
Abstract
The UK government’s leaders initially believed that it was among the best-prepared governments for a pandemic. By June 2020, the outcome of the collision between the government’s initial confidence, on the one hand, and the aggressiveness and virulence of COVID-19, on the other, was evident. The UK had one of the worst COVID-19 mortality rates in the world. This article explores the UK government’s response to COVID-19 from a public administration and governance perspective. Using factual information and statistical data, it considers the government’s preparedness and strategic decisions, the delivery of the government response, and public confidence in the government.
Points for practitioners
Possible lessons for testing through application include:
Use the precautionary principle to set planning assumptions in government strategies to create the possibility of government agility during a pandemic. Use central government’s leadership role to facilitate and enable local initiative and operational responses, as well as to take advantage of local resources and assets. Choose smart government responses that address tensions between the goal of saving lives and other government goals, and beware choices that are unsatisfactory compromises.
Keywords
Introduction 1
In 2020, the UK was one of a number of countries that suffered a relatively high loss of life as a result of COVID-19 but then managed to get the spread of the virus under control (at least until the autumn). One of the key issues to be addressed in this article is: how can we explain the UK government’s failure to contain the virus and prevent it spreading but then its success in getting the epidemic back under control?
The UK government’s handling of COVID-19 will be examined from a governance perspective. The key events and consequences of the governance of the pandemic will be analysed. This will entail looking at the preparedness for the pandemic, for example, in respect of the capacity for surveillance using Public Health England’s test and trace resources. The governance and coordination structures and the modes of crisis management (Baubion, 2013) used by the UK government will be analysed, and the transition that occurred in late March and April will be pinpointed as part of the analysis of the dynamics of the response. The critical nature of the risk assessments used in response planning will be highlighted, including their origins in a government pandemic flu strategy dating from 2011.
The final section concludes that the UK government’s planning and preparations for a pandemic ill-prepared it for COVID-19. It will also be concluded that the UK government made an abrupt transition in its mode of crisis management and then appeared to be engaged in a chaotic form of ‘muddling through’, starting with the decision to begin the first of two national lockdowns.
Governance of a pandemic
Baubion’s (2013) discussion of old and new ways in which governments manage crises can provide some ideas about the governance of COVID-19. He claimed that governments in the past mainly relied on ‘siloed approaches’, in which crisis management is on a sector-by-sector basis, rather than a national basis. He highlighted a number of specific features of a siloed approach: making risk assessments; developing emergency plans; budgeting resources for use in an emergency; stockpiling equipment and supplies; designing structures for the governance of crises; carrying out training; and running exercises and drills. Scenarios prepared by government experts, based on previous experiences, may be used as a tool in assessing risks and preparing plans. It may be inferred from all of this that the intent of this mode of crisis management is to create a government primed to execute a plan and resourced to provide response capacity.
Baubion (2013) also outlined a new mode of crisis management appropriate for novel crises, which can be characterised as being unprecedented and containing threats and risks that are unknown. In place of comprehensive planning using predefined scenarios, this new mode requires the formation of a response network that can adapt and innovate in response to a crisis. In essence, this second mode of crisis management is a whole-of-government and even whole-of-society approach. The national government is called on to facilitate the cooperation and partnership working of the entities that make up the response network. Strong leadership and shared principles and values are important (Baubion, 2013).
Other research and writing on governments operating in conditions of crisis, emergency or disaster provide further glosses to a discussion of crisis management.
Decision-making style
Two of the styles discussed in the literature are a command-and-control style and a pragmatic-experimental style. The command-and-control style may be seen as applicable to a traditional mode of crisis management. It may be assumed (wrongly or rightly) that it causes faster government action (Boin and ’t Hart, 2003). The alternative style of decision-making, based on pragmatic and experimental decision-making, could be suggested as appropriate for the mode of crisis management suited to novel crises. It incorporates learning, refinement of strategy and flexibility (Ansell and Boin, 2019).
National government’s organisational centralisation
Making a distinction between a strategic (top) level and an operational (lower) level, Boin and ’t Hart (2010: 362) claim that attempts by ‘strategic decision makers to plan and command each and every aspect’ of a response is a mistake. As implied in this statement, command-and-control and centralised decision-making might coexist.
Multi-level coordination through less centralised control could be seen as more suitable in the face of novel crises. Less centralised control might take the form of central leadership combined with local discretion (OECD, 2012).
Expert advice
According to Baekkeskov (2016: 302), ‘Experts often play important roles in crisis responses.’ His own study of the swine influenza pandemic of 2009/10 found that the Netherlands and Denmark had contrasting vaccination policies, and the experts were partly the cause of this. He also concluded that government-appointed experts might steer policy through their projections (scenarios) of future crises.
Government priorities and strategy and the nature of the expert advice provided to the government could interact in a variety of ways. A government that has decided on strategic planning for preparedness may put more emphasis on the expertise of mathematical modellers to support risk assessment, whereas a government seeking strategic agility in the face of a novel (pandemic) crisis may rely on public health expertise. Equally, the availability and influence of different types of advice might influence the government’s setting of priorities and strategic planning.
Strong leadership
Research has been published showing large international variations in leadership attitudes to the future and on avoiding uncertainty (Javidan et al., 2006). These attitudes could matter in relation to government decisions to maintain infrastructures for public health and the surveillance of epidemics in other countries, and to invest public money in hospital capacity in preparation for pandemics. That said, such foresight may be in short supply among national leaders; research has been reported which suggests that governments ‘settle for, and pay for, sub-optimal levels of safety’ (Boin and ’t Hart, 2003: 546).
During a crisis, strong leadership might be evidenced by the realism of leaders’ promises (Boin and ’t Hart, 2003). It seems likely that leaders will want to reassure the public as much as possible about the situation, and weak leaders may be tempted into making unrealistic promises about what the government can do and how quickly emergencies and crises will be over.
Competent response
A government needs to do the right things in preparing for, and responding to, a pandemic – and strategic decisions need to be executed in a way that is effective. The big decisions may include deciding how much effort and resources should go into prevention of the spread of a virus and how much should go into the treatment of very ill people. Also, for example, should the government choose measures to achieve aggressive containment and suppression through government programmes of testing, tracing and isolating, or should it choose measures to deliver containment and control through lockdowns?
Blame game
Arguably, there should be both government accountability and learning during and after a pandemic. Accountability and learning are likely to be intertwined in practice (Boin and ’t Hart, 2010), and it may prove difficult for governments to learn clear lessons because of the atmosphere created by what has been called the ‘blame game’ (Boin and ’t Hart, 2003). A blame game can be defined as consisting of public debates and disputes about who was to blame for mistakes or failures.
Elected leaders may suffer reputational damage in the blame game that may develop during and that follows a crisis. Baekkeskov (2016: 312) concluded his study of swine flu in the Netherlands and Denmark by saying that government ministers not only perceived the risks of getting blamed, but also sought to avoid blame: ‘The study found positive evidence that political leaders responsible for crisis management may take decisions with an eye to future blame games.’
Governments as well as leaders can be hurt by the blame game (Baubion, 2013: 21): The level of trust can be undermined because the government did not take the right decisions or did not appear to make its best effort to deal with the crisis. It can even be worse when people have the feeling that the government did not have a transparent and open approach, or that they were hiding either important aspects of the crisis or the failure of their approach. Clarifying how decisions were made and showing clear government accountability are the best ways of avoiding having the post-disaster phase turn into a looming political crisis, which would further diminish levels of trust.
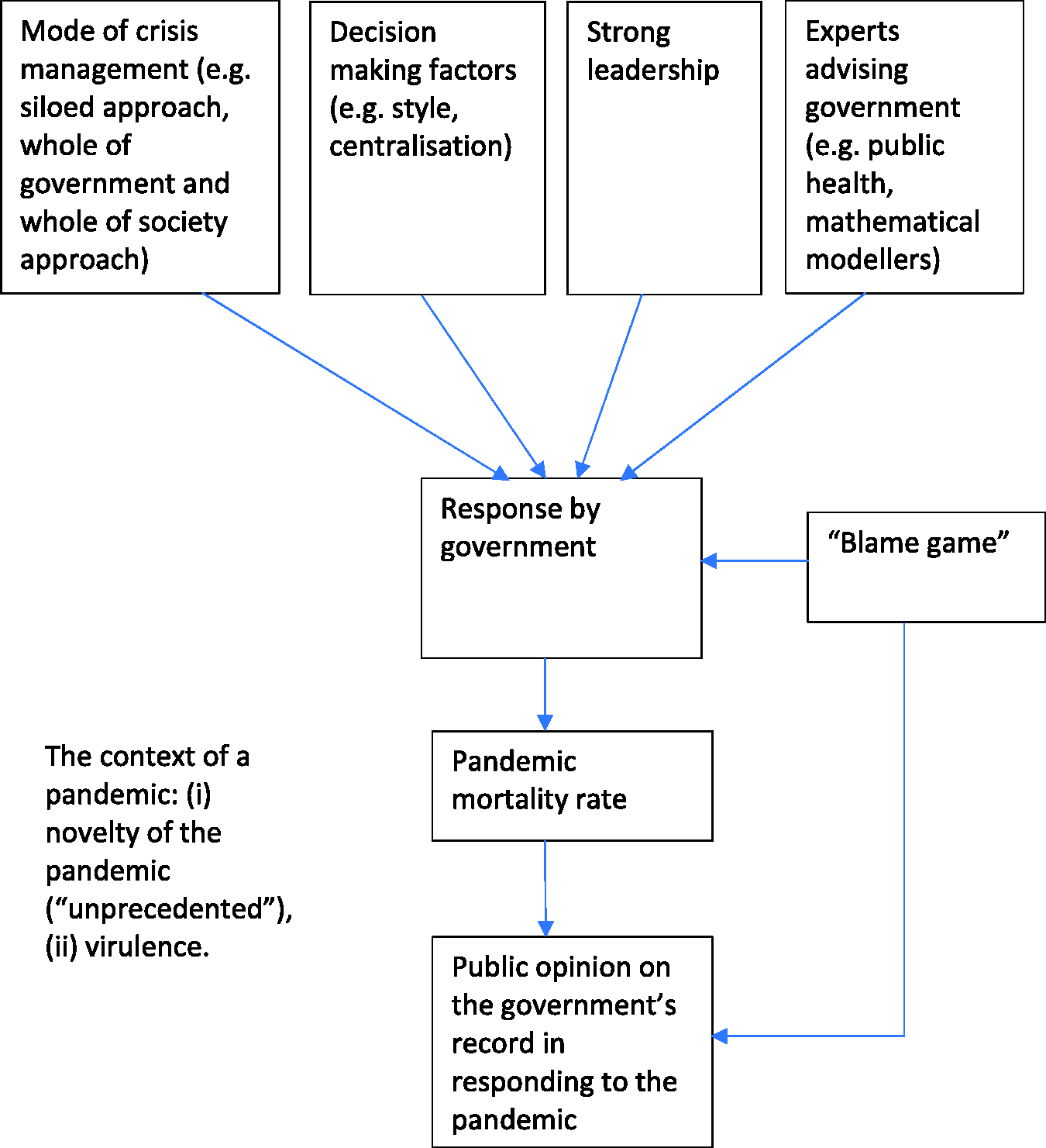
Conceptual framework for the governance of a pandemic.
Mortality rate and public opinion
On 11 April 2020, the UK had one of the worst cumulative COVID-19 mortality rates in the world. This was just one month after the Director-General of the World Health Organisation had stated that the spread of the virus warranted calling it a pandemic. Seven months later, the UK still had one of the worst cumulative COVID-19 mortality rates in the world, according to data published by Johns Hopkins University and Medicine, but it had succeeded in controlling its extent though a national lockdown beginning in late March. As Figure 2 shows, it was one of a number of countries that only managed to get the pandemic under control after many people had died. This contrasts with countries that had managed to contain the outbreak and then continued to contain it, with the result that the cumulative mortality rate in November remained relatively low. These included some European countries, notably, Finland and Norway. Such data suggested that the UK government’s response to the pandemic had been disappointing.
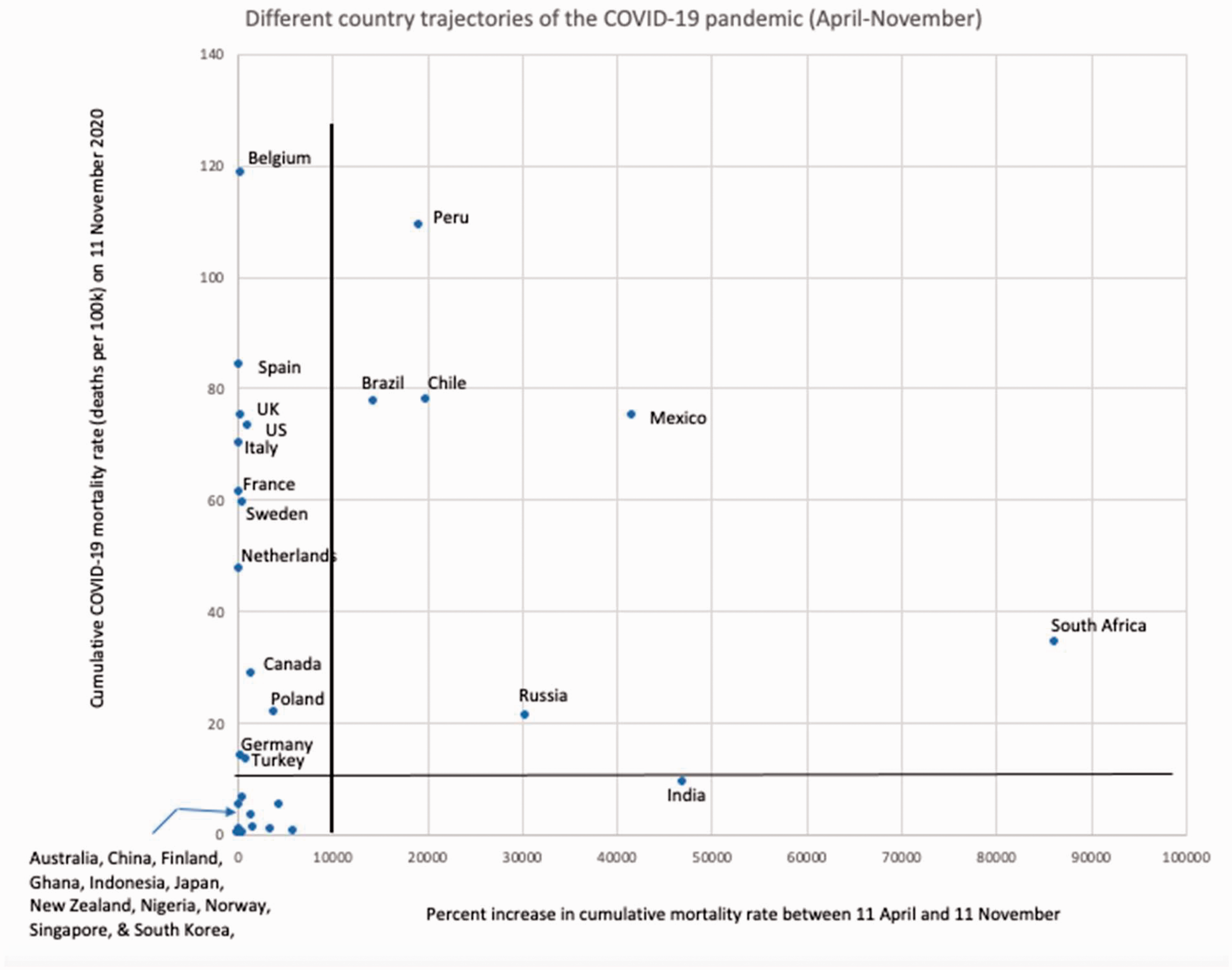
Different country trajectories of the COVID-19 pandemic (April–November).
The relatively high mortality rate of the UK was also apparent in European data on the relative cumulative age-standardised mortality rate, as shown in Table 1. These mortality rates are referred to as ‘excess deaths’ and were based on comparing 2020 data with a five-year average. As can be seen, at the beginning of June 2020, the UK and England had very high relative excess mortality rates as compared to the selected European countries shown.
Relative cumulative age-standardised mortality rate for selected European countries (from January 2020 to week starting 6 June 2020).
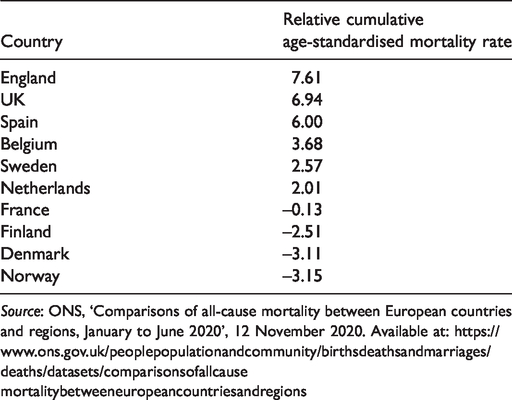
Source: ONS, ‘Comparisons of all-cause mortality between European countries and regions, January to June 2020’, 12 November 2020. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/comparisonsofallcausemortalitybetweeneuropeancountriesandregions
As noted earlier, the UK government brought in a national lockdown towards the end of March. In the middle of April, polling suggested that members of the UK public were feeling very nervous about the idea of leaving their homes if the lockdown ended (Ipsos-MORI, 2020). The public strongly supported the government lockdown rules and did not want the lockdown to be eased too quickly. Throughout May, as the UK government discussed and encouraged an easing of the national lockdown, public opinion became steadily more critical of its handling of the pandemic (YouGov, 2020a). Polls of public opinion in the middle of May found that half of those surveyed were opposed to the government’s decision to ease the lockdown, and at the beginning of June, a large majority of people surveyed thought the government had not been cautious enough in easing the lockdown (YouGov, 2020b, 2020c).
It seems likely that falls in public approval of the government’s handling of COVID-19 was a reaction to the rising cumulative COVID-19 mortality rate. However, it is possible that public opinion was also being influenced by how safe people were feeling as a result of the government’s decisions and announcements. In addition to this, members of the public were often very critical of an apparent breach of the lockdown rules by one of the Prime Minister’s political advisers. In late May, an opinion poll found that a large majority of people judged that the political adviser had broken the rules and over a half of those surveyed thought that he should resign as adviser to the Prime Minister (YouGov, 2020d, 2020e). He did not resign, and it appeared that he had been allowed to get away with breaking lockdown rules by the Prime Minister.
To put all this into some perspective, Table 2 shows the results of surveying public opinion in a number of countries between 28 May and 2 June. At the end of May, the UK had a relatively small proportion of its population that thought the government had handled COVID-19 well. It had this in common with most other countries in the table that had high COVID-19 mortality rates (e.g. a total of over 300 deaths per million population).
Government handling of COVID-19.
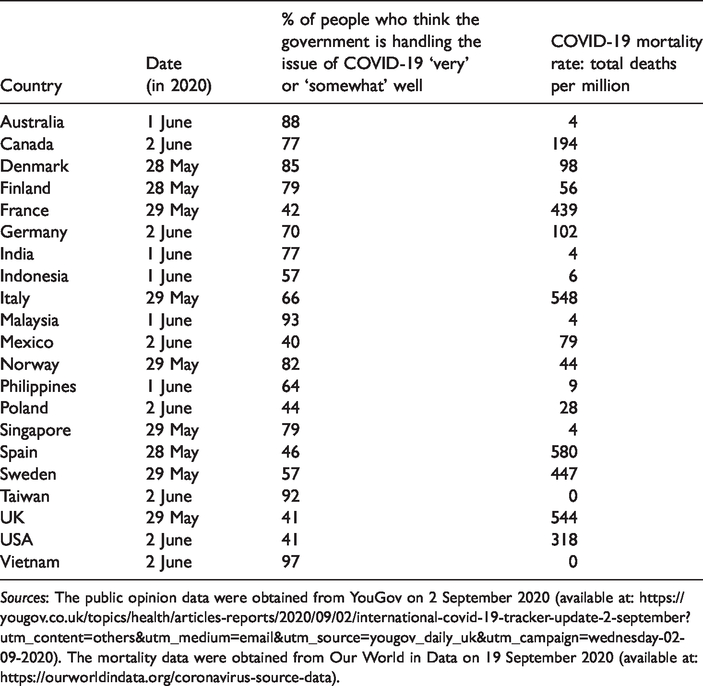
Sources: The public opinion data were obtained from YouGov on 2 September 2020 (available at: https://yougov.co.uk/topics/health/articles-reports/2020/09/02/international-covid-19-tracker-update-2-september?utm_content=others&utm_medium=email&utm_source=yougov_daily_uk&utm_campaign=wednesday-02-09-2020). The mortality data were obtained from Our World in Data on 19 September 2020 (available at: https://ourworldindata.org/coronavirus-source-data).
The initial response of the UK government
For the first phase of the UK government’s response to COVID-19, it looked as though it was following a siloed approach. The central government response to the emergency created by the spreading virus was formally coordinated through COBR (which stands for Cabinet Office Briefing Rooms), which was initially chaired by the Secretary of State for the Department of Health and Social Care. By the end of February, there had been five COBR meetings, all chaired by the Secretary of State for Health (Calvert et al., 2020).
In early February 2020, the UK government’s scientific experts said that little was known about the transmissibility of COVID-19 and advised the use of a reasonable worst-case scenario based on a flu pandemic. Despite all the uncertainty professed, the experts assumed that containment would give way to measures for delaying the virus and then case management (which meant people being treated who got ill). They assumed that contact tracing would not be useful after the containment stage (SAGE, 2020; Scientific Pandemic Influenza Group on Modelling, Operational sub-group [SPI-M-O], 2020). The initial strategic posture was not only a siloed approach, but also what may be called a ‘spectator strategy’. This strategy was in keeping with the pandemic preparedness strategy formulated by the government in 2011. Tending towards proportionality rather than the precautionary principle, the planning in the government strategy assumed that it did not make sense in terms of efficient use of resources to attempt containing the epidemic at ports of entry or halting the spread of the virus within the UK. On international travel, it stated: There are no plans to attempt to close borders in the event of an influenza pandemic.… Modelling suggests that imposing a 90% restriction on all air travel to the UK at the point a pandemic emerges would only delay the peak of a pandemic wave by one to two weeks.… there is no evidence of any public health benefit to be gained from meeting planes from affected countries or similar pro-active measures such as thermal scanning or other screening methods. Such measures are largely ineffective, impractical to implement and highly resource intensive. (Department of Health, 2011: 38)
A ‘Coronavirus: action plan’ published at the beginning of March by the Department of Health and Social Care, the Northern Ireland Department of Health, the Scottish Government and the Welsh Government (2020: 4) referred to the planning and preparation that had been done: The UK Government and the Devolved Administrations, including the health and social care systems, have planned extensively over the years for an event like this, and the UK is therefore well prepared to respond in a way that offers substantial protection to the public. keeping the country safe is the government’s overriding priority. And our plan means we’re committed to doing everything possible based on the advice of our world leading scientific experts to prepare for all eventualities. Let’s not forget – we already have a fantastic NHS, fantastic testing systems and fantastic surveillance of the spread of disease. (Johnson, 2020a)
One negative consequence of the government’s sudden alarm about hospital capacity was the move to create more capacity in hospitals by discharging elderly patients. Between 17 March and 15 April, some 25,000 people were discharged into care homes. The latter date was a critical one in policy terms: ‘Due to government policy at the time, not all patients were tested for COVID-19 before discharge.… On 15 April, the Department confirmed a new policy of testing all those being discharged from hospitals into care homes’ (NAO, 2020 : 11). This discharge policy was suspected by many of having caused a surge in the number of deaths in care homes.
The lack of testing of care home staff early on in the COVID-19 outbreak was also a source of worry in the social care sector. Many social care staff worked in more than one care home and it was thought that they might spread the virus between care homes. It struck some commentators that in its haste to protect the NHS, the government had given no thought to the risks for the social care sector. This did not look like a whole-of-government approach, even though social care and health services were all administered by the same government department.
The introduction of the national lockdown in March was an emergency measure to try to get control of the epidemic in the UK. If the lockdown was successful, what would the UK government do next? Would it go back to its previous approach, or try something new?
A new approach?
According to the minutes of a meeting of the government’s official expert committee on 18 February 2020, the capacity of Public Health England for test and trace was just five new cases a week (SAGE, 2020). Evidently, the UK government was not well placed to carry out surveillance. Even in early March, less than 2000 people were tested per day (NAO, 2020). When asked about any regrets he had, the Chief Medical Officer advising the Prime Minister said: If I had to choose one, it would be probably be looking at how we could speed up testing, very early on in the epidemic.… Many of the problems we had came because we were unable to work out exactly where we were, and we were trying to see our way through the fog. (Stewart and Sample, 2020) It first tested all those with symptoms and their contacts, then narrowed in on critically ill hospital patients and small numbers of symptomatic residents in care homes, and then extended eligibility in stages to include NHS, social care and other key workers and their households, and care home residents more widely, as testing capacity increased. (NAO, 2020: 16)
The government decided to mobilise the private sector to create, from scratch, a centralised test and trace system. Testing continued to expand month by month but tracing of contacts of those confirmed as infected with COVID-19 continued to disappoint. This failure of execution, along with problems of logistics and the supply of personal protective equipment, damaged the UK government’s reputation for competence.
This could have been a story of strategic agility when the initial strategic posture proved mistaken. What happened instead can be described as ‘muddling through’, though not the better kind of muddling through that leads to ‘satisficing’ (Lindblom, 1959), but the worst kind. This is the chaotic ‘muddling through’ that occurs in time-pressured reactive problem solving and leads to new problems, sometimes through poor execution of proposed solutions. Having begun the year by underestimating the gravity of the threat of the pandemic, the problem of the risk of the hospitals being overrun was solved by a national lockdown and discharging elderly patients into care homes without testing for COVID-19 (and possibly boosting the spread of infection and death in the care homes). The lockdown caused another problem to arise as the economy suffered collateral damage. The government responded to this by trying to ease the national lockdown while developing a centralised system of test and trace (which, as noted, proved a struggle to execute successfully). When another problem arose, which was the resurgence of infection in local areas and regions of the country, the government then came up with a solution of ordering local and regional lockdowns, which then proved insufficient. The Prime Minister reluctantly, and some said too slowly, resorted to a second national lockdown, which started in November 2020. In summary, the ‘muddling through’ consisted of the government meeting each problem only as it arose, including the problems created by preceding solutions and poor execution of intended solutions.
Command-and-control decision-making
The UK government used a command-and-control style of governing during the pandemic. This style did not go down well with all the elected Members of Parliament (MPs) in Westminster. There were complaints that government decisions were not being properly scrutinised and opportunities to take MPs with the government were being missed.
During the first half of 2020, there were many complaints by the elected mayors of major cities and conurbations, such as London and Greater Manchester, and by local government leaders about the UK government decision-making approach. The Mayor of Greater Manchester complained about the UK government’s easing of the first lockdown: In Greater Manchester, we had no real notice of the measures. On the eve of a new working week, the PM was on TV ‘actively encouraging’ a return to work. Even though that would clearly put more cars on roads and people on trams, no one in government thought it important to tell the cities that would have to cope with that. (Burnham, 2020)
There were examples of the government acting speedily: the creation of the extra hospital capacity in the form of Nightingale Hospitals is one example. However, there were constant criticisms of the UK government’s slow response. Some of this came from its own experts. One, who sat on the top expert committee (the Scientific Advisory Group for Emergencies (SAGE)) and chaired the New and Emerging Respiratory Virus Threats Advisory Group, said ministers were too slow in starting the lockdown in March (Allegretti, 2020). Another, who had resigned because he had broken a lockdown rule, told the House of Commons Science Committee that entering the lockdown earlier was warranted and that if it had been done a week earlier, it would have meant many fewer deaths (Stewart and Sample, 2020).
High degree of centralisation
The UK government favoured a high degree of centralisation in its governance of the pandemic. This can be seen in a number of the choices it made, including how it worked with the devolved government administrations of Northern Ireland, Scotland and Wales. A retired senior civil servant, who had recently been responsible for constitutional issues and devolution matters, suggested that although leaders of devolved administrations were invited to COBR’s early meetings on the pandemic, more could have been done to make their participation effective. He went on to label what was happening as ‘centralisation’: The whole COVID episode has been marked by centralisation; distrust of the devolved administrations; not involving the metropolitan mayors.… In all of the big systems – test and trace, PPE [personal protective equipment] procurements and so on – the attempt has been made to manage that, as far as possible, from central entities rather than devolving those decisions. (Ross, 2020)
The experts
The editor-in-chief of the Lancet medical journal suggested to the UK Parliament’s Science and Technology Committee that public health experts and doctors had less influence than mathematical modellers and behavioural scientists (Boseley, 2020). This may have been part of the reason why aggressive containment was not a serious option in the early months of 2020 and may have been linked in some way to the lack of test, trace and isolate capacity to carry out aggressive containment.
The dominance of experts in mathematical modelling and behavioural science presumably dovetailed very neatly into a government with a command-and-control and technocratic style. The technocratic character of the UK government might have strengthened in recent times; an Organisation for Economic Co-operation and Development report in 2020 commented on the way the UK’s open data policy had diminished in importance and analytical capacity had become more of a priority within the public sector (OECD, 2020).
Strong leadership
The Prime Minister was charged at various times of being guilty of over-promising and under-delivering. He was also accused of personal incompetence and indecision: ‘Time and again, I have heard accounts from inside government of warnings given and action exhorted only for the machinery never to properly click into gear for want of decisive leadership’ (Rawnsley, 2020).
Muddle and lack of clarity may have arisen because the Prime Minister did not want to use government power to restrict people’s freedom. He stressed the presence of the public’s libertarian beliefs as he exhorted British people to reduce social contacts and stay at home. In September 2020, in response to a question in Parliament, the Prime Minister described Britain as a freedom-loving country and he appeared to see the British nation as being different to many other countries in this respect (Johnson, 2020b). In fact, a lot of the opinion polling evidence published suggested that the British people were mostly very compliant in obeying the national lockdown rules and thought that the government had eased the first lockdown too quickly.
It was not entirely clear what priorities were being pursued by the Prime Minister in managing the crisis. This was so both when going into the national lockdown in March, and then when starting to exit the lockdown in May. On the verge of the move into the first national lockdown, some much-publicised statements were made by officials on the desirability of exiting by means of ‘herd immunity’. In a British Broadcasting Corporation (BBC) interview on 13 March, the Chief Scientific Adviser to the UK government said that the official aim was to control the pace of the spread of infection, to reduce the peak of infection without fully suppressing it and, as a result, to develop ‘herd immunity’ and bring a halt to COVID-19. Perhaps it was thought at that time that pursuing population immunity could be achieved without a lockdown and the economy could have been allowed to continue functioning more or less normally. The Prime Minister’s moves to ease the lockdown in May were also difficult to comprehend if the sole priority was to save lives. If, however, the Prime Minister was trying to balance two priorities of saving lives and restoring the economy, then it did make some sense.
Both much expert opinion and the public considered that the Prime Minister had rushed the easing of lockdown and that if it had been continued a little longer, then the virus would have been better suppressed. Professor Robert West, a member of the Scientific Pandemic Influenza Group on Behaviours, which reported into the government’s SAGE committee, was quoted as saying: The way that we’re moving to easing of this dreadful lockdown … at a time when we have still something like 8,000 infections a day, and we’re still looking at something in the region of probably 400 deaths a day, and before we have the track, trace and isolate system properly running. Put all this together and you have a huge risk, and it’s not just me saying that. (The Guardian, 2020)
Conclusions
In summing up the UK experience of the governance of COVID-19, there are a number of points that can be made to explain why the UK government did not contain the virus and prevent it spreading, but then did manage to bring the epidemic back under control once the national lockdown was implemented. The relatively high mortality rate can be seen as resulting from wrong or slow government judgements and decision-making. The risk assessments made as far back as 2011 (but continuing into early 2020) underestimated the risks that might be posed by a pandemic and led to wrong decisions on actions to contain the transmission of the virus both at ports of entry and within the UK. Ministers were too slow in starting the national lockdown in March and would have saved many lives if they had started it sooner. The decision to create more hospital capacity by discharging elderly people into care homes without testing for COVID-19 (up until 15 April) was a major mistake. Past government decisions which meant that there was a lack of capacity for testing and tracing by Public Health England during February and March was a big mistake and impeded the operation of surveillance under a siloed approach to managing the crisis. Preparations for the supply of personal protective equipment were also poor and led to shortages in hospitals and social care settings, and presumably made mortality rates among health and social care staff higher than they would have otherwise been. It seems that four or five wrong or slow major decisions can cause calamitous and maybe even disastrous results in a pandemic.
In relation to the mode of crisis management, it can be concluded that in the period of late March and April, the UK transitioned from a predominantly siloed approach to a whole-of-society approach. The UK government sought public support for a national lockdown, and this was very successful because of the high levels of public willingness to put saving lives first by having a lockdown. Also a whole-of-society move, though poorly executed, the Government turned to private sector businesses to deliver a new centralised test and trace system. The execution of a whole-of-society approach (i.e. the centralised test and trace system) and problems with whole-of-government coordination and cooperation meant that, from the middle of March, the UK governance of the pandemic is better described as chaotic ‘muddling through’ rather than strategic agility.
The whole-of-government approach was problematic before and after the transition in mode of crisis management. Public services systems were not a coordinated totality (e.g. health and social care). The UK government’s command-and-control style of decision-making and its centralisation created much-publicised problems of multi-level governance, inhibiting a spirit of cooperation and practical coordination with devolved administrations, regions and localities.
If we put all this together, it can be concluded that mistakes made under a siloed approach, on the one hand, and the support of the public that made the national lockdown a success (a whole-of-society approach), on the other, explain why the UK ended up with a relatively high mortality rate but the government was able to bring the epidemic back under control. However, the government’s ability to keep the virus suppressed after May was compromised by the failure to successfully execute the introduction of a centralised test and trace system (a whole-of-society response measure) and multi-level governance issues (whole-of-government approach). The government then turned to regional and local lockdowns as a way of subduing the epidemic.
The UK experience also yields some important insights about the public perspective in the blame game that accompanies a pandemic. These can be summed up as follows: the UK public lost faith in the government’s handling of COVID-19 for, it seems, two main reasons: (1) the relatively high mortality rate; and (2) the government’s willingness to take public health risks (such as starting the easing of the national lockdown too quickly in May). Government decisions have to be seen as putting saving lives first; the government also has to manage the crisis to avoid relatively high mortality rates.
What are the lessons of the UK experience for future crisis management? First, preparedness for a pandemic is hugely sensitive to the risk assessments that inform planning assumptions – risk assessments that may have been made many years before the crisis strikes. Second, overdoing ‘proportionality’ and ‘efficiency’ in planning preparedness jeopardises a government’s strategic agility in a pandemic. Third, when a government is focused on compromising between attempts to save lives and efforts to protect the economy, it risks producing a lose–lose situation in which a country suffers both a relatively high mortality rate and large reductions in real GDP. Fourth, getting an out-of-control pandemic back under control may require public support for lockdown restrictions, and this may be forthcoming even when governments are not that effective in carrying out other measures to defeat the pandemic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.