
Abstract
This mixed-methods study explores the incidence, manifestations, and drivers of secondary traumatic stress among service providers who work with Syrian refugees in Istanbul, Turkey. A survey of 104 social workers and other providers working in 17 public and civil society agencies in Istanbul in 2018 demonstrates that 54.81% had Secondary Traumatic Stress Scale scores indicating mild to severe secondary traumatic stress. In total, 28 qualitative interviews showed manifestations and possible drivers of secondary traumatic stress including weak supervision, heavy caseloads, and insecure working conditions. The findings suggest supervision and peer-support should be strengthened to address secondary traumatic stress among providers serving refugees.
Keywords
Introduction
Since the onset of the civil war in Syria in 2011, Turkey has become the host for one of the largest number of refugees in the world with currently around 3.5 million people, mostly Syrians (Presidency of Migration Management [PMM], 2023). Massive refugee arrivals occurred at a time when the country did not have an adequate institutional framework of reception, unlike in European Union (EU) states which have long-standing asylum structures. In this void, national and international civil society organisations (CSOs) were at the forefront of humanitarian assistance and social service delivery to Syrians. Initiated in 2016, the EU Facility for Refugees in Turkey (FRIT) helped the development of an infrastructure for public service delivery while it has also supported CSO programmes for refugees through financial and technical assistance (European Commission, 2023). Given that there was little organisational expertise and training on serving refugees, social workers and other service providers working in public agencies or CSOs have been exposed to high levels of work-related stress: in addition to heavy caseloads, they are exposed to the traumatic stories of their clients who often have had devastating experiences while fleeing their country and after arrival in Turkey. There is growing scholarly attention on the training and working conditions of social workers serving displaced populations (e.g. Boccagni and Righard, 2020; Teloni et al., 2023) in Europe. However, in Turkey, despite the increasing numbers of refugees, the training and supervision of social workers and other providers have been neglected. What are the potential consequences of this lack of attention to the conditions of providers who serve refugees in a system that is still developing? In this article, we focus on secondary exposure to trauma by providers serving Syrian refugees in Istanbul, the city with the highest number of refugees in Turkey. Secondary traumatic stress (STS), defined as stress resulting from knowledge about another person’s traumatic experiences (Bride et al., 2004), in addition to depression, anxiety and burnout, is one of the mental health problems that service providers working with refugees may face.
This article explores the incidence, manifestations and drivers of STS among social workers and other providers (psychological counsellors, lawyers, interpreters) serving Syrian refugees. The quantitative findings of the mixed-methods study demonstrate that more than half of the respondents of a survey conducted in public agencies and CSOs serving refugees had some level of STS as indicated by Secondary Traumatic Stress Scale (STSS) scores. The qualitative findings show manifestations of STS reported by interviewees and indicate possible drivers of STS such as lack of supervision, heavy caseloads and working conditions characterised by short-term funded projects in the CSOs.
Literature
STS is a theoretical construct that seeks to understand the responses of people in various helping professions to indirect exposure to trauma through clients (Ludick and Figley, 2017). STS refers to observable symptoms developed by professionals that are like post-traumatic stress symptoms exhibited by their clients. Viewing professionals in an ecological context in their theoretical model on STS, Ludick and Figley (2017: 113–117) identify two sets of variables that increase the risk of STS as (1) exposure to suffering, empathic concern and empathic ability, which inform empathic responses and (2) personal trauma history and other life demands that may disrupt a person’s functioning; and a third set of variables that might build resilience against STS, namely, self-care, detachment from client suffering, sense of satisfaction and social support.
The narrative review below includes studies on STS (1) among service providers working with refugees, (2) conducted in Turkey and (3) which discuss its correlates. Authors 1, 3, 4 and 5 reviewed the literature on Turkey and authors 1, 2 and 6 reviewed the international literature. The search terms were secondary traumatic stress, refugees, and Turkey. For (1), articles containing both empirical studies and reviews; for (2), both articles and unpublished theses and for (3), theoretical articles and reviews were included. The literature review was revised by author 1.
Service providers working with high volumes of traumatised refugee clients are vulnerable to STS and other mental health problems such as depression and anxiety (Kim, 2017; Lusk and Terrazas, 2015). In a systematic review and meta-analysis of STS among professionals and volunteers working with forcibly displaced people, Roberts et al. (2021) report nearly half of the respondents had moderate to severe levels of STS. The affected groups include social workers (Guskovict and Potocky, 2018), interpreters, psychologists, medical doctors (Kindermann et al., 2017; Živanović and Marković, 2020), lawyers (Harris and Mellinger, 2021), resettlement workers (Akinsulure-Smith et al., 2018), humanitarian aid workers (Ebren et al., 2022), both professionals and volunteers, and those working in both public agencies and CSOs (Tessitore et al., 2023). Studies also show that STS among providers working with refugees may adversely affect the services they offer to traumatised clients (Akinsulure-Smith et al., 2018; Guskovict and Potocky, 2018).
In the few studies documenting STS among providers serving Iraqi and Syrian refugees in Turkey, social workers, psychotherapists, interpreters (Denkinger et al., 2018), legal aid providers and protection workers (Turgut, 2014), and refugee aid workers (Güzey, 2020) were found to have some level of STS.
Regarding correlates, studies on STS among social workers, mental health professionals and members of other helping professions have pointed to associations between STS levels and variables such as gender, age, length of professional experience, supervision at work, perceived social support and history of personal trauma (Bride et al., 2008; Ebren et al., 2022). A meta-analysis of 17 predictors of STS found exposure to traumatised clients, personal trauma history, work support and social support to have the highest effect sizes (Hensel et al., 2015). Studies on STS in Turkey offer differing results regarding drivers such as age, years in the profession and personal trauma (Çetinkaya Büyükbodur, 2018; Demirbaş, 2021; Gürdil, 2014; Kahil, 2016; Yanbolluoğlu, 2019), whereas some studies associate absence of supervision (Deniz Pak et al., 2017; Turgut, 2014; Yıldız, 2017) or lack of in-job training (Güzey, 2020) with higher levels of STS.
Service providers working with Syrian refugees in Turkey in protection, humanitarian assistance, counselling, interpreting, healthcare and legal aid have been strained by heavy caseloads and intense and prolonged exposure to traumatic experiences without getting much professional support in an institutional environment which is still in the making. Based on this, the article is guided by the following three research questions:
What is the incidence of STS among social workers and service providers working with Syrian refugees?
How does STS manifest itself in the daily experience of providers?
What is the impact of the work environment on STS among providers?
Methodology
The Providers ASPIRE study, a collaboration between Columbia University School of Social Work and Istanbul Aydın University in 2018, is to our knowledge the first mixed-methods study exploring STS among service providers working with Syrian refugees in Istanbul. The study protocol was submitted to Istanbul Aydın University’s Ethics Committee and to Columbia University’s Internal Review Board (IRB) in February and April 2018, respectively. Ethics Committee approval from Istanbul Aydın University and IRB approval from Columbia University were received in March and July 2018, respectively. All data collection, coordinated and carried out by the investigators based in Istanbul, took place between August and October 2018.
Participants and research ethics
Service providers above 18 (social workers, protection workers, psychological counsellors, lawyers and interpreters) who worked directly with Syrian refugees, and who spoke Turkish, Arabic or English were eligible to participate. Recruitment started after IRB approval and took place in two stages. First, from a list of CSOs working on migration in Istanbul, all working directly with Syrian refugees (44 in total) were contacted by the co-investigators who were all based in Istanbul at the time of the study (authors 1, 3, 4 and 5) through email explaining the goals and ethics procedures of the study and were asked to participate in the study. The Istanbul or national headquarters of the public agencies that served Syrian refugees were contacted in writing for permission to conduct the study in their offices. In total, 17 agencies (12 CSOs and five public agencies) agreed to have the study conducted with their employees on their premises. Then, the co-investigators in Istanbul phoned each participating CSO and public agency office to identify focal points and asked for assistance in recruiting participants among employees who directly served Syrian refugees. In the second stage, agency focal points informed their employees about the study and asked them if they would be interested in participating. Co-investigators and research assistants (RAs) then spoke with providers who indicated interest and explained the goals of the study. When a provider agreed to participate, the co-investigator or RA then presented an informed consent form to potential participants in writing and explained its content verbally in a private room at the agency. The informed consent form, prepared in Turkish, English and Arabic, detailed the risks of participation such as feeling discomfort, distress and anxiety during the interview as well as the potential situations in which confidentiality may not be maintained such as imminent intent to harm oneself or others, gender-based violence and child abuse. The informed consent form also described the procedures to keep the gathered information confidential and anonymous. After explaining the form (in the language preferred by the participant), the interviewer then asked the participant to read and sign the informed consent form, only after which the interview started. The participants were not given any incentives (payments or gifts) to participate.
Quantitative data collected through Qualtrics software on password-protected tablets were stored in a password-and firewall-protected computer at Columbia University. Soft qualitative data (audio recordings and their transcriptions) were anonymised and stored in a password-protected computer and all hardcopy items with identifying information (signed consent forms and interviewer notes) were stored in a locked file cabinet, both in author 3’s office. The quantitative data and the anonymised soft data from the qualitative study continue to be stored since data analysis for writing papers is ongoing. Upon completion of the analysis, qualitative data will be erased and destroyed.
Data analysis: Quantitative assessment
Co-investigators and RAs recruited providers in the quantitative component of the study on a rolling basis to generate a convenience sample. Approximately nine quantitative surveys were collected at CSOs and public agencies with a staff size of 20 or more and approximately four quantitative surveys were collected at agencies with a staff size of less than 20. Overall, 104 individual quantitative surveys lasting around 30 minutes were completed in private rooms at the participating agencies. Some CSOs’ refusal to participate in the study precluded the possibility of a sample representing all service providers working with Syrians in Istanbul.
Survey topics included sociodemographic, employment and client profile, as well as mental health (depression, anxiety, post-traumatic stress, STS), professional quality of life, and social and organisational support scales. Interviews for the survey were conducted in Turkish, English and Arabic.
The quantitative analysis for this article consisted of descriptive statistics (including frequency and percentages) and focused on the demographic questions and STSS scores. Screening for missing data, outliers and violations of normality was conducted. Inferential statistics were conducted before qualitative interviews and expanded at the cessation of all data collection. Bivariate analyses (incl. t-tests and ANOVA) between non-STSS variables and STSS scores were examined. We explored the findings from the other mental health scales and social and organisational support scales in another article (Brooks et al., 2022).
STSS was developed and validated by Bride et al. (2004), who operationalised it in terms of symptoms of intrusion, avoidance and arousal ‘resulting from indirect exposure to traumatic events by means of a professional helping relationship with a person or persons who have directly experienced traumatic events’. The internal reliability of both the overall scale and its three dimensions were high and STSS and its subscales had good convergent, discriminant and factorial validity (Bride et al., 2004). Kahil (2016) adapted the STSS into Turkish whose study with a sample of 202 professional and 26 volunteer aid workers yielded a unidimensional structure (Kahil and Palabıyıkoğlu, 2018) unlike the three-dimensional structure of STSS in the original validation study. A subsequent adaptation of STSS into Turkish (Yıldırım et al., 2018) on a sample of 334 healthcare professionals confirmed the three-dimensional structure of the STSS. In both studies, the internal reliability of the overall scale and its three subdimensions were found to be satisfactory. This study uses Kahil’s translation of the STSS.
Data analysis: Qualitative assessment
Following quantitative data collection, co-investigators and RAs conducted one or two qualitative interviews at each site with service providers. A total of 28 individual interviews were completed with providers who were asked if they wanted to participate in the qualitative component at the time of the quantitative survey. Each lasting approximately an hour, interviews were conducted in Turkish or English using a semi-structured interview guide that included questions and probes on the description of the agency’s services for refugees, description of own work with refugees, narratives on working with traumatised clients, supervision, quality of life, self-care and stigma, prejudice and discrimination. STS was not explicitly asked about during interviews; however, its symptomology (intrusion, avoidance and arousal) emerged as a prevailing topic. Interviews, which took place in private rooms at the participating agencies, were audio recorded, anonymised and then transcribed.
Qualitative analysis began with open coding of all interview transcriptions by authors 1, 3, 4 and 5. The preliminary codes identified by each author were then compared, leading to the following seven coding themes: (1) observations about the work environment, (2) quality of life, (3) psychological symptoms, (4) supervision, (5) social support, (6) providers’ attitudes about refugees, and (7) attitudes of friends and family towards refugees. In a second round for the purposes of this article, the same authors canvassed all codes for identifying symptomology and possible drivers (caseload, working conditions, supervision) of STS. Data were integrated using the narrative approach, whereby the qualitative findings were woven with the descriptive findings from the quantitative data.
Findings
In the quantitative survey, there was an equal distribution of males and females. A minority of providers were over the age of 30 (28.88%). Most providers were either Turkish (n = 86, 82.69%) or Syrian (n = 16, 15.38%). Nearly all providers spoke Turkish (n = 99, 95.19%) while only 40.38% (n = 41) spoke Arabic. Most providers completed at least a bachelor level of education (88.46%, n = 92), the largest group having social work degrees. In the qualitative study, eight interviewees were male (28.60%) and 20 (71.40%) were female. Like the quantitative sample, most qualitative interviewees were 30 years old or younger (64.3%, n = 18).
STS symptomology
STSS is a 17-item self-report instrument that has three sub-scales which measure the frequency of intrusion, avoidance and arousal in the past 7 days on a five-point Likert-type scale ranging from 1 (never) to 5 (very often). Scores for the full STSS and its sub-scales were obtained by adding the scores for each statement (Bride et al., 2004). Mean total STSS scores for providers did not significantly vary by age, marital status, nationality, or educational level; but they varied in terms of gender. Women had a higher mean score (34.22) compared to men (29.02; p < .05). There were also no prominent differences between mean scores of the STSS sub-scales of intrusion, avoidance and arousal.
In the study, the severity indexing from the STSS indicated that 45.19% of providers met the criteria for little to no STS (n = 47), 26.92% met the criteria for mild STS (n = 28), 10.58% met the criteria for moderate STS (n = 11), 8.65% met the criteria for high STS (n = 9), and 8.65% met the criteria for severe STS (n = 9). A total score of 29–37 was classified as mild STS, a score of 38–43 as moderate STS, a score of 44–48 as high STS, and a score above 49 as severe STS (see Table 1).
Secondary traumatic stress scale findings for service providers working with Syrian refugees in 17 agencies in Istanbul (2018) (N = 104). b
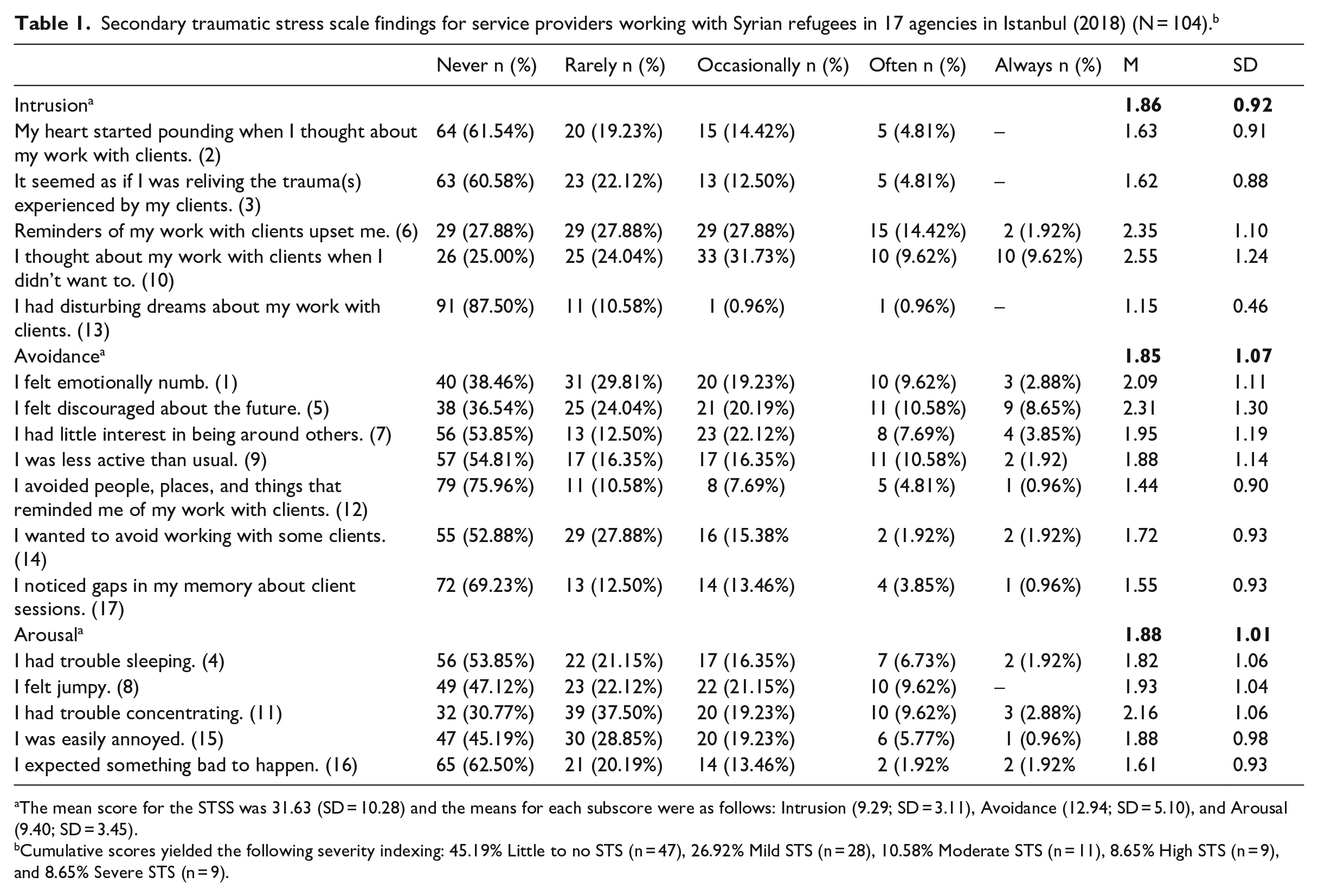
The mean score for the STSS was 31.63 (SD = 10.28) and the means for each subscore were as follows: Intrusion (9.29; SD = 3.11), Avoidance (12.94; SD = 5.10), and Arousal (9.40; SD = 3.45).
Cumulative scores yielded the following severity indexing: 45.19% Little to no STS (n = 47), 26.92% Mild STS (n = 28), 10.58% Moderate STS (n = 11), 8.65% High STS (n = 9), and 8.65% Severe STS (n = 9).
Compared to the quantitative findings, the qualitative interviews present a more in-depth picture of how participants were affected by listening to the traumas of their Syrian refugee clients. Their testimonies show how secondary exposure to suffering, and empathic concern and empathic ability lead to emphatic responses (Ludick and Figley, 2017) in the form of symptoms related to intrusion, avoidance and arousal.
Intrusion
Many of the interviewees reported feelings and thoughts that are congruent with intrusion. For some, the traumatic stories they listened to at work were ‘constantly’ on their mind after work, causing ‘emotional outbursts periodically’ or an inability to ‘adapt back to [their] own lives for a while’:
One night I got up and started to cry and could not stop myself . . . I mean, there were emotional outbursts periodically. (Interview #24, female, 30) Whenever we spend a very dense time with refugees we cannot come out of their world for a while . . . We cannot adapt back to our own lives for a while. (Interview #20, female, 24) When there is a case which makes me sad, I realise I am unhappy the whole day. I have a feeling of sadness even if I experience something good. (Interview #14, female, 24)
In some cases, the recollections were visual, indicating that the imagery does not disappear or re-emerges after a while. Others reported that their clients’ traumatic experiences intruded into their dreams:
The behaviour of those four kids (clients) always appears before my eyes. Their conduct during the interview, their movements, [they] do not go away from my sight. (Interview #1, female, 25) He showed me photos of his three children. He said they had died in the bombing. Another survived with burns. For the first time someone showed me something visual. When I went home, I saw the burns on the child. I saw the burns open. (Interview #11, male, 29) I started having dreams about [a client]. She had a second operation. I constantly saw her mother in my dream, and she gave me the news about her death. What would I do if I really got such news? (Interview #8, female, 25)
Interviews suggest that hearing traumatic experiences might have a greater impact on female providers especially if their clients are women or families with children. This is an observation that is congruent with the quantitative findings that women are more likely to have higher STSS scores:
In one session, one of my clients kept saying she hated men. I came out of that session and hated men for days. (Interview #5, female, 27) If they tell me about how their children go to sleep hungry at night . . . Whenever I hear such things, I especially bond more with female migrants. And I am equally affected when I hear these stories. (Interview #24, female, 30)
Avoidance
Prolonged secondary exposure to traumatic stories of clients may also lead to avoidant behaviour. For instance, a service provider might ‘put up a barrier’ or cease engaging with their Syrian refugee clients:
I got tired of my friends [at work] talking about that sick baby. Many babies are born like that. I think I put up a barrier. It doesn’t make so much of an impact on me. (Interview #10, female, 32) I do not listen to all the torture that the client wants to tell me about. Because if she tells all of it to me then I feel bad. Therefore, I cut it off and refer her to the psychologist. (Interview #16, male, 36)
In addition, diminished affect emerged as a potential link to avoidance. Several service providers reported that they have become ‘indifferent’ or ‘compassionless’ as a result of working with refugees in order to cope with the burdens inherent to their work:
At first, I would feel bad about cases whose problems I could not solve . . . But after some point, I started being indifferent. (Interview #18, male, 26) I have become a colder, tougher person. I saw that sometimes I can be compassionless . . . Unfortunately, being indifferent is the worst. When you take out feelings from life, nothing is left. (Interview #9, female, 29) In order to deal with myself, I no longer empathise with them [refugees]: [I] leave empathy [out] at some point and isolate myself from the situation. Just handle a case, refer her to some place and close her file. (Interview #1, female, 25)
Other important aspects of avoidance reported by interviewees were diminished interest in activities, and detachment or estrangement from others. Many interviewees said they preferred to stay alone at home after work and on weekends. Some also said that their interest in activities or events outside the scope of work was reduced:
I try to go (out) with friends, but I don’t have the energy to follow up with them. Most of the time I am tired. My mind is somewhere else. My mind drifts in sad stuff. (Interview #27, female, 31) On weekends, I just want to sit in the armchair and not get up at all. I do not want to talk to anyone or meet anyone. I just want to stare at the wall. (Interview #1, female, 25) At some point, I feel like I have great distance between me and the others because there is nothing to share with them. . . . My mind is taken with problems, . . . issues at work. (Interview #27, female, 31) My cigarette and alcohol consumption increased. Because drinking and smoking are things I can do and enjoy when I am alone. Other activities require a partner, a friend. I don’t want to get into crowds. I don’t want to talk with someone. (Interview #1, female, 25)
Arousal
Persistent arousal manifested itself in terms of sleeping problems and outbursts of anger. These responses may sometimes stem from frustration due to an inability or failure to solve a client’s problems. Not only the case with which one is dealing but also the legal and institutional context might trigger the sense of frustration, as exemplified below:
Sometimes I lose sleep. I am seriously affected when we are helpless legally and the action that will be taken will violate the rights of the [refugee]. I feel that I am psychologically distressed. (Interview #18, male, 26) The saddest part of the story is that after we found a shelter for this [battered] woman and her children, after they took us to the police station, after we try to solve her story and everything, she went back to him! . . . So because of all this, I have started not sleeping very well. (Interview #15, female, 31).
Several participants reported bursts of anger, having become more aggressive, being impatient or getting irritated easily:
It affects my mood in a way that I cannot feel, sometimes I cannot feel happy . . . It created a negative pattern in my mind so I cannot think out of it. It was hard for me to go and take stuff in the positive way. . . . I am an angry person and the first reaction for me is anger. (Interview #27, female, 31) As a result of listening to too many stories, I became more aggressive, more pessimistic, how shall I say, as if I were living in those conditions and were subjected to that abuse, as if every person was approaching me to hurt me. (Interview #24, female, 30) I get irritated quickly. That’s the effect this job had on me. I become impatient. I become an unbearable guy. . . . My patience level has gone down a little. (Interview #18, male, 26)
Drivers of secondary traumatic stress
The occupational context (workload, short-term contracts, feeling not valued by the organisation) may itself be a precursor or contributor to mental health problems among humanitarian workers (Ebren et al., 2022) in combination with secondary exposure to trauma. As we discuss below, quantitative findings in our study did not elucidate significant associations between employment characteristics and STSS scores; however, qualitative interviews clearly suggest that work-related factors may have an impact on service providers’ likelihood to exhibit STS.
Caseload size and exposure to trauma
In the quantitative sample, caseload sizes varied considerably between psychological counsellors, social workers and other providers due to differences in their work. More than half of the service providers had 20 or fewer cases per week (55.34%); 20.39% had between 21 and 40 cases; and about one quarter (24.27%) had 40 or more cases. Around 85% of the survey respondents said their refugee clients shared traumatic experiences some, half or all the time. The quantitative analysis did not yield an association between caseload size, prevalence of secondary exposure to trauma and STS. Some qualitative interviews showed how providers may be affected adversely by their caseloads, not only in terms of client numbers but also the density of the traumatic stories. One interviewee reported that she experienced more stress during periods of heavier workloads or if their client was especially traumatised, or successive clients shared traumatic stories:
Perhaps the emotional load is heavy here in some weeks according to the people who come . . . In some weeks totally new people come and each one of them has a different problem to be solved. Then it becomes the heaviest work for me because I keep listening to stories (of torture), of problems one after the other. (Interview #24, female, 30) When the workload was reduced, [my emotional outburst] changed. It is quite strange. It comes and goes. (Interview #24, female, 30)
Tenure in profession
According to the quantitative findings, a little more than half (50.95%) and about one third (32.69%) of the respondents had less than 1 year of experience in their current position and in the profession, respectively. Although the quantitative analysis did not indicate any relation between years at work and STS, qualitative findings highlighted that increasing experience might mitigate stress arising from work with traumatised refugees:
Nowadays I do not share such problems too much at home. Because they do not have as much effect on me as when I had first started [this job]. (Interview #4, male, 28) Previously I used to be really affected. I used to think about [traumatic stories told by clients] constantly. But now, after time has passed, I think I have managed to cut that. I now focus on what we can do to help [clients]. (Interview #3, female, 31)
Hiring is project-based in CSOs serving refugees, since they compete for project funding provided by the EU and other international organisations. Projects mean that employment contracts are short term and can only be renewed if the project period is extended or if there are new projects. Many interviewees reported that project-based employment created a sense of uncertainty and inability to accumulate experience or to set targets. Although not directly related to STS, these characteristics of employment might prevent service providers from gaining experience, a potential factor that could protect them from STS-related symptoms:
I was in a different project when I started. Now I am in a different project. . . . [I was asking myself] ‘Will I find a job? Will I continue in the same field?’ . . . That job lasted very short. I wish it had lasted longer. I wish I was able to develop myself more. (Interview #14, female, 24) This is my second project since I got this job. I was in a three-month project. Then it was extended for 1.5 months, making it a 4.5-month project. Now I am in a six-month project. . . . Changing projects all the time, each project has different demands . . . I would also like a one- or two-year project or a longer-term project. At least I could set targets. (Interview #23, female, 24)
Supervision availability
The quantitative findings indicate that about a quarter (26%) of the service providers did not receive any supervision. The qualitative interviews demonstrate that supervision was either irregular or more recently initiated in the CSOs, and there was none in the public agencies covered in this study. Interviewees’ accounts connect a lack of supervision to stress associated with working with traumatised refugees. One interviewee compared her emotional distress level before and after starting to get supervision:
When I first started working here . . . we did not have supervision or support. And I felt really helpless; I had outbursts of anger. (Interview #17, female, 28) [Now] I get [supervision]. As psychologists we take it individually. . . . Since we selected our supervisors, . . . probably for the past nine months, we have a support system for consulting about our cases. Of course, it is very difficult to carry on this work without supervision both emotionally and in terms of the cases. (Interview #17, female, 28)
Some interviewees also mentioned that service providers do not speak enough with each other about their experiences of being secondarily exposed to trauma and are unable to share their feelings with their co-workers. This points to a lack of peer-support in organisations, in addition to the paucity of formal supervision:
The cases are so severe that nobody (service providers) wants to talk about it or share their thoughts. But in fact, they really need to talk about it and share it. (Interview #17, female, 28) All the symptoms we observe in the clients we also see in service providers. They withdraw, they isolate themselves from social life. They don’t want to talk about work, they don’t want to talk about how they feel about it. (Interview #22, male, 25)
Discussion
This mixed-methods study demonstrates that some level of STS is common among service providers working with Syrian refugees in Istanbul. In the quantitative component of the study, more than half of the respondents’ STSS scores pointed to mild, moderate, high or severe STS, with symptoms of avoidance, intrusion and arousal.
The qualitative component of the study shows how empathy with refugee clients who share their traumatic experiences lead to empathy-based stress manifested in terms of symptoms of intrusion, avoidance and arousal among social workers and other service providers. Among the reported symptoms were recollections and dreams related to refugee clients and feeling distressed by reminders (intrusion); diminished interest in and avoidance of activities, detachment from others and diminished affect (avoidance); and sleeping problems and outbursts of anger related to their work with refugees (arousal).
The qualitative interviews also point to possible drivers of STS, although the bivariate analysis in the quantitative component did not yield significant correlates between non-STSS variables and STSS scores (aside from gender). Interviews indicate potential linkages between STS and intense caseloads, secondary trauma exposure and the absence of supervision in the workplace.
The isolation and detachment from activities, friends and family reported in the interviews may be mitigated through supervision for and peer-support among the providers. Psychological counsellors due to their educational backgrounds might be better able to cope with exposure to traumatic experiences compared to providers with degrees in social work or in other fields. Given that social work supervision programmes and research are underdeveloped in Turkey (Şahin-Taşğın, 2019), it is important to develop supervision models that cater to their needs.
The modus operandi of CSOs catering to Syrian refugees also has an impact on caseloads and the paucity of supervision. CSO serve Syrians through short-term projects and providers are often hired for specific projects. Therefore, there is not enough time for building experience and institutional support. Supervision of providers might be an afterthought in many projects, while heavy caseloads may stem from rigid performance requirements.
More than 12 years after the initial arrival of Syrian refugees in the country, institutional capacity building and the development and support of human resources for serving them are essential. The needs of service providers working with Syrian clients should be addressed, especially since this can have a reciprocal effect on the quality of services provided to the refugees themselves. Developing effective social work supervision is crucial, including formal work-related supervision as well as regular peer-support. Moreover, workplace trainings on STS to raise awareness and educational modules in social work departments in universities should be developed to train social workers who will serve refugees.
Limitations of research
While the qualitative findings are not intended to be generalisable, the non-probabilistic technique of the quantitative study restricts the representative nature of the sample. Nevertheless, a convenience sample for the quantitative component likely enabled a higher enrolment rate (100%). Another limitation is that since the study targeted extant employees of agencies, it might have missed service providers who potentially could have higher scores of STSS but who might have already quit their jobs because of an inability to cope with STS. A final limitation is that neither the qualitative nor quantitative component asked providers about their personal trauma history, despite the potential compounding nature of direct and secondary traumas. Although the fact that data was collected in 2018 could be construed as a limitation, the continued presence of refugees and the ongoing expansion of refugee services render the findings still extremely relevant.
Conclusion
Social workers and other service providers have shouldered a significant burden during the reception of Syrian refugees in Turkey. However, they have not received the requisite support from international organisations, public authorities and CSOs which either fund their work or employ them. With little organisational and institutional support and strained by heavy caseloads with traumatised refugee clients, they are exposed to secondary trauma and may suffer from other mental health problems (Brooks et al., 2022).
This article is one of the first to examine STS among social workers and other providers working with Syrian refugees in Istanbul through a mixed-methods study. The findings contribute to the literature by identifying the incidence and manifestations of STS among providers and pointing to potential drivers such as stressful working conditions and weak supervision. In particular, the study shows that project-based programmes targeting refugees create an uncertain work environment in which accumulation of experience is impeded and professional support is often an afterthought. The study points to a need for developing interventions to address secondary traumatic stress such as supervision and peer-support programmes. The findings are also a reminder that social work practice and social policy making in Turkey should incorporate the needs of those helping refugees more fully.
Supplemental Material
sj-docx-3-isw-10.1177_00208728241277924 – Supplemental material for Manifestations and drivers of secondary trauma among service providers working with Syrian refugees: A mixed-methods study from Istanbul, Turkey
Supplemental material, sj-docx-3-isw-10.1177_00208728241277924 for Manifestations and drivers of secondary trauma among service providers working with Syrian refugees: A mixed-methods study from Istanbul, Turkey by Deniz Yükseker, Melissa Meinhart, Uğur Tekin, Neşe Şahin Taşğın, Elif Demirbaş, Anindita Dasgupta, Neeraj Kaushal and Nabila El-Bassel in International Social Work
Supplemental Material
sj-pdf-1-isw-10.1177_00208728241277924 – Supplemental material for Manifestations and drivers of secondary trauma among service providers working with Syrian refugees: A mixed-methods study from Istanbul, Turkey
Supplemental material, sj-pdf-1-isw-10.1177_00208728241277924 for Manifestations and drivers of secondary trauma among service providers working with Syrian refugees: A mixed-methods study from Istanbul, Turkey by Deniz Yükseker, Melissa Meinhart, Uğur Tekin, Neşe Şahin Taşğın, Elif Demirbaş, Anindita Dasgupta, Neeraj Kaushal and Nabila El-Bassel in International Social Work
Supplemental Material
sj-pdf-2-isw-10.1177_00208728241277924 – Supplemental material for Manifestations and drivers of secondary trauma among service providers working with Syrian refugees: A mixed-methods study from Istanbul, Turkey
Supplemental material, sj-pdf-2-isw-10.1177_00208728241277924 for Manifestations and drivers of secondary trauma among service providers working with Syrian refugees: A mixed-methods study from Istanbul, Turkey by Deniz Yükseker, Melissa Meinhart, Uğur Tekin, Neşe Şahin Taşğın, Elif Demirbaş, Anindita Dasgupta, Neeraj Kaushal and Nabila El-Bassel in International Social Work
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Columbia University President’s Global Innovation Fund (2016–2018).
Supplemental material
Supplemental material for this article may be requested from the corresponding author.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.