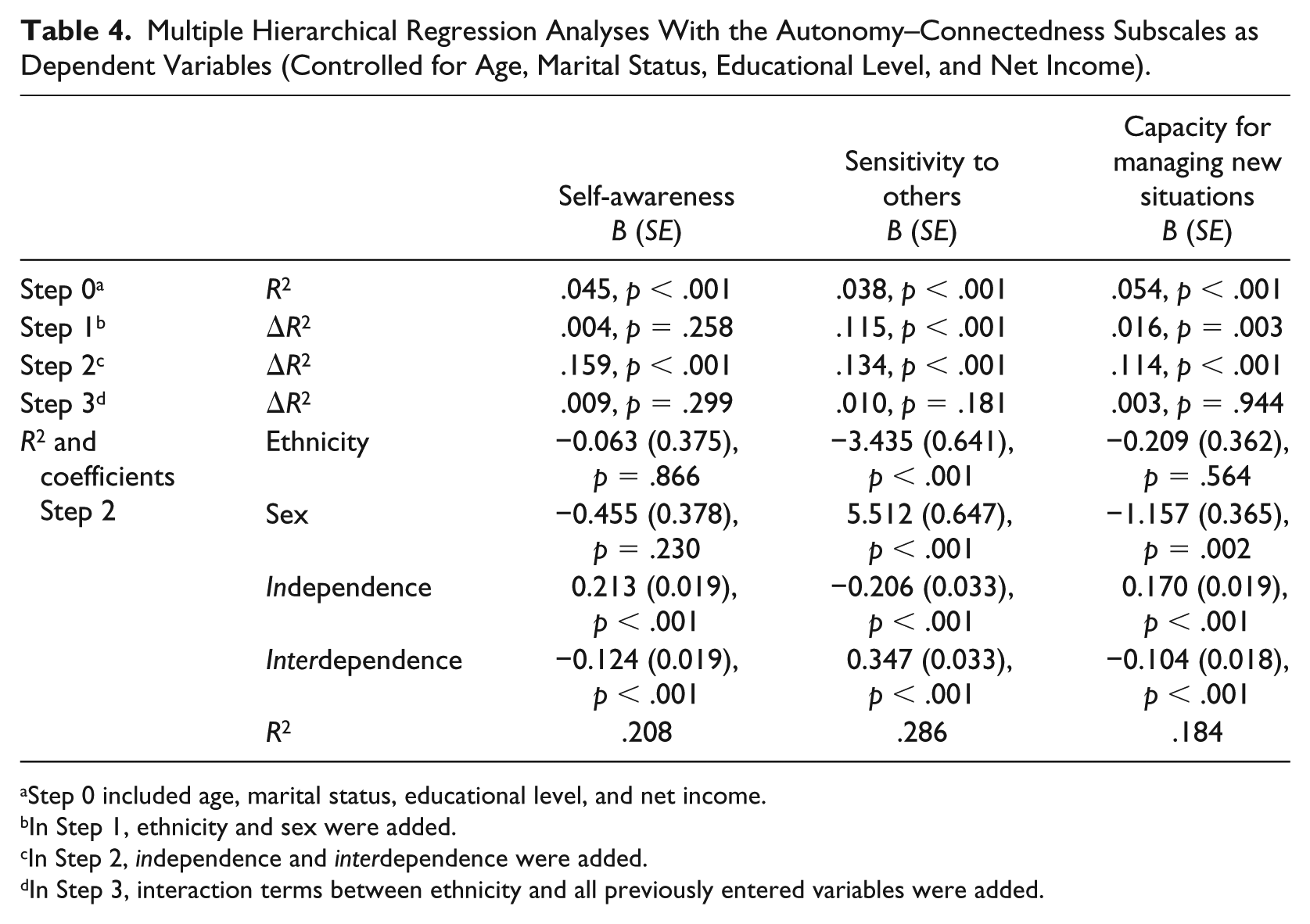
Step 0 included age, marital status, educational level, and net income.
In Step 1, ethnicity and sex were added.
In Step 2, independence and interdependence were added.
In Step 3, interaction terms between ethnicity and all previously entered variables were added.
Confirming Hypothesis 1a, an independent self-construal positively contributed to self-awareness as well as to capacity for managing new situations, and negatively to sensitivity to others. Also confirming Hypothesis 1b, an interdependent self-construal was positively related to sensitivity to other, as well as negatively to self-awareness and capacity for managing new situations. Not in line with Hypotheses 1c and 1d, in the immigrant sample, acculturation did not explain additional variance in any of the autonomy–connectedness components (Table 5). The addition of the interactions (Step 3, Table 4) with ethnicity did not add a significant amount of explained variance in any of the regression analyses, indicating these associations are not moderated by immigration status.
Results for the Multiple Hierarchical Regression Analyses Including the Acculturation Variables in Step 3 (Analyses for the Immigrants).
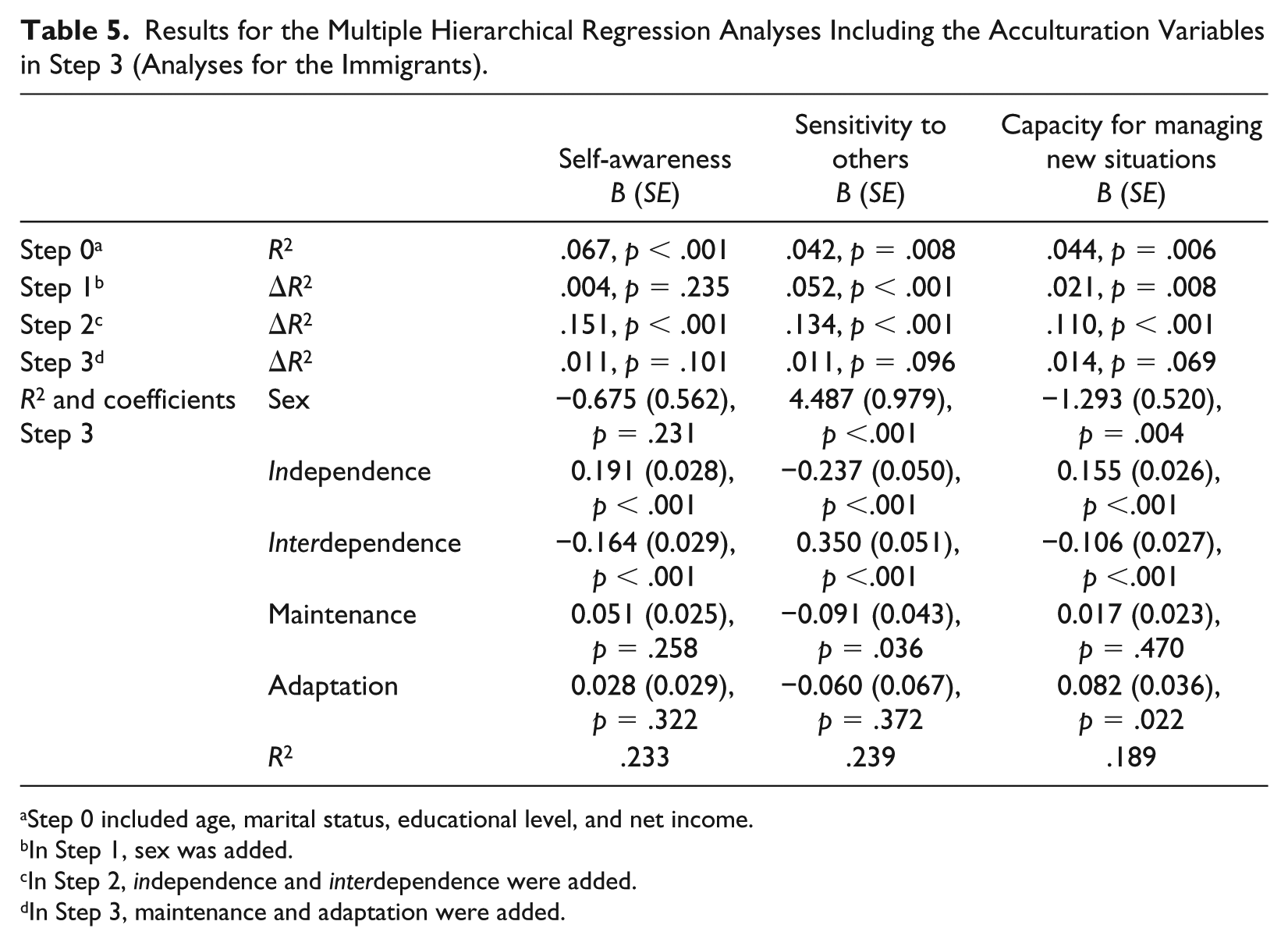
Step 0 included age, marital status, educational level, and net income.
In Step 1, sex was added.
In Step 2, independence and interdependence were added.
In Step 3, maintenance and adaptation were added.
Second Aim: Associations Between Autonomy–Connectedness and Psychopathological Symptoms, Controlled for Self-Construal and Acculturation
To investigate how much variance in psychopathological symptoms was accounted for by the autonomy–connectedness components after controlling for sex and ethnicity, self-construal, and acculturation, we conducted five separate hierarchical multiple regression analyses; one for each symptom (anxiety, depression, drive for thinness, body dissatisfaction, and bulimia). An overview of the results of the multiple hierarchical regression analyses is presented in Table 6. No multicollinearity was present in any of the analyses, as the maximum VIF was 1.821 in the analysis with body dissatisfaction as the dependent variable. The total amount of variance explained by the full model including the interactions ranged from 16.6% (bulimia) to 22.7% (depression).
Multiple Hierarchical Regression Analyses Predicting Psychopathological Symptoms (Controlled for Age, Marital Status, Educational Level, and Net Income).
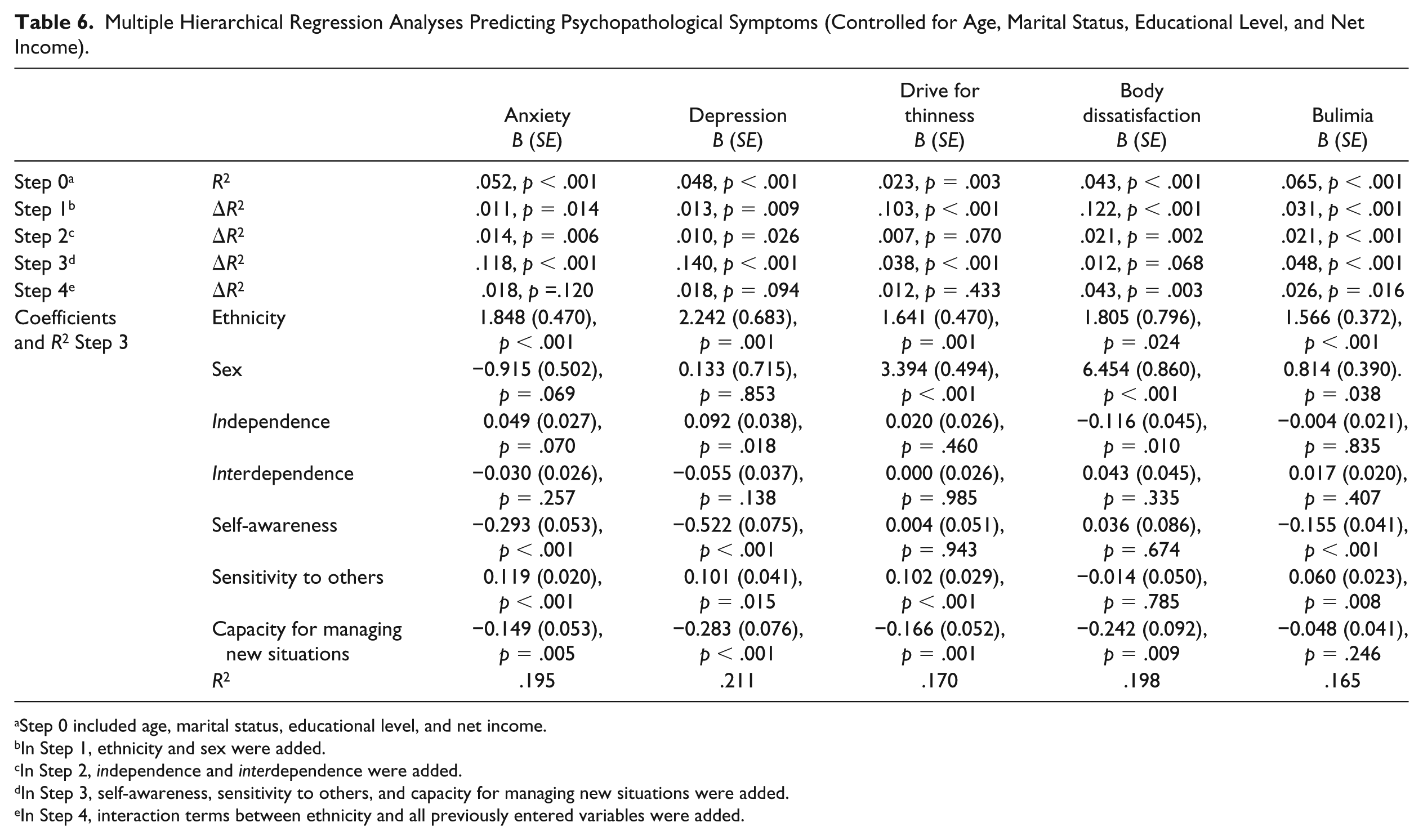
Step 0 included age, marital status, educational level, and net income.
In Step 1, ethnicity and sex were added.
In Step 2, independence and interdependence were added.
In Step 3, self-awareness, sensitivity to others, and capacity for managing new situations were added.
In Step 4, interaction terms between ethnicity and all previously entered variables were added.
Anxiety and depression
Sex and ethnicity, after controlling for age, net income, marital status, and educational level, explained a small but significant (1.3% in anxiety and 1.8% in depression) amount of additional variance. In the final model without interactions, ethnicity was still a significant predictor, but sex was not; immigrants scored higher on anxiety as well as on depression. Sex was a significant predictor for depression before taking self-construal and autonomy–connectedness into account (B = 1.654, t = 2.187, p = .004), with women scoring higher. Self-construal also added a significant but small amount of explained variance to the model (1.2% in anxiety and 1.5% in depression). Before adding the three autonomy–connectedness components, an independent self-construal was negatively associated with anxiety (B = −0.058S, t = −2.185, p = .029) and depressive symptoms (B = −0.112, t = −2.897, p = .004), whereas an interdependent self-construal was positively associated with anxiety (B = 0.063, t = 2.415, p = .016) and depressive symptoms (B = 0.088, t = 2.332, p = .020; not shown in Table 6, which only shows results of the final model). In the final model, only the association between an independent self-construal and anxiety symptoms remained, which turned positive (B = 0.062, t = 2.268, p = .024). 8 All effects of self-construal on symptoms were small at best. Next, but only in the immigrant sample, acculturation variables were added. Maintenance and adaptation did not contribute significantly to the model (see Table 7).
Results for the Multiple Hierarchical Regression Analyses Including the Acculturation Variables in Step 3 (Analyses for the Immigrants).
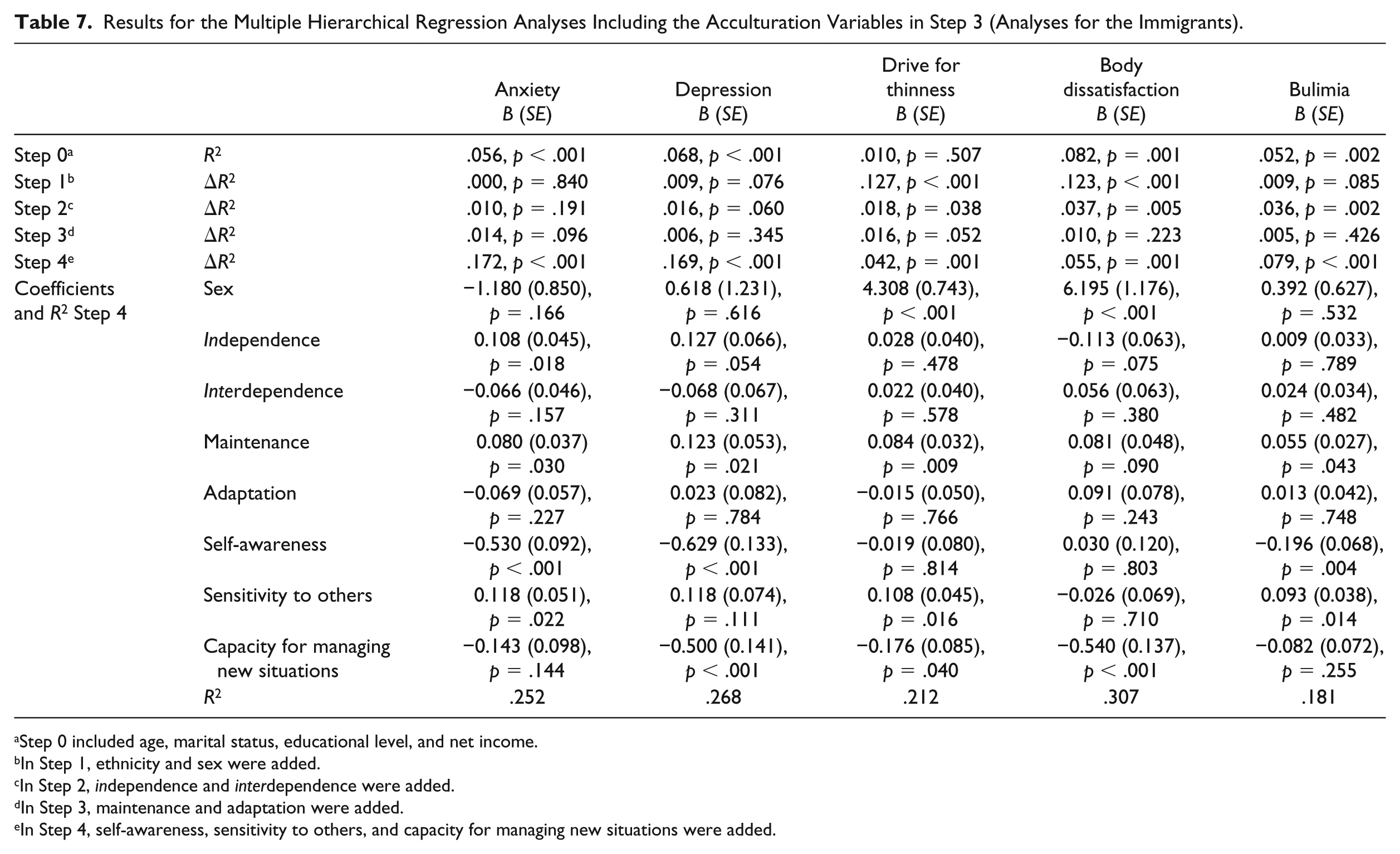
Step 0 included age, marital status, educational level, and net income.
In Step 1, ethnicity and sex were added.
In Step 2, independence and interdependence were added.
In Step 3, maintenance and adaptation were added.
In Step 4, self-awareness, sensitivity to others, and capacity for managing new situations were added.
Autonomy–connectedness (Step 3) explained 12.7% of variance in anxiety and 14.1% in depression, corresponding to strong effects. Both self-awareness and capacity for managing new situations were associated negatively with anxiety and depression, whereas sensitivity to others was associated positively with anxiety and depression. In line with Hypothesis 2, these results suggest that autonomy–connectedness deficits were associated with more anxiety and depressive symptoms.
In the last step, the interactions between ethnicity and all other variables were added. The interactions explained a significant amount of additional variance in both anxiety (2.4%) and depression (2.3%), corresponding to small effects. 9 Interactions were added separately, correcting for the amount of tests using the Bonferonni correction (p < .05/10 = .005). Adding interactions separately revealed that ethnicity was a significant moderator for the relation between self-awareness and anxiety (B = −0.287, t = −3.369, p < .001), but not for depression (B = −0.26, t = −2.116, p = .035). Associations between self-awareness and anxiety symptoms were negative in both groups, but stronger in immigrants than in Dutch natives—immigrants: B = −0.468, t = 3.369, p = .001; Dutch natives: B = −0.181, t = −2.602, p = .009.
Eating-related psychopathology: Drive for thinness, body dissatisfaction, and bulimia 10
Together, ethnicity and sex (Step 1) explained a significant amount of additional variance in drive for thinness (10.4%), body dissatisfaction (12.6%), and bulimia (3.1%), corresponding to small to medium–large effect sizes. As a block, sex and ethnicity seemed to be stronger predictors of drive for thinness and body dissatisfaction than other blocks.
In the model including autonomy–connectedness (Step 3), women as well as immigrants scored higher on eating-related psychopathology. Self-construal (Step 2) added a small but significant amount of explained variance to the models for body dissatisfaction (2.1%) and bulimia (2.1%), but not to drive for thinness (0.7%). Before taking the three autonomy–connectedness components into account, an independent self-construal was negatively associated with body dissatisfaction (B = −0.139 t = −3.412, p = .001) and bulimia (B = −0.058, t = −3.019, p = .003), whereas an interdependent self-construal was positively associated with drive for thinness (B = 0.053, t = 2.223, p = .027), as well as bulimia (B = 0.061, t = 3.219, p = .001). After taking autonomy–connectedness into account, only the negative association between an independent self-construal and body dissatisfaction remained (B = −0.113, t = −2.522, p = .012). Again, effects of self-construal were small at best. Next, but only for the immigrants, acculturation variables were added (Table 7). Acculturation did not explain a significant amount of additional variance.
In Step 3, the autonomy–connectedness components were added, which together explained a significant amount of additional variance in drive for thinness (3.7%) and bulimia (4.8%), representing medium effect sizes. Self-awareness was negatively associated with bulimia, sensitivity to others positively with drive for thinness and bulimia, and capacity for managing new situations negatively with drive for thinness and bulimia. Similar to the analyses for anxiety and depression and in line with Hypothesis 2, this reflects that autonomy–connectedness deficits associated with more eating-related psychopathology.
The model in which all interactions with ethnicity were added (Step 4) explained a significant amount of additional variance in body dissatisfaction (4.6%) and bulimia (2.5%), corresponding to small to medium effects. The interactions did not explain a significant amount of additional variance in drive for thinness (1.2%). Adding interactions separately revealed that ethnicity was a significant moderator for the relation between capacity for managing new situations and body dissatisfaction (B = −0.054, t = 3.552, p < .001). Simple effects analysis showed that low capacity for managing new situations was associated with more body dissatisfaction (B = −0.533, t = −4.308, p < .001) in immigrants, but not in Dutch natives (B = 0.008, t = 0.070, p = .944).
Discussion
The two aims of the present study were to investigate the associations between self-construal, acculturation, and autonomy–connectedness, and to investigate the relations between autonomy–connectedness and psychopathological symptoms, controlling for self-construal and acculturation, within a multicultural immigrant context. We investigated this in a large and heterogeneous immigrant sample consisting of both men and women.
Associations Between Self-Construal, Acculturation, and Autonomy–Connectedness
In line with Bekker et al. (2011), but contrasting with the idea that non-Westerners would show heightened interpersonal sensitivity, we found that immigrants scored lower on sensitivity to others than Dutch natives did. Lower scores on sensitivity to others are not necessarily characteristic of immigrants. Bekker et al. explain that immigrants’ lower scores on sensitivity to others might be due to the experience of migration and the conflicting demands of “others” vis-à-vis retention of the heritage culture and adaptation of the host culture (e.g., Rodriguez et al., 2002). Adapting to the host culture may increase intragroup marginalization (e.g., by straining relationships with one’s family), whereas staying loyal to the culture of origin may increase cultural incongruity from the host culture. In other words, migrants have a lower score on sensitivity to others, possibly because being less sensitive to the opinion of family members and members of the host culture helps them to cope with divergent expectancies.
Confirming Bekker et al. (2011) and our hypotheses, we found that an independent self-construal was positively associated with self-awareness and capacity for managing new situations, and negatively with sensitivity to others, whereas an interdependent self-construal was negatively associated with self-awareness and capacity for managing new situations, and positively with sensitivity to others. Importantly, these associations were similar for both Dutch natives and immigrants.
Not in line with our hypotheses or with Bekker et al.’s (2011) findings, we found that acculturation did not add a significant amount of additional variance to the model explaining autonomy–connectedness. An explanation for this difference could be found in the age of both samples. The sample included in the study by Bekker and colleagues had a mean age of 19.5 years, whereas our immigrant sample had a mean age of 39.5 years. Autonomy–connectedness is rooted in attachment theory (Bowlby, 1969, 1973), and is not fully developed until adulthood (Bekker, 1993). Attachment experiences related to acculturation could, therefore, possibly have had a larger impact on the younger sample in the Bekker et al. study when compared with the sample in the present study.
Associations Between Autonomy–Connectedness and Psychopathological Symptoms, Controlling for Self-Construal and Acculturation
Regarding our second aim, and in line with the literature (e.g., Bekker & Belt, 2006; Burke & Haslam, 2001; Kuipers et al., 2017), we expected autonomy–connectedness deficits to be positively associated with psychopathology symptoms. Across the different models, regression coefficients pointed in the expected direction, with lower scores on self-awareness and capacity for managing new situations as well as higher scores on sensitivity to others predicting higher scores on psychopathology. It must be noted that most but not all these effects were statistically significant.
More generally, we found that immigrants scored higher on all but one index of psychopathology we assessed. This is not an uncommon finding, as multiple studies indicate higher prevalence of psychopathology in immigrants than in natives (e.g., van der Wurff et al., 2004). Importantly, next to the fact that immigrant groups might be at greater risk of developing mental disorders, the literature shows they are also less likely to receive appropriate treatment (e.g., Alegria et al., 2008; Sempértegui, Knipscheer, & Bekker, 2018).
The autonomy–connectedness components seemed to explain most additional variance in anxiety, depression, and bulimic symptoms when compared with other constructs in the model. With regard to drive for thinness and body dissatisfaction, not autonomy–connectedness, but sex and ethnicity seemed to be the strongest predictors. Differences between cultures might have played a role in our results. Important to further note is that body image concerns in men are not likely to manifest in eating disorders (Rosenmann & Kaplan, 2014). Future research may put more focus on sex differences in this regard.
Autonomy–connectedness being a gender-sensitive construct, it may be interesting to not only focus on sex but also explicitly investigate masculine versus feminine cultures. Moleiro et al. (2016) included the cultural dimension of masculinity/femininity in their study of Portuguese natives, Portuguese Cape-Verdean (coming from a feminine collectivistic culture), and Chinese immigrants (coming from a masculine collectivistic culture). Their results indicate that both collectivism and cultural femininity were associated with lower self-awareness. No differences were found on the other two autonomy–connectedness components. Other variables future research may wish to include are whether immigrants are first- or second-generation immigrants, their language competency, as well as the length of stay in the host country, as these variables include information about acculturation.
Limitations
Several limitations of the present study have to be noted. The first concerns its cross-sectional nature, which precludes any causal conclusions. Especially for the prediction of psychopathological symptoms, it might have been valuable to assess the symptoms at a later date than autonomy–connectedness.
Second, we used online self-report questionnaires. Next to a possible social desirability bias accompanying self-report, filling out questionnaires online might have additional downsides, because participants might have been disturbed while filling out the questionnaires. Also, questionnaires were only presented in Dutch. This means that non–Dutch-speaking immigrants could not be included in the present study, limiting generalizability.
Third, multiple questionnaire items were simplified to make sure the immigrant sample would understand all questions. This concerned several scales used in the present study, including about half of the items of the autonomy scales. All participants (including Dutch natives) responded to the same simplified questionnaires. In addition, and especially with regard to the sensitivity to others scale of the ACS-30 assessing autonomy–connectedness, factor loadings were smaller than in the original version (Bekker & van Assen, 2006; Supplement B in the supplementary material). Corrected item total correlations of items with their corresponding scales were also smaller and factor analysis showed the model’s fit was unsatisfactory. This indicates that associations between the autonomy–connectedness items are probably different across groups, demonstrating violations of measurement invariance. We cannot exclude the possibility that simplification of the items may have changed the meaning of some items of the questionnaire and this affected the results and conclusions of our analyses.
A final limitation, although certainty also a strength of our study, concerns the heterogeneity of our sample. Among many others, Carta, Bernal, Hardoy, and Haro-Abad (2005) underline that it is impossible to consider migrants as a homogeneous group. Our sample indeed showed differences within the immigrant groups. To make the group more homogeneous, we decided to not analyze the Indonesian immigrants, as this group was the only group that showed consistent differences with all the other immigrant groups, plausibly because of their different immigration history than the other immigrants in our sample. Indonesia was a colony of the Netherlands, and the majority of immigrants leaving for the Netherlands were already descendants of mixed Dutch and Indonesian parents. This does not mean, however, that the remaining immigrant groups did not differ at all. Note, however, that our large and heterogeneous community sample was representative of the Dutch immigrant population, with different immigrant groups that were too small to separately subject to statistically powerful analyses.
Conclusion
In conclusion, with regard to this study’s first aim, we found that for both Dutch natives and immigrants, an independent self-construal was positively associated with self-awareness and capacity for managing new situations, and was negatively associated with sensitivity to others. An interdependent self-construal, however, was negatively associated with self-awareness and capacity for managing new situations, and was positively associated with sensitivity to others. Importantly, these associations were not moderated by immigration status.
With regard to our second aim, this study showed that autonomy–connectedness explained a relatively large amount of variance of psychopathology in both the Dutch and immigrant samples when compared with the other constructs in the model, corresponding to medium effects in eating-related psychopathology, and to large effects in anxiety and depression. Autonomy–connectedness, thus, seems to be an important construct in the study of people from a non-Western background as well. We hope that these results can motivate therapists to enhance autonomy–connectedness in their immigrant patients. Indeed clinical evidence seems to suggest that treatment aimed at increasing autonomy–connectedness in immigrants has beneficial effects (Bekker, Kouwenhoven, Rutten, & van Helsdingen, 2015). This study furthermore shows that the Autonomy–Connectedness Scale is a useful instrument in immigrant samples, largely replicating the results by Bekker et al. (2011).
Supplemental Material
Supplement_for_JCCP – Supplemental material for Autonomy–Connectedness, Self-Construal, and Acculturation: Associations With Mental Health in a Multicultural Society
Supplemental material, Supplement_for_JCCP for Autonomy–Connectedness, Self-Construal, and Acculturation: Associations With Mental Health in a Multicultural Society by J. Maas, M. A. L. M. van Assen, A. J. L. M. van Balkom, E. A. P. Rutten and M. H. J. Bekker in Journal of Cross-Cultural Psychology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.