
Abstract
Background:
Parental socioeconomic factors are associated with mental health outcomes already during childhood, but gender differences in these connections have rarely been studied.
Aims:
We explored the associations between household income and severe mental health disorders requiring psychiatric inpatient hospital care, with particular focus on gender differences.
Methods:
In this national register-based cohort study, we followed over 1.6 million children and adolescents born in Finland between 1991 and 2020 until first psychiatric hospital admission, moving away from parents, death, emigration from Finland or the end of 2020, whichever time came first. We calculated age- and gender-specific incidence rates (IRs) for first admissions. In order to evaluate gender differences and the magnitude of association between income and psychiatric hospital admission, we fitted multivariable Poisson regression models and calculated incidence rate ratios (IRRs) and 95% confidence intervals.
Results:
In total, 2.1% of the study population were admitted to psychiatric hospital for the first time within the specified period. Among girls in all income deciles, IRs distinctly peaked during adolescence. Among boys, IRs started to increase earlier, especially in the lowest income deciles, and there was no steep peak during adolescence in any income group. Lower household income was associated with higher risk for psychiatric hospital admission, and this association was steeper for boys (IRR 3.18 [2.87–3.53] than for girls (IRR 2.15 [1.97–2.35]) in the lowest compared to the highest income decile, after adjusting for potential confounders.
Conclusion:
Our results indicate that low income may play a more prominent role in severe mental disorders among boys, whereas adolescence emerges as a critical period for girls, regardless of their household income levels.
Introduction
Mental disorders account for a high proportion of the disease burden in young people in all societies and have significant human and economic consequences (‘Global, Regional, and National Burden of 12 Mental Disorders in 204 Countries and Territories, 1990–2019’, GBD 2019 Mental Disorders Collaborators [2022]). The increased need for mental health treatment already during childhood and adolescence has not been met even in high-income countries, which is a major public health issue worldwide (Patel et al., 2007).
Socioeconomic status as a determinant for mental health has been established in low- and middle-income countries and in the Nordic countries, where the population generally has relatively equal access to health services (Kirkbride et al., 2024). The indicators of socioeconomic status reflect different aspects of the environment. Of these, income most directly measures the material resources available in everyday life, and can capture the dynamic changes (Galobardes, 2006). Previous research has rather consistently reported that growing up in low-income circumstances is associated with an increased risk of developing a mental disorder: children with parents from the lowest income percentile are estimated to be 3 to 4 times more likely to experience mental disorders compared to those in the highest income percentile (Kinge et al., 2021). The association between socioeconomic factors and mental disorders has been observed in all diagnostic groups, except in the case of eating disorders (Hakulinen et al., 2020; Kinge et al., 2021), and this link persists into adulthood (Evensen et al., 2021; Hakulinen et al., 2020).
In addition, gender differences in mental disorders are well-established. Girls are more frequently diagnosed with adolescent-onset anxiety and mood disorders (Campbell et al., 2021; Dalsgaard et al., 2020; Zahn-Waxler et al., 2008) and boys with childhood-onset conduct disorders and neuropsychiatric disorders (Zahn-Waxler et al., 2008). Due to these distinctions, gender-specific investigation of risk factors is well-founded. Evidence concerning gender differences in risk factors related to socioeconomic background is limited.
In this study, we investigated severe mental disorders among children and adolescents by examining psychiatric hospital admissions provided in cases of the most serious psychiatric symptoms and significant functional impairments or risk of causing harm to themselves or others (Kronström et al., 2023). Using nationwide registry data, we studied the incidence of psychiatric hospital admissions as well as disparities related to gender and the family’s socioeconomic status, measured by household income. We reported age- and gender specific incidence rates of admissions. We hypothesised that psychiatric hospital admissions would increase particularly during childhood in boys, and during adolescence in girls, and that the increase would be greater in the lowest income groups.
Methods
Results
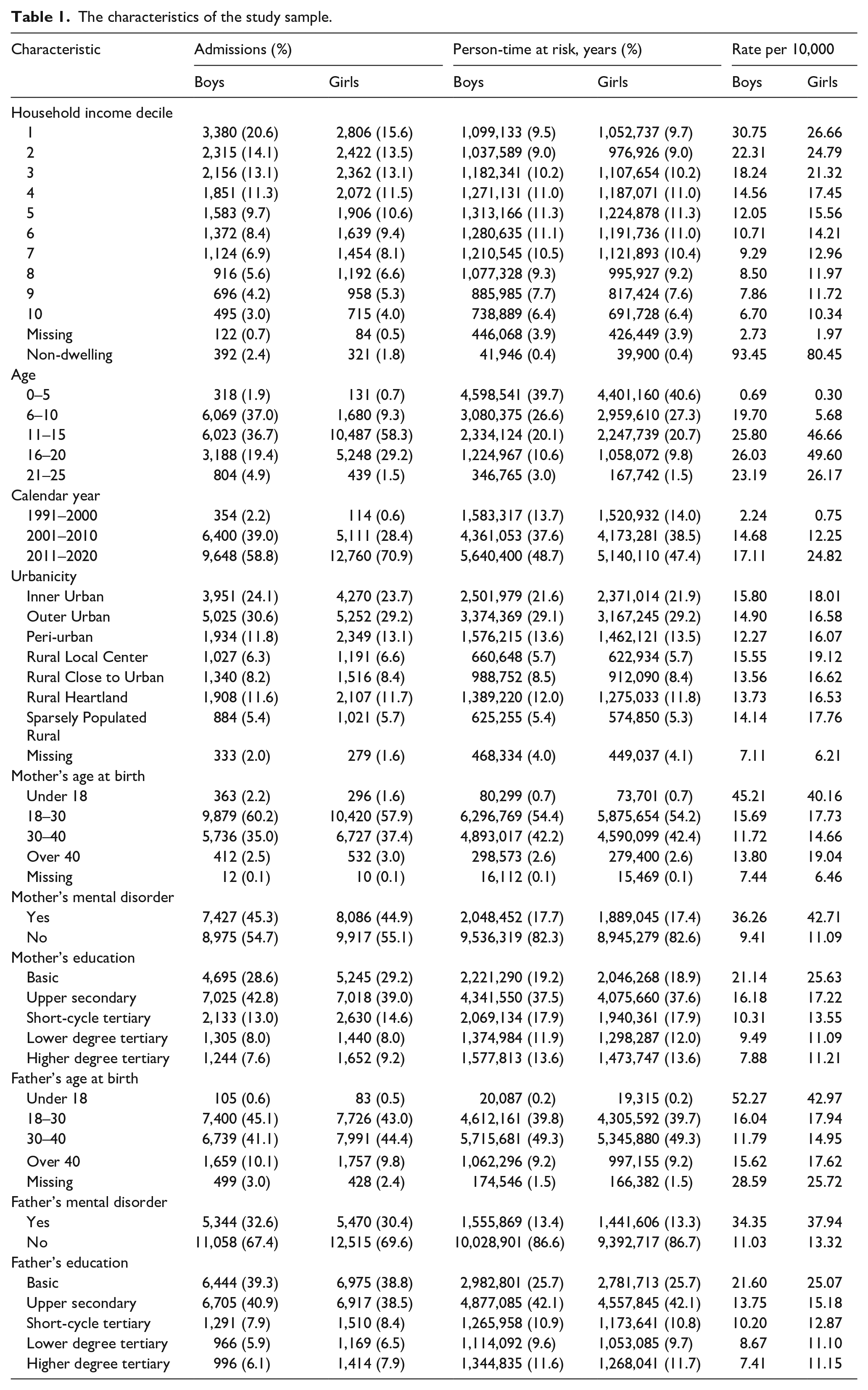
In total, the study population included 1,643,611 children and adolescents (48.9% girls), contributing over 22.4 million person-years at risk. A total of 2.1% of the study population (34,387 persons) had a first psychiatric hospital admission during the research period. Girls accounted for 52.3% of the admissions, while boys accounted for 47.7%. At the ages of 15, 18, 20 and 24, 99.6%, 88.3%, 47.2% and 6.5% of the study population were still living with at least one of their parents, respectively. The characteristics of the study sample are described in Table 1.
The characteristics of the study sample.
Gender-specific incidence rates of first psychiatric hospital admissions due to mental disorder during childhood and adolescence are shown in Figure 1. Among boys, the incidence rate increased during childhood, after which it remained at a quite steady level. Among girls, the incidence rate increased rapidly from age 12, peaking at the age of 15 years and settling near the same level as boys at the age of 20 years. Of those who were admitted, 67.6% had one, 27.1% two and 5.3% three or more diagnoses. Boys had a higher rate of hospital admissions due to substance use and psychotic disorders from age 15 onwards. Behavioural disorders were more common among boys at ages 6 to 12 and among girls at ages 13 to 17. Girls had a higher rate of mood and anxiety disorders and behavioural syndromes from age 13 onwards. Mental disorders due to physiological conditions, personality disorders and intellectual disabilities accounted for only a minor proportion (0.1%, 1.1% and 1.1%) of the admissions and are therefore not presented in the figure.
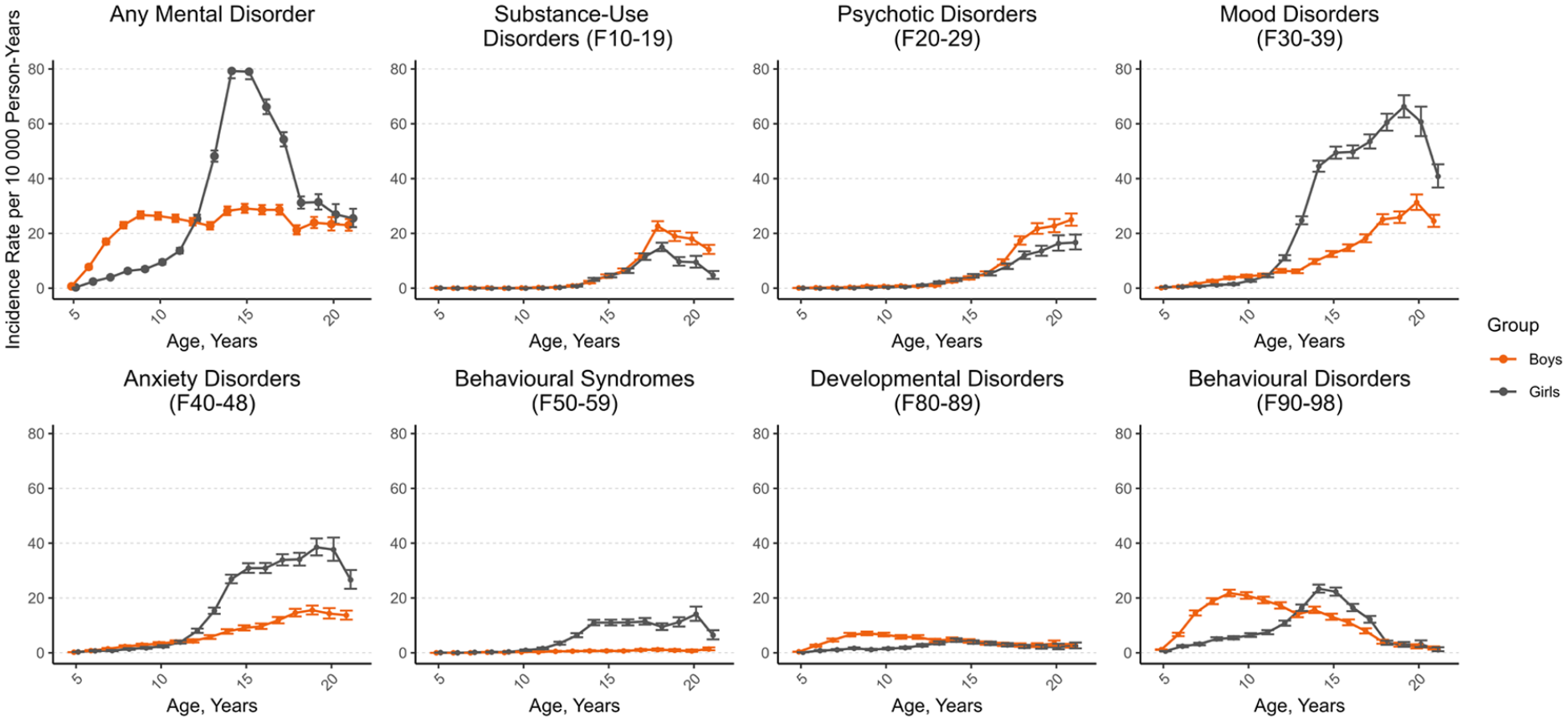
Incidence rate of first psychiatric hospital admissions by age, gender, and diagnostic group.
Age- and income-specific incidence rates of psychiatric hospital admissions due to any mental disorder diagnosis for boys and girls are presented in Figure 2. The incidence rate was highest in the lowest income decile group after the age of 5 throughout childhood and adolescence, particularly in boys. In girls, a peak in the incidence rate emerged around the age of 15 years in all income deciles.
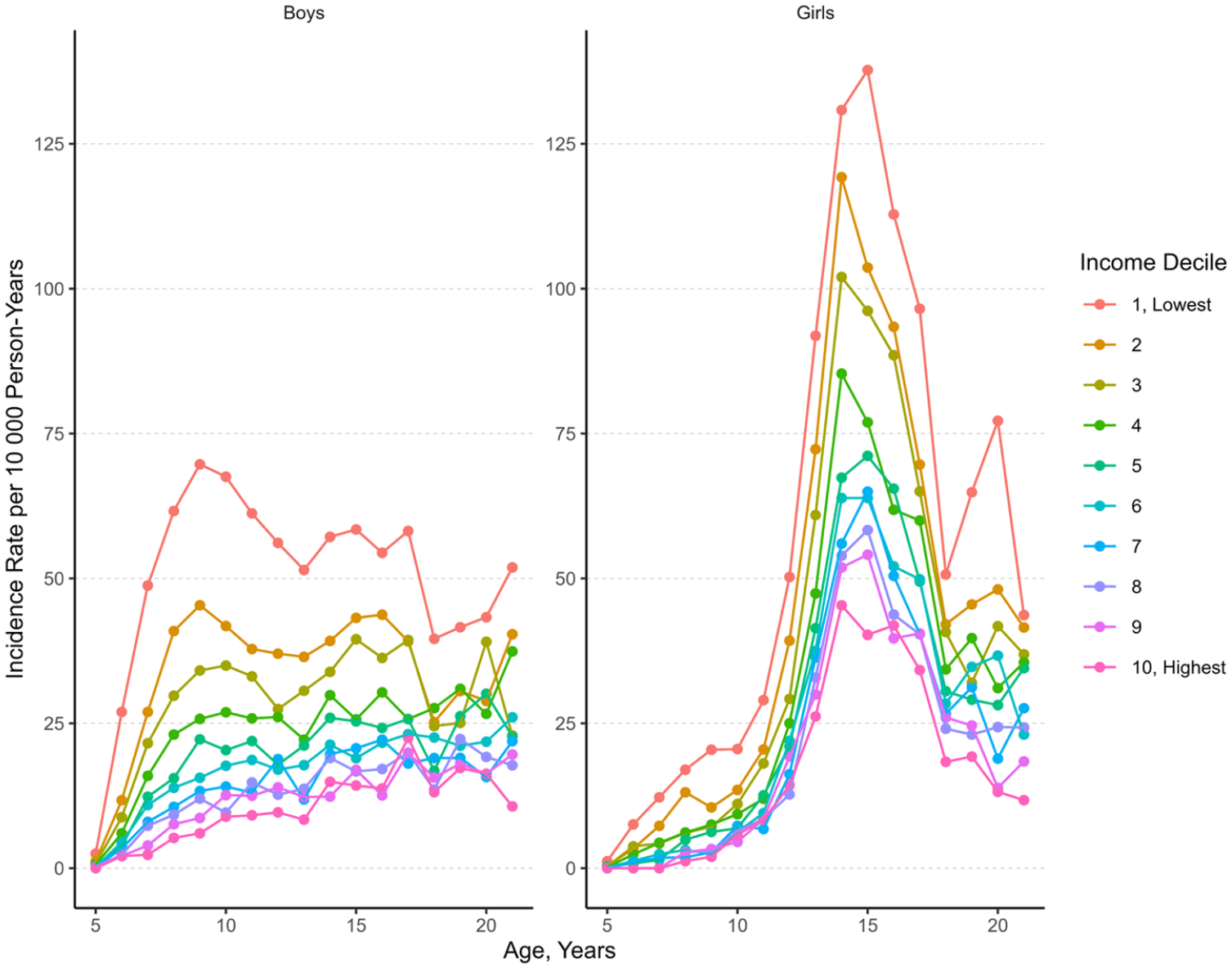
Incidence rate of first psychiatric hospital admissions by age, gender and household income.
The results of Poisson regression models are presented in Table 2. Gender comparisons for income-related associations are shown in Figure 3(a), and for age-specific incidence rate ratios in Figure 3(b). In a minimally adjusted model including income decile and age as exposures, low income was associated with higher IRR for psychiatric hospital admission (in the lowest income decile compared to the highest IRR = 6.07, 95% CI [5.50, 6.69] among boys and IRR = 3.56, 95% CI [3.27, 3.87] among girls). In a model adjusted for potential confounders including urbanicity, calendar year and parental age, education and mental disorder, the association between income and risk for psychiatric hospital admission was attenuated but remained (among boys IRR = 3.18, 95% CI [2.87, 3.53] in the lowest income decile compared to the highest and among girls IRR = 2.15, 95% CI [1.97, 2.35] in the lowest income decile compared to the highest). Furthermore, living in an urban area, parental mental disorder, mother’s low education, mother’s younger age and father’s advanced age were associated with increased risk for psychiatric hospital admission for both boys and girls. Mother’s advanced age increased the risk only for girls, and father’s lower education and younger age only for boys.
Risk factors for psychiatric hospital admissions.
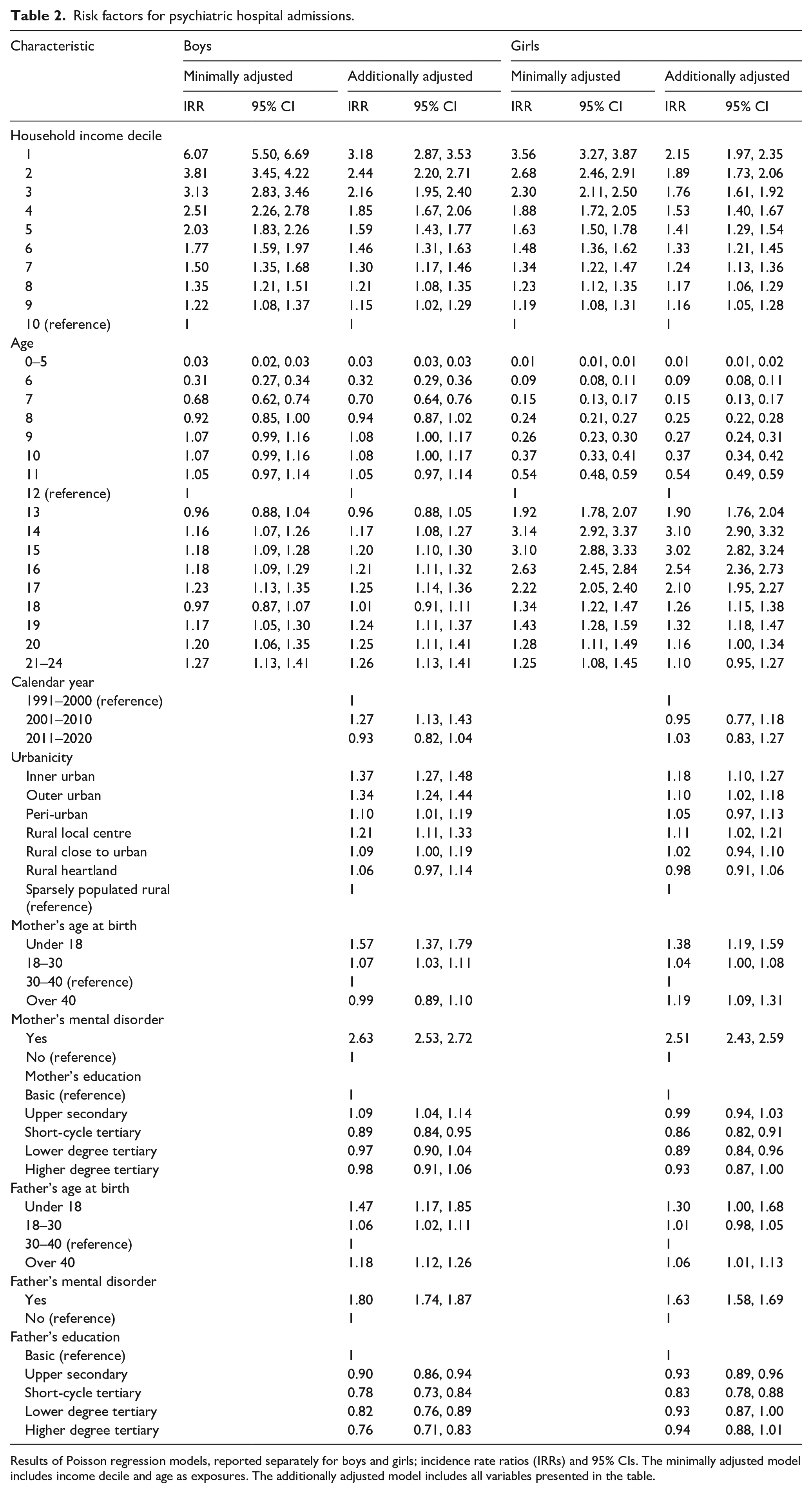
Results of Poisson regression models, reported separately for boys and girls; incidence rate ratios (IRRs) and 95% CIs. The minimally adjusted model includes income decile and age as exposures. The additionally adjusted model includes all variables presented in the table.
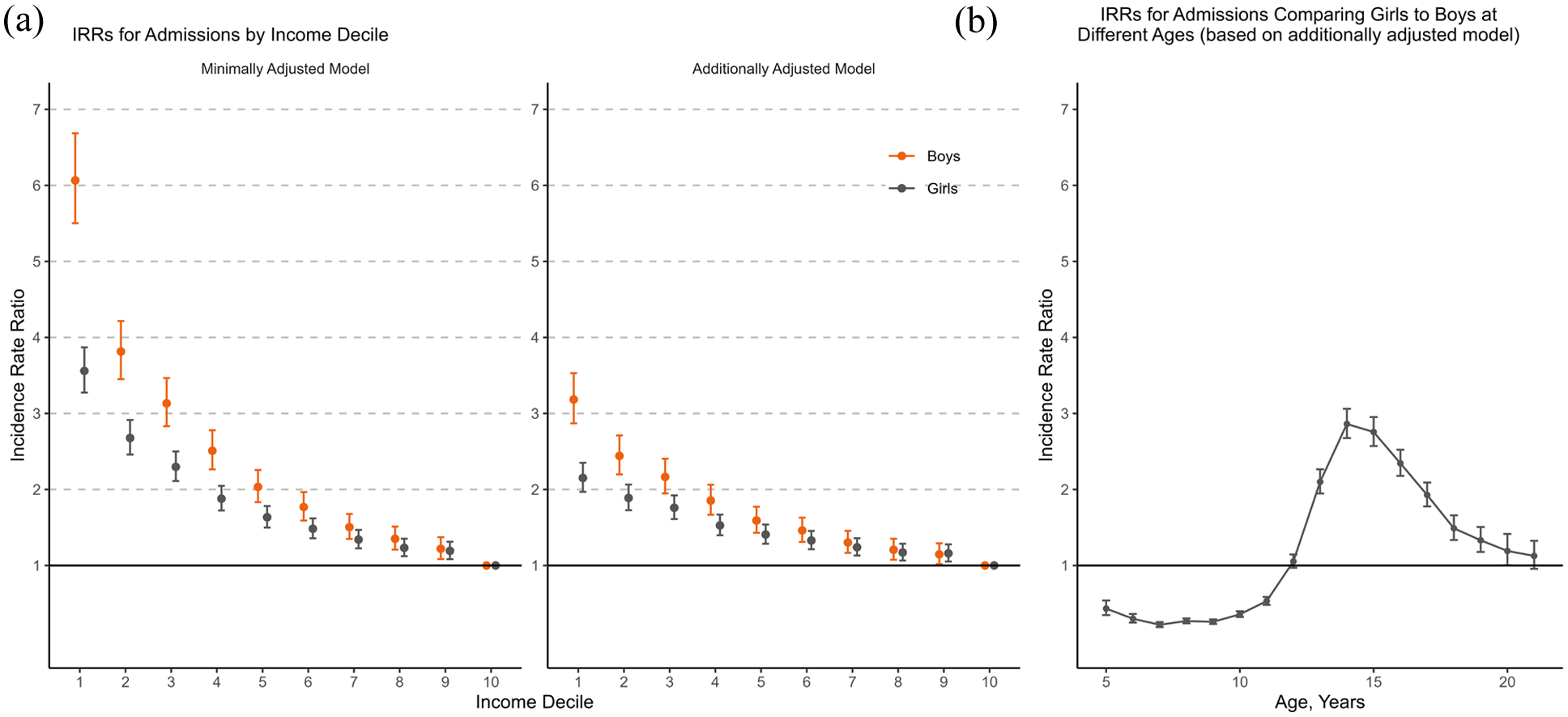
(a) Incidence rate ratios (IRRs) for first psychiatric hospital admissions by income decile, reported separately for boys and girls. (b) Incidence rate ratios (IRRs) for first psychiatric hospital admissions comparing girls to boys at different ages. Incidence rate ratios (IRRs) calculated using Poisson regression. The minimally adjusted model includes income decile and age as exposures. The additionally adjusted model includes also calendar year, urbanicity and parental age, education, and mental disorder. Income decile refers to equivalised disposable income deciles of a household, with 1 indicating the lowest income decile and 10 the highest (reference group); error bars, 95% CIs.
Discussion
Our findings suggest that there are gender differences in psychiatric hospital admissions during childhood and adolescence. Low income appears to play a more prominent role among boys, whereas adolescence emerges as a critical period for girls, regardless of their household income levels. To the best of our knowledge, this study is the first to highlight the gender dependence of the risk factors for psychiatric hospital admissions.
The incidence of hospital admissions among boys began to increase during childhood, after which their levels remained relatively stable. Conversely, among girls, the incidence of hospital admissions peaked rapidly during adolescence. At age 15, girls had over 2.5 times the number of first psychiatric hospital admissions in comparison to boys. Previously, gender-specific frequencies of mental disorders have often been studied in selected diagnostic groups. Among studies that have examined the full diagnostic spectrum, Swedish (Yang et al., 2024) and Danish (Dalsgaard et al., 2020) register-based studies reported a higher incidence of any mental disorder during adolescence among girls. In addition, a British study examining psychiatric hospitalisations during the years 1998-2004 reported higher rates among girls starting from the age of 13 (James et al., 2010). Our results are in line with this finding, indicating a pronounced increase in adolescent girls’ psychiatric hospital admissions from age 12. Register-based studies (Dalsgaard et al., 2020; Yang et al., 2024) have found that the incidence of any mental disorder increased during adolescence also among boys. However, in our study, the incidence of psychiatric hospital admissions remained at a quite steady level among boys. This raises the question of whether girls are more susceptible to the most severe mental disorders during adolescence.
The gender- and age distribution of diagnoses accounting for psychiatric hospital admissions is consistent with previous studies. Boys displayed a preponderance of behavioural disorders at ages 6 to 12, whereas girls showed a preponderance at ages 13 to 17. Mood and anxiety disorders and behavioural syndromes increased and became remarkably more common in girls from age 13. These findings are consistent with those of previous studies, which have identified male preponderance in emotional disorders before the age of 12 years, followed by a shift towards female preponderance (Wesselhoeft et al., 2015). Moreover, it has been proposed that girls might experience a delayed detection of mental disorders, particularly neurodevelopmental disorders (Dalsgaard et al., 2020). The existing literature suggests that boys may have a general pre-pubertal vulnerability to a broader spectrum of mental disorders (Dalsgaard et al., 2020; Wesselhoeft et al., 2015), and our findings align with this hypothesis.
The association between income and risk for psychiatric admission remained after adjusting for urbanicity, calendar year, parental mental disorder, parental education and parental age. Gender did not function as an effect modifier and the association between household income and risk for psychiatric hospital admission was observed in both genders, although there were differences in magnitude. After adjusting the models for potential confounders, boys in income deciles 1-3 had higher IRRs for hospital admissions than girls. To the best of our knowledge, results indicating boys in low-income groups to be more liable to hospital-treated mental disorder than girls have not been reported earlier. An income gradient for children under 18 years has been established in psychiatric hospital admissions (Suokas et al., 2020) as well as for mental disorders treated in all health services (Kinge et al., 2021). However, in the study on hospital admissions, the models were not adjusted for parental characteristics. Previous findings on gender differences in these associations are mixed. A systematic review of socioeconomic inequalities and mental health during childhood and adolescence summarised that there were no substantial gender differences (Reiss, 2013). It has been reported that socioeconomic inequalities in childhood mental disorders in general would be stronger for boys, although in the cited study income was only partly associated with an increased risk for mental disorders after adjusting for control variables (Vaalavuo et al., 2022). In addition, one study on mental disorders across the whole lifespan reported that the incidence rate differences between the sexes were greater among individuals with lower socioeconomic status (Yang et al., 2024).
There may be several explanations for results concerning gender differences in psychiatric hospital care. The pronounced incidence peak among girls during adolescence may be attributed to various gendered factors, including hormonal changes during puberty and early maturation (Zahn-Waxler et al., 2008), exposure to sexual discrimination (Klonoff et al., 2000), and pressures related to school performance (Wiklund et al., 2012) and physical appearance (Grabe et al., 2007). Furthermore, gender disparities in overall mental health tend to be more prevalent in wealthier and more gender-equal countries such as the Nordic countries, which has been attributed to the dual requirements stemming from both modern and traditional gender roles (Campbell et al., 2021; Yu, 2018).
Our results raise the question of whether boys are more vulnerable to socioeconomic adversity experienced during childhood, and whether higher household income may exert a more pronounced protective effect on boys. Some research on health economics posits that adverse social environments during childhood potentially lead to poorer outcomes in disciplinary problems and educational achievement (Autor et al., 2019), and adult employment among males (Chetty et al., 2016). Some evidence also suggests that socioeconomic risk factors are more notably pronounced in externalising disorders, which have a higher prevalence among boys during childhood (Peverill et al., 2021; Reiss, 2013).
The causal relationship between socioeconomic status and mental health is debated. Economic hardship can act as a stressor impacting mental health, while mental disorders may limit socioeconomic achievement (Mossakowski, 2014; Reiss, 2013). Childhood poverty has been established to be linked with dysregulated stress responses (Evans & Kim, 2007). Economic strain may affect child development through stress, interparental conflicts and parenting behaviours, even in welfare states with social security (Conger & Ge, 1994; Solantaus et al., 2004). Economic disadvantage may affect access to early interventions, with parents having a significant role in seeking for and participating in treatment. In Finland, mental health services are free for children, but the visits may still require everyday arrangements and resources from the parents, and place burdens on families. Children from low-income families may have less access to high-quality mental health services (Hodgkinson et al., 2017). Studies on adults suggest that low-income individuals face more barriers to care, although the evidence on parental socioeconomic factors and help-seeking for children is contradictory (Ryan et al., 2015; Sareen et al., 2007; Zwaanswijk et al., 2003).
This study has several strengths, namely that the results are population-based and free of health-related selection and non-participation biases. It also encounters some important limitations. First, our measures of financial resources may not describe the entirety of a family’s economic reality. We used equivalised household income as a measure and did not consider other forms of wealth and property, which are not captured with the national statistics. Moreover, lack of social support may be an important explanatory factor, but it is not available in the data. Nevertheless, household income probably serves as a sensitive indicator of the available material resources that parents can invest in their children (Galobardes, 2006). Second, our examination focused solely on one Nordic country, which may impact the applicability of the results. Moreover, the presence of extensive public health care and numerous free services in Finland may not reflect the health care realities of other countries. Third, the study employed a binary variable of allocated gender in population registers and did not differentiate the subjects by their experienced gender or identify gender minorities. It would be important to consider this issue in future research, since for example, transgender identity is associated with suicidal ideation and suicide attempts among adolescents and young adults (Erlangsen et al., 2023), and presumably therefore with a higher risk for psychiatric hospital care. Lastly, it is worth acknowledging that even high-quality register data are subject to certain constraints, including some uncertainty concerning the validity of the diagnoses (Sund, 2012). However, this study utilised psychiatric hospital admissions which signal significant concerns for mental well-being. Additionally, the coverage of national registry data is not as comprehensive for the migrant populations. In the context of income, it would nevertheless be important to consider, for example, precarious employment within immigrant populations, the key dimensions of which are not adequately captured in registries (Gauffin, 2022). This study excluded foreign-born individuals and those whose parents were both foreign-born, so the results are not generalisable to individuals whose parents are not of Finnish origin. In Finland, immigrant populations constitute a heterogeneous group with varying levels of pre-migration stressors and post-migration adversities (OECD, 2024). It would be important to include and focus on migrant populations in future research, given their unique psychosocial and mental health challenges, particularly in the case of individuals migrating from conflict-affected areas (Hazer & Gredebäck, 2023).
In conclusion, our findings on psychiatric hospital care indicate that girls exhibit vulnerability during adolescence irrespectively of their household income. In boys, household income plays a relatively more important role. These results suggest that low income as a risk factor for hospital-treated mental health disorder is gendered from an early age and highlights the need to consider a gender-informed approach in treatment and prevention. Removing barriers and ensuring equitable access to preventive mental health care for children and adolescents from low-income families might help in mitigating the onset of acute psychiatric conditions, especially in boys. The age-related vulnerability observed in adolescent girls underscores the importance of better recognition and management of this issue in mental health service strategies. Efforts to address mental disorders should be extended to broader societal and political reforms aimed at preventing their emergence.
Footnotes
Author contributions
Study concept and design: All authors
Acquisition, analysis or interpretation of data: All authors
Drafting of the manuscript: All authors
Critical revision of the manuscript for important intellectual content: All authors
Statistical analysis and figures: Suokas K, Nieminen V, Autio R
Study supervision: Pirkola S, Hakulinen C
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: C.H. was supported by the Academy of Finland (354237) and the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (MENTALNET, 101040247). V.N., K.S. and S.P. were supported by The Strategic Research Council (SRC) in the Academy of Finland under the Young Despair project (3121352602). V.N. was supported by MLL research foundation. The funders of the study had no role in study design, data collection, analysis or interpretation nor in writing the paper.
Ethical considerations
This study was approved by Ethics Committee of the Finnish Institute of Health and Welfare (THL/730/6.02.01/2018). Informed consent is not required in register-based studies in Finland. The study followed the guidelines of the Declaration of Helsinki.
Data availability
The data used in this study is from the National Institute of Health and Welfare (http://www.thl.fi) and Statistics Finland (www.stat.fi). Restrictions apply to the availability of these data, which were used under license for this study. Inquiries to secure access to data should be directed to data permit authority Findata (![]() ).
).