
Abstract
COVID-19 has had a significant and measurable impact on individuals and families in economically deprived areas both in the United Kingdom and internationally. This article examines issues of community resilience and service adaptability and focuses on the period during the first lockdown in the United Kingdom (May to July 2020). Data were collected from members of the local community in Southend, with specific reference to the ‘A Better Start Southend’ programme of support. The evidence presented in this article uncovers the impact of the ‘first lockdown’ on families with young children, and local children’s and community services.
Introduction
As knowledge of the epidemiology and pathology of coronavirus improves, governments across the globe have been able to develop more nuanced public health responses in comparison to the period of what is now known as the ‘first wave’ of the pandemic. In most European countries, this refers to the period late February to mid July 2020. The roll-out of a vaccine has provided opportunities for the development of approaches that are based on immunisation as well as the dynamic assessment of the vulnerability in specific population groups. Notwithstanding the appearance of COVID-19 variants, communities, in much of the world, have gradually entered a phase of the pandemic where policy making has largely moved away from generic and indiscriminate restrictions.
Despite the advances on the medical front, persistent questions about the handling, especially in relation to some of the most marginalised section of our society, remain. In a widely read Lancet editorial, Abbasi (2021) explained how ‘more than a few countries have failed in their response to the virus’ and supported calls for governments to advance equity, reinvent and modernise the global pandemic alert system, take pandemic threats seriously, and cooperate better with other nations and the World Health Organization (WHO). Social science researchers have already started investigating the ‘biopolitical’ dimension of COVID-19, highlighting the complex socio-political dilemmas emerging from state action – or inaction – in the context of the COVID-19 pandemic (see, for example, Clover, 2021; Kapilashrami et al., 2021; Lavalette et al., 2020; Levine and Manderson, 2021; Mannion and Speed, 2021). For the current pandemic, once again, demonstrates how biology and the interaction between humans and their physical environments are profoundly political and contested areas (Ioakimidis, 2020).
Indeed, there is an urgent need for a thorough exploration of both central government and civil society responses to the pandemic. Not only for purposes of transparency and accountability but also for ensuring that missteps will not be repeated as humanity enters a period of global uncertainty, owing to climate change (Intergovernmental Panel on Climate Change, 2021). It is for this reason that the period of the ‘first wave’, a period of unprecedented collective uncertainty and distress, is of particular importance for the study of community resilience and service adaptability. There has been demonstrable interest in this area, particularly on the challenges faced by practitioners and frontline workers during the pandemic (see, for example, Johnson et al., 2021; Nyashanu et al., 2020).
When considering the challenges of the pandemic, the experience of the first lockdown had a clear impact on the mental health of adults across the United Kingdom (Pierce et al., 2020). By implication, the findings from recent studies clearly have resonance with the experiences of families and young children – especially in poorer coastal towns in the United Kingdom, such as Southend-on-Sea. In support of this claim, recent evidence on the impact of COVID-19 restrictions, and early lockdown, on child and adolescent mental health is unequivocal: high levels of distress among school-aged children and young people aged between 4 and 16 years have been observed and reported (Waite et al., 2020). For the population of economically deprived areas of Southend, the negative impact of the pandemic – and attendant COVID-19 restrictions – on individual mental health further illustrates the potential for long-term social and economic consequences. A recent study conducted by the IFS (Institute for Fiscal Studies) quantified the impact of first 2 months of lockdown on mental health. Its findings show that, compared with pre-crisis trends, mental health in the United Kingdom – as a whole – worsened by 8.1% (Banks and Xu, 2020). For health and social care practitioners, findings from recent research on the psychosocial impact of the pandemic found that fatigue and exhaustion were commonly reported complaints (Aughterson et al., 2021).
This article aims to contribute to this debate through the presentation the findings of a research study which focused on the experiences of families and practitioners involved in ‘A Better Start Southend’, an extensive 10-year programme of free services to families with babies and very young children (age 0–4) in the six most economically deprived wards in Southend. Data collection took place during the period of the first lockdown (data collected between 4 May 2020 and 1 July 2020).
Aims
The aims of the study were to examine the following:
The impact of the first wave of COVID-19 pandemic and lockdown restrictions on families with babies and very young children in A Better Start Southend wards;
The impact of the first wave COVID-19 pandemic and lockdown restrictions on local children’s services and wider community organisations;
How A Better Start Southend (ABSS) services could respond effectively so that they can continue their work to improve the health and wellbeing of very young children and their families in Southend during the pandemic and its aftermath.
ABSS is a UK National Lottery funded programme which addresses the link between economic deprivation and poor life chances. It provides free services to families with babies and very young children (age 0–4) in the six most economically deprived wards in Southend. The programme aims to improve children’s diet and nutrition, social and emotional development, and speech, language and communication, thus improving their longer term life chances. The COVID-19 pandemic and associated ‘lockdown’ restrictions have changed daily life across the whole of the United Kingdom, in ways that will likely have long lasting consequences for individuals, families and communities. These consequences will be impacted by economic deprivation.
There is a well-established link between economic deprivation, ill health and poor life chances. For example, healthy life expectancy for males in the most deprived areas of England is 51.7 years, compared to 70.4 years in the least deprived areas (Public Health England, 2019). Early figures on COVID-19-related deaths suggested that individuals in areas of economic deprivation are more likely to die as a result of the virus than those in the least deprived areas. Rates for deaths occurring between 1 March and 31 May 2020 show that in the most deprived areas of England, the mortality rate for COVID-19 was 128.3 per 100,000 population, but in the least deprived areas, it was just over half that at 58.8 per 100,000 (Office for National Statistics, 2020). In addition, evidence suggests that certain social groups may be particularly detrimentally affected by COVID-19, including multigenerational families in crowded housing (Kenway and Holden, 2020) and certain minority ethnic groups (Platt and Warwick, 2020). According to figures for the total number of COVID-19 cases by lower tier local authority (up until 19 July 2020 to the period of study), the rate was 379.3 per 100,000 population for Southend-on-Sea. This compares to Leicester, which had the highest rate of 1289.1 per 100,000, and Torridge (in Devon), which had the lowest rate of 77.8 per 100,000 (GOV.UK, 2020).
This research received ethical approval at University level ensuring that confidentiality, anonymity and research governance procedures were observed to the highest level. There have been two phases to this research. Phase 1 informed a preliminary report and involved surveys with parents and focus groups with practitioners. Phase 2 involved interviews with parents and leaders in key organisations in Southend. Insights from both of these phases have been combined into this article. COVID-19 will alter the priorities of ABSS services and the ways in which they work with families.
This study is based on findings from three research methods undertaken with three different groups. These were online focus groups with frontline practitioners, a survey with parents and qualitative interviews with parents and key stakeholders (service leaders or managers in local organisations). Our data were collected between 4 May 2020 and 1 July 2020. It is necessary to contextualise the timing of the research, and the time periods in which each of the methods was conducted, in relation to the different ‘stages’ of lockdown in the United Kingdom. Table 1 outlines these stages.
Changes in lockdown restrictions in 2020 in the United Kingdom.
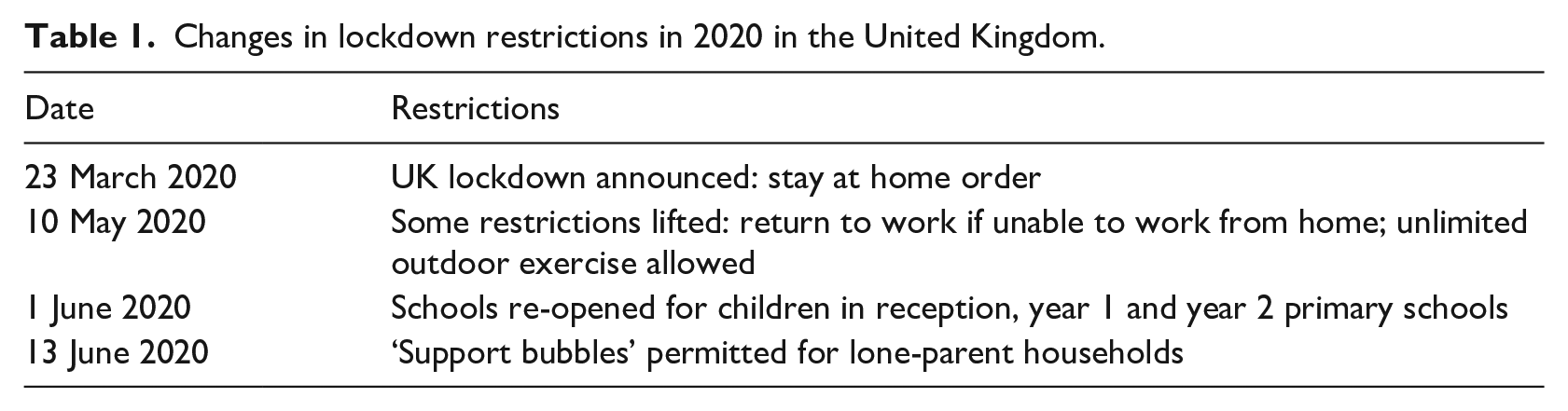
The specific time periods in which the individual methods were conducted are outlined in the description of each method that follows.
Focus groups with practitionersA total of nine frontline practitioners took part in one of three focus groups. These practitioners worked across a range of services, including those focused on breastfeeding support, speech and language, parent and community engagement, employability, family support and mental health. The focus groups ran online (on Zoom) and each lasted approximately 1 hour.
Focus groups were conducted between 30 April and 13 May 2020, and therefore reflect the experiences of practitioners during the strictest period of lockdown. Participants discussed the contact they had had with families during the pandemic, the ways the services they worked in were currently running and perceived difficulties and successes within this, challenges and difficulties faced by families during ‘lockdown’ as well as benefits, community and service responses in the local area, and ideas about what services, support and opportunities would likely benefit families.
Survey of families
An online survey was made available to families in Southend through a dedicated webpage, a link to which was shared on ABSS social media pages and emailed to potential respondents by practitioners working in ABSS services. The survey was live for the whole breadth of the research period, and was completed by participants between 4 May and 1 July. A total of 50 families responded. All but one respondent was female (n = 49), and 88% were White or British (n = 44). Respondents’ ages ranged from 20 to 59, with 64% (n = 32) in the 30–39 age bracket. There were no respondents from ‘young parent’ age groups (i.e. younger than 20 years). Nearly all (n = 46), currently had at least one child age 0–4 in their household. In total, 41 respondents lived with a partner. The total number of individuals in each household ranged from two to seven. The typical household included the respondent, a partner, and two or three children in the 0–4 and 5–10 age brackets. Ten respondents had responsibility for one or more children (aged 0–18) with a special educational or learning need, while three had responsibility for one or more children with mental health or emotional or behavioural difficulties and two for children with a serious medical need. Two respondents had a child or children receiving support from social services. Seven respondents suspected they have had (or currently have) COVID-19, but none had been diagnosed. Six reported that another member of their household has had suspected COVID-19. In three households, this included a very young child (0–4). Just over half of respondents (n = 28) had used an ABSS service within the previous 2 years.
Interviews with parents
Survey respondents were asked to leave their name and contact details if they were interested in taking part in further research. These individuals were invited to participate in a qualitative interview, and a total of five parents, all of whom were female, agreed and took part. Interviews were conducted over video platform (Zoom) or by phone between 5 June and 25 June 2020. Interviewees had therefore lived through the whole period of the strictest phase of lockdown, and some restrictions had been lifted when they took part.
Most interviewees (four) were aged 30–39, and one was 40–49. One interviewee was ‘Black/Black British’, and all others (four) were ‘White’. Most interviewees (four) lived in A Better Start wards (two in Kursaal, one in Milton and one in Shoeburyness), and one lived in Southchurch. Interviewees had between one and three children and all had at least onc child who was age 5 or younger. Three interviewees had a child (or children) who were very young (between 18 months and 30 months). Four interviewees lived with a partner, and one was a single parent. Most interviewees (four) were in paid employment at the time of the interview. One had been furloughed, two were working from home and one was a key worker who was still working outside of the home (in a care home).
Interviews with key persons
Qualitative interviews were also conducted over Zoom with four ‘key persons’, all in leadership or managerial roles in local organisations. The interviews took place between 29 May and 1 July, meaning that at least some restrictions had been lifted. Two of these interviewees were involved in leading children’s services, with one working primarily with children’s services and social care, and one in children’s public health. In these cases, interviews were conducted to gain insight into the impact of COVID-19 on children’s services, the adaptions services have made, and potential longer term consequences for services and service users. The third key person was a professional whose managerial role involved working with individuals who have experienced high-risk domestic abuse. This individual was interviewed specifically for their insight into matters related to domestic abuse during the COVID-19 period. The fourth key person was a member of the police, and this interview was conducted to provide insight into wider community responses and challenges.
Challenges and difficulties experienced by families
Findings from the survey and interviews with parents and focus groups with practitioners suggest that families experienced a range of challenges and difficulties during the first wave of the pandemic. These include those that relate to relationship stress, accessing food and medication, mental health and wellbeing, children’s needs and schooling at home, employment and income, and social distancing.
Findings relating to each of these areas are presented below. It is noteworthy that among practitioners, reports about families’ experiences during the pandemic differed in accordance with the service that practitioners worked in. This is because different services address different needs and work with different social groups. For example, a practitioner working with families who struggle with mental health difficulties may report the impact of COVID-19 particularly in terms of how this has contributed to or exacerbated mental health struggles, but these struggles will not be present to the same extent across all families and social groups in A Better Start wards.
Relationship stress and domestic abuse
Half of the survey respondents (n = 21) reported some extent of stress or worry about relationships. Survey findings show that 7 out of 42 (17%) respondents indicated that they were ‘very stressed/worried’ about their marriage or romantic relationship, and 14 (33%) indicated that they were ‘somewhat stressed/worried’.
Four of the interviewees lived with a partner, and two of these described how a pre-existing concern in their relationship with their partner was exacerbated by the lockdown situation. One interviewee (who had three children and had been shielding) explained that her partner had needed to take on extra work in order to financially provide for the family. This meant that he had spent a lot of time away and this put a strain on their relationship. The pandemic worsened this because he had taken up accommodation away from home so that he could work without bringing the virus home to his family. The other interviewee described how lockdown had put added pressures on the relationship with her partner, which was already under strain. At the time of the interview, they were negotiating ending the relationship.
In the focus group, some practitioners described having observed an increase in the amount of tension and stress between adults in the families they worked with, and the general perception was that this was worst for those families who were already experiencing ‘disharmony’ or social or communication difficulties prior to the pandemic. A practitioner working with young mums explained that family relationships had become more strained than usual, and that the individuals she works with are often already experiencing difficult relationships. They understood that relationship difficulties were exacerbated by certain living arrangements during lockdown, such as when a young mum lives in family homes where tensions are present or lives alone.
Concerns about domestic abuse were raised during focus groups. One practitioner explained how this was a ‘massive concern’ for their service and shared their concern that the channels through which practitioners might ordinarily come into contact with individuals experiencing domestic abuse were currently ‘closed off’.
The key person in domestic abuse was involved in multi-agency working with high-risk cases, where there is an immediate risk of serious harm. They shared their views on the decrease in reported cases. Their understanding was that a lot of domestic abuse had gone unreported because it is much harder for a victim to report an abuser in lockdown due to them being constantly present. They described how one avenue that is sometimes open to victims to get help is to do this when taking children to school, but that this avenue had not been available when schools closed. However, they also noted that it could also be the case that if someone is not living with the abuser, it may make it harder for them to then attend the address and be abusive.
The key person also explained that ordinarily, 70% of high-risk domestic abuse cases are referred from police. However, during the fortnight prior to their interview, there had been an increase in reports to other agencies and individuals had used the local commissioning service more than the police. They explained that this was likely a result of communications from services at the beginning of lockdown, which were shared in anticipation of an increase in domestic abuse and/or restricted opportunities for victims to report domestic abuse. These communications advertised that services were still accessible, and were shared through social media, websites and posters in supermarkets.
The key person had discussed with colleagues the discrepancy between their own referral rates (which had seen a decrease during lockdown) and the national increase in calls to domestic abuse helplines during the same period. Their personal suggestion was that people reporting to national abuse helplines had been involved in domestic conflict more so than high-risk domestic abuse. The key person also reflected on the impact of domestic abuse during lockdown on children, describing how they are likely already anxious about COVID-19 and may now also be witnessing domestic abuse during the day, without ‘escaping it’ by attending school or seeing friends or grandparents. Moreover, they explained that domestic abuse victims are unlikely to be able to emotionally support the child and meet their needs if they are overwhelmingly focused on coping with, and managing the risk of, abuse on a daily basis.
The key person in the police also described the reduction in reports of domestic abuse to the police during COVID-19, but, like others, emphasised what they called the ‘hidden harm behind closed doors where people are confined to premises’ and unreported domestic abuse. They expressed that ‘identifying that hidden harm and what’s going unreported is the priority’.
Accessing food and medication
Almost three quarters of survey respondents indicated that they had found it more difficult to access food during the pandemic. The reasons given were usually a lack of availability of food items in shops (including specialist items), shops being too busy, and being unable to access online food deliveries. Responses indicate that these issues were particularly a problem for those who could not leave the house or queue in shops easily, due to not wanting to expose children to the virus, having a new-born baby, a disability or being medically vulnerable. No survey respondents attributed the problem of accessing food to a reduced income, and although one respondent indicated that they had used a foodbank during the pandemic, this was not the first time they had done so. It is likely that reliance on donated food and an inability to afford food is prevalent among the most economically deprived and marginalised groups, who are unlikely to have completed the survey.
Just over a quarter of survey respondents indicated that the pandemic had made it more difficult to access medication. Respondents’ descriptions of this usually referred to the reduced availability of paracetamol-based painkillers and allergy medications in shops. However, other problems were also reported, such as not being able to contact a General Practitioner (GP), not being aware of changes in accessing repeat medications, and not having the relevant appointment to discuss medications. This suggests that the reduced capacity of GP services was problematic in relation to medication use. Interviewees did not discuss any particular problems accessing food or medication, apart from having to be ‘strategic’ in order to access online shopping. One interviewee also described finding ‘social distancing’ difficult in supermarkets.
Occasional cases of food poverty were described by a small number of practitioners in focus groups, and some had had contact with families who were relying on food parcels. Practitioners attributed difficulties accessing food to both financial struggles and self-isolation or other practical difficulties. Practitioners also discussed the national problem of an inability to access food due to food shortages and how this was particularly difficult for some groups, such as families with young children who are not flexible in what they eat, and individuals with specific anxieties around certain foods.
Health and wellbeing of parents
In the survey, 10 respondents (20%) indicated that they had a diagnosed medical condition or disability, seven of whom felt that this had worsened during the pandemic. Most of these seven respondents had depression or stress and anxiety, sometimes in addition to physical conditions. When discussing aspects of the survey with participants, we were able to explore explanation of why their problems had worsened, for example: Anxiety around pregnancy and birth made worse by the current outbreak and having to spend time at the hospital. Haven’t been able to have time with family and friends and have felt isolated. I can’t access regular medical appointments or blood tests for check ups
When asked whether they had felt stressed or worried about their own mental health or emotional wellbeing during the pandemic, a large proportion of respondents (83%) indicated that they were ‘somewhat’ or ‘very’ stressed/worried.
Three of the five interviewees (families) described a struggle with anxiety and/or their mental wellbeing during lockdown. Two of these explained that their pre-existing struggles with anxiety had worsened during lockdown. One, who lived with a partner and two children (aged 8 and 4), identified a number of factors that had contributed to this, including a loss of her usual forms of social support, working from home and the risk of being redeployed at work. She explained that she had had to stop spending one night a week at her mother’s house because she was vulnerable and had also had to stop seeing her friends: I [ordinarily] do lots of other things like going to see friends to keep the talk going, they’re like my own therapy. It’s not the same over the phone.
The other interviewee who had experienced exacerbated anxiety was a single mum to an 18-month-old. She found being furloughed from her part-time job difficult because it ordinarily helps both her and her son to spend some time away from each other. She also felt anxious about leaving the house due to concerns about the virus, which were worsened by others not adequately socially distancing. Anxiety about leaving the house was not a new experience for her, but had taken on a new form during the pandemic. At the time of the interview, she had recently begun therapy following a long period on a waiting list.
Practitioners in focus groups explained their views that individuals ordinarily struggling with relationship difficulties, anxiety and/or low mood were finding their struggles worsened by a lack of contact with family members. Specific examples they gave included young mums with relationship difficulties lacking support and parents with social anxiety being unable to benefit from the support of their own parents who would ordinarily take their children out for them. There was also an example given of a young mum experiencing extreme social isolation.
One practitioner explained that some parents felt isolated and were missing the simple, everyday contact with others, such as other parents at school. They felt that this was especially the case because these parents are used to being in social groups and supporting each other: [A concern is] parent isolation, having adult contacts. Even if it’s when you’re at school, having a chat in the playground really, dropping the kids off. That’s been a really big thing [. . .] the parents we work with [. . .] are very used to being in those social groups and supporting each other.
Findings from across all different strands of data collection showed that the emotional and mental wellbeing of parents during the pandemic is a concern for many families, and that there has been a reduced capacity for informal support (from friends and family) to alleviate this in the usual way.
Children’s needs and development
In the survey, just over half of respondents indicated that, for their child or children aged 0–4, they were ‘more worried than usual’ about their learning or development needs. Two thirds of parents were concerned ‘more than usual’ about the emotional health of children age 0–4, while over half were more concerned than usual about their child’s health, the amount of exercise their child is getting and enjoying relaxed time with their child. All three interviewees who had children who were younger than school age (between 18 months and 30 months) explained that being unable to take their child or children to play groups and other structured activities and/or nursery during lockdown had been a source of worry and concern.
An interviewee who was a single parent to an 18-month-old explained that she had begun to feel sad and anxious after about 4 weeks in lockdown. She worried about her son ‘missing out on integration with other children and adults’. She went on to explain that while her son is usually very sociable, she noticed that he had ‘declined a little bit’ when they recently met a new childminder. Another interviewee described how prior to lockdown, her son had been doing very well at nursery and progressing well in his physical and verbal skills. She had been concerned about not being able to ‘keep that momentum going’ during the lockdown. She had also experienced guilt seeing other families on social media doing ‘these amazing activities’ that she did not have the time or resources to do, and this had added to her worries about her son’s development. At the time of interview, her child was attending nursery again and she felt that this was the right place for them to be.
In the focus groups, practitioners suggested that some families are experiencing a ‘daily struggle’ during the pandemic. Frequent examples were offered of individual families finding it very challenging to meet children’s needs. It was suggested that it was particularly difficult for families with a child with special needs or an autism spectrum disorder diagnosis, for parents who are single or disabled, and for those living in very small or overcrowded properties and/or who are self-isolating for long periods.
One practitioner described working with parents who were struggling with their children’s ‘fussy eating’. This practitioner understood this in terms of a broader change in behaviour in the children during lockdown, which also included the child being more attached. The practitioner attributed these behaviours to factors such as a change in routine and the child having fewer opportunities to be independent (e.g. at nursery). However, this practitioner felt that their work with these families had been ‘positive’, and that on the whole most families ‘have been OK’.
Children’s living conditions
Related to the issue of children’s wellbeing is their living conditions and access to outside space during lockdown. Most respondents (86%, n = 43) reported having access to outside space, including 31 (62%) who had a private garden. A small number of respondents (n = 7) reported not having any access to outside space.
It may be that those without private access to outside space found it difficult to spend time outside with very young children during lockdown. This was a concern raised by a practitioner in a focus group, who discussed parents’ finding it difficult to spend time outside with very young children due to them feeling they need to keep ‘on the move’ and because it is sometimes difficult to prevent very young children from going near others. It was also raised by an interviewee with an 18-month-old child. She found it difficult to manage being in a public space with her child because she felt she was constantly telling them ‘no’, and that it was easier to keep themselves at home. She explained that she was unable to make use of the more ‘relaxed’ government guidelines that allowed groups of up to six to meet so long as they were socially distanced: When you’ve got rules in place that you can’t go within two metres of someone, how can you get an 18 month old to do that?
When asked how stressed/worried participants felt about their living conditions (which could include concerns about access to outside space), 70% (n = 32) indicated that they were not at all stressed/worried, and 30% that they were ‘somewhat’ stressed/worried (n = 9) or ‘very’ stressed/worried (n = 5).
All interviewees had private gardens that their children used regularly during lockdown and most explained that this was a ‘great help’ or that they considered themselves ‘lucky’ to have a garden because of its importance during lockdown. For one interviewee who was shielding and for another who struggled to leave the house due to anxiety, the garden had been especially important as the only way that their child or children were able to spend time outside. Some interviewees described their reliance on spending time outside away from the house with their children, such as by going on daily walks nearby or driving to somewhere for picnics where it was not too busy.
Employment and income
Among the 50 survey respondents, 31 were in paid employment (some of whom were also volunteers, attending university or on maternity leave) at the time of completing the survey, and 19 reported being a homemaker or full-time parent. Two thirds reported that their employment status and the nature of their work had not changed during the pandemic. Of the 17 for whom this had changed, six reported that they were now working from home, five that they were furloughed, and six had experienced other changes, such as taking maternity leave early or working fewer hours. In total, 27 of the 50 respondents reported that either they or a member of their household is currently working as a key worker. Half of these households had someone who works in health or social care, and a quarter had someone who works in education and childcare. In total, 41 respondents reported that there is another adult in their household who contributes to household income. In total, 31 of these adults were in full-time employment and five were self-employed. For many, the other adults’ employment status had not changed during the pandemic although seven were now working from home. Eight had been furloughed and two had been made unemployed (among other changes).
Of the 50 respondents, 19 indicated that their household income had decreased during the pandemic, and nine stated that they had put in a new claim for benefits. While seven of those who had applied for new benefits said that the application process was not at all difficult or challenging, one said it was somewhat difficult or challenging and one said it was very difficult or challenging. In total, 11 of the respondents who reported a decreased income indicated that they were not experiencing any problems paying for essentials such as food and rent, but six indicated that they may experience some problems paying for essentials, and two that they definitely will. The survey findings suggest that there may be a proportion of families who have been negatively impacted financially by the pandemic, and an increasing number claiming benefits. However, only a small number of respondents stated that they were ‘very worried/stressed’ about work or employment. Around half were ‘somewhat stressed/worried’, and the remainder were not at all stressed or worried.
None of the interviewees (families) described experiencing any overwhelming financial difficulties as a result of the pandemic. However, two did refer to struggles in this area. One was an interviewee with three children, who described how the financial pressures of being a family of five meant that her partner had to work a lot and missed out on family time. However, this was a pressure that was not specific to the pandemic. Another, who was a single parent who had been furloughed from her part-time job, had experienced a drop in income. She described having to use strategies such as shopping at a cheaper supermarket in person to manage this.
Overall, in line with findings from the survey, practitioners’ perceptions were that there had not been a significant impact on individuals’ income or employment among the families they worked with, apart from in a small number of cases. It was reported that mothers on maternity leave were not problematically affected, and nor were those on universal credit. For some practitioners, these groups accounted for the majority of individuals they worked with. One practitioner reported how among young mums, there was concern initially when partners were unable to access any work (due to being on zero hours contracts or working for family), but that they have since accessed universal credit.
Benefits experienced by families
It is important to highlight that participants to our study were also able to identify areas of improvement during the pandemic. Of the respondents to the ABSS survey (see Figure1) who completed the relevant questions, all identified at least one area in which they had experienced a little or lot of improvement during the pandemic, and most indicated two or more areas.
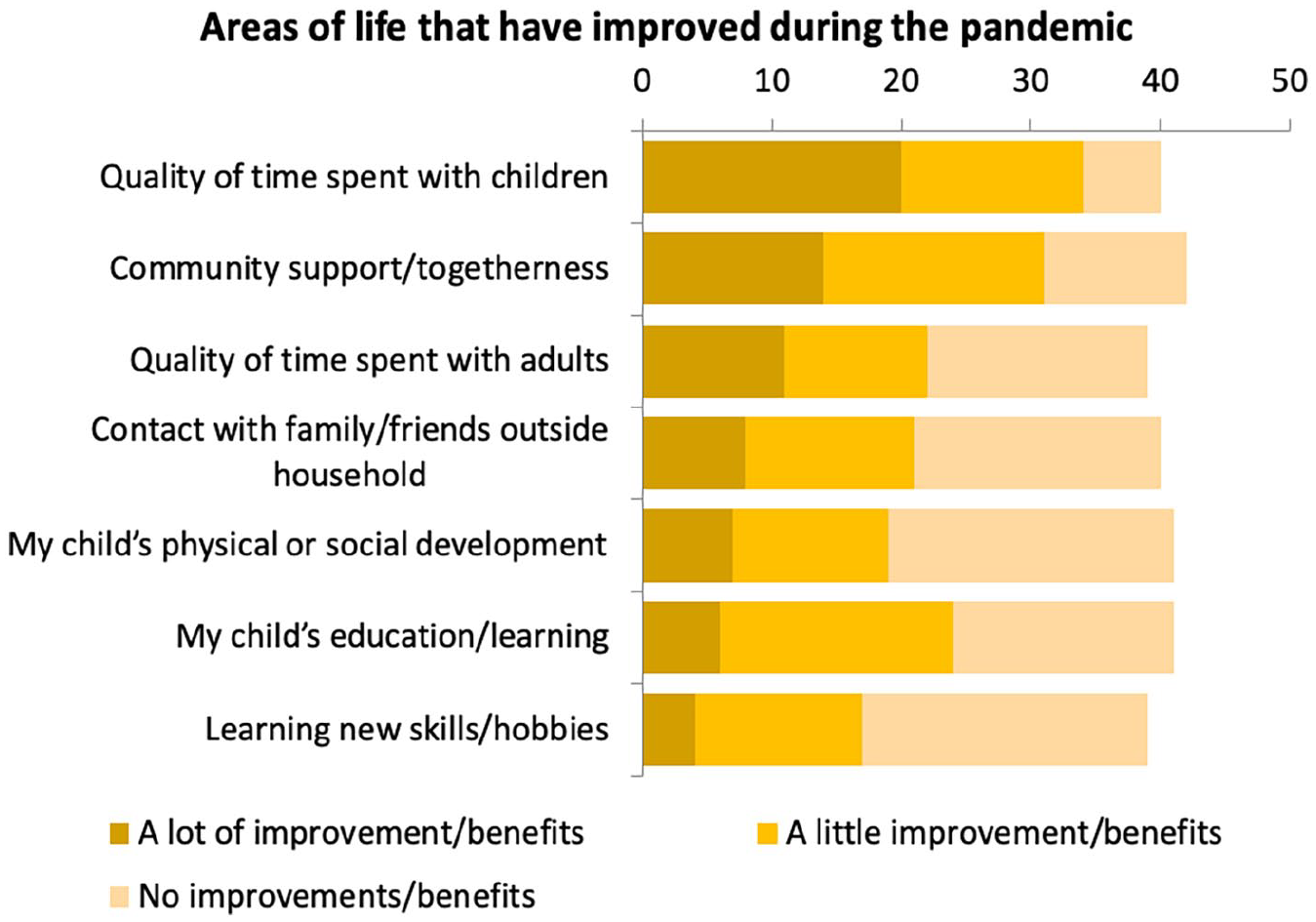
Areas of life that have improved during the pandemic in the United Kingdom.
These responses included brief descriptions of how the area of life in which there had been the most benefits had improved during the pandemic. Most respondents described improvements in spending more time with children, having a partner at home and/or spending time together as a family. For example, . . . it’s been really beneficial to have quality time with my children without all the added outside pressure to keep up with expectations. . . . My child having her father and mother in the home for more time. . . . my husband cannot work due to lockdown, therefore he has taken on the primary care giver role, and now understands the frustrations and challenges that come with this role.
Some also described improvements in their child’s learning and development or community-related benefits. Examples include, My children have improved in their academic skills from 1:1 daily input. . . . My sons’ speech has improved and my daughter seems more confident in her own abilities. A sense of community has now enabled our whole street to communicate via WhatsApp and to help those in need down the street . . .
Four of the interviewees described having benefitted in some way from additional time together as a family. Two explained that the extra time they had had with their children had been positive. One spoke of the increase in ‘bonding time’ through getting the children more involved in daily tasks, such as making dinner together. Another explained that the 3 months she had spent in lockdown with her son were extremely valuable, despite her worries about the developmental impact of him missing out on nursery: He amazes me daily, and he shows me he’s learnt something else. On that side of it it’s been an amazing three months. I don’t want this to be our life, that’s the thing. But yeah, it has been nice spending time with him and seeing all these little quirks that he’s learned. He’s funny, he makes me laugh
Two other interviewees (families) described enjoyable time together as a whole family, or a beneficial shift in family roles. Regarding the latter, one interviewee explained that her partner had benefitted from being involved in aspects of daily life looking after their children that he was not ordinarily involved in due to work, and that because he is now working from home rather than going away for work for periods during the week, he is enjoying ‘being able to see the whole piece’.
Four interviewees described benefits in terms of community support during the pandemic. Three of these explained that neighbours would look out for each other more, such as by offering to pick up items when going to the shops. Two also cited the ‘clapping for the NHS’ events as inciting a feeling of community spirit and being a chance to see and wave to neighbours they had not seen previously.
One interviewee who was shielding and who had had support from neighbours, her local church and a mother and baby group she used to attend, explained, That community spirit, calling and checking up on each other. Before, we didn’t have that. Once you might see that person on the street, oh hello, is everything OK? And now, for you to pick up the phone, just call them, check up on them, have a bit of a chat, it has really been good.
Another interviewee described her wish to support others in her community: There could be people that live over the road or live next door that just need something. I think that’s been really lovely, and it’s paying a bit more attention when I go to the shops [. . .] making sure that you do make contact with people, obviously at a distance, but I think sometimes that can make someone’s day, they might not have anyone. I think it’s been really good, really positive.
A practitioner in one focus group stressed the importance of recognising positive aspects of people’s experiences during this time, and what they have achieved: I think it’s easy for us all try and find a problem to solve, and I think that one thing that is missing from this discussion is the positives that have happened. You know, what are the parents doing that is incredible, given the current situation. There’s so many things in the community – positive things.
Practitioners generally understood that families had benefitted from spending additional time together as a family. More specifically, practitioners suggested that for those with young babies it has been beneficial to spend time together as a family without the stress of going to work (for those who are furloughed).
A practitioner working in speech and language services reported mostly hearing positive feedback from parents during the lockdown. They explained that parents of children with delayed language have appreciated the time spent with their children with less rushing around, and that they feel more in control (as opposed to the therapist). Parents have also reported that their child’s language has improved as a result. (However, this was not the case for those diagnosed with Autism Spectrum Disorder (ASD) – see above).
There were reports from one practitioner of babies breastfeeding more frequently due to families spending more time together and being in closer contact. There was also a report of instances of mothers switching from combination feeding to purely breastfeeding due to concerns about accessing formula milk. There was a discussion of the positive impact of individuals breastfeeding in terms of bonding for the mother and baby, and it was reported that some women had described breastfeeding during this time as ‘calming’. It was also suggested that people learning about antibodies to COVID-19 in breastmilk is a possible reason for individuals wishing to continue breastfeeding.
Other examples of positive experiences discussed in the focus groups included the following:
Young mums being very creative and resourceful finding ways to entertain their children indoors;
A particular family who had previously been a concern for a practitioner being resourceful, communicating well and finding ‘hidden depths’ during this time;
A family whereby a woman who has four children found that they have become closer during this period and the family is more relaxed;
Young families experiencing role changes. Where male partners were not usually at home for their baby’s bed time routine due to the nature of their work (e.g. night workers, factory workers), they now were, and this has been a benefit to some families.
Conclusion
This study focuses on the experiences of health and social care practitioners as well as families with young children who engage with the ABSS programme during the ‘first wave’ of the pandemic. As our findings suggest there have been a wide range of challenging and positive experiences among families in Southend. At the ‘worst end’, COVID-19 may have exacerbated or contributed towards food poverty and other difficulties accessing food, domestic abuse and other problematic family relations, mental distress and behavioural difficulties in children. However, for others, the situation may not have posed serious difficulties and for some may have provided benefits and opportunities, such as spending more time together as a family, strengthening social bonds and community support, less distracted time with babies and young children, and a beneficial shift in social roles within the family. The overall picture for families, services and organisations has been one of challenge, pressure, rapid adaption, and sometimes, opportunities.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by The National Lottery Community Fund as part of the broader `A Better Start Southend’ evaluation project.