
Abstract
This study investigates the relational dimensions that shape clinicians' intentionality and motivation for knowledge-sharing. Qualitative data was collected from 40 clinicians in two hospitals, and relational models theory was used to investigate the impact of different relational models (communal-sharing, authority-ranking, equality-matching and market-pricing) on clinicians' intentionality and motivation to engage in knowledge and learning. While communal-sharing and expert-based authority–ranking relationships predominantly encourage intra-professional knowledge-sharing, equality-matching encourages inter-professional knowledge-sharing. This implies that while the idea is to work together to improve public service quality, each actor has their own interests and is motivated to share knowledge for different collective and/or personal reasons/agendas. In the public sector, formal authority-ranking and market-pricing are the main driving forces of coordination of actions and knowledge flow, through the medium of money and trade. Despite this, power games and a lack of support from those in positions of authority and ignorance of potential conflicts of interest, as well as extrinsic motivators, hamper knowledge-sharing, all of which threaten patient safety.
Points for practitioners
In pursuit of public service improvement, a focus on fostering an organizational culture that promotes collective behaviour, especially among those in authority, is crucial, given that their lack of support retards knowledge-sharing. For effective knowledge-sharing, both intrinsic and extrinsic motivators are equally important depending on the relational model.
Keywords
Introduction
As in all fields of professional practice, there is growing interest in stimulating knowledge-sharing practices in healthcare organizations. The aim is to exploit and leverage knowledge to reduce the costs of medical errors caused by a knowledge gap and to improve the quality of healthcare services (Currie et al., 2008; Waring et al., 2013). Medical knowledge-sharing, however, needs careful integration of expertise from several interdisciplinary areas. In this context, high levels of interaction and cooperation are required (El Morr and Subercaze, 2010) where intentionality and motivation condition such cooperative behaviour (Nahapiet et al., 2005).
This realization has shifted the focus of literature from the technical side of knowledge-sharing to social relationships and their role in guiding knowledge-sharing behaviour (e.g. Bate and Robert, 2002; Tagliaventi and Mattarelli, 2006; Tasselli, 2015). However, current relational research has left a significant gap in our understanding of the differences in relational contexts/models and the way they shape clinicians' intentionality and motivation. Relational models theory (RMT) (Fiske, 1992) suggests that there are four relational models (i.e. communal-sharing, authority-ranking, equality-matching and market-pricing) that determine the way people interact with others. Boer et al. (2011) then argue that intentionality and motivation to share knowledge are shaped by the relational models in which they are embedded.
In discussions of relationality, dominated by communities of practice (CoP) and social networks theories, there is an emphasis on the collective and altruistic elements in clinicians' intentionality and motivation. RMT moves us beyond this limited view of intentionality and motivation, which produced inconclusive empirical results on the effectiveness of knowledge-sharing within healthcare networks (Ferlie et al., 2012). In contrast, RMT helps to better understand the various ways in which different relational models affect knowledge-sharing, with a view to illuminating better motivational strategies based on the underlying relational model(s). However, there has so far been little detail on relational models in healthcare. We know little about how different relational models shape clinicians' intentionality and motivation for knowledge-sharing, or about which relational models most encourage clinicians to participate in knowledge-sharing. This paper therefore aims to provide a detailed analysis of clinicians' knowledge-sharing behaviour by applying RMT in two National Healthcare Service (NHS) Trusts in England.
This paper begins with an examination of relational literature on healthcare and an explanation of RMT. The Methods section explains how the two NHS hospitals and 40 clinicians interviewed were selected, as well as the strategies for data collection and analysis. This is followed by an in-depth, thematic analysis of the relational models of knowledge-sharing in the NHS. The discussion highlights the findings and calls attention to the root causes of knowledge-sharing problems, and possible remedial actions to create the right atmosphere to motivate clinicians to share their knowledge.
Conceptualising knowledge-sharing in healthcare from relational perspective
Knowledge-sharing refers to the leveraging of individuals' work-related experiences and skills to reinforce performance achievement (Argote, 2012). Studies have found an emerging consensus that the most effective knowledge-sharing in the public sector is likely to occur between various professions (García-Sánchez et al., 2019; Richards and Duxbury, 2015). In healthcare specifically, a single patient is often managed by a team of professionals, where each is specialized in one aspect of care. Such shared care requires a continuous combination of different kinds of knowledge of different people/groups. In this context, knowledge-sharing requires high levels of interaction and cooperation (El Morr and Subercaze, 2010).
Just as the need for cooperation has been realized, so too has the need to understand the fundamental tenets of cooperation (motivation and intentionality). In considering why people allocate time and effort to engage in cooperative behaviour, one needs to understand what they are motivated to achieve through their collaboration with others (Nahapiet et al., 2005). Research evidence suggests that knowledge-sharing behaviour is complex and not determined by one type of motivation (Ryan and Deci, 2000; Van de Walle et al., 2015). Rather, cooperative behaviour is grounded in human intentionality, determining what ends (self or mutual interest) the outcome of cooperation is supposed to support, from which motivational mechanisms in driving behaviours flow (Nahapiet et al., 2005). In the assumptive base of self-interest, people collaborate with others to pursue their own interests and are assumed to be seeking reputation, wealth, etc. It follows that extrinsic motivators (e.g. reciprocal benefits and rewards) are required for obtaining desired behaviour (Ferraro et al., 2005). In contrast, when intentionality is based on mutual interest, people are intrinsically motivated to engage in shared activities for their resulting satisfaction and enjoyment (Chen and Hsieh, 2015; Gagné, 2009; Pinder, 2014). In this perspective, the importance of social relations and their role in guiding knowledge-sharing behaviour cannot be overstated. The nature of the connection between knowledge parties in social relations indicates how well and in what ways they contribute to knowledge-sharing (Hansen et al., 2005).
Relational literature in healthcare dominantly inspired by CoP and social network theories suggests that a shared sense of identity and belonging, and a common repertoire developed through collaborative processes such as conversation, joint activities and problem-solving, create goodwill attitudes that foster cooperative behaviour and increase the motivation for knowledge-sharing (Bate and Robert, 2002). A CoP is ‘a group of people who share a concern, a set of problems, or a passion about a particular topic, and who deepen their understanding and knowledge of this area by interacting on an ongoing basis’ (Wenger et al., 2002: 4). A social network, on other hand, is ‘a groups of people, “actors”…, with some pattern of interactions or “ties”' (Newman et al., 2002: 2566).
Successful functioning of a knowledge-sharing CoP/social networks requires the participation of all of its members (Dixon, 2000), and a strong commitment to the CoP/social networks is what drives behaviour (Oborn and Dawson, 2010; Waring et al., 2013). Especially when relationships are high in trust, clinicians are more willing to engage in the cooperative interactions required for knowledge-sharing to occur (Chang et al., 2012). The process of ‘thinking together’ about the same problem is also described by Pyrko et al. (2017) as the essential factor in promoting participation in CoP. Thinking together encourages clinicians to mutually guide each other through their understandings of the same problems, and thus is motivating to share more knowledge.
While these insights are undoubtedly useful, and have illuminated our understanding of how the structure and quality of social relations influence the collaborative environment that can stimulate knowledge-sharing, they are limited in their view of motivation and intentionality. The assumption has been that interacting parties are ‘benevolent co-operators’ who consider mutual interest as an end in social exchange. The focus of this line of research has been on altruistic, disinterested and pro-socially oriented work behaviour in the public sector (Perry and Wise, 1990) and therefore largely aimed at fostering the cooperative behaviour required for knowledge-sharing through the fulfilment of intrinsic needs, with limited attention paid to potential conflicts of interest and extrinsic motivators.
Given the theoretical bias for CoP/social networks to stimulate knowledge-sharing as opposed to hierarchies/markets (Adler, 2001; Nahapiet et al., 2005), this dominance may have been appropriate. However, empirical results on the effectiveness of knowledge-sharing within healthcare networks have been inconclusive (Ferlie et al., 2012). Research suggests, for example, that power relationships within CoP in healthcare are common. This implies that more powerful stakeholders such as doctors (Currie and Suhomlinova, 2006) or superiors (Li et al., 2009; Tasselli, 2015) privilege self-interested opportunistic behaviours and therefore push their opinions/interests rather than making opportunities for others to contribute to knowledge-sharing, as CoP theory suggests. Similarly, when Addicott et al. (2006: 92) investigated the effectiveness of knowledge-sharing in five cancer networks in the NHS, they found that knowledge-sharing was only effective in one ‘because good relationships between those within the network were pre-existing, prior to the formalization of the network’. The authors then made a case for investigating the impact of market-based relationships on the effectiveness of knowledge-sharing.
These inconclusive empirical results could be attributed to ignorance of the differences in the relational context. With reference to Adler (2001), different relational contexts (CoP, hierarchy and markets) potentially co-exist simultaneously under the same organizational setting. However, given that each relational context is radically different in its cultural implementation of rules and in the motivational basis that supports it (Boer et al., 2011), the problem for healthcare organizations (and indeed for the public sector as a whole) is that they have been trying to reinforce knowledge-sharing by applying motivational strategies that do not match the underlying relational context. It follows that if we want to fully understand how knowledge-sharing can be stimulated in a situation that requires high levels of cooperation, such as healthcare, we need a more comprehensive set of assumptions about relational contexts and their impact on clinicians' intentionality and motivation.
Fiske's relational models theory
RMT describes the cultural rules that govern individual behaviour in the context of human relations. According to this theory ‘people in all cultures use just four relational models [communal-sharing, authority-ranking, equality-matching and market-pricing] to generate most kinds of social interaction, evaluation, and affect’ (Fiske, 1992: 689). According to RMT, people usually adopt more than one model in their social interactions and work settings. The logic of this theory also suggests that conflict is likely if interacting parties expect a different relational approach to a particular issue or cannot agree on the implementation rules while using a particular relational model.
Recent work in administration (e.g. Talbot and Wiggan, 2010) and knowledge-sharing (e.g. Boer et al., 2011; Lin et al., 2012) supports the potential of RMT, which while not discussing knowledge-sharing directly, offers an important and useful alternative perspective on what drives knowledge-sharing behaviour. By showing that knowledge means different things, and has a different value and personal meaning in each of the four models, RMT leads to a far wider view of motivation and intentionality.
An intentional and motivational basis for knowledge-sharing
Communal-sharing goes beyond reciprocity and resembles CoP (Wenger et al., 2002) where group members are positively oriented towards social exchange in general and knowledge-sharing behaviour in particular. In this context, knowledge is viewed as a common resource belonging to the group. Therefore, people may give what they can and take what they need freely without being expected to receive or give something in return. As with public service motivation (Perry and Wise, 1990), in this context intrinsic motivators such as altruism are the basis of motivation that fuels cooperative behaviour. Interacting parties are motivated to benefit others, and want to achieve this through collaboration (Gagné, 2009). Hence, their cooperation with others is viewed as a means of achieving mutual interests in social exchange (Nahapiet et al., 2005).
In authority-ranking, power distances are the basis of knowledge-sharing. Boer et al. (2011) have tended to treat power distances as if they are based either on formal power (job position) or expertise (work experience). In this sense, authority-ranking relationships are a key aspect of social power theory (French and Raven, 1959). In formal power-based authority-ranking, superiors are in a stronger position and have the ability to control subordinates' knowledge-sharing behaviour (coercive power). Subordinates, however, are weaker and accept their superiors' commands as a valid reason for sharing their knowledge (legitimate power). When people interact according to expert-based authority-ranking, experts are seen to have the required knowledge in a given area (expert power); thus, less experienced individuals are more willing to engage in knowledge-sharing with them. Experts are motivated to share their knowledge with less experienced individuals by the good feeling they get from helping others and being respected (referent power).
Authority-ranking, however, is vulnerable to the fact that knowledge can be seen as a source of power. Ipe (2003) corroborates this view, arguing that knowledge-sharing is a power game. In this case, knowledge owners prefer to hoard knowledge rather than share it in order to keep their power/position. Here self-interest is at the centre of social interactions in which other people are seen as a means to pursue a personal end. Thus, in this form of relationship, social actors compete with each other rather than cooperating, as each seeks their own personal interest which may not coincide with others' benefit (Ferraro et al., 2005).
Equality-matching lies at the heart of social exchange theory (Blau, 1964) and here the desire for equality is the underling motivational factor for knowledge-sharing. In this context, cooperation with others involves cost–benefit analysis to determine the value of their exchange behaviour on the part of each knowledge-sharing actor. The knowledge-sharing process will stop if the benefits gained do not justify the cost of interaction. Unlike the final model, market-pricing, which is based on economic exchange, equality-matching centres on intangible costs (time and effort) and benefits (support, companionship, etc.) (Davenport and Prusak, 1998).
Within the context of market-pricing, knowledge is viewed as a commodity with a particular value that can be traded. Such a relationship is based on proportionality and the interacting parties orient to ratio values. Achievement motivation encourages people to participate in knowledge-sharing, and extrinsic monetary reward is typically the key reward that people expect for sharing their knowledge. Here, absolute self-interest is predominant, and people seek to maximize their utility with scant regard for the interests of others (Nahapiet et al., 2005).
Methods
A qualitative approach based on primary data was utilized to study knowledge-sharing behaviour in a relational context. The study was carried out in two NHS hospitals in England; using two case studies helped to provide rich data and yielded opportunities for literal replication across the two cases, thereby increasing the robustness of the findings. In the multiple-case studies design, there are no rigid rules about the numbers of cases required to satisfy the replication requirement (Yin, 2014). Given that multiple-case studies require more time and resources, and considering the busy environment of healthcare, two cases were chosen. Both cases were teaching hospitals where a contextual factor was similar, each with a similar knowledge management system as a result of the introduction of an NHS information strategy (NHS England, 2018).
Semi-structured interviews formed the predominant method of data collection. In total, 40 face-to-face interviews (20 in each hospital) were conducted with a number of clinicians. One-to-one interviews typically lasted for an hour and were conducted by the author in hospital wards. Given the interest in investigating knowledge-sharing in relationships among clinicians, there was a focus on sampling clinicians working in the same ward. These included two specialized departments in each hospital to triangulate data sources and cross-check findings. Notably, respondents were sampled to maximize variation and to represent different roles and positions in knowledge-sharing. With permission received from the ward managers, clinicians were approached face-to-face by the researcher for recruitment in each ward. They included nurses (16), medical staff (15), dieticians (four) and physiologists (five) in different formal positions and with different work experience. The focus of the interviews was to understand the dominant relational models in use, and in particular how different models impact clinicians' intentionality and motivation to cooperate with others. More basically, the study aimed to discover what ends their cooperation was supposed to support, and the impact of these on knowledge-sharing. Interviewees were also asked to describe the main day-to-day knowledge-sharing activities and the intra- and inter-professional knowledge-sharing opportunities/barriers within the department.
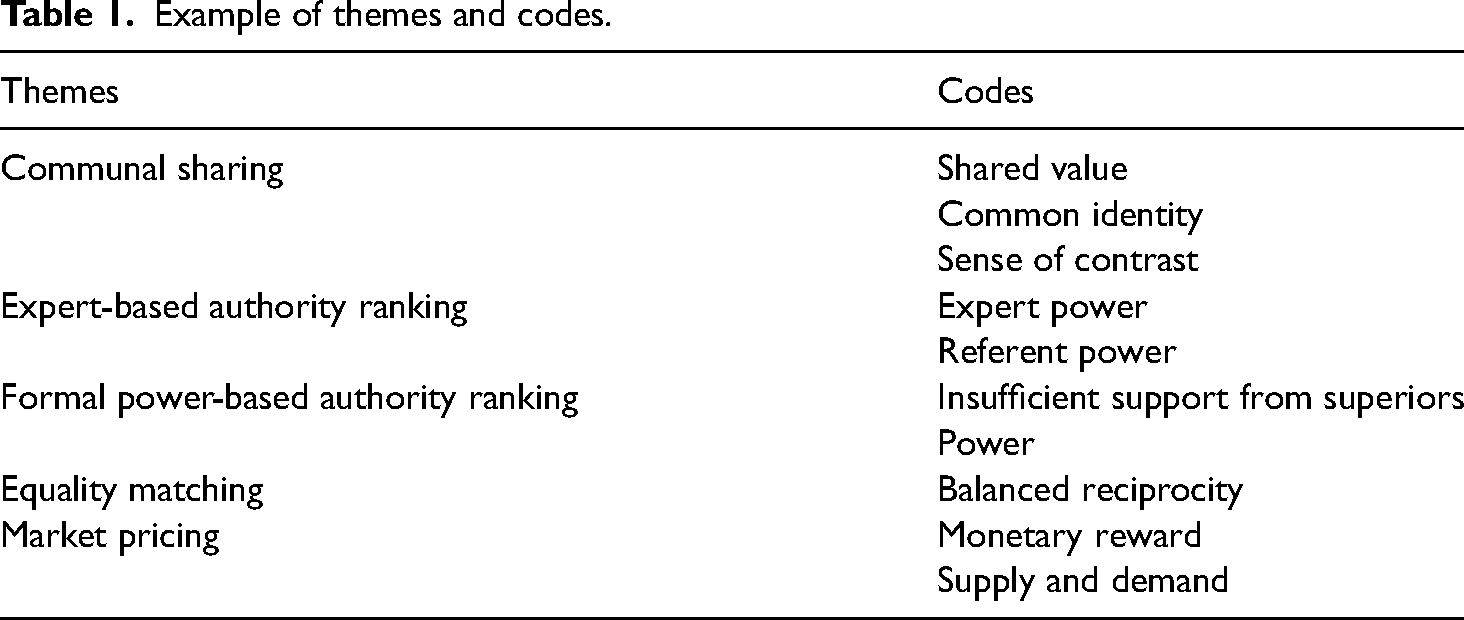
All of the interviews were tape-recorded and then transcribed prior to in-depth analysis. Initially, transcripts were examined manually by the author to distinguish the social relations within and between different positions. Deductive thematic analysis was then utilized to code the interview data for each of the relationships identified above. A predefined RMT coding frame was developed to classify similar events into groups. All elements of the data were then categorized by the author according to their relevant themes in a spreadsheet. An illustration of analytical themes and codes is presented in Table 1. This allowed the content of the interviews to be verified systematically, which enabled analysis of the large amounts of data received from the interviews (Corbin and Strauss, 2015). Finally, the coded data were regularly compared and contrasted to interpret the views of individual respondents.
Example of themes and codes.
Results
Communal-sharing
Many of the clinicians involved in the study referred to ‘patient safety’ as their joint responsibility and as a common goal. In effect, patient safety builds connections and a sense of mutual interest among clinicians. This attitude encouraged cooperative behaviour in social exchange, favouring knowledge-sharing with the aim of providing high-quality services to patients.
I always search for knowledge because of patient safety. In a job like this you've got people's lives and safety, you cannot be arrogant with your knowledge, you have to let people know and allow them to teach you.
However, reinforcing the work of Ferlie et al. (2005), the social influence of the group was stronger the more similar its members were. There was a strong tendency among clinicians to seek partners in their own professional groups; for example nurses preferred to approach nurses. Professional proximity represents the shared identity that homogenous professional groups have in common. This strengthened ties between actors involved in knowledge-sharing, which in turn encouraged individuals to actively learn from one another in their professional groups.
The communal-sharing orientation, however, created a sense of contrast, especially between doctors and other professional groups. Although patient safety created the complementary obligation to share knowledge with others who come to doctors for advice, it was evident from the way doctors discussed knowledge-sharing that they draw lines between themselves and other members of the multi-disciplinary team, especially in reading medical notes. This boundary caused doctors to sometimes miss important information, which, as in the findings of Waring et al. (2013), seemed to threaten patient safety.
Medics tend just to read the medical notes. I've seen one instance where an advanced practitioner planned a whole management plan for a patient, and it wasn't followed, because doctors didn't know to look for that under the nurses' notes.
Authority-ranking
Expert-based authority-ranking fostered the habit of cooperation and knowledge-sharing by supporting less experienced clinicians. Task independence was often expressed in the interviews by more experienced clinicians as the reason for their support. The more that junior people's work depends on seniors, the slower the jobs will be done. Seniors are therefore willing to help as much as they can to make juniors independent, which helps the team do the day-to-day tasks more quickly.
You want your colleagues to be at the right level, you help them to become independent and get the jobs done quicker as a team.
The pleasure of helping colleagues and the potential to gain respect as a result were hugely significant for understanding seniors' attitudes towards sharing knowledge with juniors. Juniors typically have many alternative seniors with whom they can engage in knowledge-sharing; seniors who fail to support or who display a lack of generosity are unlikely to be respected/acknowledged as much as supportive seniors. Equally, juniors who are more willing to learn become the recipients of more knowledge than those who are characterized as having low enthusiasm.
On the other hand, knowledge did not flow well when authority-ranking was very formal. It was evident from the way that clinicians discussed knowledge-sharing that managers channel information/knowledge upward and hand decisions/instructions down through the chain of command, without taking care to ensure that juniors observe an accurate message. This less supportive cooperative environment, which emerged when authority-ranking was very formal, appeared to have a negative influence on the effectiveness of knowledge-sharing.
Once, we just discussed a particular infection in our break. We were just told that we have to screen the patient for it. We weren't communicated any other knowledge of the actual infection; none of us knew or understood what type of patients would be more in danger of it. I think the knowledge isn't well communicated.
Closer inspection of the findings from the interviews suggested that formal authority-ranking considerably varies from profession to profession. For example, physiologists and dieticians who are not based on a particular ward receive less support from their manager in knowledge-sharing. A lack of support from managers was felt in these cases, resulting in less knowledge for clinicians.
From a physiologist's point of view, we have quite a bit of revocation of work. It's because we're all on different sides. I don't think we quite get adequate support for sharing experience that're around there. We need to get together as a peer group, then share knowledge.
Knowledge lost represented one manifestation of formal authority-ranking among medics. Those with a higher formal rank, such as consultants, were less likely to cooperate with junior doctors. Many of the doctors said that consultants give instructions about such things as changes in medication and delivery of interventions at the end of the ward round very quickly, and this leads to misunderstanding. Equally, consultants acknowledged that when knowledge gets lost, it is most often when junior doctors have to document the most important things during the ward round.
Today I saw a patient who was supposed to have one medication stopped because we were told to [by a consultant]. However, the medication wasn't stopped. [I believe] the instruction wasn't very clear at the time. The consultant reviewed the patient, gave a set of instructions. However, they weren't well written down.
Junior doctors don't document every word consultants say. One of the biggest tasks of junior doctors, who don't necessarily know the speciality well, is to document the most important things during ward round. Sometimes you have to dictate, but we don't always do that. I'm sure information recorded compared to actually what was said was not always accurate.
Further, we found that some surgeons of higher formal rank see knowledge as power. They therefore often fear sharing their knowledge because they believe it will weaken their position/authority within the hospital. At the same time, however, the principles of the NHS encourage seniors to be generous and hospitable to juniors and to exhibit responsibility in sharing their expertise (NHS England, 2018). As a result, they are deliberately slow to pass on knowledge.
Some seniors feel they are going to lose their power. Eventually, they have to pass on the knowledge; the question is how fast they do it!
Equality-matching
The importance of extra-role behaviours is well documented elsewhere and shows how supporting the non-technical core impacts the social and psychological environment of the organization, which in turn influences the technical core (Morrison, 1994). While in communal-sharing and expert-based authority-ranking relationships, clinicians were well motivated to go beyond their formal duties, in the context of equality-matching clinicians were not willing ‘to go the extra miles’ unless the recipient was able to reciprocate. For example, according to the procedures of the two hospitals investigated, clinicians need to document the results of their investigations and check the documents for any updates from colleagues (technical core). However, given the time-consuming nature of checking/reading the documents, the majority of clinicians believe that there is also a need for verbal communication to bring the attention of the relevant colleagues to what was documented. This verbal communication, however, highly depends on the clinicians’ motivation as this goes beyond their job description. For instance, it appeared that doctors especially sometimes update the medical notes after seeing patients (in-role behaviour), but do not follow up with nurses to bring their attention to the updates (extra-role behaviour). Nurses were then particularly concerned that this lack of cooperation would reduce their capacity for the delivery of safe and efficient patient care.
Some doctors tell the patient and walk off, and all the investigation they've done is not known by the nurse who looks after the patient. We only can provide the service if we know it. They document it, then we have to go on the computers and read about it, which we don't have time to do when we are on a busy shift. But if doctors come to you, it takes a couple of minutes to just update.
Being busy in the NHS was often expressed in the interviews by all clinicians emphasising ‘being busy is something that we can't eradicate’ (Doctor-38, Hospital-2). The operation principle, however, is that when clinicians relating in equality-matching receive a favour, they feel obligated to reciprocate by returning it. Balanced exchange of favours can help clinicians save time by helping each other where possible. For example, the findings suggest that under such circumstances (where nurses do not receive assistance from particular doctors), nurses are not willing to spend time and effort helping doctors. The additive tally of who owes what to whom and who is entitled to what hampered extra-role behaviour and often caused nurses to not communicate enough and not anticipate doctors. As a result, they are not always equipped with the knowledge doctors need.
If nurses have been off a bit, they often don't know it. One of the typical things they say is like ‘well it was my day off yesterday’ or ‘I’m only covering because my colleague is on a break’. And then you often don't get the information you want. It usually delays things or makes it more difficult to get the information.
Conversely, nurses placed greater value on giving support to other occupational groups, such as dietitians and physiologists, because those groups more frequently support nurses and therefore accommodate the nurses' uncertainty about receiving something of equal value in return. Such mutual benefit and dependence resulted in a reciprocally interactive relationship between nurses and other occupations. Thus, knowledge-sharing behaviour was observed more frequently.
Market-pricing
Market-pricing is essential and the basis of cooperation and knowledge-sharing. Clinicians from different professional groups need to interact with each other about patient care plans because they are paid on the outcome of their behaviour. However, in the light of the above findings, knowledge-sharing is harder to mandate when it involves effort and activities that fall outside the scope of the job description. Shift handover is a typical example of this. Clinicians codify and document noteworthy events that occur during the shift. However, they still believe that, owing to human complexity and the ‘black and white’ nature of codified knowledge, there must be an overlap between shifts. This opens a window in which to rectify any potential problems that clinicians on the next shift may face using the knowledge transferred. However, despite its importance, shift handover is not always effective. Each of the occupations has its own handover and its quality varies among different professions. For example, while shift handover takes place quite effectively among nurses, medical shift handover is not of high quality. For all of the doctors in the study, shift overlap meant allocating extra time. Unlike nurses, doctors were only willing to do it if they got paid for their extra time and effort.
The shift should overlap, rather than one doctor starting at eight and then finishing at eight, there should be 30 min overlap, and they get paid for that so we can do the handover. Because otherwise it means staying late to give the handover and some people don't want to stay late, and they rush through the handover.
Market-pricing is a distinctive way to organize social interaction and connect people through the medium of trade and money. In this regard, it has the potential to bridge the ‘structural hole’ (Burt, 1992), an issue that has been seen to be one of the main reasons for the ineffectiveness of inter-professional knowledge-sharing (Waring et al., 2013). This research found, for instance, that the nurse coordinators are paid to be responsible for collaborating with various professional groups and bridge the knowledge gap by providing feedback to those groups. The main challenge, however, is that while nurse coordinators ought not to be responsible for any patients, in order to be able to act as knowledge brokers, they usually become busy taking care of patients because of a shortage of staff. This implies that the knowledge gap between different professional groups cannot always be bridged and this can negatively impact the quality of care.
That there is a significant issue with staff retention and numbers in the NHS has been demonstrated elsewhere (Rolewicz and Palmer, 2019). From the transaction point of view, knowledge-sharing is a commodity whose value depends on clinicians' time and the fixed costs that go into them. In this context, the interaction between supply (advantages received by clinicians such as their salary/bonus) and demand (workload) determines socially generated values such as cooperative behaviour. When clinicians perceive a scarcity of human resources that leads to a higher transaction cost (higher workload), they are less happy with their job, which has an impact on the effectiveness of knowledge-sharing and accomplishing the mission of patient care.
The knowledge gap is probably due to resources. For instance, we had a patient came to us from A&E who had got lung cancer and had a heart attack just 2 weeks before his admission. But none of this information was handed over to us. We treated the patient as normal while he needed special care. This harmed the patient. I'm assuming the problem is nurses were very busy in A&E at that time to do the proper handover.
Discussion
The purpose of this study was to apply RMT to a comprehensive investigation of how different relational models shape clinicians' intentionality and motivation to collaborate and share their knowledge in order to care for patients in their daily job. Using two NHS hospitals, the study provides evidence that all four relational models (i.e. communal-sharing, authority-ranking, equality-matching and market-pricing) play a significant role in shaping clinicians' motivation to engage in knowledge-sharing. On a reflexive note, while the idea is to work together to improve public service quality, each actor also has their own interests and is motivated to share knowledge for different collective and/or personal reasons/agendas (Hartley and Rashman, 2018; Ritz et al., 2016). This study, therefore, does not support the view that public employees disregard extrinsic material incentives such as pay and value intrinsic job characteristics (Anderfuhren-Biget et al., 2010), but instead finds that a range of intrinsic and extrinsic motivators, depending on the underlying relational model, can impact the knowledge-sharing behaviour in the public sector.
The dominant relational models and consequently the basis of intentionality and motivation, however, vary within and between different professional groups. Communal-sharing and expert-based authority-ranking appeared to be the dominant models that encourage effective intra-professional knowledge-sharing. In line with recent research (Tasselli, 2015), when patient care activities among professionals of the same background are guided by shared identity, a close cognitive tie develops amongst them which intrinsically encourages them to behave cooperatively and share more knowledge. Expert and referent power motivators that fuel cooperation behaviour in expert-based authority-ranking extrinsically motivate both juniors and seniors in each professional group to share their expertise constructively.
Equality-matching is a more dominant model for a cooperative relationship between different professional groups. Here, balanced reciprocity is highly valued and is the basis for being motivated ‘to go the extra miles’ or to impose sanctions (Tagliaventi and Mattarelli, 2006). While market-pricing is a directive force that guides ‘in-role behaviour’, ‘extra-role behaviour’ requires some form of intrinsic/extrinsic motivators. When equality-matching is operative, clinicians are actively concerned to keep track of how far out of balance their relationship is. The findings suggest that nurses are more willing ‘to go the extra miles’ to support physiologists and dieticians (rather than doctors), as this support is more likely to be reciprocated by them. While most of the clinicians interacting with each other apply equality-matching to bring relevant colleagues' attention to the written documentations, adherence of some of the doctors to market-pricing (a contribution defined by a job description) normally violates the standards of equality-matching and conflict inevitably results.
Formal authority-ranking ‘permits rapid decisions and coordination of actions and information flow’ (Fiske, 1992: 714) and is therefore well fitted to the public sector with a high number of employees. However, reflecting on Adler’s (2001) analysis of hierarchy relationships, juniors lack the required incentives to use the transferred knowledge effectively, thus the importance of receiving support in the use of new knowledge from managers. Red tape, passive communication and less support from superiors in healthcare (Scott and Pandey, 2005; Tasselli, 2015) and indeed the public sector as a whole (Pandey and Garnett, 2006) crowd out effective knowledge-sharing. Furthermore, this research shows that power games among surgeons negatively impact knowledge-sharing. NHS encourages knowledge-sharing at all levels to improve patient care. However, the adaptive flexibility owing to the ambiguity in how much juniors should receive in distribution and how fast the knowledge should be passed on generates conflict.
Market-pricing connects all clinicians through the medium of trade and money to collaborate with each other for patient safety. For a productive cooperative environment, there is therefore a calculating rationale oriented towards a cost–benefit ratio. A shortage of staff, especially of nurses, in the NHS was certainly found to discourage knowledge-sharing on the basis that knowledge-sharing has a higher transaction cost. In this context, nurses in general and knowledge brokers such as nurse coordinators, in particular, are not always able to effectively participate in knowledge-sharing, and this impacts the performance of healthcare services. The importance of market-pricing is also evident when doctors are expected to receive extrinsic incentives for the extra time and effort that they are supposed to allocate for more effective shift handover. Here, managers expect clinicians to be intrinsically motivated to allocate extra time and effort for shift handover while doctors expect a market-pricing approach, thus conflicts arise which hamper effective medical shift handover. However, since the models expected by the managers and other professionals were the same (communal-sharing) the shift handover was supported. As with Andersen’s (2009) findings, this result highlights the importance of economic incentives in driving behaviour in the absence of communal-sharing.
This study takes the existing relational research in healthcare one step further by unfolding the relational models and providing a more comprehensive explanation of clinicians' intentionality and motivation. By responding to the need for further research, and focusing on missing focal points in public sector research on rational, self-interested and extrinsic motives, this study provides a more comprehensive view of public employees' motivation – one that better matches the reality (Ritz et al., 2016). Although communal-sharing relations are certainly influential in fostering cooperative behaviour and knowledge-sharing, this was not the only dimension that shaped clinicians' intentionality and motivation for knowledge-sharing. This study suggests that in addition to altruism and intrinsic motivators, it is equally important to recognize the hierarchical and transactional rationale of economic-style relationships and apply incentive-driven extrinsic motivators to transform conflict between self-interested parties into cooperation, and thus enhance knowledge-sharing.
In accordance with the results of Boer et al. (2011), evidence from this study indicated that the RMT could be seen as a powerful tool in the investigation of relational context that shapes intentionality and motivation which in turn explains how and why knowledge-sharing is promoted/hampered. This study investigated four relational models in healthcare and found that they suggest important differences in intra- and inter-professional cooperative behaviour that are more likely to encourage knowledge-sharing. This paper, hence, contributes to advancing our understanding of the RMT by providing empirical evidence from healthcare and determining how relational models work between and within professional and organizational boundaries. While communal-sharing and authority-ranking relationships are more dominant within a particular group/organization, equality-matching and market-pricing relationships will dominate across professional/organizational boundaries.
This study was conducted in two NHS hospitals to triangulate the data and increase its validity. The relational dimensions of knowledge-sharing were very similar in both cases, implying that this is the culture of the NHS (Hardy et al., 1999). The study is limited to investigating the dominant relational models and their role in shaping clinicians' intentionality and motivation to engage in knowledge-sharing. Further research is required to investigate the dynamics of the models and transformations from one model to another. Fiske (1992: 712) argues that the transformation of the relationship between group members tends to move from ‘market-pricing to equality-matching to communal-sharing, or from authority-ranking to communal-sharing’. However, it is not clear how the transformations from one model to another take place. Further research is, therefore, required to understand, for example, how equality-matching can be replaced by communal-sharing, and more basically how the organizational/occupational culture impedes/encourages the transformation.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.