
Abstract
Co-production tends to assume that co-produced decision-making leads to consensus and equality between actors with different perspectives. Drawing on ethnographic insights into interactions between professionals and patients, this article studies how consensus and equality may manifest in the professional-patient interaction throughout co-produced decision making. Characterized by three power dimensions and structured by problem-based and relation-based reasonings, our findings show how the interactions remained unequal and were directed towards seeking consent instead of consensus. These findings deepen our understanding of professional-patient interaction, not only of co-production but also of street-level work.
Keywords
Introduction
The notion of co-production is immensely popular in public services (Alford, 2014; Bovaird & Loeffler, 2012; Nabatchi et al., 2017). Co-production is an umbrella term for “a relationship between a paid employee of an organization and (groups of) individual citizens that requires a direct and active contribution from these citizens to the work of the organization” (Brandsen & Honingh, 2016, p. 431) . Especially in healthcare services, co-production is widely implemented (Palumbo & Manna, 2018). Central to the idea of co-production is the conviction that, between public professionals and service users, decision making should take place as a result of consensus and on equal footing, thereby evening out the balance of power between actors (Steen et al., 2018). Building on these expectations, co-production literature and policies promise to improve public service delivery, for example, by improving the quality, democratic character and legitimacy of public service (Bevir et al., 2019; Brandsen & Honingh, 2016).
Scholars, however, increasingly warn against the appeal of co-production, arguing that its benefits may be overestimated and that nuanced, empirical analysis of the interaction between public professionals and service users is necessary (Dudau et al., 2019; Osborne et al., 2021; Steen et al., 2018). Moreover, an overly rosy picture of co-production can mystify the power processes involved in co-produced decision making, leaving power-related questions unanswered—for example, how does co-production redistribute power, who benefits and who loses, and who can be held accountable for a “co-produced” decision (Steen et al., 2018)? Although the interaction between public professionals and service users often is viewed as the most influential factor in service delivery (Osborne, 2018), remarkably little is known about how power processes manifest in their interactions throughout co-produced decision making (Bevir et al., 2019).
To better understand how co-produced decision making between public professionals and service users takes place, we use a power-sensitive analytical lens to zoom in on two of the underlying assumptions of co-production: consensus and equality. In doing so, we ask: how do consensus and equality manifest in the power dynamics between public professionals and service users throughout co-produced decision making? To answer this question, we first explore how, in current debates, scholars understand the nature of power in co-production, before proposing an empirically grounded two-way analytical lens for studying the interactions between public professionals and service users. Then, we draw on an implemented “shared decision making” (SDM) policy in a hospital for our focused ethnographic case study, throughout which patients and surgeons made decisions about different treatment options. SDM is a fitting case for the purpose of this study, because it aims to actively involve patients in clinical decision-making processes and assumes the possibility of a decision-making process based on consensus between equal partners. Our findings provide new insights by (a) scrutinizing the possibilities for consensus and equality between healthcare professionals and patients throughout co-produced decision-making processes; (b) providing a deepened understanding of the power dynamics inherent to professional-patient interactions in the co-production; and (c) broadening street-level bureaucratic perspectives on the professional-patient interaction to include more dynamic understandings. To start, we provide a critical exploration of power dynamics in co-production literature, which allows us to build and present our analytical lens. After discussing the methodology and findings, we conclude by answering the research question and discussing the contributions and implications of this study.
Power in Co-Produced Service Delivery
In current scholarship, we identify three dimensions of power in co-production and two different narratives for the function of power in co-produced decision making. Responding to the limitations of these two narratives in explaining consensus and equality, we propose a third analytical perspective to enhance understanding of how power manifests in the interactions between public professionals and service users in co-production practices.
Co-Produced Decision Making: Emancipation or Manipulation?
We distinguish three dimensions of power in the literature on co-production: knowledge, responsibility, and legitimacy. The theoretical argument in the literature is that professional knowledge and responsibility are forms of power that healthcare professionals can “share” with their patients by empowering them to engage in decision-making processes (Avci, 2023; Haug, 2024; Meijer, 2016). Professionals obtain the power of medical knowledge through education, practical experience, and training (Hoff & Kuiper, 2021; Hofmann, 2016). Patients bring a different type of knowledge to the table—one based on their personal, bodily, emotional, and social experiences with illness—a form of knowledge that often is referred to as “lay” and contrasted with professionals’ “expert” knowledge (McMullin & Needham, 2018; Scambler & Britten, 2013). Professionals are generally considered to have a more powerful role in decision making than patients because their expert perspectives on health problems are seen as more objective (Palumbo & Manna, 2018).
Responsibility in the co-produced decision-making literature encompasses both the right to participate in decision-making processes and the accountability assigned when things go wrong (Meijer, 2016). Through co-production practices, patients are, in Foucauldian terms, “responsibilized”: they become active partners in healthcare decision making and, as a result, bear (partial) responsibility for healthcare processes and outcomes (Meijer, 2016).
Finally, power in the form of legitimacy manifests in co-produced decision making when patients and professionals deem the decision-making process to be trustworthy and just. Co-production scholarship stresses that a combination of both expert and lay knowledge and responsibility sharing are vital to achieving a high quality of care—and to increasing the legitimacy of healthcare decision making (Alford, 2014; Osborne, 2020). In this sense, legitimacy is shaped by more than just the (perceived) correctness of procedural steps; in co-production, the quality of collaboration between patients and professionals also affects the legitimacy of the decision-making process (Bevir et al., 2019; Brandsen & Honingh, 2016).
A striking example of the roles that knowledge, responsibility, and legitimacy play in shaping the balance of power can be seen in the COVID-19 crisis, during which governments, healthcare organizations, professionals, and citizens attempted to control and prevent the spread of the virus using various measures. These efforts sparked controversial and heated debates over a range of power-related issues, including which facts should be given precedence, which risks were “true” or “serious,” which preventive strategy would be most effective, whose interests were most important, who should be trusted, and who should have a say in answering such questions (La Grouw, 2021; van Dooren & Noordegraaf, 2020). The COVID-19 crisis showed why the need to integrate different perspectives also implicates a struggle over power: when there is no shared knowledge to rely on, actors will compete over who gets the responsibility of defining both the problem and its most appropriate solution (McMullin & Needham, 2018; Scambler & Britten, 2013).
In the co-production literature, we identify two narratives that are frequently invoked to frame the roles of knowledge, responsibility, and legitimacy. The dominant narrative of co-produced healthcare provision is what we call an emancipation narrative. This narrative sees co-production as a method for overcoming hierarchical boundaries and knowledge gaps, both of scholars believe hinder equality and consensus in decision making. Research in healthcare, for example, shows that co-production practices can potentially tackle the (mis)use of hierarchical power by professionals (Palumbo & Manna, 2018; Realpe & Wallace, 2010) and turn patients’ feelings of powerlessness into feelings of being in charge (Aujoulat et al., 2007). By sharing information and improving patients’ health literacy, researchers and policymakers argue that the knowledge asymmetry between professionals and patients can be corrected (Morden et al., 2012; Palumbo & Manna, 2018). This narrative builds on the assumption that co-production emancipates service users from their passive, receiving role and enables them to influence policy outcomes by involving them in service delivery (Alford, 2014; Osborne et al., 2021). By giving service users an equal or even central role in the public service delivery process, proponents expect that service users’ needs, rather than those of public organizations, also will become central (Bovaird & Loeffler, 2012; McMullin & Needham, 2018). When both public professionals and service users focus on the value of a service for its users, this shared aim should—such scholars assume—allow the two parties to more easily collaborate in public service efforts (Osborne, 2018).
In contrast, we distinguish the emancipation narrative from a manipulation reading of co-produced decision making. The manipulation narrative emphasizes co-production’s dark sides, arguing that it enables actors in formal positions—with expert knowledge, resources or rule-setting abilities—to exercise power over or increase the dependency of parties in weaker positions, who have fewer resources and abilities (Agranoff, 2016; Palumbo & Manna, 2018). Professional dominance in decision-making processes risks obscuring why certain decisions are made, thereby hindering the transparency of the process. For instance, a body of research shows that co-production may in fact facilitate the prioritization of professional perspectives (Crompton, 2019; Palumbo & Manna, 2018), the symbolic involvement of service users (Martin, 2008), and the “co-destruction” of public value, for example, by representing controversial or disruptive goals and practices or by wasting public resources on ineffective conflict-resolution efforts (Osborne et al., 2016; Steen et al., 2018). Moreover, scholars warn that co-produced decision making can be undermined by public professionals who wish to maintain control over the outcomes (Frederiksen & Grubb, 2023; Haug, 2024) and that, because equality is not guaranteed, professionals can impose consensus. Similarly, when citizens feel forced to participate in co-production, the process is less likely to improve empowerment and quality care (McMullin, 2025). The manipulation narrative thus questions whether equality is even possible given the dominance of public professionals in their interactions with service users.
Although the emancipation and manipulation narratives do help explore and assess the desirability of co-production, they are less helpful for appreciating the intricacies of the process itself. Both narratives ascribe agentic power to one actor in particular and then assume a specific power effect, thus providing a unidirectional understanding of co-production: the dominant public professional either “emancipates” or “manipulates” the passive service user into adopting an active role. However, when policy narratives imply a specific (i.e., emancipative) transfer of power, onemay become blind to the unintended or unexpected ways in which power manifests in practice. Bouchard (2016) calls this the risk of “power blindness” in co-production processes. Recent co-production scholarship takes this discussion a step further by ascribing agency to citizens in the implementation of public services: professionals can try their best, but the result of a public service depends on what the service user does with the offered service (Fledderus et al., 2015; Osborne, 2018; Osborne et al., 2021). Empirical studies have built upon this insight by examining, for example, how patients use telehealth tools in their homes (Go Jefferies et al., 2021) or the extent to which older persons are willing to adapt their lifestyle to avoid risk (La Grouw et al., 2020). Yet, these studies fail to recognize that service users might not only adopt an offered service as they bring it into practice, they may also in their interactions with public professionals influence the professionals’ “service-offering behaviour.” To empirically study how both professionals and service users mutually influence each other’s behaviour, we must move beyond a unidirectional understanding of the interaction between professionals and service users.
Applying a Two-Way Lens to Power in Co-Produced Decision Making
We propose applying a two-way analytical lens in order to capture how both public professionals and service users contribute to the power dynamics involved in co-produced decision making. Such a lens seeks to avoid power blindness while reconciling the emancipation and manipulation narratives by (1) explicitly addressing power processes and (2) treating neither professionals nor clients as if they “possess sole agentic power” over the other, but focusing instead on the interactive nature of power in decision making. This lens implies that all power dimensions in co-production—knowledge, responsibility and legitimacy—are socially constructed by both patients and professionals during their interactions as they negotiate and (re)define the roles of these dimensions throughout the collaborative decision-making process. This two-way framework builds upon a decentred (Bevir & Rhodes, 2016)—as opposed to top-down—perspective on the interaction between public professionals and service users, grounding exploration of how one actor responds to a leading initiative of the other. To direct this analysis, we distinguish between two types of responses: following responses and resistant responses. Following responses consist of discursive or bodily actions that confirm the lead of the initiating actor (Flyvbjerg, 2001) . Resistant responses consist of discursive or bodily actions that either deny the lead of the initiating actor (Flyvbjerg, 2001) or amount to silence, by failing to confirm or deny the lead (Parpart, 2020). The nature of both a leading initiative and its response depends on the reasoning structure of specific actors in particular situations: they assess as being appropriate given their situated rationality—that is, given each of their own experienced positions, knowledge, and relations at their moment of interaction (Bevir & Rhodes, 2016; Bevir & Waring, 2017; Sullivan et al., 2012)? Actors’ situated rationality can thus explain how and why certain actor behaviours emerge in specific ways in the dynamics of power. By applying this situated analytical lens to power processes across the dimensions of knowledge, responsibility and legitimacy, we are able to observe the provision of public service as a two-way process in which both public professionals and service users play a potentially active role. In this way, we aim to unravel how consensus and equality manifest in the power dynamics between public professionals and service users throughout co-produced decision-making processes.
Research Design
Research Approach and Setting
We used focused ethnography as our research approach. This approach uses episodic participant observation and interviews in specifically selected settings in which the phenomenon under study is likely to occur; in our case, to examine the power dynamics in co-production between public professionals and service users (Cruz & Higginbottom, 2013; Kuiper, 2020). We focused on the situated rationality and agency of public professionals and service users: how they experienced and used their positions, knowledge and relations during their moments of interaction.
To do so, we selected an academic hospital that was implementing a shared decision-making (SDM) policy in their vascular surgery clinic to be the focal setting. SDM policy aims to co-produce legitimate decisions and a higher quality of care, in principle achieved by striving for consensus and a shared balance of power in decision-making processes. The surgeons at the clinic received SDM training via a short course in SDM-interview techniques and explained to us, the researchers, that they saw SDM as part of the hospital’s culture. The hospital incorporated the philosophy of SDM in its external communication, as shown on posters and flyers throughout the hospital and on the website, stating, “In this hospital, we decide together.”
We consider SDM to be an extreme case of service user involvement in co-production for two reasons. First, SDM takes place in the context of healthcare service provision, meaning that, in contrast to, for example, co-produced policy design, the decision-making process directly affects the lives of every involved user, since patients’ interests are directly at stake in the decision-making process. Second, surgeons have no policy pressure to dominate patients, in contrast to street-level bureaucrats charged with a regulatory task. This suggests that, in SDM settings, co-production grants service users considerable space to influence the decision-making process.
Data Collection and Ethical Considerations
Data were collected by the first author in January and February 2019. The first author observed the patient-surgeon consultation of 41 patients, each of whom was seen by one of 10 surgeons. In addition, both parties’ experiences before, during, after and in between their meeting were captured through a mix of observations and post-consultation interviews. Specifically, the first author held 15-minute post consultation-interviews after each consultation with each patient and their family or friends, if present, in an appointed private room. During these interviews, the first author asked the patients and their companions to reflect on their consultation with the surgeon as they had just experienced it. At the end of a surgeon’s entire consultation block, the first author also held 20-min post consultation-interviews with the surgeon to capture their experiences of each consultation. Seven surgeons held between 3 to 13 consultations each. Notably, three of the participating surgeons did research on SDM practices within the department. The first author was open with the surgeons and patients about her role as a researcher, informing them that she wanted to learn more about the interaction between patients and surgeons. She limited her involvement during the surgeon-patient consultation as much as possible, to avoid interfering in the care process and to gather naturally occurring data.
The research gained permission from the ethics board of the academic hospital and was conducted in compliance with the Netherlands Code of Conduct for Academic Practice. All participants received a letter disclosing the study before their consultation appointment and gave explicit verbal consent for the observations and interviews. Two participants withdrew their consent days before the appointment, explaining they had no interest in the study. Four patients agreed to allow the first author to observe their consultation with the surgeon, but refused to participate in interviews. To protect the participants’ privacy and respect the sensitive nature of the consultations and interviews, all data have been anonymized and fieldnotes were only taken by hand; no recordings were made. Fieldnotes primarily consisted of descriptions of what the actors said, how they said it, and their body language. In addition, time schedules and organizational practices, such as moments of communication between surgeons and nurses, were observed and recorded by hand. Later, all of these raw, handwritten fieldnotes were digitally developed into thick descriptions.
Data Analysis
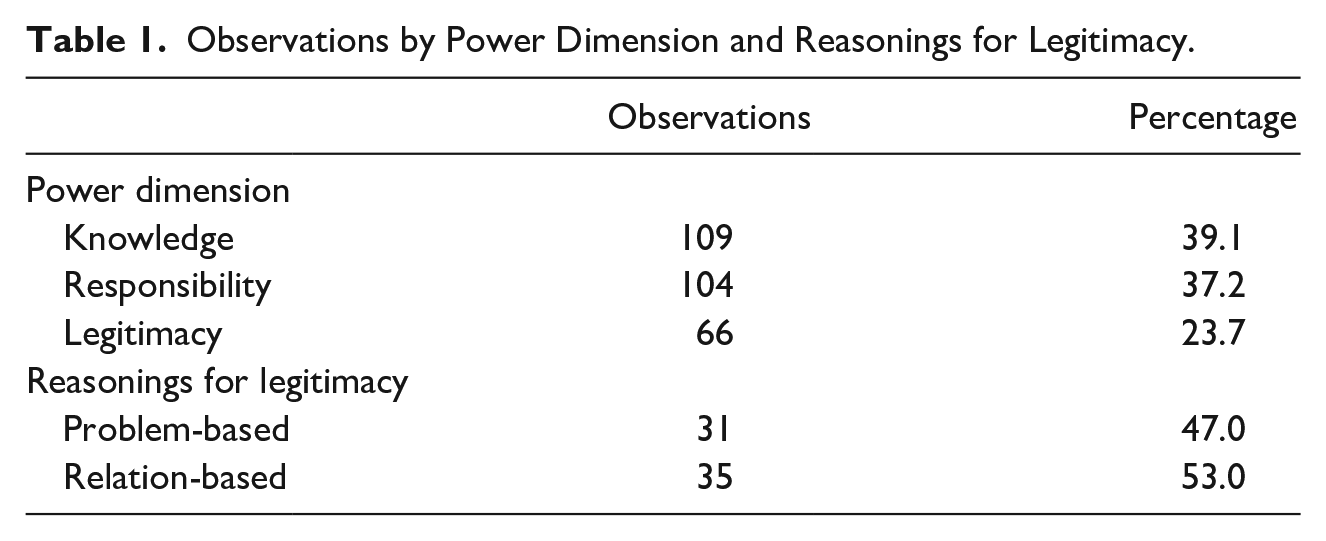
The data were analysed in three stages. In the first stage, we abductively constructed our two-way analytical lens by iteratively studying the first author’s extensive fieldnote descriptions and two strands of the literature: on power and on interactions between public professionals and service users. This iterative strategy helped us deconstruct the interactions between surgeons and patients into (a) leading initiatives and (b) following or resistant responses. Likewise, this approach helped us observe the non-vocal, or silent, forms of resistance. In the second stage, we used our two-way lens to analyse how power processes were constructed through specific situated actions. This allowed us to identify actors’ varied strategies, such as future-scenario sketching, responsibilization, consent-seeking and comfort-seeking. In the third stage, we first axially coded (Boeije, 2010) how these strategies could be categorized before linking them to the literature on power. In this way, we were able to identify three dimensions of power—knowledge, responsibility and legitimacy, each of which helped structure the observed co-production processes; this ultimately revealed that the process of power acquisition is driven by actors’ collective efforts to determine which knowledge to adhere to, how to divide responsibilities, and under which circumstances decision making should be considered legitimate. By selectively coding (Boeije, 2010) how each of these three power dimensions were reflected in the first author’s fieldwork observations, we also were able to illuminate two ways in which the three dimensions were interlinked: through problem-based and relation-based reasoning structures for legitimacy. In the end, the knowledge and responsibility dimensions were identified most frequently in the data, a phenomenon explained by an observed pattern: patients and professionals would first shift between conversations about knowledge and responsibility until they, together, had constructed a reasoning deemed as legitimate by both (see Table 1).
Observations by Power Dimension and Reasonings for Legitimacy.
Findings
Our results show how surgeons and patients engage in the construction of power dynamics through the use of leading initiatives and by reacting to these initiatives with either a following or resistant response. We also identify three key dimensions to their power dynamics: knowledge, responsibility and legitimacy. In this section, we explore how each of these power dimensions manifested and how they were interconnected following two different reasoning structures used by both actors throughout the decision-making process.
Knowledge Dimension
Throughout their shared decision making, surgeons and patients employed different strategies to determine which, and how, knowledge would be used. Surgeons often would use “scenario-sketching” to introduce a leading initiative, explaining different treatment options according to the treatment’s international guidelines, associated risks, and short- and long-term effects given the individual’s situation—including the patient’s lifestyle, medical history, and the bodily and mental experiences. For example: Patient 8 (male, 72 years old) to Surgeon 6: I think the constriction in my veins is causing me pain. I haven’t been able to walk very well for a long time. Also, I have lung problems, which makes it difficult to determine where my complaints are coming from. Surgeon 6 nods and responds: And do you also enjoy walking? Are you the running type? Patient: Well, not really. No, never have been. Surgeon: How would you feel if your ability to walk were diminished even further? Patient: Well, annoyed, of course. Surgeon: When, for example, you go to the supermarket, do you go by car? Patient: Yes, yes, I would rather drive. I’m not athletic. Wife of Patient 8: No, he doesn’t like walking at all. Surgeon: These are important things to think about. Surgery could improve your ability to walk, but also entails all kinds of possible complications. You could also say, “Well, from now on, I’ll take my mobility scooter so I don’t have to walk and my legs won’t bother me.” The patient nods. (Fieldnotes, February 2019)
Some patients resisted the lead of surgeons by, for example: not reading the medical information they had received prior to the consultation, not going along with the surgeon’s proposed future scenario—often out of fear of the suggested treatment—and/or differently interpreting or valuing the medical knowledge and solutions the surgeon suggested. These acts of resistance could be voiced or silent. Some patients would initially appear to follow the surgeon’s “scenario-sketching reasoning” during the consultation, only to realize in the post-consultation interview that they (or their companions) had not fully understood the information presented, and therefore felt unable to follow the proposed scenario. For example: During his post-consultation interview, after Patient 8 (male, 72) had just claimed that everything was very clear and that he will think about it, his wife interjected: You didn’t know what the surgeon was talking about – the complications you can get after treatment – you just went along with what the surgeon was saying. You didn’t understand what the consequences implied in the long run. (Fieldnotes, February 2019)
While most patients expressed having avoided “too much” medical information prior to meeting with their surgeon, some took a knowledge-leading initiative by emphasizing the value of their own “lay” knowledge—that is, based on their own experiences (physical, social or emotional), information gained from the internet, and/or the advice or hunches of family and friends. For these patients, such factors were relevant considerations in their decision-making process. For instance: Patient 17, in a post-consultation interview: I expected I’d need to convince the doctor of my complaints, so I prepared a whole story – I was prepared for resistance. But it didn’t seem necessary. I had a good story and have shown the motivation to change my situation. Surgeon 7, in a post-consultation interview: [Patient 17] really wanted surgery, so I went along with him, because I understand his frustration. We need to do more research in his case, and we’ll see during his next appointment. I once had a patient who could still walk four, five kilometres at a time, but said, “I really want to do a four-day, 40k walking competition.” He really wanted it, so I did the surgery to let him participate.
Surgeons would follow patients by incorporating the leading initiatives of patients into their own scenario-sketching method. When patients suggested taking a risk that surgeons believed to be unfounded, surgeons would resist the patient’s lead and correct them by referring to the scientific literature and their acquired expertise. For example: Surgeon 8 to Patient 27 (79 years old): Waiting or doing surgery, those are the options. Patient 327 laughing nervously: Surgery, I don’t know about that. I’ve understood that 50% don’t survive. Surgeon, looking surprised and seeking eye contact: Then I need to explain more about that: about what the statistics tell us and what we do in this hospital.
Responsibility Dimension
The responsibility dimension of power was observed when surgeons and patients discussed who is responsible for which part of the decision-making process. Surgeons regularly took the lead by initiating that patients should be responsible for the decision-making process, for example, by emphasizing that the decision should depend on their lifestyle choices. In our post consultation-interviews, every patient expressed feeling like a “layperson” in the decision-making process. Some patients saw their “lay role” as a reason to accept responsibility for the risks of decision making: “If I do nothing, then I’m also taking a risk. I know that being treated at a hospital entails a certain level of risk, I can accept that” (Patient 1 [male, 64] in a post-consultation interview). Surgeons often indicated that patients did not always recognize the extent of their personal responsibility for their own health, for example: Surgeon 7 to the first author, in between consultations: I don’t know if you’ve already picked up on it, but it’s a particular type of patient, the vascular patient. First author: I’m not sure I have, actually. Surgeon 7: A lot of smoking, little exercise, calcification of the veins – and then they come in here with their symptoms, but they’re not actually taking their vascular problem that seriously.
Often, surgeons would actively encourage the patient’s relatives and friends to participate in taking responsibility for the decision-making process: After examining the lower leg amputation of Patient 20 (female, 45), which failed to heal sufficiently, Surgeon 8 suggests that further amputation will probably be necessary. Surgeon: Where is [patient’s partner] today? Is there a reason he’s not here? Patient: He’s working. Surgeon: You are still together, right? Patient: Yes, yes. Surgeon: How does he feel about all this? Patient: It hurts him to know I’m in so much pain. He knows I’m a fighter, but he sees how this is breaking me. Surgeon: Talk about it at home. It’s important you both feel good about surgery. Patient nods.
For their part, family and friends were generally willing to brainstorm with the patient about how their lifestyle and future prospects could affect the decision-making process: Surgeon: You should consider whether it will still be possible to live independently at home, and whether you’ll recover enough to be able to walk again. Whether you can manage it together at home. The surgeon looks from the patient to his partner and daughter. Daughter: And if we do nothing? Surgeon: Look, if the aneurysm ruptures, then it ruptures and you’ll need acute surgery anyway. But as long as it doesn’t tear, nothing is wrong. Some people live an entire life with an aneurysm without any tearing. The question is really whether you want to take that risk and what you find important in life. Daughter nods: We’re going to have a good conversation about this at home.
In contrast, some patients resisted accepting responsibility for the outcome of the decision-making process, especially when lifestyle adaptations were put forth as prerequisites for surgery. For example, in the words of Patient 21 (male, 66) during a post consultation-interview: “I do whatever I want! And I’ll keep on smoking, the doctor can’t tell me what to do—whether surgery makes sense or not.”
Counter to the group that saw their lay role as a reason to accept responsibility in the decision-making process, another group viewed this same role as a reason to responsibilize the surgeon. Especially when surgeons posed open questions, such as, “What would you prefer?” patients often would try to reflexively elicit an opinion from the surgeon as to the best treatment option: “I don’t really have an opinion. I’m here as a layperson, and then we see what happens” (Patient 30, male, 72).
As Surgeon 9 stated in a post consultation-interview, the surgeons would only accept responsibility when a care plan fit their own views: “We’ll never do anything we deem medically irresponsible.” This is also illustrated by the following passage, observed during a consultation: When Patient 24 (female, 72) expresses a desire for surgery on her crooked toe because she finds it embarrassing – also communicating her mental health concerns due to being bullied in the past, Surgeon 8 responds: Toe surgery will pose new medical risks, with potential amputation as a consequence. These risks don’t outweigh living with a crooked toe. I’m sure no one will bully you for it. Looking disappointed and confused, Patient 24 continues to repeat her wish for the surgery, after which Surgeon 8 resolutely responds: Mrs. [last name of Patient 24], I’m not going to do it. [Silence, looking at the patient.] But we can think about alternatives. What about custom shoes? Patient 24, later, in her post consultation-interview: I may start to think about talking to a shoemaker. . . but first, I’ll explore whether another hospital is willing to help me.
Legitimacy Dimension
The legitimacy dimension of power was observed when surgeons and patients sought to determine whether a decision meshed with their own assumptions around social norms and whether it was accepted by both actors. Surgeons would first try to establish legitimacy by seeking consent from patients for the decision the surgeon deemed best. If necessary to achieve this goal, surgeons would lengthen the consultation time or make an extra appointment to postpone the decision-making moment. Surgeons’ pursuit of consent was linked to their professional ethics: “As a surgeon, it’s my duty to give a patient all the time they need” (Surgeon 6 to the first author, in between consultations). Moreover, surgeons regarded patient consent as critically important, even when its acquisition justified resisting organizational pressures, as the following illustrates: First author to Surgeon 8: The nurse just came in, for a second time. She’s stressed about the growing wait time. Surgeon smiles, friendly: My conversations with patients are often about life or death. I won’t rush such a conversation to stay within the fifteen minutes. Patients are scared and want to know where they stand – and as long as I’m a surgeon, I’ll take whatever time is necessary to help them.
Patients expressed appreciation for the long consultation time with surgeons, with some even indicating they had come to this specific hospital because of its reputation for allowing plenty of time for the decision-making process.
When patients refrained from giving verbal consent, either by resisting the surgeon’s preference or remaining silent, surgeons would gently exercise their power to intrinsically motivate patients to choose their preferred treatment option, as in the example below and explained by Surgeon 5 in a post consultation-interview: “Then I emphasize the benefits of option A and the downsides of option B, and I ask for the opinions of family and friends. Or I suggest they think about it again, and make a new appointment next week.” After stamping his feet and firmly throwing his walking stick on the bed in the consultation room, Patient 33 (male, 74) sits down on a chair with his arms crossed and refuses to look at the surgeon. Ignoring the man’s body language, Surgeon 9 shows the man the results of his CT scan and explains several treatment options. The patient remains silent, staring out the window. Surgeon 9, looking at the patient, together with his daughter and wife: I think you’re too disappointed today. You’re understandably disappointed by the test result, which was worse than we’d expected, and you’re disappointed with the waiting time, which is just too much. I suggest you calmly think about it and that we see each other again next week to discuss treatment options again.
Patients’ behaviour suggested a link between their comfort level and their perception of the decision-making process as legitimate. When patients did not see their health problem as urgent or felt emotionally unprepared to take responsibility for decision making—or to have the surgeon take responsibility, then they would either opt not to decide or fail to show up for their appointment at all. As Surgeon 6 commented between consultations: “Well, patients can be difficult, they have different priorities in life. They often don’t show up for their appointments, ‘Sorry, Doc – I was too tired!’ Yep, you’ve got to love the vascular patient!” This quote also illustrates the equally influential role patients can play in determining the pace of the decision-making process.
Moreover, patients sought comfort by translating medical knowledge into feelings. Surgeons often tried to temper patients’ emotions by seeking eye contact, sharing their medical knowledge, and allowing silences to gauge their state of mind. For example: Patient 39 (female, 79), insecure, with big eyes pointed at the floor: I pretend to take it lightly, but I keep on thinking, “What am I supposed to do?” Surgeon 8: In the Netherlands, 8% of women die in open-heart surgery. [Silence, looking at the patient and her son.] And we think that’s a very high number. [Patient and son nod, both with a hand on their mouth.] So, we looked at what those numbers were in our hospital and we saw that, in fact, no patients have ever died with us during that type of surgery. Because we carefully select for eligibility. Patient 39, relaxing her shoulders and laughing: See, that’s what I wanted to hear!
Surgeons would resist following patients who sought a treatment they deemed medically unsafe or when they believed a patient was thinking irrationally, as illustrated by both the woman with the crooked toe and the frustrated patient whose decision-making consultation was postponed.
Reasoning Structures for Legitimacy: Problem- and Relation-Based Reasonings
According to our observations and analysis, the process of negotiating power in co-produced decision making takes place across three interconnected power dimensions, all of which shape one another. The order in which these dimensions take priority, or play off each other, appears to depend on actors’ adherence to one of two reasoning structures—problem-based or relation-based reasoning; we identified both to help explain the behaviour and perspectives of the patients and surgeons.
When actors followed a problem-based reasoning structure, their primary aim was to address the problem at hand; that is, their actions were guided by their definition of the problem. The problem-based structure reasons: “First the knowledge I deem relevant structures how I believe responsibility should be divided between patient and surgeon; then these ideas about knowledge and responsibility shape my opinions about legitimate decision making.” Both surgeons and patients were seen to display problem-based reasonings, for example, when surgeons would translate patients’ lay knowledge into treatment options through their use of scenario-sketching. Consequently, patients would accept responsibility for decision making because they thought their perspective was being taken into account.
Similarly, when patients sought comfort or surgeons sought consent, they would often refer to their established ideas about knowledge and responsibility: decisions were considered legitimate when their “assigned roles” clarified how knowledge should be interpreted. For example, as described above, some patients believed the surgeon should be responsible for decision making, because (s)he is the expert. When these types of roles had been established, the surgeon would steer towards legitimacy by translating his or her knowledge about risks into emotions, as the following example suggests, in which “centimetres” translate to “level of worry”: Surgeon 7 to Patient 13: The examination indicated the aneurysm grew from 2.2 to 4.8 centimetres. Patient 13 (male, 78): When should I start worrying? Surgeon 7: Fortunately, there are very clear international agreements about aneurysms: under 5.5 cm, the risks outweigh the benefits of surgery. That means the conversation about surgery only becomes important from 5.5 cm onwards.
However, when patients took the lead in the consultation by trying to convince the surgeon of their analysis of the problem and its possible solutions, surgeons would resist the patient’s problem-based reasoning if they disagreed with the patient’s analysis. First, they would try to correct the patient using their medical knowledge and experience. If the patient failed to follow their response, then surgeons would set boundaries around the patient’s problem-based reasoning by switching to a relation-based reasoning. Then, the surgeons would emphasize their expert role and argue that, because they are the surgeon, they cannot allow themselves to follow the patient’s “lay knowledge”; instead, the lay knowledge should coincide with their medical perspective. For example: Surgeon 7 to the first author, in a post consultation-interview: In the case of Patient 11, with such an old man, I think to myself: “Stay conservative [non-interventionist] as long as possible.” It’s hard to know what’s best. After the first author then asks whether it would be useful to let the patient co-decide, Surgeon 7 responds: That’s a good question, we [the surgeons] talk about it amongst ourselves: “Are the possible treatment options equally useful?” Often, we see more disadvantages to one of the choices. And are you supposed to then leave it up to the patient, if the options aren’t 100% equal?
In contrast, some patients would resist the problem-based reasoning of surgeons by, for example, not reading the medical information they had been given prior to their consultation, not agreeing to future scenarios proposed by the surgeon when they feared the suggested treatment option, and/or interpreting or valuing the presented medical knowledge and solutions differently. These acts of resistance to the surgeon’s problem-based reasoning structure were sometimes voiced and sometimes silent. Some patients would follow their surgeon’s problem-based reasoning structure, but found it difficult to accept their own personal responsibility due to other factors that interfered with their maintenance of a healthy lifestyle. For example: Surgeon to patient (male, 50): You’re 50 now. You still have a long time to go. If you want to grow old, lifestyle is everything, lifestyle is so important. [Surgeon clenches his fist and shakes it firmly, motivating, like a sports coach.] What are the things you’d like to improve? And how do you want to get there? Patient: Well, I could try to quit smoking again. I tried to. But then my sister died. . .
When actors followed a relation-based reasoning structure, their primary focus was on the distribution of responsibilities between the surgeon and patient; that is, their actions were guided by their definition of actor roles. The relation-based structure reasons: “First I consider who is responsible for what in this decision-making process, then I consider what these roles imply in terms of how knowledge should be treated, and then these two ideas about roles and knowledge shape my opinions about legitimate decision making.” Similar to the problem-based reasoning structure, both surgeons and patients showed adherence to this structure at times. For example, when patients and surgeons established a “following lay role” for the patient and a “leading expert role” for the surgeon, the implication was that surgeons would determine the prioritization of medical knowledge in the decision-making process. For example: Patient 30 (male, 72): Do you need any information from me? I brought all the papers, but I’m just a layperson, I have no idea what you need. Surgeon 2, laughing: Then I have an advantage – your disadvantage is my advantage! [Later, after sharing information about the patient’s running test and diagnosis.] Tell me, what do you think we’re going to do? Patient: Pfff. . . I have no idea. Medication? Surgeon: Maybe. . . But that’s not the first choice. Anything else? Patient, silent at first, and then with big eyes: I really have no idea, I’m just a layman. Surgeon, smiling: Great! Then I can be the doctor. You’ll do it yourself – you’ll start with physical therapy.
In the post consultation-interview, the patient indicated he had found the surgeon capable and felt good about the decision to start with physical therapy, but also mentioned finding it strange that the surgeon had not shown interest in the information he had brought with him.
In fact, a number of patients indicated finding their relationship with the surgeon—that is, the level of comfort they felt in their conversation with him or her—more important than the proposed solutions. For example: Patient 14 (female, 50), in a post consultation-interview: I asked the doctor to be honest, that’s important – it’s good when patients ask doctors to be honest. Even when things are unclear. If the doctor explains they don’t know what’s best, then I actually trust that doctor more. It’s not just about what they can technically do, it’s also about being honest with the patient. Patient 15 (male, 78), in a post consultation-interview: Complications are technical matters and I don’t hold anyone accountable for them. But sloppiness in communication or information, being treated like a toddler – I do resent that!
Some patients resisted addressing issues of responsibility before discussing medical knowledge, steering the relation-based structure instead towards a problem-based structure: Patient 1 (male, 64), in a post consultation-interview: I don’t want to have to suggest treatment options myself – I always think, “Doctor, just tell me what’s going on.” What do they mean by “what would you like?” I just want to know what’s wrong with me!
Similar to the problem-based reasoning structure, surgeons would follow a relation-based structure when they deemed the patient’s leading initiative to be acceptable medically. Although patients would follow a relation-based reasoning structure when they felt comfortable with the surgeon in the “leading expert role” and themselves in the “following lay role,” they would resist this structure when they felt unheard or when they disagreed with the expert-laymperson role division or how knowledge was being treated. This sometimes posed a challenge for surgeons, who are trained to determine the necessity of a medical intervention, but can struggle with cultivating patient comfort and consent: Surgeon 7 to the first author in a post consultation-interview: There’s an artificial cut-off level at 5.5 cm for aneurysms. If you do surgery at 5.5 cm, no one will say: “That’s strange.” Some people are a little weak, but I still try to push them to 6 or 6.5 cm. But that’s also the hardest part: how do you get patients on board, in a positive way, throughout the decision-making process? Do they truly understand the consequences? That’s why I always want to hear from them: how is the issue currently impacting their life?
In both reasoning structures, surgeons displayed a focus on generating consent from the patient for a specific treatment option, while patients focused on achieving a sense of comfort: when the surgeon understands me, we will come to the best solution.
Discussion
The concept of co-production offers policymakers the potential to improve the decision-making practices of public professionals and service users by bucking the traditional top-down hierarchy of service delivery. Critics, however, question this potential, arguing that co-production relies on an enchanted, instead of an empirically demonstrated, assumption that collaborative decision-making practices are based on consensus and equality (Bevir et al., 2019; Bouchard, 2016; Dudau et al., 2019; Steen et al., 2018). By empirically examining how consensus and equality manifest in the balance of power between professionals and patients throughout their co-produced decision-making processes during clinical consultations, we aimed to contribute to understanding the possibilities and limits of collaboration in such settings. this assumption. We also sought to inspire current thinking about co-production by providing a theoretically and empirically grounded view of the intricacies of co-production as practiced by professionals and patients on the ground. We see four main theoretical contributions of our research as well as a number of practical and research-design implications.
First, our results provide deeper insights into the power dynamics between patients and professionals in co-produced decision making. Previous research focused on the central role of professionals in co-production as either emancipating or manipulating the patient (Alford, 2014; Avci, 2023; Bevir et al., 2019; Steen et al., 2018). Our results show that patients and professionals indeed face such tensions during co-produced decision making by zooming in on how these tensions arise and how both actors navigate the process of negotiating power. In particular, our findings suggest that the power dynamics between patients and professionals in co-produced decision making are shaped by three interconnected power dimensions: (a) knowledge, as actors initiate and respond to each other’s views on which knowledge is relevant; (b) responsibility, as actors probe how responsibility should be divided; and (c) legitimacy, as actors seek to establish the legitimacy of treatment options by cultivating agreement along either a problem-based or relation-based reasoning structure.
When patients and professionals followed a problem-based reasoning structure, knowledge played a central role in determining the legitimacy of co-produced decision making. While scholars have argued that patients’ lay knowledge is not always considered or prioritized in decision making (Crompton, 2019; Watson, 2024), we repeatedly observed its explicit inclusion in the conversation. Nonetheless, despite the promise of co-production that “knowledge sharing and combining” will break down the hierarchy between patients and professionals (Avci, 2023; Farr, 2016; McMullin & Needham, 2018), our results show that the use of a problem-based reasoning structure does not appear to overcome the dominance of the medical specialist. Surgeons can easily persist in framing both types of knowledge within the limits of what they deem medically responsible, aligning with research showing both that professionals can maintain control over the outcomes of co-production (Frederiksen & Grubb, 2023; Haug, 2024) and that there is an inherent tension between expert and lay perspectives (Crompton 2019; La Grouw et al., 2020; Morden et al., 2012). Accordingly, our results suggest that a problem-based reasoning structure obscures which knowledge is prioritized and why.
When patients and professionals in our study followed a relation-based reasoning structure, issues of responsibility were observed as initially driving the pursuit of legitimacy in co-produced decision making. By employing responsibilization methods, surgeons were able to “share” their decision-making responsibility, allowing them to both claim the leading expert role and make the patient responsible for their “decision” to trust the professional. The relation-based reasoning structure thus appears to confirm the manipulation narrative (Agranoff 2016; Bevir et al., 2019; Osborne et al., 2021; Palumbo & Manna, 2018) by allowing patients to be pushed into a passive lay role in which they must accept both the medical decision itself and its associated risks. Yet, as our results show, the relation-based reasoning structure undermines the manipulation narrative in its acknowledgment of the inherent inequality between patients and professionals: both actors were aware of their different roles and what these implied for how knowledge would be treated throughout the decision-making process. While scholars have warned that “professional power” can endanger transparency in collaborative decision making (Bevir et al., 2019; Steen et al., 2018), our case study reveals that this explicit distribution of responsibility may instead be experienced as improving transparency: it “explains” to patients why knowledge is treated in certain ways. In the setting of a vascular surgery department, where patients were faced with severe health risks that could potentially result in death, the relation-based reasoning structure provided patients with a level of certainty that addressed their need for comfort. This suggests that, when patients perceive their health risks as significant and urgent, they prefer receiving guidance and certainty during the decision-making process over control and rationality (as also argued by Willis, 2016). These insights into how patients and professionals socially construct the legitimacy of decisions—by navigating their (implicit) agreements around the use of knowledge and divisions of responsibility—suggest that relation-based reasoning “empowers” service users more than problem-based reasoning by contributing to the transparency of the decision-making process. Alongside this deepened understanding of how a relation-based reasoning can empower patients, our research provides insight into how this same reasoning can, in fact, also empower the professional—albeit through dynamics that extend beyond the direct patient-professional interaction. This insight helps answer the question of how professionals are (dis)advantaged in co-production (Bevir et al., 2019; McMullin, 2025; Steen et al., 2018) and how they can be encouraged to share their power (Haug, 2024). Surgeons’ dependence on receiving patient consent for proposed treatment options both releases them from being solely responsible for decision making and grants them more control over the duration of the decision-making process, which they can use at their discretion to resist managerial or organizational pressures.
On a broader level, our second main contribution is to highlight how the wider policy environment influences the quality of professional dominance in co-produced clinical decision making. In our case study, the “non-interventionist culture” of the hospital motivated surgeons to share their power and responsibility with patients, and patients chose and kept returning to the hospital because of the doctors’ reputation for “taking their time.” In addition to revealing how the wider policy environment can affect co-production behaviour and foster willingness among professionals (Farr 2016; Haug, 2024; McMullin & Needham 2018), these results bolster previous research showing that organizational culture and competition between hospitals can lower the chances of professionals engaging in “dark” practices, such as the misuse of a knowledge position or symbolic use of co-production (Bevir et al., 2019; Martin, 2008; Steen et al., 2018). Given these insights, we contend that empowering the professional within their policy environment can in fact enhance co-produced decision making between patients and professionals.
Third, our results challenge the policy assumption that consensual and equal decision making in co-production is even possible (Avci, 2023; Alford, 2014; Haug, 2024). We did not observe the achievement of consensus or equal standing. Instead, our results suggest that legitimacy in co-produced clinical decision making depends on the consent of the weaker actor (the patient) vis-à-vis the dominant actor (the professional). Even though patients are the weaker party in the decision-making process, surgeons still depend on their consent to pursue their preferred treatment option—consent that patients only seem willing to grant when they feel comfortable. This mutual dependency in the context of professional dominance means that co-produced decision making is both “focused on consent”(as opposed to achieving consensus) and “focused on achieving less inequality” (rather than establishing equality between professionals and service users). Therefore, our results add nuance to both the emancipation and the manipulation narratives of co-production by showing how co-produced decision making in healthcare delivery is not a one-way power transfer from professional to patient, but rather an intricate and dynamic process in which the actors depend on each other to reach “legitimate decisions.”
Fourth and lastly, the study contributes to the literature on street-level bureaucracy by offering an in-situ understanding of what “interaction” entails in public-service provision. Currently, street-level bureaucracy studies tend to use a one-way reasoning structure from the professional’s perspective as a framework for understanding the interaction between public professionals and service users: the dominant focus is on the actions and moral reasoning of the professionals, who may use discretionary space to, for example, provide tailored solutions, manage their caseloads efficiently (Lipsky, 2010; Zacka, 2017), or employ motivational strategies to “activate” service users along policy lines (Grandia et al., 2020; Gřundělová, 2021). Street-level bureaucracy research could benefit from adopting the two-way perspective employed here as it sheds light both on the situated agency of service users and on the intricate power dynamics through which service users may steer professionals to amend their service offers.
Our study also has several practical implications. To start, the findings suggest a need to temper both optimistic and pessimistic policy expectations of co-production. Public service policies that promote co-production should be cautious about claiming an emancipative effect, as this risks obscuring the dominance of professional power. Although service users can, and usually do, play an influential role in the creation of value in public service delivery, their influence cannot be separated from that of the professional. In co-produced healthcare decision making, professional power through knowledge asymmetry cannot be fully avoided and arguably is even essential. Therefore, from an ethical point of view, pushing for patient-driven co-production in high-risk medical contexts may be questionable, as it may not be fair to hold patients accountable for their own treatment decisions or to release professionals from the responsibility of creating value throughout medical decision-making processes.
Care organizations and professionals should be aware that co-produced services involve a two-way process that works towards cultivating comfort and consent, not consensus. Although the patients in this article did display agency, we know from prior research that older patients, patients with severe pain, patients who are marginalized, and patients who are socioeconomically disadvantaged are less likely to challenge professionals or refuse to comply with collaborative decision-making efforts (Fledderus et al., 2015; Salander & Moynihan, 2010; Willems et al., 2005). In these cases, collaborative decision-making processes may even reinforce and perpetuate existing social and power structures (Bevir et al., 2019; McMullin, 2025; Steen et al., 2018), making it especially important for professionals to take extra care in guiding vulnerable patients or those from lower socioeconomic backgrounds through the power dimensions of the co-production process (Chiapperino & Tengland, 2015; Willems et al., 2005).
In addition to avoiding claims about the emancipative effects of collaborative decision making, we recommend that policymakers ensure professionals have adequate time and resources to receive training on how to effectively incorporate the patient perspective. Such training should cover how to (a) take the time to listen to patients’ perspectives on their health problems, (b) foster the legitimacy of decision making by creating transparency around knowledge and responsibility, and (c) connect the lay and medical perspectives for translation into future scenarios. Healthcare practices will invariably benefit from such training as many professionals currently lack the communicative skills needed to effectively include patient perspectives (Mohd Salim et al., 2023). In addition, to navigate these pressures of collaborative decision making, professionals should be given sufficient consultation time and autonomy—a finding supported by research conducted during the COVID-19 pandemic, when healthcare professional autonomy was shown to be critical to managing uncertainty and rapid change. Instead of tightening the grip in response to uncertainty, policymakers should ask professionals, “Where are you trying to go and how can we help you get there?” (Mannion et al., 2023). Likewise, patients should be supported in developing an awareness both of the broad range of co-produced possibilities when interacting with professionals and of their own power to influence co-produced decision-making processes through their exercise of consent or resistance. As our study shows, these dynamics are often inherently subtle and complex: even silence on the part of the patient—that is, a lack of explicit consent—appears to be a powerful action in response to professionals’ leading initiatives in decision making.
Strengths and Limitations
The strength of this study lies in its systematic unravelling of the in-situ professional-patient interaction by means of an abductively developed analytical lens. This two-way power lens shows how consensus and equality in co-produced decision making are in fact not feasible when one actor remains dominant, even when “power equalizing” practices, such as knowledge and/or responsibility sharing, are applied. Decision making thus depends on actors’ willingness to follow each other through the three dimensions of power(knowledge, responsibility and legitimacy) according to the reasoning structure that best fits their own needs. However, the degree of professional dominance in co-produced decision making might be case-dependent. Specifically, our findings show that how a patient experiences their health problem matters for their willingness to follow the surgeon: patients displayed following behaviour when they experienced their health problem as threatening and displayed resistance when they perceived it as non-threatening. In addition to its theoretical importance for studying co-produced public service processes, our two-way lens supports the normative argument that service users are in fact better off assuming an active, rather than passive, role in clinical decision making. Moreover, while many co-production case studies focus on local specifics that are difficult to generalize (Steen et al., 2018), our two-way power lens can easily be transferred to other work in settings involving public professionals and service users.
Nevertheless, this lens has its limitations as well. It cannot provide insight into how collective-level issues are affected by service-level practices – for example, whether and how spending more time on decision making affects the public value of healthcare, such as its accessibility and affordability (McMullin & Needham, 2018). Given that longer consultation time could increase process costs and pressure on staff capacity (Vennik et al. 2016), future research needs to both study the connection between individual and collective-level public value (Jo & Nabatchi 2019; Osborne, 2018) and explicitly focus on the dominant role of medical professionals in shaping this link. In addition, given prior research showing that richer, highly educated citizens more easily voice their preferences in and benefit from co-production compared to those with fewer financial resources and less formal education (Hastings, 2009; Salander & Moynihan, 2010; Willems et al., 2005), further studies are needed to explore how socioeconomic, cultural and social aspects influence the balance of power. For example, future research should investigate whether, and if so why, service users with specific characteristics have fewer opportunities to influence co-produced services, particularly regarding the inclusion of lay knowledge, professional power to steer towards scenarios, and the prioritization of specific, interconnected reasoning structures. Such questions could be addressed through longitudinal studies (for instance, following a diverse group of service users) or through comparative studies (e.g., examining public service organizations with different institutional incentives and organizational cultures).
Conclusion
To capture the balance and dynamics of power in co-produced services, we abductively developed an analytical lens with which we deconstructed how both public professionals and service users use their situated agency throughout their interactions. This two-way lens allowed us to observe how—in a case study of shared decision making in a vascular surgery department—such power processes were interconnected. These interconnections occurred as professionals and patients built their reasonings by navigating through three distinct dimensions of power: knowledge, responsibility, and legitimacy. We identified two reasoning structures through which both actors connected these dimensions: a problem-based reasoning structure, in which actors saw issues of knowledge as the basis for their power negotiations, and a relation-based reasoning structure, in which actors were mainly concerned with issues of responsibility. In both problem-based and relation-based reasoning structures, professionals and patients were aware of their unequal positionings and thereby motivated to seek (or withhold) consent.
These findings contrast with the oft-stated policy aim of co-production to achieve consensus and equality in decision making between professionals and patients. Remarkably, here both actors were viewed as being empowered by the co-production process, but in different ways. Patients were empowered when their lay perspective was included in the knowledge dimension of power, which occurred only within the medical boundaries set by the professionals. Professionals were empowered by their employing organization—for example, to claim more consultation time—in pursuit of patient consent, upon which they depended for the legitimacy of their preferred treatment options. Given these insights, co-production policies in settings where actors’ power differences are difficult to bridge may be more effective not when aiming for consensus and equality, but when focused instead on cultivating consent from the weaker party in a context of acknowledged unequal positions.
Footnotes
Data Availability Statement
This dataset contains sensitive personal information. Since participants only gave consent to the VU for this specific research, the dataset is not available upon request under any circumstance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.