
Abstract
Background:
Schizophrenia is one of the most stigmatized mental disorder; yet, research on how it is perceived within the field of general nursing is limited. Since nurses play a crucial role in the care of individuals with schizophrenia, their attitudes toward this disorder can significantly impact treatment and well-being of those affected.
Aim:
The present study examines the degree of schizophrenia-related stigmatization among nurses (n = 153) compared to individuals from the broader population (n = 314), across the three key elements of stigma: stereotypes, emotional responses, and the behavioral aspects such as cooperation and interaction intentions.
Method:
Data were collected using an online questionnaire.
Results:
Group differences were observed. Nursing professionals showed higher stigma toward perceived individuals living with schizophrenia than did members of the broader community. Specifically, nurses perceived them to be less competent and warmer but not more dangerous (stereotypes), felt less admiration, empathy, and warmer attitudes, and more anxiety toward them (negative affective responses), and reported lower intentions to engage in prosocial behavior and interact (hostile behavioral intentions). The results held the same when controlling for basic socio-demographic variables.
Conclusions:
These findings highlight critical stigma-related differences between general nurses and the broader community, providing a novel comprehensive comparative examination across cognitive, emotional, and behavioral domains. This approach highlights key targets, such as emotional responses and prosocial intentions, that should be prioritized in future anti-stigma interventions within nursing.
Introduction
Scholarly investigations consistently highlight schizophrenia as a mental disorder associated with the highest levels of prejudice and discrimination (e.g., Arbanas et al., 2018; Mothersill et al., 2023). This stigmatization leads to a decline in the quality of life for those affected by schizophrenia and significantly influences their mental health outcomes. The stigma has also a detrimental impact at the structural level, exacerbating socio-economic inequality between those living with schizophrenia compared to other members of the community (Saraceno et al., 2005). According to the social causation hypothesis (Kohn, 1972), this is partly due to the life conditions associated with lower socioeconomic status, such as discrimination (Sharpley et al., 2001). In the healthcare domain, research indicates that perceived stigmatizing attitudes among individuals living with schizophrenia result in various adverse outcomes, including treatment discontinuation (Kamaradova et al., 2016), as well as increased likelihood of relapses (Rayan & Aldaieflih, 2019) and hospitalization rates (Ayano & Duko, 2017). Hence, there is a pressing need to assess the stigmatization encountered by individuals affected by schizophrenia in general healthcare. This evaluation could point the need for the development of future anti-stigma intervention strategies and highlight stigmatization areas where training might be necessary. Moreover, comparing the stigmatizing attitudes of general nurses with those of the broader community provides a valuable reference point for understanding whether health professionals hold more, less, or different types of stigma. This comparison allows us to contextualize nurses’ stigma not only within the healthcare setting but also in relation to societal norms. Healthcare providers play a crucial role in the management of schizophrenia; their attitudes toward patients can directly influence treatment engagement and well-being of those living with schizophrenia.
In the nursing field, the stigma research has been conducted largely among mental health nurses (Kolb et al., 2023), and the specific focus on schizophrenia stigma in general nursing is still lacking (Ihalainen-Tamlander et al., 2016). The present investigation aims at filling in this gap by providing an evaluation of stigma toward schizophrenia among general medicine nurses as compared to a community sample, thus addressing both the implications for mental health care and the broader social context of stigma. Moreover, the comprehensive examination considering the three dimensions of stigmatization, including its cognitive, affective, and behavioral components (Corrigan & Penn, 1999), in health setting has been under-researched (Birtel & Oldfield, 2022). This investigation specifically targets general nurses and assesses stigma across its three core dimensions. By addressing these dimensions, the study seeks to inform strategies for anti-stigma interventions and training programs, which are essential for all health and social care professions involved in the holistic care and support of individuals living with schizophrenia.
In unfolding the three basic dimensions of mental illness-related stigma (Corrigan & Penn, 1999), the cognitive dimension involves negative stereotypes, such as beliefs about people with mental illnesses (e.g., perceiving them as unpredictable, dangerous, or incompetent). Research shows that members of the wider society perceive individuals with schizophrenia as lacking warmth, and as being dangerous and unpredictable (e.g., Broussard et al., 2012; Smith et al., 2017). In the context of healthcare, Kolb et al. (2023) observed that general nurses demonstrated a lower level of accuracy in their knowledge about mental disorders compared to mental health nurses. Yet, the examination of the cognitive component of stigma among nurses in comparison to the broader population is scarce. As suggested by previous research findings (e.g., Mothersill et al., 2023), there may be substantial variations in attributing negative aspects to different mental illnesses.
As for the affective aspect of stigma—that is, emotional responses toward individuals living with schizophrenia—schizophrenia frequently evokes negative reactions from the broader community (i.e., commonly referred as general community population), including feelings of contempt (Cheung et al., 2018; Görzig & Ryan, 2022) and fear, alongside more prosocial emotions, like compassion (Thonon & Larøi, 2017). In the nursing context, general practice nurses tend to exhibit higher levels of anxiety, lower levels of empathy, and more negative attitudes toward individuals living with any kind of mental disorders compared to the wider society (Birtel & Oldfield, 2022). However, we have not found any research that specifically addresses the affective stigmatization of schizophrenia, in particular among general nurses. This focused examination is needed due to higher stigmatization of this population (e.g., Mothersill et al., 2023), and the possibly specific actions to be undertaken to reverse the situation.
Lastly, the behavioral dimension of stigma, according to Corrigan and Penn (1999), refers to discriminatory actions directed at people with mental illness. This dimension is expressed through concrete behaviors such as avoiding contact, maintaining social distance, or excluding individuals from social, occupational, or educational opportunities. Discriminatory behaviors in the broader society toward persons living with schizophrenia manifest in difficulties in forming friendships or intimate relationships with such individuals (Thornicroft et al., 2009), general patterns of social distancing (Martensen et al., 2020), or rejection to have them as neighbors, employees, or consider marriage with them as more specific behaviors (Hori et al., 2011). Studies specifically conducted with general healthcare nurses show that they exhibit lower intentions to establish future interactions with individuals affected by mental disorders compared to the broader society (Birtel & Oldfield, 2022), and a desire for more social distance than mental health nursing personnel (Kolb et al., 2023). Nevertheless, research has not addressed general nurses’ behavioral dimension of stigma toward individuals living with schizophrenia.
While stigma toward individuals living with schizophrenia is extensively studied among the broader society (e.g., Angermeyer et al., 2021), research focusing on nurses remains limited. Given that unintended stigma by nurses may deter individuals living with schizophrenia from seeking help, it is crucial to examine stigma levels among nurses (using the broader community as a reference). This study aims to compare stigma toward individuals living with schizophrenia in nursing personnel and a broader community sample across cognitive (competence, warmth, dangerousness), affective (admiration, compassion, empathetic concern, anxiety, attitudes), and behavioral dimensions (intention for social acceptance and cooperation).
This study is intended to make two relevant contributions to the literature on mental health stigma. First, it provides a comparison of how general nurses and members of the broader community perceive individuals living with schizophrenia, using a comprehensive framework that includes cognitive, affective, and behavioral dimensions. Specifically, it is among the first studies to examine: stereotypes related to competence, warmth, and dangerousness (cognitive domain); emotional responses such as admiration, compassion, anxiety, empathy, and attitudes (affective domain); intergroup cooperation intentions and social acceptance across three relational spheres—public, private, and intimate (behavioral domain). Second, the findings would allow pointing out to specific areas (e.g., emotional responses and prosocial intentions) that could be addressed in targeted anti-stigma interventions for healthcare professionals.
Methods
Participants and Procedure
After the study was approved by the Research Ethics Committee of authors’ university, the survey was distributed in two steps. First, the survey was distributed among community members through social networks and announcements using the “snowball” sampling technique; as a result, 314 responses were collected (Mage = 38.72, SDage = 13.316; 77.7% women, 74.8% had higher education). Second, the survey was also disseminated among nurses with the collaboration of the Regional Nursing Association and the Province Hospital, which led to 153 responses (Mage = 38.94 years, SDage = 10.738; 91.5% women, 100 % had higher education). In both subsamples, a similar high percentage acknowledged having acquaintances living with schizophrenia (80.9% in the community sample, 79.1% in the nurses’ sample).
Instruments
To assess different dimensions of stigma toward people living with schizophrenia, we used a multi-component approach reflecting three major domains of stigmatizing responses: cognitive, affective, and behavioral. This categorization is consistent with the widely accepted tripartite model of stigma (Corrigan & Penn, 1999). The cognitive component refers to stereotypes (e.g., perceptions of warmth, competence, and dangerousness), while the affective component includes emotional reactions (e.g., admiration, compassion, anxiety, empathy, and attitudes). Finally, the behavioral component reflects intentions to interact with or cooperate with people living with schizophrenia, operationalized as social acceptance intentions and intergroup cooperation intentions.
Cognitive Responses
We covered cognitive evaluations of people living with schizophrenia on three dimensions: warmth, competence, and dangerousness. Items were rated on a Likert scale, with responses ranging from 1 (Not at all) to 7 (Very much).
Perceived Warmth and Competence (adapted from Leach et al., 2007)
Four items measured the perceived warmth in people suffering from schizophrenia (“warm,” “friendly,” “trustworthy,” and “nice”). Cronbach’s alpha was satisfactory (community sample: .87; nurses: .91). Three items were employed to measure perceived competence (“competent,” “intelligent,” and “skilled”), showing good Cronbach’s alpha values (community sample: .81; nurses: .71).
Perceived Dangerousness
Six items were used to measure the perceived dangerousness. The participants were asked what percentage of people suffering from schizophrenia encompasses some attributes (i.e., “criminals,” “drug addicts,” “aggressive,” “threatening,” “unpredictable,” “dangerous”). Cronbach alpha values were good (community sample: .91; nurses: .91). The participants responded on a scale ranging from 10% to 100%, with 10 intervals to choose from (10%, 20%, 30%, 40%, 50%, 60%, 70%, 80%, 90%, and 100%).
Affective Responses
Different types of affective responses were collected. Participants answered about their feelings toward people suffering from schizophrenia on a Likert-7 scale (where 1 = Not at all and 7 = Very much).
Admiration and Compassion
A six-item scale was used, which was divided into the following three dimensions (Cuddy et al., 2007). Higher scores on each subscale indicate greater levels of admiration or compassion.
Admiration (three items: “admiration,” “sympathy,” and “respect”; Cronbach’s alpha for the community sample: .72, alpha for nurses: .68).
Compassion (one item: “compassion”)
Empathic Concern
The scale included four items (e.g., “understanding,” “kind,” “compassionate,” and “excited”); participants responded how they felt when thinking about person suffering from schizophrenia (Batson et al., 2007). Cronbach alpha values were good (community sample: .83; nurses: .86). Higher scores indicate greater empathic concern.
Attitudes Toward People living with Schizophrenia
This scale is composed of one item that assesses warm attitudes toward people living with schizophrenia (Lavrakas, 2008). It was formulated as follows: “My general feelings toward people suffering from schizophrenia can be described as. . .,” where 0° = very cold and 100° = very warm. Participants could choose from 11 ranges of 10ºC (0°, 10°, 20°, 30°, 40°, 50°, 60°, 70°, 80°, 90°, and 100°). Higher scores on this item indicate warmer attitudes toward people living with schizophrenia.
Behavioral Intentions
Behavioral intentions toward people living with schizophrenia were measured. All items were rated on a Likert scale from 1 = Not at all willing to 7 = Completely willing.
Acceptance in the Private life Domain (at home; two items: “invite him/her to my home,” “visit his/her home”; Cronbach’s alpha for the broader community sample: .91; alpha for nurses: .92).
Acceptance in the Public life Domain (three items: “to have lunch or dinner with him/her in a restaurant,” “to belong to the same institution s/he belongs to,” and “to talk to him/her about how to solve problems between groups”; Cronbach’s alpha for the broader community sample: .88; alpha for nurses: .88).
Intention to Involve in or Approve Romantic Relationships (two items: “to go out with him/her,” and “to approve that a son/daughter of mine would marry him/her”; Cronbach’s alpha for the broader community sample: .87; alpha for nurses: .85).
Sociodemographic Variables
Participants answered questions about their gender, age, educational level, and political orientation (1 = extreme left-wing, 7 = extreme right-wing). Additionally, they provided information regarding whether they knew any person experiencing a mental illness (dichotomous), kinship with that person, and whether they lived with that person (dichotomous).
Analytical Strategy
Statistical analyses using SPSS 28.0 were conducted in four steps. First, percentages for sociodemographic variables were computed. Second, assumptions of normality and heterogeneity were tested. Third, based on these unmet assumptions, non-parametric tests were used to examine mean differences between the two subsamples. The analyses included cognitive responses (competence, warmth, and dangerousness), affective responses (admiration, compassion, empathy, anxiety, and positive/warm feelings), and behavioral intentions (social interaction and prosocial intentions). Effect sizes of the mean differences and Cronbach’s alpha values for the scales were also provided. Forth, additional non-parametric tests controlling for gender, age, educational level, and political orientation were conducted. These covariates were included because previous research has linked them to differences in stigma: women tend to show more benevolent attitudes (Ruiz et al., 2022), some studies report that younger individuals express higher stigma (e.g., Kolb et al., 2023), higher education relates to lower stigma (Brewer et al., 2025), and authoritarian and conservative tendencies correlate with more negative attitudes toward individuals with mental illness (Gonzales, 2022; Szabó et al., 2024).
Results
The means and the values of the statistics for the comparison of the groups in the three stigma elements—that is, cognitive responses, affective responses, and behavioral intentions—are shown in Table 1. General medicine nurses exhibited higher levels of stigma toward people living schizophrenia than participants from the broader community in several aspects, although the effect sizes were not high (ηp² = ranging between .000 and .043). Specifically, compared to participants from the broader community, nurses perceived people living with schizophrenia as less friendly (Mnurses = 3.41, SEnurses = 0.09, Mcommunity = 3.83, SEcommunity = 0.06; ηp² = .030, p < .001) and competent (Mnurses = 4.10, SEnurses = 0.09, Mcommunity = 4.45, SEcommunity = 0.06; ηp² = .025, p < .001), but there were no differences regarding the perception of these individuals as dangerous (ηp² = .001, p = .529).
Mean Comparison in Stigmatization Elements between Broader Community Sample and Nurses.
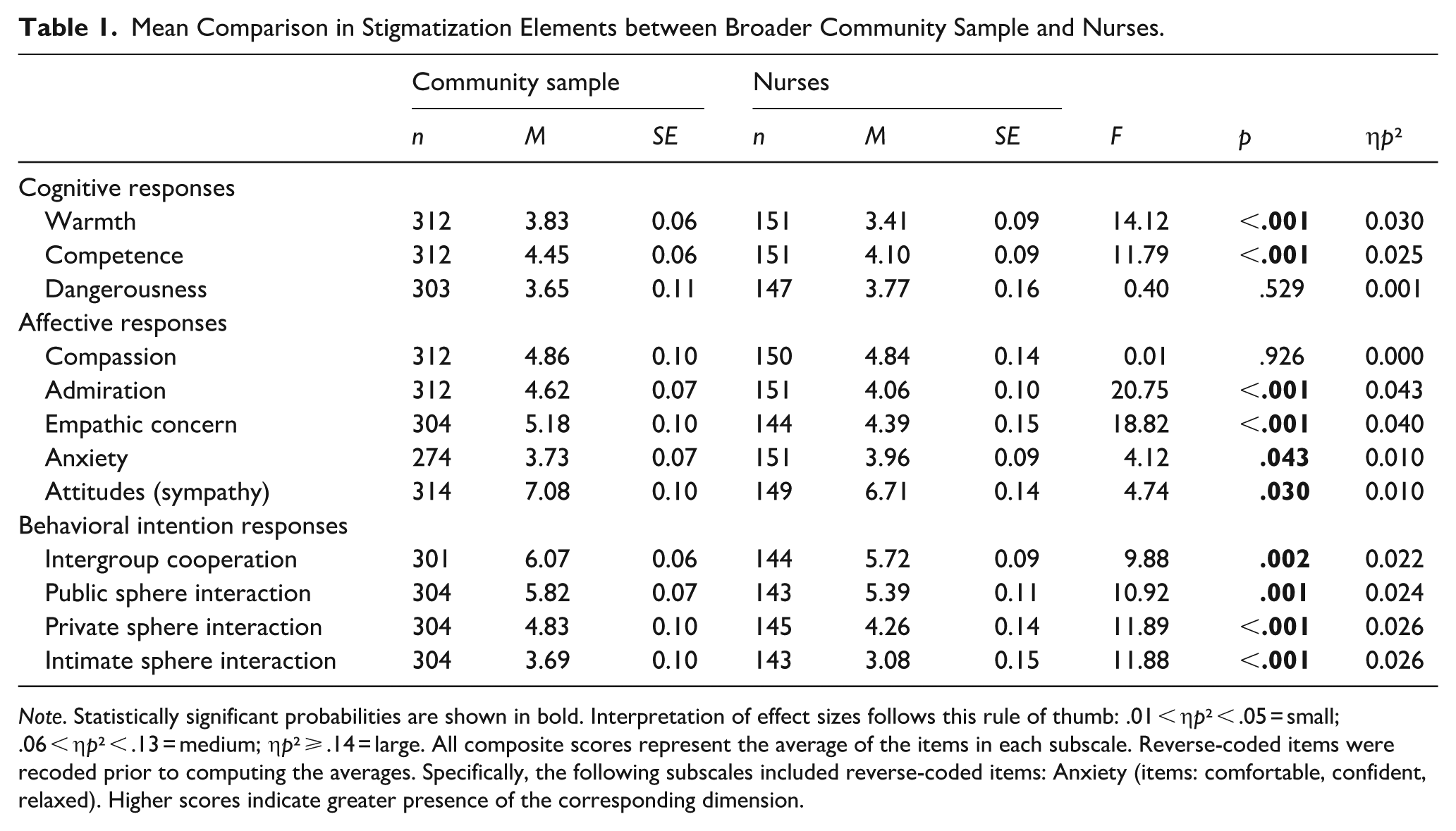
Note. Statistically significant probabilities are shown in bold. Interpretation of effect sizes follows this rule of thumb: .01 < ηp² < .05 = small; .06 < ηp² < .13 = medium; ηp² ⩾ .14 = large. All composite scores represent the average of the items in each subscale. Reverse-coded items were recoded prior to computing the averages. Specifically, the following subscales included reverse-coded items: Anxiety (items: comfortable, confident, relaxed). Higher scores indicate greater presence of the corresponding dimension.
In the affective dimension, statistically significant differences were found in the emotions of admiration (Mnurses = 4.06, SEnurses = 0.10, Mcommunity = 4.62, SEcommunity = 0.07; ηp² = .043, p < .001), empathy (Mnurses = 4.39, SEnurses = 0.15, Mcommunity = 5.18, SEcommunity = 0.10; ηp² = .040, p < .001), anxiety (Mnurses = 3.96, SEnurses = 0.09, Mcommunity = 3.73, SEcommunity = 0.07; ηp² = .010, p = .043), and general attitudes (Mnurses = 6.71, SEnurses = 0.14, Mcommunity = 7.08, SEcommunity = 0.10; ηp² = .010, p = .030) toward people experiencing schizophrenia; the effect sizes were not high, though (ηp² = ranging between .000 and .043). General medicine nurses sample felt less admiration, empathy, and warmer attitudes (or liking), and more anxiety toward people living with schizophrenia than participants of the broader community.
Finally, general medicine nurses showed more stigmatizing behaviors, as evidenced by lower intentions to engage in prosocial behavior (Mnurses = 5.72, SEnurses = 0.09, Mcommunity = 6.07, SEcommunity = 0.06; ηp² = .022, p = .002) and interact (e.g. Private sphere interaction: Mnurses = 4.26, SEnurses = 0.14, Mcommunity = 4.83, SEcommunity = 0.10; ηp² = .026, p < .001) with people living with schizophrenia, compared to participants of the broader community.
To further examine the robustness of these findings, an additional analysis was conducted controlling for gender, age, educational level, and political orientation. The results remained unchanged; they were consistently in the same direction and showed differences of the same small size, with general medicine nurses exhibiting higher levels of stigma compared to the broader community sample (see Table 2). Nevertheless, to address this concern and provide further transparency, we have included non-parametric tests in the supplementary material. The results of these analyses are consistent with the main findings, thereby reinforcing the robustness of our conclusions.
Mean Comparison in Stigmatization Elements Between Community Sample and Nurses, After Controlling for Gender, Educational Level, Age and Political Scale.
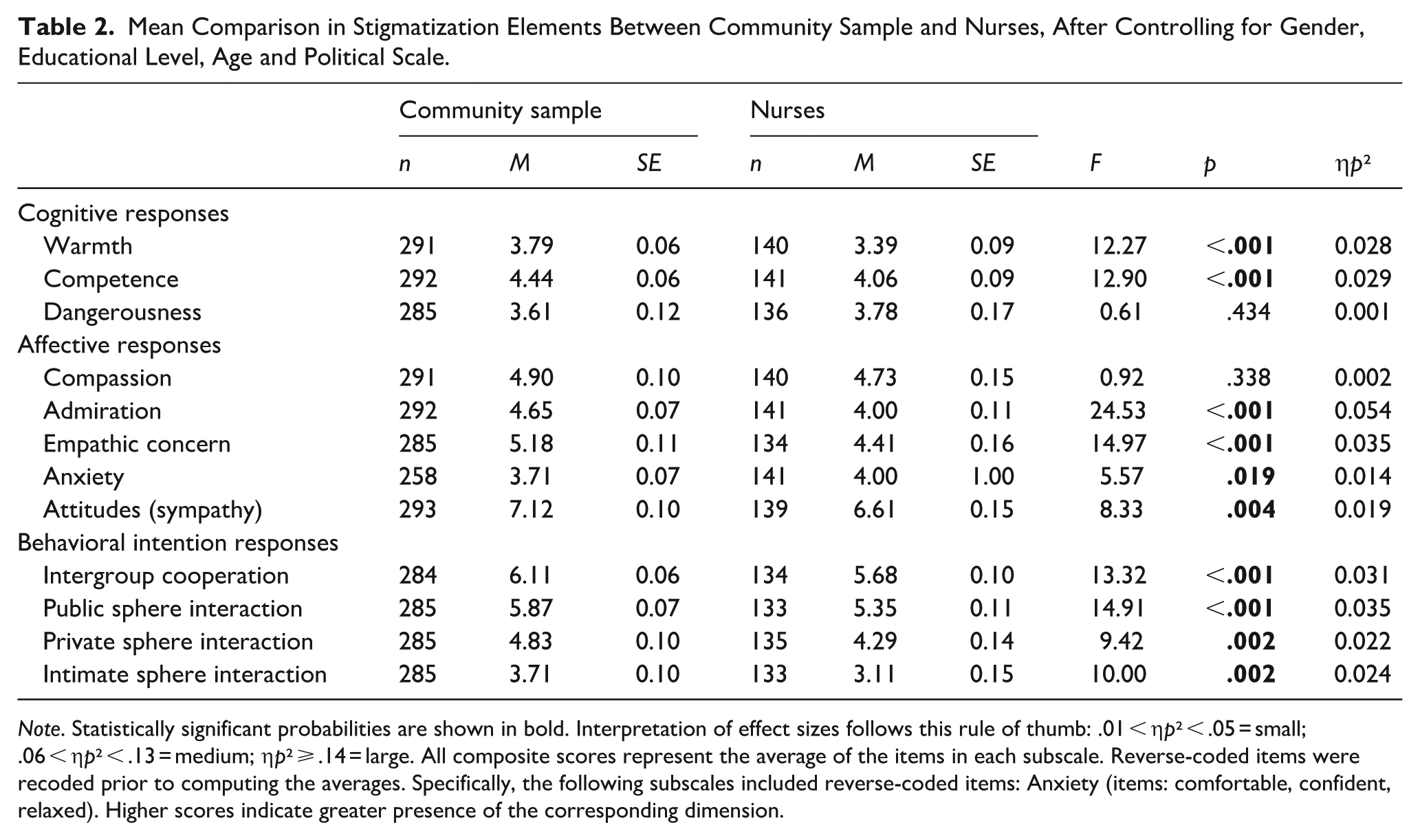
Note. Statistically significant probabilities are shown in bold. Interpretation of effect sizes follows this rule of thumb: .01 < ηp² < .05 = small; .06 < ηp² < .13 = medium; ηp² ⩾ .14 = large. All composite scores represent the average of the items in each subscale. Reverse-coded items were recoded prior to computing the averages. Specifically, the following subscales included reverse-coded items: Anxiety (items: comfortable, confident, relaxed). Higher scores indicate greater presence of the corresponding dimension.
Discussion
The present study makes a remarkable contribution to the scientific and applied nursing literature by examining the stigma associated with schizophrenia among general healthcare nurses, compared to members of the broader community and considering its cognitive, affective, and behavioral aspects. In comparison to the broader community, nurses exhibited more stigmatizing responses toward individuals living with schizophrenia in all three elements of stigma, but no differences across samples were observed regarding perceived dangerousness. Moreover, to verify the robustness of our findings, an additional analysis taking into account some sociodemographic covariates that have been observed in other studies yielded a pattern consistent with the main analysis. Gender, education level, or right-wing political orientation, which can affect how individuals perceive and react to certain groups, do not seem to account for the results. It could be argued that the healthcare environment is not immune to the stigmatization toward persons experiencing schizophrenia, being revealed among nurses possibly to a slightly greater extent.
First, there is a perception of lower warmth and competence attributed to individuals affected by schizophrenia by nurses in comparison to the rest of the community. Yet, although the difference was statistically significant, the effect size was small, suggesting only a modest difference in perceived warmth and competence between groups. Our findings are in line with Kolb et al.’s (2023). They observed that nurses in medical and surgical fields stigmatized those living with mental illnesses to a greater extent than mental health specialized nurses. This may be reflecting a cognitive (knowledge) bias in this type of nurses derived from a lower familiarity with mental health conditions compared to physical pathologies. Our study goes beyond these authors’ findings by showing that this cognitive stigma pattern also appears in general nursing, and by focusing specifically on schizophrenia—it adds a more focused layer in the analysis of stigma in relation to categories of mental illness.
Interestingly, there appears to be no statistically significant differences in the perceived dangerousness of individuals with schizophrenia between nurses and the broader community, with mean scores around the middle of the scale, suggesting a shared societal view rather than an absence of stigma. This widespread social perception might stem from distorted portrayals in the media or film industry (Perciful & Meyer, 2017). It may be worth interpreting these results in light of data regarding affective responses. In fact, despite similar perceptions of dangerousness, general nurses reported experiencing slightly greater anxiety around individuals with schizophrenia than the broader community members, echoing results related to stigma toward mental health problems (Birtel & Oldfield, 2022). The significant difference in anxiety levels was also of small effect size, suggesting a subtle distinction between groups. A tentative explanation for these results is that this anxiety among general nurses could be not due to fear of danger, but rather could also reflect uncertainty about their own preparedness or perceived ability to provide specialized care. Our study adds to this literature by pointing out that, even when perceived dangerousness is similar, nurses may experience greater anxiety, potentially reflecting concerns about their preparedness or confidence in providing care, highlighting a cognitive-affective nuance not previously detailed in general nursing populations.
Another finding that may deserve further commentary is that nurses empathize less with individuals living with schizophrenia compared to the broader community, consistent with Birtel and Oldfield’s (2022) findings. Our observed difference in empathic concern, although statistically significant, also showed a small effect size, indicating limited practical impact. On this matter, research has shown that not emotionally engaging (i.e., empathizing less) with the patient can be a mechanism to prevent burnout and emotional fatigue when caring of patients with diseases perceived as incurable (Hunt et al. 2017; Vaes & Muratore, 2013). This pattern may be understood in light of the compassion fatigue theory. According to this framework, compassion fatigue would emerge as a response to the emotional strain generated by caring for others, often resulting in symptoms such as emotional disengagement (Figley, 1995). Further conceptual analyses (Harris & Griffin, 2015; Jenkins & Warren, 2012) have identified sustained emotional exposure as the key antecedent, with consequences such as reduced professional performance and diminished well-being. Further research in this direction may help confirming this tentative explanation. Our study extends these findings by showing that this pattern of reduced empathy is observable in general nursing toward individuals living with schizophrenia, highlighting a potential link between professional experience and emotional regulation in stigma-related responses.
Finally, as for the behavioral dimension, our results align with those of Hori et al. (2011), in which medical professionals reported a desire for social distance. In our study, as it was done in Hori et al.’s (2011), we examined the intention of interaction in different social spheres. We also observed a reluctance to include individuals living with schizophrenia within the family in both the broader community context and among the nursing staff, which appears to be more remarkable in the intimate sphere. Yet, in our study such decreased intention to interact with individuals living with schizophrenia has been reported to be lower among nurses. Our study extends previous research by innovatively differentiate three distinct socialization spheres (public, private, and intimate) when comparing nurses and the general population, instead of merely relying on a single measure/umbrella concept of social distance. Despite statistical significance, here again the small effect size indicates that differences in the behavioral dimension were relatively minor. Following this lower acceptance levels of health professionals in both studies, one can elucubrate that a heightened recognition of the suffering experienced by individuals living with schizophrenia and the associated challenges in their condition may render them less attractive or desirable for a loved one in their daily life. This further underscores the presence of an invisible barrier preventing the complete elimination of discrimination barriers and confirms the phenomenon that the limit lies within our most intimate sphere of interaction, commonly referred to as “NIMBY: Not In My Back Yard” (Lauber et al., 2006; Loch & Rössler, 2017).
This study has a number of limitations that should be acknowledged. First, the cross-sectional design does not allow causal inferences, so the results only reflect associations at one time-point. Second, all measures were self-reported, which may have introduced response biases such as social desirability. Third, although some group differences were statistically significant, effect sizes were small, which may constrain the practical implications of these findings. Lastly, the samples were not fully balanced, as the nurse group included more women and both groups had a relatively high proportions of participants with university education (yet, this issue was controlled for); these differences may influence comparisons.
Despite the inherent value of the present study, future research should consider larger samples to confirm these effects and incorporate variables that can facilitate and deepen our understanding of the stigmatization of individuals living with schizophrenia. Moreover, collecting data on the experience of nursing staff and their burnout levels can provide additional information to understand differences in stigmatization, considering the observed relationship between years of experience and burnout (Koutra et al., 2022), and between years of experience and more positive attitudes toward schizophrenia (Katsuki et al., 2005).
Conclusions and Practical Implications
General healthcare nurses seem not to be exempt from having stigmatizing attitudes toward people living with schizophrenia. Additionally, the anxiety felt by nursing staff in the presence of these individuals can affect the work environment and the quality of care offered to them. Our results provide a useful perspective for the development of anti-stigma interventions and continuing education for general nurses without specialized training to effectively address the unique care requirements of persons living with schizophrenia. By looking at each element of stigma separately, we underline clues to discern which areas should be addressed. Economou et al. (2011) implemented interventions aimed to reduce stigma at the three levels within the broader community. Similar designs, with the necessary adaptations, may be incorporated in the healthcare setting. Interventions and continuing education for general nurses seem necessary and can serve a twofold purpose: enhancing the trust that those living with schizophrenia place in their primary nursing staff and ensuring that the nurses themselves feel comfortable and fulfilled in their professional roles.
The results of the present research support the idea that interventions aimed at promoting more positive stereotypes, such as warmth and competence, toward individuals living with schizophrenia should be developed for general nurses. Strategies of promoting counter-stereotypical exemplars have been shown to be effective in reducing prejudice toward individuals with mental disorders (Kashihara & Sakamoto, 2018; Maunder & White, 2023). In the context of schizophrenia, Economou et al. (2014) developed an evidence-based intervention targeting adolescents with counter-stereotypical narratives that successfully led to more positive beliefs about individuals living with schizophrenia and a decreased desire for social distance from them. Similar interventions could be adapted for nursing personnel to reduce stigma and foster a more accurate understanding of schizophrenia.
Leveraging our findings, the intervention should aim to enhance general nurses’ emotional responses, such as admiration and empathy, as well as positive attitudes and behaviors, while decreasing anxiety toward individuals living with schizophrenia. This can be practically achieved through both direct (participative) and vicarious interactions between nurses and individuals with schizophrenia. For example, collaborative activities have been shown to reduce stigma (e.g., Gao & Ng, 2021). Additionally, promoting empathy and positive attitudes can be achieved through videos of personal experiences of individuals living with schizophrenia. Sharing experiences with medication and its side effects highlights the humanity of the person, resulting in lower stigma scores compared to written vignettes with the same information (Amsalem et al., 2021). Ultimately, such interventions may bring empowerment, hope, and motivation for individuals experiencing schizophrenia when visiting healthcare settings, and help overcome the social stigma associated with their condition. Building on our findings and the proposed intervention strategies, future studies should also address unresolved challenges, such as how to effectively tailor anti-stigma interventions to different healthcare contexts, and how to ensure their long-term impact on both attitudes and clinical practice.
Supplemental Material
sj-docx-1-isp-10.1177_00207640251398264 – Supplemental material for The Stigma of Schizophrenia: Differences in Cognitive, Affective, and Behavioral Responses between Nurses and Broader Community
Supplemental material, sj-docx-1-isp-10.1177_00207640251398264 for The Stigma of Schizophrenia: Differences in Cognitive, Affective, and Behavioral Responses between Nurses and Broader Community by Sheila Azcoitia, Itziar Alonso-Arbiol and Magdalena Bobowik in International Journal of Social Psychiatry
Footnotes
Author Contributions
All authors listed meet the authorship criteria according to the International Committee of Medical Journal Editors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by research grants by the Basque Government (Consolidated Groups call: IT1598-22 and IT1797-26) and Ramón y Cajal Program, Grant Number: RYC2021-032887-I financed by MCIN/AEI/10.13039/501100011033 and European Union Program NextGeneration EU/PRTR awarded to M.B.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated and analyzed during the conduct of this study are not public due to confidentiality reasons, as specified in the ethical consent approved by the university.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.